
Abstract
Study Design
Retrospective cohort study.
Objectives
To evaluate the incidence, risk factors, and complications associated with intraoperative venous injury during anterior lumbar interbody fusion (ALIF).
Methods
This retrospective review included patients who underwent one- to four-level ALIF at an academic spine center. Patients <18 years old or those with surgical indications for trauma, infection, or malignancy were excluded. Patients were stratified by the presence of venous laceration requiring primary suture repair. Comparative analyses were performed using Student’s t test and Pearson’s Chi-squared test. Univariable and multivariable logistic regression identified independent risk factors and postoperative complications.
Results
Among 554 patients, 92 (16.61%) sustained a venous laceration. Independent predictors included age (aOR: 1.03, P < 0.01), chronic kidney disease (aOR: 5.17, P < 0.01), ALIF at L4-5 (aOR: 3.88, P < 0.01), and two-level ALIF (aOR: 1.70, P < 0.01). ALIF at L5-S1 was protective (aOR: 0.24, P < 0.001). Venous laceration was associated with longer operative times (8.02 ± 2.95 vs 6.48 ± 2.81 hours, P < 0.001), greater mean blood loss (1,271 mL vs 600.71 mL, P < 0.001), and increased risks of deep vein thrombosis (DVT) (aOR: 3.33, [1.59-10.17], P = 0.011), intraoperative transfusion (aOR: 4.43, P < 0.001), and incision and drainage (aOR: 7.45, [1.75-31.62], P < 0.01).
Conclusion
Venous laceration occurred in 16.61% of ALIF cases, with independent risk factors including age, CKD, L4-5 ALIF, and two-level ALIF. These injuries were associated with prolonged operative times and a markedly elevated risk of DVT. Future research should focus on developing risk reduction strategies for high-risk patients and developing evidence-based VTE prophylaxis protocols tailored to patients with venous injuries.
Introduction
Anterior lumbar interbody fusion (ALIF) is a widely utilized surgical procedure for treating various lumbar spine pathologies including lumbar radiculopathy, discitis, osteomyelitis, malignancy, and spinal deformity. 1 Unlike posterior fusion techniques, ALIF requires retroperitoneal or transperitoneal dissection to access the anterior spinal column. 2 This approach avoids dissection of the paraspinal musculature, minimizes manipulation of neural elements, and enables indirect decompression of neural structures. However, it also introduces a distinct set of complications. Among them is the risk of venous injury as retraction of the iliac vessels is needed to safely access the disc space.
Prior studies, including case series, have reported a wide-ranging incidence of venous injury, from 0.3% to 24%.3-11 This variability is likely due to the small sample sizes in earlier studies, which may have limited their ability to provide accurate estimates. Furthermore, some studies aggregated arterial and venous injuries into a single vascular injury cohort, further obscuring the specific incidence of venous injury.9-11 Several patient and procedural risk factors have been implicated in increasing the risk of venous injury during ALIF. Patient factors include male sex, and a history of opioid use disorder; procedural risk factors include surgical indications for malignancy, re-do anterior exposure, revision spine surgery, greater vertebral exposure, multi-level ALIF, male gender, a history of degenerative spine disease, and opioid use.3,7,8,10 Venous injury has also been associated with greater intraoperative blood loss and longer hospital stays.3,5,6 Furthermore, given that venous trauma can activate the coagulation cascade, it is biologically plausible that this complication may predispose patients to postoperative venous thromboembolism (VTE). However, whether such an association exists remains uncertain, and current evidence is limited and inconsistent.3,12
Given the rising trend of spine surgeons performing their own anterior exposures, a clearer understanding of the true incidence, risk factors, and short-term postoperative complications associated with venous injury is essential. 13 Such insights can help guide patient selection for spine surgeon-performed exposures, inform targeted risk mitigation strategies, and optimize VTE prophylaxis protocols.
This retrospective cohort study, conducted at a large, high-volume academic spine center, aims to address these gaps by comprehensively evaluating the incidence of venous injury during ALIF, identifying independent risk factors, and assessing the association between venous injury and postoperative complications, including VTE.
Methods
Patient Selection
This study was approved by the institutional review board (IRB HS-23-00758). This was a retrospective review of patients who underwent one- to four-level primary or revision ALIF, with or without posterior fusion, at an academic spine surgery center staffed by neurosurgeons and orthopaedic surgeons, between 2014 and 2023. Patients <18 years old or those with surgical indications for trauma, infection, or malignancy were excluded.
Patients were stratified into two cohorts based on the presence or absence of an intraoperative venous injury. Venous injury was defined as any laceration to a major vein (iliac veins, inferior vena cava, or iliolumbar vein) requiring primary suture repair, as documented in operative reports by the approach surgeon. Minor vein injuries managed with simple compression or hemostatic agents, without the need for suture repair, were not included in the vein injury cohort. The specific vein injured in each case was documented.
Collected data included patient demographics, comorbidities, surgical variables (number of anterior/posterior levels fused, ALIF spinal level, estimated blood loss (EBL), and duration of surgery), and postoperative complications documented up to one-year.
Risk Factors and Complications
Risk factors evaluated included age, gender, tobacco use, American Society of Anesthesiologists (ASA) score, body mass index (BMI), history of abdominal surgery, hypertension, diabetes, coronary artery disease (CAD), osteoporosis, chronic kidney disease (CDK), spinal segment, number of anterior levels fused, and revision ALIF.
Postoperative complications recorded for both cohorts included deep vein thrombosis (DVT), pulmonary embolism (PE), retroperitoneal hematoma, superficial hematoma, ileus, acute kidney injury (AKI), surgical site infection (SSI), intraoperative transfusion, the need for incision and drainage (I&D), superior hypogastric plexus injury, and one-year mortality.
