
Abstract
Study design
Retrospective study.
Objectives
The aim of this study was to evaluate the outcomes of a new modified laminoplasty, intermuscular “raising roof” laminoplasty for patients with cervical spondylotic myelopathy.
Methods
98 patients with cervical spondylotic myelopathy were involved into the study, including 44 patients underwent intermuscular “raising roof” laminoplasty (RL) and 54 patients underwent unilateral muscle-preserve laminoplasty (UL). The data, including sagittal parameters and clinical scale was collected at preoperative stage and final follow-up (at least 2 years) and compared between RL group and UL group. Multivariable liner regressions were preformed to evaluate the relationship between parameters with significant changes at the final follow-up and changes of CL, postoperative NDI and JOA. The cumulative sum (CUSUM) analysis was used for quantitative assessment of RL learning curve. All cases were divided into the learning phase and the proficiency phase according to the peak of CUSUM curve.
Results
No significant difference was found between RL group and UL group preoperatively. At final follow-up, patients in RL group showed higher JOA scores and recovery rate (RR) but lower NDI scores. For the cervical alignment, the ROM of RL group was greater significantly than UL group, whereas the T1S of RL group was lower than UL group. For the decompression, the RL group had larger CSA of spinal canal than UL group (C4: 278.16 ± 50.40 vs 233.84 ± 42.71, P < .001; C5: 279.12 ± 63.88 vs 232.41 ± 48.38, P < .001). For the muscle-preserve effect, the CSA of left-side PM in RL group decreased significantly compared to the preoperative stage on C5 level (2.92 ± 0.66 vs 3.16 ± 1.08, P < .05), and RL group showed better postoperative symmetry than UL group. The regression results indicated postoperative CSA of right-side PM on C4 level had positive impact on the change of CL (positive value increasing, P = .023). And the postoperative symmetry of PM at C4 had positively correlation with postoperative NDI (P = .034). However, the ages of patients showed negative correlation (P = .012) with postoperative JOA. Operation time of learning phase was significantly longer than proficiency phase (166 ± 34.78 vs 120.65 ± 20.36, P < .001), and blood loss of learning phase was significantly higher than proficiency phase (251.90 ± 171.27 vs 148.88 ± 82.02, P < .001).
Conclusion
Compared to UL, RL showed similar recovery of neurological functions, but with better improvement of quality of life, cervical mobility and decompression effect at 2-year follow-up. It provides a new treatment approach for degeneration cervical myelopathy.
Introduction
Cervical spondylotic myelopathy (CSM) is a common degenerative disease of the cervical spine and a major cause of spinal cord dysfunction. 1 Patients with severe neurological deficits refractory to conservative treatment or progressive worsening of clinical symptoms require surgery as soon as possible. Posterior cervical open-door laminoplasty (LP), introduced by Hirabayashi et al, 2 has been widely used to treat multilevel CSM because of its proven efficacy in improving neurological function.
However, postoperative complications of open-door laminoplasty have been reported in many studies, including 9% - 44.6% incidence of axial symptoms,3,4 9.7% - 10.8% cervical kyphosis5,6 and nearly 100% incidence of decreased cervical range of motion (ROM). 7 Research increasingly recognized that these complications were associated with surgical damage to cervical posterior muscles. Therefore, how to protect more paraspinal muscles is becoming one of the most important directions of modifications. Lin et al 8 in our hospital reported the modified LP by preserving unilateral posterior paraspinal muscles at the hinge side (UL) was able to get less cervical curvature loss and better cervical alignment during 16.7-month follow-up than conventional LP. Chen et al found that, in addition to better cervical curve, preservation of the unilateral muscle-ligament complex would reduce postoperative neck pain and the incidence of postoperative axial symptoms compared with conventional LP. 9
Since 2019, the intermuscular “raising roof” modified cervical posterior laminoplasty (RL) has been performed in our hospital. Through a bilateral intermuscular approach without blunt separation of other parts of posterior muscles which attached to cervical vertebral lamina, two metal 3D-printed prostheses were used to raise the cervical lamina bilaterally in order to expand the spinal canal and decompress the cervical spinal cord. Additionally, RL also maintained the symmetry of the posterior muscles postoperatively. In this study, we aimed to retrospectively analyze the clinical and radiological outcomes of “raising roof” laminoplasty compared to unilateral muscle-preserve laminoplasty, to investigate the long-term clinical efficacy of this modified procedure.
Methods and Materials
