
Abstract
Study Design
Retrospective cohort study.
Objectives
Severe neck pain has traditionally been considered a relative contraindication for cervical disc replacement (CDR) due to risk of persistent neck pain from the remaining mobile segment. However, recent studies suggest potential for neck pain improvement with CDR. This study aimed to compare postoperative improvements in neck pain and disability between patients undergoing anterior cervical discectomy and fusion (ACDF) and CDR.
Methods
Predominant neck pain was defined as neck pain equal to or greater than arm pain preoperatively (visual analog scale [VAS]) and neck disability index (NDI) > 20. Patients with predominant neck pain who underwent 1- or 2-level ACDF or CDR for radiculopathy between 2017 and 2023 were included. Patient-reported outcomes (NDI, VAS) were assessed up to 1 year postoperatively. Inverse probability of treatment weighting (IPTW) was used to control for confounders. Linear mixed-effect models were applied to compare postoperative outcomes.
Results
A total of 179 patients (105 ACDF, 74 CDR) were included. Both groups showed significant improvement in NDI and VAS neck scores from baseline to 1 year (NDI: β = −1.81, P < .001; VAS neck: β = −.26, P < .001). After IPTW, no significant differences were found between ACDF and CDR across all PROMs up to 1 year (NDI: β = −0.44, P = .09; VAS neck: β = −.07, P = .10).
Conclusion
CDR was associated with postoperative improvements in neck pain and disability comparable to those observed with ACDF in patients with predominant neck pain and radiculopathy. These findings suggest that CDR may be a reasonable treatment option for selected patients.
Keywords
Introduction
Neck pain is a common condition, affecting 3.5% of individuals annually, and is the 4th leading cause of disability worldwide.1-4 It can arise from multiple causes, such as disc degeneration, facet joints, or nerve root compression, making its diagnosis and treatment challenging, particularly in patients with coexisting radiculopathy. Cervical radiculopathy frequently accompanies neck pain, and several studies report concurrent improvement in neck symptoms when radiculopathy symptoms are alleviated.5-7
Anterior cervical discectomy and fusion (ACDF) is a widely used surgical option to treat neck pain caused by various cervical spine disorders such as cervical radiculopathy. Although initially controversial, recent studies consistently report favorable outcomes in terms of neck pain relief following ACDF.8-11 Fusion surgery is traditionally favored for reducing residual neck pain by stabilizing the degenerative cervical spine offering favorable environment for neurological improvement. However, the non-physiological changes induced by fusion, such as increased mechanical load at adjacent levels, raise concerns about the potential for new pain generators.
Cervical disc arthroplasty (CDR) is another surgical option for cervical radiculopathy. It preserves motion of the cervical spine and offers advantages over ACDF.12-18 Despite severe neck pain being considered a relative contraindication for CDR due to concerns that preserving motion in painful segments may exacerbate symptoms, it is often used for patients with radiculopathy and concurrent neck pain in clinical practice. However, the strict inclusion criteria in previous randomized controlled trials complicate the generalizability of ACDF and CDR for neck pain outcomes. While some studies have reported improvement in neck pain among patients treated with CDR,9,19-22 other studies have demonstrated that predominant neck pain is a predictor of poorer outcomes. 23 Although small cohort studies on CDR have accumulated, the lack of sufficient evidence in this specific patient subset with severe neck pain has made it challenging to conduct randomized controlled trials directly comparing the clinical outcomes of ACDF and CDR.
Both procedures are expected to improve outcomes if radiculopathy is appropriately managed, but their relative effectiveness in severe neck pain remains uncertain. Given the limitations of previous studies and the uncertainty regarding the relative effectiveness of CDR and ACDF, this study aims to determine whether significant differences exist in clinical outcomes between CDR and ACDF for patients with predominant neck pain.
Materials and Methods
Study Design and Patient Population
This study was an institutional review board-approved retrospective review of a prospectively collected multi-surgeon database. We included patients who underwent primary 1- or 2-level ACDF or CDR between April 2017 and Dec 2023, were over the age of 18, and had at least 6 months postoperative follow-up. Although minor technical variation may have existed among surgeons, all procedures in both groups were performed using a standard anterior cervical approach (Smith-Robinson approach) with a left-sided incision.
Predominant neck pain was defined as neck pain equal to or greater than arm pain preoperatively (measured by the visual analog scale [VAS]) and neck disability index (NDI) > 20. 24 This objective definition was not utilized clinically for surgical decision making. The inclusion criteria were patients with (1) failed conservative treatment, (2) a diagnosis of cervical radiculopathy or myeloradiculopathy, and (3) predominant neck pain. The decision to proceed with each surgery, including cases with muscle weakness, was made at the discretion of each surgeon. Exclusion criteria included patients undergoing corpectomy, those with cervical deformity, hybrid construct combining CDR and ACDF, multilevel surgery of 3 or more levels, and surgeries for tumors. Data were collected and managed using REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center for Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.25,26
Data Collection
Patient demographic data were obtained from the electronic medical record, including age, sex, race, Body Mass Index (BMI), American Society of Anesthesiologists (ASA) grades, Charlson Comorbidity Index (CCI), number of surgical levels, and surgical levels. Preoperative neck pain and arm pain were assessed using the VAS. For ACDF cases, the use of anterior plate was also recorded.
