
Abstract
Study Design
Retrospective cohort.
Objective
Despite numerous studies highlighting patient comorbidities and surgical factors in postoperative success, the role of social determinants of health (SDH) in anterior cervical discectomy and fusion (ACDF) outcomes remains unexplored. This study evaluates the predictive impact of SDH on 90-day readmission and health utilization (HU) in ACDF patients using machine learning (ML).
Methods
We analyzed 3127 ACDF patients (2003-2023) from a multisite academic center, incorporating over 35 clinical and demographic variables. SDH characteristics were assessed using the Social Vulnerability Index. Primary outcomes included 90-day readmission and postoperative HU. ML models were developed and validated by the area under the curve (AUC) for readmission and mean absolute error (MAE) for HU. Feature importance analysis identified key predictors.
Results
Balanced Random Forest (AUC = 0.75) best predicted 90-day readmission, with length of stay, Elixhauser score, and Medicare status as top predictors. Among SDH factors, minority status & language, household composition & disability, socioeconomic status, and housing type & transportation were influential. Support Vector Regression (MAE = 1.96) best predicted HU, with perioperative duration, socioeconomic status, and minority status & language as key predictors.
Conclusions
Findings highlight SDH’s role in ACDF outcomes, suggesting the value of stratifying for interventions such as targeted resource allocation, language-concordant care, and tailored follow-up. While reliance on a single healthcare system and proxy SDH measures are limitations, this is the first study to apply ML to assess SDH in ACDF patients. Further validation with direct patient-reported SDH data is needed to refine predictive models.
Introduction
Health encompasses physical, mental, and social well-being, all of which are influenced by Social Determinants of Health (SDH). These components are vital for physicians to provide equitable and culturally competent care while delivering high-quality healthcare. 1 Key aspects of SDH include education, healthcare access, geographical location, and economic conditions, which collectively contribute to health disparities among different demographics. Evidence shows that these factors affect patient outcomes across various medical disciplines.2,3 In orthopaedic surgery, SDH influences outcomes in surgeries involving the hand, shoulder, and joints.4,5 Moreover, key elements such as housing, transportation, insurance, language, disability, and socioeconomic status are needed to further understanding the impact on spine surgery. 6 Nonetheless, there is a notable gap in research regarding the impact of SDH on spine surgery.
Anterior cervical discectomy and fusion (ACDF) is a workhorse approach for treating symptomatic cervical disease and is one of the most commonly performed spine procedures. 7 ACDF has been shown to alleviate pain and disability, and overall has lower complication rates compared to other spine surgeries.8,9 However, given the increasing volume of ACDFs performed nationwide, there is a lack of understanding regarding specific drivers of complications. While studies have linked various comorbidities to postoperative success, little is known regarding the impact of SDH on cervical spine surgery.
As with any large dataset, including SDH-related characteristics alongside clinical and surgical parameters presents challenges for data analysis due to the increasing number of variables. Machine learning (ML) offers considerable advantages in managing complex datasets, identifying patterns, and making accurate predictions. Unlike traditional statistics, which rely on preprogrammed rules and assumptions, ML algorithms learn based on the data provided and generate improved models over time. 10 It should be noted that ML is not intended to replace traditional statistics but rather harness its predictive ability as another tool in a clinician’s decision-making toolbox.
ML has been applied to ACDF populations, focusing on its application and impact on clinical outcomes.11-14 To summarize, patient demographics−such as age, obesity, and ASA classification−are amongst the most predictive factors. Moreover, prior research has established the 90-day postoperative period as a meaningful time point for evaluating both cost and surgical outcomes, with admission rates ranging from 5-13%.15,16 To our knowledge, no prior study has incorporated a broad range of SDH variables. By integrating these factors, our study provides a more comprehensive understanding, offering insights that may aid clinicians in risk mitigation and targeted intervention strategies−ultimately reducing cost and improving patient outcomes. The primary objective of this study is to predict 90-day readmission rates, as well as overall health utilization (HU) using an extensive array of demographic, clinical, surgical, and SDH variables in ACDF patients. The secondary objective is to evaluate the impact of SDH-related factors impact on ACDF outcomes, providing further evidence of their clinical significance.
Methods
Adult patients who underwent single or multilevel ACDF for degenerative cervical disease at a multi-center academic health system between 2003-2023. Patients were identified from the electronic medical record (EMR) using Northwestern Medicine Enterprise Datawarehouse, with data extraction being classified using standardized current procedural terminology (CPT) codes for information collection. To minimize selection bias, only patients with completed information below and follow-up data were included in the final analysis.
A total of 40 clinical variables, including demographics (age, sex, body mass index [BMI], etc.), past medical history (American Society of Anesthesiologists [ASA] class, Elixhauser Comorbidities score, etc.), past medication history (antibiotic, neuromodulator [gabapentin, pregabalin, etc.], benzodiazepine), past surgical history, total perioperative duration (defined by the total time spend in the operating room [OR], total surgery time from incision to closure, and total time under anesthesia), postoperative complications, 30-day readmission, and 90-day readmission were included. Patients were excluded if they underwent surgery for malignancy, trauma, infection or if key clinical variables were missing. Data inconsistencies were managed by performing periodic chart reviews and cross-referencing EMR records for accuracy. If discrepancies could not be resolved, the patient were excluded from the analysis.
