
Abstract
Study Design
Retrospective cohort study
Objective
The aim of this study was to determine the relative importance and predicative power of the Hospital Frailty Risk Score (HFRS) on unplanned 30-day readmission after surgical intervention for metastatic spinal column tumors.
Methods
All adult patients undergoing surgery for metastatic spinal column tumor were identified in the Nationwide Readmission Database from the years 2016 to 2018. Patients were categorized into 3 cohorts based on the criteria of the HFRS: Low(<5), Intermediate(5-14.9), and High(≥ 15). Random Forest (RF) classification was used to construct predictive models for 30-day patient readmission. Model performance was examined using the area under the receiver operating curve (AUC), and the Mean Decrease Gini (MDG) metric was used to quantify and rank features by relative importance.
Results
There were 4346 patients included. The proportion of patients who required any readmission were higher among the Intermediate and High frailty cohorts when compared to the Low frailty cohort (Low:33.9% vs. Intermediate:39.3% vs. High:39.2%, P < .001). An RF classifier was trained to predict 30-day readmission on all features (AUC = .60) and architecturally equivalent model trained using only ten features with highest MDG (AUC = .59). Both models found frailty to have the highest importance in predicting risk of readmission. On multivariate regression analysis, Intermediate frailty [OR:1.32, CI(1.06,1.64), P = .012] was found to be an independent predictor of unplanned 30-day readmission.
Conclusion
Our study utilizes machine learning approaches and predictive modeling to identify frailty as a significant risk-factor that contributes to unplanned 30-day readmission after spine surgery for metastatic spinal column metastases.
Introduction
The annual cost of healthcare delivery in the United States (US) has recently surpassed $3.5 trillion, with spinal surgery being identified as 1 of the largest and most rapidly expanding expenditures.1-6 To address this growing economic burden, hospitals have used healthcare proxies associated with increased costs and a reduced quality of care, such as unplanned 30-day hospital readmission, to identify drivers of inferior outcomes.7-9 Consequently, the Centers for Medicare and Medicaid Services implemented the Hospital Readmission Reduction Program to financially penalize hospitals with increasing readmission rates. 10
Metastatic tumors of the spine comprise the majority of spinal tumors and are associated with increasing disability, a decreased quality of life, and a reduced overall survival. 11 Further, these tumors are of particular interest as their management requires a complex multidisciplinary approach, often necessitating surgery and/or radiotherapy, leading to major costs and resource utilization.11-13 Therefore, identifying risk factors for increased resource utilization, such as unplanned 30-day readmission, may help on the systems level to reduce overall spending.
Frailty, which is defined as an age-related accumulation of deficits that leads to an increased vulnerability to adverse healthcare outcomes, is present in an estimated 90% of patients with metastatic spinal tumors.14,15 Within the literature, classifying frailty in this population has been studied using measures such as metastatic spinal tumor frailty index (MSTFI), modified 5-item frailty index (mFI-5), modified 11-item frailty index (mFI-11), and more recently the Hospital Frailty Risk Score (HFRS). 16 In a recent study of patients undergoing spine surgery for metastatic spinal column tumors, there was a significant relationship between increasing HFRS and inferior outcomes such as high complication rates, longer length of stay (LOS), increased cost, and non-routine discharge. 16 However, there is a paucity of studies measuring the impact of frailty - as defined by HFRS - on unplanned 30-day hospital readmission rates. As there is no tool for assessing frailty for this group of patients, it is important to rigorously assess various instruments to determine whether it measures what it is intended to and whether such tools are applicable to diverse surgical populations.
Machine learning and predictive modeling have recently gained traction in spinal surgery as a powerful tool to identify important preoperative variables that have strong effect on healthcare outcomes. 17 However, few studies have utilized these advanced techniques to assess the impact of frailty on surgical outcomes in patients with metastatic spinal tumors. Therefore, the aim of this study was to determine the relative importance and predicative power of the HFRS on unplanned 30-day readmission after surgical intervention for metastatic spinal column tumors utilizing machine learning and multivariate analysis, respectively.
Methods
Data Source and Patient Population
We used the Nationwide Readmission Database (NRD), a nationally representative sample of all-payer discharges from US nonfederal hospitals, sponsored by the Agency for Healthcare Research and Quality. It contains discharge data for ∼18 million cases per year (approximately 35 million discharges, weighted) and includes over 100 clinical and nonclinical variables, including patient demographics, diagnoses, procedures performed, source of payment, total hospital charges, treating hospital characteristics, and readmission information. A retrospective study was performed using years 2016 – 2018 of the NRD for all patients with metastatic spinal column tumors (≥18 years old) undergoing surgical intervention. Institutional review board was exempted for this study.
The International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] diagnosis and procedural coding system was used to query the NRD for all hospital admissions containing a diagnosis of secondary malignant neoplasm of bone (C79.51, C79.52) and then cross matched with the surgical interventions patient received (Appendix Table 1, Appendix Table 2). Of these identified patients, only those greater than 18 years old were included. Patients who died and/or had no length of stay for the initial index event were excluded. Patients with insufficient time for 30- or 31-90-day accrual of readmissions were excluded. A patient’s first admission after the index surgery was considered a readmission, with all subsequent readmissions excluded. Unique patient linkage numbers were used to follow patients and identify 30- and 31-90-day readmission rates. Patients meeting these criteria were then stratified into frailty cohorts for the analysis. Limited by the information available within the database, unplanned readmissions may also include patients who are readmitted for oncologic reasons that may or may not be exacerbated or directly secondary to their recent operation.
