
Abstract
Study Design
Matched Retrospective Cohort Study.
Objective
To compare efficacy and safety of Halo gravity traction vs Halo pelvic traction in severe rigid spinal deformity.
Methods
We retrospectively reviewed 104 severe rigid spinal deformity patients treated with preoperative Halo traction and posterior correction surgery (2016.1-2022.12). Patients were matched 1:1 by main curve Cobb angle and age into HGT and HPT groups (33 each). Radiographic parameters were assessed before and after traction, preoperatively, and at final follow-up. Surgical planning for osteotomy and fusion segments used pre-traction imaging, compared with actual outcomes. Traction duration, surgical parameters, and complications were recorded.
Results
HGT patients had 4.5 ± 1.5 months traction, improving main curve from 138.4° to 94.9° (23.5%) and kyphosis from 87.9° to 73.1° (22.6%), with postoperative values of 51.1° and 39.7°. HPT patients had 5.1 ± 1.1 months of traction, improving main curve from 143.2° to 69.6° (51.3%) and kyphosis from 117.7° to 56.8° (49.1%), with postoperative values of 56.1° and 34.5°. HPT showed better improvement (P < 0.05). HPT achieved 50% deformity improvement after 3 months, vs 5 months for HGT. By 7 months, >60% of HPT vs <10% of HGT patients reached this threshold. Planned three-column osteotomy dropped from 90.9% to 51.5% (actual 36.4%) in HGT and 84.8% to 21.2% (actual 9.1%) in HPT. HPT reduced osteotomy grade (P < 0.05) and fusion segments (P = 0.02) more effectively. Complication rates were similar.
Conclusions
Both HGT and HPT improve preoperative deformity, but HPT is more effective and better in reducing osteotomy grades and fusion segments.
Introduction
Severe rigid spinal deformity (SRSD) is characterized by a Cobb angle exceeding 100° and a curvature flexibility of less than 30%, which may be associated with or without thoracic kyphosis.1-3 Patients with severe rigid spinal deformity often present with thoracic deformity, which can impede the growth and development of the respiratory system and restrict the movement of the thoracic cage and ribs. 4 This results in restrictive ventilatory dysfunction and a reduction in lung capacity, leading to associated cardiopulmonary impairments that significantly affect the patients' quality of life and functional abilities.5,6 If the deformity continues to progress, it may pose a life-threatening risk.
Advancements in surgical techniques, including three-column osteotomy like vertebral column resection (VCR), have improved SRSD management, enabling substantial deformity correction and spinal cord decompression.7,8 However, these procedures carry risks, such as significant blood loss, spinal cord injury, or paralysis.8,9 To minimize reliance on high-level osteotomy, preoperative halo traction has emerged as an adjunctive therapy.