The patients in Peking University Third Hospital were enrolled in this research. Inclusion criteria were: (1) diagnosed as multilevel CSM (affected segments ≥(3) based on symptoms, pathological signs and radiological results; (2) underwent UL from August 2010 to March 2015 or underwent RL from June 2019 to January 2021; (3) completed the 2-year follow-up postoperatively. Exclusion criteria were: (1) follow-up was less than 2 years; (2) combination of spinal trauma, tuberculosis or infection; (3) combination of anterior approaches; (4) history of neurological disorders; (5) presence of psychiatric conditions or cognitive impairments. This study was approved by the Ethics Committee of Peking University Third Hospital (M2022408). Age, gender, body mass index(BMI), number of affected segments and disease duration were collected as baseline information of patients.
Surgical Technique
Intermuscular “Raising Roof” Laminoplasty
After sterilizing surgical area and draping, the skin, subcutaneous tissue and ligamentum nuchae were cut through posterior median incision along the midline. Then nuchal fascia and trapezius muscle were dissected. Separating to the lateral side in the deep layer of trapezius muscle fascia to find the natural intermuscular space between Semispinalis Cervicis (SSCe) and Semispinalis Capitis (SSCa) (Figure 1A). After blunt dissection to the surface of lamina, parts of multifidus (MF) and rotator muscles were cut off to expose the junction between the lamina and the lateral mass. The lateral mass and the outer edge of the lamina were revealed. The outer cortical bone of the right lamina was resected with an ultrasonic osteotome on the medial aspect of the facet joint to create a hinge firstly (Figure 1B and C). And then on the left lamina, the entire layer of the lamina and ligamentum flavum was cut off (Figure 1D). The lamina was flipped to the right side and a custom 3D-printed artificial implants was placed between the left lamina and the lateral mass, and an electric drill was used to drill fixation holes on the left lamina and lateral mass (Figure 1G). The screws were inserted into the holes, but tightened incompletely at first. After cutting off the hinge and ligamentum flavum between right lamina and lateral mass, the lamina was flipped to the left side, and a 3D-printed artificial implants was put into the right-side junction (Figure 1H). Fixation holes were drilled and screws were inserted and tightened completely. Finally, tightening the left side screws completely and closing the incision with surgical suture. Surgical procedure of intermuscular “raising roof” laminoplasty. (A) Intermuscular exposure to the lamina. (B) Ultrasonic osteotome was used in surgery. (C) The outer cortical bone of the right lamina to create a hinge. (D) The entire layer of the left lamina and ligamentum flavum were cut off. (E) Lateral photograph of 3D-printed object. (F) Frontal photograph of 3D-printed object. (G) The 3D-printer object was put into the junction and locked by screws. (H) The fixation of 3D-printed objects had been finished. (I) Schematic diagram of the intermuscular “raising roof” laminoplasty.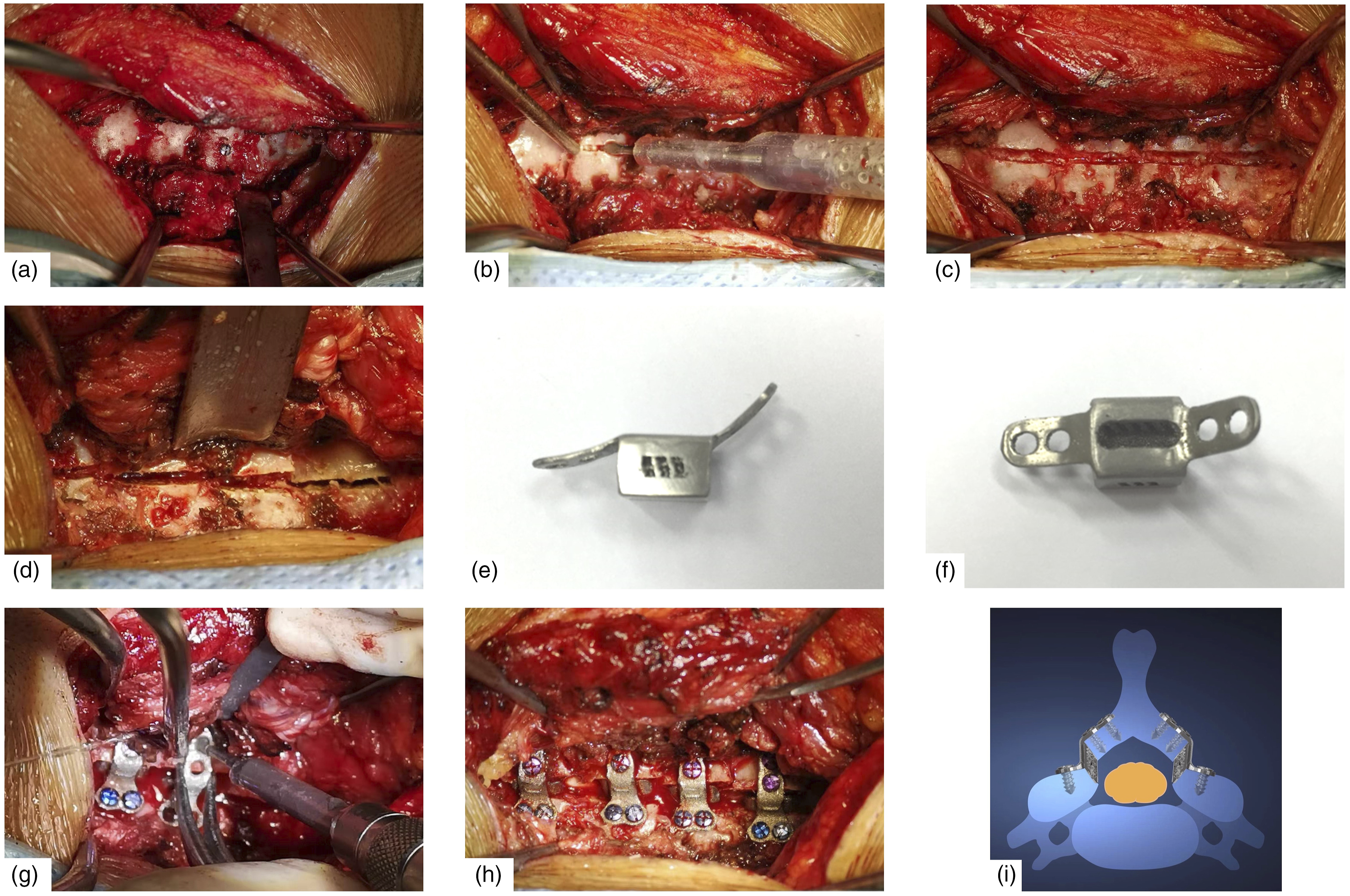
Unilateral Muscle-Preserve Open-Door Laminoplasty
After sterilizing surgical area and draping, the left paraspinal muscles were dissected to expose the left spinous process through posterior median incision along the midline. An electric saw was used to cut off the base of spinous process. At the junction between spinous process and its basilar part, separating the right paraspinal muscles from the lamina without cutting off the attachment between muscle and spinous processes. The spinous process, along with the attached right muscles was flipped to the right side to expose the junction between right lamina and lateral mass. The outer cortical bone of the right lamina was resected with an ultrasonic osteotome on the medial aspect of the facet joint to create a hinge. Then, on the left lamina, the entire layer of the lamina and ligamentum flavum were cut off. Then, the lamina was flipped to the right side. After that, one hole each was drilled with an electric drill on the spinous process and lateral aspect of the left lamina, and titanium cables were used to reconstruct and fix the spinous process-muscles complex to the lamina. The tension of right muscles would maintain the “door opening” to achieve decompression. Finally, the left-side muscles were sutured to the spinous process and the incision was closed with surgical suture (Figure 2). (A) 65-year-old male patient with CSM underwent intermuscular “raising roof” laminoplasty. Preoperative and postoperative (at final-follow) anteroposterior radiographs (A and F), lateral radiographs (B and G), lateral MR images (C and H), CT coronal planes (D and I) and MRI coronal planes (E and J).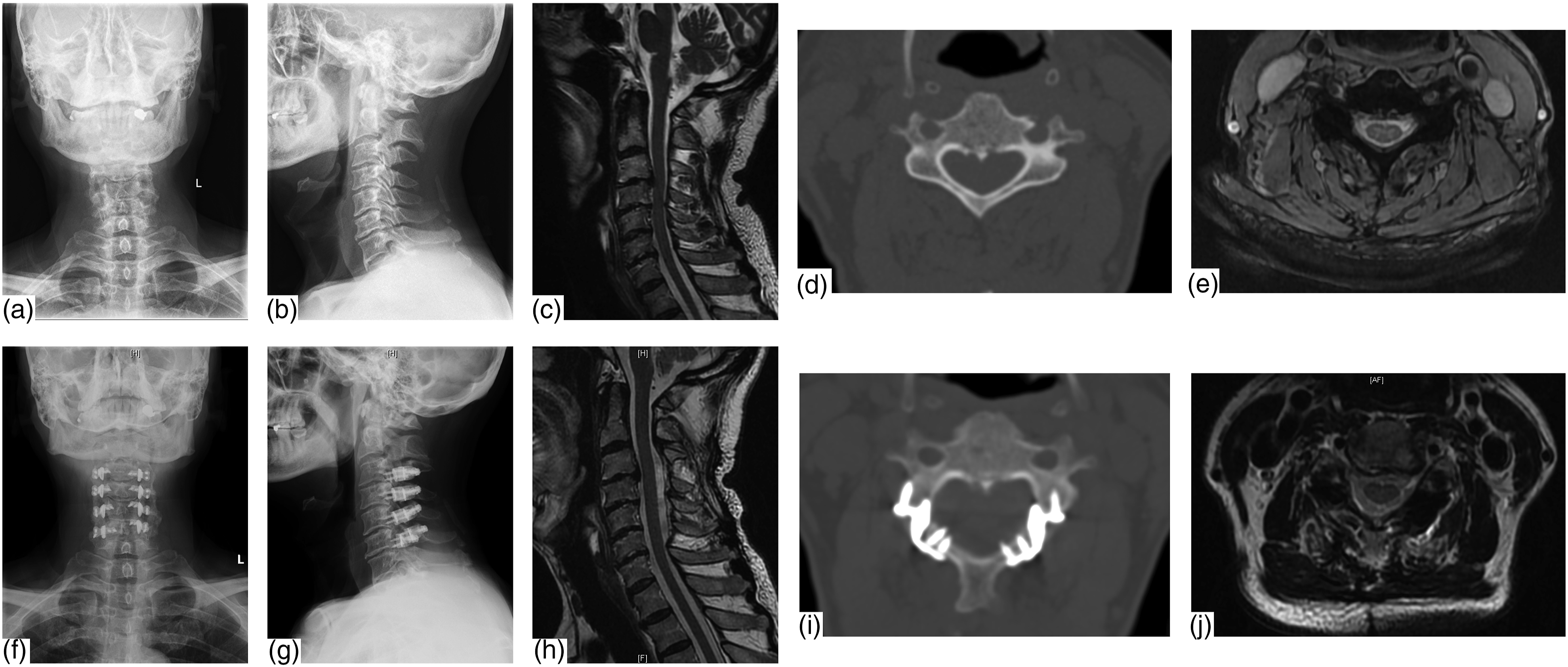
All surgeries were conducted by one experienced surgeon.
