
Abstract
Study design
Retrospective cohort study.
Objective
To analyze the efficacy and safety of Halo-femoral traction (HFT) following spinal release, and preoperative Halo-gravity traction (HGT) in patients with severe spinal kyphoscoliosis and spinal cord risk classification (SCRC) type 3 at the apex.
Methods
A total of 73 patients (24 males, 49 females, mean age 22.4 ± 6.4 years) and 56 patients (15 males, 41 females, mean age 22.9 ± 10.4 years) were included in the HFT and HGT group, respectively. Radiographic parameters were measured at the initial assessment, post-traction, post-final surgery, and during each follow-up. Neurologic function was assessed using the Frankel score system. IONM alerts and all complications were documented. Quality-of-life was evaluated using the SF-36 questionnaire.
Results
In the HFT vs HGT group, the total correction rates were 39.9 ± 7.2% v.s. 41.3 ± 6.8% for the major Cobb and 36.6 ± 9.3% v.s. 44.4 ± 9.2% for global kyphosis (GK) after final surgery, respectively. The traction contributions were 57.6 ± 11.1% v.s. 52.3 ± 9.3% for major Cobb and 70.1 ± 10.5% v.s. 63.9 ± 11.1% for global kyphosis (GK), respectively. More than half of the total correction can be achieved gradually and safely through preoperative traction with patients in an awake state. No deterioration in neurological function was found post-final surgery. During the last follow-up, SF-36 questionnaire scores improved significantly in both groups (P < .05).
Conclusions
Significant outcomes can be expected in patients with severe kyphoscoliosis, even with spinal cord risk classification (SCRC) type 3 at the apex undergoing HFT and HGT.
Keywords
Introduction
Currently, patients with severe spinal kyphoscoliosis undergoing posterior spinal correction can expect satisfactory radiographic and clinical outcomes. The three-column osteotomy (3-CO) has significantly contributed to a high correction rate.1-4 However, with the widespread application of 3-CO, neurologic complications, including spinal cord injury and paralysis, have been catastrophic for patients.5-7 To minimize iatrogenic neurologic deficits, spinal traction techniques, such as halo-femoral traction (HFT) following spinal release combined with a second-stage posterior correction procedure, and preoperative halo-gravity traction (HGT), have been proposed. These alternatives to 3-CO have shown relatively favorable radiographic and clinical outcomes.8-11
To preoperatively assess the risk of intraoperative neuromonitoring (IONM) data loss during correction surgery, the MRI-based classification of spinal cord shape and the presence of cerebrospinal fluid (CSF) at the curve apex were first reported by Sielatycki et al 12 in 2020. Their findings indicated that spinal cord risk classification (SCRC) type 3, characterized by deformation from the apical concave pedicle or vertebral body with no intervening CSF between the cord and the pedicle/body, was significantly associated with increased odds of an IONM event. These results were corroborated by the previous study, 13 which demonstrated that patients with a type 3 spinal cord presented with greater severity of spinal deformity, a higher incidence of preoperative neurologic deficits, and an elevated risk of postoperative neurologic complications during 3-CO. Consequently, we hypothesized that the HFT and HGT may be particularly suitable for patients with severe kyphoscoliosis combined with spinal cord risk classification type 3 at the apex.
The purpose of this study was 2-fold: (1) to analyze the radiographic and clinical outcomes of Halo-Femoral Traction (HFT) and Halo-Gravity Traction (HGT) in patients with severe spinal kyphoscoliosis combined with spinal cord risk classification (SCRC) type 3 at the apex; and (2) to evaluate the efficacy and safety of the HFT and HGT in this high-risk cohort.
Materials and Methods
Subjects
A retrospective review was conducted on a series of patients with severe spinal deformity who underwent posterior spinal correction surgery from January 2009 to December 2021.The inclusion criteria were: (1) patients aged over 10 years; (2) the apex of the main coronal/sagittal curve located in the thoracic spine, with a main Cobb angle greater than 90° on standing whole spinal X-rays and less than 30% flexibility of the main curve on side-bending films; (3)The initial 3D-CT deformity angular ratio (DAR)14-16 greater than or equal to 17 , and combined with spinal cord risk classification (SCRC) type 312 over the apex of the main coronal/sagittal curve; (4) undergoing either Halo-Femoral Traction (HFT) (first-stage posterior spinal release and HFT, followed by second-stage posterior spinal correction surgery) or Halo-Gravity Traction (HGT) (preoperative HGT followed by one-stage posterior spinal correction surgery); (5) possessing intact radiographic and clinical data at initial, post-traction, post-final surgery and at each follow-up; and (6) having at least 2 years of complete follow-up. The exclusion criteria were: (1) patients with any history of spinal surgery; (2) those undergoing combined anterior and posterior surgery; (3) those undergoing posterior three-column osteotomy (3-CO).
The choice of traction method for each patient was determined based on their pulmonary function and nutritional status. Halo-femoral traction (HFT) was the preferred method for patients, while Halo-Gravity Traction (HGT) was used as an alternative for patients with worse preoperative pulmonary function and poor nutrition. Ultimately, 73 patients (24 males, 49 females, mean age: 22.4 ± 6.4 years) were included in the HFT group, and 56 patients (15 males, 41 females, mean age: 22.9 ± 10.4 years) in the HGT group. This study was approved by the Institutional Review Board at our University Hospital.
