
Abstract
Study Design:
Retrospective cohort study.
Objective:
To investigate the relationship between the preoperative width of the intervertebral foramen (WIVF) and the pain relief in patients who underwent anterior cervical discectomy and fusion (ACDF) for the treatment of cervical radiculopathy.
Methods:
Patients were divided into 2 groups based on pain relief status at the 6-month follow-up (pain relief group: 430 patients; persistent pain group: 108 patients). Possible factors such as age, sex, body mass index (BMI), the symptom duration, the preoperative Japanese Orthopedic Association (JOA) scores, the canal stenosis status, and the graft material were obtained. The C2-C7 Cobb angle, disc space, and width and height of the intervertebral foramen were measured on X-ray and CT 3-dimension reconstruction. Multivariate logistic regression was performed to identify the factors that affected pain relief. A receiver operating characteristic (ROC) curve was drawn for the predictive factors to determine the optimal threshold for foreseeing persistent pain.
Results:
There were significant differences in the preoperative WIVF, symptom duration and ratio of disc space distraction between the 2 groups (each P < 0.05). The regression model showed that pain relief was negatively affected by the symptom duration and ratio of disc space distraction. Besides, an increase in the preoperative width of the intervertebral foramen (WIVF) could significantly decrease the possibility of persistent pain. Based on the ROC curve, the optimal threshold of preoperative WIVF was 4.35 mm.
Conclusion:
When the preoperative WIVF is equal to or less than 4.35 mm, the possibility of the occurrence of postoperative persistent pain significantly increased.
Keywords
Introduction
Cervical radiculopathy (CR) is one of the most common causes of neck pain and disability. The reported annual incidence and prevalence of CR are 0.83‰ and 3.5‰ respectively.1,2 Patients presenting with CR usually complain of pain in the neck and one arm, with a combination of sensory loss, motor function loss, or reflex changes in the affected nerve-root distribution. 3 These symptoms mainly result from the foraminal encroachment of spinal nerves due to a combination of factors, including decreased disc height and degenerative changes in uncovertebral joints anteriorly and zygapophyseal joints posteriorly; however, only 20%-25% of cases are caused by herniation of the nucleus pulposus. 4 Although these pathological changes can be eliminated by surgical approaches, the clinical outcomes of surgery for CR can be discrepant.5,6 In appropriate patients, ACDF provides distinct improvements in neural function, but nevertheless, the existence of persistent neck pain or axial neck pain in partial cases is noteworthy. Given that persistent neck pain is detrimental to health-related quality of life, pain relief is a crucial factor that is just as important as improvements in neural function when assessing clinical outcomes after surgery. 7
Patient-reported questionnaires are frequently applied to assess clinical outcomes concerning treatment efficacy and functional disability following spinal surgery. 8 Among these self-rated disability scores in patients with CR, the NDI is extensively recommended as a reliable and validated measure of disability in patients with neck pain.9,10 Although some predictive factors for the NDI have been observed, there is a paucity of research on the issue of the relationship between the preoperative WIVF and NDI scores. 11 Thus, the purpose of the present study is to examine the impact of the preoperative WIVF and height of the intervertebral foramen (HIVF) along with other factors on the NDI at the 6-month follow-up after surgery.
Patients and Methods
Participants
After ethics committee approval was obtained, patients aged between 20 and 70 years old who underwent 1- or 2-level ACDF (C3 to C7) for CR from September 2016 to September 2019 were reviewed. The inclusion criteria for ACDF were patients whose radiculopathy symptoms predominantly caused by intervertebral disc protrusion or osteophytes from the vertebral body or uncovertebral joint. The symptoms were consistent with radiograph findings. We excluded patients with a history of cervical spine surgery, previous spinal trauma, inadequate decompression detected on MRI at the 4-month follow-up, no fusion at the 6-month follow-up, or anyone who could not complete the NDI questionnaire. A total of 538 patients with a minimum of 6 months of follow-up were enrolled (Table 1).
