
Abstract
Study design
Systematic review and meta-analysis.
Objective
This systematic review and meta-analysis compared cervical laminoplasty (LP) with laminectomy and fusion (LF) for the treatment of degenerative cervical myelopathy (DCM), focusing on healthcare costs and patient-centered outcomes.
Methods
A systematic review of EMBASE and Medline (inception to September 2024) identified studies comparing LP and LF for multilevel DCM. Outcomes included return-to-work (RTW), direct treatment costs, and changes in pain and opioid use. Meta-analyses were performed using random-effects models to estimate pooled mean differences (MD) between treatment arms and mean per treatment for study outcomes. Study quality was assessed with the Newcastle-Ottawa Scale.
Results
Twelve retrospective cohort studies (7581 patients; LP: 1,848, LF: 5733) met inclusion criteria. After appraising the included studies, we determined that 25% were of high quality, 67% were of moderate quality, and 8% were of low quality. LF had higher treatment costs ($74,772.8 USD, 95% CI $29,503.72-$120,041.88) than LP ($52,109.07 USD, 95% CI $12,234.14-$91,985.43), with an MD of −$21,620.69 USD (95% CI −$35,215 to −$8025.53, I2 = 95%). LF led to greater pain reduction (MD in VAS = 1.60, 95% CI 0.36-2.84, I2 = 63%). Opioid use was inconsistently reported, preventing meta-analysis. One study found higher RTW rates at 12 months for LP (88.9%) vs LF (64.3%).
Conclusion
LF incurred greater costs but provided superior pain relief. Significant heterogeneity and limited high-quality evidence highlight the need for further research on cost-effectiveness and patient-centered outcomes.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is the most common cause of spinal cord dysfunction in adults. 1 DCM often leads to progressive neurological impairment, significantly impacting patients’ quality of life, functional capacity, and ability to engage in daily activities, including employment. 2 Surgical intervention is the primary treatment for DCM, and aims to alleviate spinal cord compression in order to halt disease progression and promote recovery.1,3 A recent randomized controlled trial (RCT) comparing ventral and dorsal approaches for management of DCM concluded similar improvement in physical functioning at 1-year follow-up. 4 Notably, the ventral group experienced a higher complication rate, highlighting the need to closely examine commonly used dorsal approaches, such as cervical laminoplasty (LP) and laminectomy and fusion (LF).5,6
Cervical laminoplasty is a motion-preserving procedure that decompresses the spinal cord by expanding the spinal canal while maintaining the native biomechanics of the cervical spine. This approach is often chosen where there is no significant cervical deformity, as it avoids the need for fusion and thus preserves cervical range of motion. However, laminoplasty is typically reserved for patients with minimal or no axial neck pain, as it does not address spondylotic neck pain and may be contraindicated in those with significant preoperative axial symptoms. 7 Postoperative axial pain is thought to result from degenerative discs and sponydylotic uncovertebral and zygapophyseal joints, which may remain symptomatic after motion-preserving procedures. 8 In contrast, laminectomy with fusion (LF) involves the removal of the lamina to achieve decompression, followed by stabilization of the affected spinal levels using instrumentation and bone grafts. LF is generally favored in cases with cervical kyphosis, instability, or multilevel involvement where treatment can induce iatrogenic instability. However, the risk of adjacent segment disease following fusion remains an important consideration.3,5,6
While both LP and LF are widely used, there is a lack of consensus with regards to which procedure offers superior outcomes across various clinical parameters. Numerous studies have examined the effects of these techniques on a range of outcomes, including the modified Japanese Orthopedic Association (mJOA) score, Neck Disability Index (NDI), SF-36, as well as complications, and radiographic parameters such as cervical alignment.5,6,9-12 Despite the wealth of literature on LP vs LF, there is a need for a comprehensive synthesis of evidence to guide clinical decision-making, particularly in evaluating the patient-centered outcomes of return-to-work (RTW), postoperative opioid use, and treatment costs.
