
Abstract
Study Design
Review.
Objective
Unilateral Biportal Endoscopy (UBE) is a minimally invasive surgery that is gaining recognition and being employed in clinical practice. Nevertheless, the precise method for determining UBE portals’ location varies depending on the originator’s preferences or the anatomical structure’s proximity to the portal positions. Consequently, the relationship among UBE portals' locations is messy. This study aims to elaborate on the specific portal localization and explore the positional association and commonality among different UBE approaches’ portals.
Methods
The following keywords are used to search in the PubMed, Ovid, Web of Science, ScienceDirect, SpringerLink, Scopus, CNKI, and Wanfang database: “Biportal endoscopic spinal surgery”, “Two portal endoscopic spinal surgery”, “Percutaneous biportal endoscopic decompression”, “Unilateral biportal endoscopy”, “Irrigation endoscopic discectomy”, “UBE” and “BESS”.
Results
After screening, 29 pieces of literature are included. The study summarizes different UBE approach portal localizations, categorized by fusion or non-fusion surgery and pathological classification. The study presents an inaugural method for categorizing the lumber into four surgical intervals based on bone landmarks and assigns different UBE approaches to the appropriate intervals based on their characteristics, making the selection of UBE surgical approaches’ portal locations more flexible. Additionally, the study provides an overview of the indications, complications, and distinct benefits associated with each interval, further refining the novel UBE portal interval localization method.
Conclusion
The study clarifies the interrelationship and commonality between the portals of different UBE approaches and proposes a new UBE portal interval localization method to enhance surgeons’ understanding and proficiency in UBE procedures.
Introduction
With the ongoing advancement and refinement of the concept and practice of minimally invasive surgery, its utilization has become more widespread across various medical specialties. In recent years, spinal surgery has emphasized minimizing trauma, muscle and soft tissue injuries, postoperative pain, and functional impairment in patients. 1 Over the years, there have been significant advancements in spine minimal surgery techniques, which have advanced from traditional open surgery to percutaneous endoscopic techniques, and then to unilateral biportal endoscopic technique (UBE). 2
UBE technology has progressively expanded indications from basic intervertebral disc herniation to vertebral canal stenosis, lumbar spondylolisthesis, and renovation surgery as a prominent research direction in the spinal field in recent years. 3 To accommodate a variety of indications, researchers have proposed various surgical approaches for optimal treatment effects. However, the positioning of different UBE approaches’ portals is complex and chaotic due to the distinct reference indicators of their portal position. The study aims to elaborate on the specific methods of portal localization and clarify the interrelationship and commonality between the portals of different UBE approaches to enhance surgeons’ understanding and proficiency in UBE procedures.
Methods
Literature Search
Searches are performed in PubMed, Ovid, Web of Science (including Medline), Science Direct, Springer Link, Scopus, CNKI, and Wanfang database using the following keywords: “Biportal endoscopic spinal surgery”, “Two portal endoscopic spinal surgery”, “Percutaneous biportal endoscopic decompression”, “Unilateral biportal endoscopy”, “Irrigation endoscopic discectomy” “UBE” and “BESS”. Papers published in the public domain up to October 1st, 2023, were searched, and references to all retrieved articles were searched manually, one by one, to improve the completeness of the literature. The language was restricted to English and Chinese. Mendeley (Elsevier, Amsterdam, Netherlands) is used to de-duplicate English articles, while Chinese article de-duplication is facilitated by Notepress (Aegean Software Corp., Beijing, China). After de-duplication, Rayyan is employed for the management of blinded title and abstract screening, 4 and articles that do not fit the purpose of this paper will be excluded. After the initial screening, 3 reviewers, Yixi Wang, Abulikemu Maimaiti, and Abudusalamu Tuoheti, inspect the papers’ titles, abstracts, and full texts. Discrepancies among reviewers pertaining to title and abstract screening, full-text review, and grounds for exclusion are resolved via the involvement of a fourth reviewer (Paerhati Rexiti).
Inclusion and Exclusion Criteria
Inclusion criteria: (1) patients who underwent lumbar surgery with UBE technology; (2) detailed portal positioning methods documented in the literature; (3) surgical segments in the lumbar spine.
Exclusion criteria: (1) literature in which an animal or corpse is the subject of the research; (2) literature without mentioning the portal positioning method; (3) literature that directly references the portal positioning method of another author without making any improvements; (4) surgical segment not in the lumbar spine; (5) letter to the editor, correspondence, review, communication, and conference paper.
Ethical Approval
The study design was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University before data collection and analysis (Approval No. 20210401-01). Because of the narrative review and observational nature of the study, the Ethics Committee waived informed consent.
Results
Literature Characteristic
In a total of eight databases, 2004 studies were identified. Software-based elimination of duplicate studies left 1128 studies. A total of 568 studies were omitted from the remaining 1128 due to their non-compliance with the study’s objectives, such as their classification as non-original research articles, and so on. The remaining 560 studies underwent a comprehensive text evaluation, which led to the exclusion of 479 studies, and 25 studies that satisfied the inclusion criteria 5-29 were included. To ensure the integrity of the data, a screening of included studies in recent UBE reviews 30-33 and identified 4 additional studies that were subsequently incorporated into this research.34-37 The specific search process is shown in Figure 1. Flow diagram of study selection.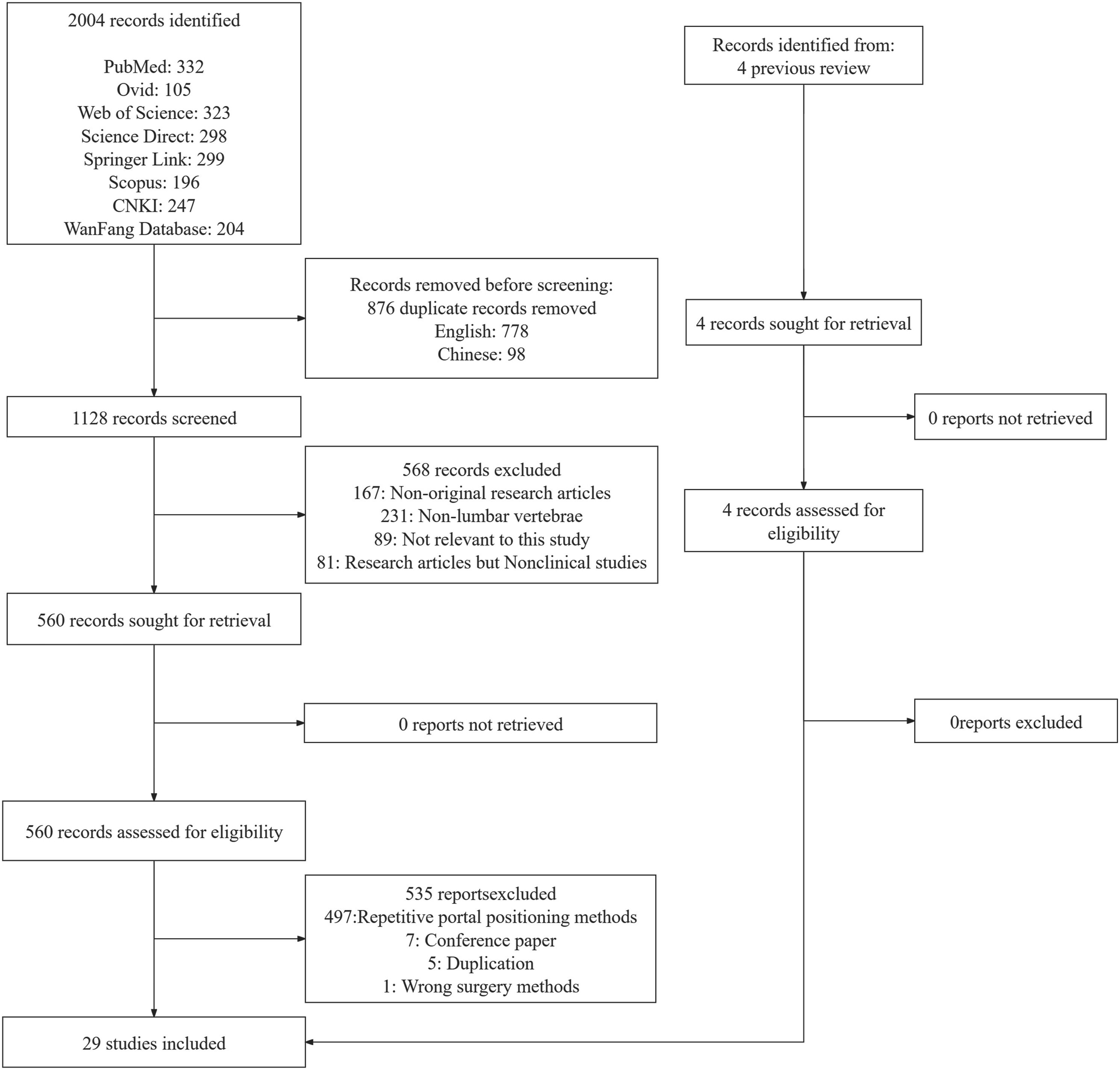
Lumbar Non-Fusion Unilateral Biportal Endoscopic Surgery
This chapter and the subsequent chapter on fusion surgery are described from the vantage point of a right-handed surgeon positioned on the left side of the patient during the surgical procedure.
Operation of Lumbar Disc Herniation
The Portal Position of the Interlaminar Approach
The UBE-Interlaminar approach mainly focuses on disc herniation at the subarticular zone (lateral recess), and there are 2 predominant techniques for portal localization in the interlaminar approach. One method for identifying portals is as follows: A plumb line is positioned 1 cm parallel to the posterior midline. The cephalic portal is situated at the intersection of the plumb line and the intervertebral disk, serving as the gateway for the endoscopy. While the caudal portal is located 3-4 cm below the cephalic portal and is used for surgical instruments. The surgeon has the option to modify the portals utilized throughout the surgical procedure according to their personal taste (Figure 2A, Green Dots).
5
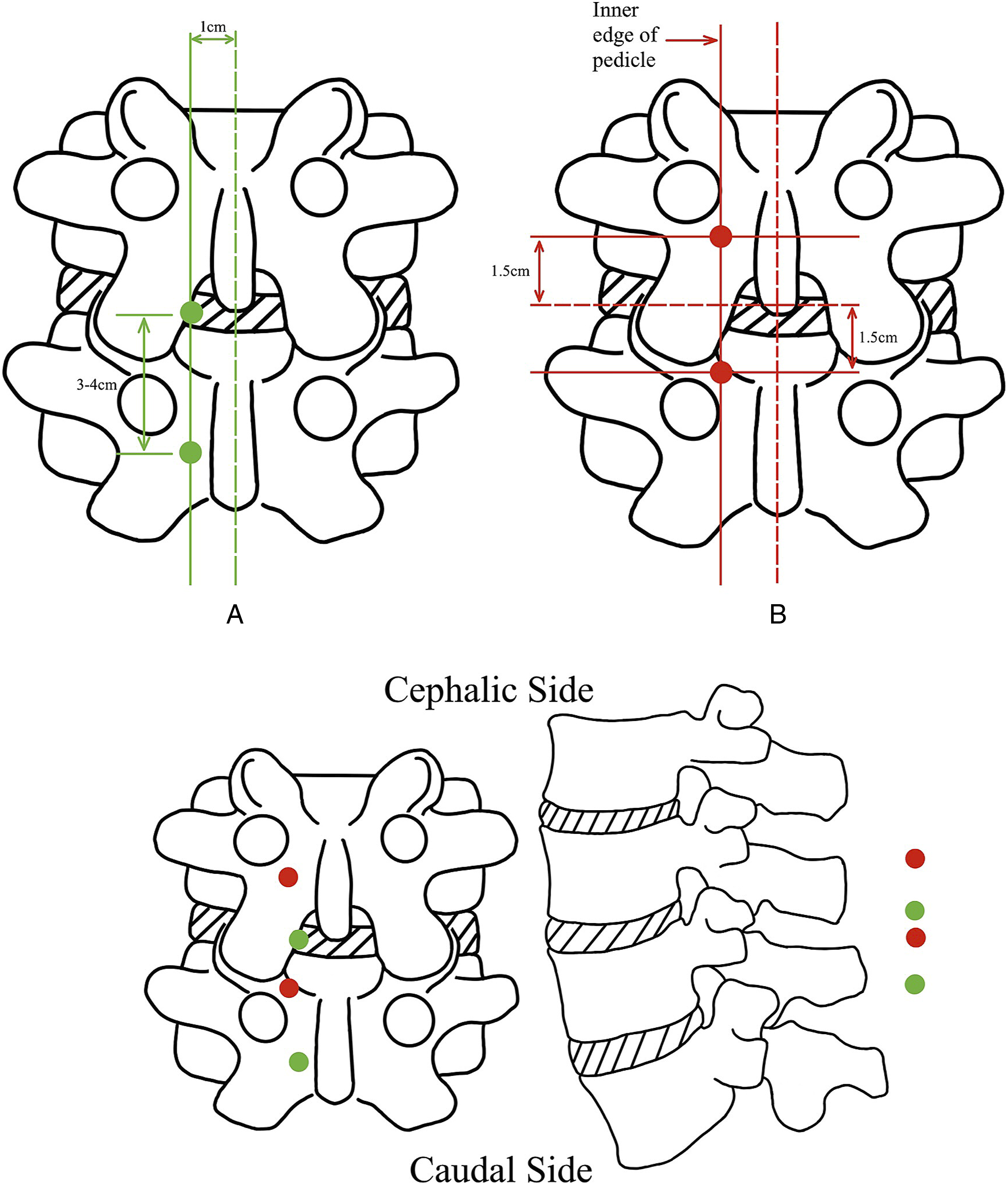
Another method for identifying portals is as follows: Make a horizontal line at the level of the responsible intervertebral space and find the intersection point between the tangent line of the inner edge of the pedicle and the above horizontal line. A 15 mm distance from the intersection point towards the cephalic sides along with the tangent line is the endoscopic portal position, and a 15 mm distance towards the caudal side is the working portal position. During the procedure, the surgeon can assess the distance between the spinous process and the inner edge of the vertebral pedicle to determine whether the 3 cm channel spacing is appropriate and adjust if necessary 6 (Figure 2B, Red Dots).