HFRS
In our study, frailty was defined using the HFRS, an ICD-10 coding algorithm developed and validated by Gilbert et al in 2018, 18 which has since been applied in various medical and surgical contexts.19-21 The algorithm was created using 109 ICD-10 diagnostic codes that were over-represented in frail patients, including codes for dementia, heart conditions, chronic pulmonary disease, and renal failure. 18 Each ICD-10 code was assigned a number of points from .1 to 7.1, depending on how strongly the variable predicted frailty. 18 All ICD-10 codes for the admission were entered into the calculation. In addition to presenting frailty as a continuous variable, we then stratified the frailty score into Low (HFRS<5), Intermediate (HFRS 5 – 14.9), and High (HFRS ≥ 15), as previously described. 18
Data Collection
Patient demographics, comorbidities, adverse events (AE), length of stay (LOS), discharge disposition, total cost of admission, and 30- and 90-day readmission rates were assessed. Additional hospital characteristics such as size by bed volume and teaching status (metropolitan non-teaching, metropolitan teaching, and nonmetropolitan) were also collected from the NRD. Elixhauser Comorbidity Index was used to evaluate incidence of congestive heart failure (CHF), cardiac arrhythmias, valvular disease, hypertension (HTN), pulmonary circulation disorders, peripheral vascular disorders, paralysis, other neurological disorders, chronic pulmonary disease, diabetes, hypothyroidism, renal failure, liver disease, rheumatoid arthritis/ collagen vascular diseases, coagulopathy, obesity, fluid and electrolyte disorders, anemia (blood loss or deficiency), alcohol abuse, and drug abuse. In addition, incidence of cord compression, neoplasm-related pain, prior irradiation, prior antineoplastic chemotherapy, pathologic fracture, protein calorie malnutrition, current opiate use, current aspirin use, current anticoagulant use, anemia of chronic or chemotherapy-related, affective disorder, and nicotine dependence were assessed (Appendix Table 1).
Adverse events associated with the index hospital encounter and at 30- and 31-90-days after discharge were calculated by identifying the primary diagnosis code associated with each patient upon readmission. The AE included urinary tract infection (UTI), post-procedural fever, phlebitis, pulmonary embolism, acute post-hemorrhagic anemia, displacement of internal fixation device of vertebrae, wound disruption, mechanical device complication, post-procedure hematoma, nervous system complication, acute deep vein thrombosis (DVT), post-procedural digestive complication, acute kidney injury, acute myocardial infarction, pressure ulcer, sepsis, and cardiogenic shock (Appendix Table 1, Appendix Table 2).
The primary outcome investigated in this study was the relative importance of the HFRS for patient’s undergoing surgical intervention for metastatic spinal column tumors using machine learning analysis. Secondary outcomes included impact of frailty as defined by this tool on hospital LOS, total cost of admission, and discharge disposition.
Statistical Analysis and RF Machine Learning
National estimates were calculated by applying discharge weights developed for the NRD prior to analysis. All-payer inpatient cost-to-charge ratios were used to convert total hospital charge to total cost of admission. Postoperative outcomes (LOS and total cost) were compared by two-way independent t test and Mann-Whitney U test. The χ2 test was used to compare the frequencies of nominal data. The frequencies of 30- and 31-90-day readmissions were described using percentages for the most common primary diagnoses. A P-value of less than .05 was considered to be statistically significant. Weighted univariate and multivariate logistic regressions were fitted for 30-day readmission rate. Backward stepwise multivariable logistic regression analysis was used to select predictors in the final model, with .1 set as the entry and stay criteria. All P-values < .05 were considered to be statistically significant and all statistical analysis was performed using R Studio, Version 3.6.2, RStudio Inc., Boston, MA.
The Random Forest (RF) machine learning classification algorithm was used to predict 30-day patient readmission. Random forest classification is an ensemble-based supervised machine learning method consisting of randomized decision trees. The RF training algorithm applies bagging, or bootstrap aggregating, in which each decision tree is trained on a subsample of the data (sampling with replacement) and the final prediction is the majority class prediction across all trees. The combined classifier often outperforms individual estimators by decreasing variance and reducing overfitting, thus yielding more predictive models and increasing generalizability. 22 The dataset was first split into training (80%) and testing (20%) sets. The training set was used to construct prediction classifiers and the holdout test set was used to estimate predictive performance. We included all demographic and pre-operative comorbidities in the initial ML model.
Using the training set, stratified k-fold cross validation (k = 4) with hyperparameter tuning was employed to generate an initial RF classifier. Then, the relative importance of features were quantified using the Mean Decrease Gini (MDG) metric. Mean decrease gini is a common estimate of feature importance that represents the average decrease in Gini impurity across all nodes that use a given feature. The depth in which a feature is used in a decision tree reflects that feature’s influence in a tree’s prediction—features present in nodes towards the top of a tree influence a greater proportion of samples and are thus assigned higher importance.
Using the top 10 features with highest MDG, a second RF classifier was constructed using the same procedure as above. Both RF classifiers were then evaluated on the holdout test set by constructing Receiver operating characteristic (ROC) curves and computing the associated area under the ROC curve (AUC), and MDG values for these features were recomputed. Python (version 3.8.12, Python Software Foundation, Wilmington, Delware) was used to create the RF models and for plotting feature importance and ROC curves.