This systematic review and meta-analysis will aim to synthesize the existing evidence on the primary outcomes of RTW, postoperative opioid use, and treatment costs in patients undergoing LP vs LF for DCM. In addition, we will compare each approach with respect to postoperative pain as measured by the Visual Analog Scale (VAS), given its relationship to analgesic requirements, to provide a comprehensive comparison of these 2 surgical techniques. By conducting this review, we hope to generate evidence that informs surgical decision-making, optimizes patient-centered care, and supports cost-effective treatment strategies in managing degenerative cervical myelopathy.
Methods
Study Design
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 13 The study protocol was pre-registered in a systematic review database (PROSPERO ID CRD42024605897).
Search Strategy and Study Eligibility
Original studies were retrieved from EMBASE and Medline from the earliest available date to September 2024 using the search strategy outlined in supplemental Table 1. Reference lists of retrieved studies were screened to identify additional articles meeting inclusion criteria that were not captured in primary database search. We included all English language studies involving adult human subjects (age ≥18 years) comparing LP and LF for multilevel degenerative cervical myelopathy reporting on at least one of the following outcomes: return-to-work, pain, opioid use, and treatment cost. Studies containing anterior surgery cohorts were included if the LP and LF cohort analyses were reported independently. Studies involving laminectomy alone, laminoplasty with selective instrumented fusion, or combined anterior-posterior surgical approaches were excluded. Studies involving patients with oncologic, traumatic, or infectious pathologies were excluded. Case series with less than 5 patients, cadaver studies, or studies involving non-human subjects were excluded. In addition, reviews, commentaries, editorials and conference proceedings were excluded. Abstracts were reviewed based on study criteria, with data subsequently summarized from relevant full text using Microsoft Excel version 16. Studies for which only the abstract was available were excluded. For meta-analyses, studies were excluded if they did not report return-to-work in the proportion of patients, total index hospital cost in dollar value, baseline and postoperative pain scores as measured by the Visual Analog Scale (VAS), and total postoperative opioid use in morphine milligram equivalents (MME).
Data Collection
Initial title and abstract screening were performed by a single reviewer (VK). Full-text reviews were conducted independently by 2 reviewers (VK and HS), with discrepancies resolved through consensus. Publication variables collected included first author, year of publication, study design, and location. Baseline characteristics collected included sample size, age, sex, and preoperative pain scores. Postoperative variables collected included treatment cost, proportion of patients returning to work, postoperative opioid use, postoperative pain scores as measured by VAS, and follow-up period.
Bias and Certainty of Evidence Assessment
The methodological quality of the included studies was assessed using the Newcastle-Ottawa scale (NOS) for observational studies. 14
Study Outcomes
Study outcomes assessed included postoperative opioid use (morphine milligram equivalents and proportion in %), return-to-work (proportion in %), treatment costs in US dollars (USD), and pain scores (VAS). Cost data was adjusted to January 2024 USD using the medical component of the consumer price index. 15 Studies reporting total direct costs associated with an index hospital stay for LP and LF were pooled for analysis to calculate the average cost for each surgical treatment and the mean difference (LP vs LF). For studies reporting pain outcomes, baseline VAS and postoperative VAS scores at last follow-up were extracted. We then calculated change in VAS scores within each treatment arm across the included studies. This was then used within the pooled analysis to calculate the average change in VAS for each surgical treatment and the mean difference in change in VAS (LP vs LF).
Data Synthesis and Statistical Analyses
All statistical and meta-analyses were performed using R version 4.4.1 with the meta library package. An a priori significance level of P = .05 was used for two-tailed tests. Descriptive statistics were reported as mean and standard deviation for continuous variables and count with proportions for categorical variables. Pooled estimates for patient-level characteristic (age and sex) were calculated by treatment group (Table 2).