The Portal Position of the Transforaminal Approach
In contrast to the UBE-Interlaminar approach, the UBE-transforaminal approach is applicable for basically all types of disc herniation, even extreme lateral herniations. The prevailing technique for identifying the portal through the transforaminal approach is as follows: Portals are created at a distance of 2-3 cm from the outer edge of each pedicle. The positioning of the portal is modified at the L5-S1 level due to the presence of the iliac crest. The left portal adheres to the positioning strategy previously discussed. The portal on the right side has been relocated to a position 1 cm closer to the midline than its customary placement.
7
See Figure 3A for a detailed schematic (Red Dots).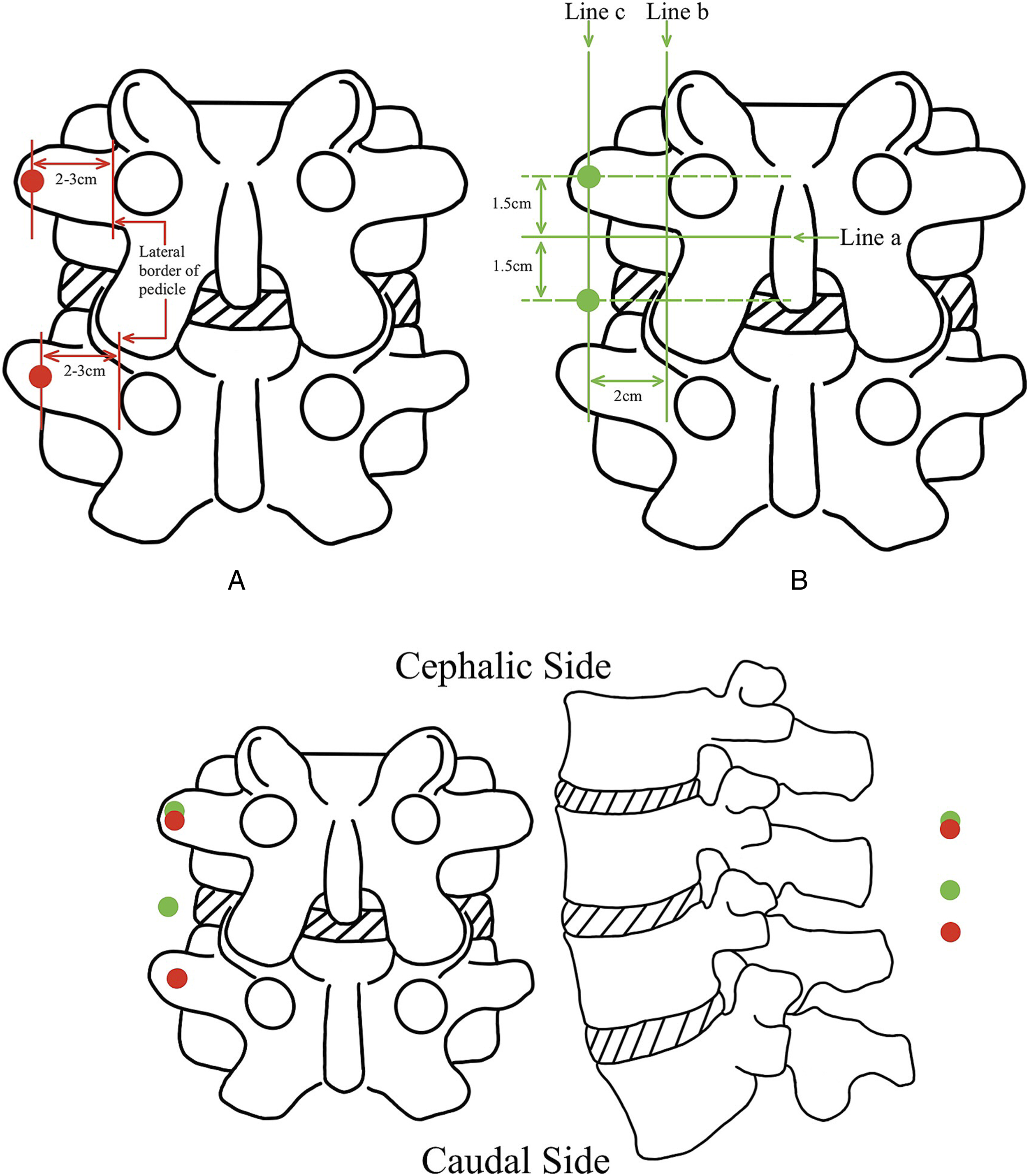
In treating far lateral lumbar disc herniation (LDH), it is necessary to modify the portal position by the location of the lesion. The repositioning portal procedure is as follows: Draw a horizontal line “a” across the center of the left-sided isthmus and a vertical line “b” along the outer edge of the left-sided pedicle. Both lines are drawn with the anatomical landmarks of the superior vertebrae in the surgical segment. A parallel line “c” is drawn 2 cm outside line “b”. The endoscopic and working portal positions are 1.5 cm each away from the cephalad and caudal to the intersection point of lines “a” and “c”. 8 See Figure 3B for a detailed schematic (Green Dots).
Operation of Lumbar Posterior Apophyseal Ring Separation
Lumbar posterior apophyseal ring separation (PARS) is secondary to lumbar disc herniation in children and adolescents, distinguished by the free bone pieces. 38 PARS can be categorized into 4 distinct categories based on fracture locations. 39 Typically, type I (avulsions of the posterior cortical vertebral rim) and type III (lateralized chip fractures), involving smaller bone fragments that align with the mobility classification’s mobile type, are the primary indications for undergoing UBE surgery. 39 Type II and type IV, which involve larger bone fragments or have more extensive damage, can be considered relative contraindications to UBE surgery.
The UBE approach for treating PARS type I resembles the UBE-interlaminar approach employed for disc herniation since it has a similar lesion position. Precisely, however, typically, its endoscopic and working portals are positioned more downward overall compared to the UBE-interlaminar approach for the treatment of LDH because the lesion of the PARS type 1 generally is located at the same level as the upper endplate of the vertebrae below the affected segment. The exact location of the endoscopic and working portals can be seen in Figure 4.9,10 In theory, PARS type III can be treated using the UBE-transforaminal approach, but no similar study has been published so far.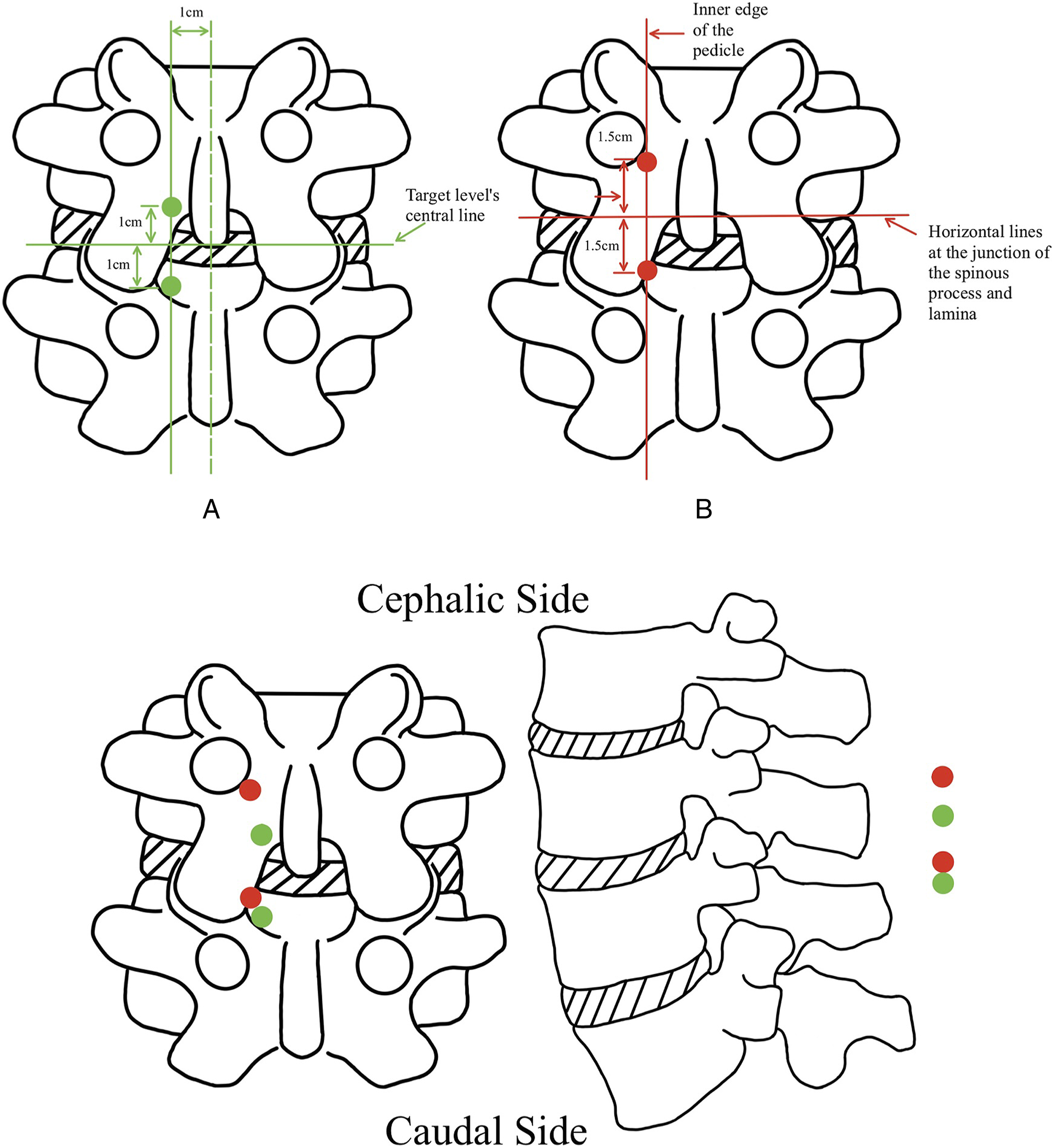
Operation of Spinal Epidural Abscess
According to the classification based on the original anatomical site, lumbar spine infection can be divided into spondylitis, discitis, and epidural abscess. 40 In the case of epidural abscess, the main surgical procedure is non-fusion drainage, while some types of spondylitis and discitis often require the placement of a cage with antibiotics to alleviate the condition. This section will focus on the UBE surgical portal localization method for epidural abscesses. The subsequent fusion section will address the UBE method for spondylitis and discitis.
The UBE portal position for a localized epidural abscess is similar to the 2 primary approaches of the UBE-interlaminar approach for LDH To obtain additional information, refer to Figure 5 which illustrates the primary position of endoscopic and working portals in relation to the UBE-interlaminar approach for spinal epidural abscess.17,18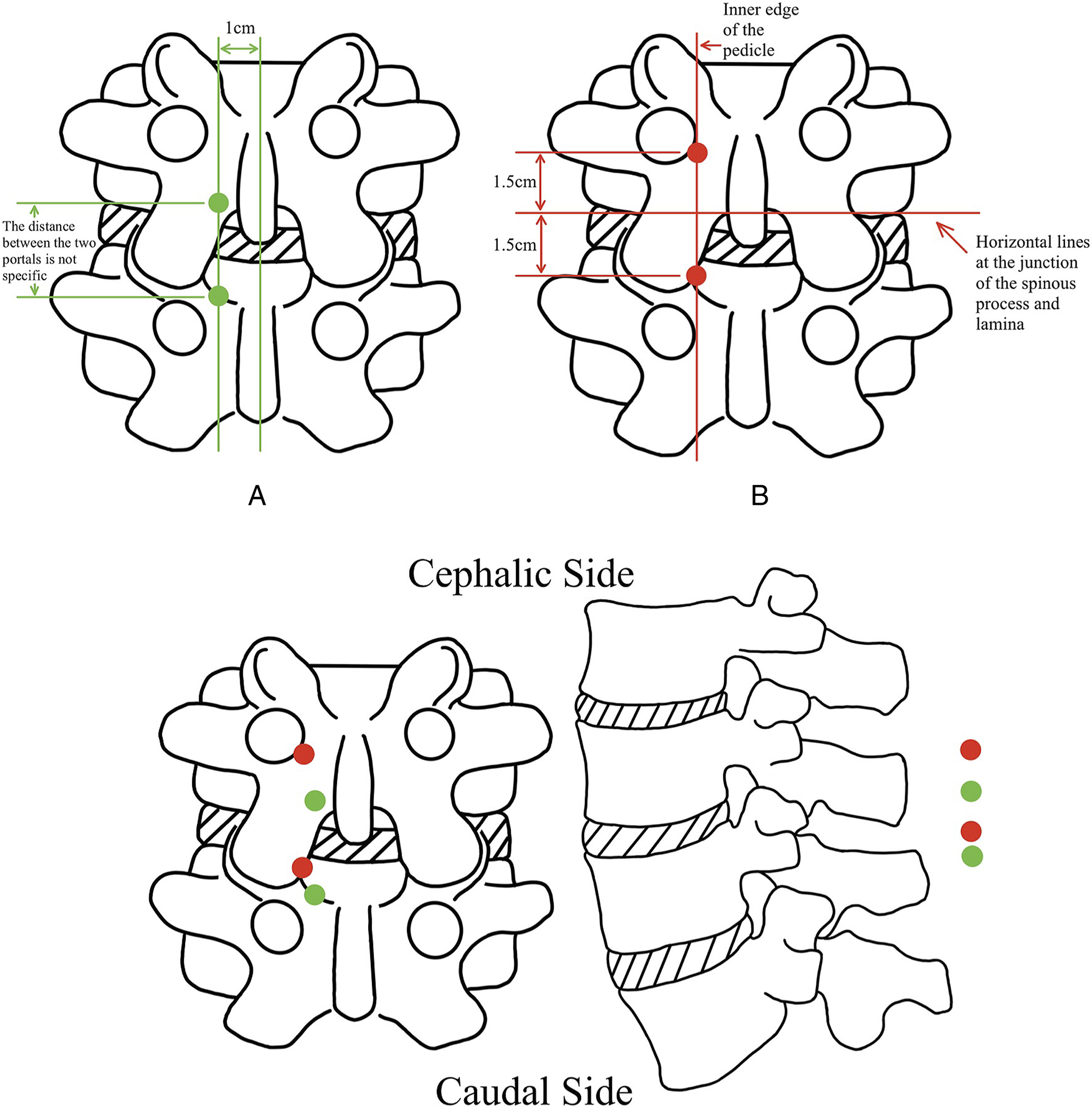
In contrast to localized therapy, managing extensive epidural abscesses usually necessitates endoscopic surgical interventions over numerous segments. Managing extensive epidural abscesses from the L1 to L5 vertebrae involves initially using the UBE interlaminar technique at the L1-L2 level, with the main aim of evacuating the epidural abscess. A further UBE interlaminar approach is performed at the L4-L5 level to carry out discectomy, debridement, and extract pathogenic bacteria. 28
Operation of Lumbar Spinal Stenosis
Due to the submerged field of view, the UBE-Unilateral Laminotomy with Bilateral Decompression (ULBD) is particularly beneficial for bilateral lateral recess decompression in Lumbar Spinal Stenosis (LSS). The initial UBE-ULBD portal positions,
11
depicted in Figure 6A as green dots, have been mostly substituted by the method shown in Figure 6B and 6C. The positions of the endoscopic and working portals for 2 regularly utilized UBE-ULBD approaches 12,34 can be likened to the 2 types of UBE-interlaminar approaches employed for treating LDH, as illustrated in Figure 6B (Red dots)
34
and Figure 6C (Orange dots).
