
Abstract
Objective
We aimed to assess hypertension prevalence and management in Central China.
Methods
In this cross-sectional study conducted from February 2019 to February 2020, we applied stratified multistage random sampling to investigate residents aged 35 to 75 years in Dancheng county of Zhoukou city and Xincai county of Zhumadian city, both in Central China.
Results
We enrolled 63,940 participants in this survey. A total of 43.6% (95% confidence interval [CI]: 43.2–44.0) of participants had hypertension. Of these, 49.3% (95% CI: 48.7–49.9) were aware of their diagnosis, 36.5% (95% CI: 35.9–37.1) took antihypertensive medication, and 14.3% (95% CI: 13.9–14.7) had their blood pressure under control. Only 31.4% of hypertensive people receiving antihypertensive treatment had achieved control. The hypertension prevalence was lower in urban areas than in rural areas, with higher rates of awareness, treatment, and control. Among subgroups, rural men had the highest prevalence of hypertension. Prevalence, awareness, and treatment rates all increased with age, except for control rates, which declined in the 65- to 75-year-old group.
Conclusions
People in Central China have a high hypertension prevalence but low rates of awareness, treatment, and control. Great effort is needed to improve the prevention and management of hypertension in this region.
Introduction
Hypertension (HTN) is the most common chronic noncommunicable disease and the largest single factor leading to the global burden of disease and global mortality. Approximately 9.4 million people die from HTN-related diseases each year, of which cardiovascular diseases account for more than 70%. 1 In China, high systolic blood pressure (SBP) accounted for 2.54 million deaths in 2017, and cardiovascular diseases gave rise to 95.7% of these deaths. 2 As reported in surveys conducted in China, the prevalence of HTN has continued to rise, and prevention and management of HTN needs to be further improved.3–5 It is urgent to assess epidemic trends and characteristics as well as to formulate scientific measures to reduce the occurrence of HTN-related cardiovascular diseases.
Central China is one of the seven geographic divisions in China and includes Henan, Hubei, and Hunan provinces. This region is in the central part of China and is characterized by a large population base and high population density. As the most populated (99.0 million in 2019) province in Central China, Henan has a high proportion of rural residents (46%). 6 To obtain the latest information regarding the prevalence and management of HTN in Central China, we used 2019 Henan survey data to describe the status of HTN prevalence, awareness, treatment, and control. Previous studies have suggested that there are geographic differences concerning HTN prevalence in China, but regional inconsistencies remain with regard to urban–rural differences.5,7 Therefore, to clarify these inconsistencies, in the current study, we investigated HTN-related situations according to subgroups of age, sex, and residential area.
Methods
Study design and participants
The current study was a cross-sectional survey conducted from February 2019 to February 2020. Using stratified multistage random sampling, eight districts (or townships) were selected from Dancheng county of Zhoukou city and Xincai county of Zhumadian city, both in Henan Province, Central China. Then, six villages or communities were selected from each district or township. We collected demographic information, including age and sex as well as history of HTN and use of antihypertensive medication.
The medical ethics committee at Henan Provincial People’s Hospital approved the study (02-Jan-2018, 2017(58)). Participants in this study provided verbal informed consent. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 8
Measurement of blood pressure (BP)
BP was measured using a medical BP meter (Maibobo RBP-9807; Shenzhen Raycome Technology Co., Ltd., China). Before measuring BP, participants rested for 5 minutes and were asked to avoid any obvious postural changes and emotional agitation. With the participant in a seated position, BP was consecutively measured on the right arm at 1-minute intervals. If the difference in systolic blood pressure (SBP) values between two measurements was greater than 10 mmHg (1 mmHg = 0.133 kPa), then a third measurement was taken. BP values of the latter two measurements were recorded and used for analyses.
Definitions
HTN was defined as SBP ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg, or a history of HTN (previously confirmed HTN or administration of antihypertensive medication 2 weeks before BP measurement). 9 HTN prevalence was defined as the proportion of hypertensive residents among the general population recruited in this study.