Results
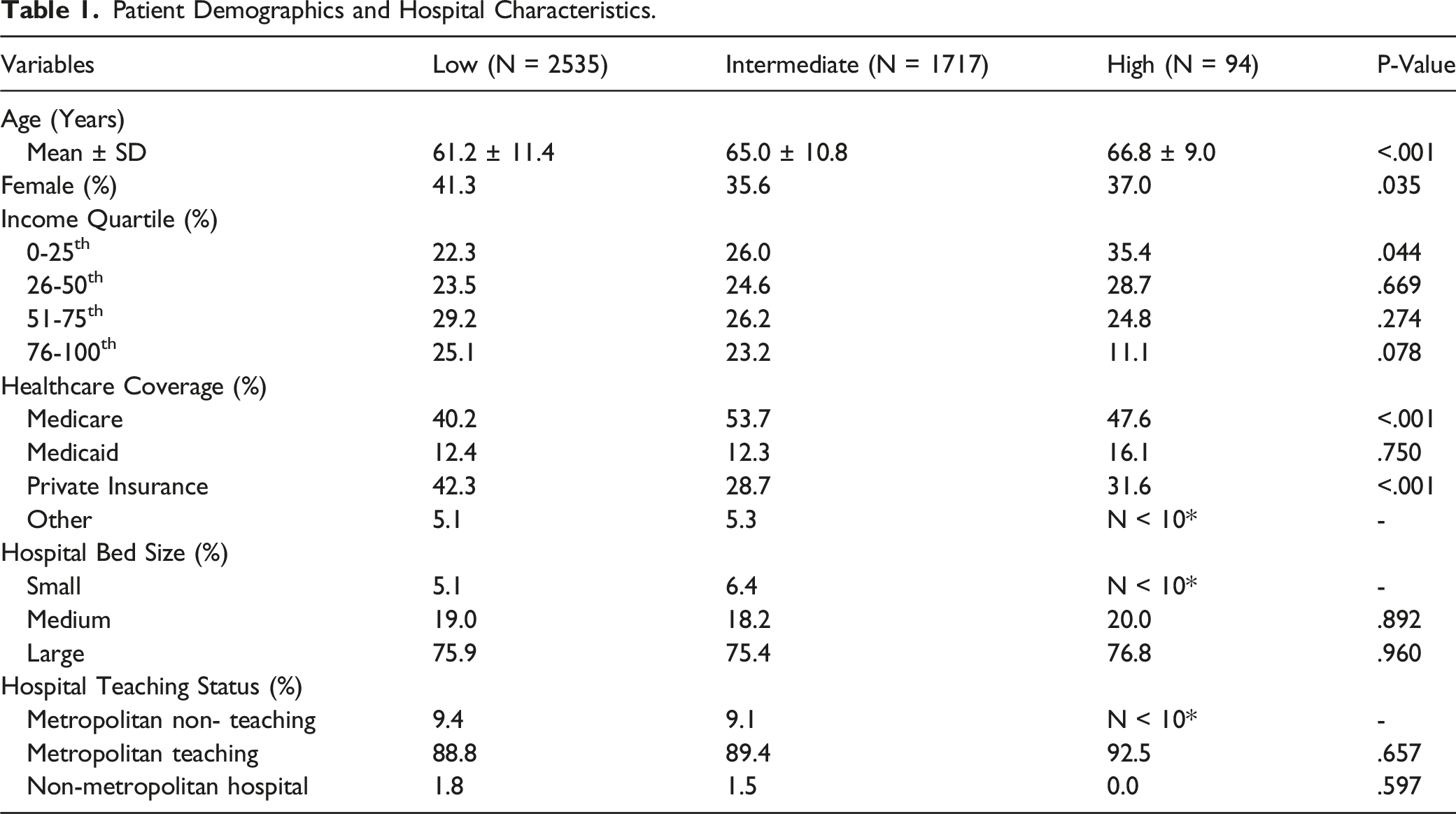
Patient Demographics and Hospital Characteristics
Patient Demographics and Hospital Characteristics.
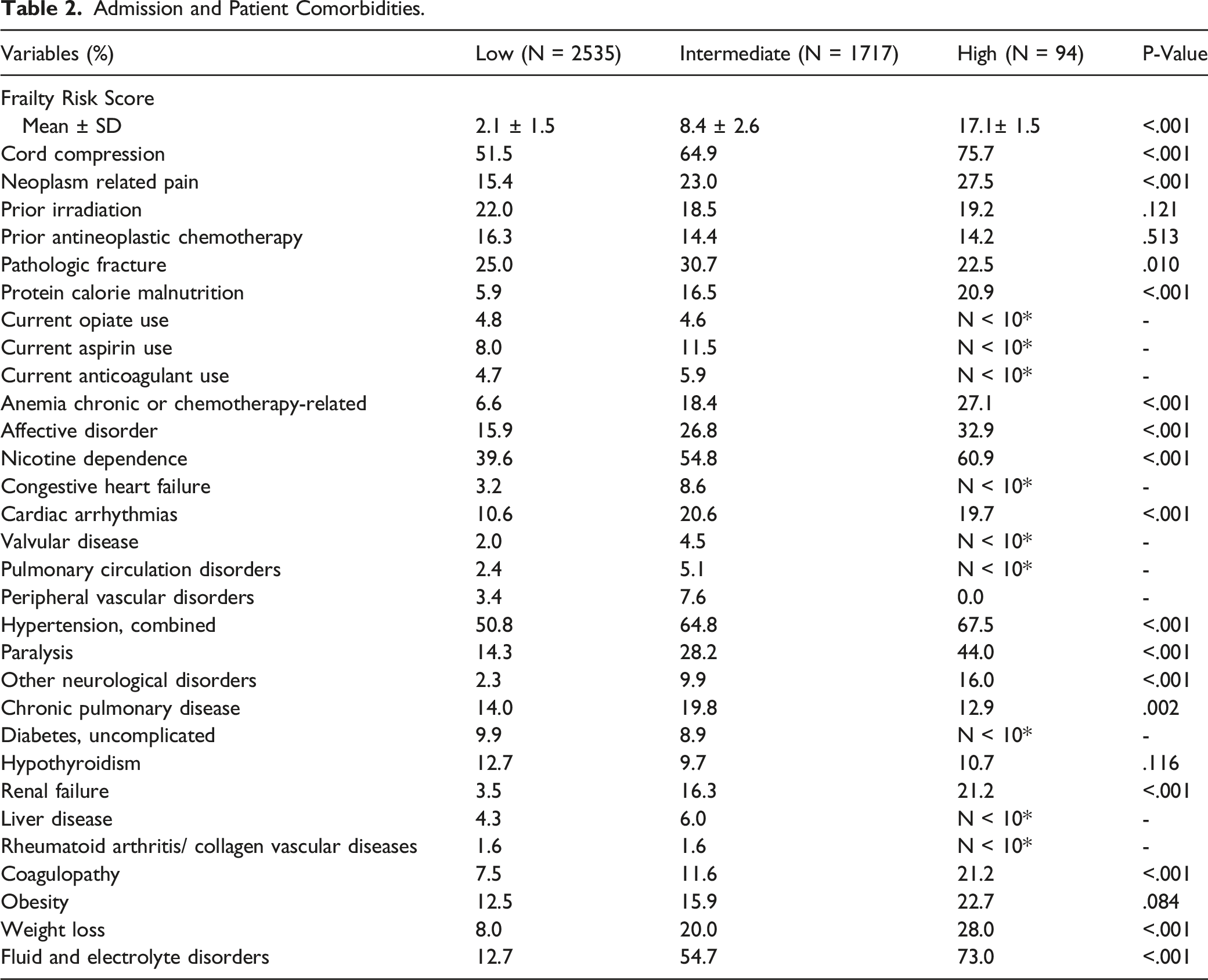
Admission and Patient Comorbidities
Admission and Patient Comorbidities.