12
The primary distinction between the 2 approaches is that the orange dots method involves the simultaneous downward and outward movement of both the endoscopic and working portals as a single unit based on the red dots methods, which is particularly suitable for patients with large vertebrae due to portals far from the spinous process. Moreover, it employs the patient’s inherent anatomical landmark (the tangent line of the inner edge of the pedicle) as a reference, which allows for greater flexibility in making personalized adjustments and exhibits a higher level of applicability.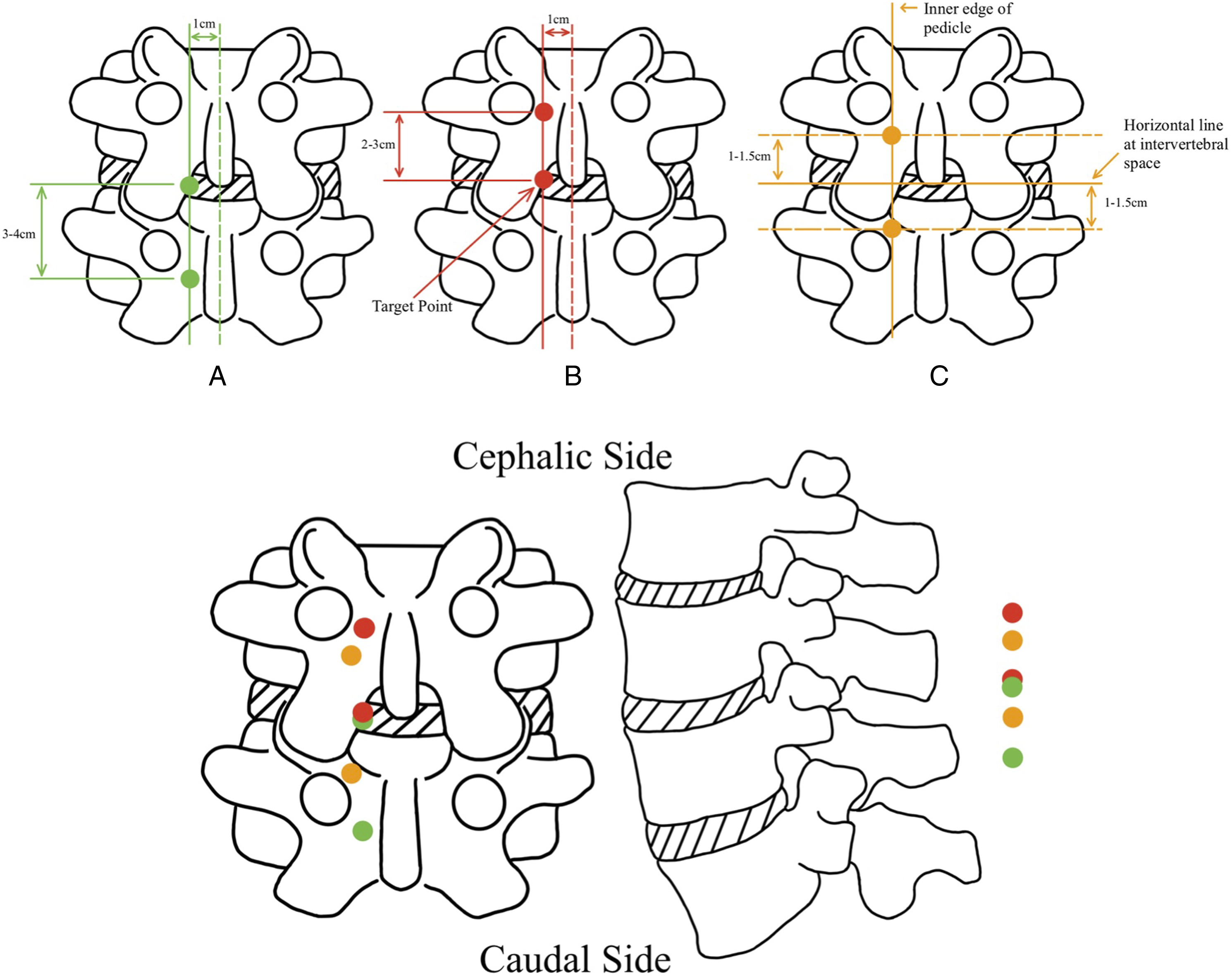
The UBE-ULBD for LSS was previously employed to treat patients with severe lumbar spinal stenosis (SLSS), as depicted in Figure 7A (Green Dots).
13
Nevertheless, the above approaches may cause significant damage to the facet joints in SLSS patients, due to the pronounced structural abnormalities and constricted anatomical spaces. To resolve this problem, the portals undergo internal repositioning (moving inward) and give priority to decompression on the opposite side or remove additional bone at the base of the spinous process to achieve thorough decompression. The new SLSS UBE approach portal position method is shown below: The working portal, measuring 8-10 mm, is around 5 mm lateral to the posterior midline, specifically at the upper boundary of the lower lamina. The endoscopic portal, measuring 4-6 mm, is approximately 25-30 mm superior to the working portal,
14
as seen in Figure (Red Dots) (Figure 7).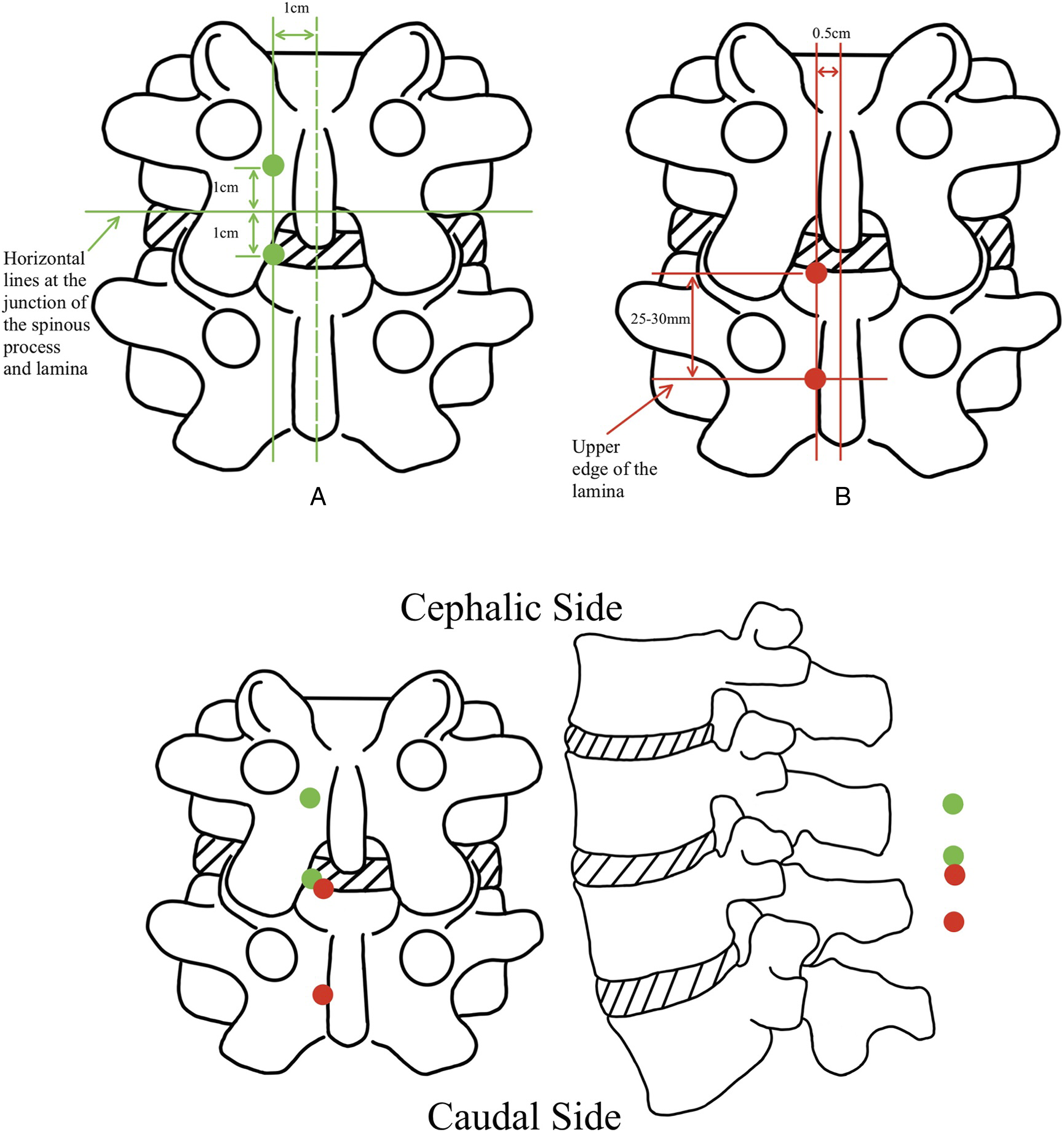
Even though the portal site of UBE-ULBD exhibits similarities to the UBE-interlaminar approach (all close to the posterior midline), it is still advised to go for the portal position situated more outside. The logic is that the portal away from the spinous process facilitates access to the contralateral side of the lumbar canal from the same side. Otherwise, navigating the endoscope across the midline via the base of the spinous process and into the contralateral spinal canal would be difficult, leading to significant bone injury and an increased risk of fracture at the base of the spinous process. As a result, during UBE surgery, the surgeon may suitably adjust the ULBD portal position outward based on the patient’s condition, thus facilitating the procedure.
Operation of Adjacent Segment Disease (Decompression Only)
Patients with Adjacent Segment Disease (ASD) who exhibit less severe symptoms and have fewer pathological alterations in bone structure may be candidates for an adjusted UBE-interlaminar approach surgery. Refer to Figure 8 to observe the precise endoscopic and working portal positions of the UBE-interlaminar approach (ASD).15,16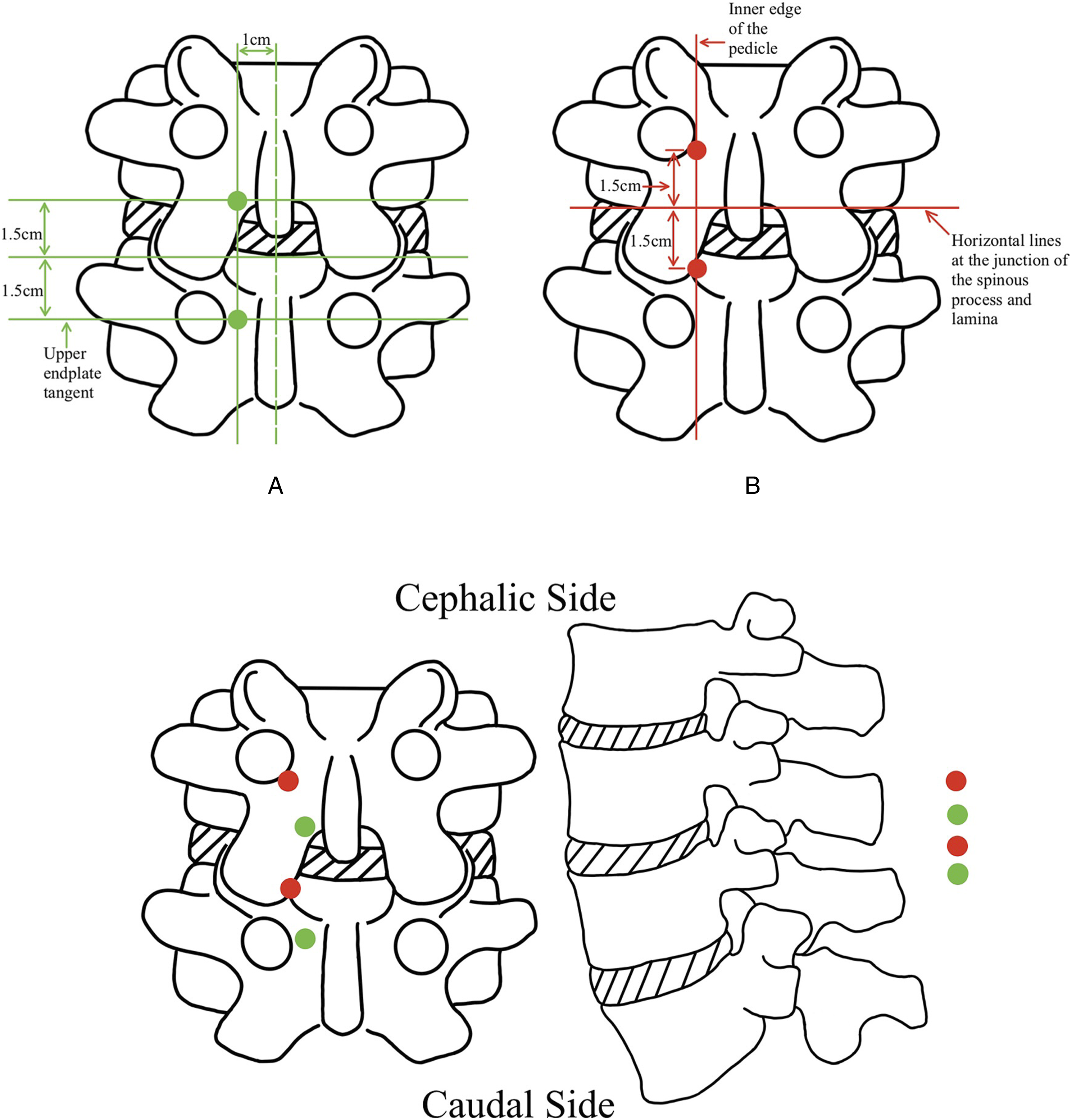
In addition to the aforementioned, the UBE-interlaminar approach can also be employed for a specific type of ASD mostly caused by degenerative changes in soft tissues, such as ossification of the ligamentum flavum. 16 After the UBE non-fusion approach is used to remove the soft tissue lesion, patients often experience significant alleviation without requiring additional fusion surgery to the adjacent deteriorated segment. For this specific form of ASD, the UBE approach does not have a fixed endoscopic and operational portal position. Instead, it should be adaptable based on the location of the soft tissue lesion. For instance, ASDs resulting from lesions such as spinal epidural lipomatosis can be effectively treated using the UBE-interlaminar approach, whereas posterolateral disc herniations can be treated using the UBE-transforaminal approach.