The Social Vulnerability Index (SVI) was used to assess SDH at the census tract level. SVI scores were derived from the U.S. Census Bureau, which provides validated demographics metrics. The Geocodio platform was utilized to assign patient addresses to census tracts, ensuring alignment with census tract boundaries. The SVI ranks each tract based on 15 social factors (i.e., poverty, lack of vehicle access, and crowded housing). These factors are grouped into four sub-domains: socioeconomic status, household composition, minority status and language, housing type and transportation. Each sub-domain is scored from 0 to 1 at the census tract level, with higher scores reflecting greater social vulnerability. The overall SVI score is computed by summing the sub-domain scores and normalizing them to percentile ranking. To validate the SVI assignment, the values were cross-referenced with the Centers for Disease Control and Prevention (CDC), a publicly available geographic dataset.
The primary outcomes were 90-day readmission and postoperative HU. 90-day readmission is defined as any inpatient admission within 90 days of ACDF. HU was calculated as the sum of all emergency department or urgent care visits, invasive procedures (including cardiac catheterization, IVC placement, and laryngoscopy), non-routine testing (e.g., electromyography), and non-routine imaging (computed tomography, magnetic resonance imaging) in the first 90 days after surgery.
Statistics
Data was analyzed using RStudio v. 2024.12.0 + 467 (RStudio PBC Boston). Statistical analysis was completed to show comparison between readmission vs non-readmission groups. A sub-analysis was conducted between single vs multi-level fusions. Differences between groups were detected using the student’s t test for means and chi-squared test for categorical variables. A P-value of <0.05 was considered significant.
Machine Learning
ML models were run using custom Python scripts and were validated by the area under the curve (AUC) for a 90-day readmission and mean absolute error (MAE) for HU. The data was split into training/testing sets. An 80/20 train-test split was selected as it provides a balance between training the model on sufficient data while reserving enough unseen data to evaluate generalized performance. This proportion is commonly used in ML studies to ensure model robustness while preventing overfitting. Validation was performed on withheld test data following optimization. For 90-day readmission, Extreme Gradient Boosted Tree Classifier (XGBoostC), Balanced Random Forest (BRF), Elastic-Net Penalized Logistic Regression (ENet), and Deep Learning Neural Net (DNN) were used given the categorical nature of the outcome. Alternatively, Extreme Gradient Boosted Tree Regressor (XGBoostR), Random Forest (RF), and Support Vector Regression (SVR) were used for HU as a continuous type of outcome. The algorithms were selected based on their strength in handling structured clinical data, prevalence within the current literature, ability to manage class imbalance and nonlinear relationships.
To further mitigate overfitting, hyperparameter tuning was performed using Bayesian Search Algorithm over 15 iterations and across 5-fold cross-validation. This optimization criteria were model specific: mean AUC was used for classification models (XGBoostC, BRF, ENet, and DNN) and mean MAE for regression models (XGBoostR, RF, SVR). The best-performing hyperparameters were selected based on these respective metrics. Tuned hyperparameters varied by model but included learning rate, tree depth, and number of estimators, among others. Furthermore, inverse class weighting based on frequencies were used to address class imbalances. This approach ensured robust parameters selections while minimizing overfitting and avoiding data imbalance.
The DNN model was created using Sequential API (Tensorflow Keras) library with an input layer connecting to a deeper connected layer, dropout layers to prevent overfitting, and an output layer with a sigmoid activation function. Similarly, hypertuning and inverse class weighting were used based on previously mentioned methods.
The best-performing models were determined by the highest mean AUC and lowest mean MAE. Feature selection was not conducted prior to model development; all features were included in training/testing to allow the models to autonomously determine relevant predictors. This approach was chosen to avoid potential bias from arbitrary feature exclusions and to ensure no potentially important variables were omitted before model optimization. Feature importance was evaluated using SHAP values to understand the relative contribution of each feature. Additionally, the whole process was repeated 50 times to ensure randomness was preserved, given the repeated data partition throughout the analysis. Feature importance plots were created based on the best-performing models. Standard deviations were calculated for AUC and feature importance. A histogram was created of some of the top predictors for 90-day readmission and HU. All ML models were run using their respective implementations in Python: scikit-learn, shap, Tensorflow, and Keras packages.
Results
Demographic for ACDF Cohort.