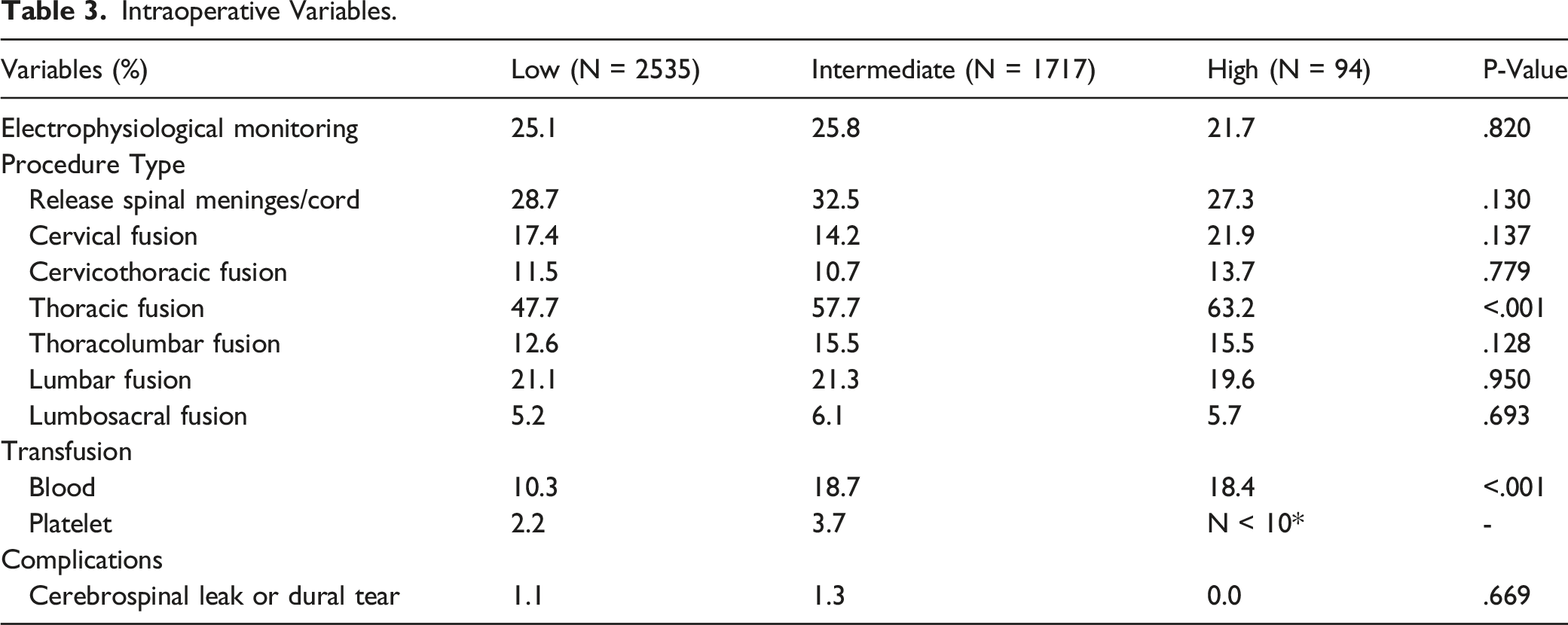
Intraoperative Variables
Intraoperative Variables.
Postoperative Adverse Events
Postoperative Adverse Events.
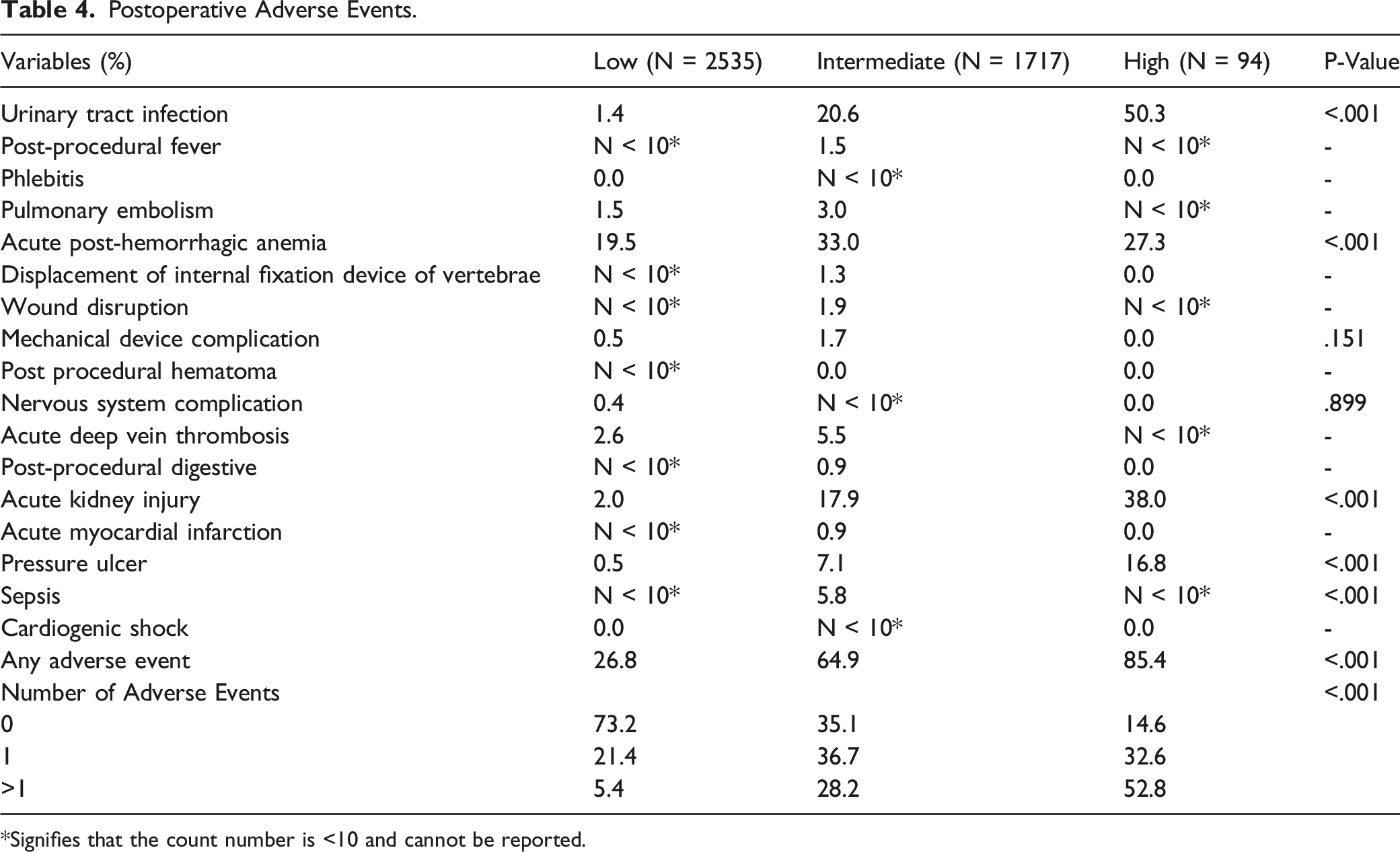
*Signifies that the count number is <10 and cannot be reported.
Postoperative Inpatient Outcomes and Unplanned 30- and 90-Day Readmission Rates