Lumbar UBE Fusion Surgery
Following the widespread use of the UBE technique in non-fusion surgery, Korean surgeons have extended its application to fusion surgery, thereby making significant contributions to the advancement of UBE technology. Recently, a growing body of studies have focused on applying the UBE technique in lumbar interbody fusion procedures to treat lumbar degenerative disease, ASD, and spondylitis.
Operation of Lumbar Degenerative Disease
For the UBE surgery, the indications of lumbar degenerative disease mainly refer to lumbar spinal stenosis with instability (including central canal stenosis and foraminal stenosis), lumbar spondylolisthesis of grade II below, lumbar disc herniation. Absolute contraindications to UBE fusion surgery for lumbar degenerative disease include severe osteoporosis, III degrees spondylolisthesis, and severe epidural scarring, whereas infection (early period) can be considered a relative rather than an absolute contraindication to UBE fusion surgery, which contrasts with open surgery. 17
The Portal Position of the UBE-PLIF Approach
Optimal indications for UBE-PLIF (Posterior Lumbar Interbody Fusion) are patients who require only ipsilateral traversing nerve root decompression or do not require nerve root decompression. During surgery, UBE-PLIF requires a nerve pull, but the nerve is particularly vulnerable at the level above L2 (Conus Medullaris), which means any shock of laminectomy or slight extrusion of the spinal canal may cause nerve injury. Hence, UBE-PLIF is exclusively applicable for treating segments below L3, while lesions in segments L2 and beyond are considered absolute contraindications.
The conventional portal location method of UBE-PLIF involves the following steps: Draw horizontal lines that correspond to the lower edge of the upper and lower vertebral pedicles in the surgical segment. Additionally, draw a vertical line parallel to the spinous process and locate it 1 cm away. The endoscopic portal and working portal are located where the upper and lower horizontal lines cross with the vertical line,
19
as depicted in Figure 9A (green dots).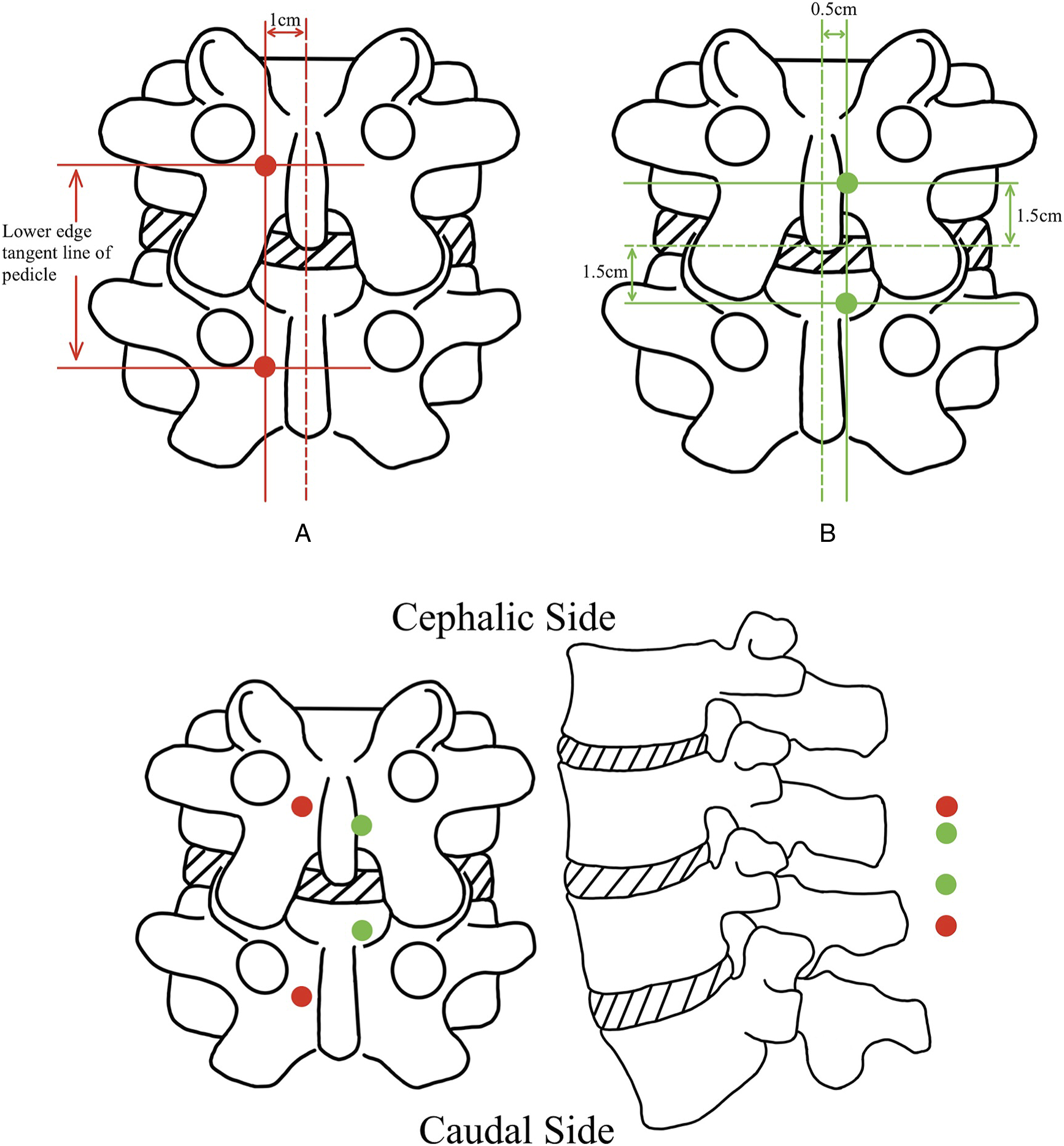
For a more similar surgical perspective to standard open PLIF surgery, the fresh portal position has been inwardly shifted and designed as follows: Make a vertical line parallel to the posterior median line with a distance of 0.5 cm, and draw horizontal lines 1.5 cm above and down the intervertebral space. The location of the endoscopic portal (approximately .5 cm in length) and the working portal (approximately 1.5 cm in length) at the points where the upper and lower horizontal lines cross with the vertical line, 20 as shown in Figure 9B (red dots).
However, there is a contentious debate around the alteration above, as several surgeons argue that endoscopic surgery should not be equated with open surgery. Although the inward displacement of the surgical portals does improve the similarity of the surgical field to open surgery, the proximity of the UBE-PLIF surgical portals to the spinous process poses a challenge in effectively utilizing instruments for the removal of the spinous process and other bony structures via the working portal. Therefore, a suggestion from Li has been put out to relocate the portals of the UBE-PLIF approach outward. 29 Unfortunately, Li’s study does not include details about the position used for the endoscope and working portals, and the account only mentions the pedicle as the anatomical reference. 29 Nevertheless, it is essential to acknowledge that the UBE-PLIF approach, which involves moving the incision outward, is increasingly gaining favor among surgeons.
Synthesizing the location of different UBE-PLIF approach portals, the UBE-PLIF approach demonstrates a lower degree of closeness to the midline of the spinous process when compared to the UBE-interlaminar approach. One primary rationale for choosing a UBE-PLIF portal at an extended distance from the midline is that positioning the portal of the UBE-PLIF approach closer to the midline of the spinous process results in a reduction in the surgical operating range and convenience. The second objective is to optimize the positioning of the fusion device inside the intervertebral space. Due to the small size of the PLIF technology fusion device, it is difficult for the surgeon to accurately place the cage in the middle of the intervertebral space during the UBE procedure, which may result in an uneven position of the cage within the intervertebral region, potentially leading to misalignment of the lumbar spine in the coronal plane. To solve this problem, it could move the surgical portal outward during fusion surgery to horizontally place the large-sized cage under endoscopy. So, when the portal of UBE-PLIF is positioned farther away from the midline, it facilitates the installation of the large-sized cage and ensures the optimal positioning of the fusion device inside the intervertebral space. The UBE-interlaminar approach does not have the issue of cage placement, so the portal location is generally closer to the posterior midline. Furthermore, the UBE-interlaminar approach is mainly used to treat paracentral types of disc herniation, so choosing a slightly off-midline approach through the lamina is more beneficial for the surgical procedure.
The Portal Position of the UBE-TLIF Approach
The optimal indication for UBE-TLIF (Transforaminal Lumbar Interbody Fusion) is patients who require decompression of both the ipsilateral traversing and exiting nerve roots. Unlike UBE-PLIF, UBE-TLIF can be used in all lumbar segments with no obvious characteristic contraindications.
The portal position method of the classic UBE-TLIF approach is cumbersome as follows: Endoscopic and working portals are placed at a distance of 1.5 cm above and below the point where the horizontal extension line of the lower part of the cranial lamina intersects with the perpendicular bisector of the upper pedicle,
35
as seen in Figure 10A (Green Dots).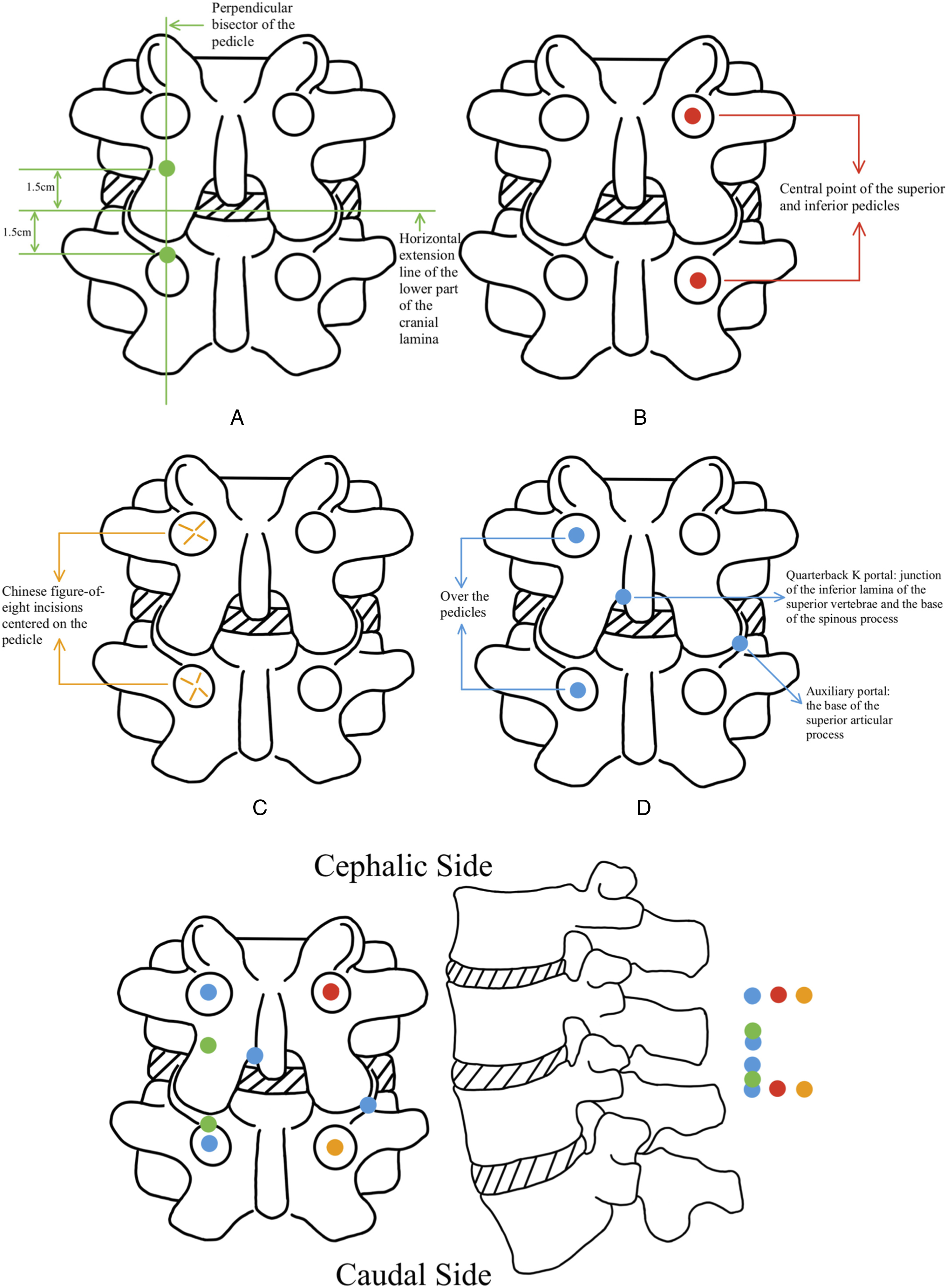
For simplified portal position methods of UBE-TLIF, 1 is to create portals at the central point of the superior and inferior pedicles of the surgical segment, which serves as the endoscopic and working portals, respectively, 21 as seen in Figure 10B (Red Dots). Another is to make a Chinese figure-of-eight (八) incision centered on the vertebral pedicle, with the caudal side as the working portal and the cephalic side as the endoscopic portal, 22 as seen in Figure 10C (Orange Dots).