Clinical and Radiological Outcomes Evaluation
Patients with multilevel CSM was enrolled in a standardized follow-up protocal, including a short-term follow-up at 3 months and 6 months, and a long-term follow-up at 2 years. At each follow-up node, JOA score was recorded to evaluate neurological status, while NDI and VAS for neck pain were collected as functional outcomes. To complete the imaging assesment, the patients were also advised to undergo cervical lateral plain radiography, CT scan and MRI.
The clinical outcomes of cervical neurological functions were evaluated using the Japanese Orthopedic Association (JOA) score system at the preoperative stage and final follow-up (at least 2 years postoperatively). The recovery rate (RR) of the JOA score was calculated using the method by Hirabayashi et al (RR = (postoperative JOA score - preoperative JOA score) × 100/(17 - preoperative JOA score)). Minimal clinically important difference (MCID) was defined in previous article of our group which was defined as change of JOA >1.25 or RR of JOA > 31.25%. 10 Neck pain, defined as nuchal and/or scapular pain, was assessed by visual analog scale (VAS) score. The Neck Disability Index (NDI) was also used to assess the patients’ quality of life influenced by the neck pain. Incidences of complications were also calculated including new axial pain, cervical kyphosis, infection and readmission rate within 30 days.
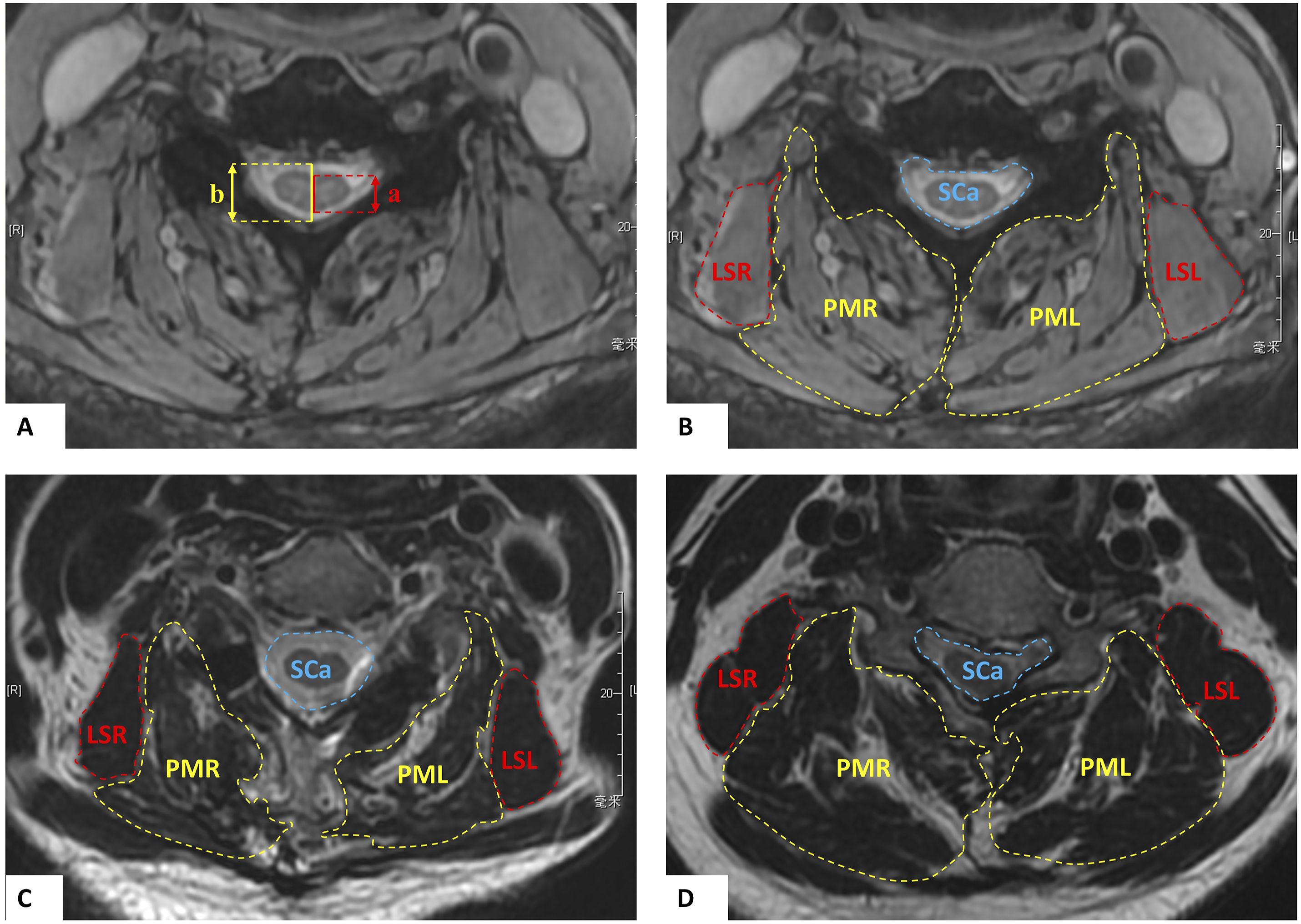
The cervical lordosis (CL), range of motion of the C2-7 Cobb angle (ROM), T1 slope (T1S), C2 to C7 sagittal vertical axis (SVA) were measured using Picture Archiving and Communication Systems (PACS) by lateral/flexion/extension plain radiography. CL was defined as the angle between the tangential lines along the posterior borders of the C2 and C7 vertebral bodies (Figure 3A). The ROM was defined as C2-7 Cobb angle between maximum flexion and maximum extension of cervical spine. The T1S was defined as the angle between the horizontal plane and a line parallel to the superior T1 end plate. The C2 to C7 SVA was measured as the distance from the posterosuperior corner of C7 to the plumbline from the centroid of C2 vertebral body (Figure 3B). The retention rate of ROM (Retention rate = postoperative ROM/ preoperative ROM) was calculated to assess the changes of ROM after surgery. Space available for cord (SAC), cross-sectional area (CSA) of spinal canal and CSA of posterior paraspinal muscles were used to assess the decompression effect of the surgery and paraspinal muscles atrophy after surgery on T2-weighted magnetic resonance imaging (MRI) using ImageJ imaging software. The region of interest (ROI) was manually segmented on MRI for the measurements of CSA. In this research, CSA of posterior paraspinal muscles were defined as the ratio of the area of muscle to the area of vertebral body minimize the effect of interindividual variation on the study