
Abstract
Study Design:
Narrative review.
Objective:
This article seeks to provide a narrative review regarding the ability of opportunistic information available from computed tomography (CT) scans to guide decisions in spine surgery related to patient bone quality.
Methods:
A review of the literature (limited to human and English language) was performed via PubMed and Google Scholar using the search terms; “osteoporosis” AND “opportunistic” AND “computed tomography” AND “spine surgery.” The titles and then abstracts of all identified citations were reviewed for inclusion by 2 of the authors (MS, BAF). Relevant articles were then studied in full text.
Results:
A review of the literature found 25 articles that were selected for inclusion in this narrative review. These articles were broadly divided into 4 subcategories: (1) opportunistic CT (oCT) and osteoporosis detection, (2) oCT data and the quality of screw fixation, (3) utilization of Hounsfield units to assess clinical and/or radiographic outcomes following spine fusion, and (4) virtual stress testing in spine surgery.
Conclusion:
The literature on oCT, as well as associated virtual stress-testing techniques, demonstrate the potential to enhance spine surgery outcomes by preoperatively identifying at-risk patients in need of bone health optimization and informing best techniques for performing spinal fusion surgery on patients with diminished bone quality. While our narrative summary of the limited literature to date suggests a promising future for oCT data, significant additional research and/or radiographic workflow standardization is needed to validate these methods for clinical use.
Background
Osteoporosis and low bone mineral density (BMD) represent a significant risk of morbidity for patients with spinal pathology. In addition to predisposing to fragility fractures. 1,2 Low BMD has been shown to adversely affect outcomes following instrumented spinal fusion surgery, as well as health care costs. 1 -3 There is a well-established correlation between diminished bone quality and poor spine surgical outcomes, which in turn leads to increased and more challenging revision spine surgery. 4 -8 According to the National Inpatient Sample, in 2009 there were more than 22 000 revision spine fusion surgeries performed in the United States resulting in longer hospitalizations and greater total costs. 9 Given that osteoporosis medications are effective at reducing vertebral compression fractures (VCF) and can improve outcomes after spinal fusion surgery, proper screening for low bone density and appropriate perioperative bone health optimization is more relevant than ever. 10,11
The gold standard screening modality for osteoporosis is measurement of the areal bone mineral density in g/cm2 (BMD) via dual X-ray absorptiometry (DXA). Unfortunately, DXA has several inherent limitations. First, a DXA scan only evaluates one parameter of bone strength (ie, BMD). It lacks the ability to evaluate bone architecture and quality. 12 As an example, it has been demonstrated that densitometric T-scores derived from DXA scans are not predictive of osteoporosis-related complications (ORCs) in spine surgery. 4 Second, DXA scans are subject to artifacts created from implants or degenerative changes (subchondral sclerosis, osteophyte formation, soft tissue calcification, etc), which frequently coexist in patients with low bone mass. 13 Third, BMD can only be inferred at vertebral levels outside those assessed by the DXA scan. 3 The bone located at potential surgical sites must also prove to be of adequate quality to perform well under the stress of implants. In this light, densitometric imaging capable of isolating regions of interest focused in the projected path of a pedicle screw, may offer better insight into the ability of the bone-screw interface to withstand the mechanical challenges faced after spinal surgery. Finally, a DXA scan, unlike computed tomography (CT), is a testing modality that has no shared purpose in the evaluation of spine pathology. 14
The use of CT scans obtained for clinical purposes other than preoperative measurement of BMD and/or multiplanar evaluation of bone structure is considered an opportunistic CT (oCT). Between 15% and 30% of the estimated 100 million annual emergency department encounters in the United States result in a CT scan being obtained—many of which contain images of the spine. 15 CTs contain vast amounts of potential information regarding bone health. Traditional CT scans display 2D computer-generated images of tissues based on linear X-ray attenuation coefficients. The X-ray attenuation output are voxels in a grayscale known as Hounsfield units (HU) and are proportional to atomic density. In contrast to DEXA, CT scans of the spine not only can take into account bone mineral density but also provide insight to the adequacy and quality of the bone structure present at specific regions of interest (ROI). Once an ROI is identified, standard imaging software can calculate the average HU in the area of interest, thus potentially inferring BMD. 16 Sagittally reconstructed CT scans also provide improved holistic morphometric analysis of vertebral bodies to detect vertebral compression fractures, which are independently diagnostic of osteoporosis. Last, finite element analysis (FEA) and/or virtual stress test (VST) software can leverage CT data to model and predict bone strength and/or bone fixation quality in spine surgical patients. 17,18 As such, the use oCT in the preoperative evaluation of a potential spine surgery patient is intriguing. The use of CT to measure and evaluate BMD is not new. Using CT to explicitly measure BMD is termed quantitative CT (qCT). 19 qCT follows a specific imaging protocol that requires synchronous scanning of a phantom and a patient, or asynchronous scanning from daily calibration with phantoms. While qCT is a validated method for diagnosing osteoporosis, and would allow for site-specific interrogation of bone density and quality, these scanning protocols and phantoms are not ubiquitous and cannot be reconstructed from opportunistically available CT scans, which are routinely ordered for diagnosis of spinal disease and/or surgical planning.
