
Abstract
Study Design
Retrospective Cohort Study.
Objective
This study examines the consistency of Vertebral Bone Quality (VBQ) and Computed Tomography Hounsfield Units (CT HUs) with Dual-energy X-ray absorptiometry (DXA) as a reference standard, evaluating the diagnostic performance of these 2 imaging techniques across different age groups and genders. Particular attention is given to the applicability of VBQ in different age and gender cohorts.
Methods
We included 972 eligible patients, from which 569 patients were randomly selected and included in the analysis according to the inclusion criteria. These patients underwent lumbar Magnetic Resonance Imaging (MRI), lumbar CT, and DXA within 3 months of hospital admission. The study assessed the correlation and diagnostic efficacy of these techniques in measuring lumbar and femoral neck bone mineral density (BMD).
Results
It showed good correlation between VBQ and CT HUs with DXA in individuals under 70 years of age. However, in the population over 70 years, the correlation of VBQ with DXA significantly decreased (lumbar BMD pr = −.145 P > .05; femoral neck BMD r = −.097 P > .05), whereas CT HUs maintained high diagnostic performance. The ROC curve analysis indicated that the AUC for differentiating osteoporosis (based on lumbar spine BMD) by VBQ was .545 in males over 70 and .487 in females over 70. However, CT HUs demonstrated diagnostic performance across all groups.
Conclusion
VBQ is effective in assessing osteoporosis in patients under 70 but shows decreased efficacy in those over 70. When using VBQ to predict osteoporosis in patients on opportunistic grounds, it is still necessary to incorporate additional reference indicators, such as CT HUs.
Introduction
Osteoporosis is a metabolic bone disease that significantly affects the elderly population worldwide, particularly among women, where the incidence increases markedly with age. 1 In China, the prevalence of osteoporotic fractures among the elderly is 18.9%, with fracture rates increasing with age. 2 The central Dual-energy X-ray absorptiometry (DXA) of the hip and lumbar spine remains the recognized method for bone mass assessment. 3 However, due to additional economic burdens and radiation exposure, as well as potential inaccuracies in bone mineral density (BMD) and T-scores measured by DXA due to conditions like spinal scoliosis, lumbar spondylosis, or abdominal aortic calcification,4-7 alternative measurement methods are needed for osteoporosis screening.
Previous studies have shown that vertebral Tomography Hounsfield Units (CT HUs) obtained from existing CT scans can serve as a supplementary method for measuring bone density and have been proven to correlate positively with BMD.8-10 The Vertebral Bone Quality (VBQ) is a method for evaluating vertebral bone quality based on Magnetic Resonance Imaging (MRI), 11 which considers the decline in trabecular bone quality and increase in fat infiltration in osteoporosis patients by measuring the T1 signal in lumbar MRI and normalizing it against the cerebrospinal fluid at the L3 level. Several studies have indicated that VBQ is a valuable diagnostic tool for osteoporosis and significantly correlated with BMD values.12-14
Although previous studies have shown the potential of VBQ and CT HUs in identifying osteoporosis, these studies typically utilized smaller sample sizes or did not differentiate between age groups, thus limiting their general applicability and statistical significance. Therefore, this study aims to comprehensively assess the consistency of these imaging parameters with the DXA standard and their diagnostic efficacy in clinically diagnosing osteoporosis by broadly collecting data across different age groups, and we aim to determine whether VBQ is a reliable predictor of osteoporosis regardless of age or gender.