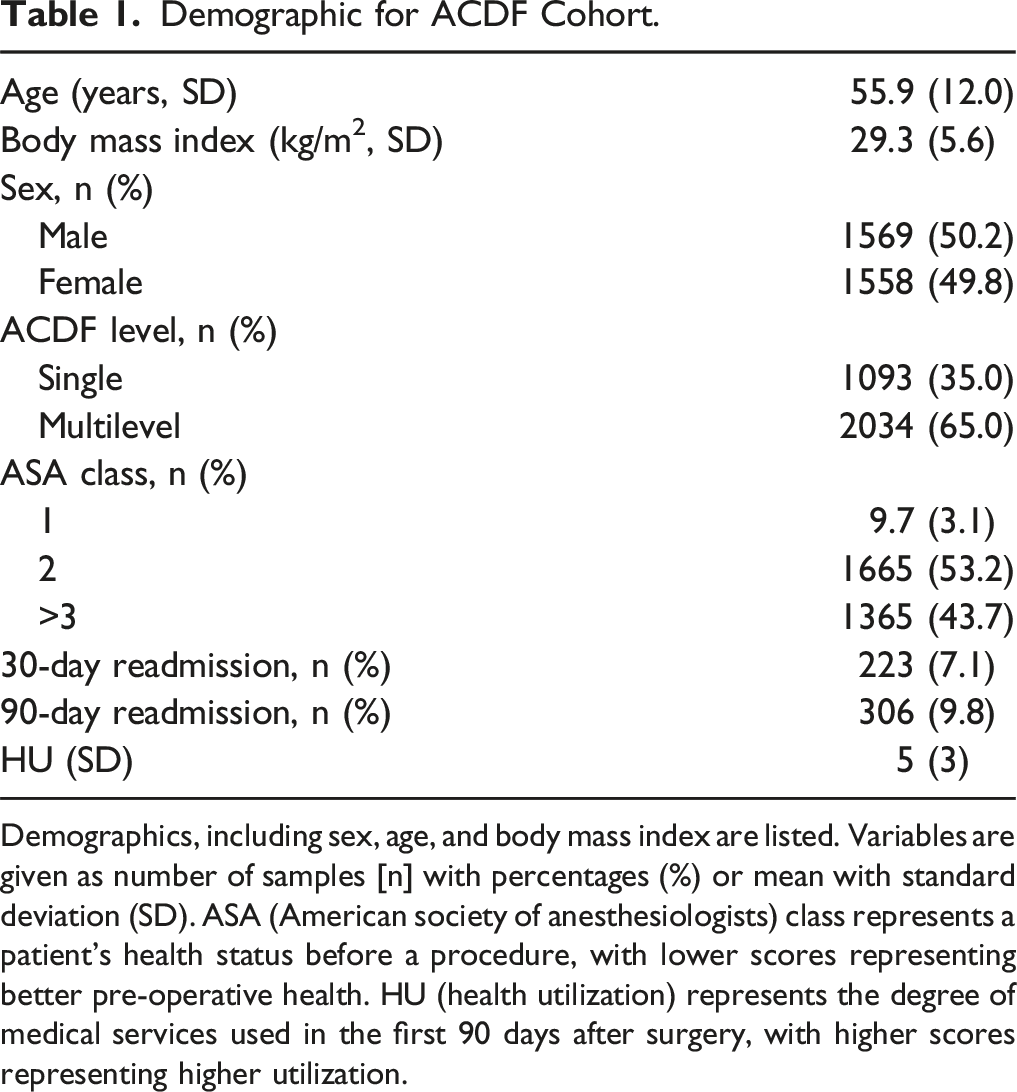
Demographics, including sex, age, and body mass index are listed. Variables are given as number of samples [n] with percentages (%) or mean with standard deviation (SD). ASA (American society of anesthesiologists) class represents a patient’s health status before a procedure, with lower scores representing better pre-operative health. HU (health utilization) represents the degree of medical services used in the first 90 days after surgery, with higher scores representing higher utilization.
Comparison Between Readmission vs Non-readmission Patients.
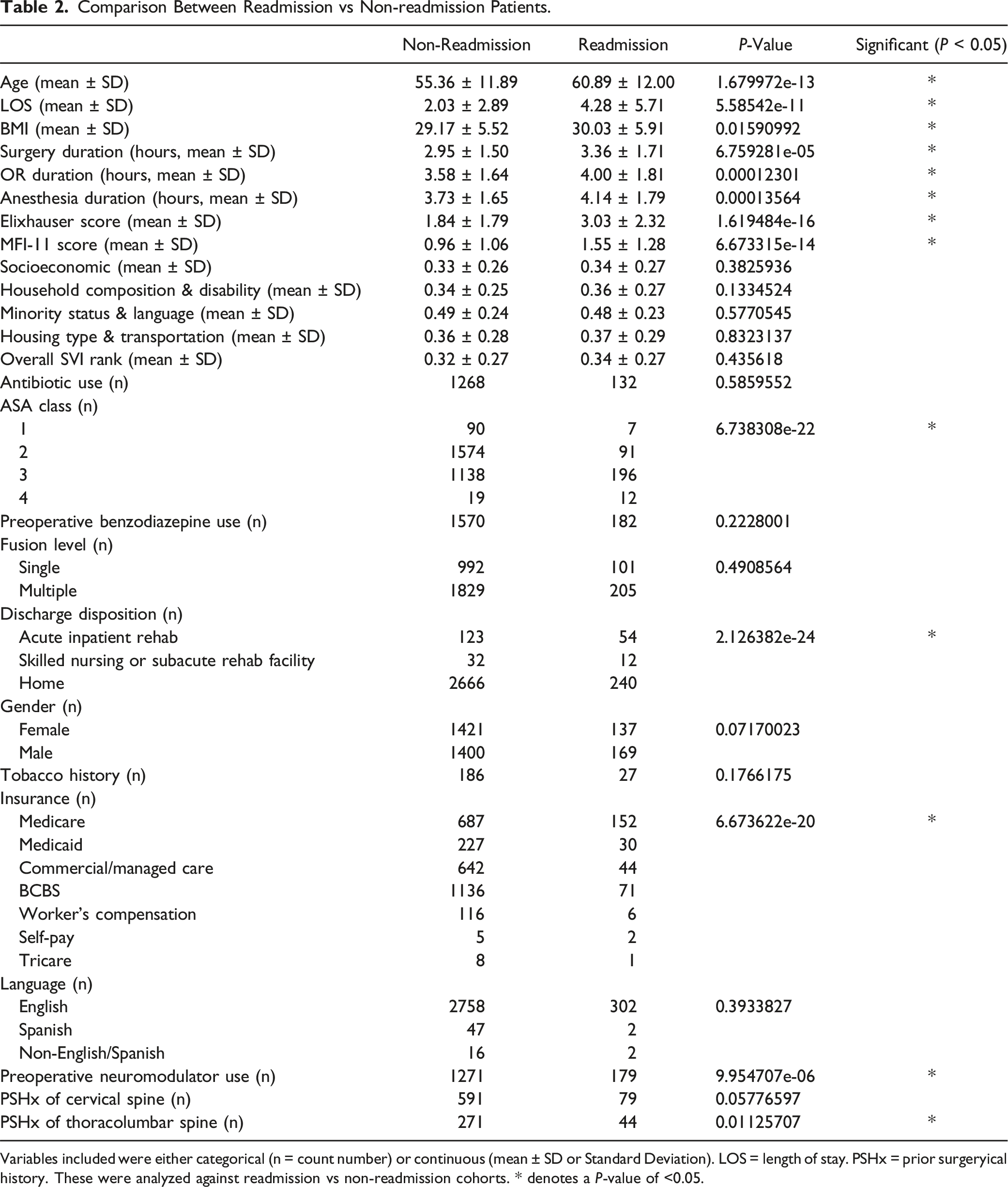
Variables included were either categorical (n = count number) or continuous (mean ± SD or Standard Deviation). LOS = length of stay. PSHx = prior surgeryical history. These were analyzed against readmission vs non-readmission cohorts. * denotes a P-value of <0.05.