results. Symmetry between left- and right-side muscles was calculated as the ratio of the CSA of right-side muscle to the CSA of left-side muscle. SAC was defined as sagittal diameter of the spinal canal minus sagittal diameter of the spinal cord (Figure 4A). The CSAs of posterior paraspinal muscles was categorized into posterior medial (PM) group and levator scapulae (LS) group (Figure 4B–D). PM group included multifidus, semispinalis and splinius, while LS group included levator scapulae. All measurements on MRI were carried out at the mid-level slices of C4 and C5 vertebral body because all surgeries of patients included these two segments. The cervical lordosis (CL), range of motion of the C2-7 Cobb angle (ROM), T1 slope (T1S), C2 to C7 sagittal vertical axis (SVA) were measured. (A) CL was defined as the angle between the tangential lines along the posterior borders of the C2 and C7 vertebral bodies. The ROM was defined as C2-7 Cobb angle between most flexion and most extension of cervical spine. (B) The T1S was defined as the angle between the horizontal plane and a line parallel to the superior T1 end plate. The C2 to C7 SVA was measured as the distance from the posterosuperior corner of C7 to the plumbline from the centroid of C2. Space available for cord (SAC) and the cross-sectional area (CSA) of posterior paraspinal muscles and spinal canal showed on MR images. (A) Length of a indicates the sagittal diameter of spinal cord (SDSCo). Length of b indicates the sagittal diameter of spinal canal (SDSCa). SAC was defined as SDSCa minus SDSCo. SAC = b – a. (B) Preoperatively. (C) After intermuscular “raising roof” laminoplasty at final follow. (D) After unilateral muscle-preserve laminoplasy. SCa indicates spinal canal; PMR, right-side of posterior medial muscles; PML, left-side of posterior medial muscles; LSR, right-side of levator scapulae; LSL, left-side of levator scapulae.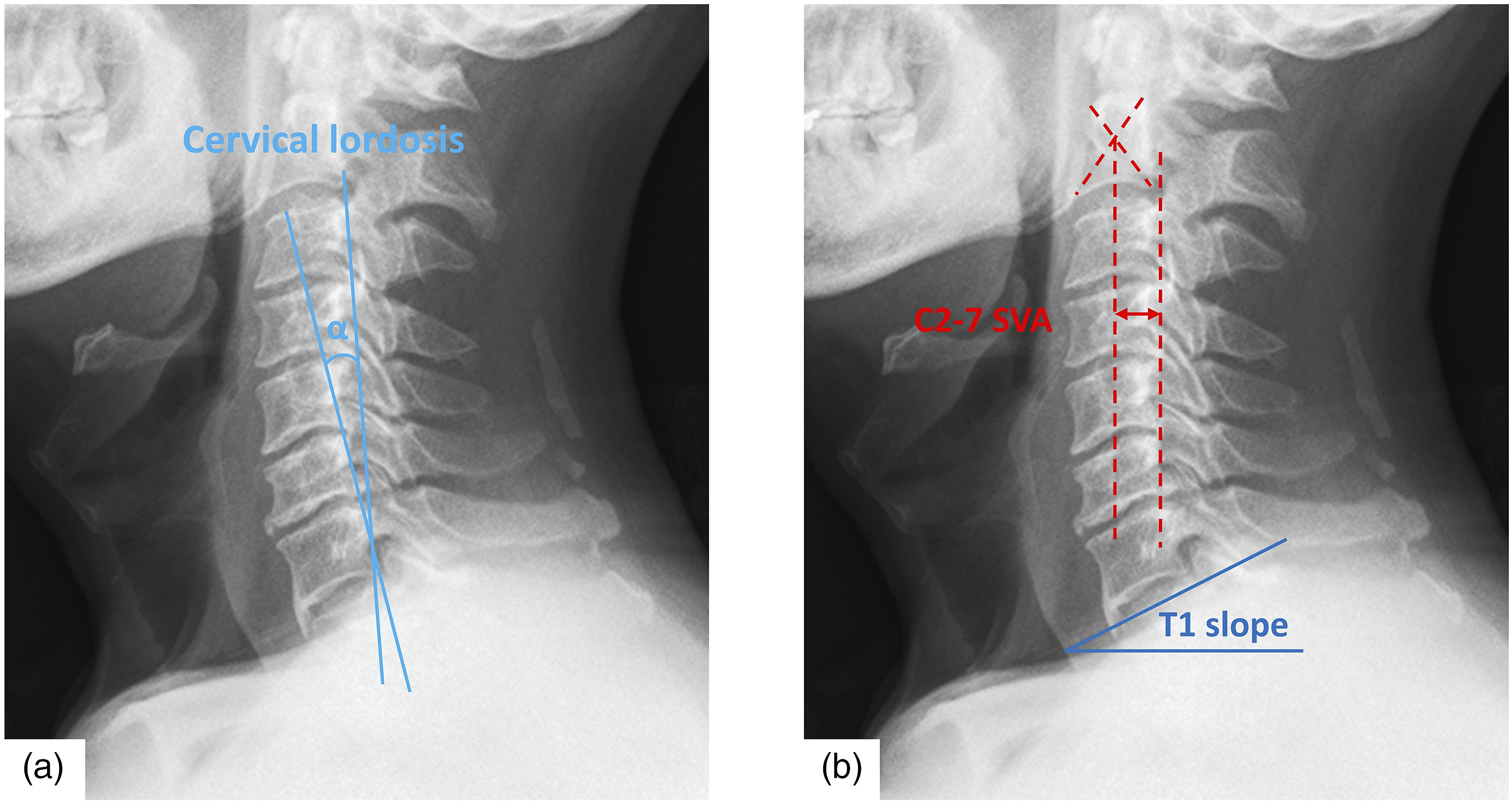
Cumulative Sum Analysis
The cumulative sum (CUSUM) analysis was used for quantitative assessment of RL learning curve. We collected operation time and blood loss of 126 cases who underwent RL in the same period as the above RL group, and cases were ordered chronologically from the earliest to the most recent date. The formula for CUSUM is as follows:

Statistical Analysis
All statistical analyses were carried out by IBM SPSS Statistics Version 27.0 software package (SPSS 27.0, Inc., USA). Distributions of variables were described as the mean (MD) and standard difference (SD). Student’s t test and analysis of variance (ANOVA) for continuous variables and Chi-square tests for categorical variables. Interobserver reliability of the radiograph measurement was analyzed using Intraclass Correlation Coefficient (ICC). For all statistical analyses conducted in this study, significance was defined by P-values < .05.
Results
Demographic and Baseline Characteristics of Patients.