The HFT Group
The surgical procedure for the HFT group was conducted in 2 stages. In the first stage, patients were positioned prone, and pedicle screws were inserted at predetermined levels through a posterior midline incision. Multiple-level Ponte osteotomies were performed around the apex, and the incision was closed without rod fixation. Before the patient was brought out of anesthesia, the cranial halo pins were tightened, and bilateral femoral supracondylar traction pins were inserted with the patient in a supine position. Patients then underwent supine HFT in bed, typically beginning 3 days postoperatively. The initial traction weight was set at 2 kg and gradually increased to 30-50% of the patient’s body weight as tolerated. The final traction weight was adjusted based on each patient’s tolerance. Traction was applied for at least 12 hours daily, with nighttime traction set at 50% of the maximum. Patients undergoing Halo-Femoral Traction (HFT) are required to remain bedridden during traction. While movement is possible when traction is not applied, mobility is limited and must be performed with caution due to the presence of femoral pins, which restrict long-distance ambulation. Patients underwent daily neurologic assessments to monitor for any HFT-related complications. The second stage, consisting of posterior spinal correction and fusion, was generally performed 3 weeks after initiating traction. 10
The HGT Group
In the HGT group, preoperative HGT was administered using a wheelchair setup. Four to eight halo pins were placed and tightened to a torque of 6-8 pounds, depending on the patient’s age and cranial bone quality. The initial traction load was set at 2 kg, with daily increments of 2 kg until reaching a target of 30-50% of the patient’s body weight, based on patient tolerance, with a maximum limit of 15 kg. Traction was applied for more than 12 hours daily, with the weight halved during nighttime. Patients undergoing Halo-Gravity Traction (HGT) are able to move with the assistance of crutches or a wheelchair during the traction process, and they can ambulate without traction as well. Patients underwent daily neurologic assessments to monitor for any HGT-related complications. The duration of HGT was determined based on the improvement in coronal and sagittal curves, pulmonary functions, and neurologic status. Termination of HGT was recommended for patients showing improvement or stabilization in these areas. Subsequently, a one-stage posterior spinal correction and fusion surgery was performed, incorporating multiple-level Ponte osteotomies around the apex. 17
All patients remain hospitalized throughout the traction process but are transferred to rehabilitation ward beds to avoid occupying surgical ward beds for an extended period.
Radiographic Parameters
During the initial assessment, post-traction, post-final surgery, and last follow-up, standing whole spinal X-rays were obtained for all patients. Each evaluation was conducted using the Picture Archiving and Communication System (PACS) workstation. All data were measured and recorded independently by 3 senior spine surgeons at our center. The average of the 3 measurements was then taken for presentation and analysis. The radiographic parameters assessed included the Cobb angle of the main curve and the distance between C7 plumb line and central sacral vertical line (C7PL-CSVL). Additionally, sagittal plane parameters such as global kyphosis (GK), sagittal vertical axis (SVA) were measured. The flexibility of the main curve was evaluated using the following formula:

All the collected data were utilized to calculate the total correction rate after the operation, as well as the contributions of both traction and the final surgery. The total correction rate refers to the proportion of the overall correction achieved compared to the initial deformity on standing upright radiographs. The contribution of traction or final surgery is defined as the proportion of the correction achieved specifically by either the traction process or the final surgical intervention. These values were calculated using the following formulas:



Clinical Assessments
Neurologic function was assessed during the initial assessment, post-traction, post-final surgery, and at each follow-up visit using the Frankel score system. Intra-operative neurophysiological monitoring (IONM) alerts were recorded if any of the following occurred: (1) an increase in somatosensory evoked potentials (SSEP) latency exceeding 10%; (2) a decrease in SSEP amplitude exceeding 50%; or (3) a decrease in motor evoked potentials (MEP) amplitude exceeding 80%. All complications arising during traction, surgery and at each follow-up visit were meticulously documented. Additionally, the Short Form (SF-36) questionnaire was used to evaluate quality-of-life.
Statistical Analysis
Statistical analysis was conducted using SPSS software version 22.0 (IBM, NY, US). Descriptive statistics were used to analyze patient demographics, with data presented as mean ± standard deviation. Categorical data comparisons were performed using the Chi-square or Fisher’s exact test, as appropriate. The paired t-test was used to compare the mean differences between initial, post-traction, post-final surgery, and last follow-up measurements. A P-value of <.05 was considered statistically significant.
Results
General Data
The General Data of Patients in the HFT and HGT Groups.