Model Performance for 90-Day Readmission and Health Utilization (HU).
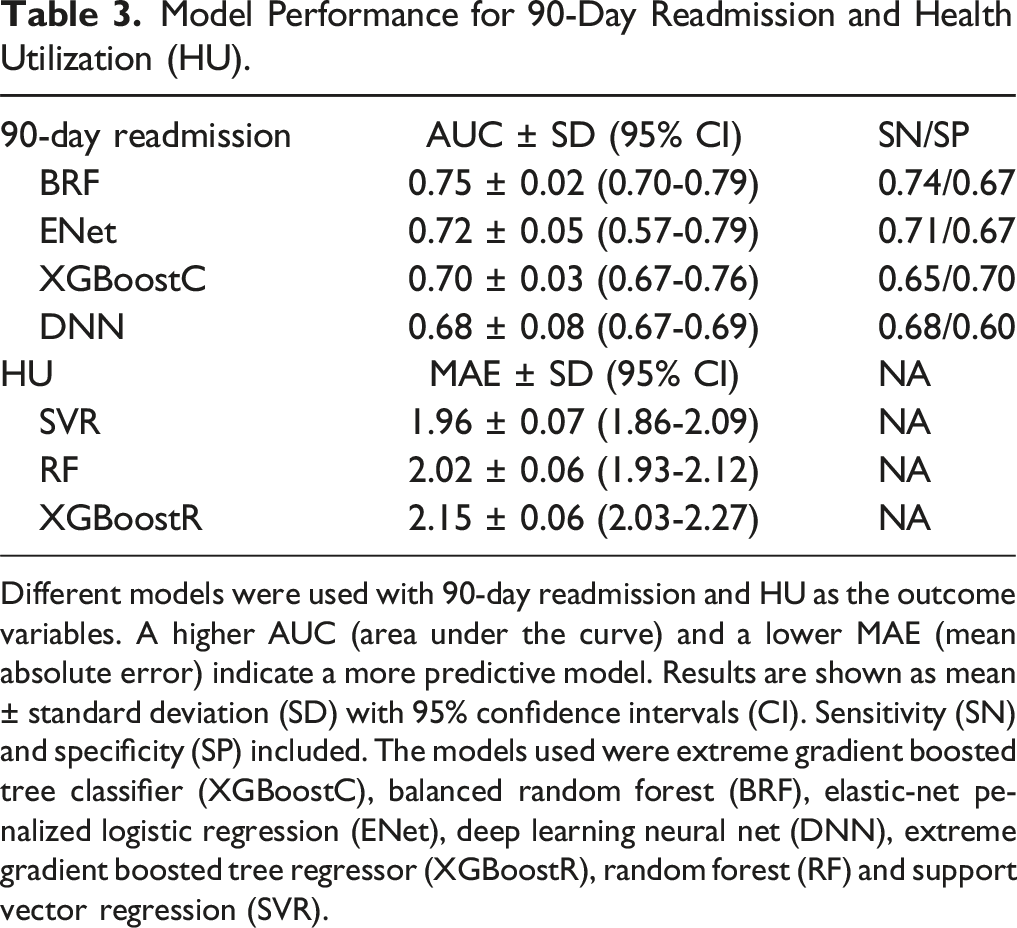
Different models were used with 90-day readmission and HU as the outcome variables. A higher AUC (area under the curve) and a lower MAE (mean absolute error) indicate a more predictive model. Results are shown as mean ± standard deviation (SD) with 95% confidence intervals (CI). Sensitivity (SN) and specificity (SP) included. The models used were extreme gradient boosted tree classifier (XGBoostC), balanced random forest (BRF), elastic-net penalized logistic regression (ENet), deep learning neural net (DNN), extreme gradient boosted tree regressor (XGBoostR), random forest (RF) and support vector regression (SVR).