Studies included in meta-analyses were those that reported treatment cost (total index hospital in USD) and pain (VAS). Return-to-work and opioid use were not considered for meta-analyses due to an insufficient number of studies and inconsistent reporting across studies, respectively. For studies that did not report standard deviations directly, we estimated standard deviation using reported 95% confidence intervals, quartiles, or ranges where available, as described in the Cochrane Handbook.16,17
Random-effects meta-analysis was performed to account for heterogeneity across studies. To compare treatment groups, pooled mean differences with 95% CIs between LP and LF for continuous outcomes were calculated and visualized on forest plots. The pooled estimates of the mean for outcomes was calculated with 95% CIs. Heterogeneity across studies was evaluated with Cochran’s Q and I2 statistics, with P ≤ .10 or I2 > 50% considered significant heterogeneity. 18
Results
Overview of Studies and Patients
Summary of Findings From Systematic Review for Outcomes After LP and LF
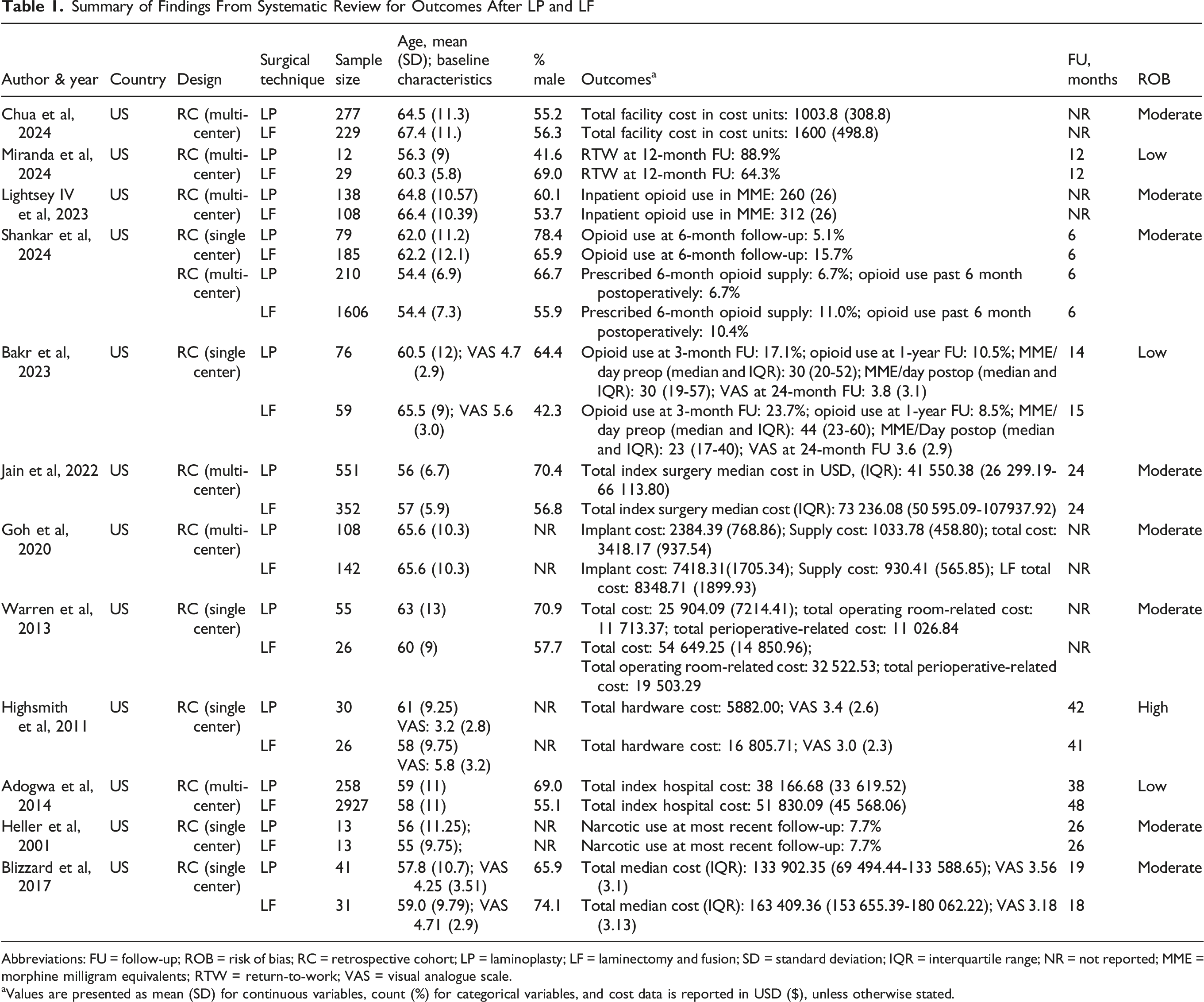
Abbreviations: FU = follow-up; ROB = risk of bias; RC = retrospective cohort; LP = laminoplasty; LF = laminectomy and fusion; SD = standard deviation; IQR = interquartile range; NR = not reported; MME = morphine milligram equivalents; RTW = return-to-work; VAS = visual analogue scale.