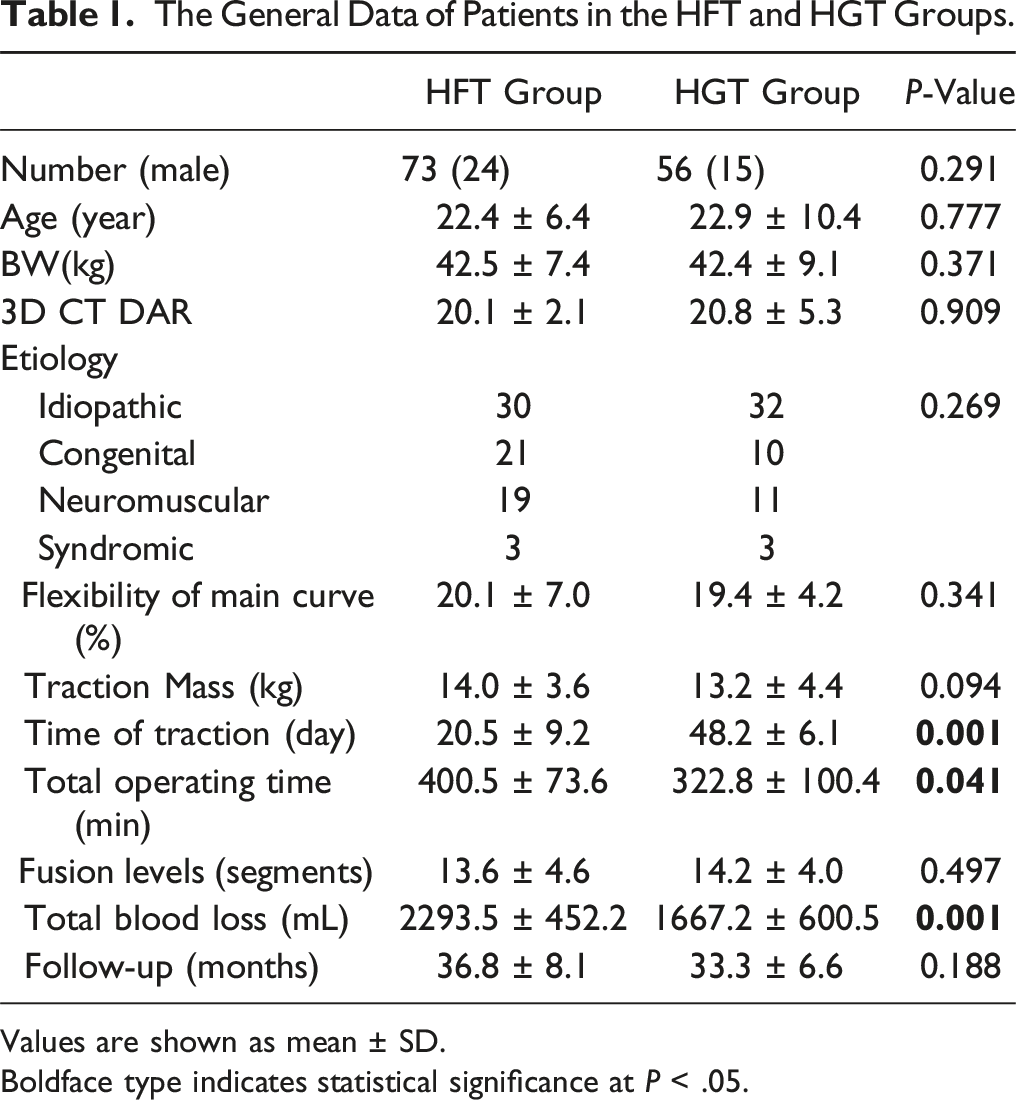
Values are shown as mean ± SD.
Boldface type indicates statistical significance at P < .05.
Radiographic Outcomes
In the HFT group, the average Cobb angle of the main curve was 121.1 ± 13.9° at initial assessment, which significantly decreased to 93.3 ± 18.8° post-traction and further to 72.8 ± 20.6° post-final surgery (P < .001). Similarly, the average global kyphosis (GK) angle was 86.5 ± 19.4° at initial assessment, significantly decreasing to 64.3 ± 12.1° post-traction and 54.8 ± 13.1° post-final surgery (P < .001). Along with the significant improvements in the Cobb angle and GK angle, notable improvements were also observed immediately post-final surgery in the horizontal distance between the C7 plumb line and central sacral vertical line (C7PL-CSVL), sagittal vertical axis (SVA) compared to initial values (P < .05 for all). No significant loss of correction was observed during the last follow-up.
The Details of Radiographic Parameters in the HFT and HGT Groups.