Postoperative Inpatient Outcomes.
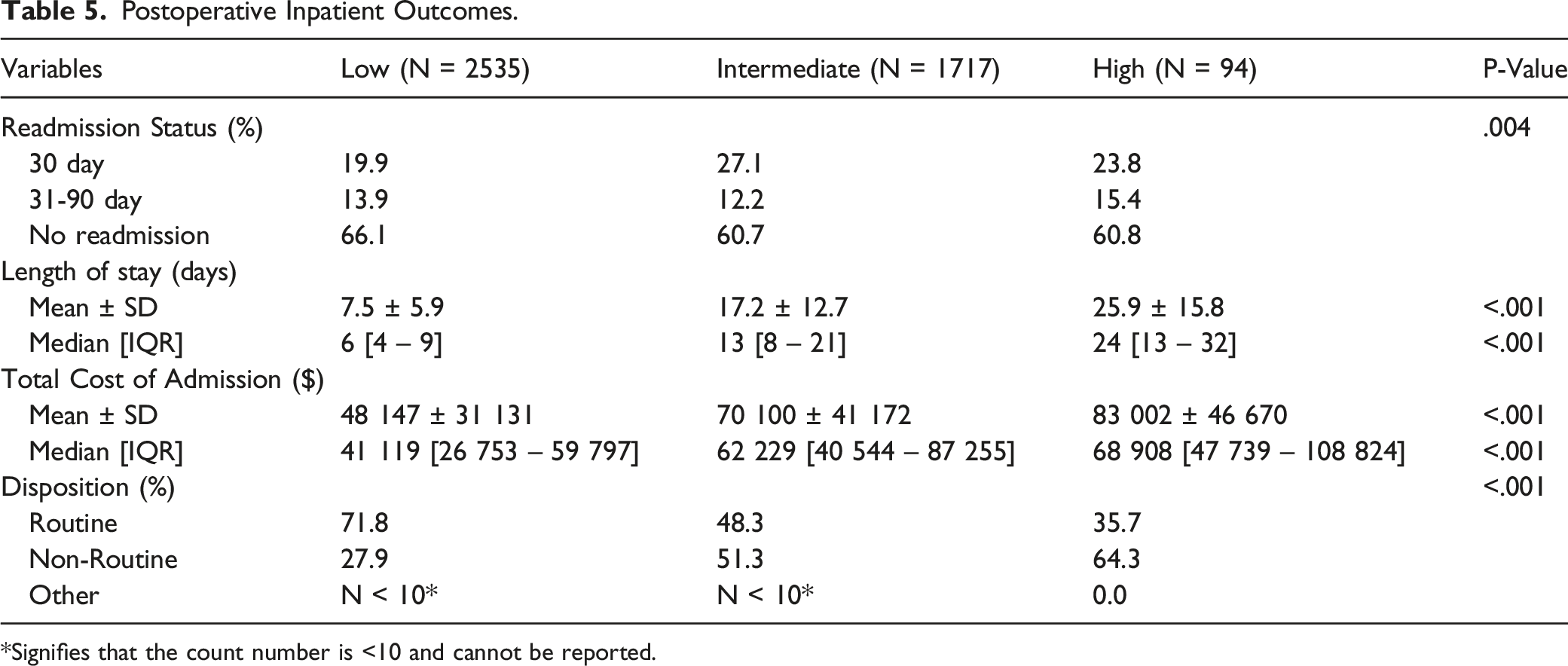
*Signifies that the count number is <10 and cannot be reported.
Multivariate Regression Analysis on 30-day Readmission
Logistic Multivariate Regression Analysis on 30-Day Readmission.