To mitigate the high settling rate after the implantation of a single cage, a novel UBE-TLIF approach has been proposed with a modification by introducing an auxiliary portal on the non-surgical side to facilitate the placement of another cage, resulting in a bilateral double-cage fusion operation. The specific 4 portals’ positions are as follows: Endoscopic and working portals’ locations are the same as the red dots approach (Figure 10B), while the auxiliary portal is positioned over the base of the superior articular process on the non-surgical side, and a quarterback k portal is placed at the intersection of the inferior lamina of the superior vertebrae and the bottom of the spinous process on the surgical side, 37 as seen in Figure 10D (Blue Dots). Optimal indications for this novel UBE-TLIF approach also include lumbar spondylolisthesis and patients with central spinal stenosis requiring contralateral decompression.
Unlike the position relation between the UBE-interlaminar approach and UBE-PLIF, the portal position of the UBE-TLIF is more inward than the UBE-Transforaminal approach. The UBE-Transforaminal approach is mainly aimed at treating the nucleus tissue near the intervertebral foramen or the central disk herniation, especially in the treatment of the latter, in order to obtain a better surgical vision and operating space, requiring a larger channel inclination angle, so it is necessary to move the position of the surgery incision further out (even requires some shaping of the intervertebral foramen better to reach the central area of the intervertebral space). While placing the cage during UBE-TLIF surgery, it needs the resection of the inferior facet joint of the superior vertebral body and the superior facet joint of the inferior vertebral body of the diseased segment. Therefore, the portal position is more inclined to the back of the vertebrate (ie, dealing with nerve compression in a certain overhead view angle), and there is no need for larger perpendicular and more distant portals such as the Transforaminal approach.
The Portal Position of the UBE-EFLIF Approach
In order to mitigate harm to the facet joints during fusion surgery, the surgeon has put forth the UBE-EFLIF, which draws inspiration from the Endo-TLIF procedure, originally evolved from Extraforaminal Lumbar Interbody Fusion (EFLIF). 23 The optimal segments for the UBE-EFLIF approach are the L4-5 and L5-S1 segments, and the best indications are intervertebral foraminal stenosis and/or ipsilateral lateral recess stenosis without central canal stenosis and contralateral lateral recess stenosis.
UBE-EFLIF technique comprises three portals, two of which are roughly 1.5 cm long and act as the endoscopic or working portal, positioned 2 cm outside the upper and lower pedicle. A supplementary portal, referred to as the “quarterback portal,” is created to facilitate the rotation of the cage to a horizontal orientation by making a 1 cm incision where the intervertebral space intersects the tangent line at the inner edge of the vertebral pedicle,
23
as seen in Figure 11. The mainstream portal positions of the UBE-EFLIF approach
23
. (The dot size only provides a general indication and does not represent a specific proportion).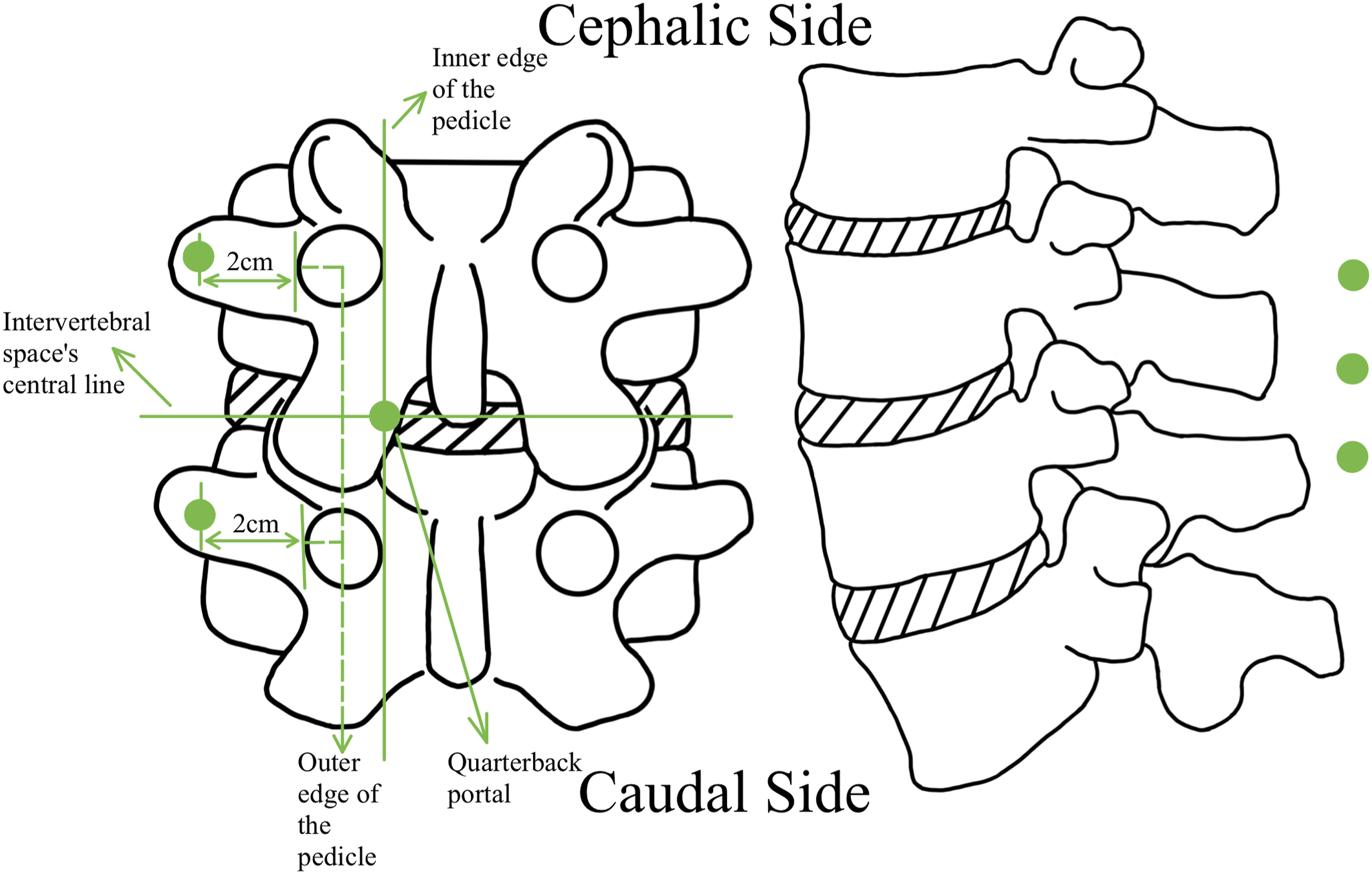
The location of the portal in UBE-EFLIF is closer to the outer side compared to UBE-TLIF due to the placing of a larger cage in UBE-EFLIF approach, which requires the cage’s placing position to be close to the front and central spacing region to keep the cage’s horizontal position. Therefore, it is necessary to take the portal’s position further away than the UBE-TLIF approach.
The Portal Position of the Ex-TLIF Approach
The Ex-TLIF (Extreme transforaminal lumbar interbody fusion) approach has been offered to address the issue of rapid cage sinking caused by the small volume of the implanted cage in the UBE-TLIF approach. 24 Its method to deal with the above problem is to install an Oblique Lateral Interbody Fusion (OLIF) cage, which has been proven workable and does not injure the traversing and exiting nerve roots at L4-5 and L5-S1 segments. 24 Ex-TLIF is recommended for treating various forms of spinal stenosis and low-grade lumbar spondylolisthesis. However, it is essential to note that Ex-TLIF should only be performed if the space between the traversing and exiting nerve roots is longer than 20 mm, which could be considered a relative contraindication to the Ex-TLIF approach.
The portal positioning method utilized in the EX-TLIF approach shares a fundamental similarity with the UBE-TLIF approach, which means that in both methods, the endoscopic portal and working portal are created at the upper and lower pedicles. However, to properly install the giant OLIF cage in the Ex-TLIF approach, not only a higher inclined angle is required, but also an additional paravertebral portal is made for the insertion of a large OLIF cage.24,36
In comparison to the UBE-EFLIF approach, the EX-TLIF approach has implemented 2 noteworthy enhancements. Initially, the auxiliary portal is relocated to the outer margin of the pedicle. Additionally, the complete removal of the facet joint is undertaken to facilitate the insertion of a giant OLIF cage. In contrast to the UBE-TLIF technique, the distinguishing characteristic of the EX-TLIF approach is the utilization of a giant Cage, which is implemented following the principles of the UBE-TLIF. Apart from this, the procedure of cage implantation in Ex-TLIF entails navigating through the Kambin triangle and requires preoperative evaluation of the base length of the Kambin triangle, which is a notable distinction from the UBE-TLIF approach.
Operation of ASD
Patients diagnosed with ASD who exhibit minor symptoms may only need decompression treatment as mentioned above. Nevertheless, individuals experiencing severe symptoms may necessitate the implementation of a fusion device and internal fixation to mitigate clinical manifestations (lumbar fusion extension surgery). By improving the UBE-TLIF approach, the UBE can now be utilized in treating ASD patients who require fusion surgery called UBE-Fusion Extension Surgery (FES). The indications for UBE-FES are identical to conventional FES, mainly for individuals with symptomatic ASD, including adjacent lumbar stenosis, adjacent lumbar instability, and instrument failure due to fractured screws and rods, while contraindications include junctional vertebral fracture, infection, junctional kyphosis, and deformity correction surgery.
The UBE-FES exhibits greater complexity than the UBE-TLIF, as it involves 2 kinds of portals including the placement of the fusion cage and the subsequent removal and insertion of the internal fixation. The positions about portals for cage placement are as follows: Portals of 1.5 cm in length are created either vertically or horizontally at the position of the upper and lower pedicle or screw head over the ASD segment. The endoscopic portal is situated on the cranial aspect, while the working portal on the caudal side is employed for surgical procedures, as seen in Figure 12A (Green Dots). And the positions of the portals for the operation of internal fixation are as follows: The portals previously used for the placement of cages and a new portal measuring approximately 1.5 cm in length located at the outer edge of the pedicle of the surgical segment vertebrae (close to the original fusion segment side) are both employed for the remove and installation of the internal fixation, as seen in Figure 12B (Red Dots). Due to the UBE endoscope with a diameter of roughly 4 mm, sufficient room is supplied to accommodate 2 portals at 1 incision. Based on this, to enhance operational convenience, the approach innovatively employs the placement of the endoscopic and working portals into a singular incision and achieves good therapeutic results.
25
The mainstream portal positions of the UBE technique to treat ASD (Fusion).
