
Abstract
Study Design
Retrospective cohort study.
Objective
Lumbar segmental instability is a key factor determining whether decompression alone or decompression and fusion surgery is required to treat lumbar spinal stenosis (LSS). Some recent reports have suggested that facet joint effusion is correlated with spinal segmental instability. The aim of this study is to report the effect of facet effusion without radiographic segmental instability on the outcome of less-invasive decompression surgery for LSS.
Methods
Seventy-nine patients with LSS (32 women, mean age: 69.1 ± 9.1 years) who had no segmental instability on dynamic radiographs before undergoing L4–L5 microsurgical decompression and who were followed for at least 2 years postoperatively were analyzed. They were divided into three groups on the basis of the existence and size of L4–L5 facet effusion using preoperative magnetic resonance imaging: grade 0 had no effusion (n = 31), grade 1 had measurable effusion (n = 35), and grade 2 had large effusion (n = 13). Japanese Orthopedics Association (JOA) score, visual analog scale (VAS), and the Short-Form (SF)-36 scores were recorded preoperatively and 12 and 24 months postoperatively.
Results
JOA score; VAS of low back pain, leg pain, and numbness; and SF-36 (physical component summary and mental component summary) scores did not differ significantly between the three groups in every terms (p = 0.921, 0.996, 0.950, 0.693, 0.374, 0.304, and 0.624, respectively, at final follow-up).
Conclusion
In the absence of radiographic instability, facet joint effusion has no effect on the outcome of less-invasive decompression surgery.
Introduction
Surgeries for symptomatic lumbar spinal stenosis (LSS) are more effective than continued conservative treatment when the latter has failed for 3 to 6 months. 1 Nowadays, there are two main methods to treat LSS: (1) decompression and (2) decompression and fusion. Whether the spinal fusion is needed in addition to a decompression surgery for symptomatic LSS may depend on the stability of the involved spinal segments. Several studies support the application of decompression and fusion in patients with lumbar segmental instability. 2,3 For this reason, it is important to accurately identify patients who have lumbar segmental instability in addition to spinal stenosis for determining the most appropriate surgical treatment approach. A lot of imaging methods including traction–compression radiography, 4 dynamic magnetic resonance imaging (MRI), 5 and three-dimensional dynamic computed tomography have been reported to be useful for evaluating instability in the lumbar spine. 6 However, lumbar instability evaluated using weight-bearing lateral flexion–extension radiographs as anteroposterior translation, spondylolisthesis, and segmental kyphosis are accepted as the gold standard for evaluating segmental instability. 7,8
Several studies have suggested that fluid collection within the lumbar facet as detected on MRI is indicative of segmental instability. 9 –12 They concluded that facet joint effusion on MRI should raise an increased suspicion of lumbar instability. Although most of these reports were designed to verify the relationship between facet effusion and radiographic instability, surgeons may hesitate to perform lumbar decompression surgery with facet joint effusion, even though radiographic evaluation shows no instability. However, we hypothesized that excess facet fluid without radiographic instability has no impact on the results of minimally invasive decompression surgery. To verify this hypothesis, the purpose of this study was to determine whether facet effusion affected the outcome of minimally invasive decompression surgery in patients with LSS with no radiographic instability.
Materials and Methods
This study protocol was approved by the Institutional Review Board of Osaka City General hospital. Written informed consent was obtained from the patients for publication of current research and any accompanying images.