Given the abundance of CT imaging studies performed annually and the importance of defining site-specific bone quality prior to major spinal surgery, much interest has been generated for using oCT scans to screen for low bone mass in patients presenting for elective spine surgery. This article seeks to lead the reader through literature on oCT use in spine surgery and inform basic understanding of the topic.
Methods
A narrative review of the literature was performed via a search of PubMed and Google Scholar using the search terms; “osteoporosis,” “opportunistic,” “computed tomography,” “Spine,” and “Spine Surgery” on January 31, 2019. The search was limited to articles that were published in (or subsequently translated to) English. No restriction on date published was enforced. All study designs were included and ranged from expert opinion to randomized controlled trials. The titles and then abstracts of all relevant citations were reviewed for inclusion by 2 of the authors (MS, BAF). As the intent of the review was narrative, inclusion was not based on a systematic assessment of article quality, but rather relevance to one of the 4 subcategories of interest. Relevant articles, as deemed so by the authors, were then studied in full text. Articles were sorted into 4 general categories for discussion: (1) oCT and osteoporosis detection, (2) oCT data and the quality of screw fixation, (3) utilization of HU to assess clinical and/or radiographic outcomes following spine fusion, and (4) virtual stress testing in spine surgery.
Results
While the use of oCTs as a potential osteoporosis screening modality is well debated in the literature, there exists a relative paucity of information on the use of oCT specifically in spine surgery. Our literature search yielded 25 relevant articles from the above search criteria (Figure 1). Of the 25 articles, 6 articles related oCT and osteoporosis detection (Table 1), 8 articles related oCT data and the quality of screw fixation (Table 2), 6 articles described utilization of HU to assess clinical and/or radiographic outcomes following spine fusion (Table 3), and 5 articles addressed virtual stress testing in spine surgery.
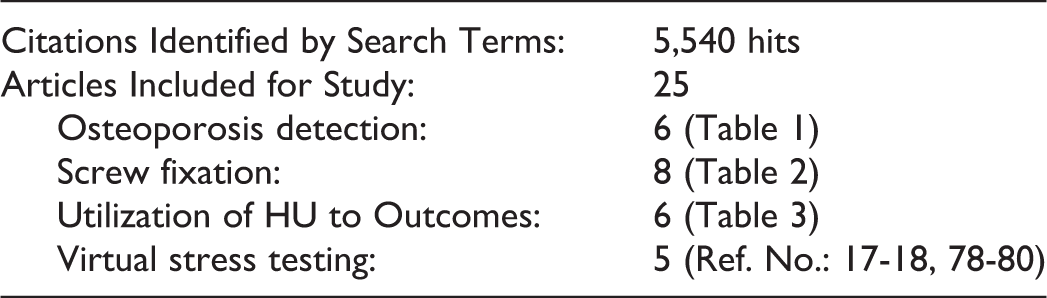
Article search and inclusion method.
Opportunistic Computed Tomography in Osteoporosis Screening.
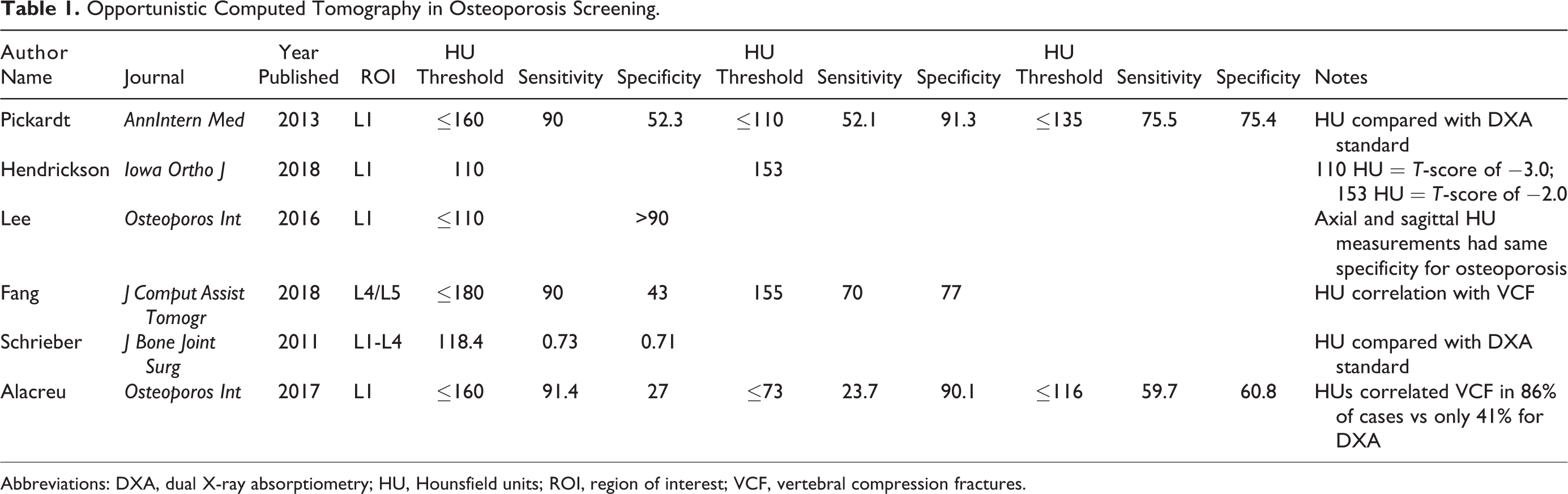
Abbreviations: DXA, dual X-ray absorptiometry; HU, Hounsfield units; ROI, region of interest; VCF, vertebral compression fractures.