25
(The dot size only provides a general indication and does not represent a specific proportion).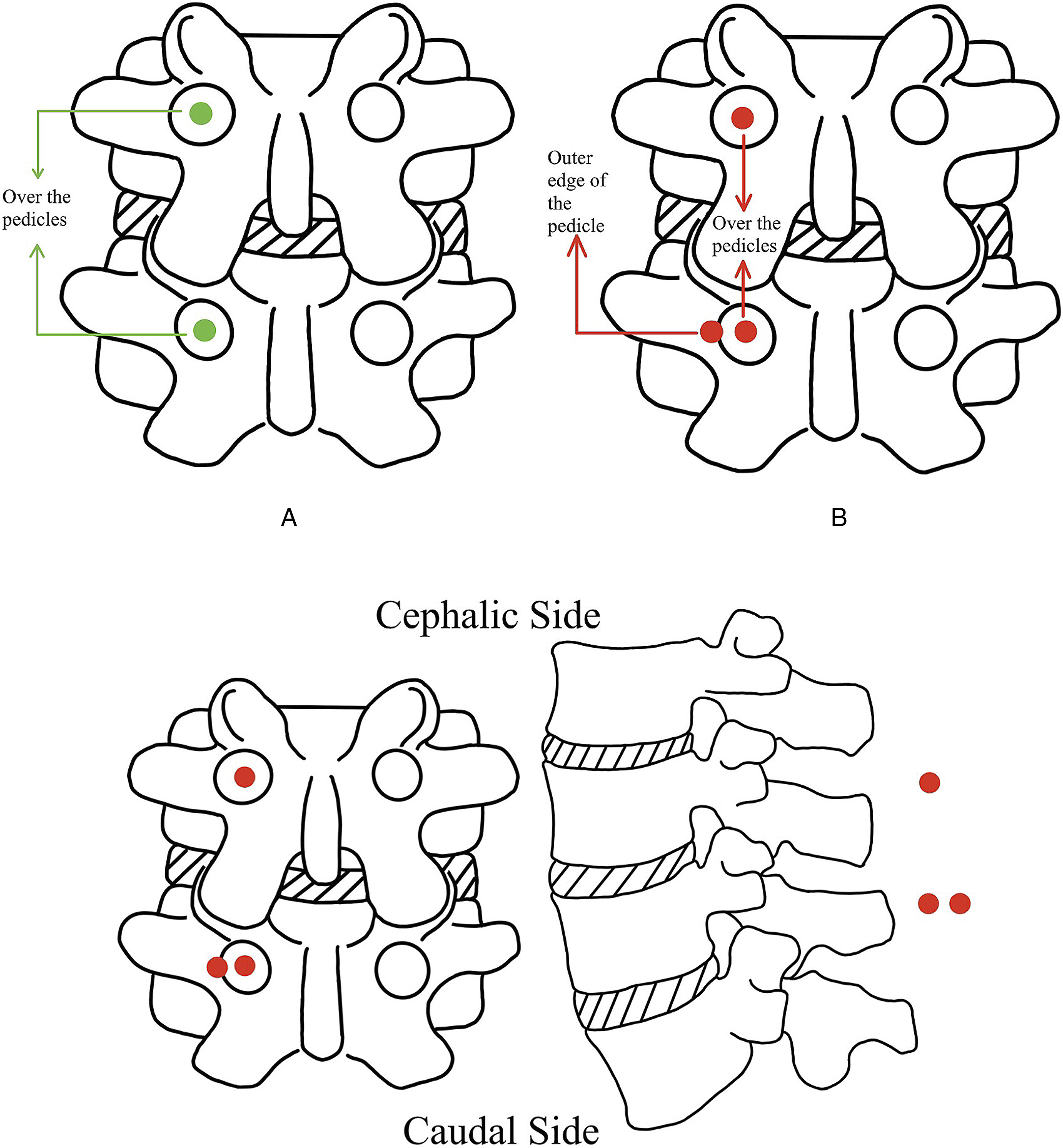
Operation of Lumbar Spondylitis
Antibiotics are less efficacious in treating granulomatous spondylitis and typically necessitate surgical intervention in patients with severe symptoms.41,42 For granulomatous spondylitis (especially referred to as tuberculosis and brucellosis), the following has been suggested as the universal UBE approach’s portal position method: A horizontal line is formed at the juncture where the base of the spinous process intersects with the lower border of the lamina on the upper vertebrae in the operative segment. Concurrently, a vertical line is delineated along the outer edge of the upper pedicle. The intersection of these 2 lines functions as a reference point. Longitudinal incisions, measuring 1.5 cm in length, are executed at locations 1 cm above and below the designated reference point. The cephalic incision acts as a portal for endoscopy and lavage procedures, while the caudal incision operates as a portal for working and drainage activities,26,27 as seen in Figure 13.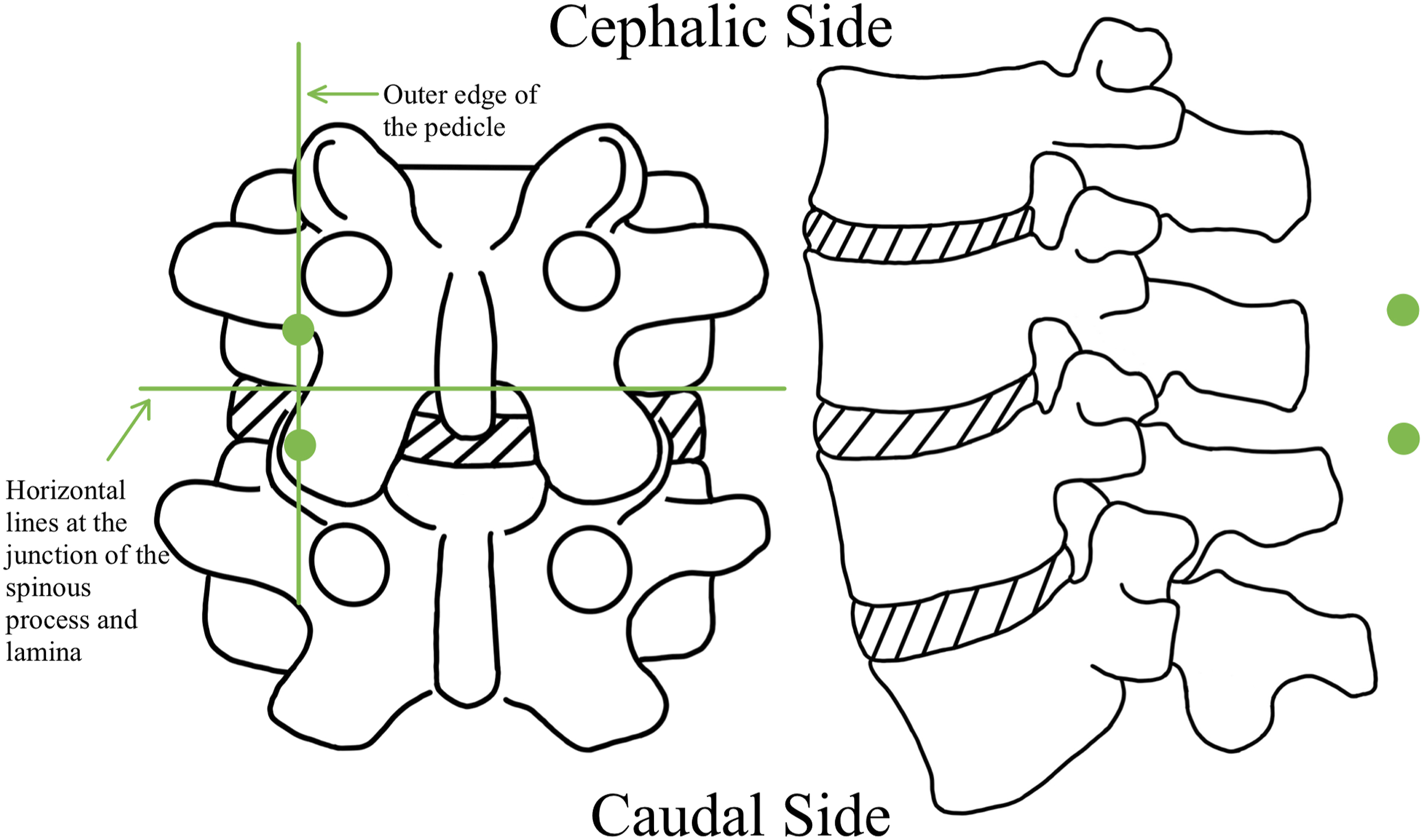
Compared to the UBE portal position designated for treating epidural abscesses, the UBE portal position for treating spondylitis is located closer to the outside. This is due to the primary goal of treatment for a pure epidural abscess is to drain the pus, and the surgical portal positioned on the posterior side can take advantage of the interlaminar approach to remove the lamina for decompression and fully expose the dural sac, facilitating the continuous irrigation and drainage. Patients with granulomatous spondylitis often have pathogens hidden within the intervertebral disc and surrounding structures. If not thoroughly debrided, the disease frequently recurs shortly after surgery. Portals close to the intervertebral foramen are more advantageous for removing intervertebral discs and upper and lower endplate cartilage, purulent fluid in the spinal canal and around the vertebral body, as well as sclerotic bone. In addition, in patients with granulomatous spondylitis, the upper and lower endplates at the affected segment are usually severely invaded and damaged, resulting in significant collapse of the intervertebral space, making it difficult to implant a cage. Therefore, fusion is often performed in the anterior part of the intervertebral space using bone grafting, followed by the implantation of a cage containing doxycycline or rifampicin in the posterior part after the height of the intervertebral space is restored. So, the portals closer to the outer side would be more favorable for surgical instruments accessing the anterior part of the intervertebral space and facilitating the surgical procedure. If a patient has both epidural abscess and spondylitis, a combined method can be employed for treatment using both fusion and non-fusion UBE infectious approaches.
Relationship Between the Different UBE Surgical Approaches
Based on the above methods for localizing different UBE portals, it becomes evident that the principal surgical portals for UBE are primarily situated at the 5 mm lateral to the spinous process, 1 cm lateral to the spinous process, the inner edge of the pedicle, the central point of the pedicle, the outer edge of the pedicle, and 2 cm away from the outer edge of the pedicle. Among these localization indicators, the positions between the 1 cm lateral to the spinous process and the inner edge of the pedicle are not precise, while the relative positions between the other localization markers are clear.
Distance Between the Medial Edges of the Narrowest Section of the Vertebral Pedicle. 43
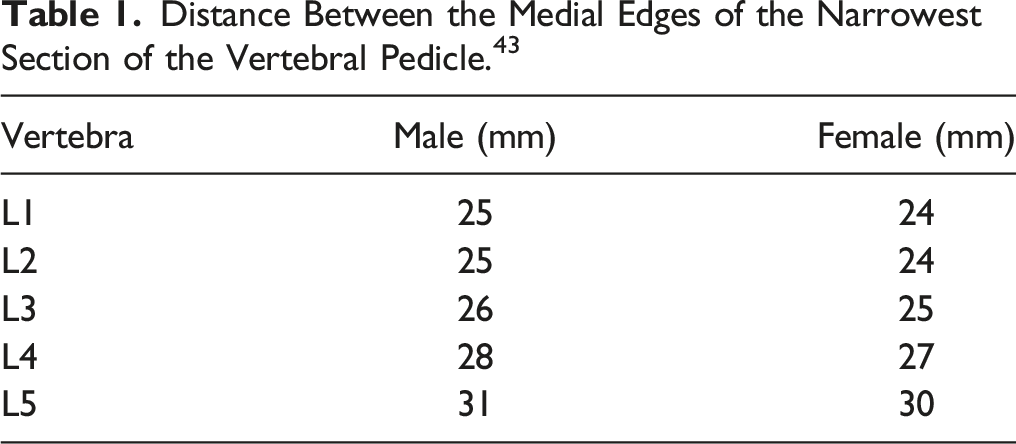
Posterior midline as the reference standard, it becomes apparent that the sequence of UBE portals, progressing from innermost to outermost, includes UBE-interlaminar approach (Disc herniation, PARS, ASD, and Epidural abscess), UBE-PLIF, UBE-ULBD, UBE/Ex-TLIF and UBE-FES, UBE-Spondylitis, UBE-EFLIF and UBE-Transforaminal approach. The location relations of the different UBE surgical approaches in the horizontal plane and the coronal plane are seen in Figure 14. Schematic diagram of the portal location of different UBE approaches in the horizontal plane and coronal plane.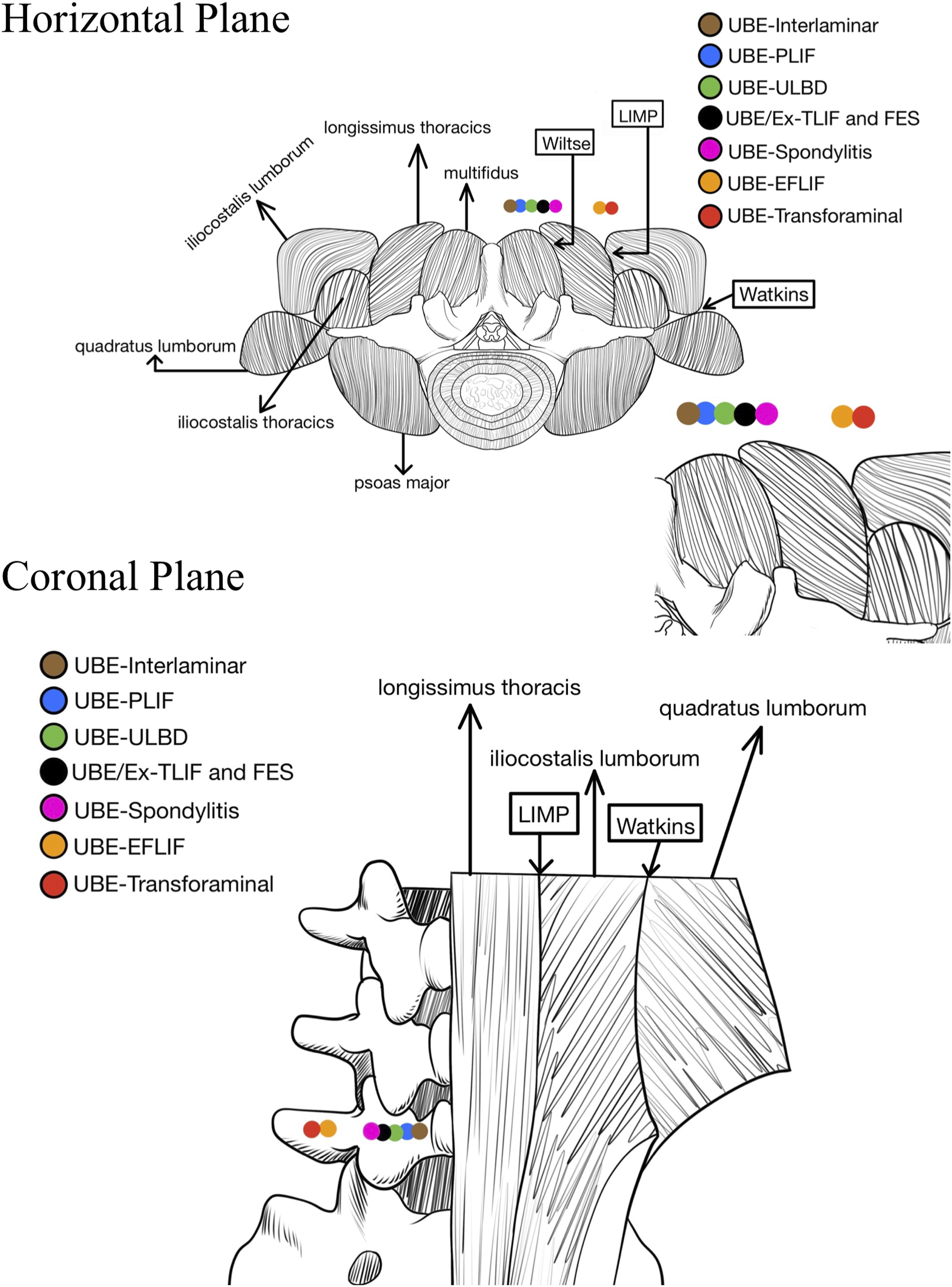
Discussion
As previously stated, the diverse UBE portal position methods may pose challenges for novices, impeding their ability to comprehend and proficiently grasp the interconnections among these approaches promptly. At the same time, an overly mechanized selection of portal locations may pose challenges for surgeons when operating on atypical types of spinal lesions during surgery. Hence, the positioning of the portal for UBE lumbar spine surgery can be modified to accommodate varying patients’ lesions according to the dividing surgical areas. Specifically, the localization method of surgical portals should be returned to the constant bony anatomical landmarks of the lumbar vertebrae. In contrast to other surgeons proposing specific portal localization methods for a particular approach, the portal position of different UBE approaches can be defined within a specific range delimited by a series of related constant anatomical landmarks. Surgeons can flexibly and adaptably choose the surgical portal position from a designated range, considering the patient’s current condition and the precise location of the lesion.