Halo gravity traction (HGT) facilitates gradual deformity correction without prolonged bed rest, enhancing pulmonary function, nutritional status, and surgical tolerance.10,11 Studies suggest HGT may reduce the need for extensive osteotomy.12-14 Halo pelvic traction (HPT), offering stronger traction forces, may achieve superior deformity correction and similar physiological benefits. 15 According to existing literatures,10,16 both Halo traction methods yield satisfactory outcomes as adjunctive treatments for severe rigid spinal deformity. However, comparative studies assessing their efficacy and safety—particularly in reducing osteotomy levels, improving pulmonary function, and optimizing nutritional status—are lacking. Understanding these differences is critical for informed preoperative planning and optimizing patient outcomes.
Our center conducted a matched retrospective study to compare the safety and efficacy of HGT and HPT in preoperative SRSD management. This analysis aims to clarify each method’s role in enhancing deformity correction, minimizing surgical risks, and improving patient health, guiding evidence-based treatment decisions.
Methods
Patients Selection
A retrospective study was conducted to include patients with severe rigid spinal deformity who underwent preoperative Halo traction combined with staged posterior spinal deformity correction surgery at our institution from January 2016 to December 2022. The inclusion criteria were as follows: 1) presence of scoliosis with or without associated kyphosis, with a Cobb angle>100°; 2) bending flexibility<30%; 3) undergoing Halo gravity traction or Halo-pelvic traction combined with posterior spinal deformity correction surgery during hospitalization; 4) at least 2 years of follow-up postoperatively. Exclusion criteria included: 1) history of prior spinal surgery; 2) previous thoracoplasty or spinal release surgery prior to traction; 3) traction duration <2 weeks; 4) presence of spinal developmental abnormalities such as syringomyelia or split cord malformation; 5) data missing. All included patients were divided into 2 groups: the Halo-gravity traction + Posterior Spinal Fusion Surgery group (N = 36) and the Halo-pelvic traction + Posterior Spinal Fusion Surgery group (N = 68). To ensure comparability, a 1:1 matching based on Cobb angle and age resulted in 33 patients in each group, Figure 1. Flow diagram showing the participants’ progression through the study.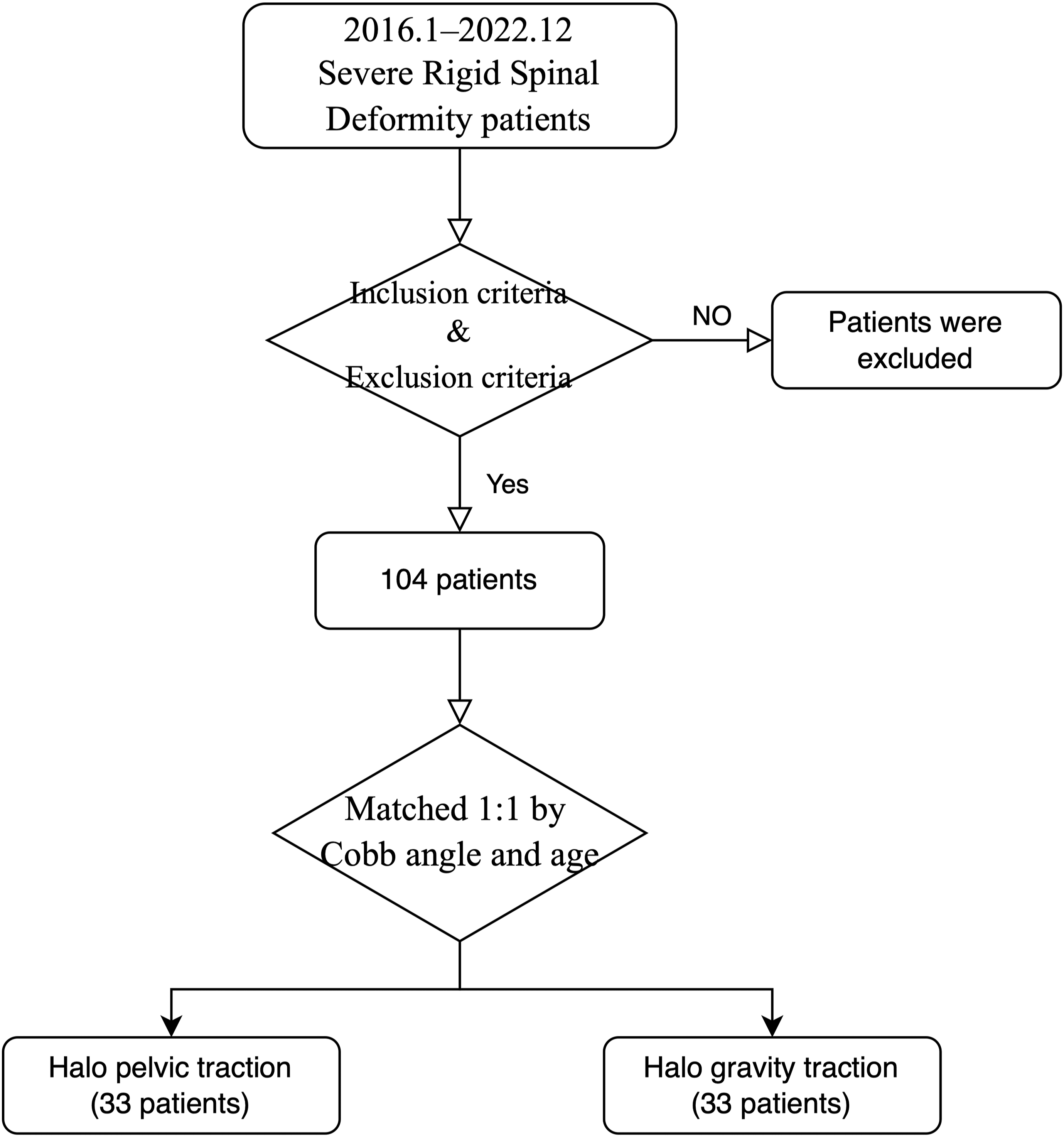
Demographic information of the patients was gathered, encompassing age, gender, body mass index (BMI), and etiology of deformity. The research was conducted in accordance with ethical guidelines outlined in the Declaration of Helsinki and received approval from the Ethics Committee of our Hospital. Informed consent was secured from all participants in the cohort, along with parental consent for patients under 18 years old.