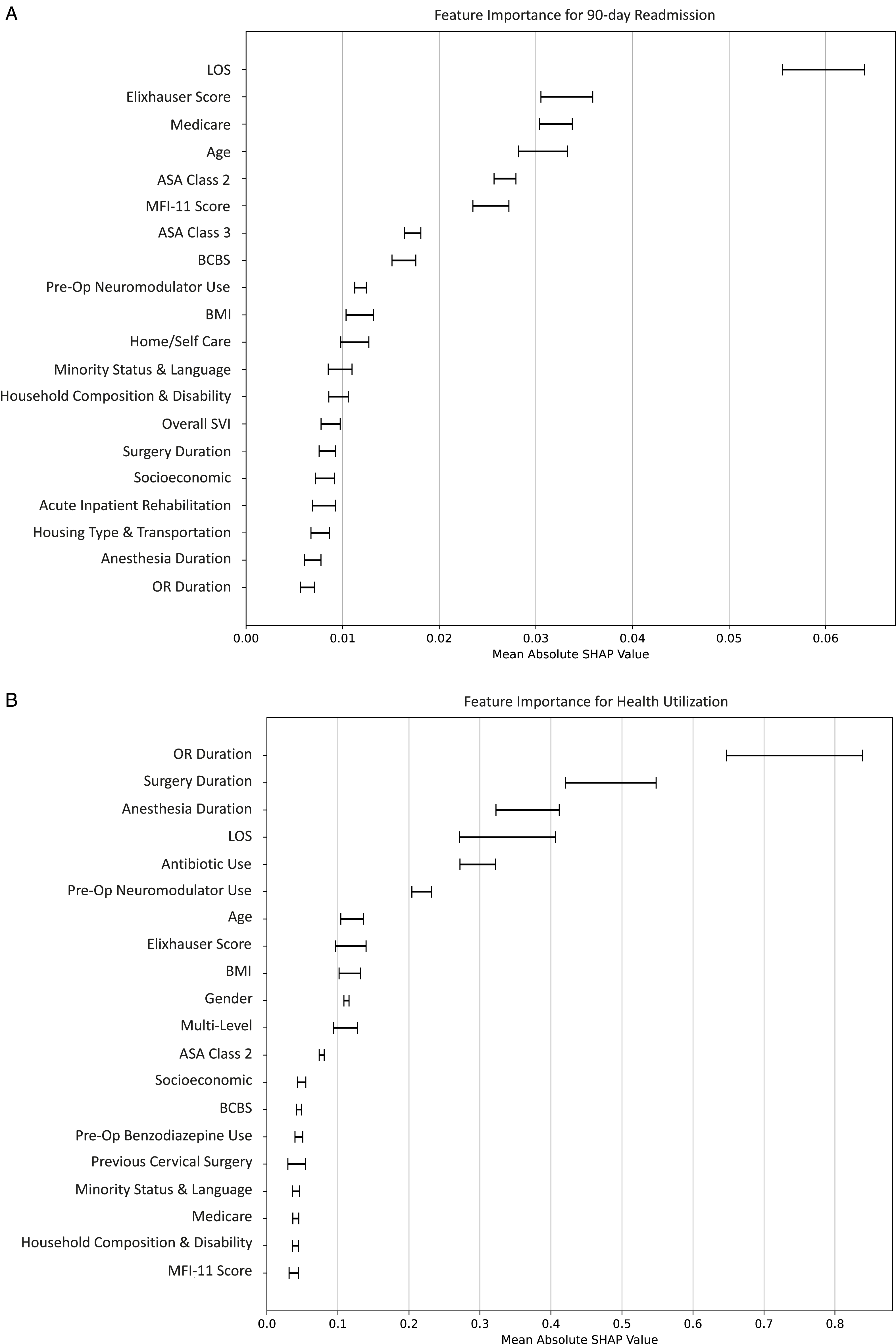
(a) Feature Importance Plot 90-Day Readmission. (b) Feature Importance Plot for Health Utilization. The plot, based on SHAP values, shows overall feature importance based on the best performing model for the 90-day readmission outcome. The order of feature listing on the y-axis denotes global variable importance to the model prediction with correlated mean SHAP value on x-axis. Variables include Length of stay (LOS), Blue Cross Blue Shield (BCBS), Body Mass Index (BMI), Operating room (OR), and Modified Frailty Index-11 (MFI-II).