Patient-reported outcome measures (PROMs) included VAS neck, VAS arm, NDI, Short Form 12 Physical Component Score (SF-12 PCS) and Mental Component Score (SF-12 MCS), and Patient-Reported Outcomes Measurement Information System Physical Component (PROMIS).27-29 PROMs were collected prospectively at preoperative, 2 weeks, 6 weeks, 12 weeks, 6 months, and 1 year or later postoperative time points.
Sample Size Estimation
To estimate the sample size required to detect a 10% difference in NDI scores between groups, thus we used a standard deviation (SD) of 17 based on our previous institutional data. 30 The effect size (Cohen’s d) was calculated as 0.59. With a significance level of 0.05 and a desired power of 80%, the sample size calculation indicated that 46 participants per group would be necessary to detect a statistically significant difference.
Statistical Analysis
Statistical analyses were performed using R (ver. 4.3.1, R Core Team (2024), Vienna, Austria). To compare the ACDF and CDR groups, we initially performed univariate analysis. Continuous variables were analyzed using independent t-test, while categorical variables were analyzed using either the Chi-Square test or Fisher’s exact test, with the latter being employed in cases of small sample sizes. Effect size to show the difference between the groups for univariate analysis were reported with standard mean difference (SMD).
To account for potential confounding factors and create a balanced comparison between the ACDF and CDR groups, we applied inverse probability of treatment weighting (IPTW) based on propensity scores. These propensity scores were calculated from background variables identified as significant through univariate analysis and clinical significance. Given the substantial baseline differences between the groups, a trimming level of 5% was applied to the weights to reduce the influence of extreme values and improve the robustness of the comparison.
After generating the IPTW-adjusted cohort, we assessed the balance between the groups by examining the distribution of propensity scores and calculating the SMD for each covariate. An SMD of less than 0.2 was considered indicative of negligible differences between the groups. The difference with SMD exceeding 0.2 in weighting cohort was assessed based on clinical significance.
Postoperative changes in PROMs were compared between treatment groups using linear mixed-effect models (LMMs). The LMMs were selected over standard two-group comparisons due to their ability to account for the correlation between repeated measures within the same patient. The models included fixed effects for treatment group, timepoint, and their interaction, allowing us to assess how the treatment effect varied over time. The beta coefficient (β) for the treatment group and its interaction with time was used as the effect size, providing a quantitative measure of the treatment impact on PROMs. Random effects were specified for the intercepts of individual patients, accounting for baseline differences in PROMs across patients. By including a random intercept for each patient, the LMM adjusts for intra-patient variability, reflecting the natural correlation in repeated measurements and reducing the