aValues are presented as mean (SD) for continuous variables, count (%) for categorical variables, and cost data is reported in USD ($), unless otherwise stated.
Pooled Baseline Summary Statistics for Patients Treated With LP and LF From a Meta-Analysis of Baseline Characteristics From Individual Studies
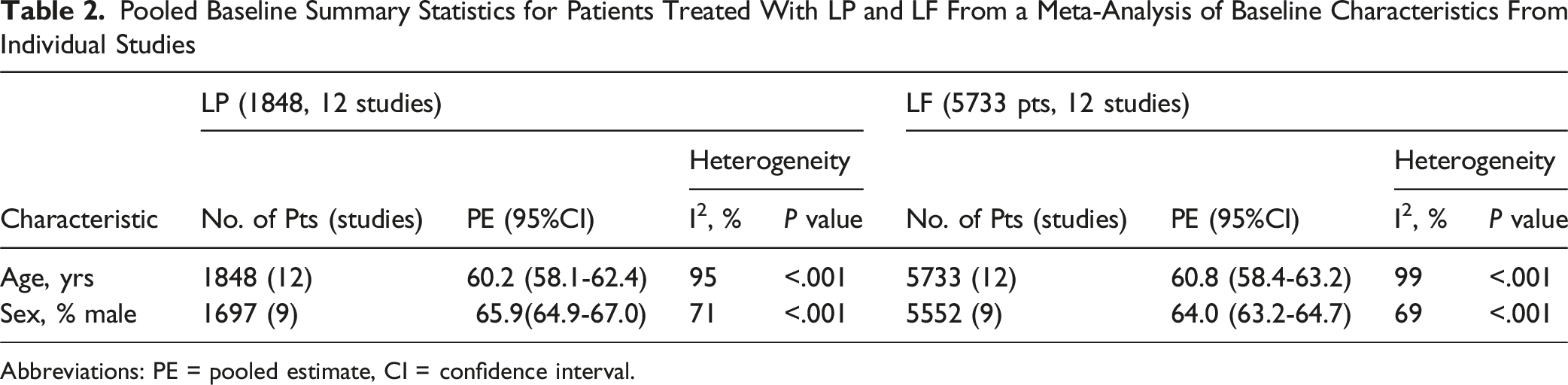
Abbreviations: PE = pooled estimate, CI = confidence interval.