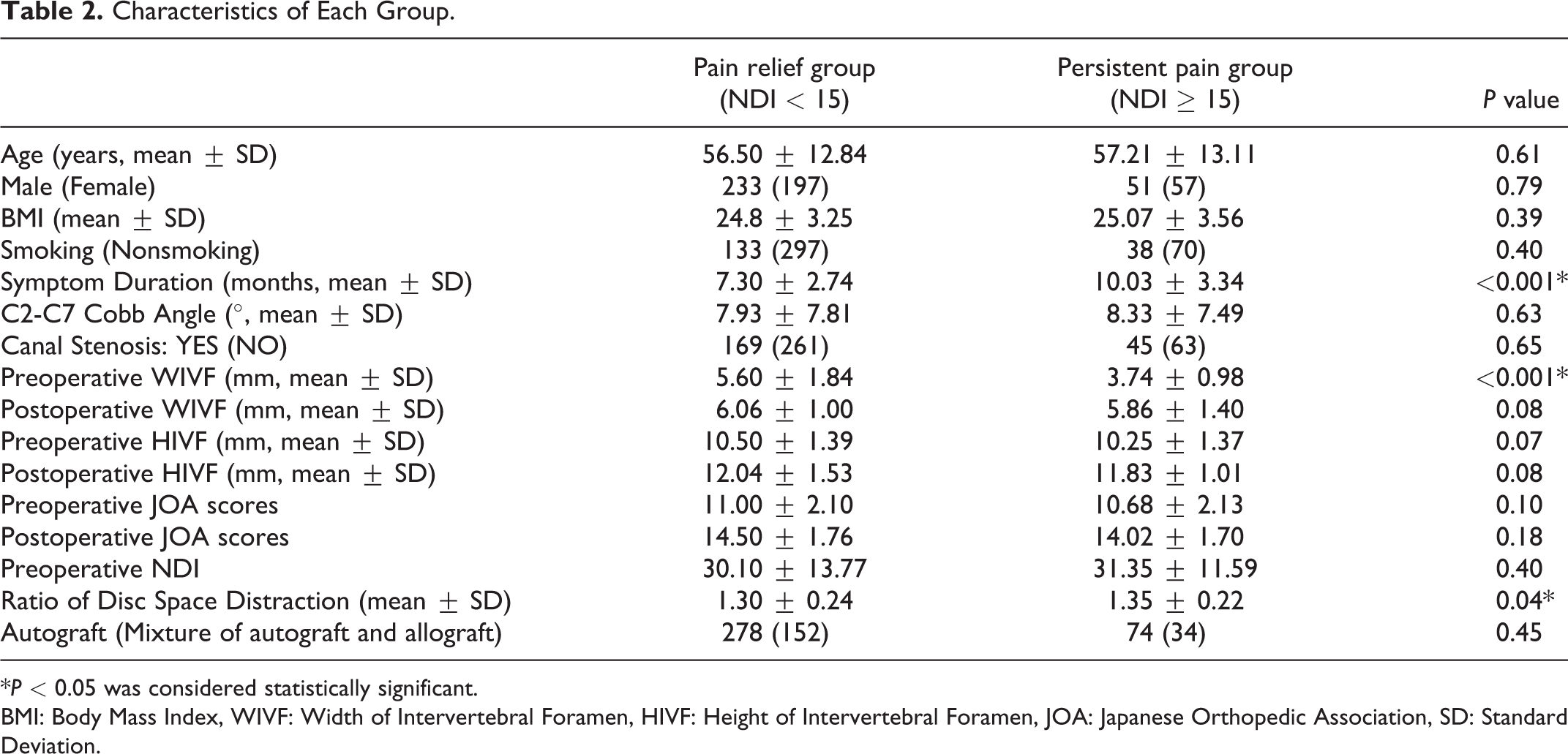
The Baseline Data of the Enrolled Patients.
BMI: Body Mass Index, WIVF: Width of Intervertebral Foramen, HIVF: Height of Intervertebral Foramen, JOA: Japanese Orthopedic Association, NDI: Neck Disability Index, SD: Standard Deviation.
Surgical Approach
All ACDFs were performed in our orthopedic spine department by 2 experienced professors following a standard anterior procedure. After the appropriate level was confirmed, a Casper distractor was used to obtain adequate space to perform the discectomy. To avoid excessive distraction of the disc space, the deep distractor was properly used, while sufficient decompression space could not be supplied by using the Casper distractor. The posterior longitudinal ligament was fully removed to ensure that the decompression was complete. After removing the osteophytes from the intervertebral foramen, a nerve root hook was applied to explore the canal of the intervertebral foramen so that ascertaining the decompression of the uncinate process osteophytes was adequate. Following sufficient discectomy and endplate preparation, the appropriate interbody cage filled with bone graft material was packed into the center of the intervertebral space. The plates and fusion materials included Skyline (Johnson and Johnson Co., Depuy Spine Ltd., Ryhamn, MA) and Elite plates (Medtronic Sofamor Danek Inc., Memphis, TN). All patients were suggested to wear a Philadelphia collar for no more than 2 weeks after the operation. The MRI was performed to confirm the decompression status at the 4 months follow-up.