Methods
Subjects
This retrospective study evaluated 1735 lumbar spine surgery patients admitted to our hospital for lumbar degenerative diseases between January 2018 and June 2023. These patients underwent lumbar MRI, lumbar CT, and DXA measurements within 3 months of admission. Exclusion criteria included: (1) patients under the age of 18; (2) abnormalities at the L1-L4 level such as a history of vertebral fractures, infections, tumors, scoliosis, ankylosing spondylitis or any instrumentation in the lumbar spine; (3) patients with other metabolic bone diseases such as hyperparathyroidism, diffuse idiopathic skeletal hyperostosis; (4) history of osteoporotic fractures; (5) MRI study relaxation times (TR and TE) not within the optimal range for marrow assessment (TR = 400-850 ms, TE = 8-20 ms); (6) insufficient image quality or inability to measure lumbar VBQ. In total, 972 patients met the inclusion criteria. The patients were divided into 5 groups according to age: under 40, 40-49, 50-59, 60-69, and 70 years and older. There were fewer patients under 40 years old, totaling 90. To avoid a large disparity in the number of patients between the first group and the others, 120 patients who met the inclusion criteria were randomly selected from each of the remaining groups. (Diagram depicting the flow of patients shown in Figure 1). Diagram depicting the flow of patients included in the study.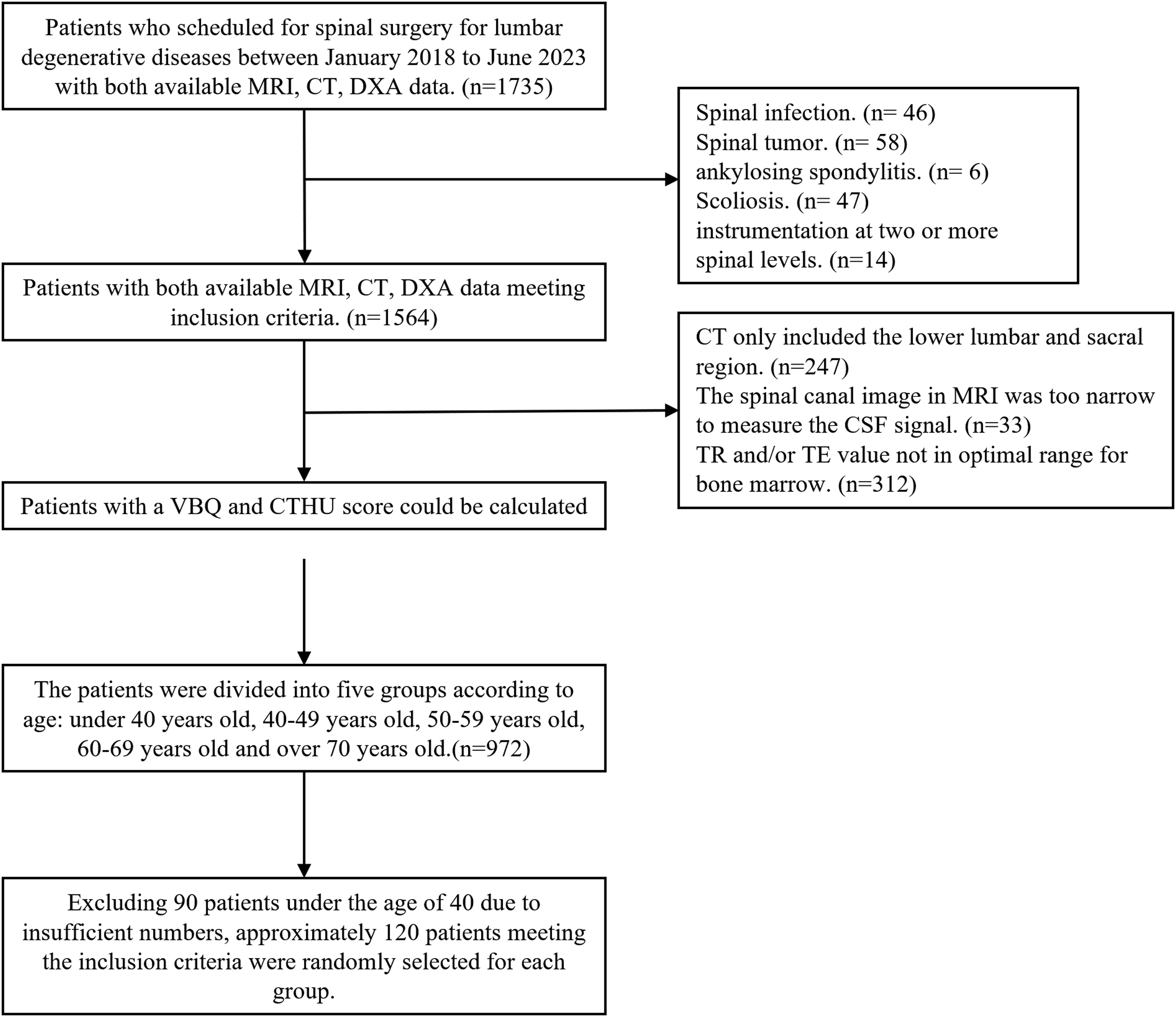
VBQ Measurements
Patients underwent non-contrast imaging using a 1.5 Tesla MRI scanner. All images were transmitted to the computer in DICOM format and evaluated and analyzed using PACS software. T1WI non-enhanced lumbar images were used for VBQ measurement by placing a circular ROI in the medullary part of the vertebral bodies from L1 to L4 and in the CSF space at the L3 level on the midsagittal T1-weighted MRI image. If prominent venous plexuses or hemangiomas were observed on the midsagittal image, ROIs were selected on parasagittal slices, and if terminal inflammation was present, the ROI was appropriately reduced to avoid the inflamed area. When nearly all sagittal slices showed abnormalities, that segment was excluded from the study. If spinal stenosis was prominent in the L3 segment, CSF measurement was taken above or below the next possible segment (L2 or L4). The median SI of the L1-L4 vertebrae was calculated and then divided by the average signal intensity of the CSF from L1 to L3 to obtain the patient’s VBQ11,15:

VBQ measurement is shown in Figure 2. ROIs drawn on each vertebral body and the L3-CSF to generate values for VBQ calculation.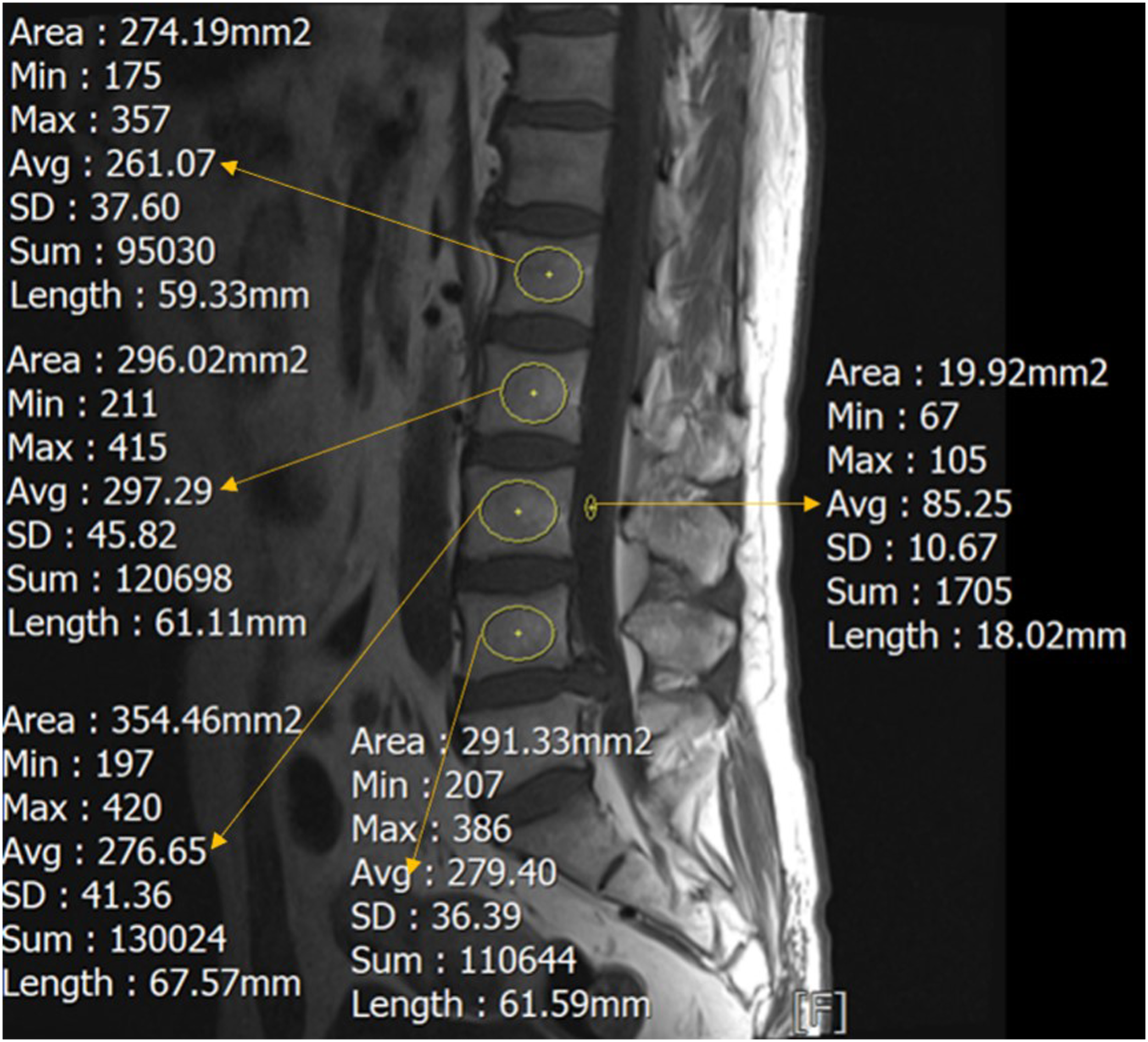
HUs Value Measurements
HUs value was measured on lumbar CT using the ROI tool in the PACS software. When an ROI was placed at any location on the CT image, the software automatically calculated the average HUs of the selected area. It is important to note that the window setting of the CT image does not affect the average HUs. HUs value was measured at 3 independent locations on each vertebra (below the upper endplate, in the middle of the vertebrae, and above the lower endplate), expanding the ROI as large as possible but limiting it to the cancellous bone area to minimize the influence of cortical bone and avoiding areas with posterior veins and bone spurs. If terminal inflammation was present at any location, that position was excluded from the study. The HUs value for each vertebra was the mean of the HUs values at the 3 independent locations. The average lumbar HUs was the mean HUs from L1 to L4.