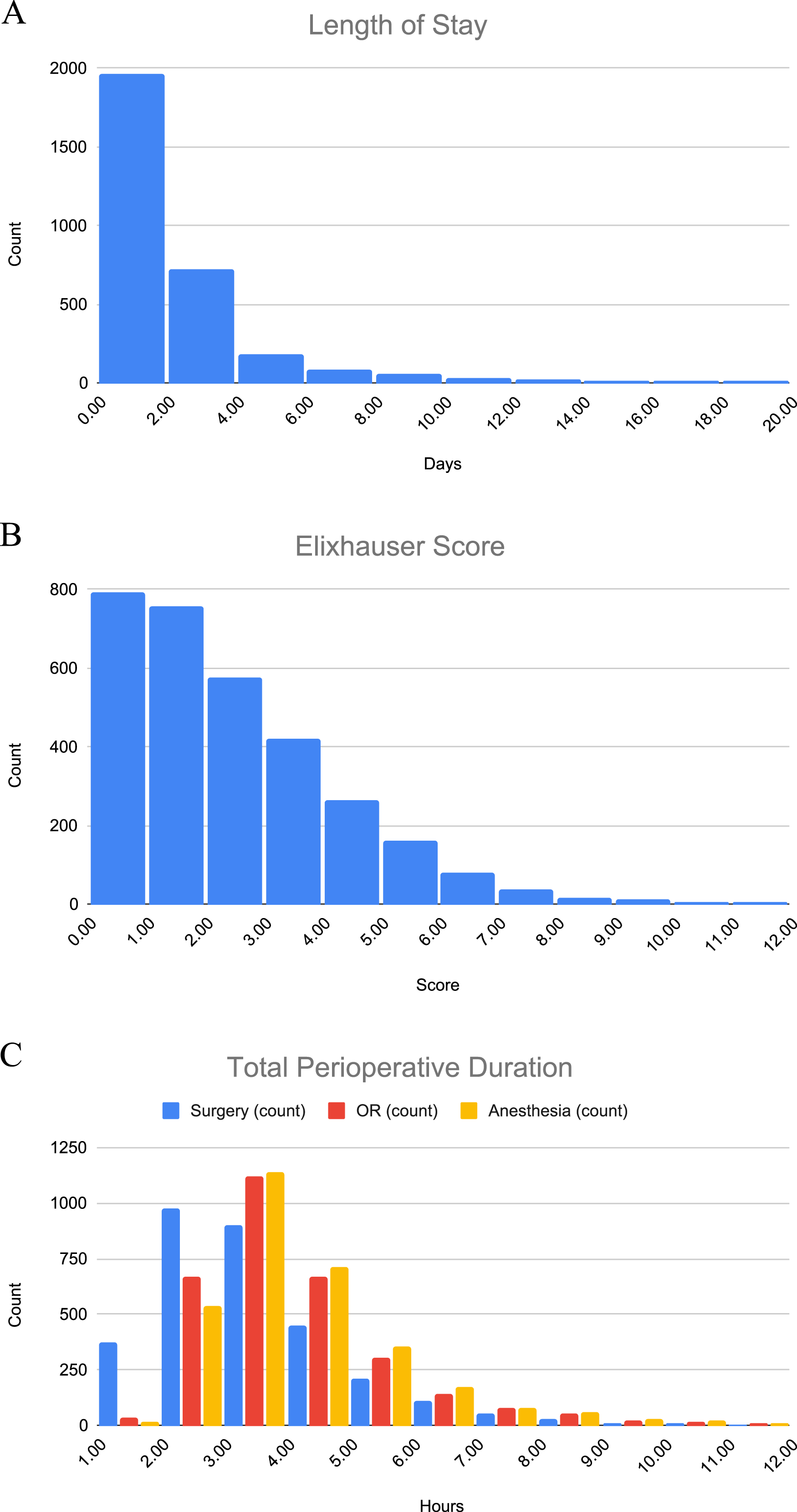
Histograms of top predictors for readmission and HU. (a) Length of stay in days (b) elixhauser score (c) total perioperative duration in hours. Color denotation of surgery time (blue bars), OR time (red), and anesthesia time (yellow).
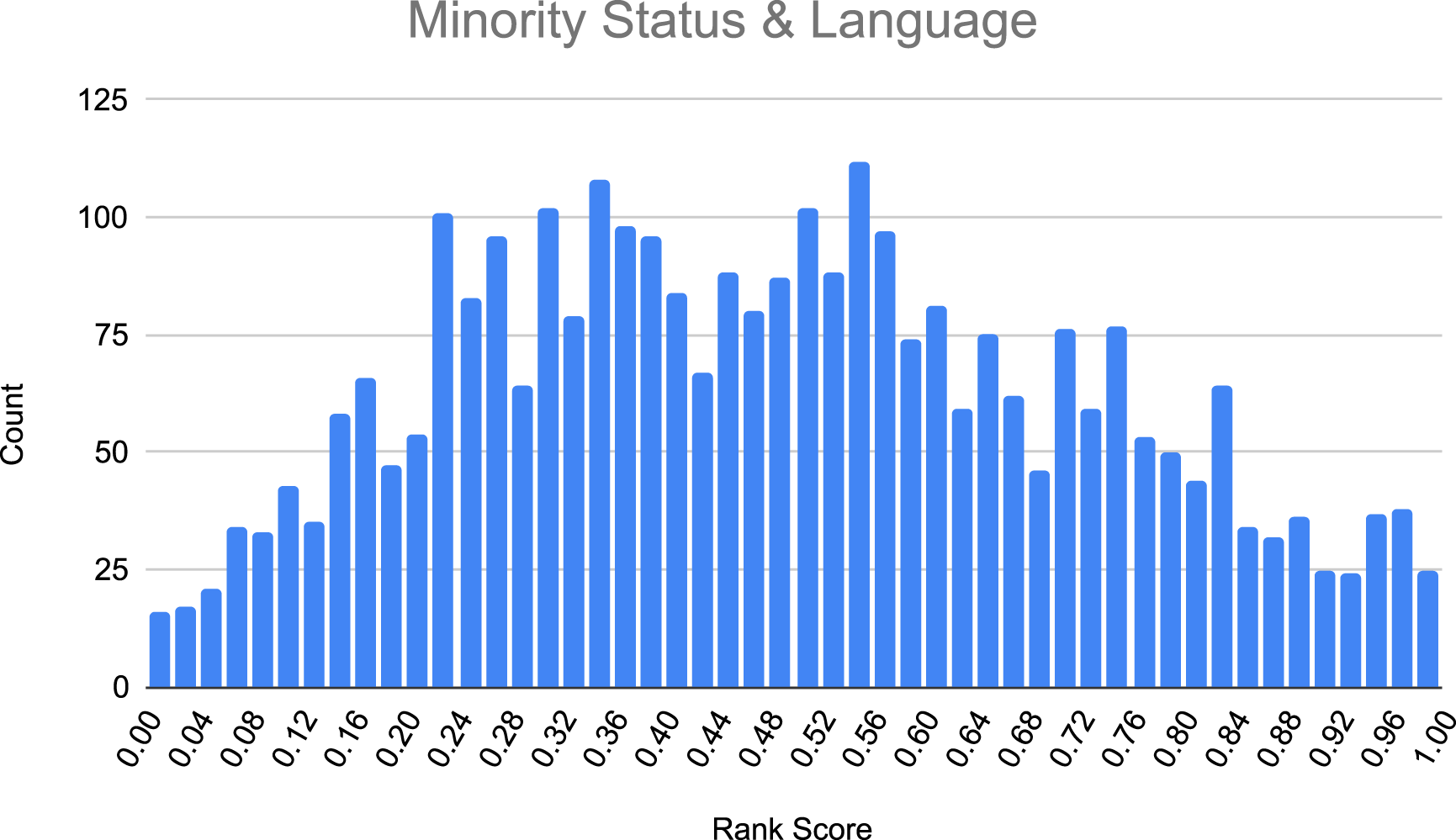
Histogram of minority status & language. Distribution of the Minority Status & Language variable, with patient count on the y-axis and the SVI-derived rank score (0 to 1) on the x-axis.
Discussion
SDH are recognized for their influence on patient’s health beyond conventional clinical parameters. These factors, such as minority status and education, have been shown to significantly influence both clinical outcomes and patient longevity. 17 In recent years, the application of ML in predicting surgical outcomes has increased. While traditional statistics are crucial for understanding linear relationships through hypothesis testing, ML excels at capturing complex patterns over large datasets while adapting new data to predict outcomes more accurately. ML has been applied in various fields to improve the decision-making between clinicians and patients, with practical applications such as predicting readmission for heart failure patients. 2 Several studies have utilized ML in predicting surgical outcomes in ACDF populations; however, no prior study has conducted an in-depth analysis of SDH’s influence on 90-day readmission or HU using ML.12,14,18
In this study, several ML models were utilized to predict 90-day readmission and HU in ACDF patients. BRF performed the best for predicting 90-day readmission, achieving an AUC of 0.75. SVR produced the best MAE of 1.96 for HU (Table 3). These results, as previously mentioned, likely reflect BRF’s ability to handle class imbalance while enhancing discriminative power, and SVR’s strength in capturing complex, non-linear relationships with robust outliers. 19 Feature importance analysis revealed that, besides SDH factors, other clinical variables such as LOS and total perioperative duration were among the top predictors for both 90-day readmission and HU. Additionally, some of these predictors were reinforced by the findings of our comparison analysis for 90-day readmission with factors such as LOS, Elixhauser score, insurance, age, BMI, ASA class, and