Patients
This research was conducted with retrospective analysis of prospectively collected data. Patients with symptomatic LSS but no radiographic instability who experienced mainly lower-extremity symptoms and claudication and for whom conservative treatments were unsuccessful were candidates for a kind of minimum invasive lumbar decompression surgery: microsurgical bilateral decompression via a unilateral approach (MBDU). 13,14 The surgical procedures of MBDU is as follows. The laminotomy was performed on the side of approach in the area of the ligamentum flavum insertion, and resection of the articular process was performed in a trumpeted fashion to the inner aspect of the pedicle, with slight lateral tilting of the microscope. After the side of approach had been completely decompressed, the operating table and microscope were tilted ∼15 degrees to observe the contralateral side. The basal part of the spinous process of the caudal half of the cranial lamina and a small cranial portion of the caudal lamina were removed with a high-speed drill. Then, the contralateral lamina was undercut with a high-speed air drill, leaving the ligamentum flavum in place as protection for the dural sac and nerve root. Following sufficient resection of the bony segment, the ligamentum flavum was removed en bloc with a curette while protecting the dural sac and contralateral nerve root with a patty. Adequate decompression of the contralateral side was confirmed by recognition of the inner aspect of the contralateral pedicle. Radiographic instability was evaluated using dynamic radiographs, and the absence of instability was defined by the following three criteria 15 : <25% slip of L4–L5 in neutral position, <3 mm in translation between flexion and extension bending, and <5 degrees of local kyphosis angle in flexion position. Surgery for revision cases, disk herniation cases, and cases followed less than 2 years after operation were excluded. From January 2008 to December 2010, a total of 378 patients were surgically treated for LSS and followed for at least 2 years. Of these, 120 patients underwent decompression and fusion surgery due to segmental instability as defined by the above criteria. Of the remaining 258 patients, 179 underwent MBDU for multilevel decompression or decompression at levels other than L4–L5. Finally, a total of 79 cases fulfilled our investigation criteria of not having segmental instability and having undergone MBDU at L4–L5 only and then at least 24 months of follow-up (Fig. 1). These 79 patients included 32 women and 47 men who had a mean age of 69.1 ± 9.1 years (Table 1).
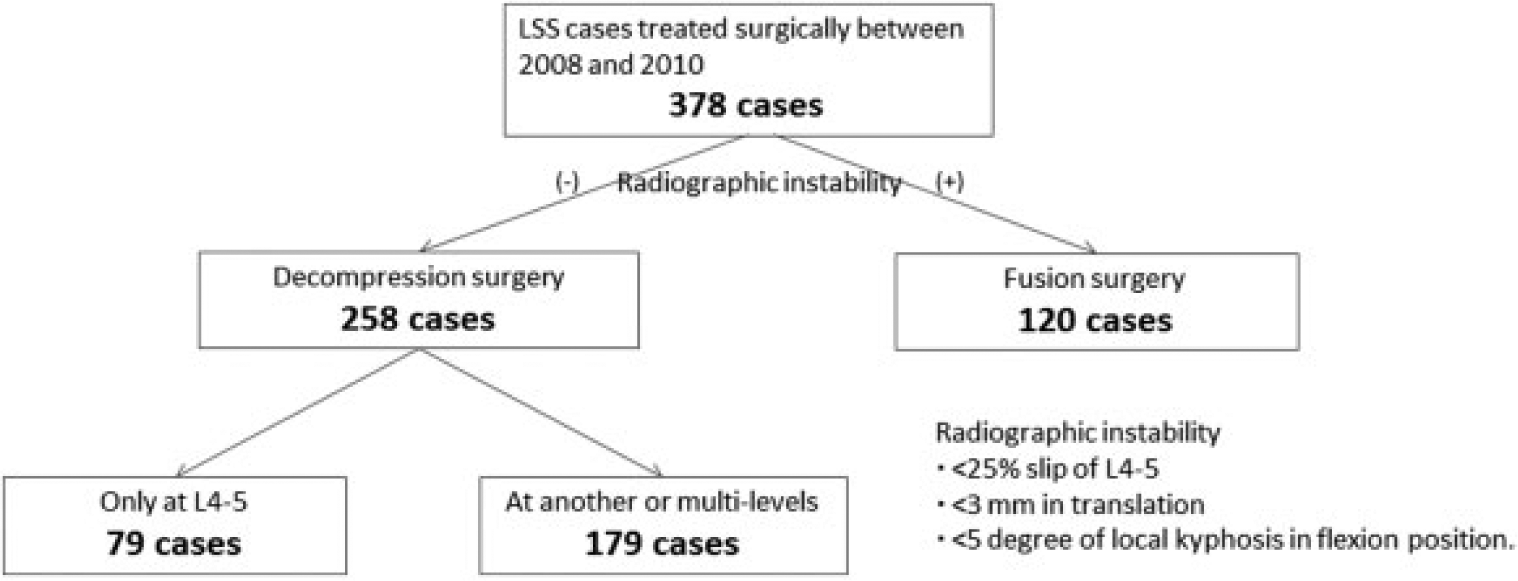
Diagram of patients with lumbar spinal stenosis treated by surgery from 2008 to 2010.