Pooled Estimate for Cost in LP and LF
Pooled Estimates of Cost and VAS From the Meta-Analyses of Outcomes From Individual Studies
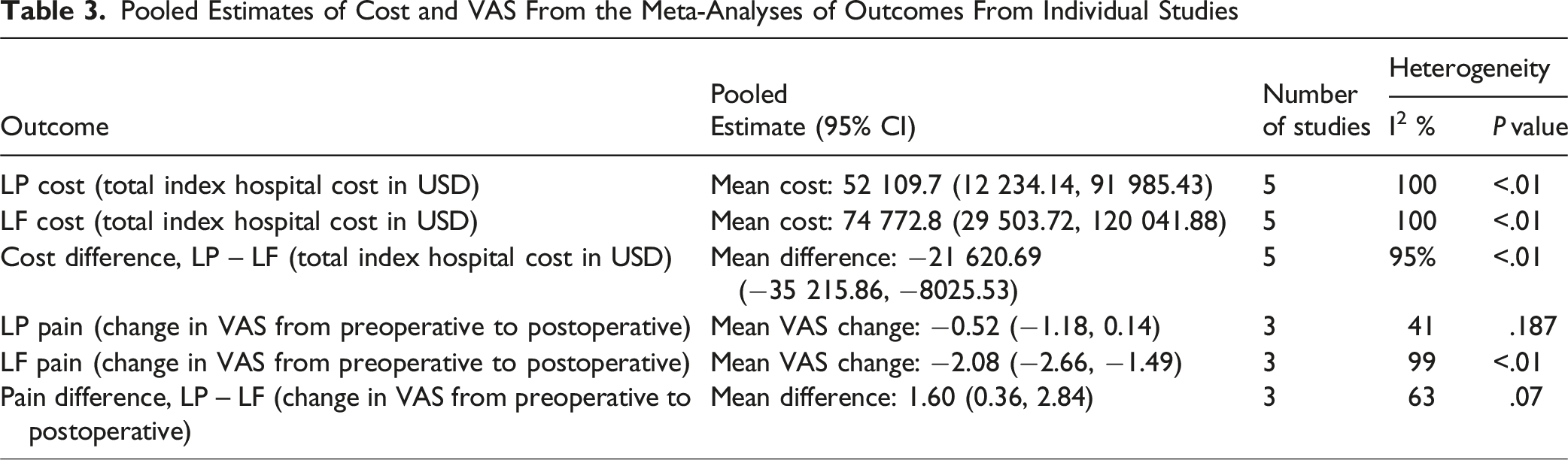
The random-effects model demonstrated a significant difference in treatment cost between LP and LF (mean difference = −$21,620.69 USD; 95% CI −$35,215.86 to −$8025.53 USD) (Figure 1). We found significant heterogeneity in cost reporting across studies (I2 = 95%, P < .01). Forest Plot of Studies Showing Mean Difference in Total Index Hospital Cost after LP vs LF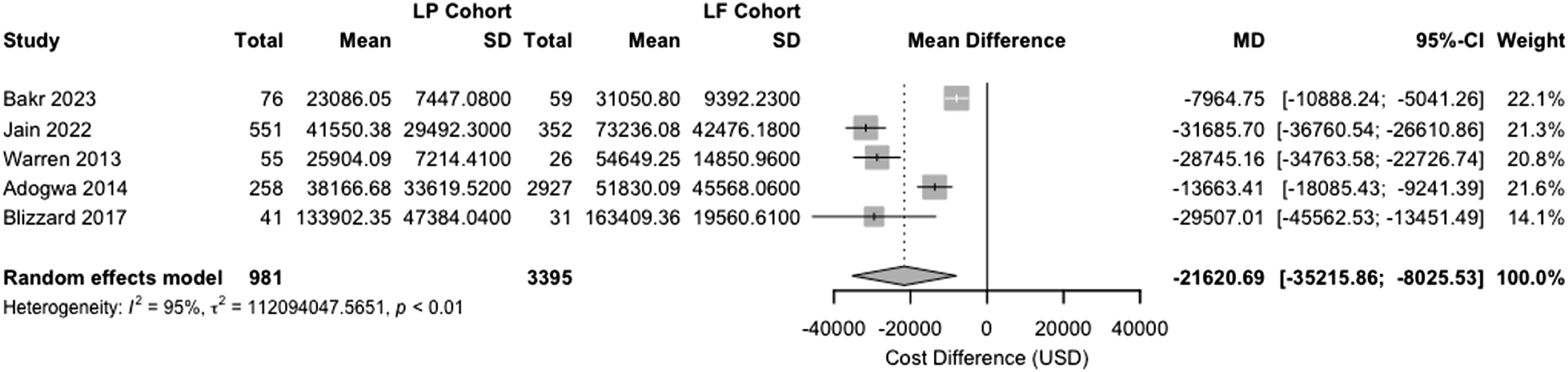
Pooled Estimate for Pain in LP and LF
Three studies were included in the meta-analysis comparing changes in VAS between patients undergoing LP and LF.23,27,30 When examining the mean change in VAS after surgery across studies, the LP group showed a smaller reduction in pain from baseline to postoperative assessment, with a mean change in VAS of −0.52 (95% CI −1.18 to 0.14), indicating no significant change postoperatively relative to baseline. In contrast, the LF demonstrated a larger reduction in pain, with a mean change of −2.08 (95% CI −2.66 to −1.49) postoperatively. The heterogeneity assessment for mean VAS change was low for the LP group (I2 = 41%, P = .187) but high for the LF group (I2 = 99%, P < .01), suggesting greater variability in LF pain outcomes across included studies (Table 3).