Statistical Analysis
Data were analyzed using International Business Machine (IBM) Statistical Package for the Social Sciences (SPSS) version 30. Descriptive statistics were calculated, and differences in patient demographics, comorbidities, surgical variables, and postoperative complications between cohorts were assessed using Pearson’s chi-squared test of independence and Independent Sample’s t test. Multivariable logistic regression analysis was performed to identify independent risk factors for venous injury, adjusting for covariates such as the number of anterior and posterior levels fused, age, ASA score, BMI, tobacco use, and gender. A separate regression model, incorporating intraoperative transfusion as an additional covariate, was used to assess the impact of venous injury on postoperative complication risk. Covariates included in the multivariable logistic regression models were selected based on their previously established associations with medical and surgical complications following ALIF.7,14,15 For models evaluating postoperative complications, intraoperative blood transfusion was also included as a covariate, given prior evidence linking transfusion to an increased risk of venous thromboembolism. 16
To assess multicollinearity among covariates, particularly between age and CKD, we performed a linear regression analysis using all independent variables from our logistic regression model. Tolerance and Variance Inflation Factor (VIF) values were reviewed, and no variable exceeded a VIF of 2.0, indicating that multicollinearity was not a concern.
Results
Patient Cohort
A total of 554 consecutive patients were included. Of these, 92 (16.61%) sustained a venous injury requiring primary suture repair. Most surgical approaches (543 patients, 98.01%) were performed by a vascular surgeon, while only 11 (1.99%) were performed by an orthopaedic spine surgeon. The majority of incisions were paramedian or midline. All cases were performed using a retroperitoneal approach, with none utilizing a transperitoneal approach.
Frequency of Vein Injury by Vein.
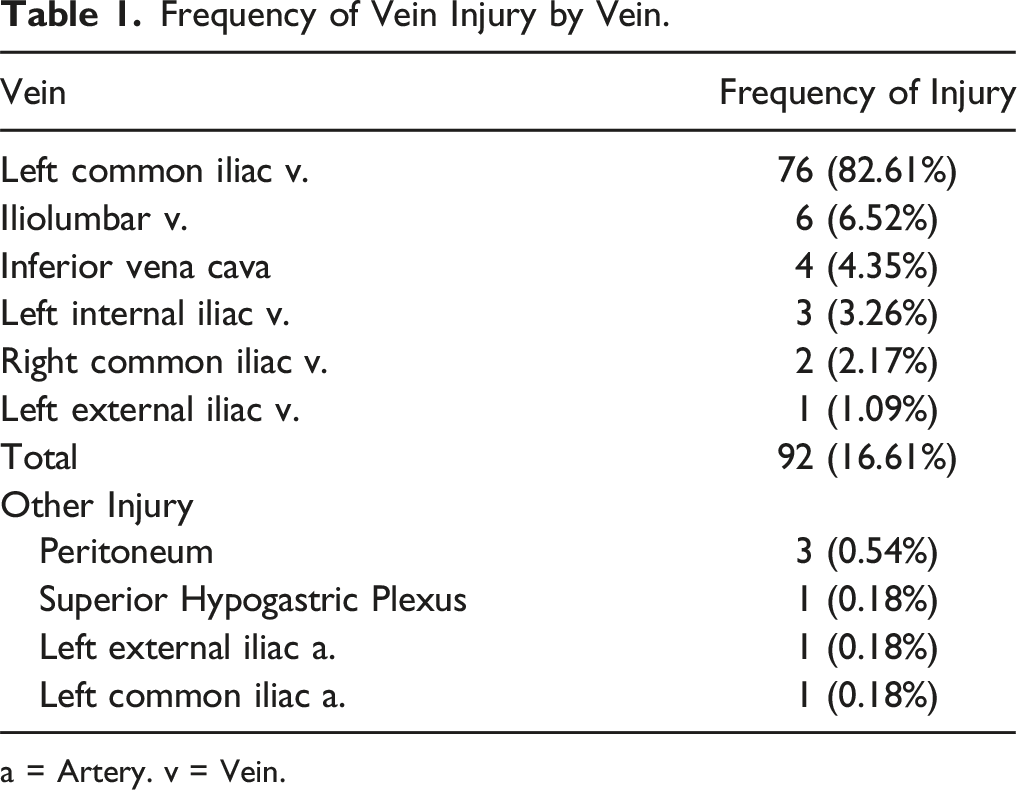
a = Artery. v = Vein.
Patient Characteristics
Differences Between Demographics, Comorbidities, and Surgical Variables.