Patient demographics of all cases
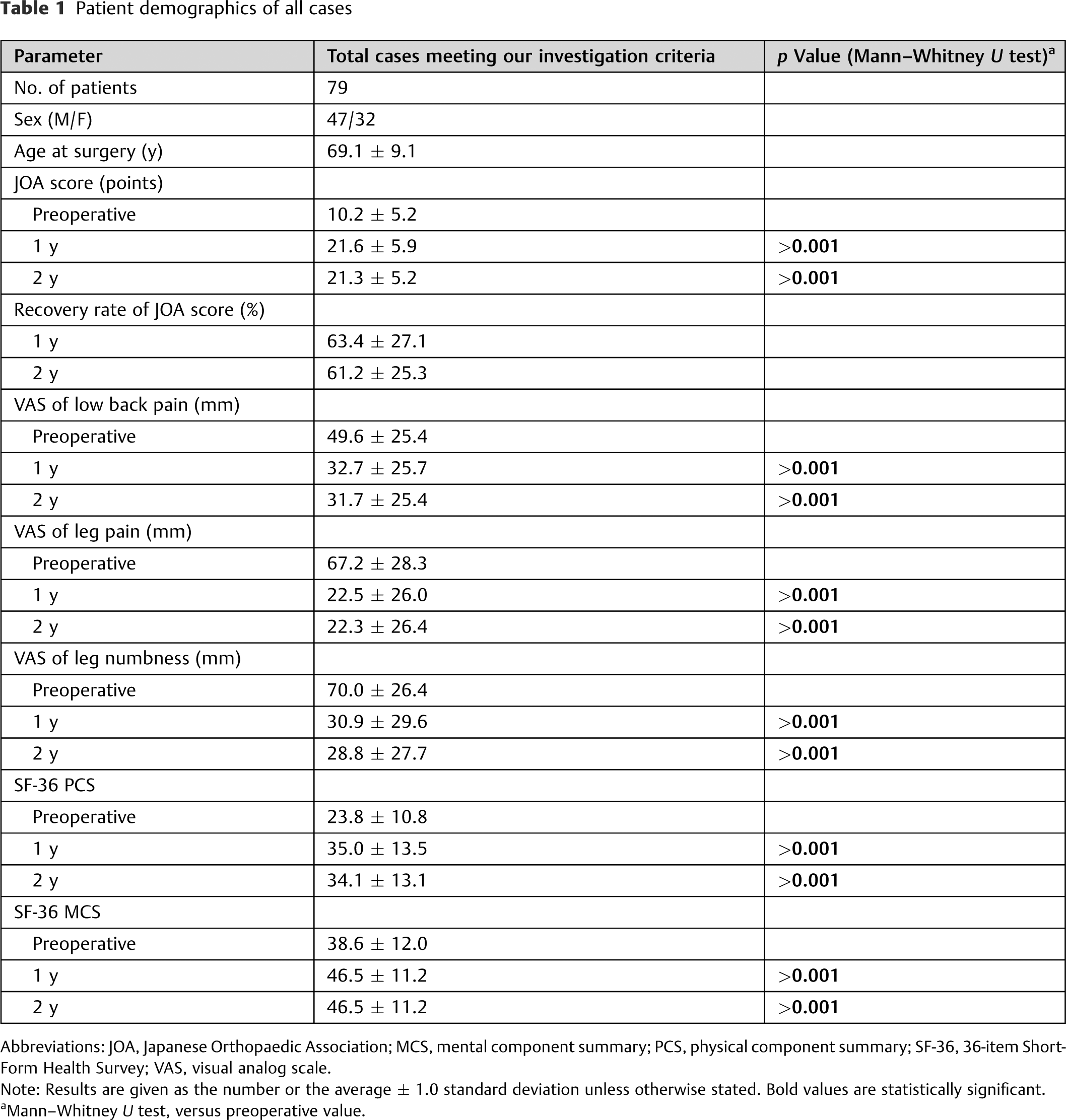
Abbreviations: JOA, Japanese Orthopaedic Association; MCS, mental component summary; PCS, physical component summary; SF-36, 36-item Short-Form Health Survey; VAS, visual analog scale.