Surgical Protocol
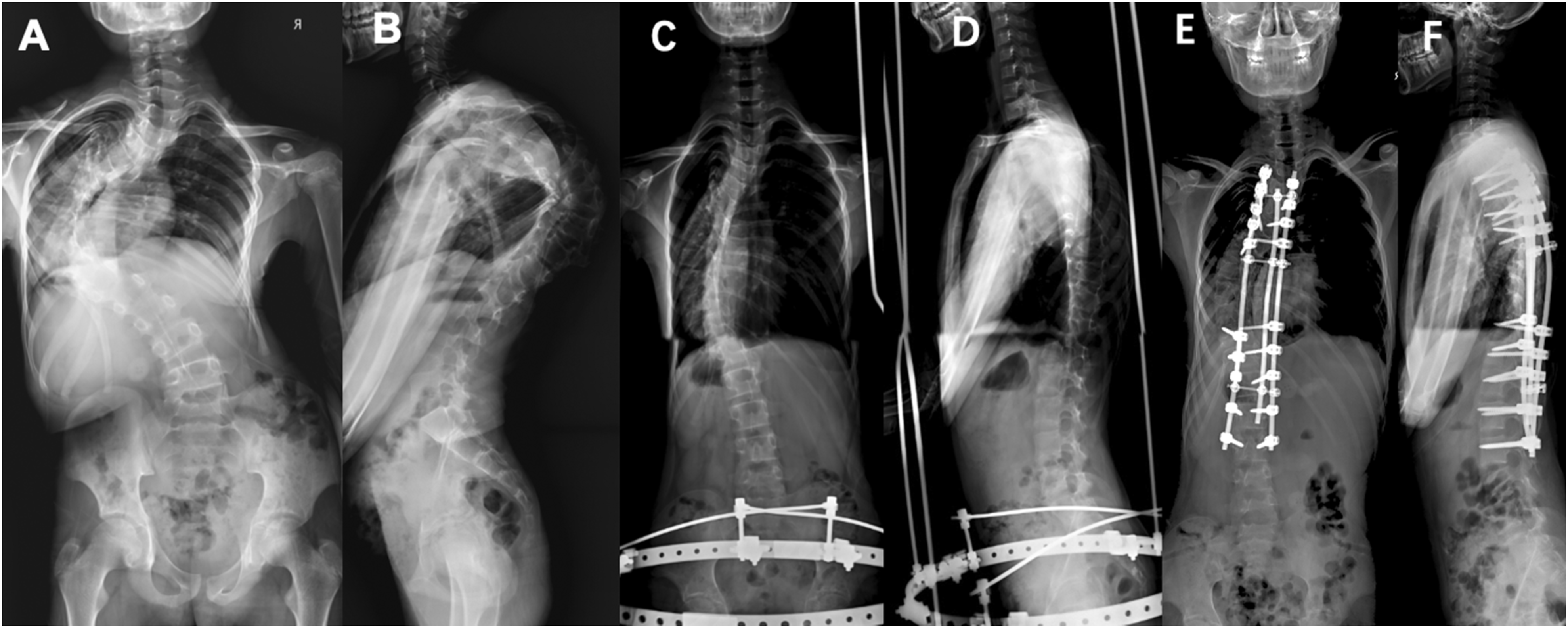
Halo gravity traction (HGT) starts 3 days post-halo ring placement, with patients sitting in a wheelchair for >12 hours daily. Initial traction weight is 20% of body weight, increased by 3-5 kg daily to 40%-50%, based on tolerance. Halo-pelvic traction (HPT) involves inserting two 4.0-mm pins bilaterally into the iliac spines under anesthesia, connecting halo and pelvic rings via four rods. Distraction begins post-pain relief, increasing 1-2 cm daily for 1 week, then 2-5 mm until tolerance limits. Both require daily pin-site disinfection and neurological monitoring. Biweekly X-rays assess deformity improvement. Surgery follows 50% scoliosis correction, recording osteotomy, fusion segments, blood loss, transfusion, and duration (Figures 2 and 3). (A) and (B) A 9-year-old male patient with severe rigid kyphoscoliosis. (C) and (D) Scoliosis and kyphosis were both corrected after 3 months of Halo-gravity traction. (E) and (F) Scoliosis and kyphosis were significantly corrected after surgery. (A and B) A 14-year-old male patient with severe rigid kyphoscoliosis. (C and D) Scoliosis and kyphosis were both significantly corrected after 3 months of Halo-pelvic traction. (E) and (F) Scoliosis and kyphosis were further corrected after surgery.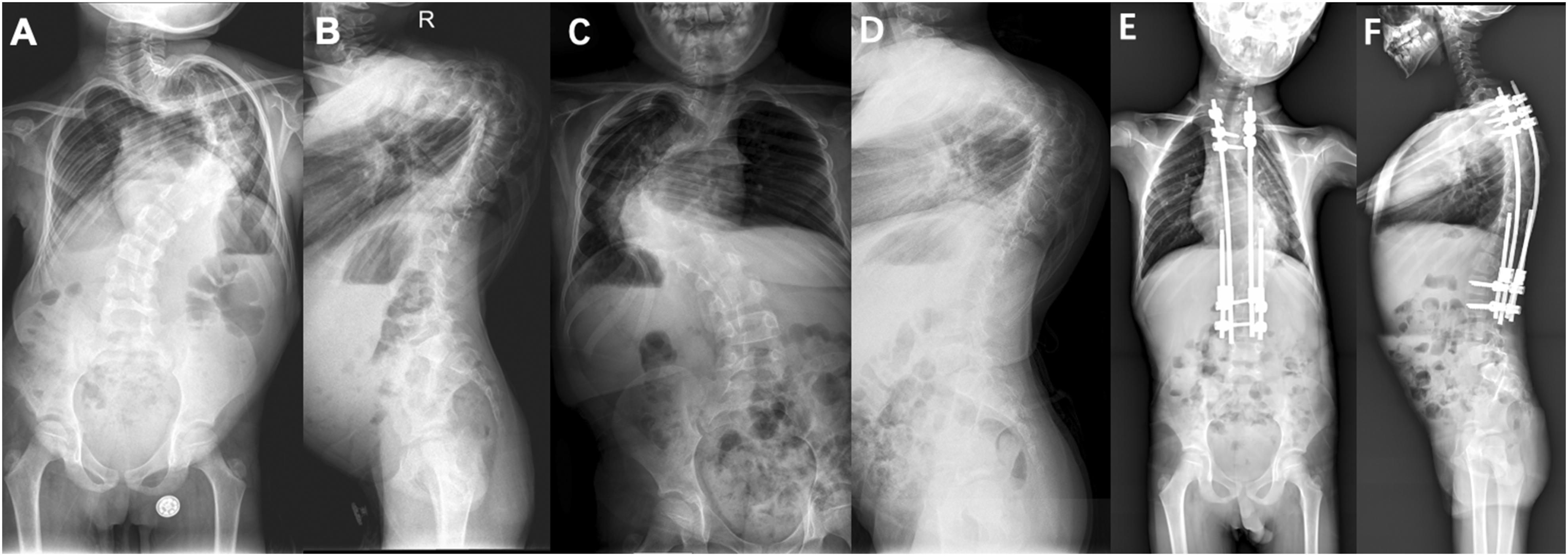
Data Acquisition
Two trained spine surgeons measured and averaged imaging data, assessing coronal parameters (main curve Cobb angle, C7PL-CSVL, T1-S1 length, AVT) and sagittal parameters (maximum kyphosis angle, SVA). Deformity correction rate was calculated as: ([pre-traction Cobb angle - post-traction Cobb angle]/pre-traction Cobb angle) × 100%. Two senior experts independently analyzed pre- and post-traction whole spine X-rays, planning osteotomy grade and fusion segments. Plans were re-evaluated after 1 month; discrepancies prompted a third surgeon’s review. Patients underwent follow-up at 3, 6, 12 months, and annually thereafter with whole spine X-rays, documenting complications to assess preoperative halo traction and posterior correction surgery safety and efficacy.
Statistical Analysis
Using SPSS (v22.0) and R, we analyzed continuous variables (means ± SD, normality assessed) with repeated measures ANOVA to compare imaging and pulmonary function across pre-traction, post-traction, post-surgery, and follow-up. Independent t-tests evaluated deformity correction rates between traction methods. Propensity score matching in R (v3.1.3) adjusted for age and Cobb angle. Categorical variables, reported as frequencies and percentages, were compared via Chi-square tests for high-grade osteotomy rates. Significance was set at P < 0.05.
Results
Demographics and Clinicopathological Data
Demographic and Baseline Characteristics of Patients.