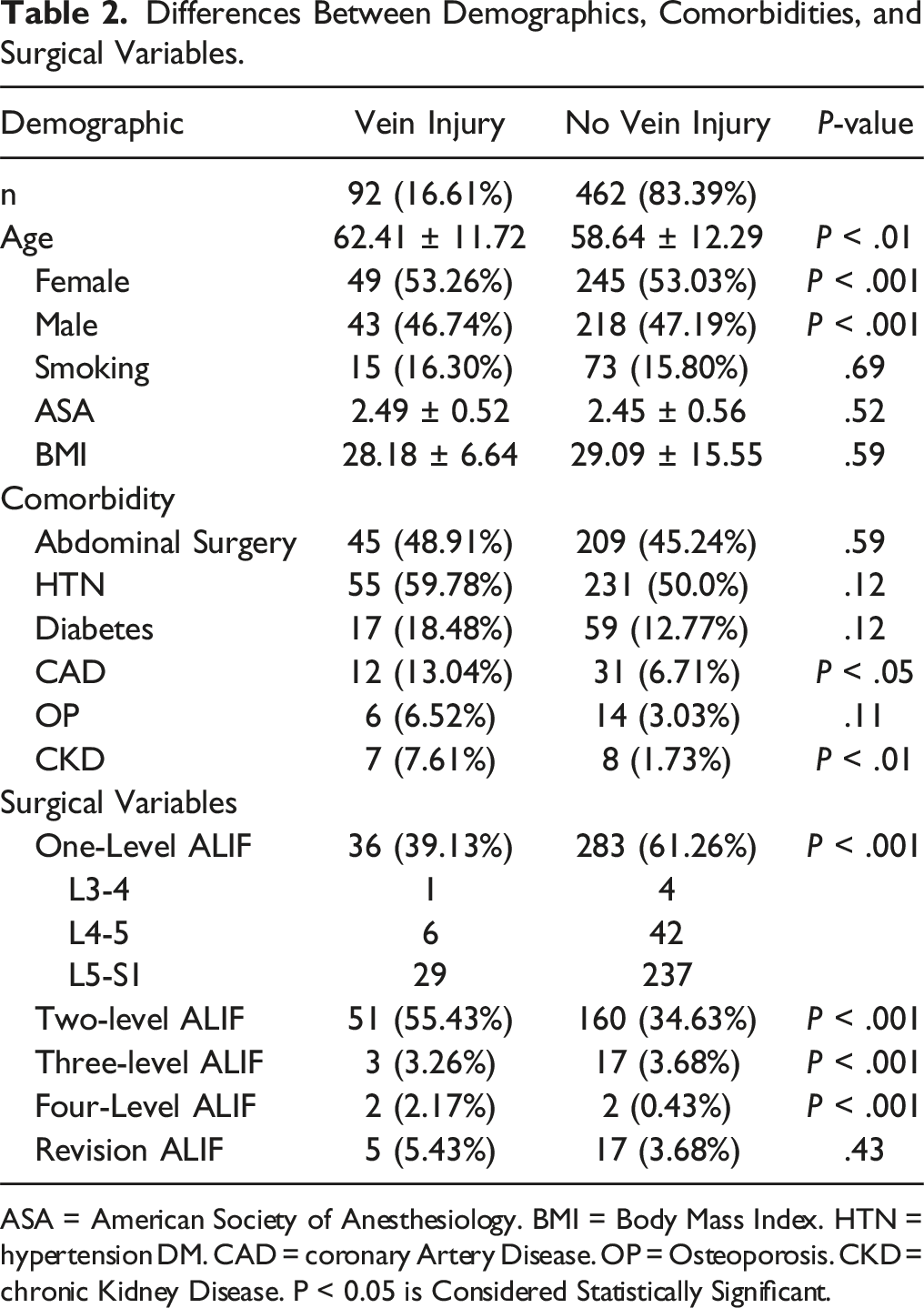
ASA = American Society of Anesthesiology. BMI = Body Mass Index. HTN = hypertension DM. CAD = coronary Artery Disease. OP = Osteoporosis. CKD = chronic Kidney Disease. P < 0.05 is Considered Statistically Significant.
However, the vein injury cohort had higher rates of CAD (13.04% vs 6.71%, P < 0.05) and CKD (7.61% vs 1.73%, P < 0.01).
Regarding surgical variables, the vein injury cohort had a lower proportion of one-level ALIFs compared to the no-injury cohort (39.13% vs 61.26%) but a higher proportion of two-level (55.43% vs 34.63%), four-level (2.17% vs 0.43%), and revision ALIF procedures (5.43% vs 3.68%) (all P < 0.001) (Table 2). Three-level ALIFs were comparable between groups (3.26% vs 3.68%, P < 0.001).
Predictors of Vein Injury
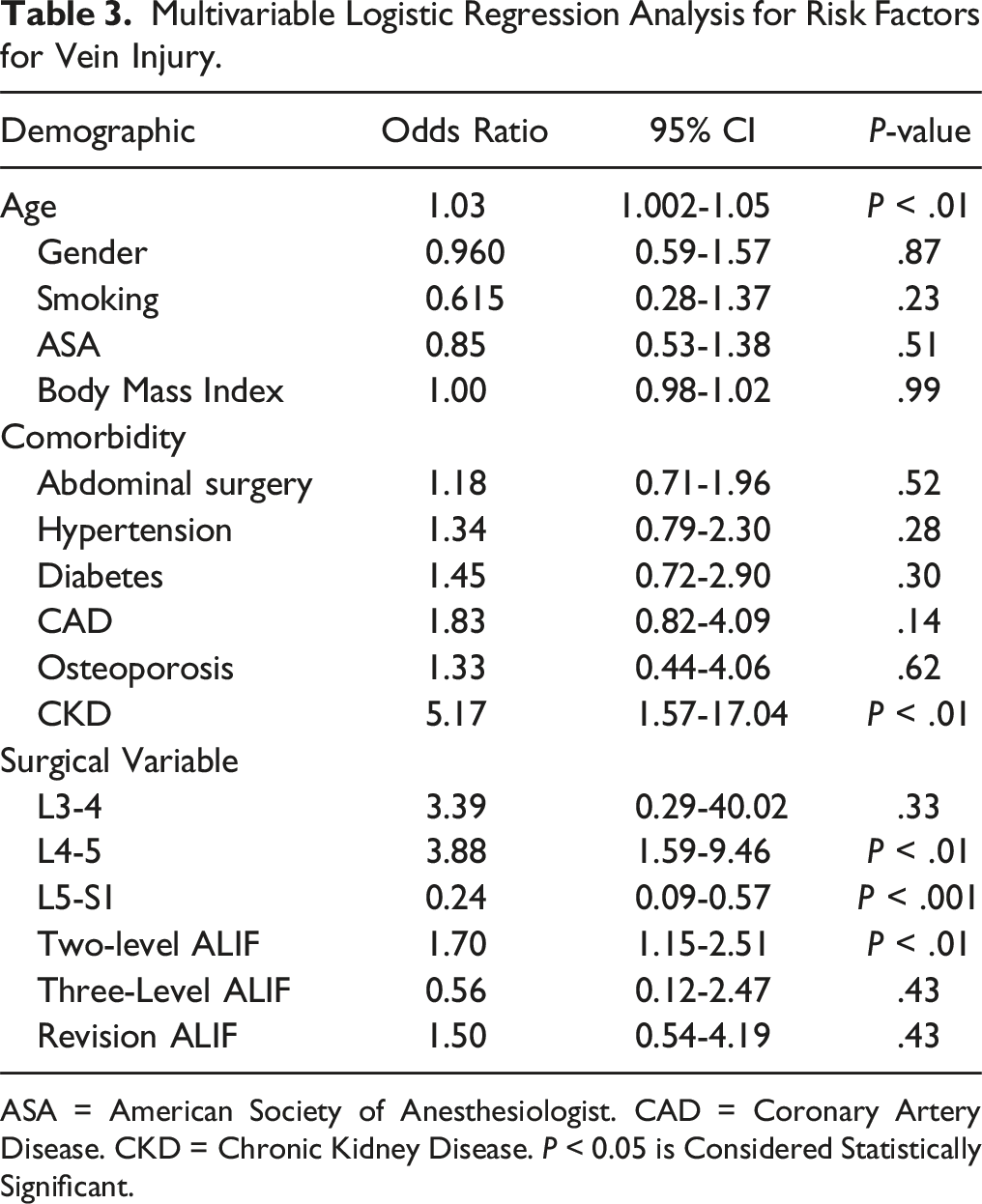