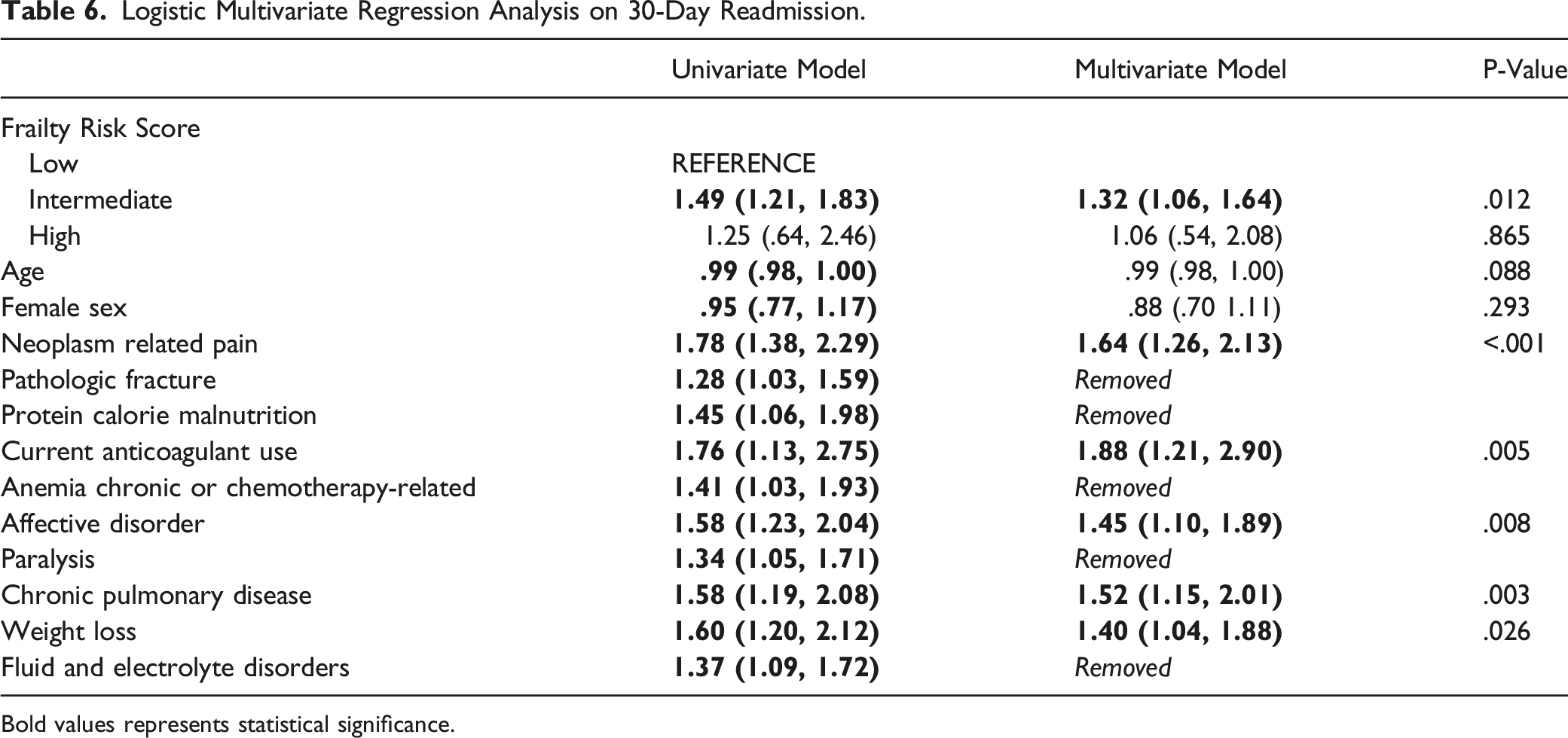
Bold values represents statistical significance.
RF Machine Learning
In assessing features of importance for 30-day readmission, the RF classifier trained on all features (AUC = .60) achieved similar performance to the RF classifier retrained only on the top 10 most important features (AUC = .59). The feature importance (MDGs) of the Top 10 RF classifier and the AUC curves for both models are shown in Figure 1. The most important feature in both models was the HFRS, followed by neoplasm-associated chronic pain and weight loss. Other important features identified included fluid and electrolyte disorders, pulmonary circulation disorders, affective disorder, protein calorie malnutrition, pathologic fracture, anemia chronic or chemotherapy-related, and acute DVT. Machine learning analysis. Summary of machine learning findings for 30-day readmission including feature importance (mean decrease gini) of the top 10 features random forest classifier (A), and AUC Curves for all features random forest (green), Top 10 Features random forest (dark blue), Chance (dotted light blue line) (B). ACCR = Anemia chronic or chemotherapy related. DVT = Deep vein thrombosis.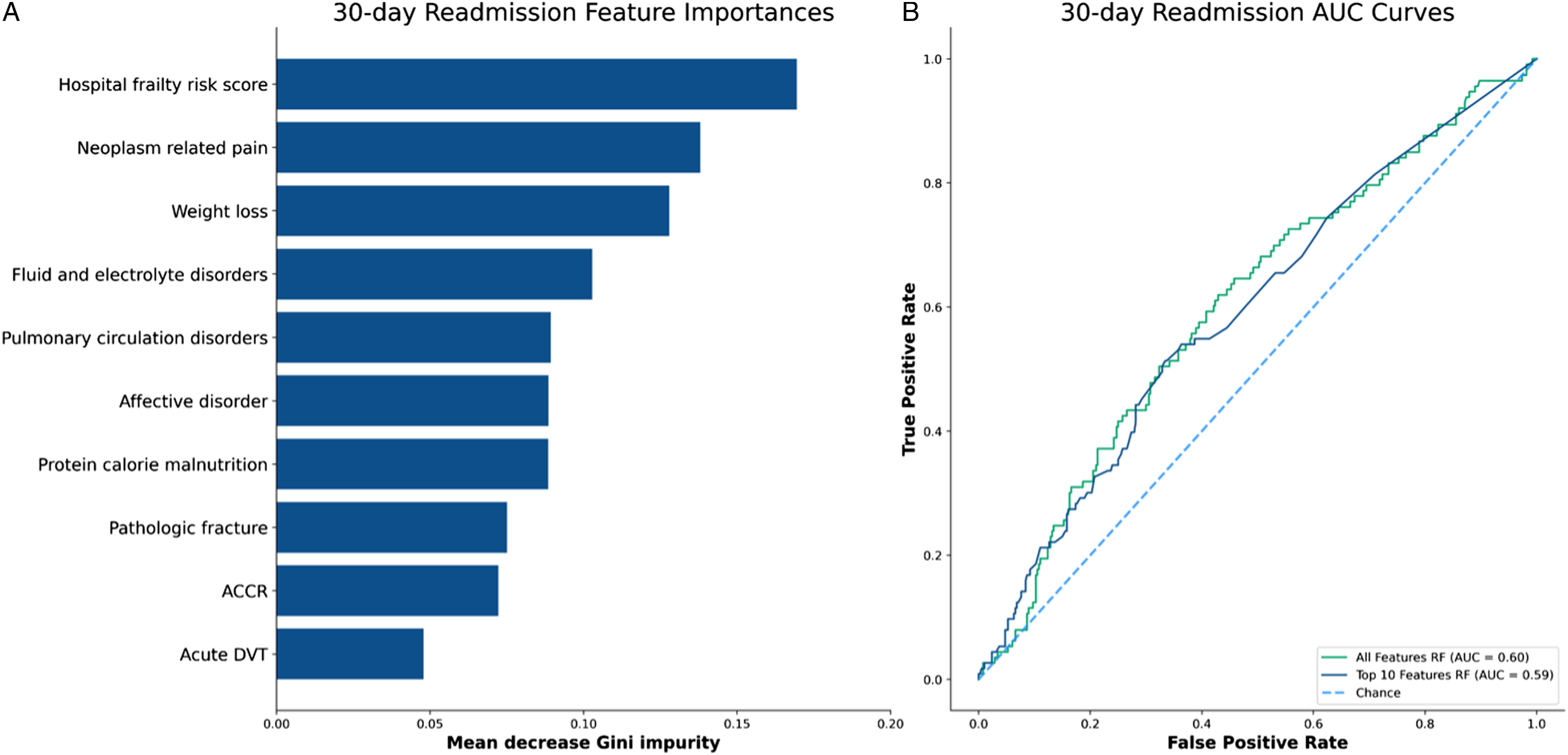
Discussion
In this retrospective NRD study of 4346 patients who underwent spinal surgery for a metastatic spinal column tumor, we found utilizing machine learning analysis that HFRS was the top feature of importance for unplanned 30-day readmission. Additionally, Intermediate frailty (HFRS 5-14.9) was an independent predictor of unplanned 30-day readmission, further demonstrating the clinical impact that HFRS-defined frailty has on patient care and healthcare resource utilization.
Frailty has recently come into focus as a major risk-factor that drives inferior outcomes in many different realms of spinal surgery. Given this potential impact and the significant burden metastatic spinal tumors have on healthcare, previous studies have attempted to determine the prevalence of frailty in patients undergoing spinal surgery for metastatic tumors. For example, in the study of 4583 patients who underwent spinal surgery for a metastatic spinal tumor, De La Garza Ramos et al found that 82.8% of patients had some level of frailty as determined by the MSTFI. 23 In this study, 40.1% were considered mildly frail (MSTFI = 1), 24.7% were moderately frail (MSTFI = 2), and 18.0% were severely frail (MSTFI ≥ 3). 23 In another retrospective, single-institution study of 479 patients undergoing spinal surgery for a metastatic tumor, Massaad et al found a comparatively high rate of frailty among their patient population, reporting that 93.5% of patients were considered some level of frail by MSTFI criteria. 