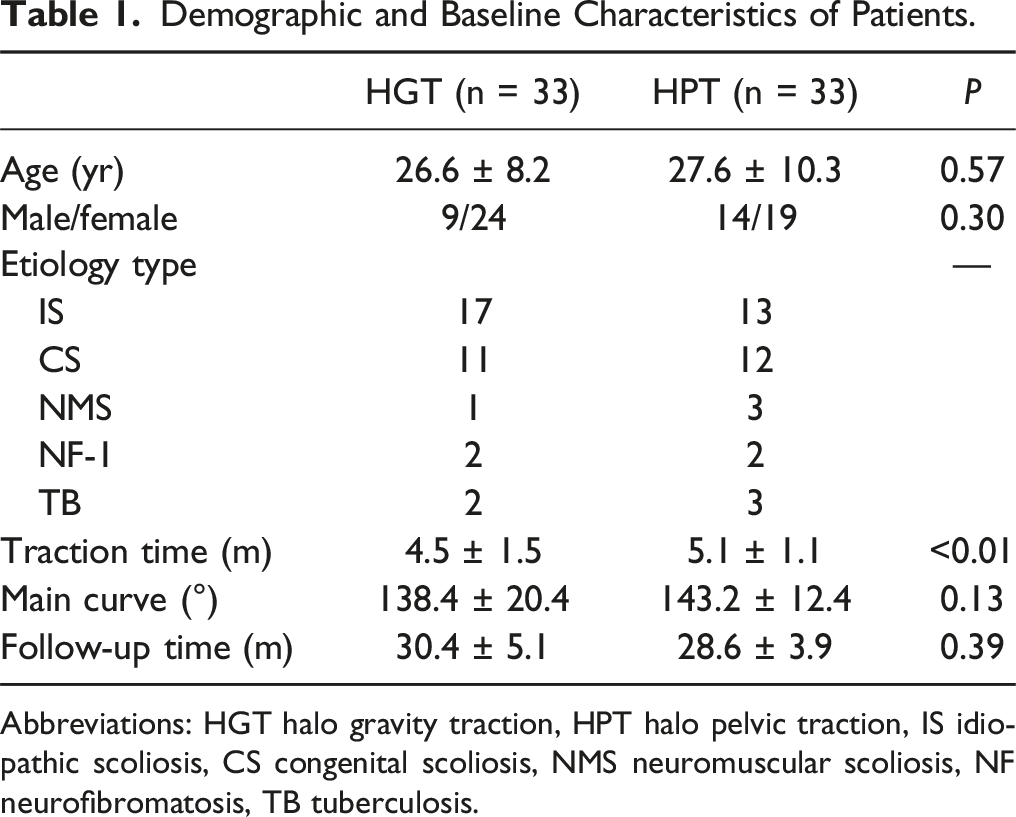
Abbreviations: HGT halo gravity traction, HPT halo pelvic traction, IS idiopathic scoliosis, CS congenital scoliosis, NMS neuromuscular scoliosis, NF neurofibromatosis, TB tuberculosis.
Radiographic Evaluation
Main Curve Cobb Angle
Comparison of Radiographic Parameters Between Two Halo Traction Methods.
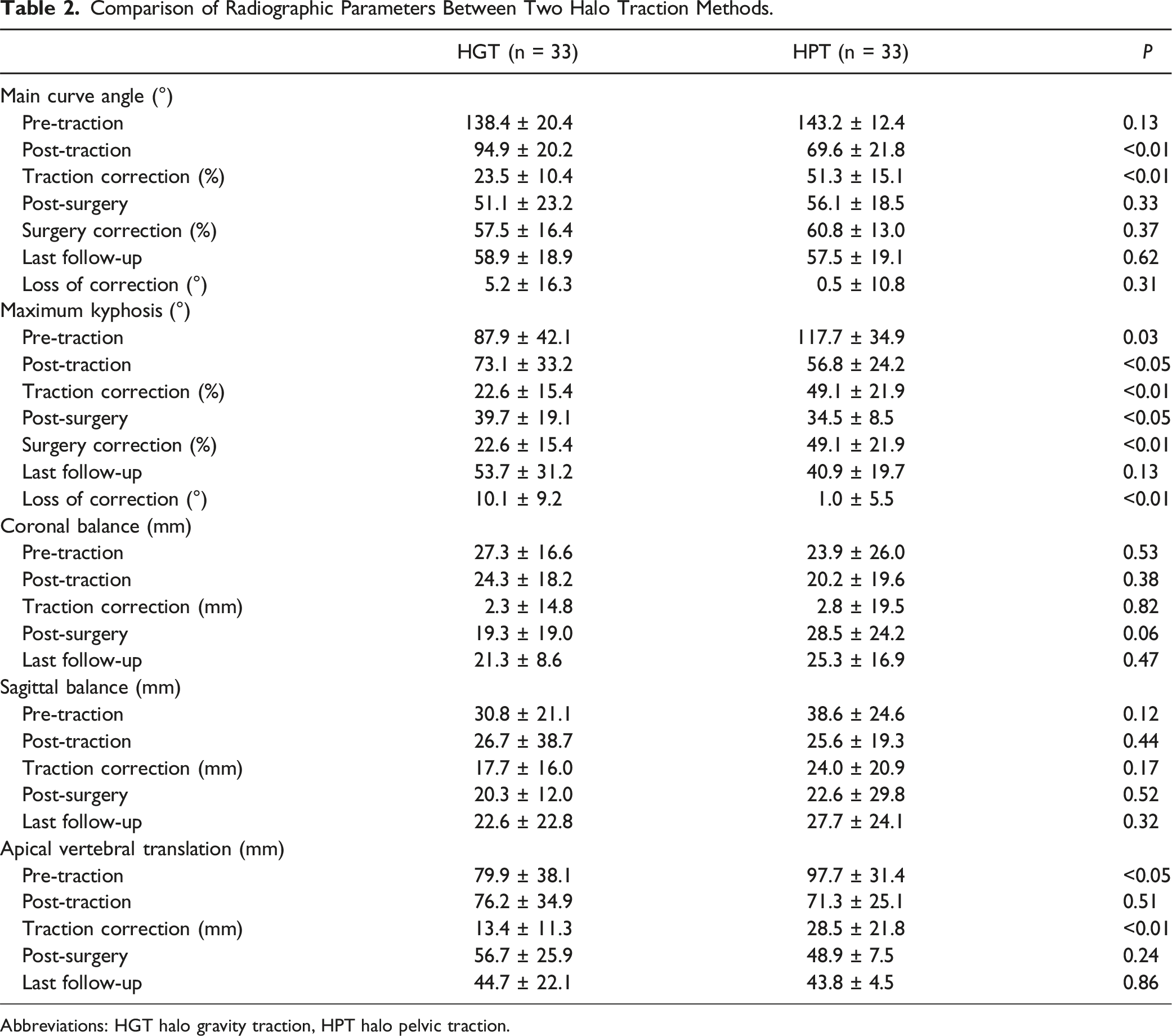
Abbreviations: HGT halo gravity traction, HPT halo pelvic traction.