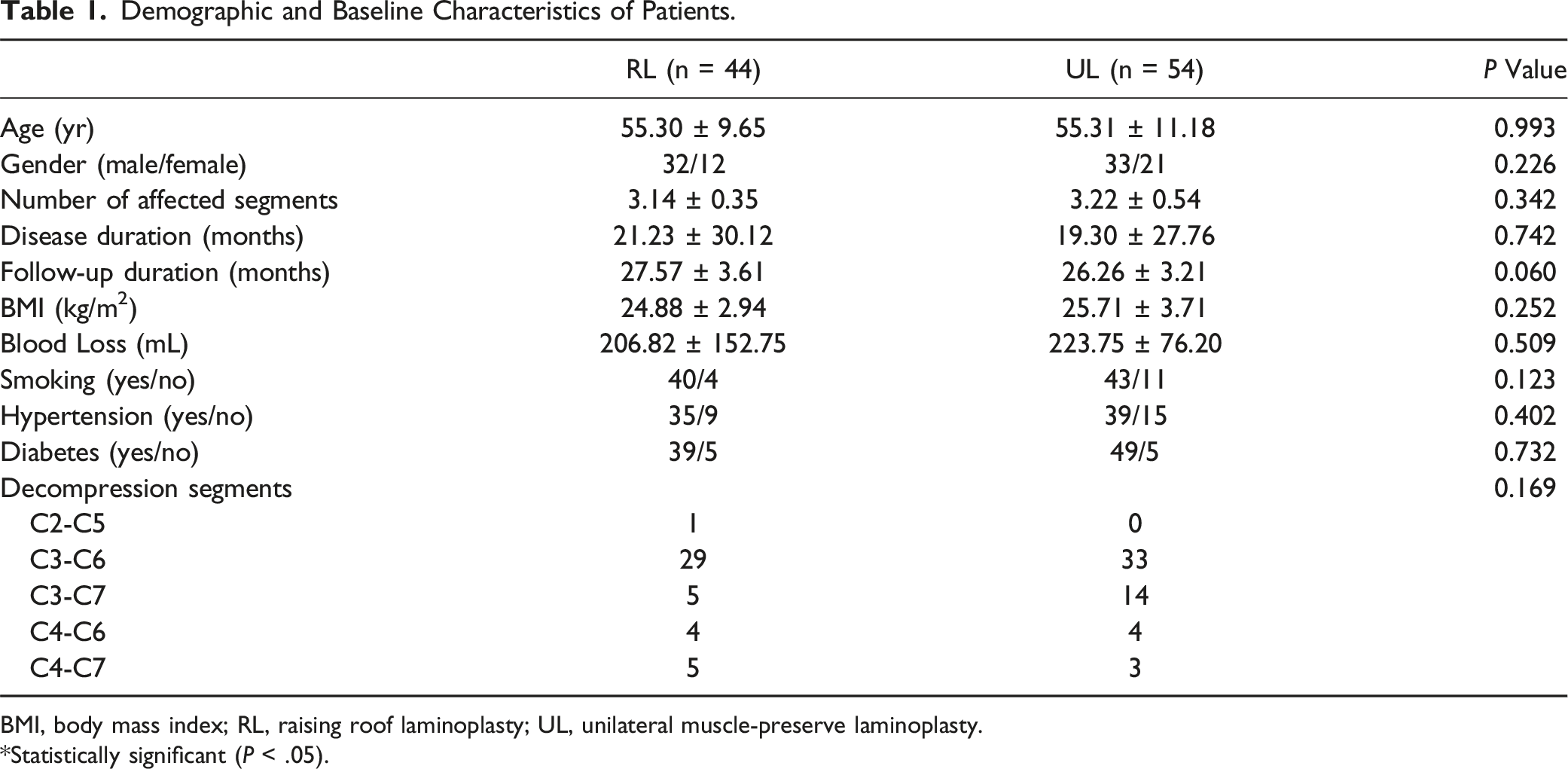
BMI, body mass index; RL, raising roof laminoplasty; UL, unilateral muscle-preserve laminoplasty.
*Statistically significant (P < .05).
Clinical Outcomes
Clinical and Radiological Outcomes and Complications of Patients.
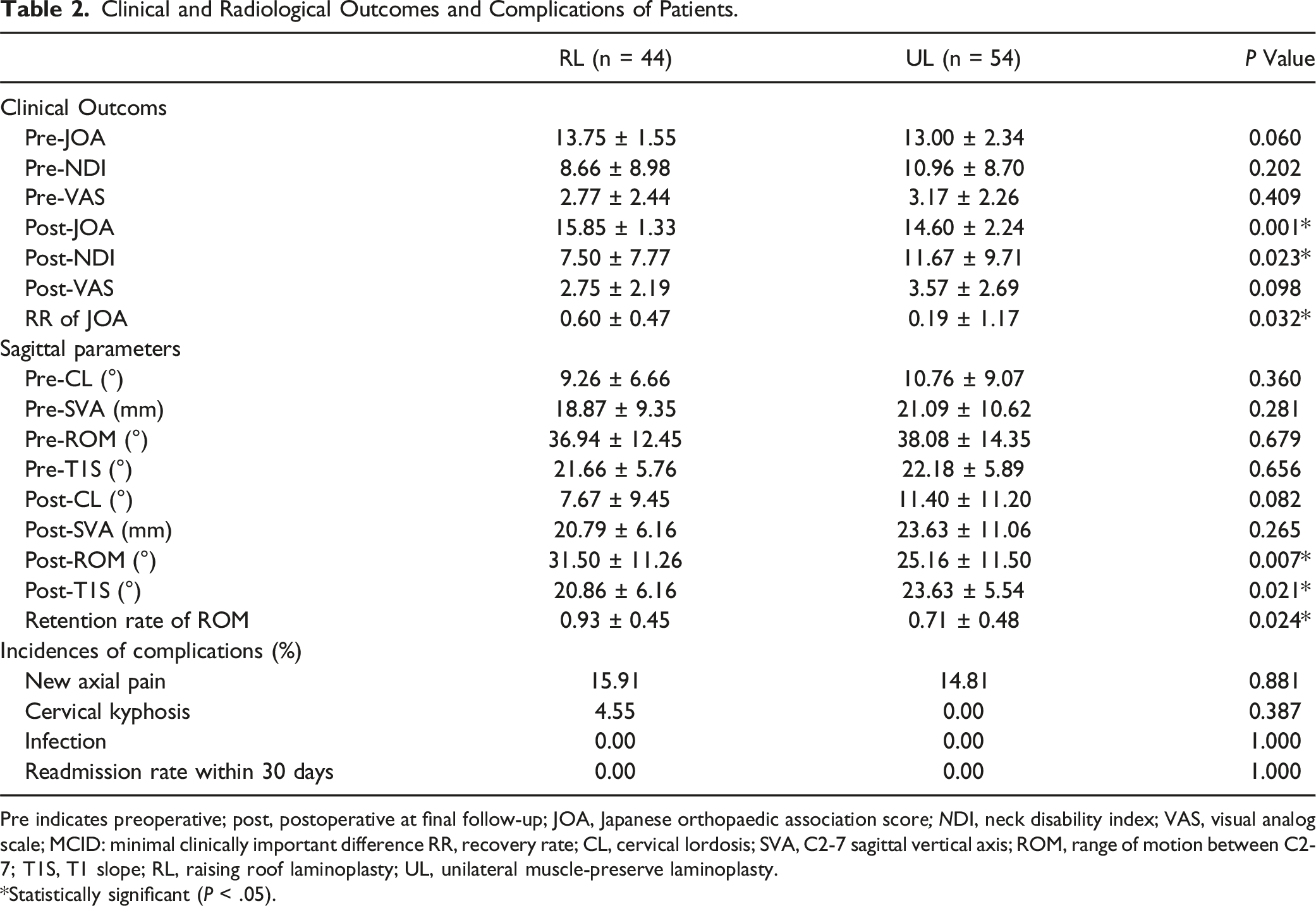
Pre indicates preoperative; post, postoperative at final follow-up; JOA, Japanese orthopaedic association score; NDI, neck disability index; VAS, visual analog scale; MCID: minimal clinically important difference RR, recovery rate; CL, cervical lordosis; SVA, C2-7 sagittal vertical axis; ROM, range of motion between C2-7; T1S, T1 slope; RL, raising roof laminoplasty; UL, unilateral muscle-preserve laminoplasty.