The meta-analyses of LP vs LF, with respect to magnitude of change in VAS from baseline to postoperative assessment, revealed a significant mean difference in VAS score between the 2 surgical approaches. The pooled mean difference was 1.60 (95% CI 0.36 to 2.84), suggesting that the LF group experienced a larger reduction in VAS scores compared to the LP group (Figure 2). There was significant heterogeneity among the included studies (I2 = 63%, P = .07). Forest Plot of Studies Showing Mean Difference in Change in VAS after LP vs LF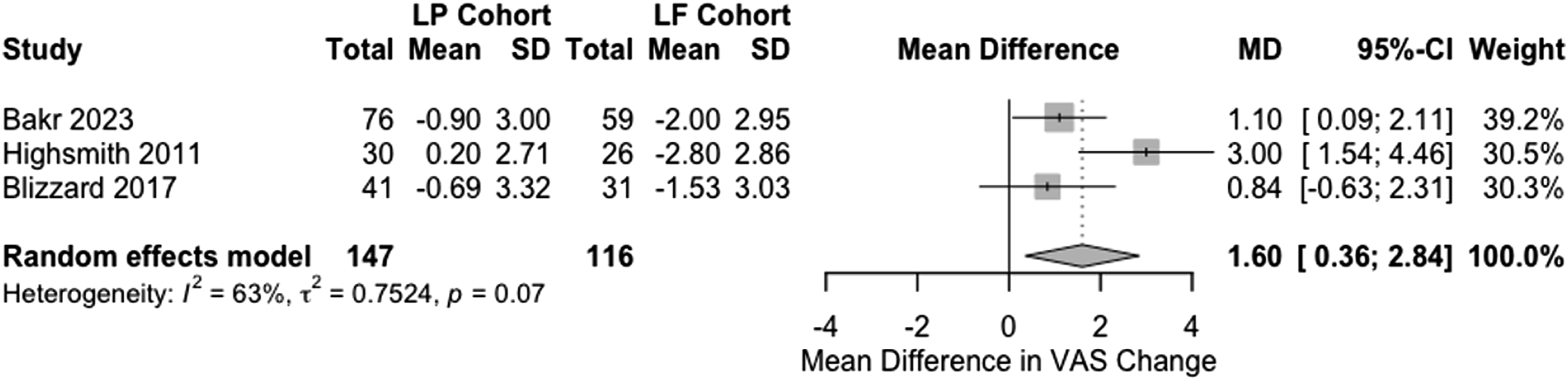
Postoperative Opioid Use
Four studies reported outcomes for patient opioid use following LP and LF.21-23,29 Due to variability in the reporting of opioid use outcomes across the studies, with 1 study reporting total inpatient opioid use in MME and 3 reporting the proportion of patients using opioids at varying follow-up intervals, a meta-analysis was not feasible. However, the extracted data provide relevant insights into opioid utilization patterns following LP and LF. Lightsey IV et al reported total inpatient opioid use, with the LF group requiring a higher opioid dose of 312 MME compared to 260 MME in the LP group (P = .03). Shankar et al examined opioid use at different time points within a single-surgeon cohort, demonstrating that the LF group had higher 6-month opioid use of 15.7% compared to 5.1% in the LP group (P = .02). This study also examined national cohort data, reporting 6-month opioid use of 10.4% in the LF group compared to 6.7% in the LP group (P = .09).