risk of type I errors. LMMs were constructed both before and after applying IPTW. The weighted LMM retained the same fixed and random effects as the unweighted model, providing a robust comparison of the clinical outcomes between ACDF and CDR. Statistical significance was defined as a P-value of less than 0.05.
Results
Patient Demographic Data
Demographic Data.
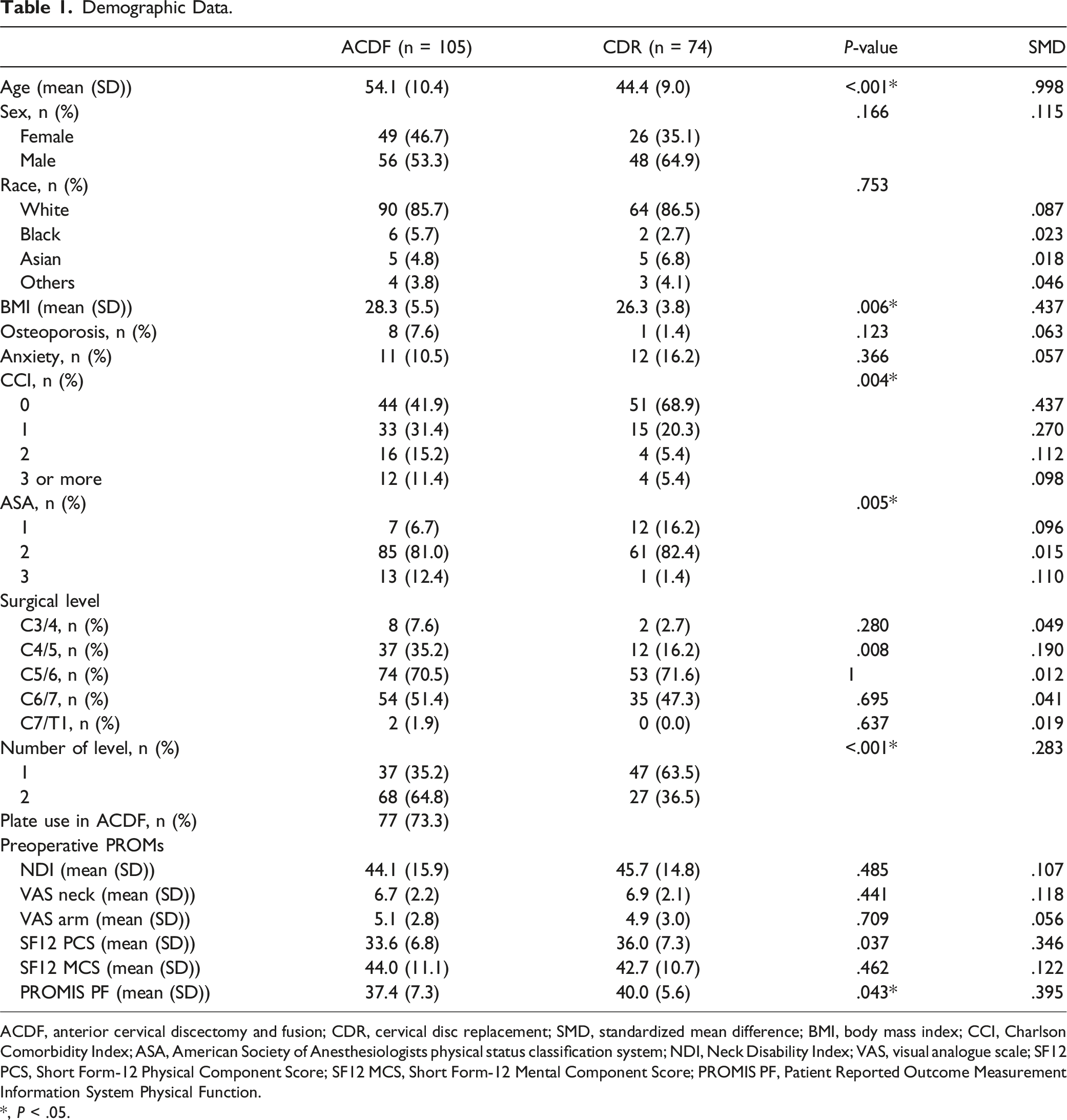
ACDF, anterior cervical discectomy and fusion; CDR, cervical disc replacement; SMD, standardized mean difference; BMI, body mass index; CCI, Charlson Comorbidity Index; ASA, American Society of Anesthesiologists physical status classification system; NDI, Neck Disability Index; VAS, visual analogue scale; SF12 PCS, Short Form-12 Physical Component Score; SF12 MCS, Short Form-12 Mental Component Score; PROMIS PF, Patient Reported Outcome Measurement Information System Physical Function.
*, P < .05.
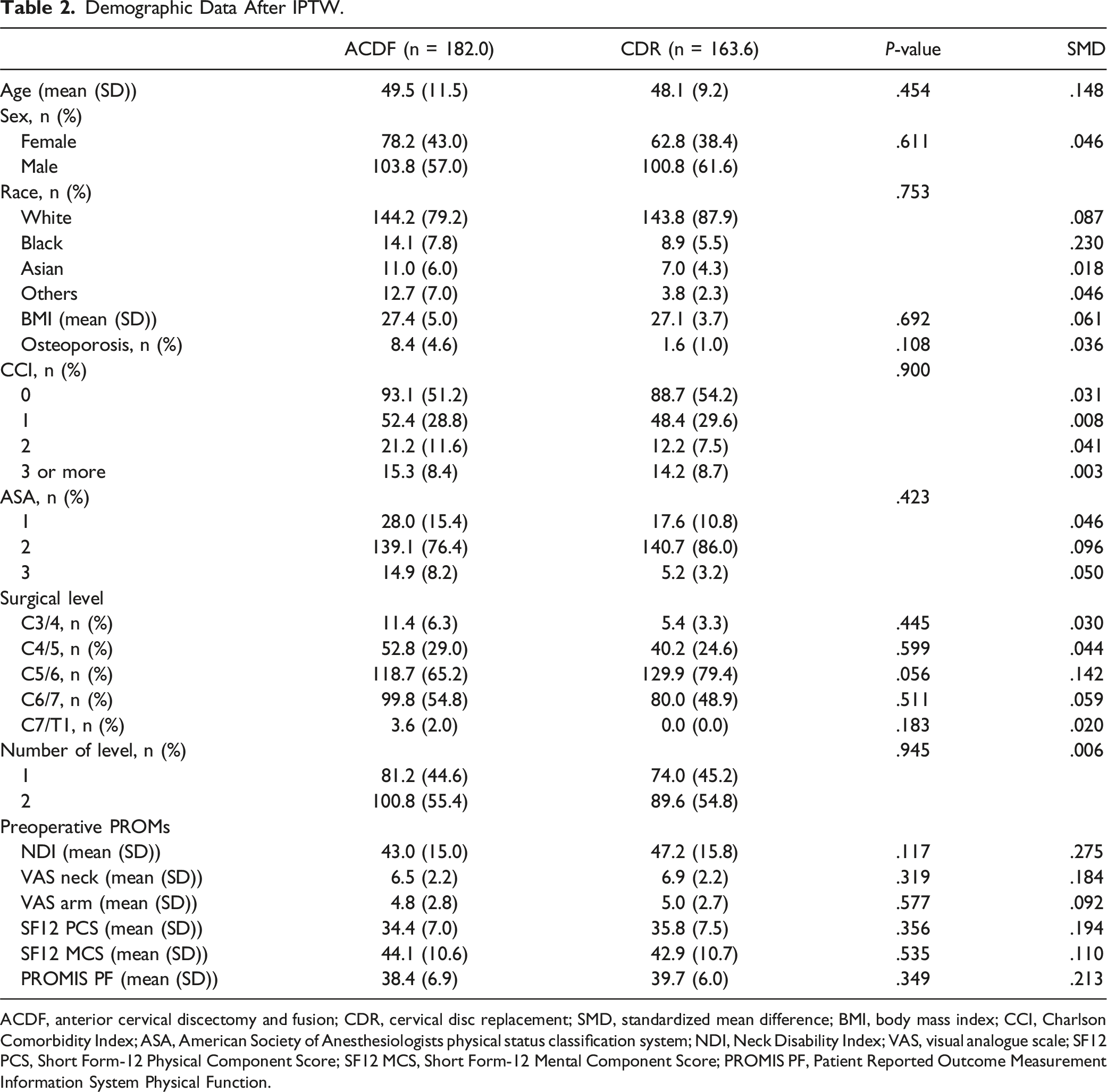
Propensity scores were calculated using age, sex, BMI, CCI, number of levels, and history of osteoporosis. In weighted cohort, propensity scores and each covariate showed the SMD less than 0.2, indicating acceptable balance in background (Figure 1A). The distribution of propensity score also exhibited acceptable balance between the ACDF and CDR groups (Figure 1B). There was no significant difference in background characteristics in the weighted cohort, and the SMD indicated that the groups were well balanced (Table 2). Preoperative background assessment before and after inverse probability of treatment weighting (IPTW). (a): Covariate balance between anterior