CT Hus measurement is shown in Figure 3. (1A)-(4C): An ROI was drawn in the cancellous region of the vertebral body, avoiding the cortical and vascular areas of the bone. Ave, average; max, maximum; min, minimum. (D): HUs were measured for the upper, middle and lower each vertebral body from L1 to L4.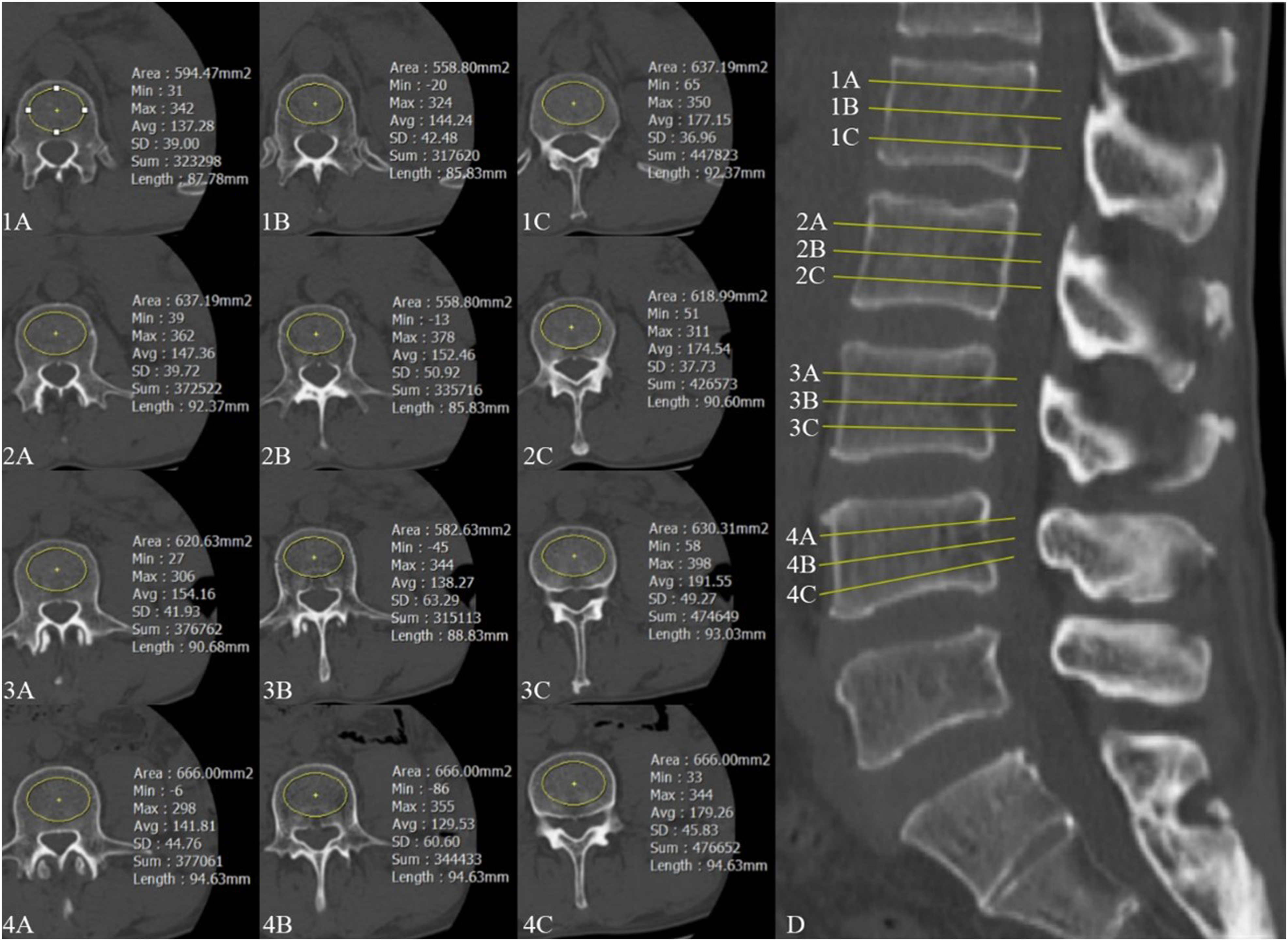
Collecting T-Score by Dual Energy X-ray Absorptiometry
Dual-energy X-ray absorptiometry (DXA) measurements of bone mineral density were assessed at the lumbar spine and femoral neck. Based on World Health Organization diagnostic criteria, osteoporosis is defined as a T-score of −2.5 or lower, while osteopenia is characterized by a T-score between −1.0 and −2.5.
Statistical Analysis
The data above were obtained by professional spine surgeons through measurement. First, we included the mean values of VBQ, CT HU, and DXA for different age groups. To assess the correlation between VBQ, CT HU, and DXA values in different age groups, we used Pearson correlation analysis. To control for potential confounding effects of age, we used partial correlation analysis to evaluate the overall associations among the 3 parameters. VBQ and CT HUs were independently measured by 2 researchers, who were blinded to the clinical information of the subjects. The interclass correlation coefficient (ICC) was calculated to assess inter-observer reliability, with ICC values classified as excellent (>.90), good (.80-.90), acceptable (.70-.80), and poor (≤.70). The statistical significance level was set at P < .05.
In order to evaluate the diagnostic performance of VBQ and CT HU values for osteoporosis using DXA as the gold standard, we plotted ROC curves by age group, gender, and menopausal status.
Results
Basic Radiological Data of 569 Included Patients (Data Reported as Mean ± SD or n).
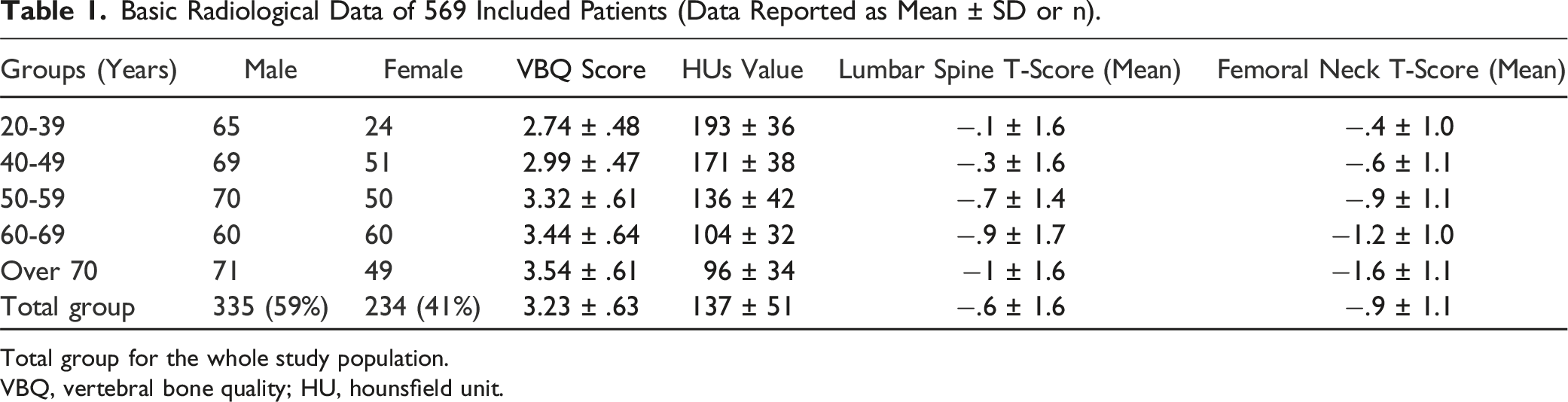
Total group for the whole study population.
VBQ, vertebral bone quality; HU, hounsfield unit.
Pearson Correlation Results for Lumbar Spine BMD, Femoral Neck BMD and VBQ Score, Hus Value.