Note: Results are given as the number or the average ± 1.0 standard deviation unless otherwise stated. Bold values are statistically significant.
Mann–Whitney U test, versus preoperative value.
Surgical Outcome
For all patients, surgical outcomes were evaluated before surgery and 12 and 24 months after surgery according to the Japanese Orthopedics Association (JOA) scores. The recovery rate was calculated using the formula established by Hirabayashi et al 16 : (postoperative JOA score − preoperative JOA score)/(17 − preoperative JOA score) × 100 (%). Scores on two patient-oriented questionnaires, the visual analog scale (VAS) of pain and numbness of lower extremities and low back pain, and the 36-item Short-Form Health Survey (SF-36) for evaluating health-related quality of life. 17
Evaluation of Facet Effusion on Magnetic Resonance Imaging
Based on the classification scheme described by Chaput et al, 9 facet joint effusion was defined as a measurable, curvilinear, high-intensity signal within the facet joint, which closely matched that of cerebrospinal fluid, on axial T2-weighted MRI images. Measurements were taken perpendicular to the apparent joint line, and the largest value was recorded as the effusion size. Only bilateral L4–L5 facets were evaluated, and the worst grade for either side of each joint was recorded. According to the presence and size of the effusion, the patients were divided into three groups by the following grades: grade 0 had no effusion, grade 1 had measurable effusion (<1.5 mm), and grade 2 had large effusion (≥1.5 mm; Fig. 2).

Representative magnetic resonance images of facet joints showing effusions. (A) Grade 0 had no effusion. (B) Grade 1 had measurable effusion (<1.5 mm). (C) Grade 2 had large effusion (≥1.5 mm).
Statistical Analysis
Statistical analyses were performed with SPSS, version 12.0.1, for a personal computer (SPSS Inc., Chicago, Illinois, United States). Descriptive statistics were calculated, including the frequencies for categorical and ordinal variables and the means, medians, standard deviations, and ranges for continuous variables. One-way analysis of variance or Fisher exact test was used to analyze significant differences among the three groups at each point. A p value < 0.05 was considered to indicate statistical significance.
Results
According to the MRI evaluation in the 79 patients included in this study, 31 patients had grade 0 effusion, 35 patients had grade 1 effusion, and 13 patients had grade 2 effusion. Table 2 shows the demographics of these three groups. There are no significant differences in sex, age, and each preoperative surgical score between these three groups. Table 3 shows the preoperative and postoperative surgical outcomes of these three groups. None of the 79 patients experienced major complications following MBDU, and no patient required additional surgery at the lumbar spine, such as a fusion procedure, during the follow-up period. The average JOA scores, recovery rate of JOA scores, VAS, and SF-36 at 1 and 2 years postoperatively did not differ significantly between these three groups.