cervical discectomy and fusion (ACDF) and cervical disc replacement (CDR). Background differences between the groups are expressed as absolute standardized mean differences (SMD). Pink dots represent unweighted cohorts, while green dots represent weighted cohorts after IPTW. The green dots show that all covariates included in the propensity score calculation were adjusted within an acceptable SMD threshold of less than 0.20. (b): Distribution of propensity scores in the unweighted (unadjusted) and weighted (adjusted) cohorts. Dark blue and light blue areas represent the propensity score distribution for ACDF and CDR, respectively. The graph demonstrates sufficient overlap in propensity scores after IPTW, indicating successful adjustment. Demographic Data After IPTW. ACDF, anterior cervical discectomy and fusion; CDR, cervical disc replacement; SMD, standardized mean difference; BMI, body mass index; CCI, Charlson Comorbidity Index; ASA, American Society of Anesthesiologists physical status classification system; NDI, Neck Disability Index; VAS, visual analogue scale; SF12 PCS, Short Form-12 Physical Component Score; SF12 MCS, Short Form-12 Mental Component Score; PROMIS PF, Patient Reported Outcome Measurement Information System Physical Function.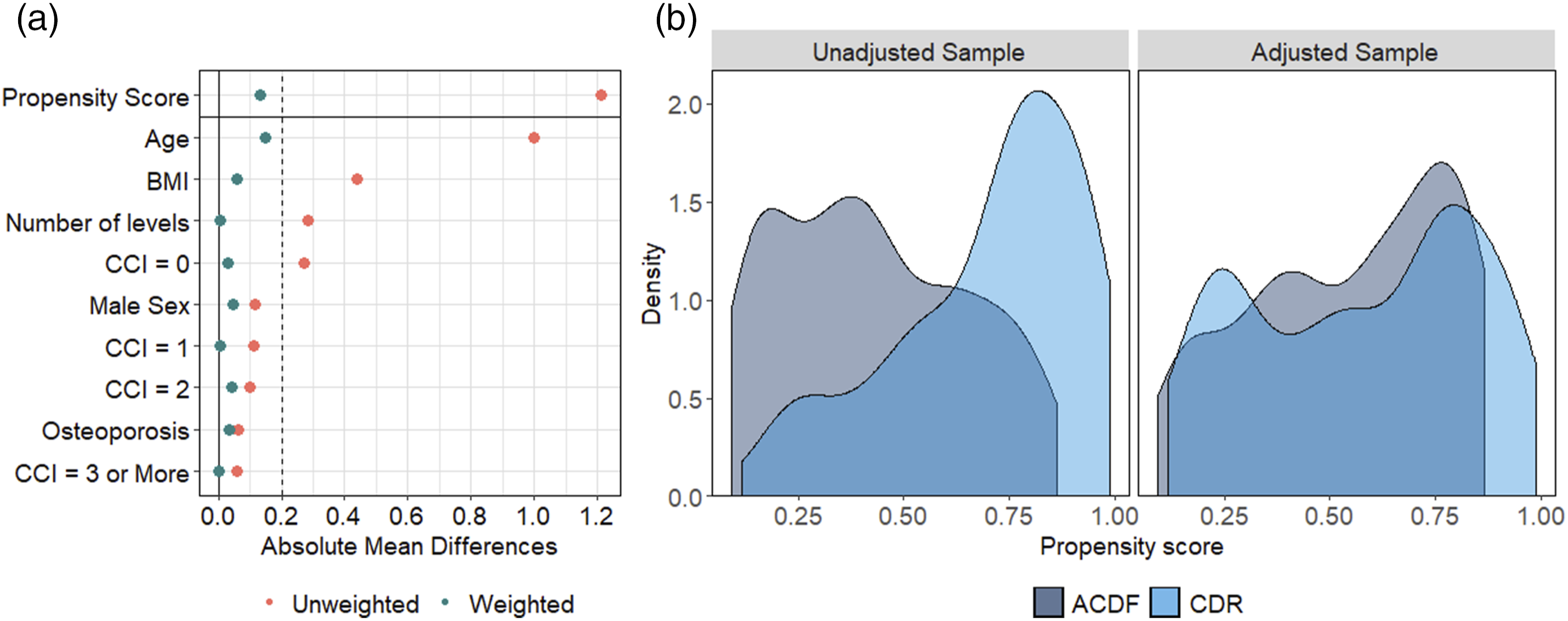
Comparison of PROMs Between ACDF and CDR
Results of Linear Mixed-Effect Models.
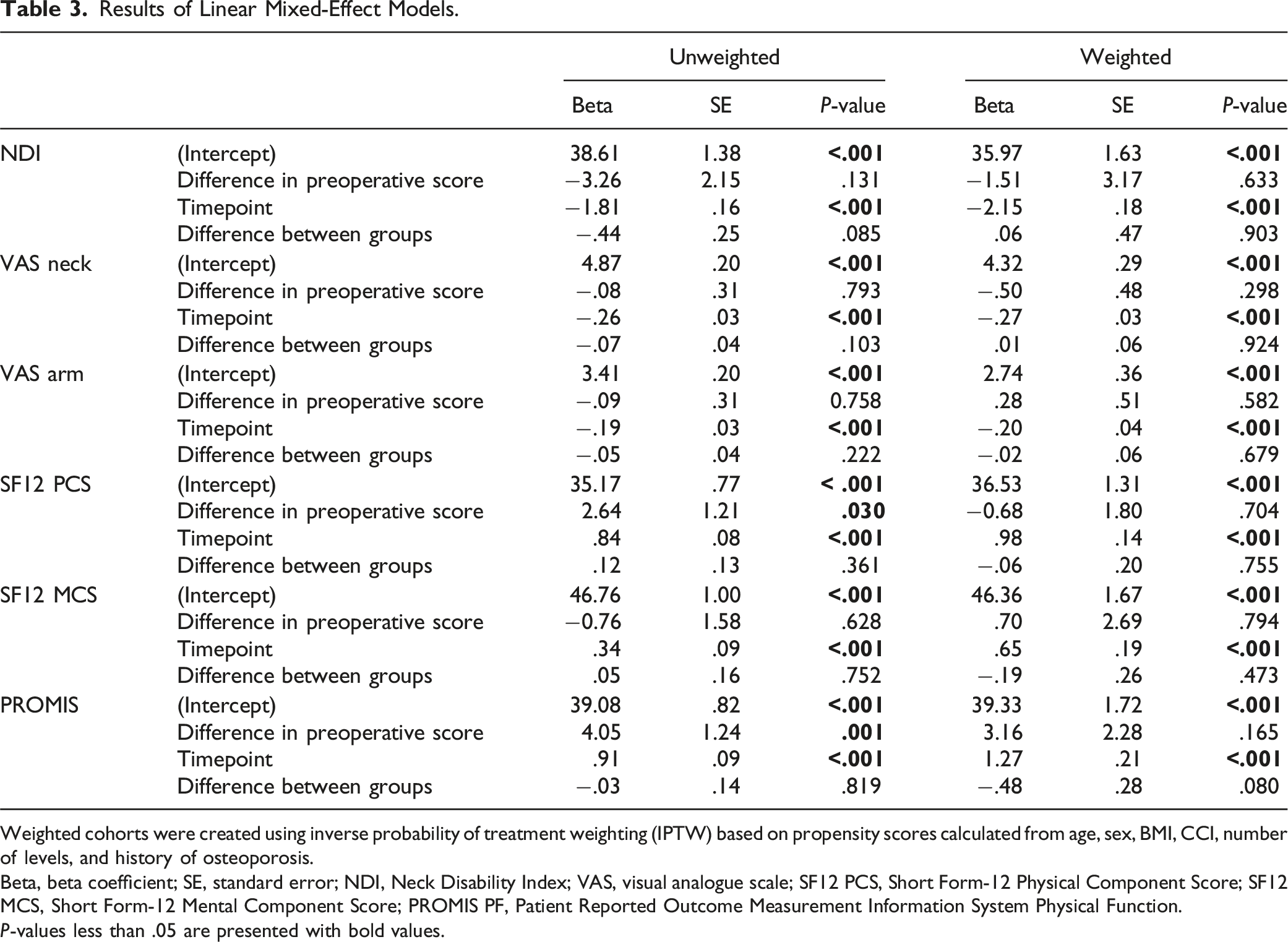
Weighted cohorts were created using inverse probability of treatment weighting (IPTW) based on propensity scores calculated from age, sex, BMI, CCI, number of levels, and history of osteoporosis.