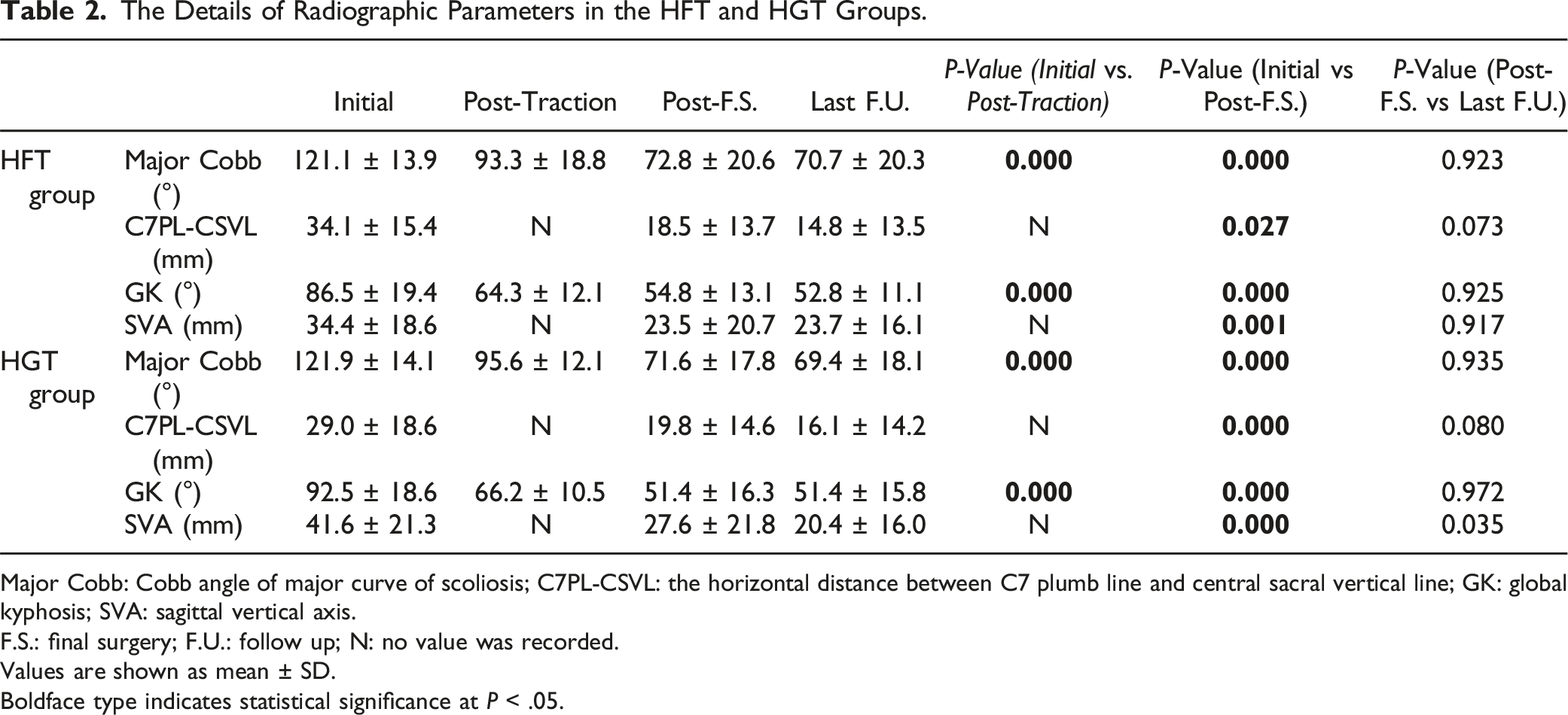
Major Cobb: Cobb angle of major curve of scoliosis; C7PL-CSVL: the horizontal distance between C7 plumb line and central sacral vertical line; GK: global kyphosis; SVA: sagittal vertical axis.
F.S.: final surgery; F.U.: follow up; N: no value was recorded.
Values are shown as mean ± SD.
Boldface type indicates statistical significance at P < .05.

A patient undergoing HFT is presented. An 18-year-old female was diagnosed with severe adolescent idiopathic scoliosis (a and b), with SCRC type 3 over apex (i), and the bending films showed a rigid curvature (c). The patient underwent a first-stage procedure involving the posterior pedicle screw insertion and multiple-level Ponte osteotomies around the apex (d). After 2 weeks of supine halo-femoral traction in bed, the second-stage posterior spinal correction and fusion were performed (e and f). At the 2-year follow-up, the correction was well maintained with no evidence of correction loss (g and h).
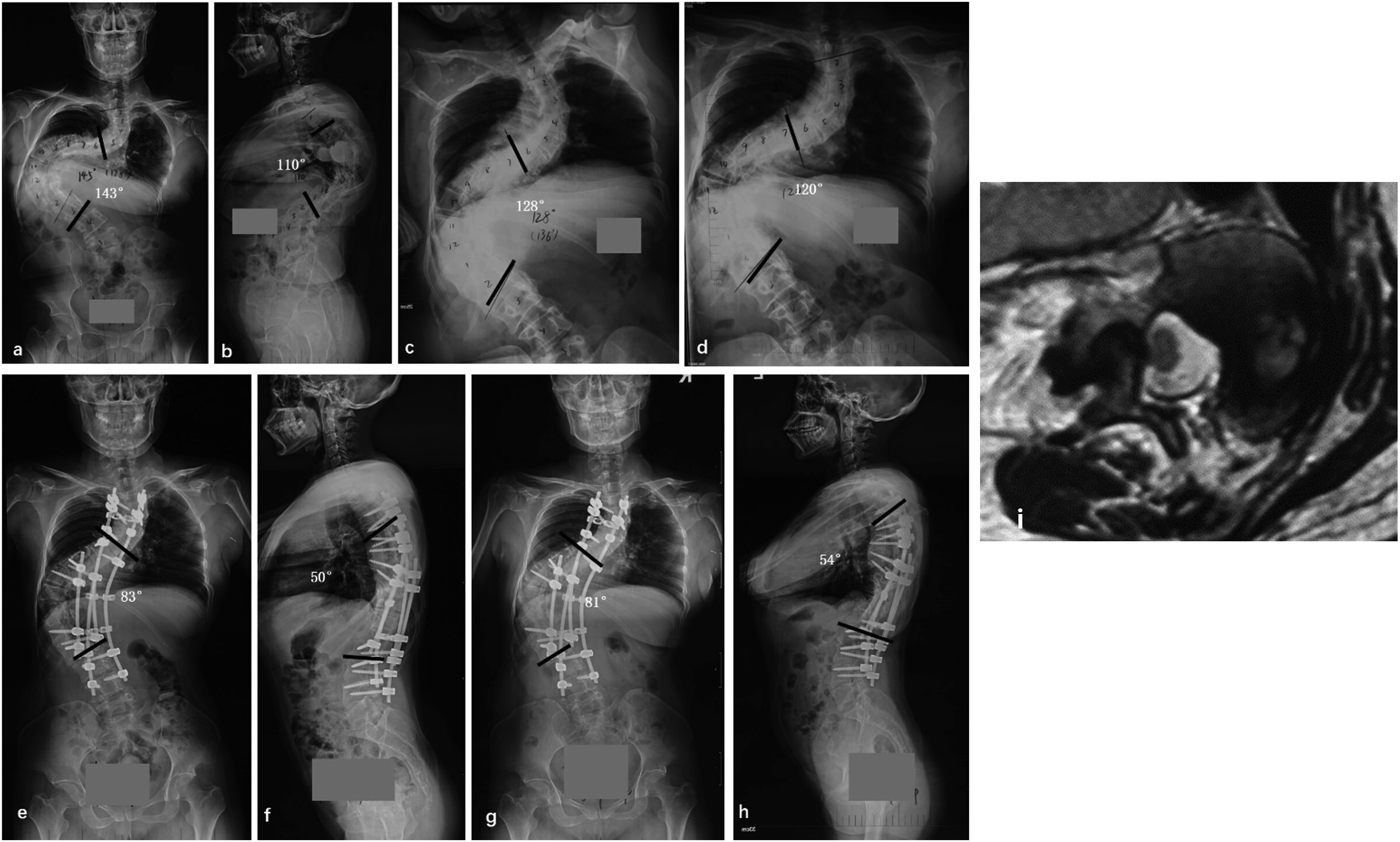
A patient undergoing HGT is presented. A 24-year-old female was diagnosed with severe neuromuscular kyphoscoliosis (a and b), with SCRC type 3 over apex (i), and the bending films showed a rigid