HTN awareness referred to a self-reported history of HTN (previously confirmed HTN or use of antihypertensive medication 2 weeks before BP measurement). The awareness rate referred to the proportion of people who were aware that they had HTN among respondents who had HTN. Treatment was defined as self-reported administration of antihypertensive medication 2 weeks before BP measurement. The treatment rate entailed the proportion who were treated for HTN among hypertensive respondents. Control was defined as SBP <140 mmHg and DBP <90 mmHg, and the control rate was defined as the proportion of participants who had achieved the control standard among hypertensive respondents. The medication control rate referred to the proportion who had achieved the control standard among hypertensive respondents who were taking antihypertensive drugs.
Statistical analysis
We used IBM SPSS 20.0 software (IBM Corp., Armonk, NY, USA) for statistical analysis. All personal information had been de-identified and participants with missing data were excluded prior to the analysis. All reported rates in this article were standardized directly for age, sex, and/or residential area. Continuous variables are expressed as mean ± standard deviation and compared using one-way ANOVA; a Games–Howell test was used for multiple comparisons. Categorical variables are presented as percentages and analyzed using the chi-square test; the Bonferroni method was used for multiple comparisons. The trend chi-square test was used to assess trends across subgroups. Logistic regression was performed to evaluate the influence of geographic factors and interactions on HTN prevalence. A two-sided test was used and P < 0.05 was considered statistically significant.
Results
General characteristics
A total of 63,940 participants were enrolled, after excluding 418 residents with missing data for BP and other variables. Mean age was 55.3 ± 9.8 years (range 35–75 years), and 25,198 (39.4%) participants were men. In total, 16,398 (25.6%) participants reported that they had been diagnosed with HTN or were taking antihypertensive drugs. Among the total, mean SBP was 134.4 ± 19.0 mmHg, and mean DBP was 81.3 ± 11.1 mmHg. Average SBP/DBP was 136.1/82.7 mmHg in rural areas and 132.7/79.9 mmHg in urban areas (P < 0.01). SBP levels increased with age (F = 7083.7, P < 0.01). SBP among men younger than age 55 years was higher than that among women in the same age group; after age 55 years, SBP was higher in women. There was no linear relationship between DBP and age. The data are detailed in Table 1 and Figure 1a.