Nowadays, there is a growing popularity in the field of robot-assisted UBE surgery. 45 The robot utilizes preoperative CT and intraoperative fluoroscopy to accurately identify significant bone landmarks and is then used to determine the most suitable UBE surgical portal position for the patient and assist in establishing the surgical path. The constant anatomical landmarks of the lumbar spine (not susceptible to degenerative deformities) proposed as markers for different surgical intervals in this study can be maximally compatible with robotics, and more conveniently and succinctly indicate surgical intervals for the robot, thus constructing individualized UBE portal positions and surgical pathways. Furthermore, radiation-free ultrasound-guide has also been made in endoscopic spinal surgery. 46 Dividing the area between the midline of the spine and the transverse process into different intervals using the anatomical landmarks helps to summarize and identify the unique sonographic features of each zone, promoting surgical safety and efficiency and reducing x-ray radiation.
The specific novel UBE portal interval localization method is as follows: The segmentation of portal locations for various UBE approaches can be divided into 4 distinct intervals by utilizing 3 bony landmarks, namely the spinous process, pedicle, and transverse process, along with the identification of 3 well-known muscle gaps in the posterior aspect of the lumbar spine (in order from the inside to the outside, Wiltse approach, Lateral Intramuscular Planar (LIMP) approach, and Watkins approach).47-49 Segment 1 - from the midline of the spinous process to the inner edge of the pedicle; Segment 2 - the region of the pedicle; Segment 3 - from the outer edge of the pedicle to the midpoint of the transverse process; Segment 4 - from the midpoint of the transverse process to the distal end of the transverse process. Refer to Figure 15 for a visual representation of the 4 anatomical intervals and the corresponding UBE approaches associated with each interval. Schematic diagram of 4 anatomical intervals.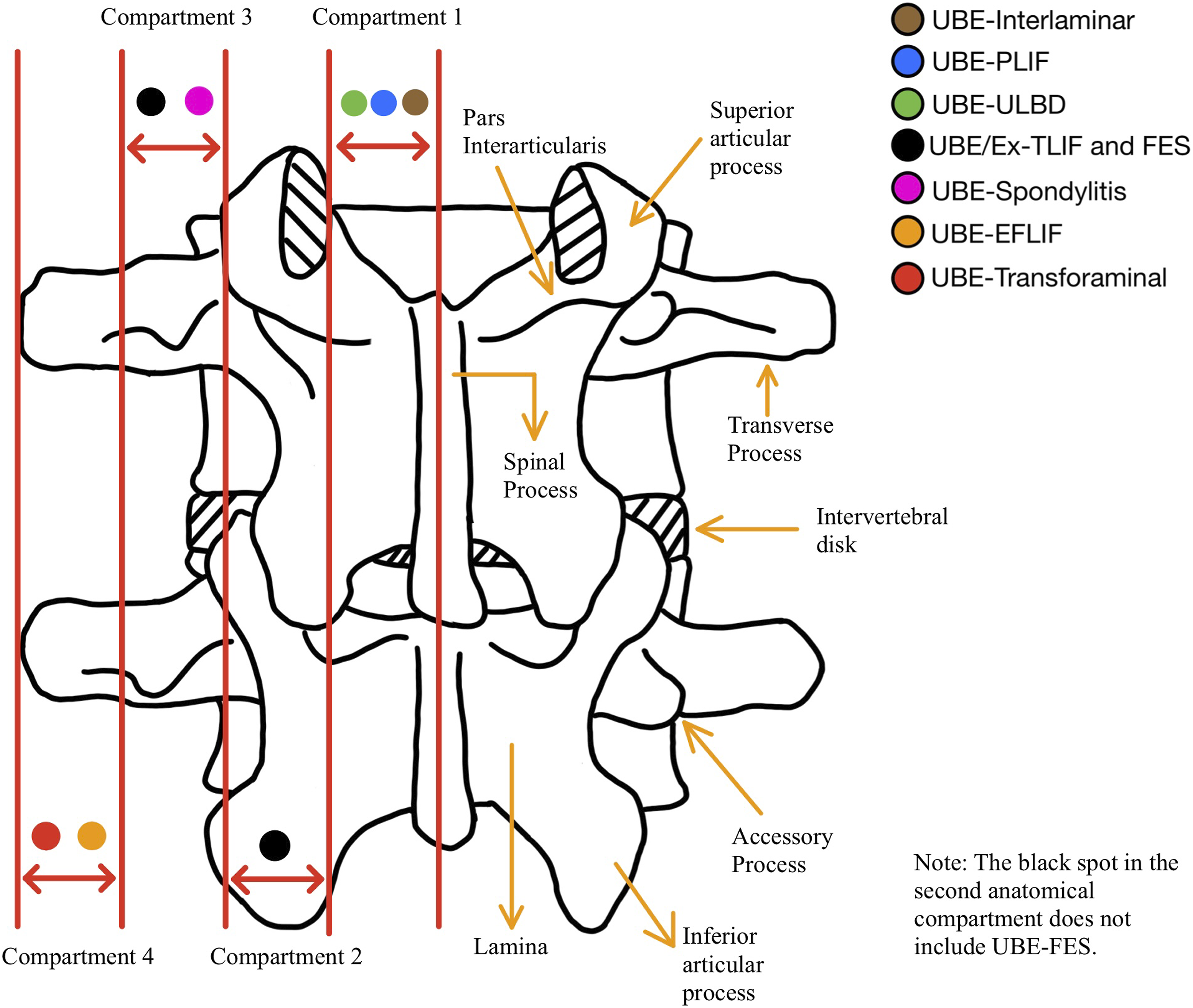
The first anatomical segment comprises 3 UBE approaches: the UBE-Interlaminar approach (Disc herniation, PARS, ASD, and Epidural abscess), the UBE-PLIF, and the UBE-ULBD. The indications for the first anatomical interval mainly include the intervertebral disc herniation located in the subarticular zone (lateral recess), PARS type I, epidural abscess, mildly symptomatic ASD as well as ASD caused by degenerative changes in the posterior soft tissue structures of the lumbar spine. In addition, it encompasses diseases such as LSS and SLSS, including hypertrophy of the ligamentum flavum, bilateral lateral recess stenosis, and contralateral exiting nerve root stenosis, as well as degenerative lumbar spine diseases requiring fusion surgery without neural root decompression or with only decompression of the traversing nerve root.
Rather than adhering to a rigid portal positional relationship among those 3 UBE approaches, the 3 UBE approaches’ portal positions can be chosen somewhere within the confines of the first segment, with necessary modifications contingent upon the individual patient’s unique circumstances.
The pars interarticularis of the upper lumbar spine (L1-L3) is often characterized by narrowly spaced. 50 When decompressing or removing a disc in the upper lumbar spine, if the endoscopic view is restricted to the lower part of the lamina, there is a significant danger of unintentionally decompressing externally and causing harm to the pars interarticularis unless exact preoperative calculations are made. The pars interarticularis is the area that undergoes the highest stress level during the movement of neighboring segments of the spine, and damage to the pars interarticularis during surgery could lead to the development of secondary lumbar spondylolisthesis following the procedure. 51 In the first anatomical interval, this problem could be solved efficiently using the significant landmarks: the medial edge of the facet joint to help determine the range of decompression required and then minimize pars interarticularis injuries during UBE surgery, which could be seen as the advantage of executing UBE surgery in the first anatomical interval.
During UEB surgery in the first anatomical interval, the primary complications that may arise are cauda equina nerve injury and dural sac tear. Cauda equina nerve injury primarily occurs during the contralateral decompression procedure of the UBE-ULBD, wherein a 0° spinal endoscope is employed to exert pressure on the dural sac, accordingly damaging the cauda equina nerves. Hence, it is advisable to exercise caution while conducting UBE-ULBD over-the-top procedure and prioritize the utilization of a 30° endoscope whenever feasible. Dural sac tear may occur in all UBE surgeries performed in the first anatomical interval, which is mainly caused by the poor anatomical understanding of the operator, severe spinal canal stenosis, etc. To address this issue, minimizing the traction tension on the dura when resecting the ligamentum flavum and managing blood pressure throughout the procedure to prevent complications effectively is beneficial. 52
The second anatomical region encompasses the UBE-TLIF and the Ex-TLIF. This anatomical interval is specially designed for patients with lumbar degeneration who require fusion surgery and simultaneous decompression of both the traversing and exiting nerve roots. Because of the removal of the facet joint, in the context of UBE/Ex-TILF surgeries, the incisions are recommended to be close to the outer side of the second anatomical interval, and the whole third anatomical interval. In clinical practice, partial medial facetectomy can also fulfill the needs of decompression and cage implantation without necessitating complete removal of the facet joint, making it a viable option in surgery. This fusion operates between PLIF and TLIF and can be referred to as UBE-PTLIF. While the direct proposal of UBE-PTLIF is lacking, certain surgeons have actually incorporated the UBE-PTLIF surgical method within their UBE-TLIF surgery. 53 The benefit of this new approach is that it maintains partial stability on the operational side while preventing irritation to the exiting nerve roots and scar formation in the intervertebral foramen that can lead to nerve root adhesion. The endoscopic and working portal positions of UBE-PTLIF are identical to UBE-TLIF. However, to accommodate contralateral decompression needs, the portal position of UBE-PTLIF may be slightly shifted inward, potentially reaching as close to the junction between the second and first anatomical intervals. Overall, the range and variability for selecting UBE/Ex-TLIF incisions are considerable.
As stated above, the best indication for UBE/Ex-TLIF surgery in the second anatomical interval is patients requiring bilateral root decompression, especially exiting nerve roots. To achieve good decompression of the exiting nerve root, most surgeons currently believe that removing the tip of the superior articular process and removal of the ligamentum flavum in the intervertebral foramen area is sufficient while neglecting decompression in the inner and lower region of the pedicle. Decompression in the inner and lower region of the pedicle is mainly for decompression of bony stenosis combined with hypertrophy of the ligamentum flavum, which facilitates good mobility, pulsation, and reperfusion of the exiting nerve root. When carrying out UBE surgery in the second anatomical interval, it is relatively easy to complete decompression in the inferior pedicle region while removing the tip of the superior articular process, and it also provides reasonable consideration for the Corner region without oblivion. In addition, not all patients have the tip of the articular process covering the exiting nerve root and abutting the lower edge of the transverse process. 54 For such patients, direct removal of the tip of the articular process may cause damage to the exiting nerve root. Within the second anatomical interval, using the position near the inferior wall of the pedicle as the first dock point and finding the exiting nerve root located at the lower wall of the pedicle is practical for all patients, and this is also the unique advantage of UBE surgery in the second anatomical interval.
Complications that are prone to occur during surgery in the second anatomical interval are mainly epidural hematoma (hidden bleeding) and dural injury. The leading cause of epidural hematoma is the radicular artery accompanying the nerve root in the area outside the intervertebral foramen, and the artery is easily injured when handling the nerve root. After the injury, the radicular artery bleeding is intense. Meanwhile, high irrigation water pressure during the procedure can cover up the bleeding point, leading to inadequate hemostasis. There is no specific solution to this problem, and the key lies in being familiar with the anatomy of the intervertebral foramen area, as well as controlling blood pressure during withdrawal of the tracheal tube (for general anesthesia patients) or choosing spinal subarachnoid block anesthesia, controlling water pressure during surgery (recommend 2.41-22.84 mmHg 55 ), and ensuring adequate hemostasis, which can play a certain preventive role.
Furthermore, for novices, undergoing UBE\Ex-TLIF surgery in the second anatomical interval can also easily lead to postoperative non-surgical side neurological symptoms. This is mainly due to inadequate decompression of the intervertebral space, forcibly implanting the cage, causing the cage to tilt towards the surgical side, resulting in rotation of the upper vertebral body and reduced height on the non-surgical side. Occasionally, symptoms may also occur because the cage is too close to the non-surgical side, causing the facet joint on the non-surgical side to open and dislocate anteriorly, leading to radicular symptoms. The primary solution to postoperative non-surgical side neurological symptoms of UBE\Ex-TLIF is accurately placing the cage. Additionally, if signs of contralateral intervertebral foramen stenosis are found, preventive excision of the facet joint tip can be performed. Moreover, for patients with degenerative spondylolisthesis, full release and reduction with the cage should be performed, avoiding traction reduction that may lead to excessive reduction, causing the tip of the contralateral superior articular process entrapment on the exiting nerve root.
In the third anatomical segment, in addition to the above-mentioned UBE/Ex-TILF, the portals for UBE-FES and UBE-spondylitis can also be selected in this anatomical interval. The boundaries on the inner and outer sides of the third anatomical segment are consistent with the commonly used 2 muscle gaps in clinical practice: the Wiltse approach on the inner side and the LIMP approach on the outer side. UBE/Ex-TILF surgery in the third segment is mainly for patients with abnormalities in immunity and resilience who are prone to delayed wound healing and wound infection after surgery, and in severe cases, septic shock may occur.56,57 For these special patients, the 2 naturally existing anatomical gaps in the posterior lumbar spine can be fully utilized. Specifically the UBE/Ex-TLIF surgery can be made through the muscle gap between the multifidus muscle and the longest muscle (Wiltse approach) to reach the facet joints to complete the surgery, or then outwardly through the LIMP approach between the longest muscle and iliopsoas muscle, which all can further minimize the damage of the surgery on the patient’s muscles and benefit the patient’s postoperative recovery. This is also the reason why the portal position of UBE-spondylitis for granulomatous infection is sited in this segment.