curvature (c). The patient underwent preoperative HGT for 2 months (d), followed by posterior spinal correction and fusion with multiple-level Ponte osteotomies around the apex (e and f). At the 2-year follow-up, the correction was well maintained with no evidence of correction loss (g and h).
Clinical Outcomes
In the HFT group of 73 patients, initial neurologic deficits in the lower extremities were observed in 11 cases (15.1%), comprising sensory deficits in 4 patients and motor deficits in 7 patients, respectively. All 11 patients had an initial Frankel score of grade D, with 2 improving to grade E post-final surgery. Intraoperative neurophysiological monitoring (IONM) alerts occurred in 2 patients (2.7%) during the second-stage posterior spinal correction procedure, but no new neurologic deficits were observed post-final surgery. Incidental findings included a dural tear in 1 patient, pedicle screw misplacement in 3 patients, and superficial infections in 3 patients, respectively. Follow-up revealed proximal junctional kyphosis in 4 patients (5.5%) and rod breakage in 2 patients (2.7%).
Summary of the Clinical Outcomes of Patients in the HFT and HGT Groups.
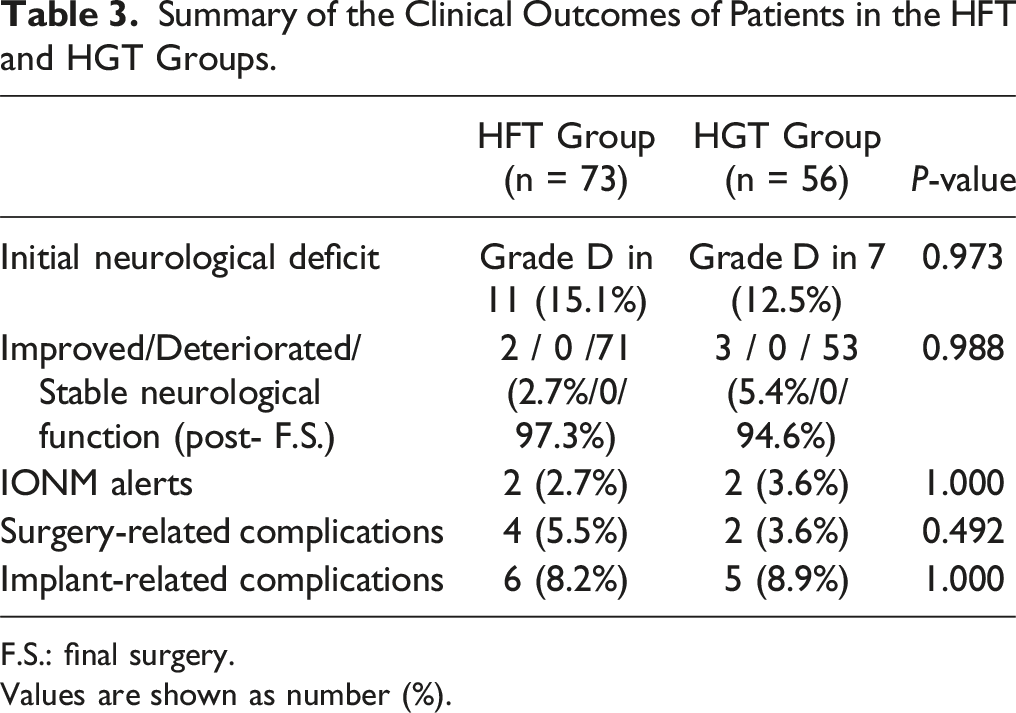
F.S.: final surgery.