perioperative duration being found to be statistically significant (Table 2). Notably, multiple SVI-related variables, including socioeconomic status, household composition & disability, minority status & language, housing type & transportation, and the overall SVI ranking were not found to be significant using traditional statistics but emerged as important predictors in our ML model (Figure 1(a) and (b)). This underscores the advantage of ML in capturing complex, multifactorial relationships that influence patient trajectories beyond isolated variable comparisons, offering a more comprehensive approach to risk stratification.
To our knowledge, this is the first study to assess the impact of SDH on ACDF outcomes. Our findings align with other outcomes research within spine and orthopaedics. A study examining minority differences discovered that Hispanic patients had higher rates of emergency department visits after lumbar fusion.
20
Additionally, one review of patients undergoing spine and other orthopaedic procedures found that 64% of studies reported disparities affecting minorities.
21
Our analysis revealed that housing type & transportation, as well as household vulnerability & disabled populations (increased number of young, old, disabled, or single-parent household members), were predictors of 90-day readmission. When analyzing ACDF outcomes outside of SDH features, our results are consistent with the current literature. In one study utilizing a smaller cohort of ACDF patients, several health comorbidities – such as pulmonary, endocrine, and GI conditions and age – were highly predictive of 90-day readmission.
12
Similarly, our study found that Elixhauser score, MFI-11, and age were top predictors of 90-day readmission. Karabacak et al identified age and factors such as preoperative laboratory values, diabetes mellitus, and current smoker status as predictors of readmissions and length of stay.
22
Interestingly, our analysis found ASA class and insurance status were top predictors of 90-day readmission. ASA class has been correlated with ACDF readmission in traditional regression analysis.
23
Furthermore, a propensity-matched cohort comparing Medicare and private insurance patients found lower readmission rates in the Medicare group, aligning with our traditional statistics analysis (Table 2).