Clinical Parameters and Analysis
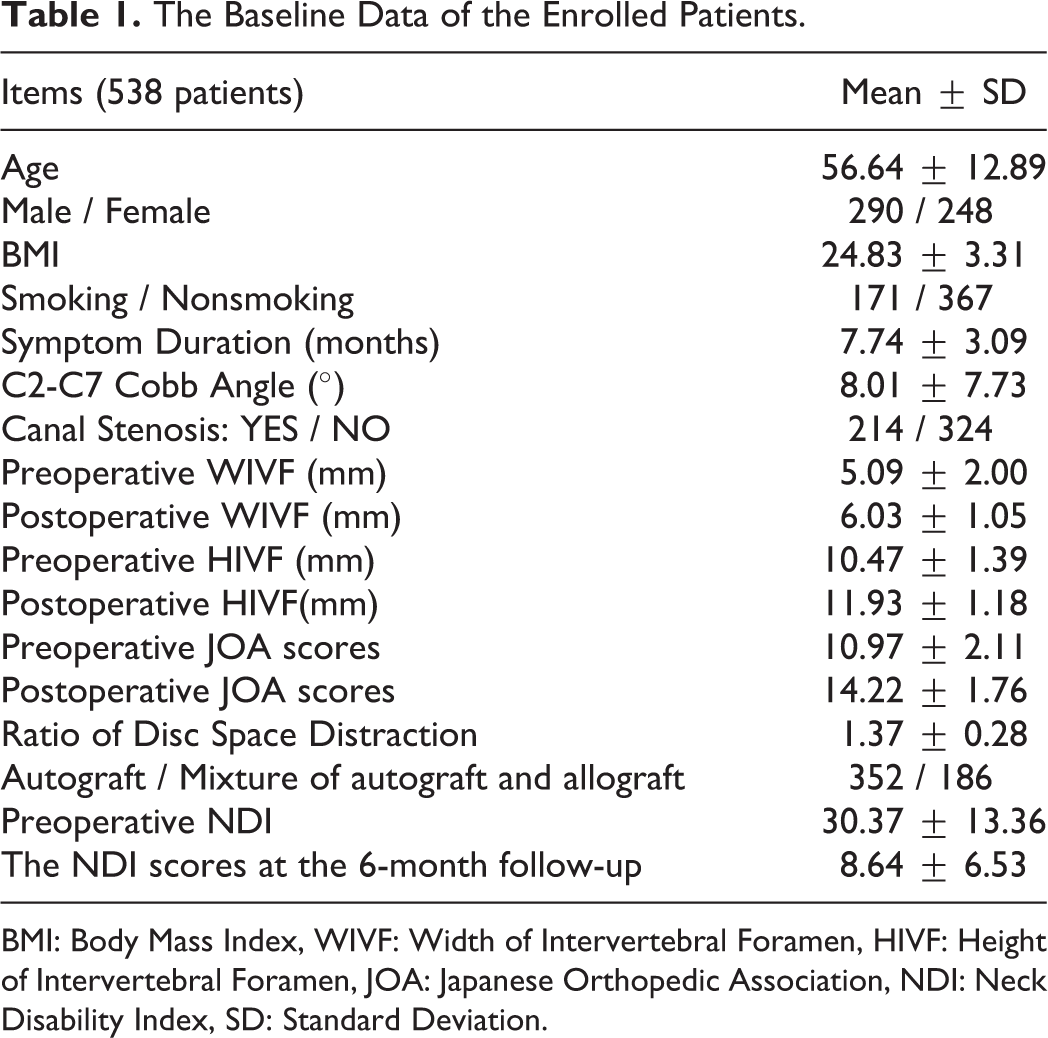
We accounted for several independent variables including age, sex, BMI, current smoking status, symptom duration, the preoperative C2-C7 Cobb angle, the JOA scores and the canal stenosis status before surgery, the preoperative WIVF and HIVF, and the postoperative ratio of disc space distraction. The postoperative WIVF and HIVF were also measured to confirm the intervertebral foramen spurs were utterly addressed. The WIVF and HIVF were measured with a CT 3-dimension reconstruction to minimize the bias of measurement accuracy (Figure 1). 12 The disc space was measured by X-ray, and the ratio of disc space distraction was equal to the postoperative intervertebral space/preoperative intervertebral space, which was calculated by 2 residents (Figure 2). We also included the type of bone graft. We used NDI to assess pain status. The patients were divided into 2 categories based on whether the NDI score was less than 15 at the 6-month follow-up. One group contained patients with NDI scores less than 15, and the other group included patients with NDI scores greater than or equal to 15. An independent t-test or chi-squared test was used to identify significant differences between the groups. Then, we corrected for a number of independent variables in the multivariate logistic regression analysis, which contained the symptom duration, preoperative WIVF and HIVF, and postoperative ratio of disc space distraction. After that, a receiver operating characteristic (ROC) curve was used to determine the optimal threshold of the prognostic factors for predicting postoperative NDI scores. The value corresponding to the optimum Youden index was the targeted value.