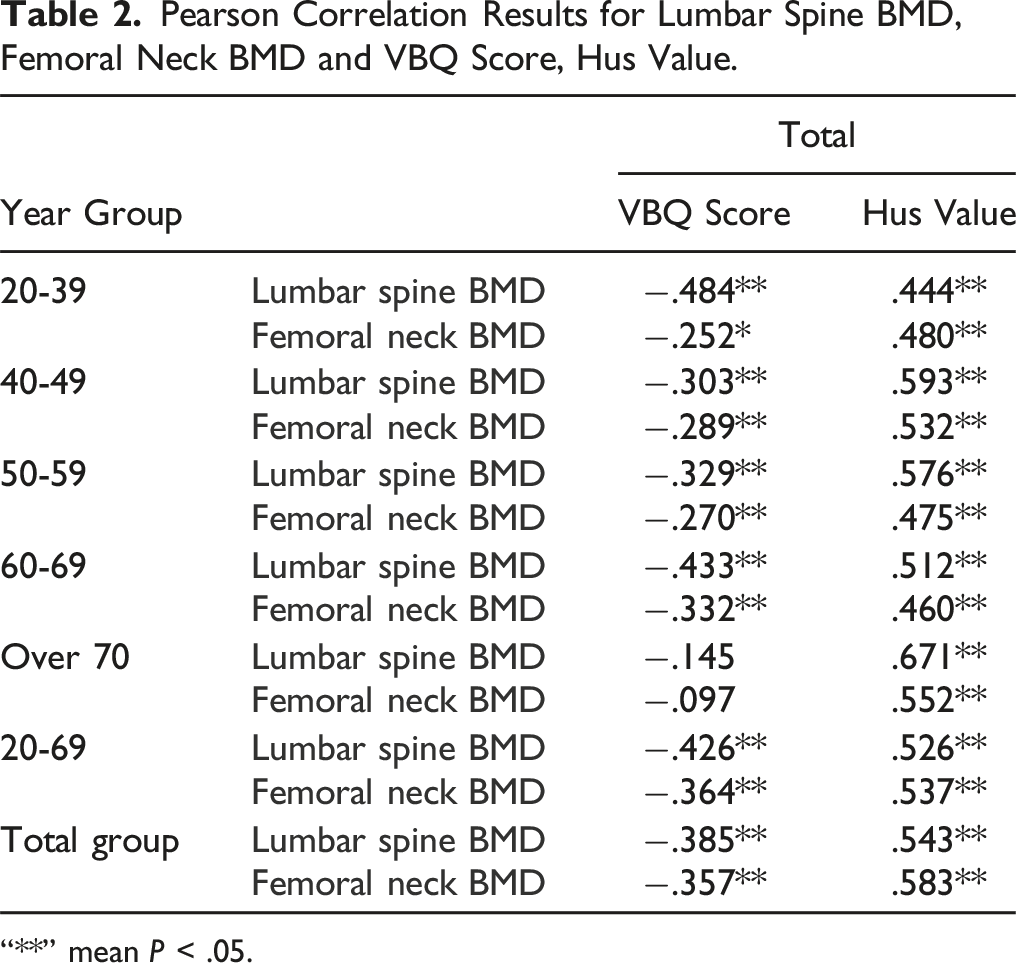
“**” mean P < .05.
Partial Correlation Results for Lumbar/Femoral Neck DXA and VBQ Score, CT HUs Value After Controlling for Age in Total Group.
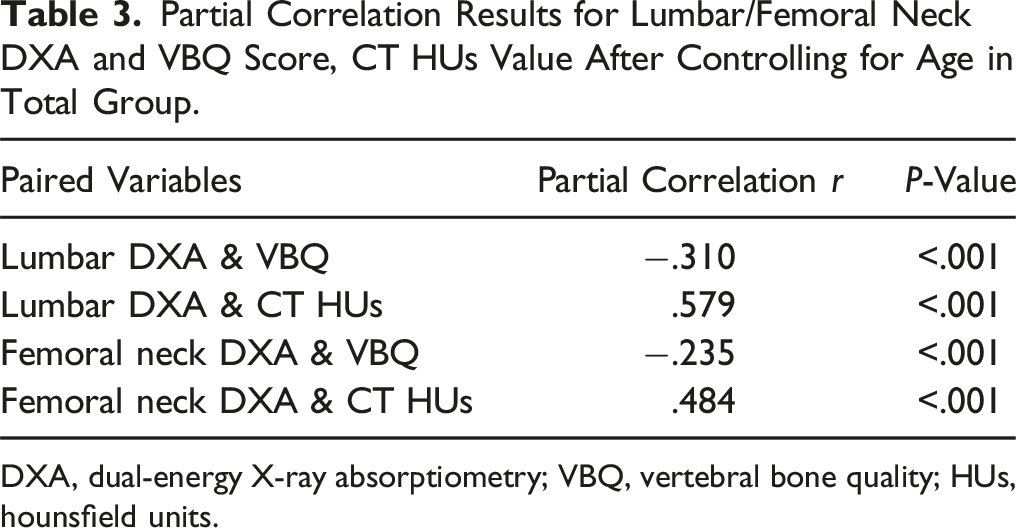
DXA, dual-energy X-ray absorptiometry; VBQ, vertebral bone quality; HUs, hounsfield units.
Analysis of VBQ Score and HUs Value Based on Lumbar Spine BMD as a Standard in Different Age Groups and the General Population.
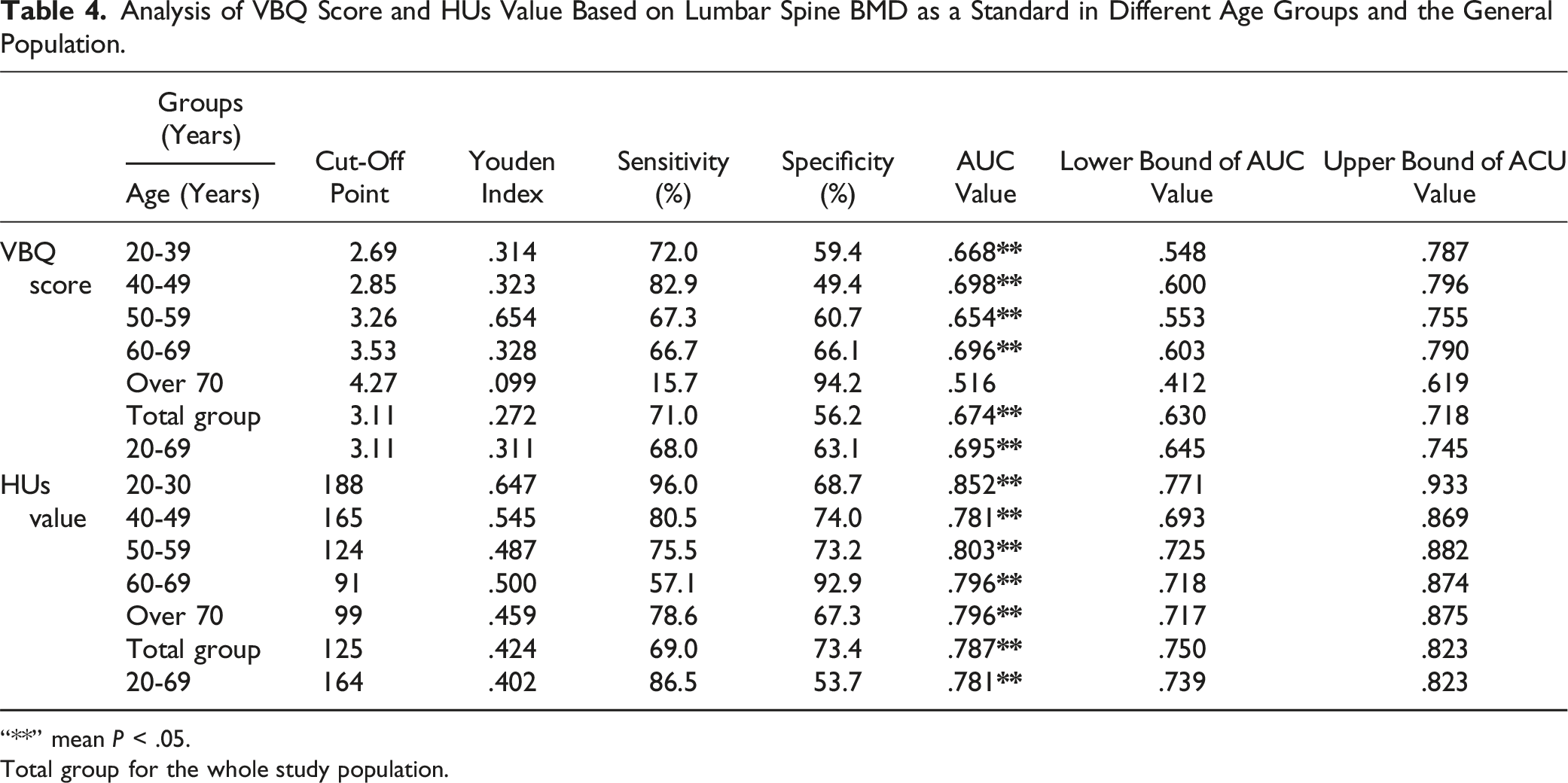
“**” mean P < .05.
Total group for the whole study population.