Opportunistic Computed Tomography in Pedicle Screw Loosening.
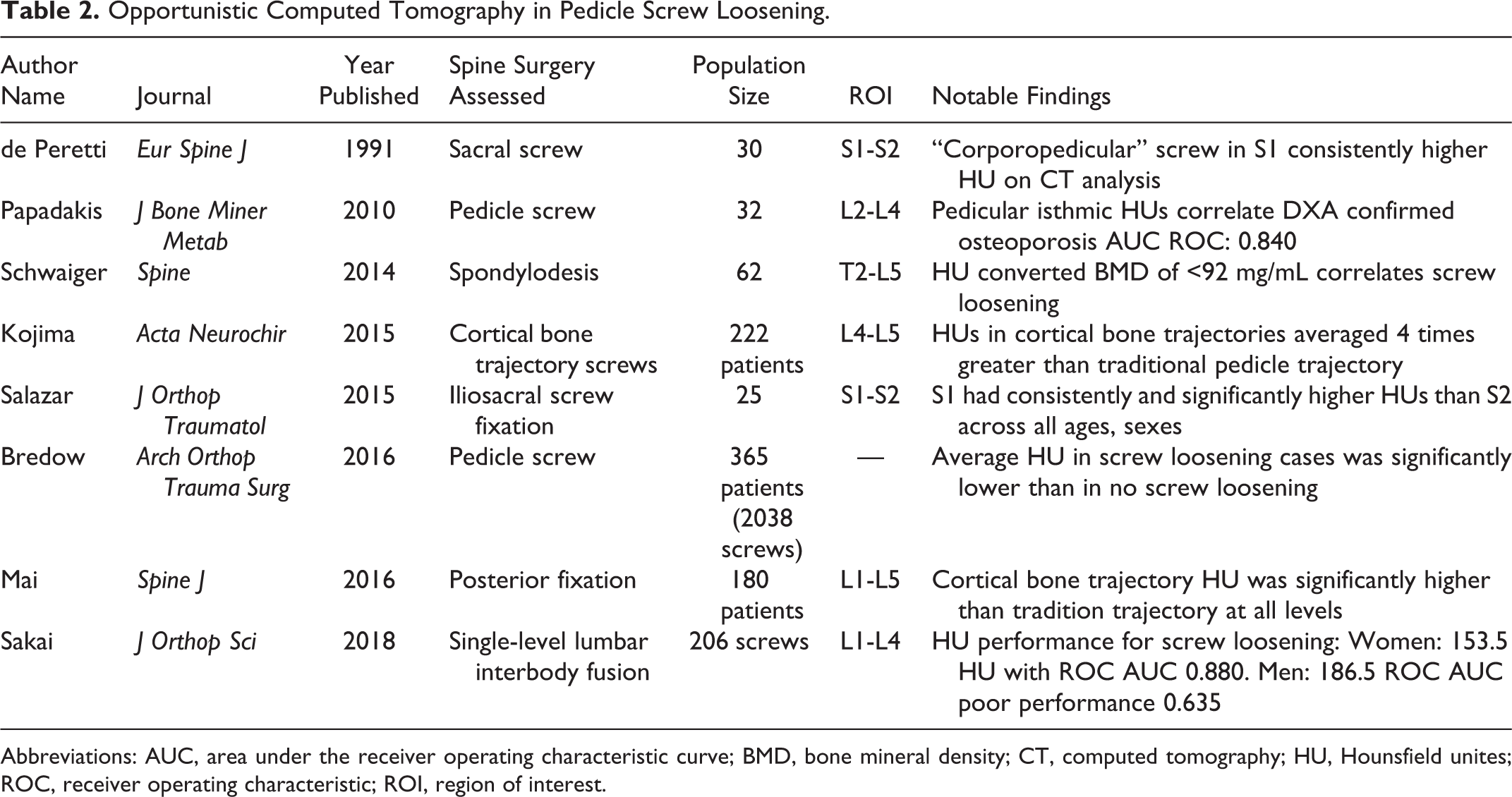
Abbreviations: AUC, area under the receiver operating characteristic curve; BMD, bone mineral density; CT, computed tomography; HU, Hounsfield unites; ROC, receiver operating characteristic; ROI, region of interest.