Values are shown as number (%).
According to the data presented in Table 3, there were no statistical differences between the 2 traction groups in terms of initial neurological status, the probability of neurological function changes post-final surgery, IONM alert probability, or the rate of surgery or implant related complications.
Comparison of SF-36 Questionnaire Scores Between Initial and the Last Follow-Up in the HFT and HGT Groups.
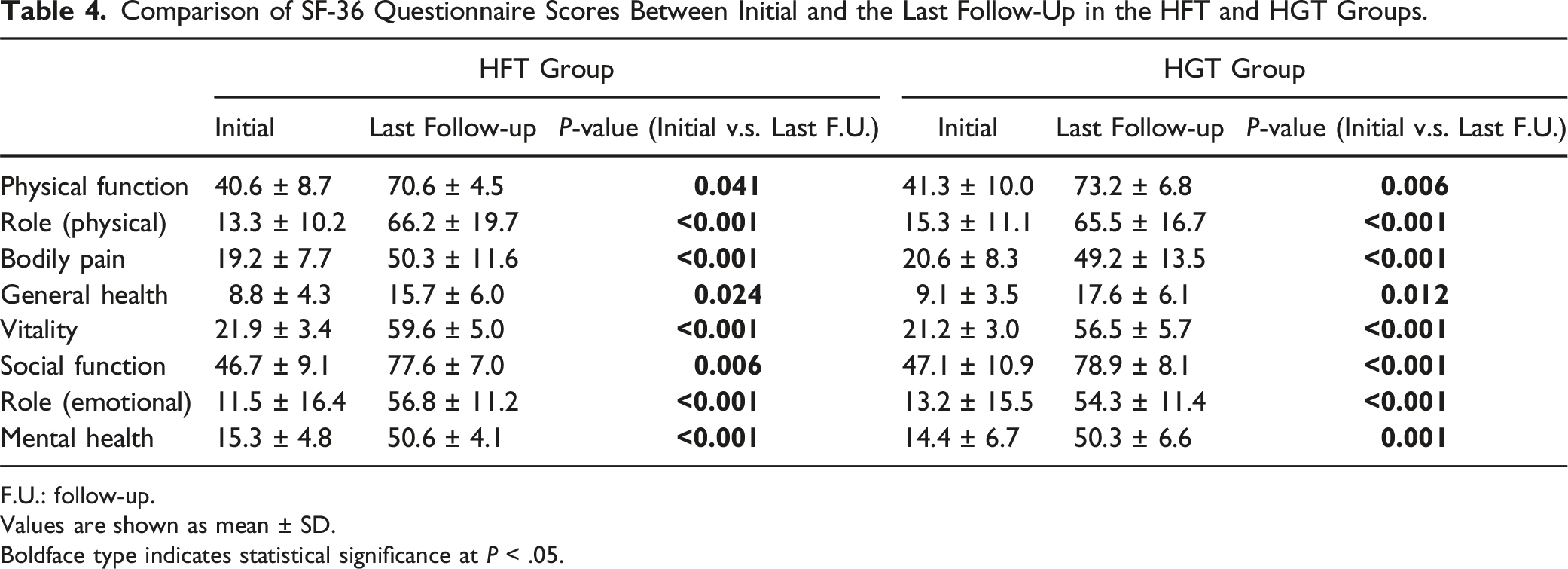
F.U.: follow-up.
Values are shown as mean ± SD.
Boldface type indicates statistical significance at P < .05.
Traction-Related Complications
In the HFT group, deep venous thrombosis was observed in 3 patients (4.1%). While no cases of traction pin loosening were reported, superficial infection around the pin was observed in 1 patient (1.4%).
In the HGT group, there were no instances of deep venous thrombosis or brachial plexus injury. Traction pin loosening occurred in 3 patients (5.4%), with superficial infection around the pin in 1 patient (1.8%).
Discussion
The mean preoperative radiographic parameters showed no difference in the coronal Cobb angle and global kyphosis (GK) angle between the 2 study groups. At the end of the surgical treatment, improvements in the major curve Cobb angle were obtained immediately, with a mean total correction percentage of 39.9 ± 7.2% vs 41.3 ± 6.8% for the 2 study groups based on the aforementioned formula. Similarly, in the sagittal plane, the global kyphosis (GK) angle improved with a mean total correction percentage of 36.6 ± 9.3% vs 44.4 ± 9 .2%. There were no significant statistical differences between the 2 groups in terms of the total correction rate of the major Cobb and GK angles.
Comparison of Correction Rate, Traction Contribution in the HFT and HGT Groups.