Analysis of VBQ Score and HUs Value Based on Femoral Neck BMD as a Standard in Different Age Groups and the General Population.
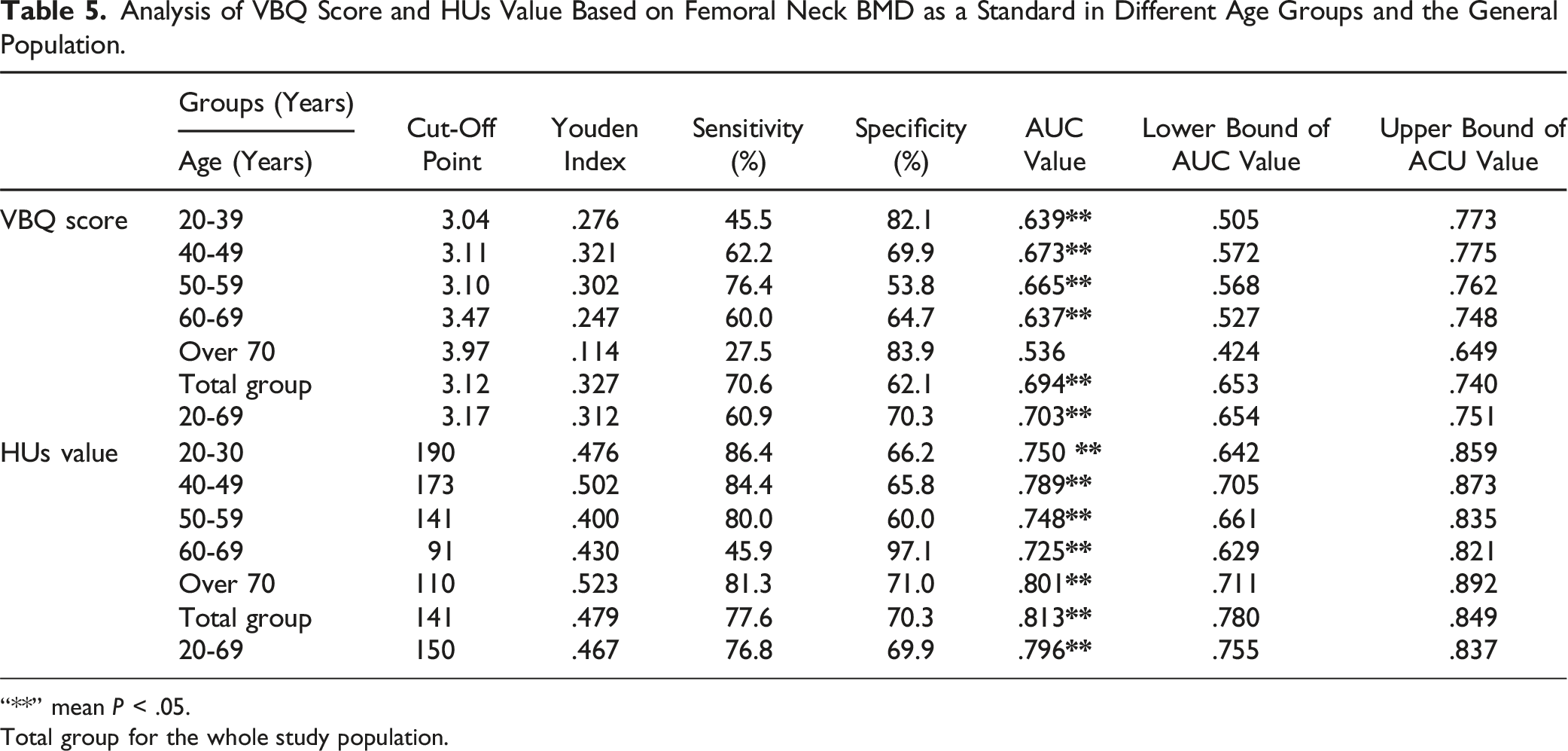
“**” mean P < .05.
Total group for the whole study population.
Analysis of VBQ Score and HUs Value for Individuals Over 70 Years Old.
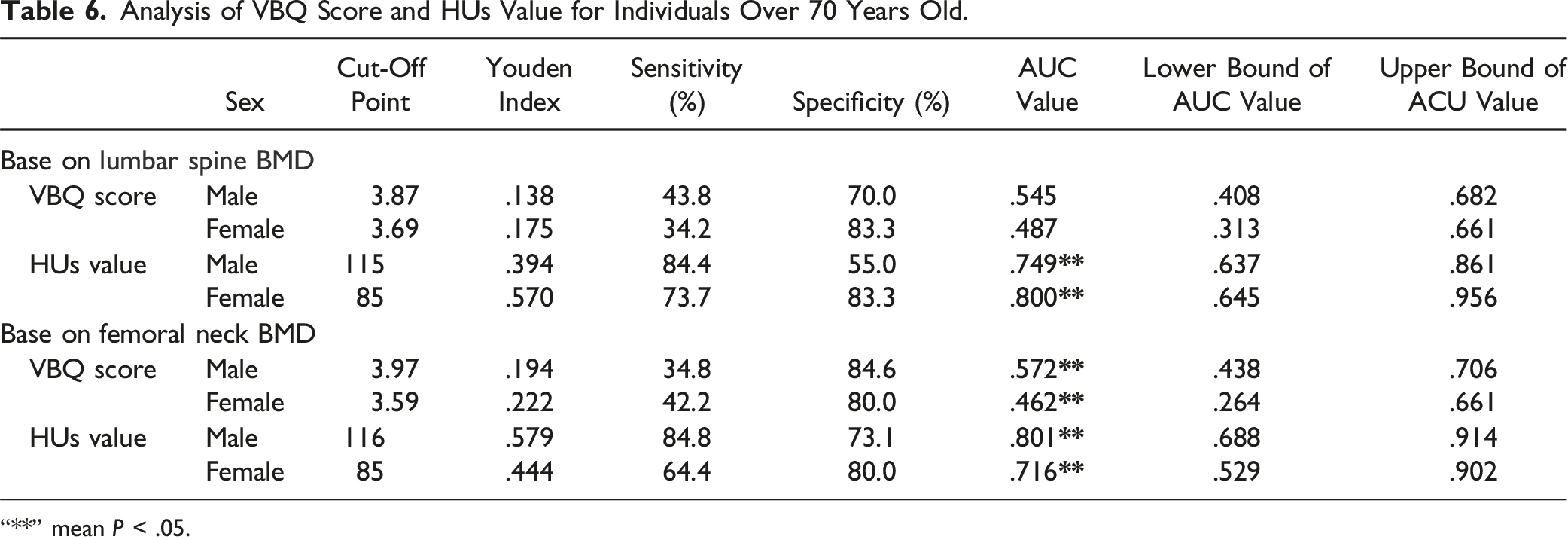
“**” mean P < .05.