Maximum Kyphosis Angle
Before traction, the HPT group had a significantly larger maximum kyphosis angle compared to the HGT group (117.7° ± 34.9° vs 87.9° ± 42.1°, P = 0.03). After traction, the kyphosis angle decreased to 56.8° ± 24.2° in the HPT group and 73.1° ± 33.2° in the HGT group (P < 0.05), with the HPT group showing a 49.1% improvement compared to 22.6% in the HGT group (P < 0.05). Postoperatively, both groups showed further improvements, with the HPT group reaching 34.5° ± 8.5° and the HGT group 39.7° ± 19.1° (P < 0.05).
Balance
Both groups showed significant improvements in coronal and sagittal balance after traction (P < 0.05), though no significant differences in balance were observed between the groups before or after traction. The HPT group had significantly greater apical vertebral translation (AVT) prior to traction (P < 0.05), but no significant difference in AVT was found after traction (71.33 mm vs 76.24 mm, P = 0.51). At final follow-up, both groups maintained satisfactory deformity correction and balance, with no significant changes observed compared to the postoperative status, indicating stable long-term correction (Table 2).
Traction Duration and Correction
Regarding traction duration, the HPT group reached a 50% deformity correction rate within 3 months, with over 60% achieving it by 7 months. In contrast, the HGT group did not reach 50% improvement until 5 months. At the end of traction, the HPT group showed a 51.3% improvement in primary curve Cobb angle and 49.1% in kyphosis angle, while the HGT group showed 23.5% and 22.6%, respectively, Figure 4. Relationship between improvement of main curve in HPT and HGT traction patients and traction duration.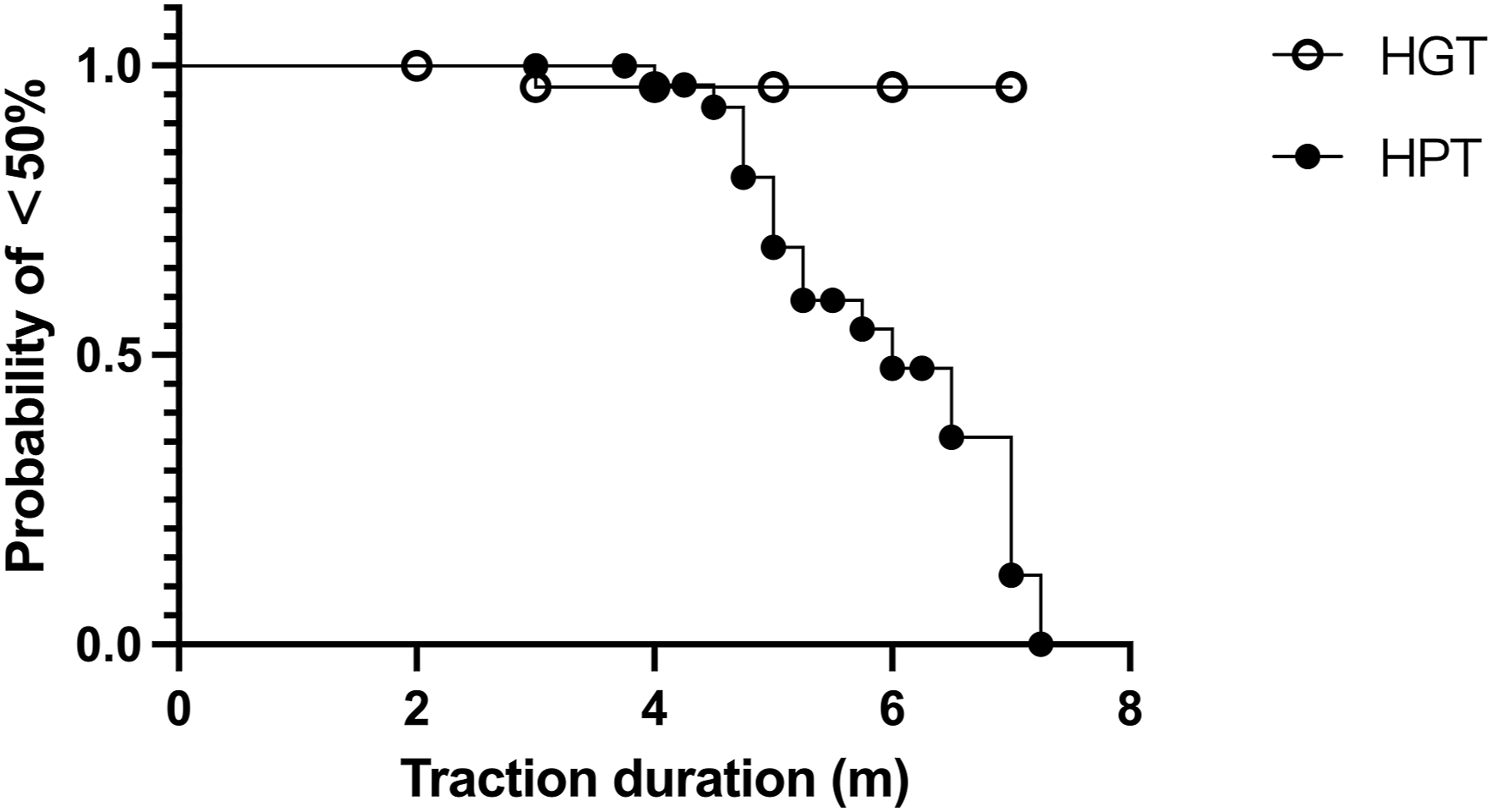
Grade of Osteotomy
Osteotomy procedures were planned by two spinal surgeons independently based on pre- and post-traction imaging. In the HGT group (33 patients), traction reduced the need for three-column osteotomy (90.9% vs 51.5%, P < 0.05). In the HPT group (33 patients), the number of patients requiring three-column osteotomy decreased from 28 to 7 post-traction (84.8% vs 21.2%, P < 0.05). The HPT group also used fewer three-column osteotomies than the HGT group (21.2% vs 51.5%, P < 0.05), Figure 5. Post-traction osteotomy planning (A) and intraoperative osteotomy procedure (B) in 2 groups.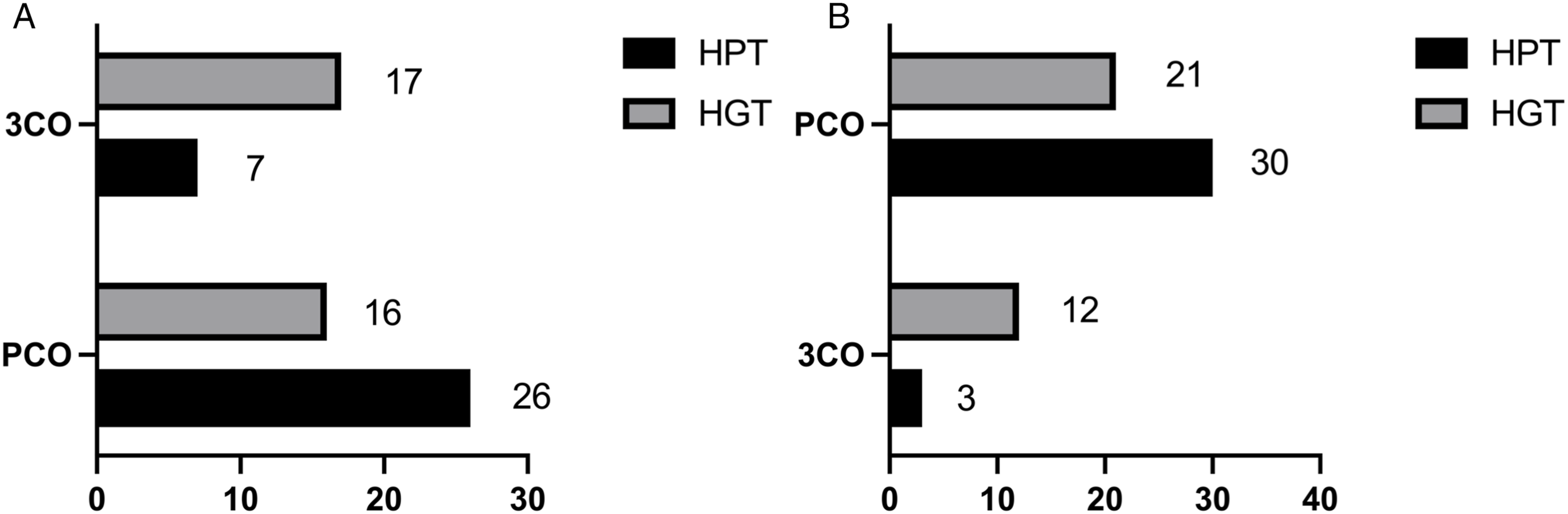
Fused Segment and Clinical Outcome
After traction, the average number of fused segments in the final surgery for patients in the HGT group was 13.5 ± 1.4 segments, while in the HPT group, it was 12.8 ± 1.16 segments. There was a significant difference of 0.73 ± 0.32 fused segments between the two groups (P = 0.02). Regarding other surgery-related parameters, such as intraoperative blood loss and operative time, no significant differences were observed between the two groups, Figure 6. Comparison of the number of fused segments in surgical procedures between 2 groups of patients with Halo traction.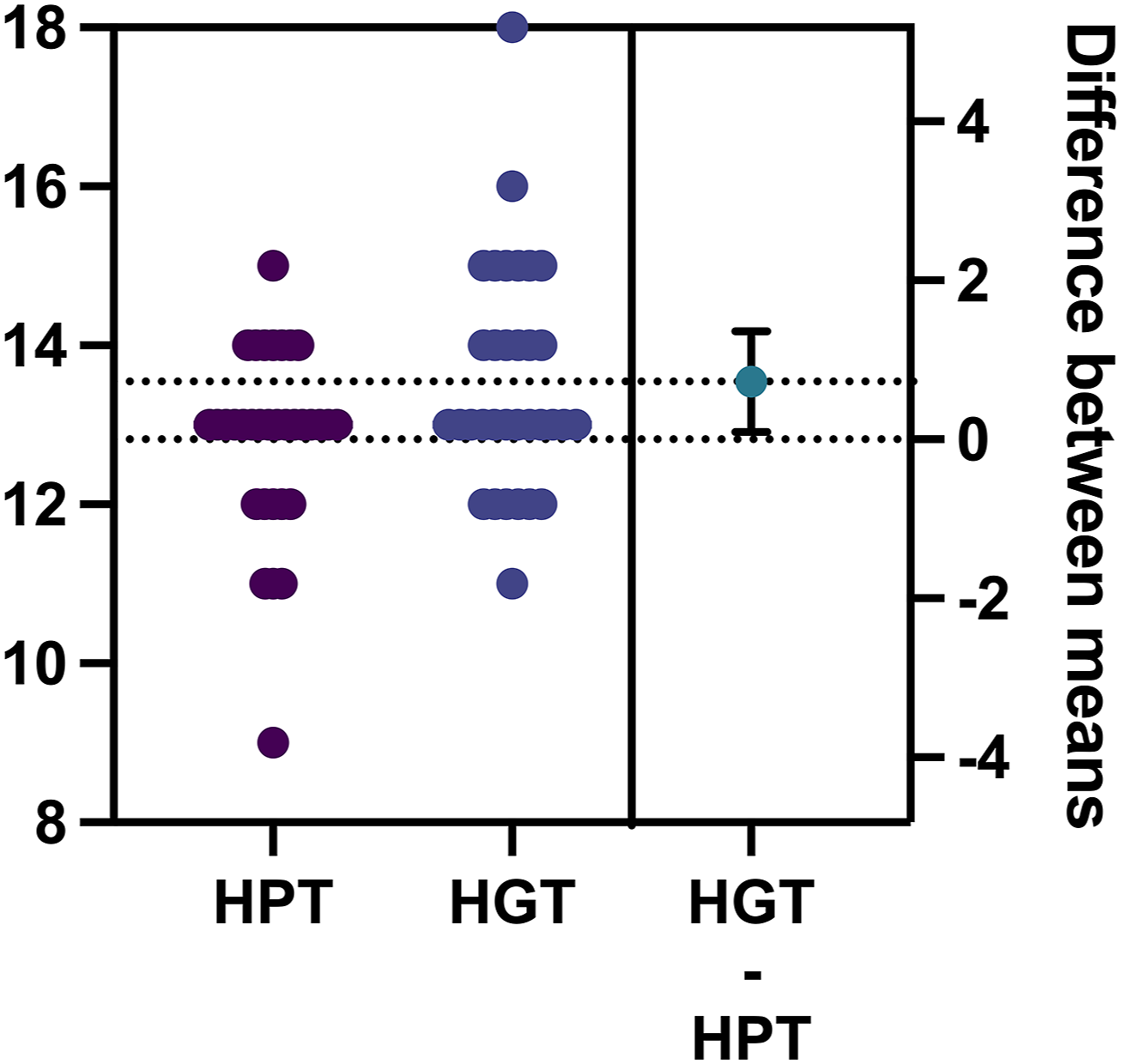