Opportunistic Computed Tomography in Spine Surgery Outcomes.
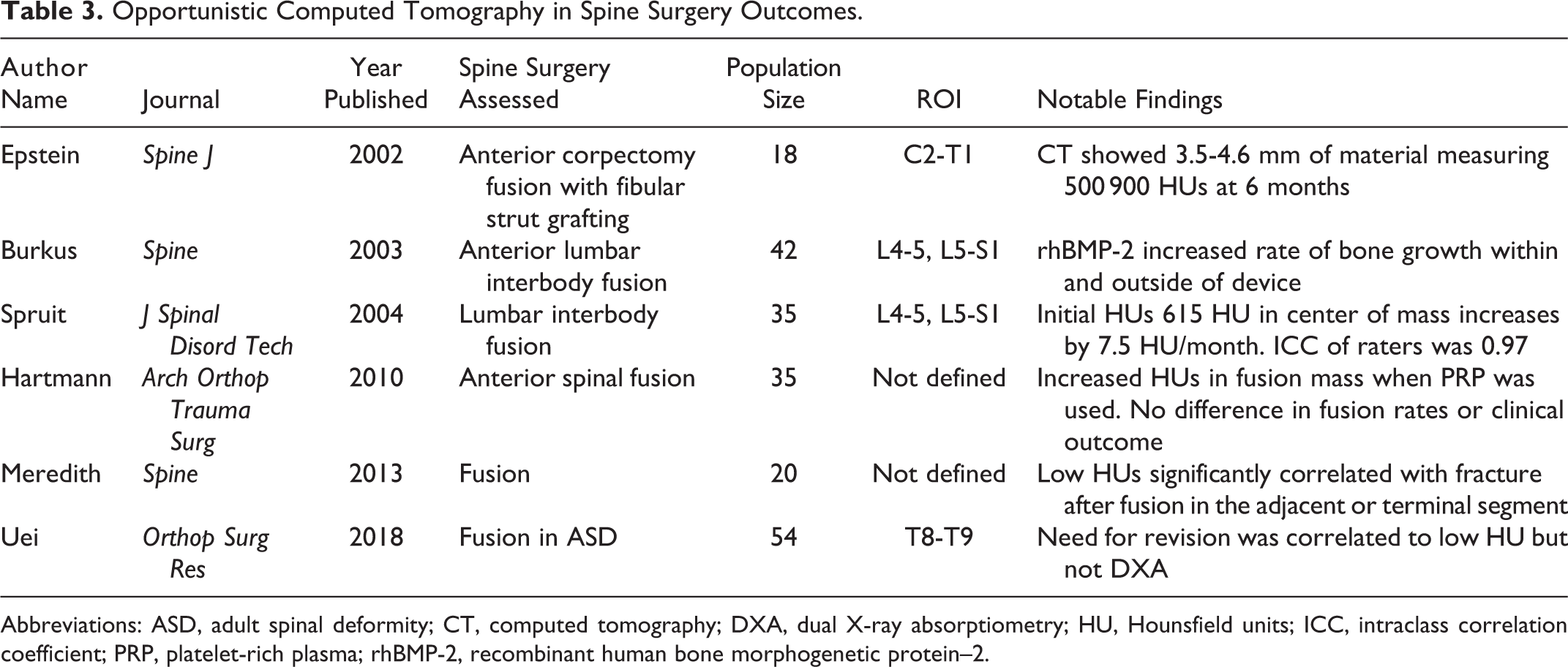
Abbreviations: ASD, adult spinal deformity; CT, computed tomography; DXA, dual X-ray absorptiometry; HU, Hounsfield units; ICC, intraclass correlation coefficient; PRP, platelet-rich plasma; rhBMP-2, recombinant human bone morphogenetic protein–2.