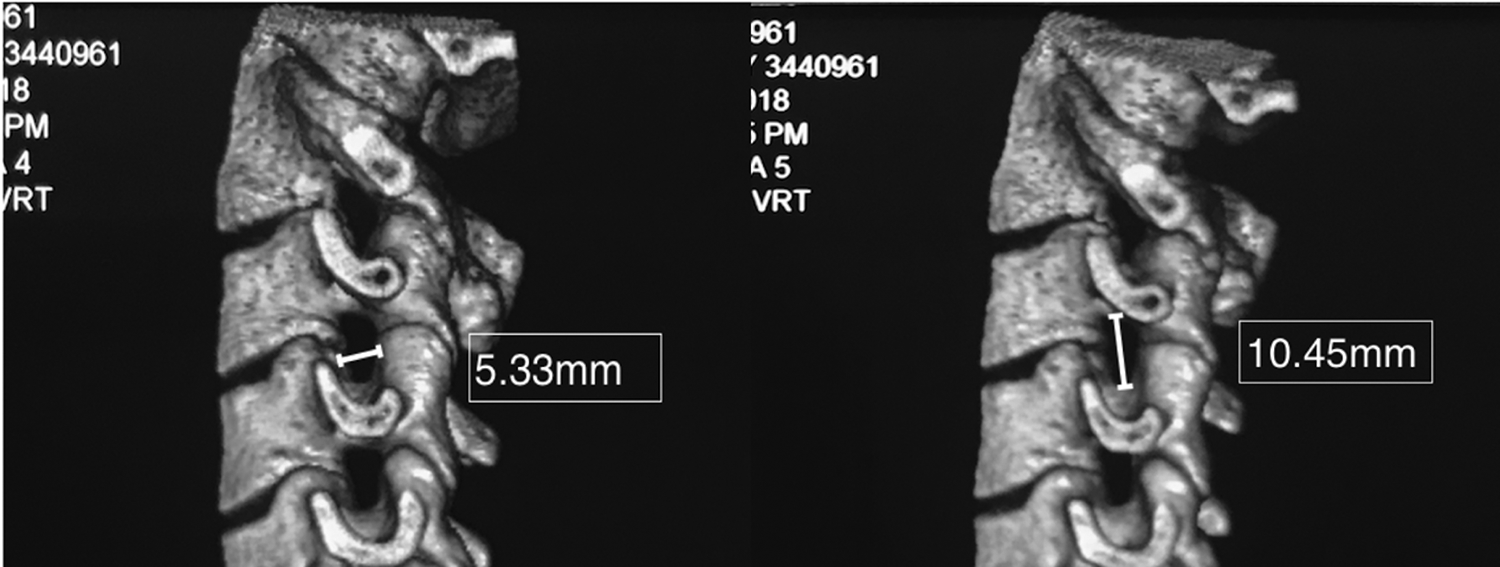
Diagram of WIVF and HIVF assessed by CT 3-dimension reconstruction. The width was defined from the anterior medial zone of the superior vertebrae to the posterior medial zone of the inferior vertebra. The height was defined as the distance between the middle medial zone of adjacent vertebra. WIVF: Width of Intervertebral Foramen, HIVF: Height of Intervertebral Foramen.
Diagram of disc space distraction ratio, the ratio was equal to postoperative intervertebral distance/preoperative intervertebral distance. In this case, the ratio was 6.8/5.4 = 1.26.
Statistical Method
Data were analyzed by using the SPSS version 20 software package (IBM SPSS Statistics 20.0, IBM Corporation, Armonk, NY). A P value < 0.05 was considered statistically significant.