24
Contradictory, our predictive modeling identified Medicare status as an impactful variable for readmission, highlighting its ability to account for nonlinear interactions and complex connections such as differences in baseline health, care coordination, and post-discharge support. For discharge status, Taylor et al. found that non-routine discharge status correlated with readmission rates, which agrees with our findings that discharge to acute inpatient rehab is predictive of readmission.
25
While home/self-care was identified as a top predictor, further analysis is needed to determine whether its presence or absence is a positive or negative predictor. Limited studies examining the effect of SDH on postoperative HU in ACDF found that minority status patients were at risk for longer postoperative LOS and medical complications compared to non-minority patients, directly contributing to higher HU rates in patients undergoing spine surgery.
26
Das et al. found that higher-income patients fared better than lower-income patients in terms of complications following ACDF.
27
Although a direct comparison was not completed in ACDF populations, our study was consistent with this association. Unsurprisingly, our study found that perioperative duration was the top predictor of HU.
28
Longer total
These SDH-related factors, such as minority status & language, are likely contributing to poorer outcomes through multiple mechanism, including disparities in healthcare access, communication barriers, and differences in post-discharge support. Studies have found that language barriers are associated with higher healthcare cost and poorer health outcomes. 31 Patients with limited English proficiency may struggle to fully understand discharge instructions, medication adherence, and follow-up care which increases the risk of complications and subsequent healthcare utilization. 32 Studies have found that language concordance−patient and clinician speaking the same language−increases trust and understanding while reducing clinician frustration.33,34 Implementing target interventions−such as SDH screening, tailored social work support, language-concordant staff −could not only improve patient outcomes but also optimize resources by reducing preventable readmission and excess HU, ultimately leading to cost savings for healthcare systems.
Even looking into lumbar fusion populations, disparities in postoperative outcomes have been well documented, with higher rates of pseudoarthrosis and postoperative complications observed in groups with higher social vulnerability.6,35 However, in a propensity-matched study, authors found no difference in readmission rates between disparity groups at 30 and 90 days, suggesting that traditional statistics may not fully capture the complexity of these associations. Similarly, Holbert et al. found no changes in 30-day readmission status amongst SDH variables. 36 In contrast, our ML analysis identified multiple SVI-related factors as important predictors of 90-days. One possible explanation for this discrepancy is the differing biomechanical and recovery profiles of lumbar vs cervical spine surgeries; ACDF patients may require additional consultation from vascular or ENT for preoperative evaluation. Furthermore, differences in post-discharge care pathways−rehabilitation requirements or mobility limitations−may further contribute to observed impact of SDH factors in our cohort.
This study is not without limitations. Our sample size was limited following data cleaning, resulting in a lower specificity even for the best model. This indicates that the model had a reduced ability to accurately predict positive outcomes, specifically patients who experienced readmission and HU. Increasing the sample size in future studies could improve specificity and consequently, AUC. Additionally, the analysis was conducted using data from a single health system, which may limit generalizability to other institutions with different patient demographics, healthcare infrastructures, and clinical workflows. Future multi-institutional studies could help validate these findings in broader patient populations.
Another limitation includes our reliance on proxy measures to estimate SDH, such as SVI, rather than direct patient reported data. While SVI provides valuable insights at a population level, it may not fully capture nuanced, patient-specific socioeconomic factors that contribute to health disparities. Additionally, while our analysis accounted for insurance types, it did not control for insurance compensation levels, which have been shown to influence patient trajectories and healthcare utilization in spine surgery. Moreover, psychological and social influences, including factors related to secondary gain, may influence patient behavior and post-treatment outcomes. While out study did not account for these factors, incorporating direct patient-reported SDH measures in subsequent research may improve the comprehensiveness of future studies. Furthermore, as a retrospective study, this analysis is inherently subject to biases related to unmeasured confounders and coding inaccuracies. The use of ML in clinical decision making also raises ethical considerations, particularly regarding transparency, potential bias in algorithmic decisions making, and the need for equitable model implementation. As ML becomes increasingly integrated into healthcare, it is essential to ensure that these tools are used to enhance−not replace−clinical judgment while mitigating risks of algorithmic bias and united disparities in care.
Nevertheless, our findings are significant as they represent the first reported analysis of the predictive effects of SDH in anterior cervical discectomy and fusion patients, providing an important foundation for future research. By leveraging these clinical and SDH-related factors, predictive modeling can help identify high-risk patients more accurately, enabling targeted interventions such as enhanced discharge planning, closer follow-up, and tailored resource allocation to reduce cost and readmission risk. Future studies can implement questionaries or surveys—such as the PRAPARE assessment tool—to directly query patients about a range of SDH characteristics, thereby eliminating the need for proxy social vulnerability measures. 37
Conclusion
Over the last decade, the growing body of literature on SDH has dramatically increased, supporting these factors as influential in medicine and surgery. 38 Several SDH variables were found to be top predictors of 90-day readmission and HU following ACDF. These findings underscore the potential value of integrating SDH assessments into preoperative risk stratification, allowing for targeted interventions such as social work consultation, language-concordant care, and tailored post-operative follow up. Demonstrating the predictive value of SDH in diverse populations will require prospective, multi-institutional studies to further enhance clinical applicability and refine risk stratification models. Additionally, developing and validating ML-based clinical decision support tools that integrate SDH factors could help refine risk assessment and improve postoperative care pathways. By further investigating the intersection between SDH and spine surgery, researchers can enhance predictive modeling approaches and promote high-quality care delivery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Statement
IRB approval was granted by our institution to perform this research.