Multivariable logistic regression identified age (adjusted OR: 1.03, [1.002-1.05], P < 0.01), CKD (aOR: 5.17, [1.57-17.04], P < 0.01), ALIF at L4-5 (aOR: 3.88, [1.59-9.46], P < 0.01), and two-level ALIF (aOR: 1.70, [1.15-2.51], P < 0.01) as independent predictors of venous injury (Figure 1, Table 3). ALIF at L5-S1 was associated with a lower likelihood of venous injury (aOR: 0.24, [0.09-0.57], P < 0.001). Forest plot of predictors of venous injury. Multivariable Logistic Regression Analysis for Risk Factors for Vein Injury. ASA = American Society of Anesthesiologist. CAD = Coronary Artery Disease. CKD = Chronic Kidney Disease. P < 0.05 is Considered Statistically Significant.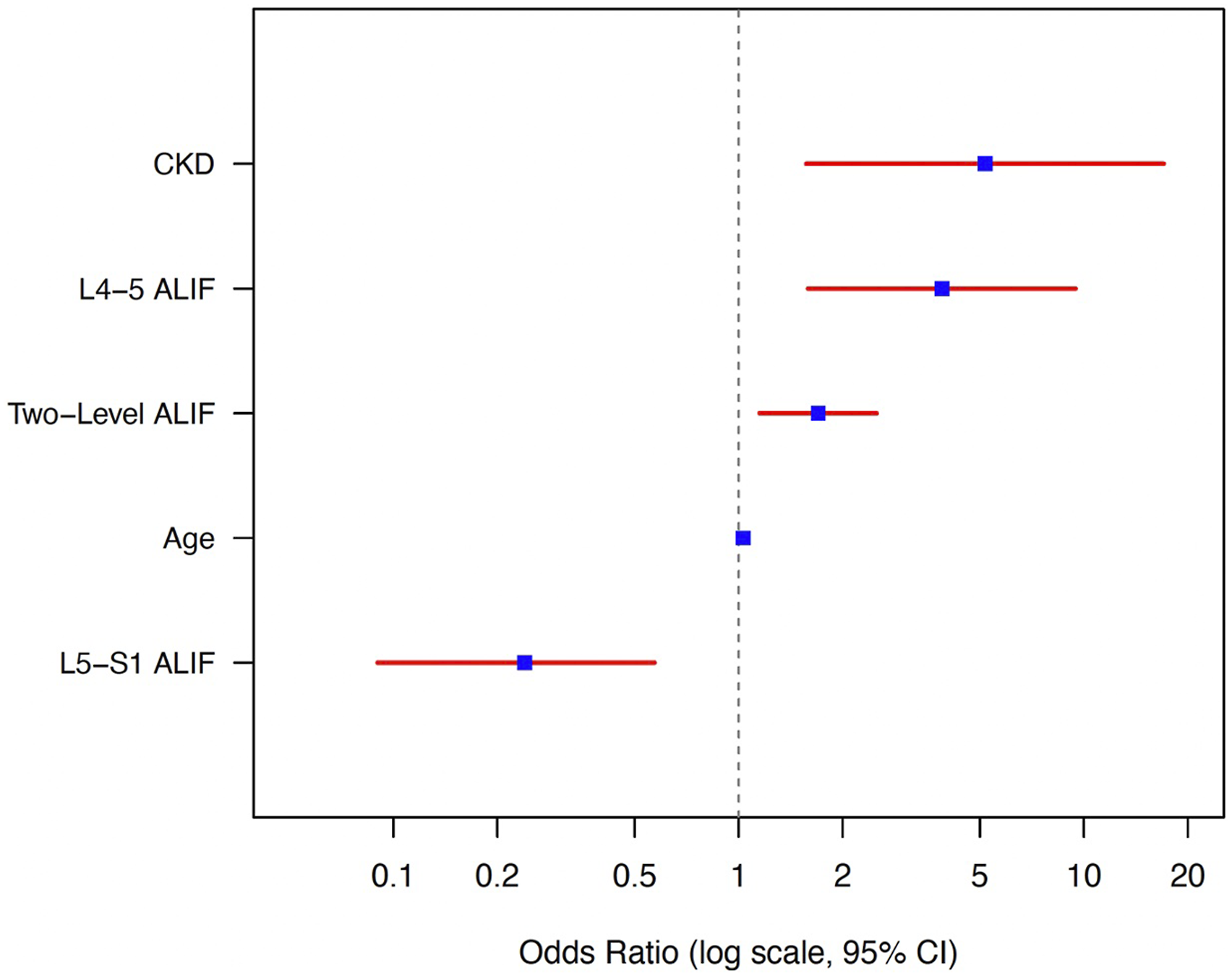
Complications of Vein Injury
Operative time was significantly longer in the vein injury cohort (8.02 ± 2.95 vs 6.48 ± 2.81 hours, P < 0.001). Mean EBL was also higher (1271 ± 1607.60 mL vs 600.71 ± 1150.06 mL, P < 0.001). EBL ranged from 80 to 10,000 mL in the venous injury cohort, with 29.35% of cases exceeding 1500 mL.