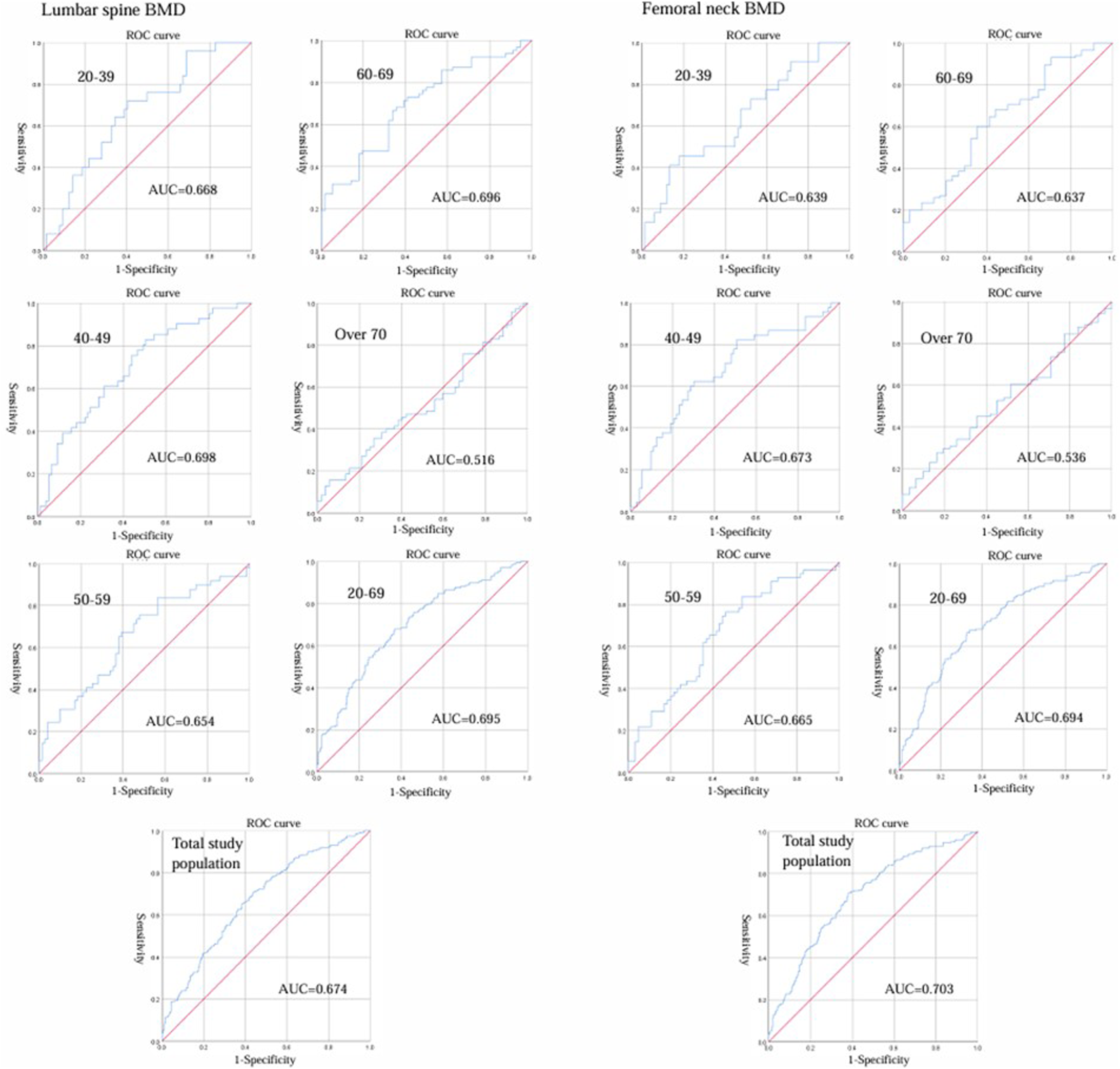
Receiver operation characteristic curve analysis was used to evaluate VBQ and DEXA-measured BMD at the lumbar spine and femoral neck in groups. VBQ, vertebral bone quality scores; BMD, bone mineral density; DEXA, dual-energy X-ray absorptiometry; AUC, area under curve.
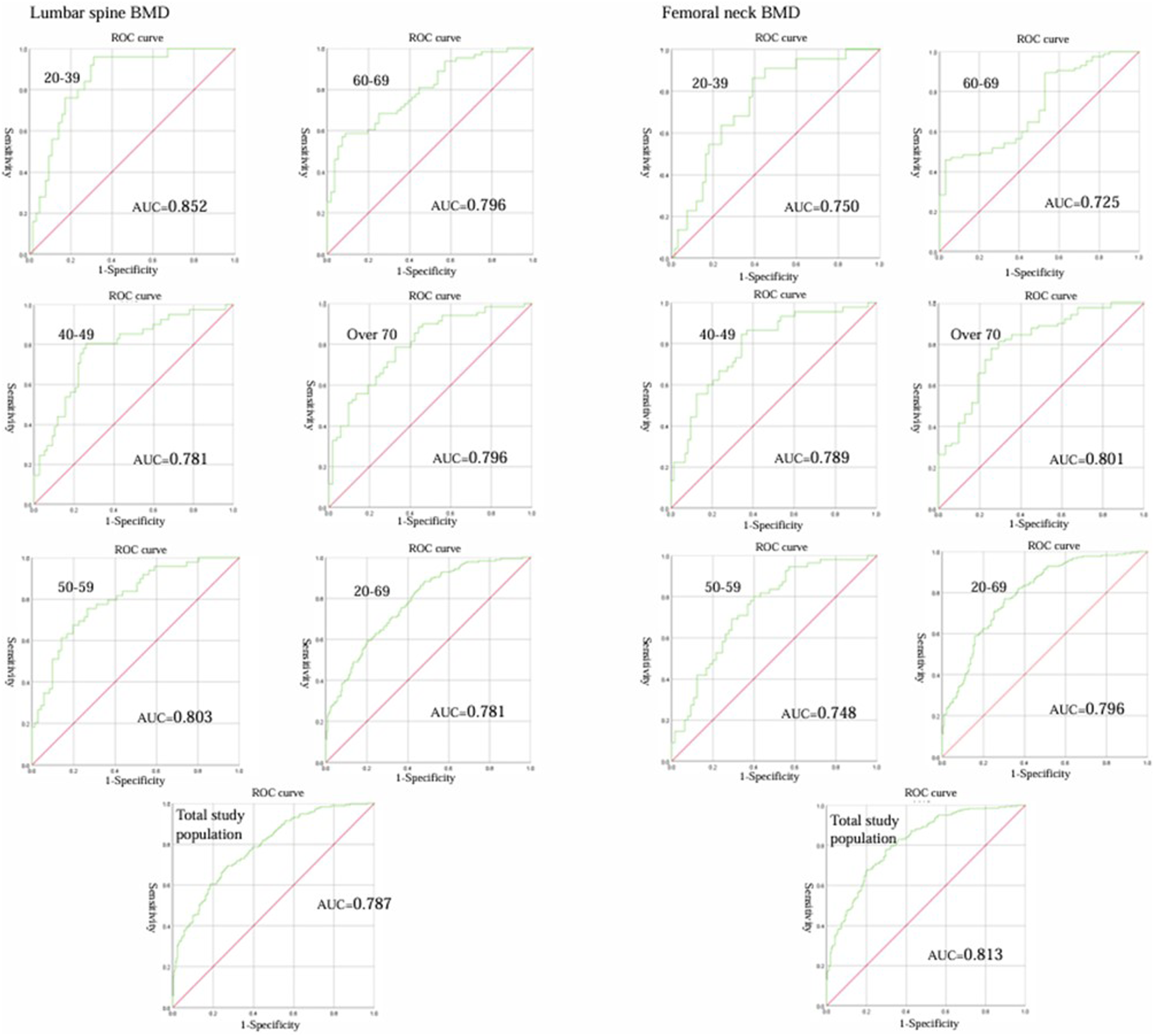
Receiver operation characteristic curve analysis was used to evaluate CT HUs and DEXA-measured BMD at the lumbar spine and femoral neck in groups. CT HUs, CT Hounsfield units; BMD, bone mineral density; DEXA, dual-energy X-ray absorptiometry; AUC, area under curve.
Overall Analysis of VBQ Scores and HUs for Gender-Based Grouping.