15 Similarly, in a retrospective, single-institution study of 108 patients who had spinal surgery for a metastatic tumor, Bourassa-Moreau et al reported that 81.5% of patients were considered frail, with a score of at least ≥1 on the modified mFI-5. 24 Furthermore, in a retrospective, national inpatient sample (NIS) database study of 11 480 patients undergoing surgery for a metastatic spinal column tumor, Elsamadicy et al found that 38.2% of patients qualified as having either intermediate or high frailty, with an HFRS of ≥ 5. 16 Analogously, our study, which included only patients with some component of frailty, found 58.3% of patients had Low frailty, 39.5% had Intermediate frailty, and 2.16% had High frailty by HFRS criteria. Given these high incidences of frailty in the metastatic spine tumor patient population, a better understanding of frailty and its potential impact on patient care and healthcare resources is warranted.
Previous studies have attempted to assess the impact that frailty has on postoperative complications. In the study of patients undergoing surgery for a spinal metastasis by De la Garza Ramos et al, the authors found on multivariate analysis that even mild frailty significantly predicted AEs, with the likelihood of experiencing a complication significantly increasing as frailty score progressed. 23 Similarly, in a retrospective cohort study of 322 patients who underwent operations for spinal metastases at a single cancer center, Hersh et al found that increased frailty, as determined by the MSTFI and mFI-5, was independently predictive of experiencing ≥ 1 complication. 25 Analogously, our study found that the number of postoperative AEs significantly increased along with progressing frailty, with the proportion of patients experiencing at least 1 AE increasing nearly 10-fold from 5.4% in the Low frailty cohort to 52.8% in the High frailty cohort. While these studies suggest frailty to be a good predictor of complications in patients undergoing surgery for a metastatic spinal lesion, other studies have found frailty to be a poor predictor of postoperative AEs in this patient population. For example, in a retrospective, National Surgical Quality Improvement Program (NSQIP) database study of 2170 patients who underwent surgery for a primary or metastatic spine tumor between 2008 and 2014, Lakomkin et al found on multivariate regression analysis that frailty, defined by a mFI-11 score of ≥.27, was not a significant predictor of minor or major postoperative complications. 26 Additionally, in a single-center, retrospective cohort study of 41 patients who underwent spinal surgery for a metastatic lesion, Mohd Rothi et al found that frailty, similarly defined by an mFI-11 score of ≥.27, did not associate with a greater risk of complications. 27 As the current literature has variable findings, further studies are required to better elucidate the impact of frailty on complication rates in patients surgically managed for spinal metastases.