Complications
Fifteen patients experienced traction- or surgery-related complications during the study. In the HPT group (21.2%), 7 patients had complications, including 3 traction-related issues (9.1%). In the HGT group (24.2%), 8 patients had complications, with 1 traction-related issue (3.0%). There were no significant differences between the groups. HPT complications were mostly traction-related (eg, dysphagia, deltoid weakness), resolving with reduced traction, while HGT complications were primarily fixation-related, requiring revision surgery. Halo traction-related complications observed in both patient groups included neurological injuries, such as brachial plexus paralysis (upper limb weakness), cranial nerve paralysis (dysphagia), atlantoaxial subluxation, and pin-site infections. All patients experiencing neurological complications were promptly managed by reducing traction height or weight and administering neurotrophic medications. If symptoms persisted after 1 week, immediate spinal corrective surgery was performed. For patients with atlantoaxial subluxation during traction (2 cases in the HPT group, none in the HGT group), urgent spinal surgery was performed, followed by cervical collar immobilization for one month. Follow-up CT scans confirmed complete reduction of the atlantoaxial subluxation. Patients with pin-site infections were treated with wound dressing changes and oral antibiotics, achieving full resolution within 1 week. No cases of permanent neurological injury or mortality attributable to traction were reported among the study participants.
Discussion
In severe rigid scoliosis, thoracic deformity often impairs respiratory function, reducing blood oxygen saturation levels and hindering daily activities. 17 This decline also increases anesthesia risks and postoperative pulmonary complications. 18 Untreated patients face higher mortality rates due to respiratory failure and cardiovascular diseases. 19
Three-column osteotomies, such as vertebral column resection (VCR), effectively correct severe deformities,20,21 but carry risks like spinal cord injury, significant blood loss, and neurological complications (up to 8% incidence, with 2-6% permanent deficits),8,22,23 increasing surgical complexity.22,24