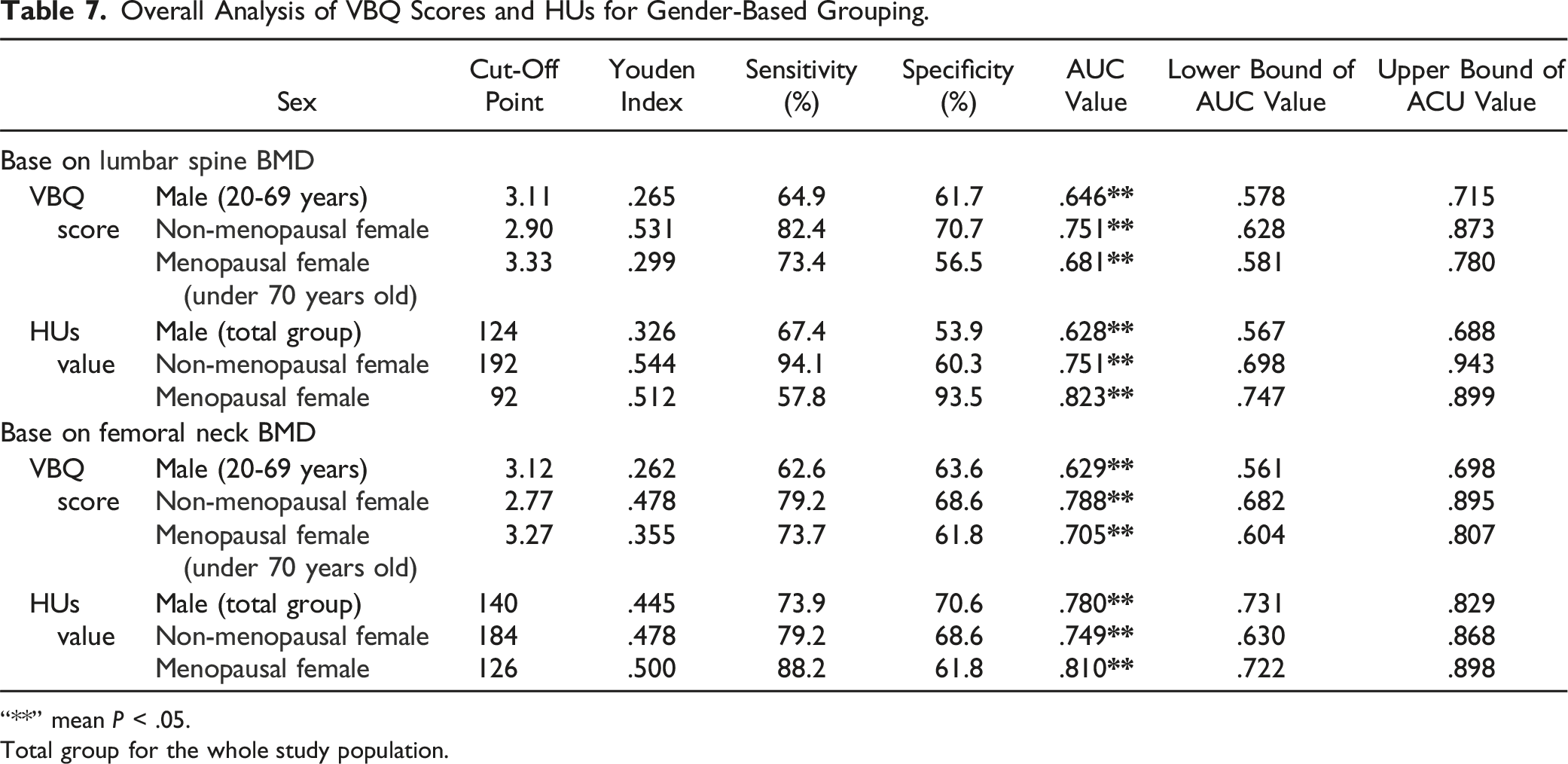
“**” mean P < .05.
Total group for the whole study population.
The Cut-Off Value of VBQ Score and Hus Value for Study Population.
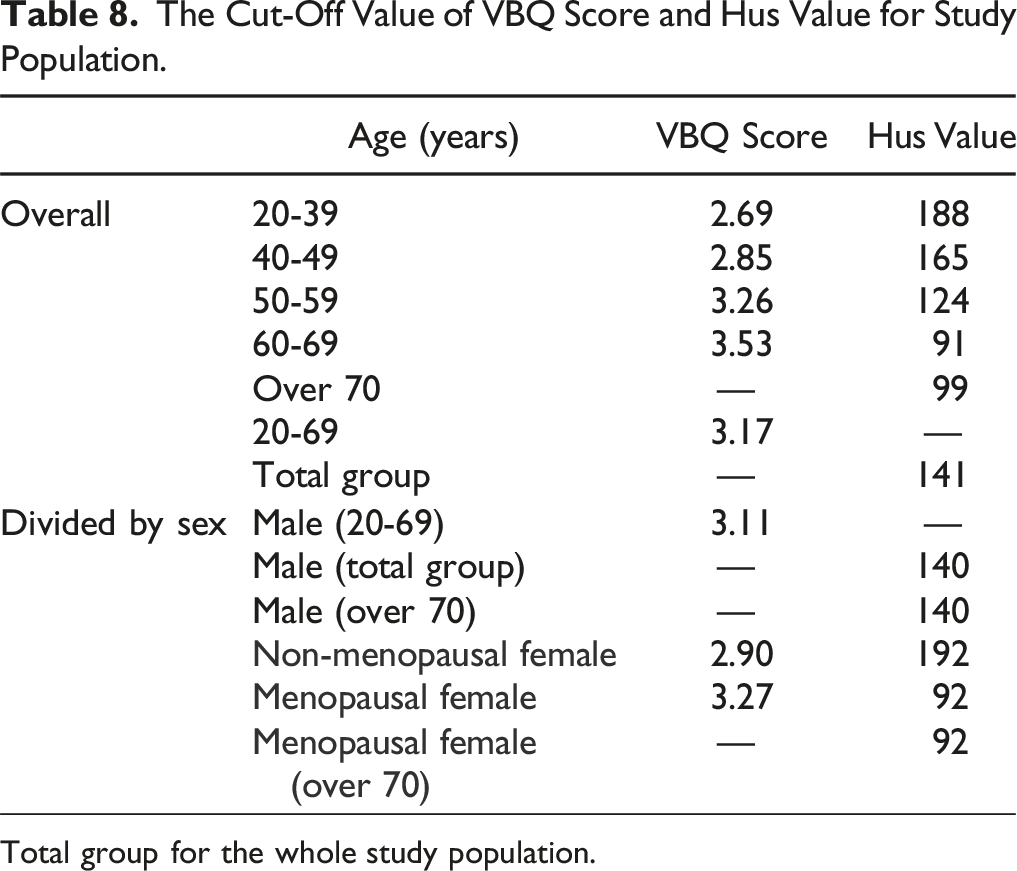
Total group for the whole study population.
Taking the results mentioned above into account, Table 7 mainly includes the reference values for lumbar spine VBQ and CT HUs for individuals with normal/osteoporosis as suggested by us. For males, the most appropriate VBQ diagnostic threshold value is 3.11 (AUC value is .674, P < .05) for the population with osteoporosis, while for males over 70 years old, due to the low diagnostic efficiency of VBQ, the most appropriate CT HUs diagnostic threshold value is 140 as a diagnostic criterion for osteoporosis. Among females, for non-menopausal female, VBQ threshold value is 2.90 (AUC value is .751, P < .05) and CT HUs threshold value is 192 (AUC value also is .751, P < .05) as diagnostic criteria for osteoporosis. For menopausal female, VBQ threshold value is 3.27 (AUC value is .705, P < .05) and CT HUs threshold value is 92 (AUC value is .823, P < .05) as diagnostic criteria for osteoporosis. Similarly, for females over 70 years old, as VBQ has low diagnostic efficiency for BMD, the CT HUs for menopausal female threshold value = 92 can be an alternative prediction (Table 8).