*Statistically significant (P < .05).
Radiological Outcomes
Preoperatively, there were no significant differences in sagittal parameters such as CL, C2-7 SVA, T1S, and ROM between the RL group and the UL group. Similarly, there were also no significant differences in CL and SVA at final follow-up between two groups. However, RL group showed a significantly higher ROM (31.50 ± 11.26 vs 25.16 ± 11.50, P = .007) and a significantly higher retention rate of ROM (0.93 ± 0.45 vs 0.71 ± 0.48, P = .024) at final follow-up compared to UL group. Conversely, T1S in UL group was significantly higher than RL group (20.86 ± 6.16 vs 23.63 ± 5.54, P = .021) (Table 2).
Comparison of the Posterior Paraspinal Muscles and Spinal Canal Between Two Groups at Preoperative Stage and Final Follow-Up.
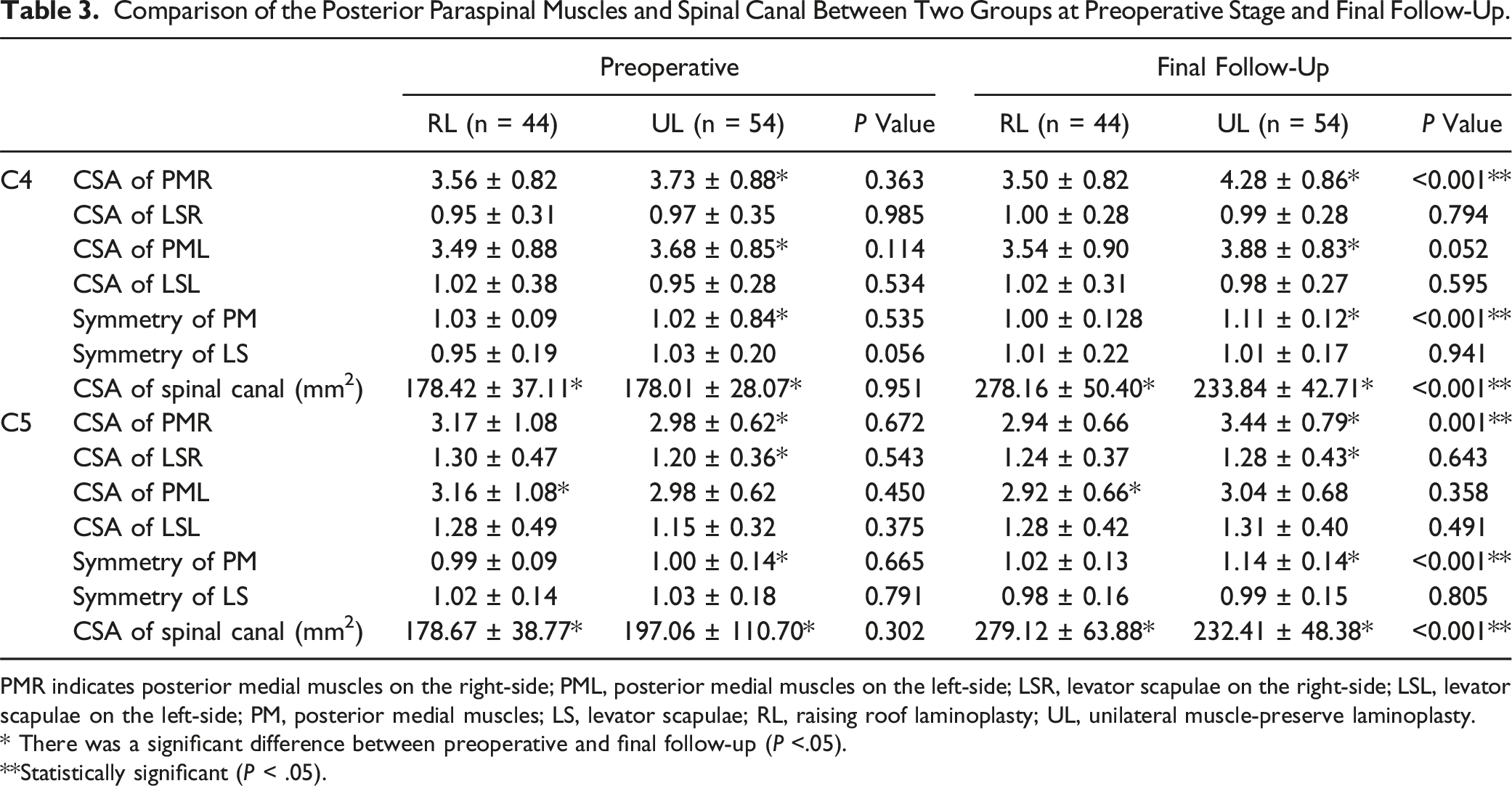
PMR indicates posterior medial muscles on the right-side; PML, posterior medial muscles on the left-side; LSR, levator scapulae on the right-side; LSL, levator scapulae on the left-side; PM, posterior medial muscles; LS, levator scapulae; RL, raising roof laminoplasty; UL, unilateral muscle-preserve laminoplasty.
* There was a significant difference between preoperative and final follow-up (P <.05).
**Statistically significant (P < .05).
As shown in Table 3, there was no significant difference of the CSA and symmetry of the posterior muscles (including PM and LS) between RL group and UL group preoperatively. At the final follow-up, interestingly, the CSA of right-side PM at both C4 (4.28 ± 0.86 vs 3.73 ± 0.88, P = .004) and C5 (3.44 ± 0.79 vs 2.98 ± 0.62, P < .001) level were larger than those preoperatively in UL group. However, the CSA of left-side PM, left and right-side of LS did not show significant difference at final follow-up compared with those preoperatively in UL group. Additionally, the CSA of PM and LS at both sides did not change significantly postoperatively in RL group. There was a significant difference in the symmetry of PM between RL group and UL group at the final follow-up (C4: 1.00 ± 0.128 vs 1.11 ± 0.12, P < .001; C5: 1.02 ± 0.13 vs 1.14 ± 0.14, P < .001), and RL group showed a better symmetry. The symmetry of LS showed no significant difference between two groups (Table 3).
Multivariable linier regression of change of CL, postoperative NDI and postoperative JOA.