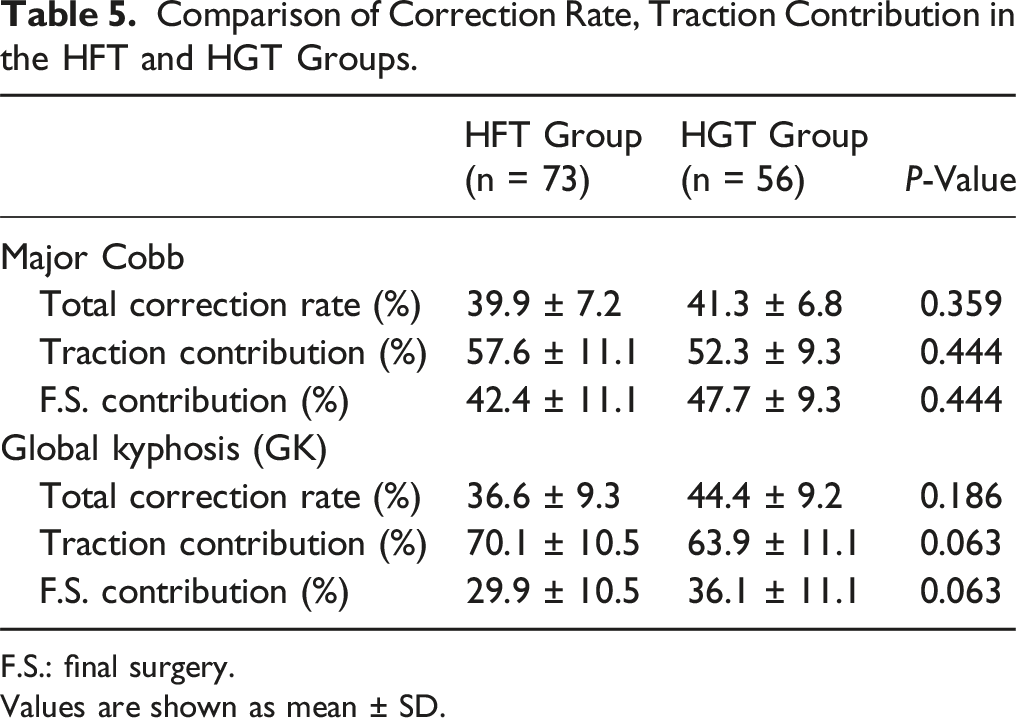
F.S.: final surgery.
Values are shown as mean ± SD.
According to the previous studies, Chen et al 18 reported that in 51 patients with severe spinal kyphoscoliosis undergoing the HGT, the Cobb angle of the main curve improved from 140.7° to 120.2° after traction, yielding an average correction rate of 14.6%. Postoperatively, the Cobb angle further decreased to 63.9°, achieving a total correction rate of 54.6%. Zhang et al 19 demonstrated an average correction rate of 39.3% after the HGT and 54.7% following a second-stage spinal correction. Shi et al 10 reported average correction rates of 44.7% for the HFT and 39.0% for the HGT. Compared with their study and another study published by Zhang et al 20 with the same ethnicity and etiology, the values were approximately equivalent. This suggests that our preoperative traction strategy may be considered rational and acceptable. Despite the discomfort and inconvenience associated with traction, the quality-of-life questionnaire (SF-36) revealed significant improvements in each domain at the last follow-up (P < .05).
Patients with severe spinal kyphoscoliosis often present with neurologic deficits, vertebral rotational subluxation, and limited pulmonary function, among other complications, posing significant challenges and risks for correction surgery.4,11,21 Iatrogenic neurologic complications during such surgery represent a primary concern for both patients and surgeons.22,23 Over recent decades, despite the proposal of various indicators for assessing the risk of neurologic complications, the MRI-based classification of spinal cord shape (SCRC) and CSF presence at the curve apex, as proposed by Sielatycki et al, has been demonstrated to be effective.12,13 In their study, the incidence of intraoperative neurophysiological monitoring (IONM) events in the type 3 spinal cord group during three-column osteotomy (3-CO) was 80%, significantly higher than in the type 1 and type 2 spinal cord groups (6% and 12.5%, respectively). Even though Hyndman-Schneider procedure24,25 has been proposed to manage the IONM events during deformity corrective surgery, it may not effectively improve neurological safety related to subsequent spinal correction. Additionally, the irritation to the high-tension spinal cord during procedures such as apical pediculectomy, circumferential spinal cord decompression, and osteotomy may also lead to irreversible complications.
