
Abstract
Study Design
Retrospective study.
Objective
To investigate the clinical and radiological outcomes of patients with lumbar degenerative disc disease (DDD) treated with one-level Direct lateral interbody fusion (DLIF) in combination with minimally invasive percutaneous pedicle screw fixation (PPSF) and percutaneous facet joint fixation (PFJF).
Methods
This retrospective single-center study included 98 patients (67 men, 31 women) aged 28 to 59 years with one level lumbar DDD with foraminal and central stenosis, were divided into groups after DLIF: PPSF (n = 50) and PFJF (n = 48). Intraoperative parameters, perioperative clinical data and radiological assessment with X-ray, MRI and CT were used before operation and mean 45-month follow-up. Workload intensity criteria were used to analyze return to work rate.
Results
The DLIF-PFJF group had significantly shorter surgery time (P = .04), duration of anesthesia (P = .02), X-ray time (P = .02), less back pain (P = .03), better functional status according to ODI (P = .04) and SF-36 PCS (P = .04), less atrophic changes in the multifidus muscle compared with DLIF-PPSF. There were no statistically significant differences in the volume of blood loss, duration of inpatient treatment, VAS leg pain, SF-36 MCS, Macnab results, mean disc height, intervertebral foramen height, sagittal disc angle, global lumbar lordosis, fusion rate, and the number of complications. In heavy/very heavy workload patients, the DLIF-PFJF had a statistically significantly higher rate of return to work compared to the DLIF-PPSF group.
Conclusions
DLIF-PFJF appears to be superior to DLIF-PPSF, minimizing invasiveness, which significantly reduces the damage to the paraspinal muscles and also has significant long-term clinical advantages and return to work rates. Both minimally invasive techniques have comparable radiographic parameters, including the height of the intervertebral foramen and disc, fusion rates, global and segmental sagittal correction after surgery.
Keywords
Introduction
Direct lateral interbody fusion (DLIF) is a minimally invasive lateral lumbar interbody fusion (LLIF) technique 1 that is a popular treatment for various degenerative lumbar spine diseases. 2 The main advantages of DLIF include: the possibility of indirect decompression, effective correction of coronal and sagittal imbalance, the absence of complications occurring with anterior and posterior approaches.3,4 In addition, the anterior and posterior longitudinal ligaments remain intact, which provides stability and may enhance fusion rates. 5
For additional stabilization of the posterior support complex after DLIF, open and percutaneous pedicle screw fixation are often used. 2 Percutaneous insertion has been shown to result in less damage to paravertebral soft tissues, muscles and ligaments, reduce postoperative pain and improve quality of life compared to open techniques. 6 On the other hand, percutaneous fixation is associated with a higher risk of screw malposition and damage to neurovascular structures, as well as increased intraoperative radiation.7,8 Facet fixation is another technique for posterior fixation, which has the theoretical advantage of reducing surgical trauma. 9 The most common translaminar fixation technique in combination with LLIF has been reported to have good clinical and radiological results.10,11 Studies have demonstrated that using bilateral titanium wedge-shaped plate-cages in the facet joint in addition to DLIF is effective at reducing pain and improving quality of life. 2
To our knowledge, there is a paucity of studies comparing percutaneous bi-pedicle screw fixation and bilateral facet fusions using titanium wedge-shaped plate-cages in addition to DLIF. We therefore undertook this comparative analysis of the clinical and radiological results after one-segment DLIF and minimally invasive posterior stabilization with two different systems.
Therefore the purpose of our retrospective study is to investigate the clinical and radiological outcomes of patients with lumbar degenerative disc disease (DDD) treated with one-level DLIF in combination with minimally invasive percutaneous pedicle screw fixation (PPSF) and percutaneous facet joint fixation (PFJF).
Materials and Methods
Subjects and Methods
A total of 12 087 procedures were performed in patients with degenerative disease of the lumbar spine between 2005 to 2020 at the Neurosurgery center of Irkutsk Railway Clinical Hospital. Each patient gave voluntary statement regarding informed consent to be included in the study. The course and nature of the surgical intervention were explained to the patients in details. The study was approved by the Ethics Committee of Irkutsk State Medical University.