Beta, beta coefficient; SE, standard error; NDI, Neck Disability Index; VAS, visual analogue scale; SF12 PCS, Short Form-12 Physical Component Score; SF12 MCS, Short Form-12 Mental Component Score; PROMIS PF, Patient Reported Outcome Measurement Information System Physical Function.
P-values less than .05 are presented with bold values.
Despite the improvements over time, there were no statistically significant differences between the ACDF and CDR groups across all outcome measures at the 1-year postoperative mark (Table 3, Figure 2). This finding was consistent in both the unweighted and weighted analyses, suggesting that both ACDF and CDR offered comparable outcomes in this patient cohort. For instance, in the Neck Disability Index (NDI), the postoperative difference between groups was not significant (unweighted: β = −.44, P = .085; weighted: β = .06, P = .903). Patient-reported outcomes and measures (PROMs) change up to 1 year postoperatively. In the weighted cohort, no significant differences were found between ACDF and CDR groups in terms of improvement trends, as analyzed by linear mixed-effect models. All PROMs showed significant improvement from baseline to the 1-year postoperative time point in both the ACDF and CDR groups, with no significant differences observed between the two groups. (a): Neck Disability Index (NDI); (b): Visual Analog Scale (VAS) for neck pain; (c): VAS for arm pain; (d): Short Form-12 Physical Component Score (SF-12 PCS); (e): SF-12 Mental Component Score (SF-12 MCS); (f): Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function.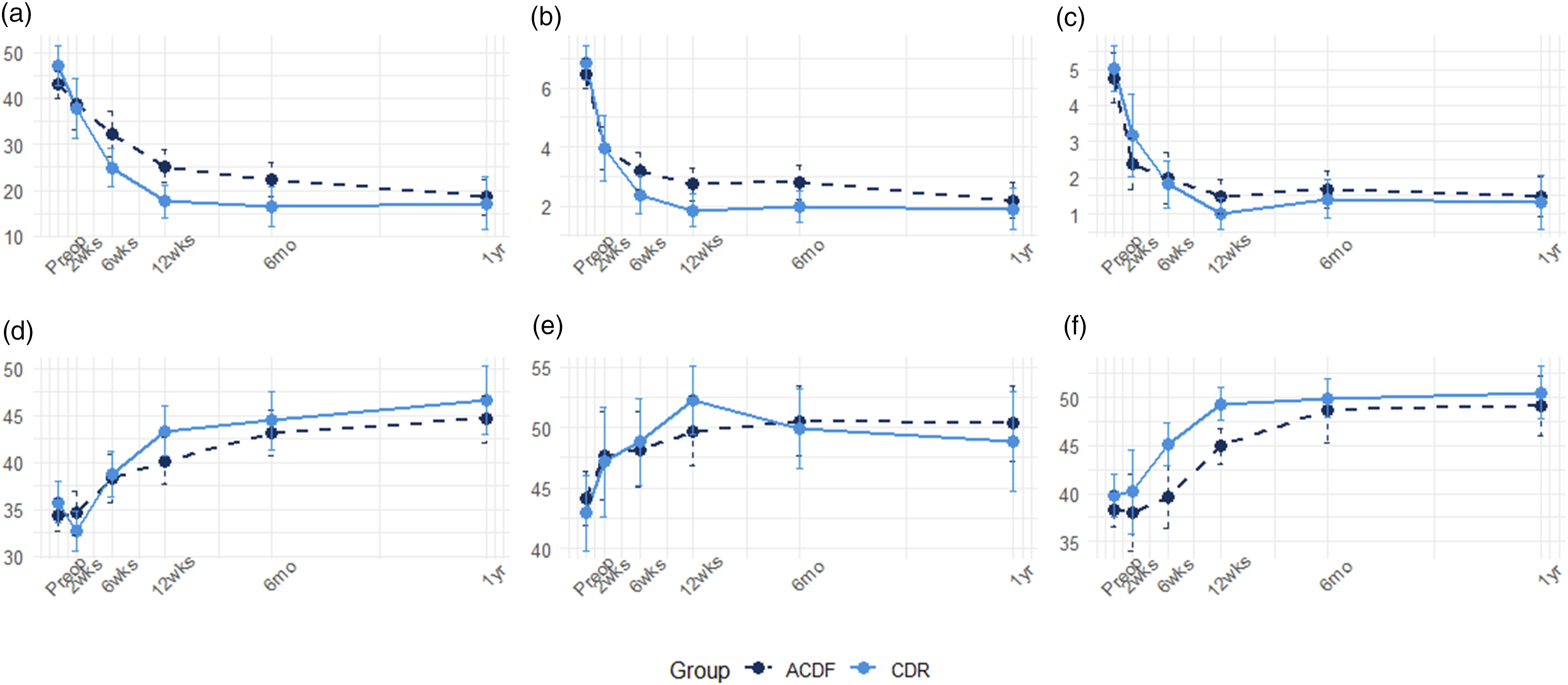
Differences in preoperative PROMs between the groups did not lead to significant postoperative differences in all outcome measures except SF-12 PCS and PROMIS in unweighted cohort (SF12 PCS: β = 2.64, P = .030; PROMIS: β = 4.05, P = .001). There were no significant differences in preoperative PROMs in weighted cohort between the groups. This suggests that initial disparities were effectively balanced after weighting, underscoring the robustness of the propensity score matching and IPTW methods used in this study. The unweighted analysis showed a higher preoperative SF-12 PCS score in the CDR group (β = 2.64, P = .030), but after applying the weighted analysis, this difference was no longer significant (β = −0.68, P = 0.704).
In weighted cohort, NDI at postoperative 1-year timepoint were 19.1 ± 17.3 and 18.8 ± 15.6 in CDR and ACDF, respectively (SMD = .019, P = .931), indicating minimal differences in postoperative NDI at 1-year postoperatively.
Discussion