To minimize the risk of iatrogenic neurologic complications during correction surgery, Halo-Femoral Traction (HFT) and Halo-Gravity Traction (HGT) have been demonstrated as effective alternatives to three-column osteotomy (3-CO). Traditionally, radiographic outcomes, particularly the correction rate, serve as direct and intuitive criteria for evaluating treatment strategies. Previous studies have reported average curve corrections ranging from 30° to 54° following 3-CO.10,26,27
In this study, the total correction rate of 39.9 ± 7.2% and 41.3 ± 6.8% for the major Cobb angle and 36.6 ± 9.3% and 44.4 ± 9 .2% for global kyphosis (GK) in the HFT and HGT groups, respectively. These values indicate that HFT and HGT can achieve final radiographic outcomes comparable with 3-CO with relative safety. Based on the aforementioned formulas, the traction contribution percentages for the major Cobb were 57.6 ± 11.1% and 52.3 ± 9.3% in HFT and HGT groups, respectively. Similarly, the traction contribution percentages for global kyphosis (GK) were 70.1 ± 10.5% and 63.9 ± 11.1% in HFT and HGT groups, respectively. More than half of the total correction of kyphoscoliosis can be achieved gradually and safely through preoperative traction with patients in an awake state. This approach can make the surgical part much safer by reducing the chance of rapid spinal column realignment and higher neurological risks, especially when associated with a type 3 spinal cord over the apex.
Three-column osteotomy (3-CO) in patients with severe spinal kyphoscoliosis is associated with a greater risk of deteriorative neurologic function, with reported rates28-31 ranging from 8.5% to 35%. Preoperative neurologic deficits and a type 3 spinal cord at the apex have been identified as high risk for IONM events and postoperative neurologic complications.5,13,16,32,33 One study also revealed the use of HGT can reduce the level of osteotomy, contributing to a lower incidence of complications. 20 In the current study, preoperative neurologic deficits were observed in 11 of 73 (15.1%) patients in the HFT group and 7 of 56 (12.5%) patients in the HGT group, with no new neurologic deterioration noted in either group. The preoperative traction correction method allows the high-tension type 3 spinal cord to gradually release tension and undergo shape modification over time. This approach is performed while the patient is awake, enabling continuous monitoring of neurological function and allowing for reversible adjustments as needed.
Despite several complications, such as pedicle screws misplacements, superficial infections, and proximal junctional kyphosis detected in both groups, significantly higher scores on the SF-36 questionnaire during the last follow-up demonstrated the satisfactory clinical outcomes in patients with a type 3 spinal cord after undergoing the HFT and HGT treatments. It should be highlighted that the HFT group experienced significantly longer total operating time and blood loss, aligning with previous studies. 10 These results were anticipated due to the inherent necessity of 2 separate procedures, including steps of exposure and closure.
While the HGT group demonstrated better performance in radiographic parameters, operative time, and blood loss, it required a longer traction period, which raises concerns regarding patient tolerance. Although the radiographic correction rate appeared superior in the HGT group, there was no statistically significant difference compared to the HFT group. Therefore, the 2 traction methods are suited to different clinical scenarios. HFT is more appropriate for patients with better preoperative pulmonary function, good nutritional status, and lower traction tolerance. In contrast, HGT is better suited for patients with compromised pulmonary function, poor nutritional status, but higher traction tolerance. Due to compromised pulmonary function, performing general anesthesia with intubation and Ponte osteotomy prior to HGT may increase the risk of difficult extubation and subsequent airway and pulmonary complications. This serves as the rationale for the use of direct HGT.
Traction-related complications should not be overlooked. In the HGT group, the most common traction-related complications were traction pin loosening and superficial infection around the pin. These issues can be attributed to the relatively longer duration of traction. Conversely, patients in the HFT group experienced a higher risk of deep venous thrombosis and superficial incision infection, likely due to the prolonged period of supine traction and the necessity of 2 surgical procedures. Shi et al 11 investigated preoperative HGT in patients with severe type 1 neurofibromatosis and congenital scoliosis, reporting 5 traction-related complications in 35 patients. Similarly, Shi et al 10 noted 1 complication in 30 patients in the HGT group and five complications in 30 patients in the HFT group. Therefore, while traction-related complications are relatively common, they are considered acceptable risks, given the effectiveness and safety of these correction techniques.
Limitations
This study has several limitations that should be considered. Firstly, the relatively small sample sizes of both groups and the study’s retrospective nature may introduce bias into the results. Secondly, variations in etiology, curve severity, apex level, and fusion levels between the 2 groups limited the ability to conduct comparative analyses. Thirdly, the decision to use Halo-Gravity Traction (HGT) or Halo-Femoral Traction (HFT) was made collaboratively by spine surgeons, patients, and their parents, so this study is not a randomized double-blind trial, which may introduce a certain degree of bias. Despite these limitations, the study systematically demonstrates satisfactory clinical and radiographic outcomes in patients with severe kyphoscoliosis and spinal cord risk classification (SCRC) type 3 at the apex undergoing HGT and HFT, highlighting their efficacy and safety as alternative strategies to three-column osteotomy (3-CO) in this patient cohort.
Conclusion
In conclusion, patients with severe kyphoscoliosis classified as spinal cord risk classification (SCRC) type 3 over the apex can achieve significant deformity correction and improvements in quality-of-life following HFT and HGT treatment. By employing HFT and HGT with strict indications, the risk of iatrogenic neurological deficits can be minimized. Therefore, both HFT and HGT techniques are effective and safe options for managing severe kyphoscoliosis with a SCRC type 3 over the apex.
Footnotes
Acknowledgments
The author wishes to acknowledge the help of Professor Ben-Long Shi in developing the study design.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent and IRB Approval
Consent was obtained from all study participants and approval obtained from Institutional Review Board at China Medical University Hospital (No. CMUH111-REC1-128).