Results
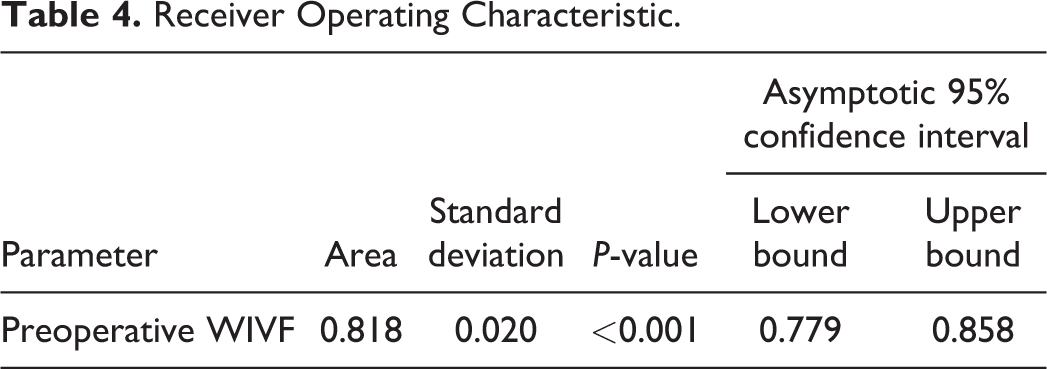
A total of 538 patients were enrolled in this study, and the baseline characteristics are shown in Table 1. A total of 430 patients reported NDI scores of less than 15 in the pain relief group; 79.9% of the patients enrolled achieved acceptable pain relief. In contrast, 108 patients with NDI scores higher than or equal to 15 were included in the persistent pain group. 20.1% of the patients in this study still complained of chronic pain at the 6-month follow-up. There were no significant differences in age, sex, BMI, current smoking status, the preoperative C2-C7 Cobb angle, the JOA scores and the canal stenosis status before surgery, the preoperative HIVF between the 2 groups, or the postoperative WIVF and HIVF. However, the preoperative WIVF in the persistent pain group was significantly lower than that in the pain relief group (P < 0.05). In addition, there were significant differences in the symptom duration and the ratio of disc space distraction between the 2 groups (each P < 0.05, Table 2). Although there was no significant difference in the preoperative HIVF, considering that the HIVF is a common parameter for gauging the intervertebral foramen, we still included it in the multivariate logistic regression model. After analyzing the variables, there was no significant association between the preoperative HIVF and postoperative pain relief. However, the analysis showed that symptom duration (OR = 1.169, 95% CI: 1.076-1.269) and the ratio of disc space distraction (OR = 6.063, 95% CI: 2.319-15.853) were negatively associated with pain relief. In addition, the preoperative WIVF (OR = 0.555, 95% CI: 0.467-0.660) was a significant predictor correlated with pain relief (Table 3). Based on the ROC curve, the preoperative WIVF corresponding to the optimal Youden index (0.623) was 4.35 mm (sensitivity 0.870, specificity 0.753). Thus, if the preoperative WIVF was equal to or less than 4.35 mm, the possibility of postoperative persistent pain would increase (Figure 3, Table 4).
Characteristics of Each Group.
*P < 0.05 was considered statistically significant.
BMI: Body Mass Index, WIVF: Width of Intervertebral Foramen, HIVF: Height of Intervertebral Foramen, JOA: Japanese Orthopedic Association, SD: Standard Deviation.
Factors Associated With Pain Relief at 6-Month Follow Up (Multivariate Logistic Regression).
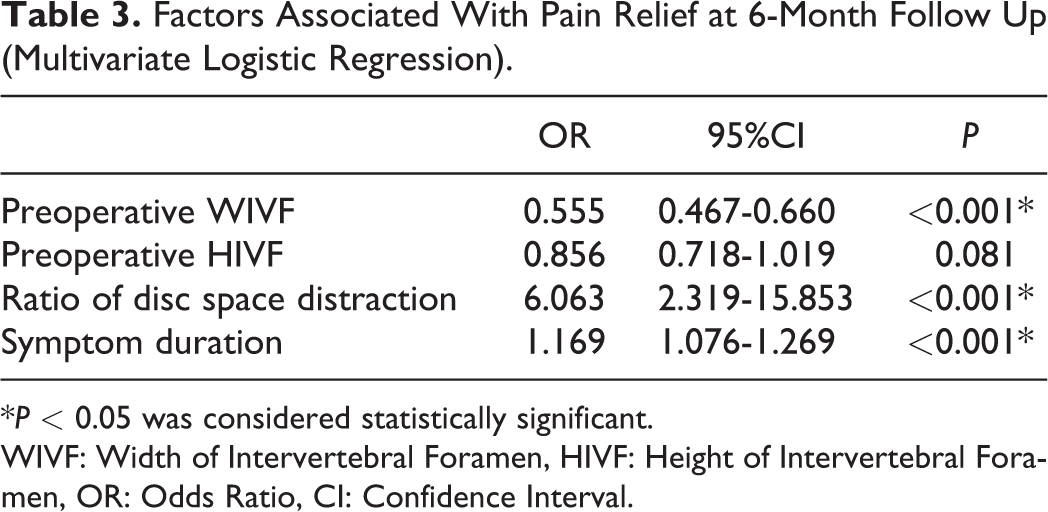
*P < 0.05 was considered statistically significant.