Unlike simple fusion surgery, The UBE-FES procedure entails the extraction of the preexisting screws and connecting rods, with particular emphasis on the complete removal of the connecting rod by utilizing its inherent curvature. Identifying soft tissue damage at the surgical site has been recognized as a potential etiological component contributing to the development of ASD. 58 Utilizing the Wiltse approach and LIMP approach within the third anatomical segment as a natural pathway to remove the initial internal fixation and insert a new internal fixation can effectively reduce the musculoskeletal system damage, thereby diminishing the long-term recurrence rate of ASD. Furthermore, individuals diagnosed with ASD who need fusion surgery generally necessitate the insertion of a larger-sized cage during the secondarily affected segment (First segment above the orginal fusion site). 59 This is done to preserve a greater height of the intervertebral space and reduce the likelihood of excessive settling, thus mitigating the potential development of ASD. Therefore, in the context of surgical procedures, certain medical practitioners may opt for using the EX-TLIF surgical technique to place a large cage instead of solely conducting fusion surgery akin to UBE-TLIF (First step in UBE-FES). Based on this, employing portals at the third anatomical segment to perform UBE-FES surgery offers more significant benefits in facilitating the surgical procedure and enhancing the overall efficacy of the therapy for the patient.
In contrast to other anatomical intervals, the endoscopic and working portals of the third anatomical interval are relatively fixed because of the heavy reliance on intermuscular space for surgery in this interval. The portals are basically located near the skin entry point of the intermuscular space and then fine-tuned based on this, unlike other anatomical intervals where the surgical approach can be adjusted throughout the entire anatomical interval corresponding to the location of the lesion and the surgeon’s habits. This is precisely the unique advantage and disadvantage of the third anatomical region.
In general, the third anatomical interval is located laterally to the lumbar vertebrae, which means that during the cage implantation in this interval, it is unnecessary to fully resect the facet joint, unlike in the second anatomical interval. Typically, it is sufficient to solely resect the facet joint on the outer side to insert the cage. This implies that the placement path of the cage in the third anatomical interval is closer to the front side of the Kambin triangle (the angle between the endplate and the exiting nerve root), making a greater likelihood of compressing and harming the nerve root during the implantation process. In order to avoid damage to the nerve root during surgery in the third anatomical interval, foraminotomy can be carried out to enlarge the space for the insertion of a cage. For beginners, it is also possible to carry out early cadaver simulation training to enhance spatial orientation during endoscopy and optimize the utilization of surgical equipment. Furthermore, surgical procedures in the third anatomical interval mainly target patients who are infected or have a high susceptibility to infection. To prevent postoperative infections, unnecessary tissue damage should be avoided as much as possible during the surgery, and attention should be paid to managing postoperative drainage tubes to prevent retrograde infections.
Both the EFLIF approach and the UBE-Transforaminal approach are situated within the fourth anatomical interval. The indications for the fourth anatomical interval include intervertebral disc herniation in basically all regions, PARS type III, lumbar canal stenosis especially in the intervertebral foramen and lateral recess, and lumbar spondylolisthesis of up to grade II.
The portal of the EFLIF approach is situated in closer proximity to the posterior midline, whereas the portal of the UBE-Transforaminal approach is positioned nearer to the distal end of the transverse process. In the context of the EFLIF surgery, it is crucial to ensure that the incision is positioned in close proximity to the midline of the transverse process (allowing for changes in the vicinity of the midline). This is due to the necessity of promptly performing hemostasis on the epidural blood vessels that are bleeding following the removal of the lateral portion of the facet joint on the same side and the ligamentum flavum during the EFLIF procedure. If the incision deviates excessively inwards, it could impede the extraction of the superior facet joint and the placement of a sizable cage at an oblique orientation towards the central axis of the intervertebral space. In a situation in which the incision extends excessively outside, it has the potential to limit the efficient removal of the lamina and ligamentum flavum, as well as the efficient management of bleeding from the epidural blood vessels. While performing the UBE-Transforaminal approach, in order to completely remove the nucleus pulposus and preserve the integrity of the annulus fibrosus for annular repair surgery on the outer edge of the nerve root, it is necessary to expose the intervertebral disc in the intervertebral foramen adequately. If the surgical portal of the UBE-Transforaminal approach is too inward, it may impede the surgical field by encountering structures such as the facet joint, thus hindering the surgical procedure. Additionally, if the UBE-Transforaminal approach is used to deal with central intervertebral disc herniation, it is crucial to consider the distance between the skin incision and the spinous process. By appropriately adjusting the incision location outward, the surgical instruments can be positioned closer to the herniated disc, thereby facilitating the successful completion of the surgery.
The advantages of the fourth anatomical interval mainly lie in the uniqueness of the field of vision. The fourth anatomical interval, due to its overall outer position, allows for a complete lateral view of the entire vertebral pedicle area during the operation, that is, a direct view of the intervertebral foramen and the Kambin triangle, making it more convenient for the operating surgeon to determine the scope of the foraminotomy, thus providing a more complete exposure of the lateral recess compared to other anatomical intervals in UBE surgery. At the same time, due to the outer position of the portal, UBE surgery in the fourth anatomical interval can also better handle the Far-out syndrome (lesion located in the region formed by transverse processes, sacral wings, and iliolumbar ligaments), 60 further expanding the surgical indications. In addition, UBE surgery in the fourth anatomical interval can more conveniently observe and treat lesions near the anterior aspect of the vertebrae, such as extreme lateral disc herniation, reducing the difficulty of this type of surgery.
A unique complication that tends to occur in the fourth anatomic interval is retroperitoneal effusion. 52 The transverse ligament is located within the fourth anatomical interval. When selecting the surgical portal in the fourth anatomical interval, if the surgeon is not familiar with the anatomical structures or exerts excessive force, it may easily push the endoscope to the ventral side of the transverse ligament, causing injury to the psoas major muscle and leading to irrigation fluid entering the retroperitoneal space. Additionally, prolonged surgical duration and high water pressure are also causes of retroperitoneal fluid collection. To address this, reducing water pressure, lowering power radiofrequency output, and shortening the surgical duration can help, especially in preventing the endoscope from penetrating the ventral side of the transverse ligament. Furthermore, for beginners, due to the distance between the fourth anatomical interval and the intervertebral foramen, the instruments often form a certain angle with the intervertebral foramen region, which may result in visual aberration during processes such as upper facet joint resection, nucleus pulposus removal, decompression, or even insertion of a fusion device, which can lead to inadequate decompression and early recurrence. In this regard, the correct selection of the surgical approach, meticulous preoperative assessment of the lesion site, and intraoperative fluoroscopy assistance are better solutions.
Summary of the Different Anatomical Interval.
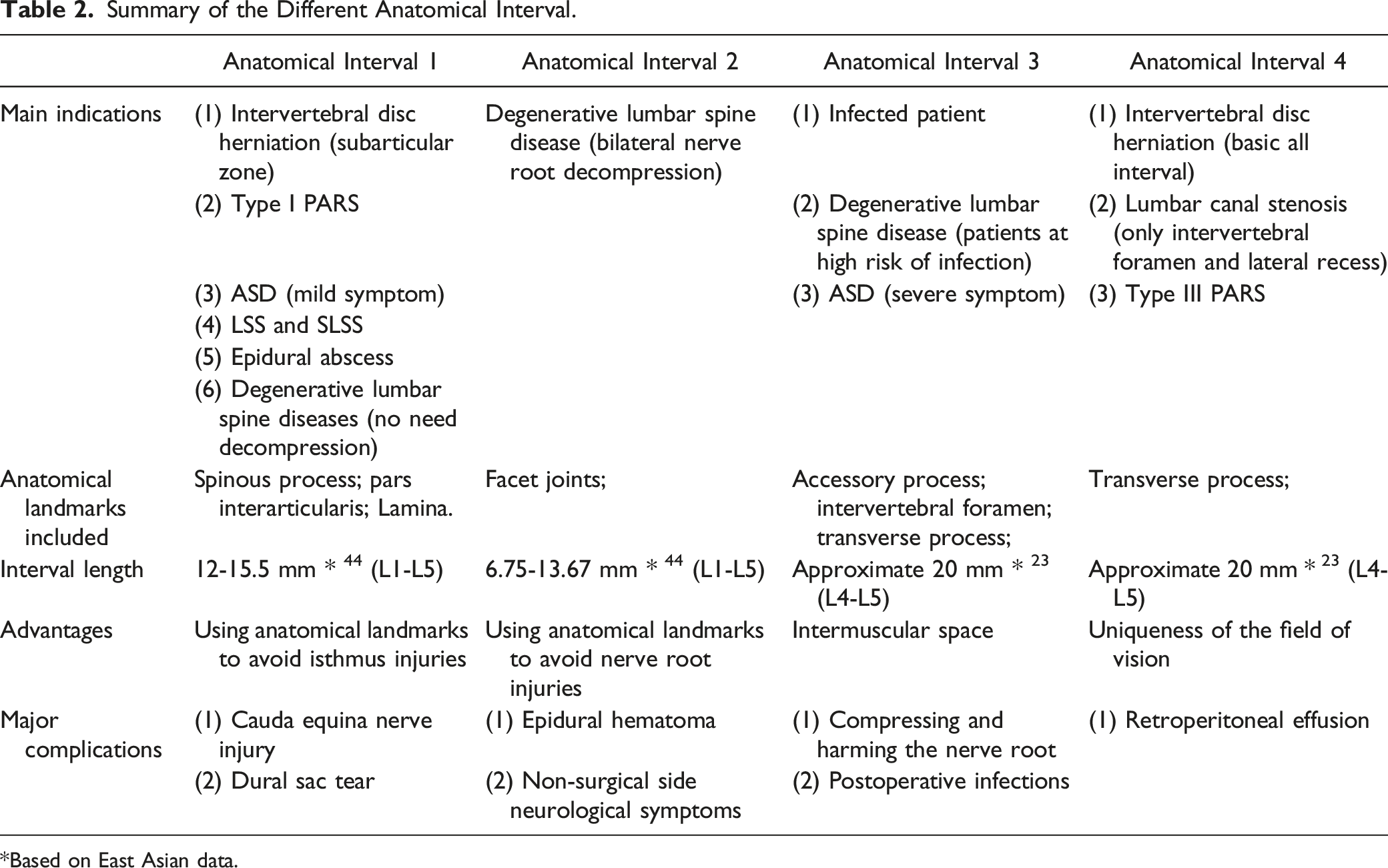
*Based on East Asian data.
The study reviewed the literature and researched the relationship between different surgical portals for UBE. Nevertheless, it is essential to acknowledge certain constraints or restrictions. For instance, some studies that have made only minor changes to the mainstream portal positioning methods (such as changes in endoscopic and working portal distances) have yet to be included in the literature list and mentioned in the results section. Additionally, some less commonly used UBE surgeries, such as the use of UBE techniques to treat pseudomeningocele caused by dural tears after lumbar spine surgery, have not been included in this study. 61
Conclusion
The research presents a preliminary overview of the historical evolution and methodologies for determining the portal sites of various UBE approaches. Furthermore, the study elucidates the correlation among distinct portal locations, drawing upon pertinent anatomical research material. Based on this, the study develops a standardized framework for various portals in different UBE approaches, and these portals will be classified into distinct anatomical intervals. Through this study, it is expected that in clinical practical work, the surgeons, according to the different locations of the lesion and in combination with the appropriate anatomical markers of the lumbar vertebrae, will reasonably and accurately select the UBE approach, which will improve the minimally invasive and accuracy of the endoscope technique.
Supplemental Material
Supplemental Material - The Method of Portal Making in Lumbar Unilateral Biportal Endoscopic Surgery with Different Operative Approaches According to the Constant Anatomical Landmarks of the Lumbar Spine: A Review of the Literature
Supplemental Material for The Method of Portal Making in Lumbar Unilateral Biportal Endoscopic Surgery with Different Operative Approaches According to the Constant Anatomical Landmarks of the Lumbar Spine: A Review of the Literature by Yixi Wang, Abulikemu Maimaiti, Abudusalamu Tuoheti, Yang Xiao, Rui Zhang, Alafate Kahaer, Dongshan Liu, and Paerhati Rexiti in Global Spine Journal
Data Availability Statement
All datasets generated for this study are included in the article.
Footnotes
Acknowledgments
We want to extend our sincere appreciation to Han-Fei Zhang, a scholar affiliated with Southwest University in China; Yu-Qiao Tang, a researcher associated with Northeastern University in the United States; Ruo-Xuan Fu, an academic from The University of Utah in the United States; and Lin-Huan Lei, an English expert from Southwest University in China, for their invaluable contributions in enhancing the linguistic quality of the article and evaluating the revised manuscript. We would also like to express our gratitude to Lin-Tao Xia from Chongqing Medical University in China and Yi-Shan Ding from Columbia University in the United States for their invaluable assistance and direction in carrying out the literature search. In addition, we would like to express our gratitude to Jing-Jie Wang from Xinjiang Medical University in China for his invaluable assistance and support in developing the graphics. Finally, we thank Hong-Yuan Jiang, Yan-Song Li, Dilzat Zulphcar, Hong-Yu Pu, Yuan-Long He, Zhi-Hao Zhou, Qi-Hao Chen, and Xin-Liang Peng, junior orthopedic surgeons from the First Affiliated Hospital of Xinjiang Medical University, for their suggestions on the sequential arrangement of the content of the article.
Author Contributions
Yixi Wang, Abulikemu Maimaiti, Paerhati Rexiti designed the study, Yixi Wang and Abudusalamu Tuoheti, Abulikemu Maimaiti, Yang Xiao and Alafate Kahaer performed the literature search, Yixi Wang, Dongshan Liu, Abulikemu Maimaiti, Rui Zhang wrote the manuscript, Yixi Wang, Alafate Kahaer, Abudusalamu Tuoheti, and Paerhati Rexiti proofread the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Central-class public welfare research institute project of Chinese Academy of Medical Sciences (Grant Number 2022-JKCS-19) and The Xinjiang Uygur Autonomous Region Science and Technology Major Project (Grant Number 2022A03011).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.