This study aimed to compare the outcomes of ACDF vs CDR in patients with radiculopathy and predominant neck pain, defined as preoperative neck pain equaled to or exceeded arm pain. We focus on the postoperative improvements in neck pain and disability, comparing outcomes between these two procedures after balancing patient characteristics. We applied IPTW to ensure comparable baseline characteristics between the ACDF and CDR cohorts. Both the unweighted and weighted analyses showed significant improvements in neck pain from the preoperative period to the 1-year follow-up. Importantly, no significant differences were observed in the improvement of neck pain and associated disability. These results underscore the effectiveness of CDR in alleviating neck pain, which was not inferior to ACDF, even in patients traditionally considered less suitable for motion-preserving procedures.
These results should be considered in the context of the evolving surgical guidelines for CDR, which initially imposed strict criteria for its use in FDA trials, excluding patients with severe spondylosis, collapse of the intervertebral disc space, marked instability, and axial neck pain.31,32 Although these criteria were initially strict, the use of CDR is now used more broadly, extending beyond traditional CDR criteria. 33 With these broader indications, recent real-world data suggest that CDR may be effective in a wider range of patients, although further study is needed to validate its use in those with severe neck pain. Case-series studies focusing on either ACDF or CDR have reported improvement in neck pain among patients with predominant neck pain.19-21 However, other studies have identified predominant neck pain as a risk factor of failure to achieve improvement in both ACDF and CDR.23,34 While both procedures have shown some success in alleviating neck pain, this inconsistency highlights the need for more comparative data. Our study contributes valuable comparative data on ACDF and CDR in this patient population, filling a gap in the literature and providing a foundation for future research.
We employed IPTW to balance patient characteristics, a critical part when comparing procedures that may have a slightly different patient selection. Ensuring no significant differences between groups after weighting is crucial for providing accurate insights into the possible indication of CDR. A previous studies comparing ACDF, CDR, and posterior cervical foraminotomy to see the outcomes of neck pain by radiculopathy, the conclusion was limited due to the number of patients included (55 ACDFs, 21 CDRs, and 21 foraminotomies) and its lack of focus on predominant neck pain patients. 22 Furthermore, studies showing faster recovery with CDR compared to ACDF might have been influenced by unbalanced patient backgrounds as CDR is likely to be indicated to younger patients. 20 By using IPTW in our study, we minimized these differences, allowing for a more reliable comparison. Notably, CDR was relatively superior to ACDF in PROMIS scores after weighting without significant difference (Figure 2, Table 3), suggesting that CDR may offer better functional outcomes, particularly in preserving physical function.