WIVF: Width of Intervertebral Foramen, HIVF: Height of Intervertebral Foramen, OR: Odds Ratio, CI: Confidence Interval.
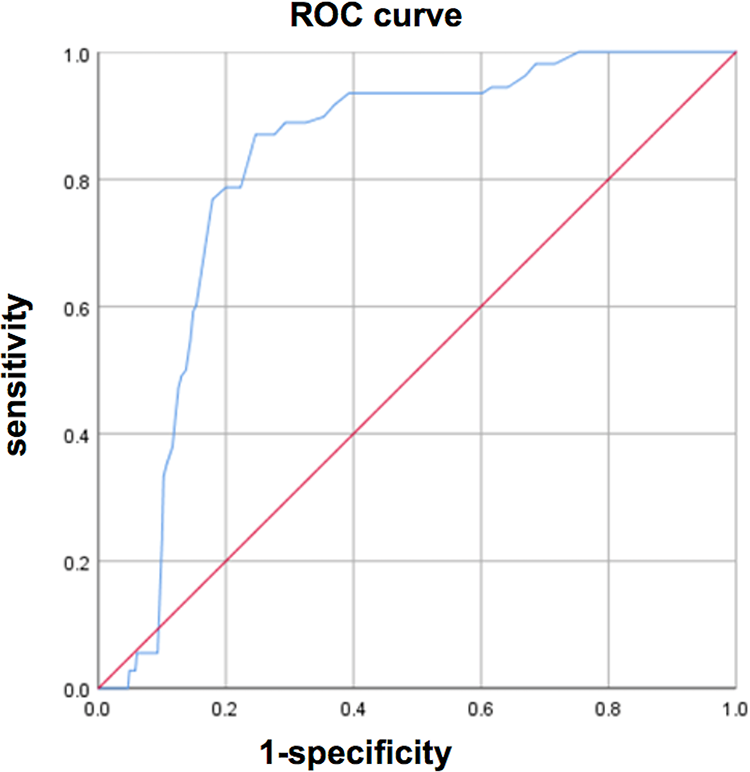
Receiver operating characteristic (ROC) curve.
Receiver Operating Characteristic.
Discussion
The NDI is a validated outcome measurement tool for assessing self-rated disability in patients with neck pain, especially in cervical radiculopathy patients and whiplash patients. 13 However, the current category values of the NDI for illustrating the degree of pain recovery is variable. Nevertheless, Nederhand et al. and Bono et al. indicated that the cut-off NDI value of 15 (0-14 vs 15-) was strongly correlated with outcome at 6 months.14,15 Thus, based on the NDI scores at the 6-month follow-up, we included 430 patients in the pain relief group, and the others were included in the persistent pain group. According to a previous study, major symptoms, such as neck pain or arm pain caused by nerve root irritation, can be relieved by 4∼6 months after ACDF. 16 In our study, nearly 80% of patients had achieved significant pain alleviation, but 20% of patients still complained of disability with neck pain or arm pain. The surgical outcome of cervical radiculopathy was similar to others’ results. 17
The most important finding in the present study was that the preoperative WIVF was significantly associated with pain relief after ACDF. Since the WIVF is an important factor for gauging the intervertebral foramen stenosis status before surgery, oblique X-ray and CT scans are widely used to observe whether the canal of the nerve root is narrow or not. However, the grade of cervical foraminal stenosis is not clearly defined. Kadish and his colleagues found that although some patients had an excessive formation of uncinate process osteophytes, these patients might not present with any clinical symptoms. In other words, only if the foraminal stenosis is severe to an extent should pathological changes be addressed. To our knowledge, this is the first study to evaluate the relationship between preoperative WIVF and clinical outcome. According to the predictive threshold based on preoperative WIVF values, our study