Given these risks, including paraplegia and mortality, many researchers recommend avoiding single-stage surgery, favoring preoperative strategies to improve spinal and cardiopulmonary function, reducing complications.22,25,26 Halo-gravity traction (HGT) and halo-pelvic traction (HPT) are common preoperative methods. Studies show both are effective,14,27,28 but their comparative safety and efficacy remain underexplored. HPT provides stronger, controlled forces with free walking, while HGT offers flexibility and gentler traction with wheelchair or staying in bed.29-31 This study’s retrospective matched cohort analysis compares deformity correction, osteotomy grade reduction, and safety between HGT and HPT to guide personalized preoperative traction choices.
Comparing Traction Methods in Deformity Improvement
In 2013, Lenke et al 8 eported that vertebral column resection (VCR) osteotomy reduced coronal and sagittal spinal deformities by 54% and 47%, respectively. Our study found that preoperative halo-pelvic traction (HPT) improved the primary Cobb angle by 51.3% and maximum kyphosis by 49.1%, comparable to VCR outcomes and consistent with prior studies.30,32 In contrast, halo-gravity traction (HGT) achieved only 23.5% and 22.6% improvements in Cobb angle and kyphosis, aligning with reported ranges of 12-35%.33-35 Thus, HPT outperforms HGT, particularly for kyphosis, making it preferable for severe rigid scoliosis with significant kyphosis.
No significant differences were observed between HPT and HGT in coronal or sagittal balance correction. However, clinical experience suggests HGT struggles to target balance, whereas HPT’s adjustable external fixation frame offers advantages for complex deformities and improving balance, especially in the sagittal plane.30,36
To date, no studies have directly compared the optimal traction durations for HGT and HPT. Park et al 37 claimed HGT achieves 67% of its final effect within 1 week, and beyond 3 months, HGT yields minimal additional correction. 35 Although this study indicates that patients in the HPT group had a longer traction duration compared to the HGT group (5.1 months vs 4.5 months, P < 0.01), as illustrated in Figure 4, most patients in the HGT group reached a plateau phase before 5 months of traction, with no further progress and failing to achieve a 50% deformity correction rate by the end of traction. In contrast, the HPT group attained a 50% deformity correction rate within 3 months, with over 60% of patients achieving this by 7 months. Therefore, it is not the extended traction duration that led to better deformity correction in the HPT group; rather, the superior traction efficacy encouraged patients to persist with longer traction periods. For the HGT group, extending traction duration did not overcome the limitations inherent to the traction method, as patients, once reaching the plateau phase, typically opted to discontinue traction.