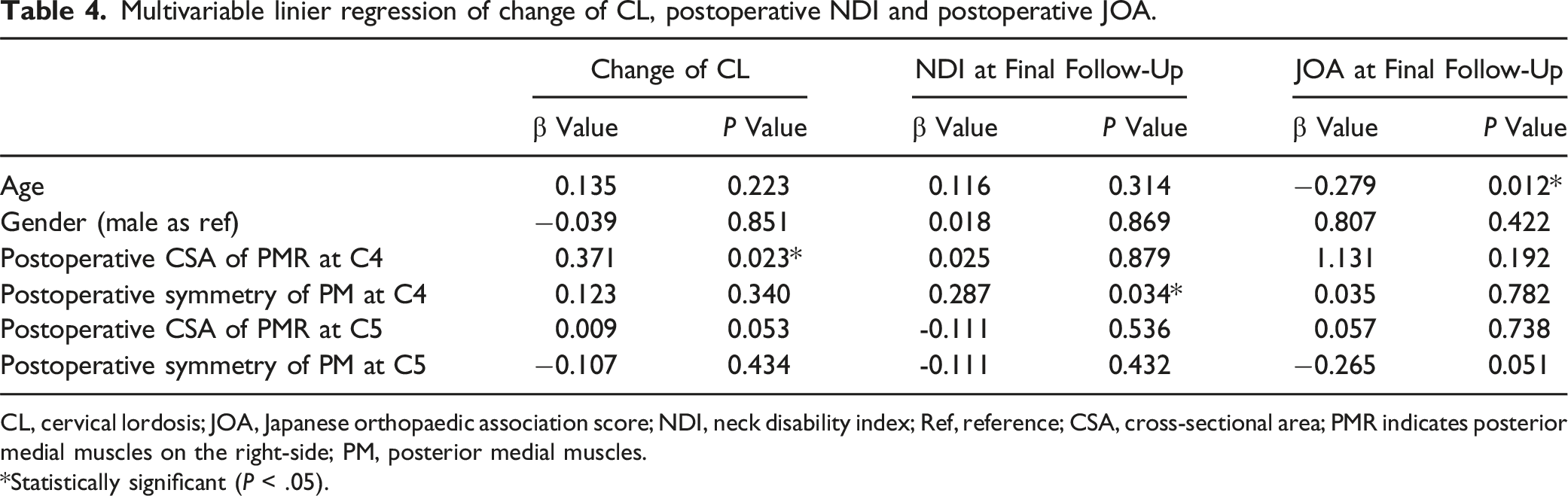
CL, cervical lordosis; JOA, Japanese orthopaedic association score; NDI, neck disability index; Ref, reference; CSA, cross-sectional area; PMR indicates posterior medial muscles on the right-side; PM, posterior medial muscles.
*Statistically significant (P < .05).
Learning Curve
CUSUM analysis indicated that both operation time and blood loss diminished after 58th case (Figure 5), and the learning curve was best modeled as a third-order polynomial with the follow equation: CUSUM(operation time) = 0.0008x3-0.5006x2 + 51.01x-149.3 (R2 = .942); CUSUM(blood loss) = 0.0023x3-1.093x2 + 102.1x + 31.84 (R2 = .899). All cases were divided into learning phase (n = 58) and proficiency phase (n = 68). Operation time of learning phase was significantly longer than proficiency phase (166 ± 34.78 vs 120.65 ± 20.36, P < .001), and blood loss of learning phase was significantly higher than proficiency phase (251.90 ± 171.27 vs 148.88 ± 82.02, P < .001). (Table 5) CUSUM of operation time and blood loss plotted against case number. The solid lines represent the best fit third-order polynomials. CUSUM indicates cumulative sum. Comparison of Operation Time and Blood Loss Between Two Phases. *Statistically significant (P < .05).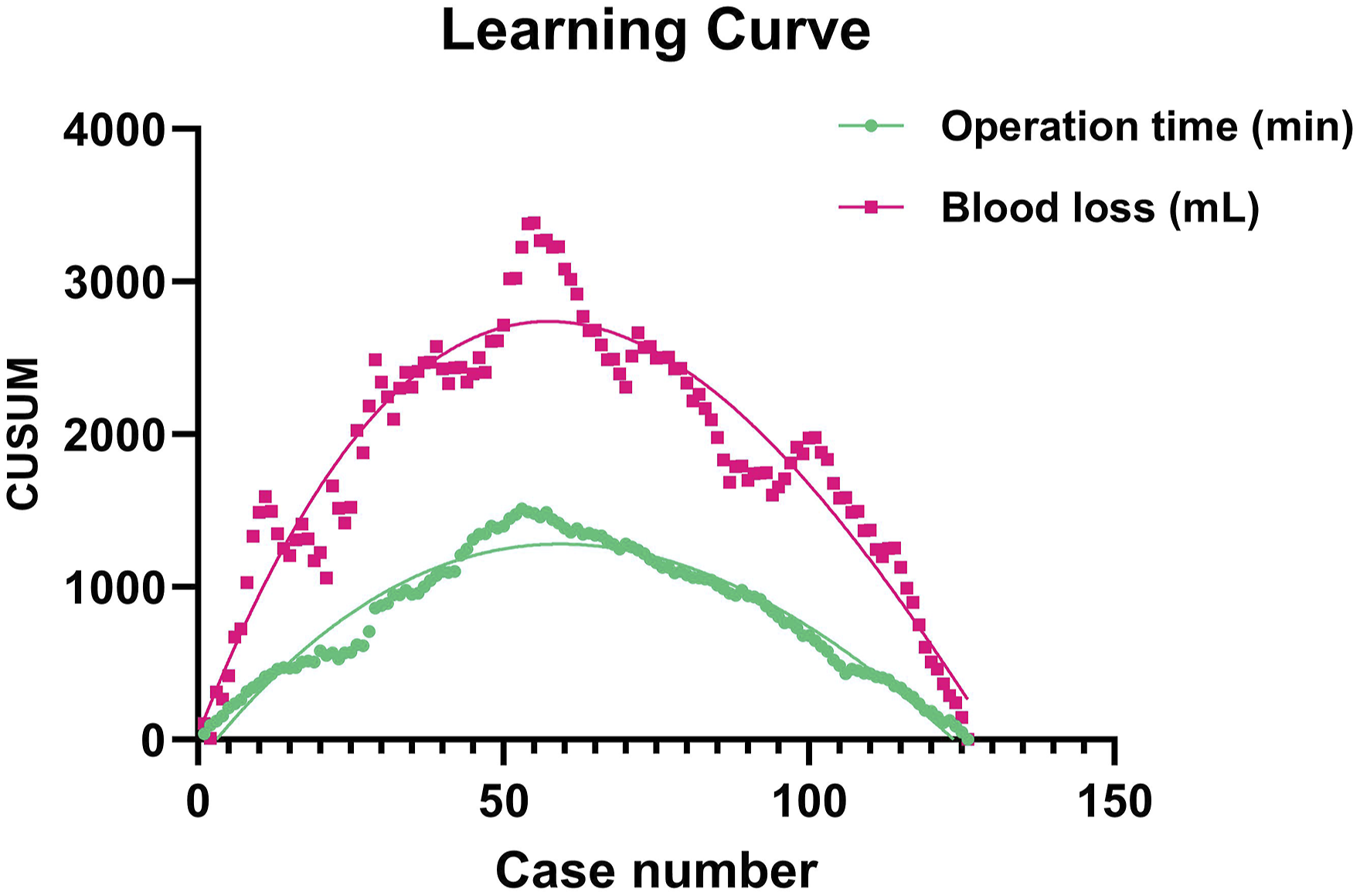

Discussion
Traditional LP, as reported by Hirabayashi et al, in 1980s, 2 has been widely proven to improve neurological outcomes, especially in CSM patients with multilevel compression. 1 Preservation of posterior muscles during LP has been shown to be an effective method to reduce loss of cervical curve, cervical malalignment and ROM which would also release the scale of neck pain and axial symptoms.11-13 Therefore, various modified laminoplasty were developed in previous studies. Shiraishi et al 14 reported ‘skip laminectomy’ technique, which preserved half of the attachments of the semispinalis cervicis and multifidus muscles at the segments of laminectomy and all muscular attachments at other segments. Over an approximately 2 years follow-up, skip laminectomy was shown to significantly reduce the loss of ROM and incidence of axial symptoms. 15 However, the application of this method might be limited as it could not provide sufficient decompression for patients with multilevel compression, continues ossification of posterior longitudinal ligament (OPLL), or developmental cervical stenosis. Some researchers have explored whether preserving the attachments of paraspinal muscles on the spinous processes of C2 and C7 improves the postoperative performances. And the results indicated that preserving more attachments on the spinous processes of C2 and C7 was associated with a higher retention rate of ROM postoperatively.16-19 Our department reported UL, which preserving almost all attachments of paraspinal muscles on the hinge side, resulting in better cervical alignment, less cervical curve loss and more retention rate of ROM postoperatively in 2015. 8 These findings were consistent with Chen et al. 9 who reported that UL could also reduce the neck pain after surgery compared with traditional LP. What’s more, Guo et al. 20 explored whether preserving posterior paraspinal muscles on both sides could get better outcomes. Surprisingly, with similar neurological recovery and scale of neck pain, the CSA at open side in patients with preserving paraspinal muscles on both sides decreased significantly compared with the patients in whom preservation was limited to only hinge side. The asymmetry of posterior structures of the cervical spine caused by laminoplasty might be one of the primary reasons increasing the mechanical stress at the open side. 20
In this study, we introduced a new modified laminoplasty, raising roof laminoplasty (RL). We found a gradual decrease in operation time and blood loss as the number of completed cases increased. The CUSUM learning curves for operation time and blood loss reached their peaks in 58 cumulative cases, suggesting that proficiency in the technique was usually achieved after so many procedures, whereby operation time decreased from a mean of 166.72 to 120.65 minutes and blood loss decreased from a mean of 251.90 to 148.88 mL.