Univariable and Multivariable Logistic Regression Analysis for Postoperative Complications Associated With Vein Injury.
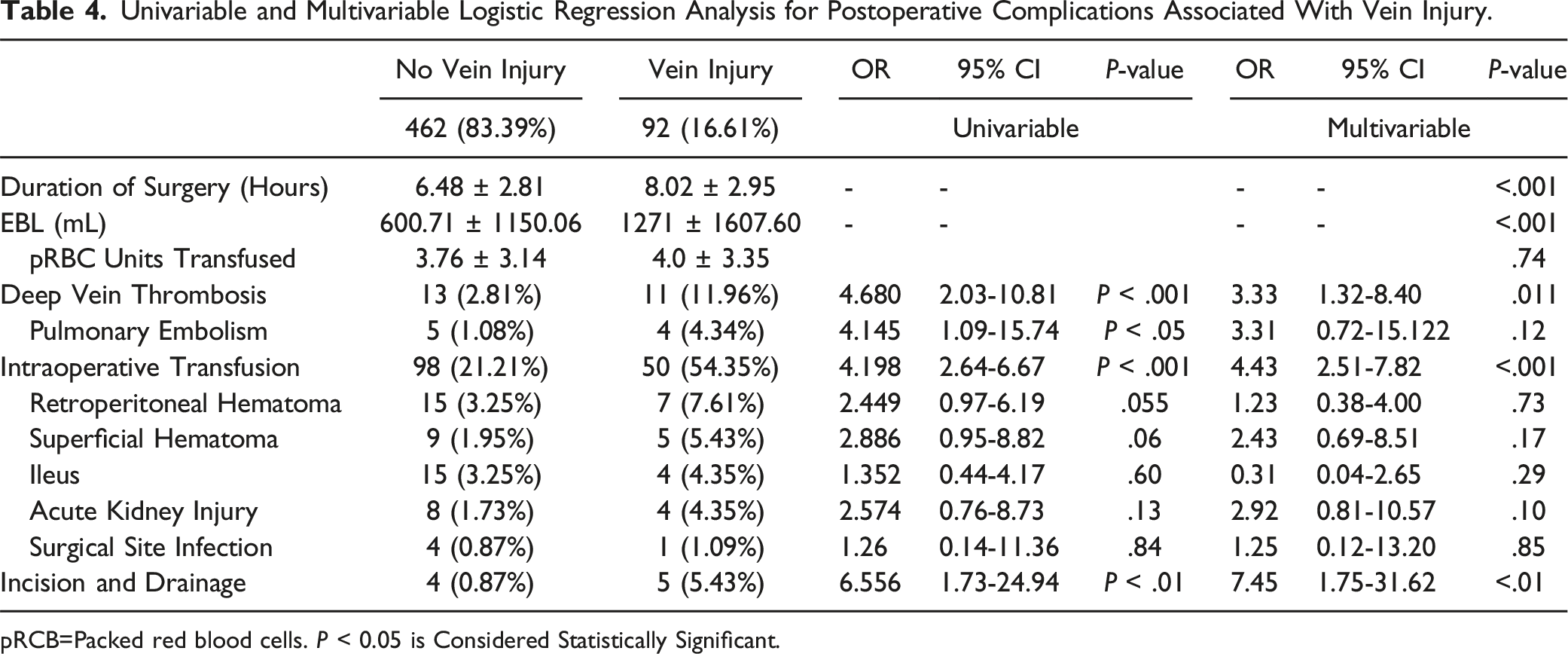
pRCB=Packed red blood cells. P < 0.05 is Considered Statistically Significant.
There were no mortalities in the venous injury cohort. In the no-injury group, one mortality occurred one month postoperatively due to diffuse cerebral edema from septic shock and metabolic derangements, deemed unrelated to surgery. One patient required abortion of the ALIF procedure due to a severe injury at the IVC bifurcation. Among patients who received intraoperative transfusions, the number of units transfused was similar between groups (4.0 ± 3.35 vs 3.76 ± 3.14, P = 0.74).