Consequently, under equivalent traction durations, HPT results in more significant deformity correction and typically reaches the standard for discontinuing traction (50% improvement rate) within approximately 6 months. For patients with higher spinal flexibility, the traction period may be reduced to 3 months.
Comparing Traction Methods in Respiratory Function Improvement
Numerous prior studies on Halo traction have explored the effects of HPT and HGT on improving pulmonary function in patients with severe spinal deformities. These studies indicate that both traction methods can enhance pulmonary function to some extent in patients with SRSD. During traction, partial correction of spinal deformities increases thoracic cavity volume and improves diaphragmatic function.31,38 Consequently, HPT, which is theoretically more effective in correcting deformities compared to HGT, is expected to yield greater improvements in respiratory function. 39 Previous research has reported that HGT improves pulmonary function by 6.6-9.5%,28,40 while HPT achieves improvements ranging from 15.6-29.4%.27,39 Chen et al 39 suggested that HPT is more suitable for SRSD patients, offering superior respiratory function outcomes. Although this is the first study to comprehensively compare the therapeutic efficacy of HGT and HPT for SRSD, it is limited by the absence of a direct comparison of their effects on pulmonary function improvement.
Comparing Traction Methods in Changing Surgery Procedure
Preoperative halo traction can reduce osteotomy grades in surgery, minimizing the need for vertebral column resection (VCR) and enhancing perioperative safety for patients with severe rigid spinal deformity. Wang et al 15 reported a 2-year follow-up where patients receiving preoperative halo-pelvic traction (HPT) with deformity correction surgery (without VCR) achieved a 64% correction rate, compared to 65% with VCR. This suggests HPT can deliver comparable deformity correction without VCR, a method often used to assess traction’s impact on osteotomy levels.
This study pioneers chi-square tests to compare three-column osteotomy use before, after traction, and during surgery. Pre-traction, 90.9% of HGT and 84.8% of HPT patients required osteotomy. Post-traction, rates dropped to 51.5% (HGT) and 21.2% (HPT) (P < 0.05). HPT reduced osteotomy needs more than HGT. Combined with posterior correction, preoperative traction matches VCR correction, enhancing safety and efficacy for severe rigid spinal deformity.
This study is the first to investigate whether preoperative halo traction reduces fused segments in final surgery. Comparing HPT and HGT groups, HPT required 1 fewer fused segment, suggesting deformity improvement influences segment selection. Although no non-traction group was included, the findings highlight HPT’s advantage. Preoperative traction lowers osteotomy levels, and when combined with low-level posterior osteotomy, it sustains deformity correction. At final follow-up, both groups maintained stable correction and balance, consistent with prior studies.15,30,41 This also suggests that the treatment approach of combining preoperative halo traction with low-level posterior osteotomy can help patients with severe rigid spinal deformity achieve effective and lasting deformity correction.
Comparing Traction Methods in Complication
This study found complication rates of 21.2% for HPT and 24.2% for HGT, with all traction-phase issues resolved promptly. Halo traction, particularly Halo Pelvic Traction, may result in neurological injury to the brachial plexus or cranial nerves during the traction, manifesting as upper limb weakness or dysphagia. In this study, all such complications were effectively managed by reducing or discontinuing traction and proceeding to timely surgical intervention, with no instances of permanent neurological damage or mortality. Infectious complications associated with traction were successfully controlled with oral antibiotics. Perioperatively, only 2 HPT and 1 HGT patients developed neurological complications, far fewer than in prior first-stage surgeries.8,22 Staged preoperative halo traction with posterior correction distributes risks, reducing complications via gradual traction, especially for VCR osteotomy. HPT showed more immediate traction risks, while HGT had more fixation-related issues, but overall complication rates were similar. Despite the potential for complications during Halo traction, the overall safety of the treatment process for severe rigid spinal deformity is enhanced by reducing surgery-related complications. 15
Limitation
This study has several limitations. As a single-center retrospective cohort study, it is inherently susceptible to selection bias. Preoperative factors, such as pulmonary function and spinal rigidity, may influence the choice of traction method. Due to the limited sample size, subgroup analyses based on scoliosis etiology were not feasible. Additionally, this study primarily focused on deformity correction and surgical guidance, overlooking comparisons of the traction methods’ effects on pulmonary function and quality of life. To address these limitations, our team plans to conduct multicenter prospective controlled studies with larger sample sizes to minimize bias, evaluate key confounders, and investigate the impact of traction methods on pulmonary function and quality of life, thereby providing robust evidence to guide clinical decision-making.
Conclusion
Halo gravity traction (HGT) and halo pelvic traction (HPT) effectively correct severe rigid spinal deformity and imbalance. Both reduce high-grade osteotomy needs compared to initial plans. HPT outperforms HGT in deformity correction, osteotomy grade reduction, and fusion segment minimization. (1) HPT achieves double the deformity reduction of HGT, enabling earlier surgical readiness (50% correction at 3 vs 5 months) (2) Enhanced preoperative correction preserves spinal mobility with fewer fusion segments, particularly beneficial for young patients with residual growth potential. (3) HPT reduces high-risk three-column osteotomies significantly compared to HGT, minimizing neurological risks and surgical complexity. (4) Directional force modulation in HPT optimizes sagittal alignment, critical for rigid kyphoscoliosis requiring multiplanar correction.
Footnotes
Author Contributions
(I) Conception and design: Lijin Zhou, Jianqiang Wang; (II) Administrative support: Yong Hai, Lijin Zhou; (III) Provision of study materials or patients: Yiqi Zhang, Yunsheng wang; (IV) Collection and assembly of data: Jianqiang Wang, Honghao Yang; (V) Data analysis and interpretation: Lijin Zhou, Jianqiang Wang; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by National Key Research and Development Program of China (2022YFC2407206).
Ethical Statement
Data Availability Statement
The data used to support the findings of this study are available from the first author upon request.