Discussion
This study aimed to comprehensively assess whether VBQ and CT HUs correlate with the DXA standard and to evaluate the diagnostic efficacy of VBQ and CT HUs in patients diagnosed with osteoporosis by DXA. Across the general population, we found that both VBQ and lumbar T-scores and femoral neck T-scores as measured by DXA increase with age, consistent with prior research.16-18 Ting et al also reported a significant correlation between VBQ and DXA (r = −.398 P < .05), as well as between HUs and DXA (r = .617, P < .05),9,10,19 confirming these correlations in our study. Moreover, we found that HUs had a higher correlation with DXA than VBQ across all patients. Osteoporosis is known to increase in prevalence with age. To assess whether age influences these correlations, we adjusted for age as a potential confounding factor. Partial correlation analysis confirmed the statistically significant association between VBQ, CT HUs, and DXA, further demonstrating the robustness of their correlation.
It is worth noting that, although DXA may not be the absolute “gold standard,” it still holds significant clinical value due to its widespread use. Therefore, this study is entirely based on osteoporosis diagnoses made using DXA. Unlike previous studies, this is the first large-sample study to investigate the correlation and diagnostic efficacy of DXA with VBQ and HUs across different ages and genders. We found that for the population over 70, VBQ had no significant correlation with either lumbar DXA (r = −.145) or femoral neck DXA (r = −.097), in contrast to HUs which correlated with DXA across all age groups. Further analysis of patients over 70 showed that VBQ has very low efficacy in diagnosing osteoporosis based on lumbar DXA (male AUC value = .545; female AUC value = .487). Additionally, considering the hormonal changes in postmenopausal female patients, we divided the population into menopausal and premenopausal females under 70, and men under 70, finding that VBQ shows good diagnostic efficacy for both lumbar and femoral neck DXA in these groups. Notably, HUs maintained significant correlations with DXA and good diagnostic efficacy for osteoporosis across all age groups.
Thus, we conclude that for the population over 70, VBQ cannot effectively diagnose osteoporosis, whereas for those under 70, regardless of gender or menopausal status, VBQ performs well. Hormonal changes in postmenopausal females do not affect the effectiveness of VBQ. Osteoporosis leads to a reduction in trabecular bones and an increase in fat cells that replace the trabecular structure, weakening it overall. 20 As women age, the rate of marrow fat transformation is faster than in men, especially after menopause,21,22 and the T1 signal, which is sensitive to fat, indicates higher VBQ scores with increased bone fat content. However, does vertebral fat tissue only relate to osteoporosis, and is VBQ scoring only influenced by fat tissue? Previous research has shown that bone marrow fat tissue can play a role in bone health through its paracrine and endocrine interactions with other bone components. 23 For instance, increased bone fat content in type 2 diabetes is not related to reduced bone mass. 24 Bredella studied 47 premenopausal women with varying BMIs and found that vertebral marrow fat increase correlates positively with visceral fat and negatively with IGF-1. 25 Moreover, we cannot exclude the changes in the collagen and hydroxyapatite within bones, or potential changes in water content in the lumbar spine in the elderly, might affect VBQ. Therefore, for individuals over 70, the lack of correlation between VBQ and DXA-determined bone density suggests that VBQ reflects not just bone density but bone quality, or more broadly, bone composition. Changes in organic or inorganic components of bones affect bone fragility. Ehresman found that compared to BMD obtained from DXA, VBQ is an independent predictor of thoracolumbar fragility fractures. 26 Aynaszyan et al’s study also showed that hyperlipidemia significantly raises VBQ, and controlling for hyperlipidemia improves the accuracy of VBQ in predicting osteopenia and osteoporosis. 27 Roch et al combined VBQ scores from different MRI sequences with vBMD, finding improved correlation between VBQ scores and vBMD, 14 although this requires more time to calculate scores, suggesting a direction for optimizing VBQ. Given the potential changes in bone composition in the elderly, we believe it is necessary to cautiously use VBQ to test for osteoporosis in individuals over 70. Due to bone changes in menopausal and premenopausal females, we separately recommend VBQ = 3.27 and VBQ = 2.90 as diagnostic thresholds for osteoporosis, whereas previous studies based on all patients suggested a threshold of 3.18,28
Our study found good correlation between HUs and both lumbar and femoral neck T-scores by DXA across all age groups, regardless of the menopausal status of female patients. Through ROC, we found that 141HUs was determined as the best sensitivity/specificity ratio for distinguishing between normal and abnormal BMD individuals. Pickhardt et al found a balanced HUs of 160, while Cohen et al found it to be 149.10,29 Additionally, we discovered that after dividing the population into different age groups, genders, and menopausal statuses, the thresholds for HUs varied. Furthermore, for the population over 70, we determined male HUs balance value to be 140 and female to be 92, and since VBQ’s diagnostic efficacy is too low to distinguish between normal and abnormal BMD individuals effectively, we recommend using HUs as an alternative to DXA and not using VBQ for diagnosing abnormal bone mass.
Most patients visiting for lumbar spine diseases routinely undergo lumbar spine CT or MRI, making it very convenient and reliable to measure HUs or VBQ values using existing images, without always incurring the additional economic burden and radiation exposure of DXA. As an opportunistic preoperative tool that has emerged in recent years, VBQ has the advantage of no radiation exposure, making further research into its prospects for use necessary to determine whether VBQ can serve as an independent diagnostic tool. In our study, although VBQ performed poorly in the elderly population over 70, it showed good performance in postmenopausal females and other age groups. Meanwhile, HUs can avoid interference from bone spurs, spinal scoliosis, and aortic calcification, theoretically providing a more accurate spinal bone density assessment. 30
While our study focused on the correlation of lumbar and femoral BMD with CT Hounsfield Units (HUs) and VBQ for diagnosing osteoporosis, comprehensive approaches are required for osteoporosis diagnosis in clinical practice, such as incorporating fracture history and FRAX risk assessment. Nevertheless, it is noteworthy that FRAX’s requirement for detailed clinical variables (eg, smoking status, parental hip fracture history) may limit its utility in time-constrained clinical scenarios. In contrast, VBQ and HUs demonstrate particular clinical utility in opportunistic screening scenarios, particularly during outpatient evaluations where obtaining comprehensive patient histories proves challenging. These imaging-driven approaches address the growing clinical demand in resource-limited diagnostic settings.
While our study provides valuable insights into the correlation between VBQ and HUs with DEXA and their diagnostic efficacy, there are several limitations. Firstly, despite a relatively large sample size, the fact that all data were obtained from a single medical center may constrain the generalizability of the results. Secondly, this study was limited to using DEXA as the gold standard, focusing primarily on further research to assess whether opportunistic methods are consistent and comparable with DEXA. Although DEXA is the most commonly used method clinically, compared to QCT, it is not widely used in clinical practice. However, as mentioned in the introduction, DEXA can be affected by certain degenerative diseases and is only traditionally considered the gold standard for BMD. Thirdly, due to the retrospective design, our data may be subject to selection bias. Additionally, despite efforts to minimize measurement errors, technical differences between different devices and operators may affect the accuracy of the results. Furthermore, the measurement of VBQ and CT HUs relies on high-quality imaging data, and poor image quality may affect the accuracy of the measurements. Lastly, our study did not extensively explore patient populations of different races and regions, data on fragility fractures, FRAX risk assessment and factors other than age and gender were not systematically collected; future research should consider these factors to enhance the representativeness and generalizability of the study findings.
Conclusion
This study found that, although VBQ had lower diagnostic efficacy for patients over 70 years old, it showed good diagnostic accuracy for postmenopausal women under 70 and other age groups. In contrast, CT HUs demonstrated higher correlation and bone density assessment capability with DXA across all age groups. When using VBQ to predict osteoporosis in patients on opportunistic grounds, it is still necessary to incorporate additional reference indicators, such as CT HUs. Additionally, further research is needed to optimize the use of MRI as an opportunistic method for predicting osteoporosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets analyzed during the current study are not publicly available due to involving patients’ imaging examination results and other personal information but are available from the corresponding author on reasonable request.