Univariable logistic regression analysis revealed associated between venous injury and elevated risk for DVT (OR: 4.68, [2.03-10.81], P < 0.001), PE (OR: 4.15, [1.09-15.74], P < 0.05), intraoperative transfusion (OR: 4.20, [2.64-6.67], P < 0.001), and I&D (OR: 6.56, [1.73-24.94], P < 0.01) (Table 4).
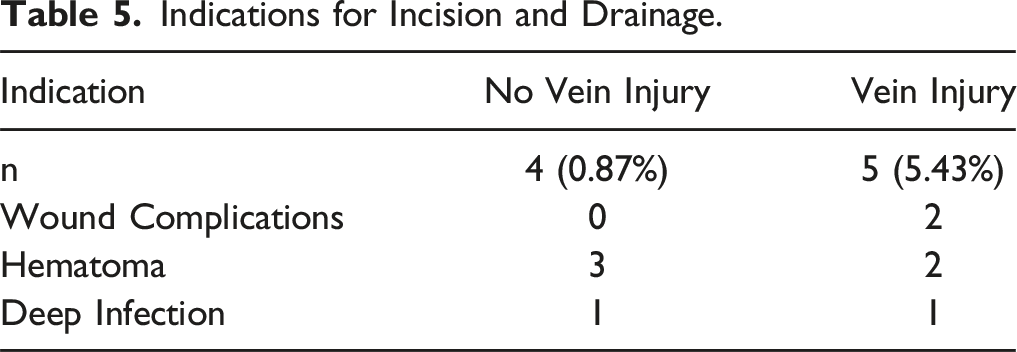
Multivariable logistic regression confirmed venous injury as an independent predictor of DVT (aOR: 3.33, [1.32-8.40], P = 0.011), intraoperative transfusion (aOR: 4.43, [2.51-7.82], P < 0.001), and I&D (aOR:7.45, [1.75-31.62], P < 0.01) (Figure 2, Table 4). Intraoperative transfusion was also independently associated with an increased risk of DVT (aOR: 3.93 [1.35-11.53], P = 0.012). Primary indications for I&D included wound complications (two vs zero cases), hematoma (two vs three cases), and deep infection (one case in each cohort) (Table 5). Forest plot of complications associated with venous injury. Indications for Incision and Drainage.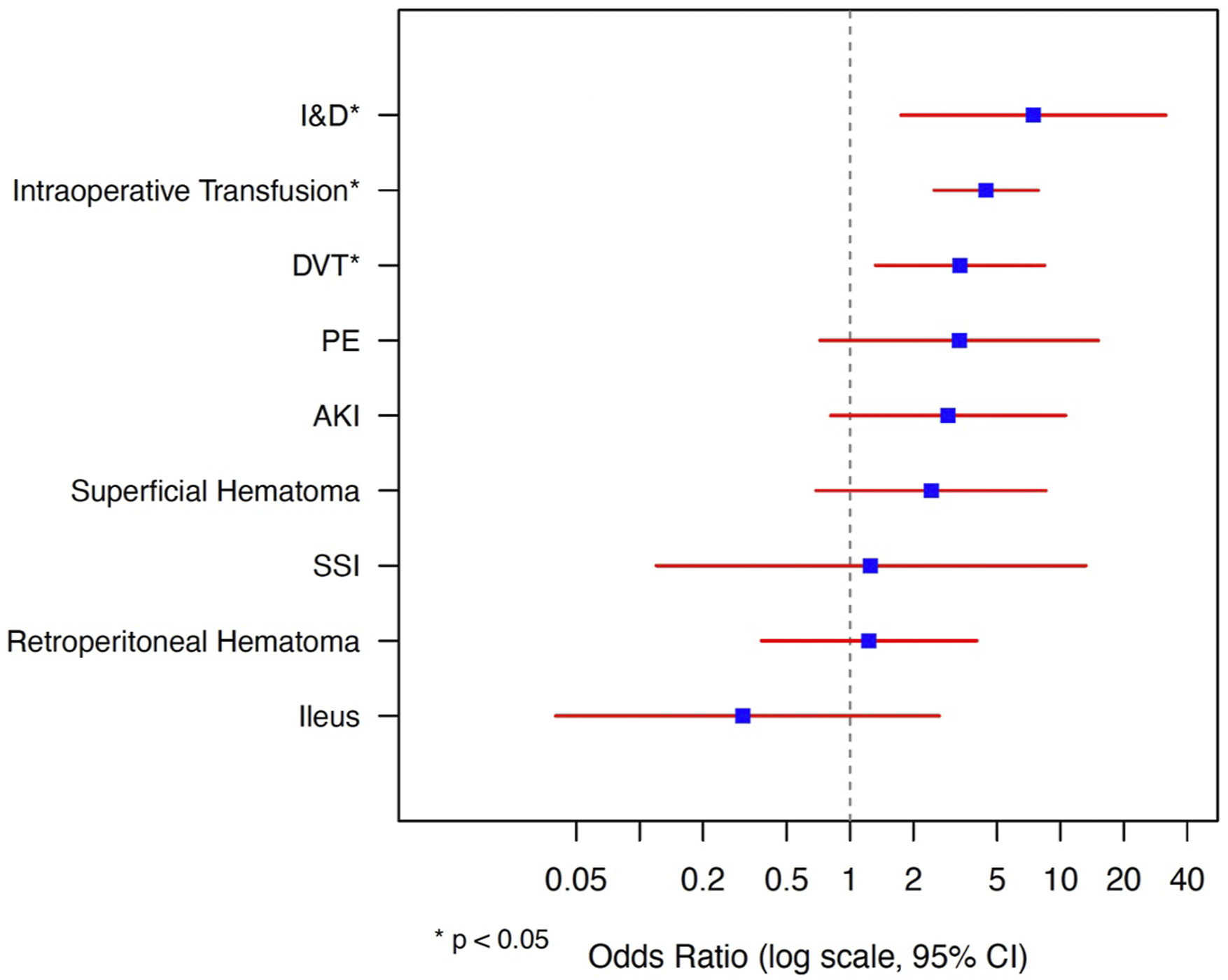
Discussion
This study highlights the incidence, risk factors, and complications associated with intraoperative venous injury during ALIF. In an analysis of 554 consecutive ALIF cases at our high-volume academic center, the most comprehensive study to date, venous injury occurred in 16.61% of cases, most commonly involving the left common iliac vein. Independent predictors of venous injury included age, CKD, ALIF at L4-5, and two-level ALIF. Importantly, venous injury was associated with longer operative times, increased blood loss, and nearly a fourfold higher risk of intraoperative transfusions and DVT. Furthermore, our finding that intraoperative transfusion independently increased the risk of DVT suggests that more severe vein injuries may confer an even greater thrombotic risk. These findings underscore that venous injury during ALIF is not uncommon and emphasize the need for standardized perioperative management strategies to mitigate the risk of thromboembolic complications in this vulnerable patient population.