Managing predominant neck pain surgically is challenging due to lack of definitive diagnostic modalities. Neck pain can arise from various sources, such as impingement of neural elements, degenerative change in facet joint or intervertebral space, and surrounding soft tissues including ligament and muscles. 5 A systematic review suggested that Modic change at intervertebral disc space was associated with neck pain, although another review is against it.35,36 Additionally, X-ray and computed tomography (CT) have shown poor reliability in diagnosing facet joint pain, whereas bone marrow edema in magnetic resonance imaging (MRI) may offer some diagnostic potential. 37 Both ACDF and CDR address intervertebral degeneration through complete discectomy, but they differ in their impact on segmental motion and the facet joints. Prior biomechanical studies suggested that ACDF may reduce motion at the index level while potentially increasing stress on adjacent segments, where CDR preserves motion but may place greater load on facet joints.38,39 In contrast, CDR preserves motion, which has less impact on the adjacent level, but may exacerbate pre-existing facet degeneration. Differentiating the source of neck pain remains challenging, especially in patients with concurrent radiculopathy. Sclerotomal pain patterns may overlap with facet-mediated or discogenic pain, complicating diagnosis. Radionucleotide imaging, such as SPECT or bone scintigraphy, has shown potential in localizing active degenerative changes and may help distinguish pain generators.40,41 Although these modalities were not used in our study, future prospective research incorporating functional imaging could improve patient selection for surgical intervention.
Inflammation around facet joint caused by segmental motion is closely linked to radicular symptoms, complicating the strict differentiation between radicular and spondylotic neck pain. 38 While medial branch injection offers greater ability to treat facet joint pain than intraarticular injection, it also lacks the ability to definitively separate facet joint pain from radicular pain in patients with cervical radiculopathy. 37 Thus, identifying the source of neck pain improvement after ACDF or CDR remains difficult. Given the significant improvement observed with CDR, spondylotic pain in intervertebral space or radicular pain from nerve impingement could be a source of neck pain in most patients with cervical radiculopathy. Further research is needed to clarify which patients may benefit from facet-targeted interventions, such as facet joint arthrodesis.
There are several limitations to this study. First, the retrospective single-center study design inherently limits the generalizability of our findings and introduces potential selection bias. Although we employed IPTW to mitigate background differences between the ACDF and CDR cohorts, this method can only account for observed confounders. Unmeasured variables, such as patient preference, surgeon experience, and subtle clinical differences, may still influence outcomes and lead to residual bias. While the overall surgical indications followed national standards and defining predominant neck pain was conducted retrospectively, individual surgeon preference inevitably played a role in the choice between ACDF and CDR based on patients’ condition. These preferences may be shaped by factors such as patient characteristics, surgeon-patient communication, insurance coverage, financial considerations, and perceived expectations, all of which are part of real-world clinical decision-making. Although this heterogeneity may limit consistency in treatment indications, it also enhances the generalizability and applicability of our findings to broader clinical practice. Second, age and surgical levels showed residual differences with standardized mean differences over 0.1. Although these differences were statistically notable, the actual mean difference in age was only 1.4 years, which we believe is unlikely to be clinically meaningful. The distribution of surgical levels differed primarily at C5/6, but its impact on postoperative neck pain remains unclear in the current literature. While these residual imbalances may have limited influence on the results, they highlight the inherent limitations of observational studies. Third, the single-center nature of this study means that the results may not be fully applicable to other institutions, although we collected the data from nine surgeons. Forth, it is challenging to distinguish the origin of neck pain with current imaging modalities. We do not collect schematic pain distribution to elucidate if the pain is along with radicular type. Neck pain concurrent with cervical radiculopathy could be radicular, spondylotic (intervertebral joint or facet joint), or a combination of both. Further investigation with advanced imaging techniques may help clarify the source of neck pain and improve patient selection for surgical treatment.
In conclusion, CDR in patients with predominant neck pain was associated with significant improvement in both neck pain and disability, with postoperative outcomes that were not significantly different from those of ACDF. While the differences between the two procedures were minimal in this cohort, our findings suggest that CDR may be a reasonable alternative to ACDF in selected patients with radiculopathy and severe neck pain. These results may help inform clinical decision -making and support the consideration of broader indications for CDR in this context. However, further prospective studies are needed to confirm these findings and refine patient selection criteria.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Companies / Organizations: Globus Medical, Inc.; SpineGuard, Inc.; Stryker K2M; Surgalign; Viseon, Inc.; AMOpportunities; Simplify Medical, Inc.; Minimally Invasive Spine Study Group; LifeLink.com Inc.; Spinal Simplicity, LLC; HS2, LLC; Tissue Differentiation Intelligence Editorial Board / Society Roles: Association of Bone and Joint Surgeons (ABJS); Cervical Spine Research Society (CSRS); International Society for the Advancement of Spine Surgery (ISASS); North American Spine Society (NASS); Society of Minimally Invasive Spine Surgery (SMISS); Lumbar Spine Research Society (LSRS); Annals of Translational Medicine (ATM) – Editorial Board; Contemporary Spine Surgery; Hospital for Special Surgery Journal.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No direct funding was received for this study. However, this study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.
IRB
This study was approved by our instituition’s review board.