Demographics of three groups divided by the amount of facet effusion
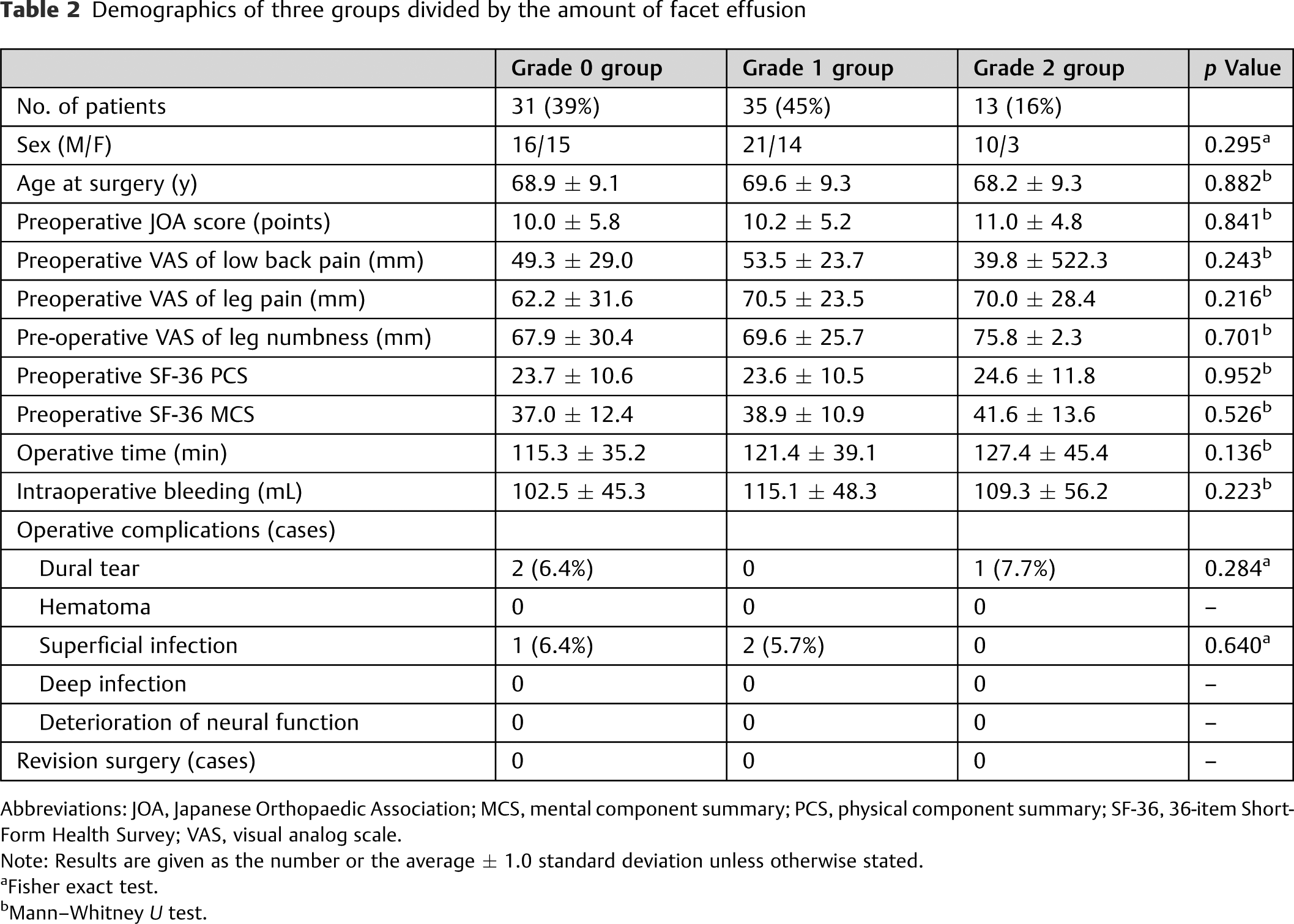
Abbreviations: JOA, Japanese Orthopaedic Association; MCS, mental component summary; PCS, physical component summary; SF-36, 36-item Short-Form Health Survey; VAS, visual analog scale.
Note: Results are given as the number or the average ± 1.0 standard deviation unless otherwise stated.
Fisher exact test.
Mann–Whitney U test.