Blood pressure levels and hypertension prevalence.
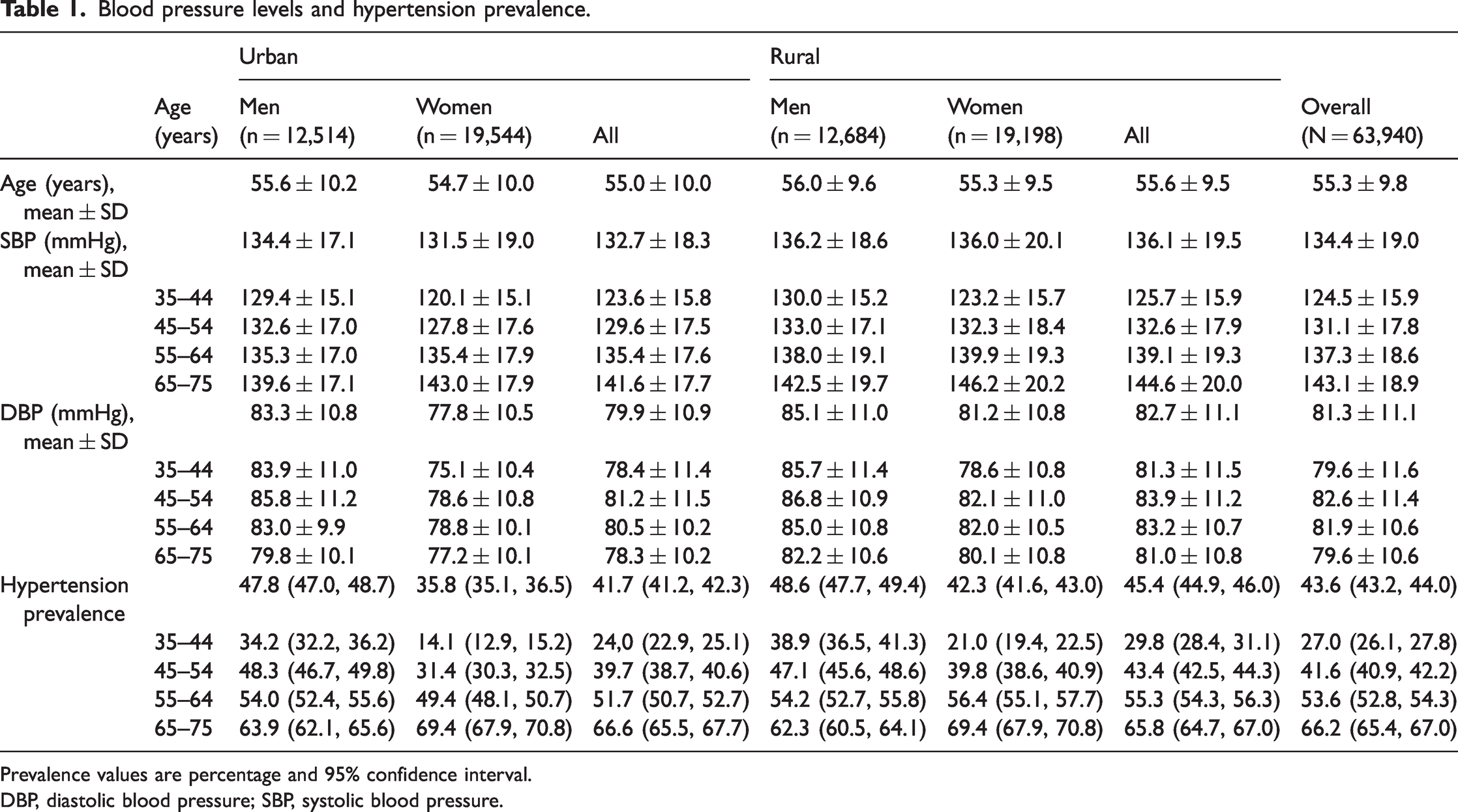
Prevalence values are percentage and 95% confidence interval.
DBP, diastolic blood pressure; SBP, systolic blood pressure.

Prevalence, awareness, treatment, and control of hypertension in different groups. (a) Mean systolic blood pressure (SBP) among participants by sex and residential area. (b) Hypertension prevalence by sex and residential area. Ptrend < 0.01 in four subgroups. (c) Prevalence, awareness, treatment, and control of hypertension by sex and residential area. Φ, compared with women in urban areas (P < 0.05);*, compared with men in rural areas (P < 0.05); #, compared with women in rural areas (P < 0.05) and (d) Prevalence, awareness, treatment, and control of hypertension by age.
Overall, 30,094 participants had a history of HTN or SBP/DBP of at least 140/90 mmHg. Awareness of HTN was reported by 16,398 hypertensive participants, with 12,558 taking antihypertensive drugs and only 4742 being controlled.
HTN prevalence
In total, the HTN prevalence was 43.6% (95% CI: 43.2–44.0). HTN prevalence in urban areas was 41.7% (95% CI: 41.2–42.3), and the prevalence in rural areas was higher at 45.4% (95% CI: 44.9–46.0; χ2 = 87.3, P < 0.01). After adjusting for age and sex, the difference in HTN prevalence between urban and rural areas was still significant (unadjusted odds ratio [OR] = 1.20, 95% CI: 1.16–1.24, adjusted OR = 1.18, 95% CI: 1.14–1.22; both P < 0.01).
Participants were divided into four subgroups according to sex and residential area: men in urban areas (MU), women in urban areas (WU), men in rural areas (MR), and women in rural areas (WR). The difference in HTN prevalence among the four groups was significant (χ2 = 693.0, P < 0.01), being highest among MU and MR and lowest among WU (all P < 0.05; Table 1 and Figure 1c). The HTN prevalence among WR exceeded that in MR older than age 55 years. The HTN prevalence among WU and WR exceeded that in both MU and MR older than age 65 years. HTN prevalence tended to increase with age (χ2trend = 4132.9, P < 0.01), and the highest was in the age group 65 to 75 years. The growth trend was more significant in women (Pinteraction < 0.01 (Table 1 and Figure 1b).