oCT and Osteoporosis Detection
Multiple authors have demonstrated a moderate correlation between oCT data and DXA-defined BMD at various anatomic regions (area under the receiver operating characteristic curve [AUC] 0.64-0.89) 20 -24 —suggesting a possible role for oCT in osteoporosis detection. In support of this, investigators have found HUs to strongly correlate with true biomechanical properties of bone specimens. 25 -27 Hendrickson et al 28 performed a robust study in which normative data for lumbar HUs was established in a healthy, nonosteoporotic reference group and then compared with an older group of individuals who had undergone CT and DXA scans. They found that T-scores derived from lumbar DXA were significantly higher than T-scores from HU analysis, which raises questions about which technology may be most sensitive in assessing bone strength in adult patients. Some have reasoned that because DXA scans take into account the posterior elements of the spine, including degenerative tissue, their BMD estimations are falsely elevated. This proposed underreporting of spinal osteoporosis could explain why HU analysis has been more reliable in predicting VCFs than DXA. 28
As with the study by Hendrickson et al, 28 various authors have sought to establish HU thresholds to screen osteoporosis or risk of VCF. Different thresholds have been proposed using receiver operating characteristic (ROC) analysis to optimize sensitivity and specificity (Table 1). 22,23,25,28 -30 Pickhardt et al 22 found that optimum thresholds for prediction of osteoporosis were less than 100 HU, while normal bone could be considered greater than 150 HU. Among other studies, highly specific HU lower limit thresholds range between 73 and 100, while highly sensitive cutoffs range between 100 and 180 (Table 1). To date, no unanimous HU threshold has been found to directly correlate with DXA-defined osteoporosis.
Due to the wide range of HU cutoffs reported, there exists skepticism regarding oCT use to screen for osteoporosis. 31 -34 While recent studies have attempted to allay those concerns by reporting excellent intra- and interobserver reliability when measuring HUs across spine ROIs in the cervical, thoracic, and lumbosacral spine, 24,34 -40 others have shown that variable scanning techniques and parameters (such as use of intravenous contrast) significantly affect HU values and thus BMD interpretation. 22,41,42 In addition, differences in outcomes between different scanner manufacturers are of unknown significance and require further study. 31
The presence of a vertebral compression fracture is a powerful predictor of future fracture, 43 and thus the presence of osteoporosis. Reformatting oCT scans to sagittal reconstruction does not alter HU measurements and allows an observer to simultaneously screen for VCFs. 29 Thus, oCTs enable morphometric analysis for the detection of VCFs, which can be difficult to detect on plain radiographs, especially in patients with low bone density and/or spinal deformity. oCT data has been shown to accurately correlate to current and future VCFs with diagnostic accuracy as high as 97.4% and AUC = 0.978. 30,44 -47 oCT has outperformed DXA in the prediction of VCFs. 23,24 oCT has even been used to screen for cervical spine and hip fractures among the elderly. 37,48,49 As stated above, it has yet to be shown that oCTs can accurately and reliably replace the use of the DXA scans for osteoporosis diagnosis, but current literature is encouraging regarding its ability to correlate to vertebral compression fractures. 28
As an adjunct to standard oCTs, virtual stress testing (VST) and FEA are noninvasive tests to estimate bone mechanical properties via virtual biomechanical testing. VST leverages routine phantomless CT attenuation data (HUs) to create geometric BMD units. Each BMD density unit is then assigned an independent biomechanical property based on established finite element technique/analysis. Once a 3-dimensional model of many small finite elements is constructed, various loads/sheers/torsions can be applied to estimate strength, mechanical properties, and failure points. 50 Clinically, the use of FEA/VST is known as biomechanical computed tomography (BCT). The ability to not only asses the quality of the bone in its natural state but also evaluate its performance under the stress of spinal implants could be fundamental to reducing ORCs. FEA is a validated engineering technique that has been successfully employed to asses bone strength in the hips and spine. 51 -54 It already has been reported to be superior to DXA scans in predicting fragility fractures at the hip and spine, 53,55 -63 and could provide further insight into the diagnosis and risk stratification of osteoporotic patients prior to undergoing surgical procedures of the spine.
While oCT is an enticing diagnostic test, it is still limited in its sensitivity and specificity to be used as a diagnostic tool. One of the major limitations of oCT is that these studies were performed for clinical reasons unrelated to the calibrated measurement of bone density. Because calibration is a critical part of any diagnostic instrument, the best use of oCT may be for what is termed “case finding.” With case finding, the pretest probability is low and the testing method possesses significant ability to detect disease, but lacks the validity (and Food and Drug Administration approval) to “diagnose” disease. Currently, oCT can and should be used to find patients at heightened risk of disease, while DXA, qCT, and BCT analysis should be used to diagnose it.
oCT Data and the Quality of Screw Fixation
In the early 1990s, de Peretti et al 64,65 published a pair of articles in which HUs were used to asses BMD of the first and second sacral levels of young healthy controls, followed by pull-out testing of various S1 screw trajectory. They found that the trajectory with the strongest biomechanical advantage was consistent with the bony regions with the greatest BMD in their CT assessments, implying the potential utility of CT-guided BMD analysis as a tool for identifying ideal screw placement in the spine. 64,65 These were some of the earliest reports linking CT HUs to biomechanical properties of bone as it relates to screw placement.