The reported incidence of vascular injury during ALIF varies widely, ranging from 0.3% to 24%. 3 Our observed rate of 16.61% falls within this range but is notably higher than most studies, such as those by Brau et al (1.4%), Ho et al (6.5%), and Fantini et al (2.9%).6,8,11 This disparity may stem from several factors. First, our study is among the largest to date, which may have enabled a more accurate characterization of venous injuries, whereas smaller sample sizes in previous studies may have underestimated the true incidence. Second, this study was conducted at a major academic spine center, which managed a more complex patient population. For instance, nearly half of our cohort (45.77%) had a history of abdominal surgery, and 3.97% had undergone prior ALIF. Both factors are known to increase adhesion formation and complicate dissection in the retroperitoneal plane. 3 Revision cases, especially those requiring the removal of interbody devices carry an inherently higher risk of vascular injury. 17 Additionally, our results may have been influenced by the referral pattern at our center, which tends to treat patients with more advanced degenerative spine pathology. For instance, Fantini et al. identified spondylolisthesis, large anterior osteophyte complexes, and anterior migration of interbody devices as significant risk factors for venous injury.
Independent risk factors for venous injury included age, CKD, ALIF at L4-5, and two-level ALIF, while ALIF at L5-S1 was associated with a significantly lower risk. The association with age is consistent with prior studies demonstrating age-related venous changes, such as reduced elastin and collagen content, weakened endothelial cells, and increased fragility, making veins more prone to tearing during retraction. 18 While Tigre et al identified age as a predictor in univariate analysis, our study is the first to confirm this association in a large multivariable analysis. 7 CKD emerged as another significant predictor, likely due to venous morphological changes such as intimal hyperplasia and calcifications, which compromise vascular integrity rendering them more prone to injury during surgical manipulation. 19 Additionally CKD patients–particularly those on peritoneal dialysis–are prone to peritoneal fibrosis, retroperitoneal lipomatosis, and intrabdominal adhesions, which may complicate retroperitoneal dissection. 20 These retroperitoneal changes may also tether vessels to surrounding soft tissues, complicating dissection planes. This is the first study to establish an association between CKD and venous injury during ALIF. Our findings corroborate prior research indicating that ALIF at L4-5 significantly increases the risk of venous injury.3,10 This is attributed to the anatomical course of the left common iliac vein, the most frequently injured vessel in our study (82.61%). This vein lies anterior to the L5 vertebra and often traverses the L4-5 disc space, necessitating significant retraction during endplate preparation. Conversely ALIF at L5-S1 was associated with a decreased risk of venous injury, likely due to its anatomical location below the aortic bifurcation and iliocaval confluence, often requiring less aggressive retraction to adequately access the disc space. 13 Lastly, two-level ALIF was associated with increased risk, likely due to the greater degree of vein retraction required for multi-level procedures and possible need for mobilization and control of the iliolumbar vein. Similar findings have been reported by Tigre et al and Ho et al, both of whom demonstrated an elevated risk of venous injury in multi-level ALIF procedures.7,8 With the increasing number of spine surgeons independently performing anterior exposures, these findings offer practical guidance for surgical planning. 13 Specifically, collaboration with a vascular surgeons should be strongly considered in high-risk cases––such as multi-level ALIF, procedures involving the L4-5 disc space, and patients with advanced age or CKD. Conversely, younger patients undergoing one-level L5-S1 ALIF, which is anatomically less complex and associated with a lower risk of venous injury, may be appropriate candidates for spine surgeon performed exposure. Additionally, prior research has shown that the transperitoneal approach may be associated with a higher risk of venous injury compared to the retroperitoneal approach, likely due to the need for more extensive mobilization of abdominal contents. 21 As such, a retroperitoneal approach should be favored in high-risk patients to minimize vascular complications.
Patients with venous injury experienced significantly higher rates of retroperitoneal hematoma. Although not significant in the multivariable analysis, the markedly higher incidence (7.61% vs 3.25%) compared to the control group warrants attention. Retroperitoneal hematomas pose substantial risk, and, in some cases, can lead to subsequent complications. Herein, several patients in the vein injury cohort with retroperitoneal hematomas developed hydronephrosis due to ureter compression or required incision and drainage; one patient developed a life-threatening cardiac arrhythmia. These events likely contribute to increased hospital length of stay and overall healthcare costs. As such, surgeons should have a low threshold to obtain cross sectional imaging in venous injury patients with symptoms concerning for retroperitoneal hematoma.