HTN awareness
The rate of awareness about an HTN diagnosis among all participants with HTN was 49.3% (95% CI: 48.7–49.9); this rate was higher in urban areas (55.4%, 95% CI: 54.6–56.2) and lower in rural ones (43.6%, 95% CI:42.8–44.4). After categorization by sex and residential area, the difference in HTN awareness among the above four groups was significant (χ2 = 376.8, P < 0.01), with the highest in urban groups and the lowest in the MR group (all P < 0.05, Table 2 and Figure 1c). HTN awareness tended to increase with age (χ2trend = 528.3, P < 0.01), and the highest was in the group aged 65 to 75 years (Table 2 and Figure 1d).
Hypertension awareness, treatment, and control in subgroups (sex, residential area, and age).

Values are percentage and 95% confidence interval.
*Among the total participants with hypertension. †Among participants who were aware that they had hypertension. #Among participants receiving treatment.
HTN treatment
Among all participants with HTN, the rate of HTN treatment was 36.5% (95% CI: 35.9–37.1). This rate was higher in urban areas than in rural ones (42.5% vs. 30.9%, χ2 = 404.8, P < 0.01). In urban and rural areas, there was no significant difference in HTN treatment between men and women in urban and rural areas (Figure 1c). The rate of HTN treatment in respondents who were aware that they had HTN was significantly higher than the rate among the total participants with HTN (72.7% vs. 36.5%, χ2 = 4834.0, P < 0.01, Table 2). Among all participants with HTN, HTN treatment tended to increase with age (χ2trend = 536.9, P < 0.01), and the highest was in age group 65 to 75 years (Table 2 and Figure 1d).
HTN control
HTN control rates were 14.3% (95% CI: 13.9–14.7) among all hypertensive participants and 31.4% (95% CI: 30.0–32.8) among those who received treatment. Participants from urban areas were more likely to have controlled HTN than those living in rural areas (control: χ2 = 291.0, medication control: χ2 = 73.5, both P < 0.01). There was no significant difference in HTN control between men and women in urban or rural areas (Figure 1c). HTN control among people who were aware that they had HTN was significantly higher than in the total population who had HTN (28.3% vs. 14.3%, χ2 = 1180.1, P < 0.01; Table 2).
Discussion
In this study, we set out to describe HTN prevalence, awareness, treatment, and control among residents in Central China during 2019 and to investigate differences in HTN prevalence and management by subgroups of age, sex, and residential area. The mean SBP/DBP among all participants was 134.4/81.3 mmHg, which was at the high-normal level (120–139/80–89 mmHg) as defined in the 2018 Chinese guidelines for the prevention and treatment of HTN. 9 This value reached HTN stage 1 (130–139/80–89 mmHg) as defined in the 2017 American College of Cardiology/American Heart Association guideline for high BP. 10 Mean SBP increased linearly with age. Before age 55 years, men had higher SBP, similar to the results of a previous survey. 11
The overall HTN prevalence was 44.7% in the China PEACE study, a population-based screening project that enrolled approximately 1.7 million adults aged 35 to 75 years from all 31 provinces in mainland China during 2014 to 2017. 12 A prior survey conducted among residents aged 30 to 79 years by the China Kadoorie Biobank project (a prospective cohort of chronic diseases in China, 2004–2008) also showed that HTN prevalence in Henan (Central China) was 40.2%, which was at a high level and only slightly lower than the highest prevalence of 44.4% in Zhejiang (Eastern China). 13 In this study, the HTN prevalence in Central China was high at 43.6%, showing that preventive measures to control the incidence of HTN are needed.
Based on previous studies, rural residents have a significantly lower HTN prevalence rate, and the gap gradually narrowed from the 1990s to 2010 in comparison with people living in urban areas. 14 Although the China Hypertension Survey in 2012 to 2015 found no significant difference in prevalence between urban and rural areas of China, these differences could be found in some provinces. 5 The Prospective Urban Rural Epidemiology study surveyed people aged 35 to 70 years from 2005 to 2009 and found that the HTN prevalence in rural areas was higher than that in urban areas. 15 Consistent with these results, the HTN prevalence in rural areas was significantly higher than that in urban areas (45.4% vs. 41.7%) in our study. These findings suggest that increased attention is needed in rural areas, especially in specific geographic regions, with intensive measures in HTN prevention. Inconsistency among study findings may be owing to the large difference in urbanization levels among different regions (provinces or cities) of China. 6 For example, Beijing (North China) has more urban areas than Henan; this topic requires further discussion and research. Furthermore, we analyzed the HTN prevalence according to age, sex, and residential area. Male and rural residents had poorer HTN prevention. It is worth noting that HTN prevalence among women over age 55 years exceeded that of men, which was similar to the change trend for SBP levels.