We retrospectively studied 98 patients having undergone DLIF at our surgical institution. Anterior fixation with DLIF cage was performed followed by one of two posterior fixation techniques: (1) percutaneous pedicle screw fixation and (2) percutaneous facet joint fixation. The subjects railway workers who underwent one-level short-segment lumbar fixation for lumbar degenerative disk disease with foraminal and central stenosis, mean follow-up period 49 (30;57) months for DLIF-PPSF group and 45 (31;52) months for DLIF-PFJF group. In 15 cases, patients refused the proposed participation in the study and were excluded from it. The study design is shown in Figure 1. Study flowchart. DLIF – direct lumbar interbody fusion. Excluded reason (1): Reason * - Isolated decompression; Reason ** - Another type of decompression-stabilization (TDR, ALIF, TLIF or combination). Excluded reason (2): Reason * - single-level DLIF for deformity or instability; Reason ** - multilevel DLIF or combination of TLIF and ALIF; Reason *** - revision surgery. Exclude reason (3): Reason * - loss of follow-up; Reason ** - refusal to participate in the study; Reason *** - death unrelated to the operation (in these cases, there were no postoperative complications).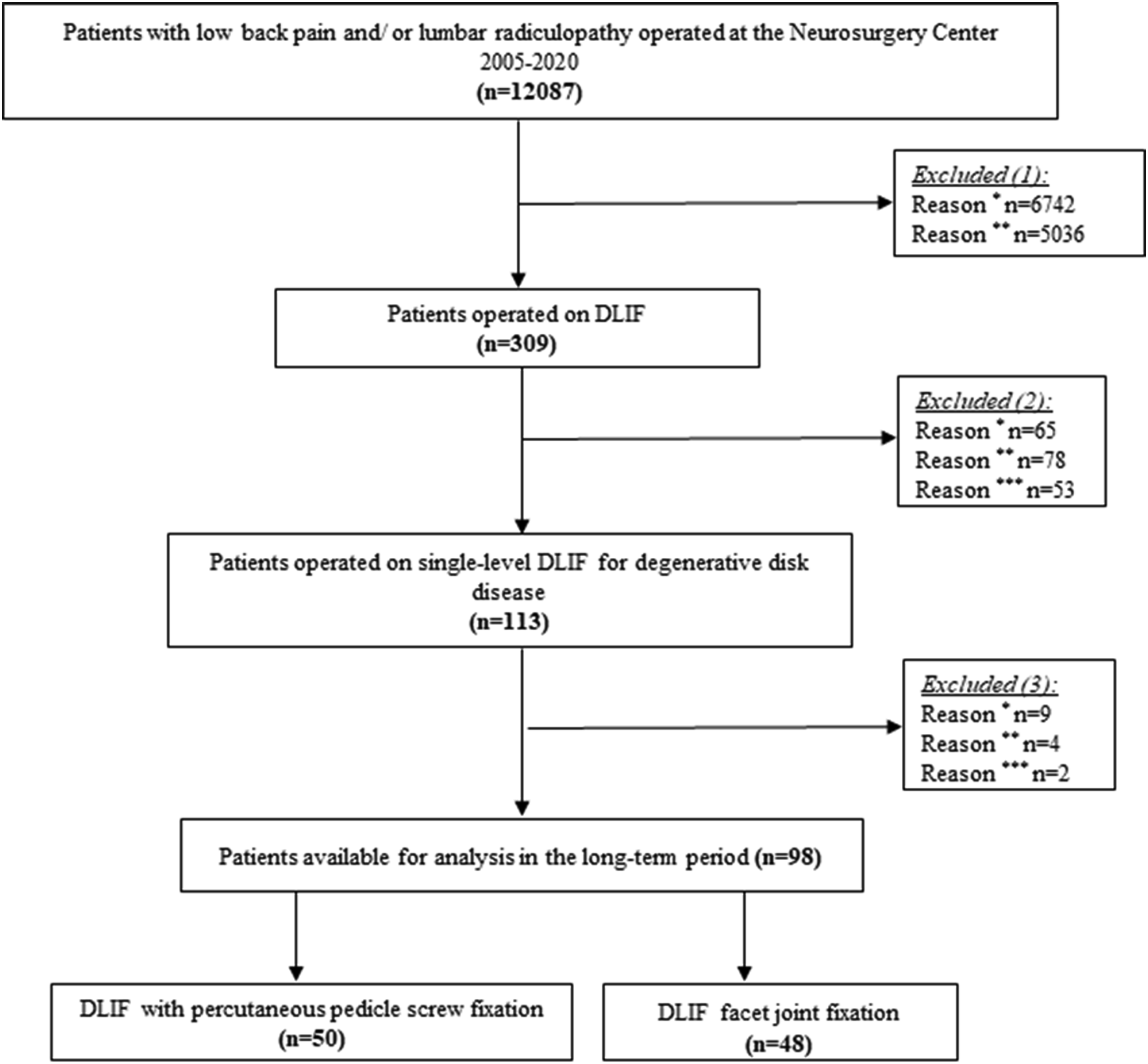
The patients’ data used to support the findings of this study are restricted by the Ethics Committee of Irkutsk State Medical University in order to protect of the patient privacy. Data are available from the corresponding author Vadim A. Byvaltsev for researchers who meet the criteria for access to confidential data. The analysis of the clinical material was carried out in accordance with the principles of the Declaration of Helsinki. Primary and secondary endpoints of the study were from preop to a mean of 45 months post-op.