Bakr et al reported opioid use rates of 23.7% at 3 months and 8.5% at 1 year in the LF group, compared to 17.1% at 3 months and 10.5% at 1 year in the LP group (3-month P = .340, 1-year P = .689). This group also reported lower inpatient postoperative opioid consumption for the LF group (23 MME/day) compared to the LP group (30 MME/day), though this difference was not statistically significant (P = 1.00). Heller et al reported equal rates of narcotic use (7.7%) at the latest follow-up in both groups. Overall, there was considerable heterogeneity in reported opioid use postoperatively due to small sample sizes, variability in reporting methods, and differences in follow-up periods.
Return-to-Work
Only 1 study comparing LP and LF reported on return-to-work (RTW) rates at various time points, including 1, 3, 6, and 12 months postoperatively. At the 12-month follow-up, 88.9% of the LP cohort had returned to work compared to 64.3% of those who underwent LF. 20
Quality Assessment of Studies Comparing LP and LF
All twelve included observational studies were evaluated using the Newcastle-Ottawa Scale (NOS), with only 3, 25%, categorized as high-quality studies. The remaining studies were rated as moderate (N = 8, 67 %) and low quality (N = 1, 8%) due to several factors, including inadequate follow-up and lack of cohort comparability (Supplemental Table 2).
Discussion
This systematic review and meta-analysis provides important insights into the comparative effectiveness of LP vs LF for the treatment of DCM. Through the analysis of 12 retrospective studies encompassing 7581 patients, we found significant differences in treatment costs and postoperative pain outcomes between the 2 procedures while identifying important knowledge gaps in return-to-work outcomes and postoperative opioid use patterns.
We found a substantial difference in treatment costs between the 2 procedures, with LF associated with a higher average total hospital index cost $74,772.8 USD (95% CI $29,503.72 to $120,041.88 USD, I2 = 100%) compared to $52,109.07 USD (95% CI $12,234.14 to $91,985.43 USD, I2 = 100%) for LP. The pooled mean difference between LP and LF (MD = −$21,620.69 USD; 95% CI −$35,215 to −$8025.53 USD, I2 = 95%) reinforces the significant cost difference associated with these 2 treatments. This cost differential likely reflects several factors, including the additional instrumentation required for fusion, longer operative times, and potentially extended hospital stays associated with LF. These differences in treatment costs have important implications in the context of value-based care. Prior studies have demonstrated that the lower cost associated with LP does not compromise safety or effectiveness. In fact, patients undergoing LP have been shown to experience shorter hospital length of stays, fewer complications, and reduced rates of unplanned reoperations, highlighting the potential of LP to serve as a cost-effective strategy in appropriately selected patients.23,31 Conversely, in those with more significant cervical deformity, instability, or significant preoperative axial neck pain, LF may offer improved postoperative pain symptoms and structural correction. 32 From a health system perspective, these comparative cost insights can support more nuanced surgical decision-making, guide institutional resource allocation, and inform the development of reimbursement policies that align with patient complexity and expected value of care. Overall, these estimates provide valuable reference points for healthcare systems and payers, though the high heterogeneity observed suggests that costs vary considerably across different healthcare settings and geographic regions.