Additional studies have analyzed the impact of frailty on LOS, which has served as a proxy reflective of both healthcare quality and cost.28,29 In a retrospective cohort study of 113 patients undergoing spinal surgery for a primary or metastatic tumor, Charest-Morin et al found on multivariate analysis that frailty, when determined by a mFI-11 score of ≥.21, was an independent predicator of prolonged LOS. 30 Similarly, in the study of 322 patients who underwent surgery for a spinal metastasis by Hersh et al, the authors found that increasing scores in both the MSFTI and mFI-5 were both independentlypredictive of prolonged LOS. 25 Furthermore, in the study of surgically managed patients with primary or metastatic tumors by Lakomkin et al, the authors determined that frailty was significantly associated with elongated LOS. 26 Moreover, in the study of metastatic spinal tumor patients by De la Garza Ramos et al, the authors showed that mean LOS nearly doubled from patients with no frailty to patients with severe frailty. 23 Similarly, our study found that mean LOS got significantly longer with progressing frailty, increasing nearly 4-fold from Low to High frailty classification. In other studies, however, authors have noted there to be no relationship between frailty and LOS in patients undergoing surgery for a metastatic spinal lesion. For instance, in a retrospective study of 350 patients surgically treated at a single cancer center for either primary or metastatic tumors of the vertebral column, Ehresman et al found that frailty, as determined by the mFI-5, did not associate with a prolonged LOS. 31 Analogously, in the study by Massaad et al, the authors found that although mean LOS did increase alongside progressing frailty, the difference was determined to not be statistically significant. 15 Given the variable findings reported across the current literature, additional studies are required to further understand how frailty may impact LOS.
Rates of unplanned readmissions after spine surgery have ranged throughout the literature.32,33 Despite the high rates of frailty and potential negative impact on surgical outcomes in patients with metastatic spinal lesions, there remains a paucity of studies that analyze how frailty may influence unplanned hospital readmissions. There have been a few studies that suggest that drivers of readmission after surgery for a spinal metastasis may be due to surgical complications, 33 while others have reported medical complications as primary drivers. 34 In our study, we found that increasing frailty, as defined by HFRS, was the highest feature of importance for 30-day unplanned readmission, and intermediate frailty was an independent predictor of 30-day unplanned readmission. Thus, it is reasonable to suggest that a patient’s frailty status may have increase the risk of both medical and surgical complications. However, high frailty was not found to independently predict 30-day readmission on multivariate analysis. This finding may be secondary to multiple confounding factors. First, patients with high frailty were significantly older, with higher rates of comorbidities and perioperative complications. Therefore, the established care of these patients is likely long term as compared to the less frail patients, which may increase the threshold for which this patient group would return to the hospital. Second, a significantly greater proportion of patients in the High Frailty cohort were discharged to a nursing or rehab facility. The focused care of 1 of these facilities may have reduced the need to return to the hospital. Lastly, severely frail patients may die at higher rates following surgery, which would not be reflected in the analysis. Interestingly, the Intermediate frailty population are the ones who are impacted the most, as they are more inclined than the low frailty cohort to suffer adverse health events but are likely managed less intensively postoperatively than patients in the high frailty cohort. A further understanding of the complex relationship between frailty and outcomes following surgery for a metastatic spinal lesion could be yielded by comparing population-level differences between the Intermediate and High frailty cohorts. Nevertheless, while these studies suggest some level of frailty to be a key risk-factor for these proxies of cost-driving adverse outcomes, the current paucity of literature makes the results difficult to verify. This highlights the need for further studies assessing how frailty impacts unplanned return to hospital after discharge.
Machine learning is an emerging field in spinal surgery that utilizes large data to identify important preoperative variables that may influence postoperative outcomes, aiding surgeons in decision-making and outcome prediction. Better outcome prediction in patients undergoing spinal surgery could dramatically reduce healthcare resource utilization, as it is estimated that 21 to 47% of the annual US healthcare costs were attributable to avoidable events, such as readmissions. 17 Here, we demonstrate how machine learning was used to identify HFRS-defined frailty as an important preoperative factor that contributes to increase rates of readmission in patent’s undergoing spinal surgery for metastatic tumors. Such an approach could be used in clinical practice and by hospital administrators to tailor risk models based on institutional data. This data may help identify and create opportunities to for pre and postoperative programs to be established to better serve higher risk patients, such as enhanced recovery after surgery protocols (ERAS). While further investigations are ongoing, a better understanding on the relationship between the severity of frailty and unplanned hospital readmissions after spine surgery may provide better patient care and reduce high healthcare expenditures.
Our study has several limitations inherent to administrative database studies. First, the analysis is retrospective, with data available only by ICD-10 diagnostic and procedural codes, which may contain coding and reporting biases. Second, as the analysis was generated from data contained within a national database, there may be misclassified, or incomplete data reported. Third, as the NRD has limited preoperative and intraoperative variables included, there may be an underlying consistent difference between the 3 cohorts that has an underappreciated effect on our results. Additionally, further granularity of the extent of comorbidities is limited by the ICD-10-CM coding in the available database. However, despite these limitations, our study utilizes machine learning and 1 of the largest national readmission databases in the US to provide unique insights into the impact frailty has on unplanned 30-day hospital readmission after spine surgery for metastatic spinal column tumors.
Conclusion
Our study utilizes machine learning approaches and predictive modeling to identify frailty as a significant risk-factor that contributes to unplanned 30-day readmission after spine surgery for metastatic spinal column tumors. Further multi-institutional, prospective studies are needed to validate these findings and better understand how the severity of frailty impact patient outcomes.
Supplemental Material
Supplemental Material - Utilization of Machine Learning to Model Important Features of 30-day Readmissions following Surgery for Metastatic Spinal Column Tumors: The Influence of Frailty
Supplemental Material for Utilization of Machine Learning to Model Important Features of 30-day Readmissions following Surgery for Metastatic Spinal Column Tumors: The Influence of Frailty by Bogdan G. Popescu and Mircea Popa in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.