To our knowledge, HTN awareness, treatment, and control rates are lower in low- and middle-income countries than in high-income countries and are higher in urban areas compared with rural ones in low- and middle-income and low-income countries.16,17 A comparative study among people aged 45 to 75 years revealed a large gap in HTN treatment (46.8% vs. 77.9%) and control (20.3% vs. 54.7%) between China and the United States. 18 The rate of awareness may be somewhat limited by the fact that few individuals have their BP checked either in self-testing or primary health care in China. Although antihypertensive drugs are widely used in China, availability of medications, inefficient treatment, and high costs are possible barriers to improving HTN management levels, especially in rural areas.16,19–21 Our study showed that the awareness, treatment, and control rates in Central China were 49.3%, 36.5%, and 14.3%, respectively. However, these rates did not reach the national level according to a survey conducted from October 2012 to December 2015 (46.9%, 40.7%, and 15.3%) 5 and were much lower than those in the United States.16–18,22 Less than half (49.3%) of respondents with HTN were aware of their diagnosis and not all individuals who self-reported HTN were taking antihypertensive medications. An important problem that emerged from these data is that only a few hypertensive individuals (14.3%) and only approximately one-third (31.4%) of people who took antihypertensive drugs had controlled BP. Furthermore, the treatment and control rates of participants who were aware that they had HTN were 72.7% and 28.3%, respectively, which has important implications for target measures to improve HTN management. For sex and residential area, the situation in rural areas was worse than that in urban ones (Table 2), and we found a significant difference in HTN awareness between rural men and women. In accordance with the present results, previous studies have demonstrated that HTN detection and medication use among rural adults is suboptimal, which deserves the attention of health policymakers and researchers.14,16
Aging is an important and irreversible contributor to the incidence of HTN. 23 It is estimated that the number of elderly people aged over 65 years in China will reach 400 million (26.9% of the total population) by 2050. 24 In our study, the HTN prevalence rose with increasing age, and the highest was 66.2% in people aged 65 to 75 years. We also analyzed associations between age and HTN awareness, treatment, and control. Our findings revealed that awareness and treatment rates rose with increased age, but a decline in the rate of HTN control was found among people aged 65 to 75 years. These findings suggested that future research should focus not only on identifying efficacious methods to improve HTN control but also on how to prevent potential health events posed by HTN at older ages. Various methods and approaches need to be considered to reduce HTN-related diseases and economic burdens caused by aging.25,26
The present study has several limitations. First, the survey area included in this study is limited because it is very difficult to conduct large-scale multi-center research studies in a short period of time. We attempted to increase the sample as much as possible to alleviate the problem of representation. Second, we did not have access to the patients' medication details for an analysis of HTN control in relation to medication classification.
The prevalence of HTN continues to rise in China and BP remains poorly controlled. Our study results suggest that appropriate measures must be taken and promoted for comprehensive improvement in HTN prevention and control. Given the large geographic and urbanization gaps in China, more targeted policies to address the management of HTN are necessary.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221148905 - Supplemental material for Prevalence and management of hypertension in Central China: a cross-sectional survey
Supplemental material, sj-pdf-1-imr-10.1177_03000605221148905 for Prevalence and management of hypertension in Central China: a cross-sectional survey by Wenlu Xing, Shan Wang, Xinyun Liu, Jicheng Jiang, Qiuping Zhao, Yuming Wang, You Zhang and Chuanyu Gao in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank all members of the Scientific Committee and the Executive Committee for their contribution to this survey. We also thank all regional officers and research staff for data collection.
Author contributions
CYG, YZ, and YMW conceived this study. WLX, SW, XYL, JCJ, and QPZ were involved in data quality evaluation and data checking and management. WLX performed all statistical analysis. CYG, YZ, and YMW supervised the study. WLX wrote the initial draft of the manuscript. WLX, SW, YZ, and CYG were involved in critical revision of the manuscript. All authors reviewed the manuscript and approved the final version.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This survey was supported by the National Key Research and Development Program of China (2018YFC0114502).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.