Pre- and postoperative surgical outcomes of the three groups
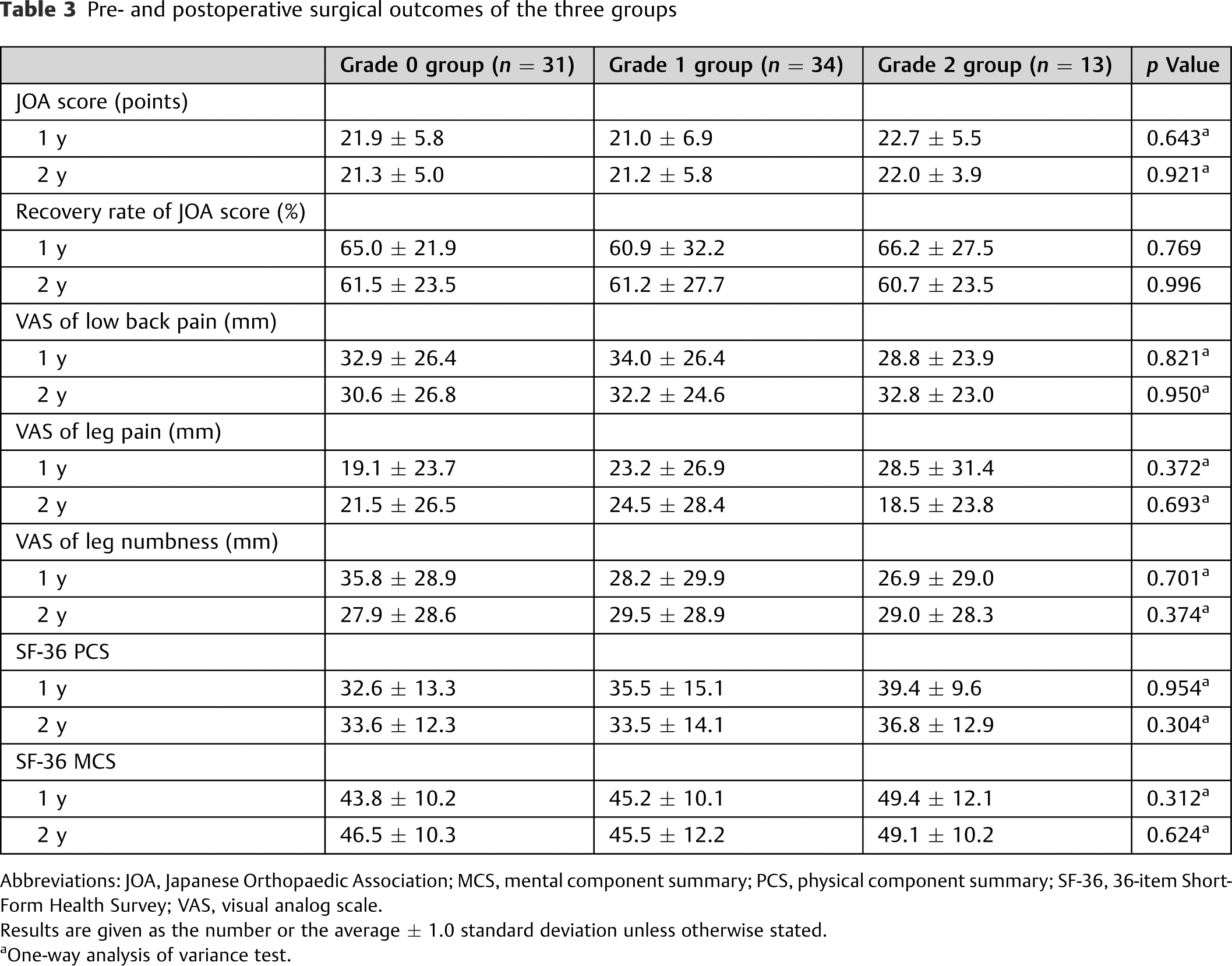
Abbreviations: JOA, Japanese Orthopaedic Association; MCS, mental component summary; PCS, physical component summary; SF-36, 36-item Short-Form Health Survey; VAS, visual analog scale.
Results are given as the number or the average ± 1.0 standard deviation unless otherwise stated.
One-way analysis of variance test.
Discussion
Previous studies have suggested that facet joint effusion is a sign of lumbar segmental instability. This hypothesis was first studied by Chaput et al in 2007 9 and later confirmed by Rihn et al, 10 Cho et al, 11 and Lattig et al. 12 Rihn et al reported a close linear association between the facet fluid index and the degree of radiographic instability and concluded that facet fluid on MRI should raise an increased suspicion of lumbar instability. 10 Lattig et al reported a correlation between the extent of facet joint effusion on MRI and the extent of spontaneous reduction of anterolisthesis measured in supine MRI compared with standing lateral X-rays, as well as a correlation between the existence of translational rotation in the anterior–posterior X-ray and the right–left side difference in facet joint effusion on MRI. 12 Most of these reports demonstrated the relationship between facet effusion and radiographic instability, meaning two-dimensional instability. However, surgeons hesitate to perform lumbar decompression surgery with facet joint effusion even though radiographic evaluation shows no instability, because facet effusion may correlate with three-dimensional instability, which cannot be detected with dynamic radiography. Intraoperative biomechanical studies reported by Hasegawa et al demonstrated an increase in the neutral zone in the segments showing facet joint effusion, which also supported the association between facet effusion and segmental instability. 18 Therefore, we undertook the present study to verify the impact of facet effusion on decompression surgical outcomes. This report is the first offering guidance to surgeons in planning the surgical treatment of patients with LSS and facet effusion.