Later, Papadakis et al 66 compared lumbar CT scans of 32 postmenopausal women with compression fractures to abdominal oCT of 38 women without compression fractures. All women had lumbar DXA scan of L1-L4. All CT imaging compared several morpho-densitometric data, including an ROI that was a cross-sectional area within the endosteum of the pedicle (vertical to the pedicle axis) and an axial ROI of the vertebral body. Both the endosteal pedicle and vertebral body HUs, were then compared with osteoporotic status as determined by DXA scans. The ROI within the pedicle isthmus was most correlated to DXA- and VCF-confirmed osteoporosis with ROC: 0.840. This finding is significant because it showed that HU measurements within a ROI very specific to spine surgery planning (ie, the pedicle isthmus) was consistent with osteoporosis status and fragility fracture. 66
In more recent studies, several authors have utilized oCT to validate nontraditional screw trajectories. Kojima et al 67 used trajectory-specific ROIs to compare HUs for cortical bone trajectory (CBT) with traditional pedicle screws. The authors used opportunistic lumbar spine CT scans of 222 patients with degenerative lumbar spine disease, and evaluated ROIs matching CBT and traditional pedicle screw trajectories at the L4 and L5 levels. The authors found that CBT averaged 4 times higher BMD than traditional tracts. 67 Mai et al 68 followed this study with a cross-sectional anatomic study in 180 patients who had oCT scans of the lumbar spine. The authors compared trajectory-specific ROI analysis in L1-L5, again finding that the CBT ROIs were consistently denser via HU analysis than traditional pedicle tracts. 68
Salazar et al 69 performed a similar analysis of screw trajectories at S1 and S2 in 25 consecutive trauma patients. Their intent was to shed light on whether placing iliosacral screws through S1 versus S2 made any difference. The authors found that iliosacral screw trajectory ROIs within S1 had a statistically significant higher average HU than S2 and thus led the authors to recommend caution when using S2 as iliosacral fixation point for sacral insufficiency fractures. 69
Several authors have utilized an oCT model for prediction of screw loosening. While the above studies used HUs to propose theoretical advantage, there are some studies that correlate CT findings to clinical results. Schwaiger et al 44 used follow-up lumbar CT scans in patients who had undergone a spinal fusion with pedicle screws to assess the relationship between HU and screw loosening. They found that patients with a BMD of less than 92 mg/mL (BMD estimation from qCT analysis) was correlated with radiographic evidence of screw loosening (ROC 0.827, sensitivity 0.81, specificity 0.79). 44 Sakai et al 70 performed a case-control series in which 206 screws distributed across 21 male and 31 female patients after single-level lumbar fusions were evaluated for postoperative loosening. Preoperative HU of the screw trajectory was analyzed by superimposing preoperative and postoperative CT images using image analysis software. Multiple variables including BMD via DXA analysis were analyzed in multivariate logistic regression analysis. They found a HU cutoff of 153.5 possessed an ROC AUC of 0.880 for the association to screw loosening in women and HU 186.5 with ROC 0.635 in men. 70
Similarly, Bredow et al 71 performed a retrospective review of 365 patients (2038 pedicle screws) who had preoperative CT scans of their lumbar spine. All instrumented levels underwent HU analysis to determine BMD. All the patients underwent post-operative CT scans to assess for screw loosening. A total of 62/2038 (3%) screws were found to be loose. The authors found an average of 116.3 HUs in the vertebral bodies of screws that loosened versus 132.7 in screws that did not loosen (P = .003). 71
The majority of work to date regarding the use of oCT in adult spinal deformity patients has been retrospective, and therefore capable of determining correlations between, as opposed to predictions of, events. Validation of the predictive value of a diagnostic or prognostic modality requires prospective study. These studies are needed to define predictive thresholds for ORC events such as screw loosening. Until such studies are available, the ability to fully leverage the information contained in oCTs toward defining best practices in adult spinal deformity patients will remain anecdotal or hypothetical. On the other hand; while the literature on utilization of oCTs to detect ROI-specific areas of inadequate bone strength is limited, it does suggest the potential of the technology for patient-specific preoperative planning. Indeed, as evidenced by Schwaiger et al, 44 Sakai et al, 70 and Bredow et al, 71 HU thresholds can be used to anticipate screw loosening but suffer the same HU variability seen with osteoporosis detection. While the general cutoffs established by these studies are roughly in line with the cut-offs established by studies investigating osteoporosis/VCF diagnosis summarized in Table 1, the patient-specific approach requires further study for validation.