Using the intermuscular approach between SSCa and SSCe as Guo et al. 20 reported, the area of blunt separation was limited around the positions at which the 3D-printed implants were located. At the same time, this approach could also preserve the connections between posterior deep extensors (mainly SSCe and MF) and the spinous process. Most importantly, the effect of the procedures during RL symmetrical on both sides of the cervical spine. The distance raised at the both sides was the same, determined by the size of 3D-printed prostheses. This resulted in balanced mechanical pressure between the left and right sides. Based on the result of the CSA of paraspinal muscle at final follow-up in our study, we found that the symmetry of postoperative muscle in RL group was better, approaching approximately 1.00.
For the clinical outcomes, the JOA scores at the final follow-up in RL group were found better than UL group in this study. Our team had reported the 1-year follow-up results comparing RL and LP 21 : the advantages of RL included a higher retention rate of ROM and less change of cervical malalignment with similar neurological recovery, neck pain and neck disability postoperatively. Fujiyoshi et al demonstrated that a sufficient posterior shift of the spinal cord and neurologic improvement are not obtained after posterior decompression surgery. 22 However, sufficient decompression does not guarantee satisfactory neurological recovery with certainty. 23 Despite the postoperative CSA of spinal cord in RL group significantly larger than that in UL group, these might not be responsible for the differences of JOA scores at 2-year follow-up, as sufficient radiological decompression was observed in the MRI of patients in both groups, with comparable MCID rates. In Table 4, we performed a multivariable liner regression to explore the possible reasons. We found that age had a negative impact on JOA scores at 2-year follow-up, although the baseline at enrollment being comparable between RL and UL. Therefore, we confirmed that RL was able to achieve comparable neurological recovery with UL in CSM patients.
Our results suggested that the preservation of biliteral posterior muscles in RL might not result in lower VAS but was associated with better NDI compared to the approach preserved only one side at 2-year follow-up. Wang et al. 24 reported that preserving both sides of posterior muscles in RL might be meaningful for releasing the VAS scores of neck pain within the first three days postoperatively compared to UL and LP. When the duration of follow-up was reached 6 months or 1year, the protection of posterior muscles in UL or RL did not show superior results for neck pain but did for less neck disability compared to LP. As the duration of follow-up increased, the statistic still supported this hypothesis. 20 In this study, we found that changes of CSA in right-side of PM on C4 or C5 level were not correlated with the significant alterations in postoperative NDI. However, postoperative symmetry of posterior PM on C4 level had positive impact on NDI. In other words, the imbalance in the cervical spine caused by LP was exacerbated when considering preserving or reconstructing posterior cervical muscles. Interestingly, the double-door LP, which involved a larger area of blunt separation than RL, as reported by Wang et al., 20 performed even better than RL in terms of NDI. Fortin et al also found an association between cervical muscle morphology and clinical symptoms and functional status, with greater bilateral asymmetry of the semispinalis capitis being associated with higher NDI.25,26
Our study demonstrated that compared with UL group, the patients underwent RL had better ROM at final follow-up. The relationship between paraspinal muscles and postoperative ROM has been widely discussed. According to the hypothesis of previous research, more muscles resulted in better ROM. In patients who received UL, because of the reconstruction of the spinous process and the loss or weakening of left-side muscles, the extension and flexion arm would become different from preoperative situation, and finally resulted into the loss of ROM. Unlike UL, the RL technique could better preserve cervical posterior structures, and the more symmetrical structures after surgery might provide mechanical conduction system more similar to normal physiological situation.13,15,16,27 Interestingly, we found that the CSA of right-side PM in UL group at final follow-up was even larger than preoperatively. On the one hand, as the left-side PM atrophy and the extension arm increasing, maybe the right-side PM had to grow compensatively to ensure the cervical mobility and stability. 13 On the other hand, after UL, parts of posterior muscle-ligament complex on the open side were reconstructed crossing the midline to the hinge side. Importantly, our results supported that RL maintained the volume and the symmetry of bilateral paraspinal muscles. This postoperative state resulted in a balanced extension of the flexion arm in bilateral muscles, more closely resembling the preoperative condition. In our study, there was no significant difference of CL and C2-7 SVA between two groups at the final follow-up. We also found that postoperative CSA of right-side PM on C4 level had a negative impact on the change of CL (with an increasing negative value). However, the T1S in the UL group increased significantly than RL group, which suggested a tendency for the head and neck to tilt forward of the patients in UL group. This tendency may place a greater burden on the extensors, and finally resulting in the muscle compensation, 13 as evidenced by the increased CSA of the right-side PM muscle in the UL group reported in our study.
There are some limitations in this study. First, it was a retrospective cohort study and the level of evidence was not substantially high. Secondly, limited by the MR images sequences, we were unable to measure the fat infiltration of the muscles, which might influence on the clinical results and be associated with the unusual changes of CSA between RL and UL groups. Thirdly, the two procedures were not performed in the same period. Fourthly, the 3D-printed implant was designed to make sure the fusion between vertebra and dissociative lamina, but we couldn’t demonstrate it only by normal CT scan, although it has been demonstrated in our previous study. 28 Finally, we need prospective and biomechanical studies to further explain its possible advantages.
Conclusions
In conclusion, we developed an intermuscular RL technique utilizing 3D-printed implants. Compared to UL, this technique demonstrated comparable recovery of neurological functions, improved quality of life, greater cervical mobility and a better decompression effect in a 2-year follow-up. This intermuscular RL, which preserves the cervical posterior structures symmetrically and makes its mechanical properties closer to preoperative situation, provides a new treatment approach for degeneration cervical myelopathy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Research and Development Program of China (2023YFC3604404).