We have shown in the current study that in patients without radiographic instability, facet joint effusion has no effect on the outcome of minimally invasive decompression surgery for LSS. Our results indicate that decompression surgery can be performed without any concern regarding facet effusion if dynamic radiographs show no segmental instability.
Facet joint effusion can be caused by multiple factors including but not limited to segmental instability. Osteoarthritis of facet joints can result in effusion. 19 Gellhorn et al suggested that facet effusion is a characteristic feature of osteoarthritis, given that the facet joints are synovial joints, similar to the knee and hip joints. 20 Furthermore, inflammation of the facet joint, resulting from conditions such as a pseudo–gout attack, 21 also shows facet effusion on MRI. Because cases of radiographic instability were excluded from our study, cases with facet effusions caused by segmental instability were also excluded. Therefore, we can conclude that the outcome of MBDU is the same independent of the presence of facet effusion.
In addition, we performed MBDU for lumbar decompression, which may partly be responsible for the same treatment outcomes observed, independent of the presence of facet effusion. In 1991, Young et al described the microsurgical fenestration technique and devised MBDU as a minimally invasive technique. 22 Thereafter, Weiner et al reported satisfactory results in follow-up periods averaging up to 2 years, 23 and Sasai et al, 14 Toyoda et al, 13 and Kato et al 24 also reported satisfactory outcomes over longer-term follow-ups of 24 to 71 months. Although our study did not include evaluation of postoperative radiographic changes, the study of MBDU by Sasai et al revealed that the postoperative progression of slip percentage is almost the same as that of the natural course reported by Matsunaga et al in an analysis of spondylolisthesis in 145 nonsurgical patients followed for at least 10 years. 25 Because minimally invasive surgeries such as MBDU can preserve posterior elements including the facet, spinous process of vertebra, and interspinous ligaments, which can contribute to spinal stability after the operation, the progression of spondylolisthesis should not be exacerbated compared with that observed in the natural course. Therefore, this advantage of MBDU may have contributed to the current result.
Some limitations to the present study should be considered. First, patients were evaluated in a retrospective fashion, which may have introduced a certain bias into the analysis. We designed this investigation to eliminate confounders as much as possible by including cases with only one lesion level, evaluating facet effusion and operation at only one level, and setting the minimum follow-up period to 2 years. However, there may be additional confounding factors that we have not yet considered or measured. Additionally, the postoperative radiographic instability was not evaluated. Second, not all minimally invasive decompression surgeries can be expected to obtain the same results. We mentioned one type of minimally invasive decompression surgery, but there are many others. Moreover, there is no clear definition of minimally invasive decompression. A third limitation is the middle-term follow-up periods. To exclude the negative impact of facet effusion on surgical outcomes completely, a longer follow-up period such as 5 or 10 years is essential. Finally, although this study is the first of the effect of facet joint effusion without radiographic instability on surgical outcome, the group sizes were rather small, and thus the present investigation can only be considered a pilot study. Further studies should attempt to replicate these findings in larger groups of patients with longer follow-up periods evaluating postoperative radiographic stability.
Conclusion
Once the absence of segmental lumbar instability is confirmed on dynamic radiographs, minimally invasive lumbar decompression can be expected to result in the same outcome, independent of the presence of facet joint effusion.
Footnotes
Disclosures
Koji Tamai: none
Minori Kato: none
Sadahiko Konishi: none
Akira Matsumura: none
Kazunori Hayashi: none
Hiroaki Nakamura: none