Our analysis of pain outcomes revealed that LF was associated with a greater reduction in pain, from baseline to postoperative assessment, compared to LP (MD of change in VAS = 1.60, LP vs LF; 95% CI 0.36 to 2.84, I2 = 63%). One possible explanation is that patients undergoing LF may have higher baseline axial neck pain, reflected in greater preoperative VAS scores, thereby allowing for greater absolute improvement post-operatively. While this differs from previous meta-analyses that reported no significant differences between the 2 treatments,5,6,9,11,12,33 our finding should be interpreted with caution given our smaller sample of included studies (n = 3). The limited number of studies in our analysis increases the risk of sampling error and reduces the precision of our effect estimate.
The examination of postoperative opioid use patterns, while limited by heterogeneous reporting methods, suggests a complex relationship between surgical approach and analgesic requirements. Some studies indicated higher early and late postoperative opioid requirements with LF,21,22 while others showed comparable or lower usage patterns.23,29 This variability underscores the need for standardized reporting of opioid outcomes in future prospective studies, particularly given the current emphasis on opioid stewardship in surgical practice.
The paucity of data on return-to-work outcomes represents a significant gap in the current literature. The single study reporting these outcomes suggested superior return-to-work rates with LP at 12 months (88.9% vs 64.3% for LF). 20 While this finding is intriguing and potentially related to the motion-preserving nature of LP, the limited data prevents firm conclusions about the relative impact of these procedures on occupational outcomes.
Limitations
This meta-analysis had several important limitations. Notably, since only studies that reported costs in USD were included in the pooled analysis, the generalizability of our findings is limited beyond the United States. Overall, there was a general lack of high-quality studies reporting on outcomes of interest, particularly on return-to-work and opioid use. All included studies were retrospective in design, with no prospective cohort or RCTs comparing LP and LF. There was significant heterogeneity amongst included studies, particularly in follow-up periods across studies, contributing to inconsistent outcomes. For example, all 3 studies reporting on postoperative VAS scores had different time points for assessment, corresponding to different follow-up intervals. A few studies had relatively small sample sizes (n < 15) within treatment arms, which can further affect the precision of effect estimates. Lastly, there was significant variability in outcome reporting across studies. For example, some studies examining cost reported total costs associated with the index surgery, while others reported on specific cost components such as implants. Similarly, studies examining postoperative opioid use varied, with some reporting inpatient opioid needs in MME and others focusing on the proportion of patients using opioids at different follow-up intervals.
Conclusion
In this systematic review and meta-analysis, we found some evidence demonstrating that in patients with multilevel DCM, there is a higher treatment cost but greater improvement in postoperative pain associated with LF compared to LP. However, due to significant heterogeneity of the included studies, these findings should be cautiously interpreted and warrant future prospective RCTs comparing these 2 treatments using standardized outcome measures.
Supplemental Material
Supplemental Material - Laminoplasty Versus Laminectomy and Fusion in the Treatment of Degenerative Cervical Myelopathy: A Systematic Review and Meta-Analysis of Cost and Patient-Centered Outcomes in the United States
Supplemental Material for Laminoplasty Versus Laminectomy and Fusion in the Treatment of Degenerative Cervical Myelopathy: A Systematic Review and Meta-Analysis of Cost and Patient-Centered Outcomes in the United States by Vishwathsen Karthikeyan, Husain Shakil, Christopher S. Lozano, Armaan K. Malhotra, Uzondu F. Agochukwu, Ankit I. Mehta, C. Rory Goodwin, Nathan Evaniew, Paul A. Koljonen, Allan R. Martin, James D. Guest, Kurpad SN, Jefferson R. Wilson, and Aditya Vedantam in Global Spine Journal
Footnotes
ORCID iDs
Author Contributions
VK, HS, JRW, AV contributed to the conception and design of the study. Data collection and analysis were performed by VK and HS. VK drafted the manuscript. All authors provided critical revisions. Study supervision was provided by AV.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international spine experts, and AO Spine North America. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization based in Davos, Switzerland
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.