Utilization of HU to Assess Clinical and/or Radiographic Outcomes Following Spine Fusion
While the gold standard for assessing spine fusion is surgical exploration, clinicians and surgeons gauge success of spinal fusion based on clinical exam and postoperative imaging. No standard method, radiographically, has been shown to reliably assess for fusion. Validated CT technology measuring HUs could offer the clinician a way to monitor and assess fusion in a more objective and reproducible fashion. Multiple authors have utilized CT technology to evaluate for postoperative outcomes, and these efforts will be reviewed here.
Epstein et al 72 investigated the use of postoperative CT scans to quantitatively assess fusion progress in patients undergoing multilevel anterior cervical corpectomy and fresh frozen fibular strut grafting. The authors measured the amount of linear trabecular bone ingrowth into the canal of the fibular strut graft via CT as a means of fusion assessment. HU range of 300 to 600 was used to confirm material ingrown was indeed bone. The authors did not compare CT versus plain dynamic X-ray for prediction of failure in their cohort. Nonetheless, their article provided an early assessment of an adjunctive technique for assessing fusion following reconstructive spine surgery. 72
Burkus et al 73 performed a prospective randomized study that employed HUs to assess the osteoinduction in anterior lumbar interbody fusions (ALIF) with the use of recombinant human bone morphogenetic protein–2 (rhBMP-2) as compared with iliac crest autograft (ICBG). Twenty-two patients were randomized to ALIF with rhBMP-2 delivered into cage (Medtronic Titanium LT-Cage) via collagen sponge versus 20 patients with ICBG. CT scans were performed at 2 days, 6 months, 12 months, and 24 months after surgery. CT imaging was analyzed with standard HU mean measurements with a ROI within the ALIF cage to compare the 2 cohorts. The authors were able to successfully differentiate fusion mass between rhBMP-2 and ICBG via HU analysis. This highlighted the ability of CT HU analysis to asses a fusion progress and end-result within a specific ROI that is poorly analyzed using traditional imaging techniques. 73
Spruit et al 36 followed the study by Burkus et al 73 with a cross-sectional study of single-level (L4-5 or L5-S1) lumbar interbody fusions using titanium alloy cages (SynCage: Mathys Medical Ltd) packed with morselized ICBG. The authors assessed postoperative CT data by measuring HUs with a specific ROI that focused on the intradevice fusion mass. The study examined fusion masses among 21 patients at various time points spanning 1 to 44 months after surgery. The authors found an interclass coefficient of 0.97 for measuring HUs. Each HU measurement was plotted against time and a linear regression estimated an initial BMD of 615 HU that averaged an increase of 7.5 HU per postoperative month. 36 While the variability inherent in comparing measurements across time from different vertebral levels in different patients makes the average change in HU difficult to interpret, this study demonstrated a high interclass coefficient among raters using CT to measure BMD within an interbody device, implying a role for evaluation of postoperative fusion-mass progress using HUs.
Hartmann et al 74 evaluated 35 patients undergoing anterior thoracolumbar fusion with titanium cages (Synex; Synthes Inc.) in the setting of trauma. All underwent autologous interbody bone grafting alongside cages, some with local administration of platelet-rich plasma. The patients were followed with CT scans of the spine and the graft-bone interface was analyzed. Assessment was performed on the fusion masses using site-specific ROIs and HU analysis. While there was no significant difference in fusion rates, absolute bone density of the platelet-rich plasma group was found to be higher than the control group (639.7 vs 514.2 HU), again suggesting the potential role in monitoring and comparative analysis of fusion mass density via HU analysis. 74
It should be noted that in 3 of the above studies using interbody cages, all used conventional CT scans to assess and measure bone formation within or adjacent to a metallic interbody cage. While the authors were able to measure differences in fusion mass density over time, this was done under the assumption that any artifact created by the metallic implants was constant. Burkus et al 73 adjusted ROIs to be >3 mm from the walls of the metallic device to help mitigate artifact, 75 Spruit et al 36 used metal reduction postprocessing of CT images, and Hartmann et al 74 merely excluded the metal implant from the ROI. Readers should be cautioned that BMD inference from HU analysis in the setting of metal artifact is an unresolved issue, given the propensity of “streaking” to artificially increase HUs of tissues near metal object. 76
Meredith et al 77 performed a retrospective case-control study on adults undergoing posterior spinal fusion for deformity who subsequently suffered a fracture at the terminal instrumented vertebra or the adjacent vertebral level of the construct. All adults undergoing surgery had preoperative CT scans of the spine within 6 months of the index procedure. HU analysis at the preoperative fracture site and global spine average were calculated for each case and control according to the method described by Schreiber et al. 25 The authors found that the cases had lower average BMD (HU) at the fracture site than controls, 145.6 versus 199.4 HU, P = .006. In addition, global thoracolumbar spine BMD was lower in the cases than controls 139.9 HU versus 170.1, P = .032. 77 The authors concluded that preoperative BMD analysis via HU measurement can be used to screen for fracture risk at terminal or adjacent segments in posterior fusions for adult spinal deformity.