demonstrated that if the value was equal to or less than 4.35 mm, persistent pain would be more likely to occur. In contrast, when the preoperative WIVF was over 4.35 mm, the possibility of persistent pain dramatically decreased. First, a previous study found that the average bony foraminal width and height were 6-7 mm and 8-11 mm, respectively. 12 However, the nerve root only consumes less than 30% and 50% of the available width and height of the intervertebral foramen in the neutral position, and the proportion of nerve tissue in the entire intervertebral foramen is only approximately 2%-35%. 18 Despite the existence of soft tissue, there is still adequate space for the nerve root. 19 Even though foraminal decompression has to be performed in some cases, there is some extra space to address herniated discs and osteophytes, avoiding the irritation of nerve roots in some patients whose preoperative WIVFs are greater than 5 mm. Second, the average width of nerve roots is approximately 2 mm, but the average width of dorsal ganglia is nearly 4 mm. 12 Therefore, decompressing the intervertebral foramen with a Kerrison rongeur when patients’ preoperative WIVF is no more than 4 mm is highly likely to exacerbate the irritation of the spinal dorsal ganglion (Figure 4). In addition, for these patients, the WIVF might not be broadened as significantly as the HIVF after cage insertion. These might be the reasons why postoperative persistent pain likely exists in patients whose WIVF is less than 4 mm. In our experience, using an ultrasonic bone curette is suggested to decompress nerve root canal osteophytes, or complete uncinate process resection from the anterior approach is recommended under this circumstance.
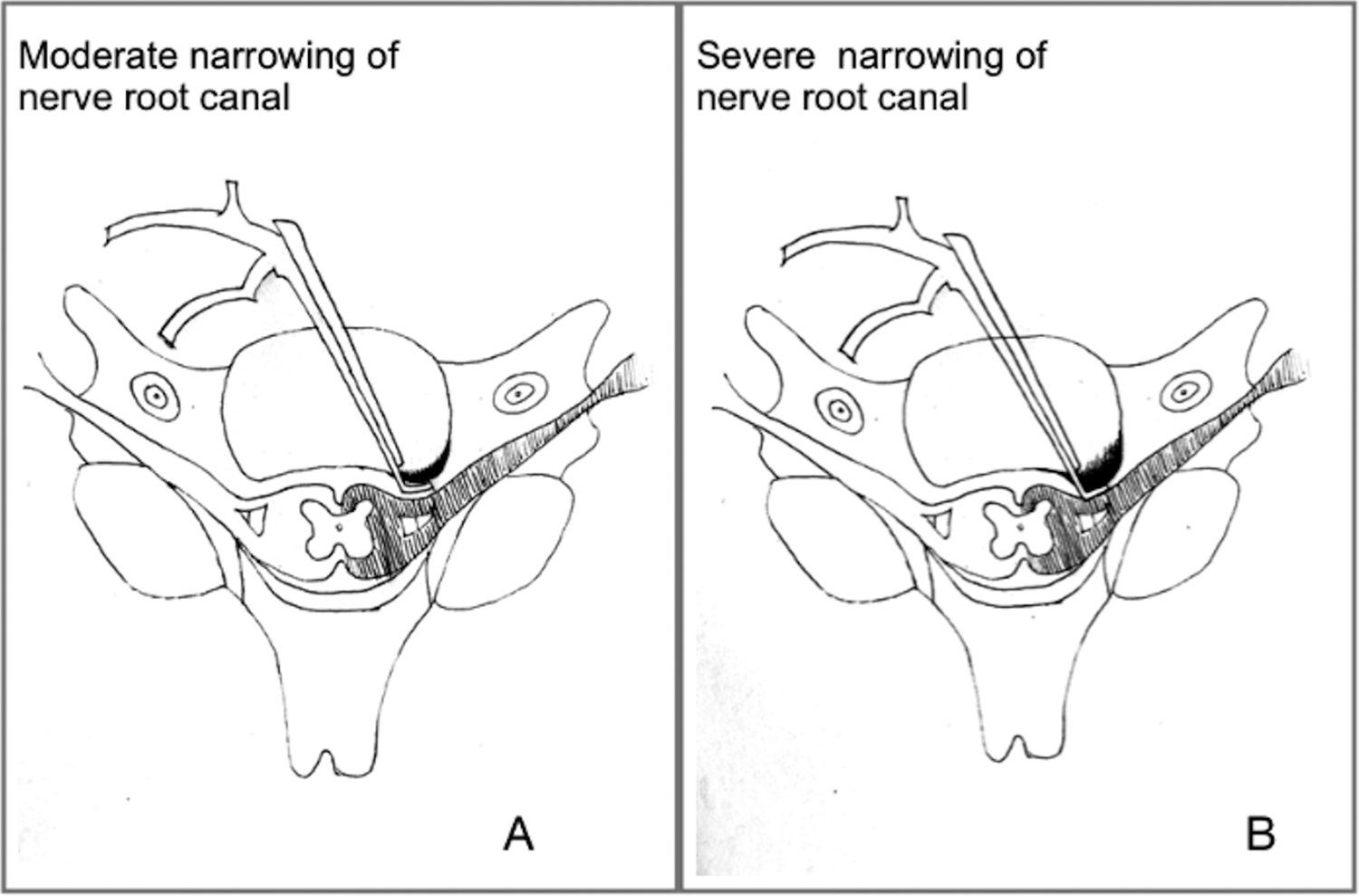
Illustrations showing how preoperative WIVF influence surgical procedures. A, We considered that it was much safer to address the nerve root canal when preoperative WIVF was over 4 mm because there was still adequate space for decompression. B, For those patients whose preoperative WIVF were less than 4 mm was considered as severe narrowing, decompression by the Kerrison rongeur was more likely to bring on iatrogenic injury.