The nearly four-fold increase in DVT risk observed in this cohort is not unexpected. This finding remained significant even after adjusting for known thrombosis risk factors, including obesity, age, smoking, transfusion, and multi-level procedures. The pathophysiology underlying this increased risk aligns with Virchow’s triad. Prolonged operative times in the vein injury cohort result in extended periods of venous retraction, leading to venous stasis. Additionally, direct trauma to the vein causes endothelial cell damage, triggering the coagulation cascade and creating a nidus for thrombus formation. Zahradnik et al. also examined thrombosis risk following venous injury during ALIF but did not find a significant association, likely due to their smaller sample size. 3 Interestingly, in alignment with prior research, this study identified intraoperative transfusion as an independent risk factor for DVT. 16 The mechanism underlying this association is likely multifactorial and may occur through transfusion-induced inflammatory responses that promote a hypercoagulable state.22-24 Furthermore, transfusion necessity may serve as a marker for more severe vascular injury, with greater endothelial disruption and subsequent activation of the coagulation cascade. Given the association between venous injury and DVT, it suggests that patients with venous injury requiring transfusion are at particularly high risk. These findings underscore that in high-risk patients, preoperative hemoglobin optimization and intraoperative strategies to reduce blood loss (ie, TXA and use of topical hemostatic agents) are imperative. 22 Importantly, all patients in the venous injury cohort who developed thrombosis had received standard perioperative VTE prophylaxis, with no modifications made to the postoperative protocol. This included initiation of subcutaneous heparin on postoperative day zero. These findings underscore the need for more aggressive VTE prophylaxis strategies in this high-risk population, despite the potential trade-off of an increased hematoma formation. Furthermore, they highlight a critical gap in evidence-based guidelines for optimal VTE prophylaxis in this patient population. For example, as recommended by The American Society of Hematology and supported by prior studies, combining intermittent pneumatic compression devices and graduated compression stockings with early postoperative mobilization may reduce DVT risk without significantly increasing bleeding complications.25-27 Additionally, minimizing intraoperative transfusion––an independent risk factor for DVT––can further mitigate thrombotic risk. This can be achieved through preoperative hemoglobin optimization and the use of intraoperative blood conservation strategies, such as tranexamic acid and topical hemostatic agents. Risk stratification tools should also be employed to better characterize individual thrombotic risk in this high-risk population. The Caprini score, for instance, has been shown to accurately predict VTE risk in patients undergoing orthopaedic surgery. 28 Until specific chemoprophylaxis protocols are developed for this high-risk population, these conservative measures offer a practical approach to balancing the risk of thrombosis against the potential for postoperative bleeding. Future studies are needed to develop tailored protocols to balance the risks of thrombosis and bleeding, thereby optimizing care for these patients.
Limitations
This study has several limitations. First, both the vascular and spine teams comprised several surgeons, resulting in variability in surgical skill and experience, which we were unable to control for. This variability may have influenced the incidence of venous injury. Second, the retrospective nature of this study limits our ability to recommend specific thromboprophylaxis regimens or standardize perioperative management strategies. The retrospective nature also introduces the potential for selection bias and unmeasured confounders, which may have influenced both the identification of risk factors and the observed associated postoperative complications. These limitations are inherent to retrospective designs and may affect the generalizability and causal interpretation of our findings. Future prospective studies should aim to mitigate these biases through standardized data collection and uniform perioperative protocols, allowing for more accurate adjustment for confounders and a clearer understanding of the relationship between risk factors and complications associated with venous injury. Additionally, as a single-center study conducted at a major academic institution, the findings may not be generalizable to other settings, such as community hospitals or smaller practices. The follow-up period of one year represents another limitation, as it may be insufficient to capture long-term complications such as recurrent thromboembolic events, chronic venous insufficiency, or late sequelae of retroperitoneal hematoma. Future studies should incorporate extended follow-up periods of at least 2-5 years to better characterize the long-term impact of intraoperative venous injury. Furthermore, only 11 approaches were performed by a spine surgeon, making it difficult to draw conclusions about the safety and efficacy of spine surgeon-performed approaches.
Despite these limitations, this study has notable strengths. Its large sample size allowed for a more precise estimate of the incidence of venous injury and enabled the identification of risk factors and postoperative complications. These findings provide valuable insights into the inherent risk factors and complication rates associated with venous injury during ALIF, highlighting areas for future research and potential improvements in surgical practice.
Conclusion
Venous injury during ALIF occurred in 16.61% of cases at a high-volume academic center, with independent risk factors including advanced age, CKD, L4-5 ALIF, and multi-level ALIF. These injuries were associated with significantly prolonged operative times, markedly increased blood loss, and a higher risk of intraoperative transfusions and DVT. Notably, intraoperative transfusion itself emerged as an independent predictor of DVT, underscoring the heightened thrombotic risk in patients with more severe venous injuries. Future research should focus on developing strategies to minimize the risk of venous injury, particularly in high-risk patient populations, and on establishing evidence-based VTE prophylaxis protocol tailored to patients with venous injuries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Henry Avetisian, Camille Flynn, Rakhi Banerjee, Vivek Satish, Joshua Davood, William Karakash, Matthew C. Gallo, Mirbahador Athari, anf Gregory Magee have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccential Robotics for lectures and presentations
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data is not publicly available but can be available upon request.