Similar to Meredith et al, 77 Uei et al 3 retrospectively reviewed 54 adult spinal deformity patients who had undergone posterior spinal fusion of at least 4 levels. DXA and spine CT were performed within 3 months of surgery. Patients were divided into cases requiring revision surgery (n = 14) and controls who did not require revision (n = 40) for proximal junctional kyphosis or vertebral fracture. The authors found that preoperative lumbar DXA was no different between the 2 groups. However, the authors found that BMD (via HU analysis) at T8 and T9 was significantly lower in the revision group and that pedicle screw loosening at the uppermost level was significantly correlated with needing revision surgery. Interestingly, the revision group had higher BMD per HUs at L4 and L5, which the authors attributed to increased spondylotic sclerosis. 3 Nonetheless, the authors demonstrated the ability of oCT to correlate to postfusion outcomes where DXA lacked significance.
In summary, though there is a paucity of literature directly evaluating the role of CT in postfusion radiographic evaluation and ORCs, existing studies show potential power of site-specific CT analysis to assess the quality of fusion mass and stratify risk factors for postsurgical complications. As with the use of oCT for osteoporosis detection, more research must be performed to help establish standardized protocols that can produce normative data to inform surgical planning and decision making.
Virtual Stress Testing in Spine Surgery
As noted above, VST is based on FEA of bone data acquired by CT and represents an additional analytical tool beyond a traditional oCT. Known clinically as biomechanical computed tomography (BCT), it can serve as a powerful tool to assess, predict, and design fusion/instrumentation of the spine. BCT is a calibrated approach to defining bone density and strength that has been validated for the diagnosis of osteoporosis. Its more robust analytics has undergone and has withstood the scrutiny of regulatory bodies. It stands as one of 3 approved methods for diagnosing osteoporosis.
Various authors have shown that BCT can accurately predict screw pull-out strength, 78 identify patients preoperatively who are at risk for ORCs, 79 inform device manufacturers on failure mechanisms for spinal implants, 80 and test virtual models of spine fusion to find optimal indications for a particular surgery. 18 While the above studies support the use of BCT in evaluating vertebral bone–screw interfaces and properties, there is a paucity of data supporting clinical application, particularly in spine surgery. Burch et al 79 performed a retrospective cross-sectional analysis of vertebral bone quality on spine fusion patients. Utilizing the preoperative CT scans for a cohort of women planning to undergo spine fusion, the authors utilized phantomless preoperative CT scans to estimate vertebral bone mineral density via HU analyses, and to simulate vertebral compressive strength in L1 and L2 via BCT. Using previously established thresholds for osteoporosis (trabecular BMD 80 mg/cm3) and fragile bone strength (vertebral strength of 4500 N or less); it was found that 29% were classified as having either osteoporosis or fragile bone strength. 79 In a nonspine series, Petfield et al 17 retrospectively predicted clinical failure of comminuted tibia shaft fracture healing in soldiers with a sensitivity of 100% and specificity of 76.8% using VST. 17
These studies present the potential for further spine-specific and nonspine-specific investigations to use BCT techniques with oCT images to predict and reduce ORCs. Application and expansion of BCT techniques may be the critical link for functionalizing the vast imaging data available from opportunistic sources for accurate prediction of adverse outcomes and guided preoperative bone health interventions.
Summary
DXA, the current clinical standard for diagnosing osteoporosis, has inherent limitations, especially in the spine surgical patient. Some of these limitations can be overcome with CT data. Most surgical patients have readily available CT data of the spine for opportunistic use. The studies reviewed in this article, while potentially biased by nonsystematic inclusion criteria, collectively suggest that oCT analysis represents an underutilized resource that has the potential to improve spine surgical outcomes by identifying at-risk patients and best practices for performing spine surgery in patients with diminished bone quality. Work is still left to solidify the clinical utility of this concept, for example, specific HU thresholds capable of diagnosing osteoporosis or predicting ORCs have been postulated (Tables 1-3) but are yet to be validated. That said, the collective published experience with oCT data in adult spine patients is promising and suggests that it may be a more reliable technique to find and predict VCFs and ORCs. In addition, evidence supports its use to evaluate the quality of screw trajectories and fusion mass in spine surgery. Last, VST is a powerful tool that exists today and has been demonstrated to be predictive of ORCs in spine surgery. To date, this powerful technology has been relatively unexplored and underutilized in the prediction of adverse events in adult spinal deformity patients. It too deserves further prospective research to define its best use in spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.