Another finding was that both the symptom duration and ratio of disc space distraction were negatively correlated with pain relief. However, the current study found mixed results regarding the effect of symptom duration on outcome. One study indicated that patients with less than 6 months of symptoms presented with greater relief of arm pain but no differences in NDI scores. 20 In contrast, a previous study concluded that a longer symptom duration negatively affects health-related quality of life (HRQL) after surgery for cervical radiculopathy, especially when the symptom duration is more than 2 years. 21 In this research, the number of patients was much greater and the average symptom duration was greater than those in previous studies. Thus, the present study further suggested that a longer preoperative symptom duration could also negatively impact pain relief.
The ratio of disc space distraction was found to be another predictive factor negatively impacting pain relief. Inappropriate cage insertion can lead to excessive disc space distraction, which might cause neck pain due to an increasing load on the facet joint capsule.22,23 Furthermore, excessive disc space distraction has been suggested as a risk factor for the development of radiographic adjacent segment degeneration (ASD). 24 Based on our analysis (OR = 6.063, 95% CI: 2.319-15.853), we highly suggest that cages should be selected cautiously to avoid excessive distraction. In our experience, the postoperative ratio of disc space distraction should not exceed 1.5.
The current study is not without limitations. First, this is a retrospective study, and it is, therefore, subject to all the inherent biases in this study design. Specifically, it is unable to account for some confounding factors such as various procedures of physical therapy, psychosocial determinants, and other variables that may influence the NDI score. Besides, some postoperative factors, such as the application of drugs, working pressure, and other potential factors that may affect self-rated disability scores, were not included. However, this article aims to illustrate the relationship between the preoperative intervertebral foramen parameter and postoperative pain relief instead of showing all the variables that may affect NDI. Second, all procedures were performed by 2 surgeons under the supervision of a well-experienced professor at an individual academic institution, which may limit the generalizability of the results undergoing ACDF. The third limitation is that the period of follow-up is only 6 months. Although most of the patients achieved significant pain relief after surgery within 6 months, the longer follow-up period may provide better evidence that explain the impact of WIVF on persistent pain.
Conclusion
According to the current study, we suggest that the preoperative WIVF is a predictive factor associated with pain relief. However, when the foraminal width is equal to or less than 4.35 mm, the possibility of postoperative persistent pain palpably increases. In addition, the symptomatic duration and ratio of disc space distraction might negatively influence postoperative pain relief. Age, sex, BMI, current smoking status, the preoperative C2-C7 Cobb angle, the canal stenosis status, the graft material, and the preoperative HIVF are not significantly related to pain relief.
Footnotes
Authors’ Note
Baifeng Sun, MD, Chen Xu, PhD, and Min Qi, MD, contributed equally to this work. This study was approved by ethics committee (Changzheng Hospital, Second Military Medical University; IRB number: 13 071 002 114). Each author certifies that the institution approved the human protocol for this investigation and that all written informed consent was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the (82072471, 81 772 392, 81972090, 81 871 802, 81 772 376, 81 702 225), Shanghai Rising-Star Program (20QA1409200), Shanghai Education Development Foundation and Shanghai Municipal Education Commission “Shu Guang” Program (17SG35), “Chen Guang” Program (17CG36) and Shanghai “Rising Stars of Medical Talent” Youth Development Program.