Inclusion Criteria
- degenerative disk disease with foraminal and grade 1 (mild) central stenosis based on Lee et al
12
; - failed to respond to conservative therapy for 4 to 8 months and discography-proven origin of pain; - back pain with radicular pain; - monosegmental lesion and/or the need for a single-level surgical intervention; - primary surgery in the lumbar spine.
Exclusion Criteria
- adult spinal deformity; - degenerative spondylolisthesis with or without stenosis; - polysegmental lesion and/or the need for multilevel surgical intervention; - revision cases; - refusal to participate in the study.
Surgical Techniques
One primary surgeon (Vadim A. Byvaltsev) performed all cases with DLIF and minimally invasive posterior fixation. Patients were positioned in the lateral decubitus position under general anesthesia. The DLIF technique involved a standard muscle splitting retroperitoneal approach using blunt dissection. Triggered and free running electromyography (EMG) monitoring was used to avoid injury to the lumbar plexus and ensure neural elements were not traversing the operative field. After lateral annulotomy, a thorough discectomy and endplate preparation using cup and box curettes were performed. The contralateral annulus was then released and the disc space assessed with trial implants before inserting an appropriate sized polyether ether ketone (PEEK) interbody implant (Oracle, DePuy Synthes, USA, no conflict interest). After this, in the prone position, percutaneous pedicle screw fixation was performed in 50 cases (Group I, DLIF-PPSF). Percutaneous bilateral facet-joint fixation with titanium wedge-shaped plate-cages were performed in the lateral decubitus position in 48 cases (Group II, DLIF-FJF). In all cases we did not use bone morphogenetic protein.
Perioperative Outcomes
Surgery time, duration of anesthesia, blood loss, fluoroscopy times, duration of inpatient treatment were recorded by medical card after surgery.
Clinical Outcomes
Clinical outcomes, including Visual Analogue Scale (VAS) back pain and leg pain scores, Macnab scale, Oswestry Disability Index (ODI) and SF-36 scores were obtained pre- operatively and last follow-up. Workload intensity criteria were used to analyze return to work at last follow-up period (mean 45 months after operation), which included sedentary, light-moderate and heavy-very heavy type of the workload (https://occupationalinfo.org).
Radiological Evaluation
Radiological outcomes were assessed pre- and postoperatively (mean 45 months after operation) using a combination of magnetic resonance imaging scans, computed tomography scans and plain X-rays of the lumbar spine. We measured mean disc height, sagittal disc angle, intervertebral foramen height, the multifidus muscle area at the preoperative and last postoperative follow-up period. Fusion rate was assessed at the final postoperative follow-up period using the Bridwell fusion grading criteria on CT scans. 13
Mean disc height was calculated as the mean value of the anterior disc height (mm) and posterior disc height (mm) in lateral images. Sagittal disc angle was measured between the lower endplate of the upper vertebra and the upper endplate of the lower vertebra. Global lumbar lordosis was measured between the superior endplate of L1 and the superior endplate of S1.
Facet height was measured by the distance between the inferior margin of the pedicle of the upper vertebra and the superior margin of the pedicle of the lower vertebra on the lateral X-ray.
The multifidus muscle area was calculated from anonymized axial T2w MRI images using the MultiVox DICOM Viewer software (Gamma Multivox, Moscow, Russia). Multifidus muscles were segmented from preoperative and postoperative MRIs using anatomical landmarks, and the total area for the right and left sides of each level were recorded. 14 The average muscle area across all three levels (overlying segment, operation level, underlying segment) was calculated. The postoperative muscle areas were subtracted from the preoperative area for each patient, then divided by the preoperative area in order to assess a percent area change for each individual. Statistical analysis was performed on the percent area change metric as one indication of muscle atrophy. In this study, multifidus fat content was not assessed.
MRI and CT patient data were de-identified and performed by two independent reviewers (neurosurgeon and radiologist). Statistical evaluation of expert agreement on each question was carried out using Kappa statistics (Graph Pad Software, Inc, USA).
Surgical Complication Assessment
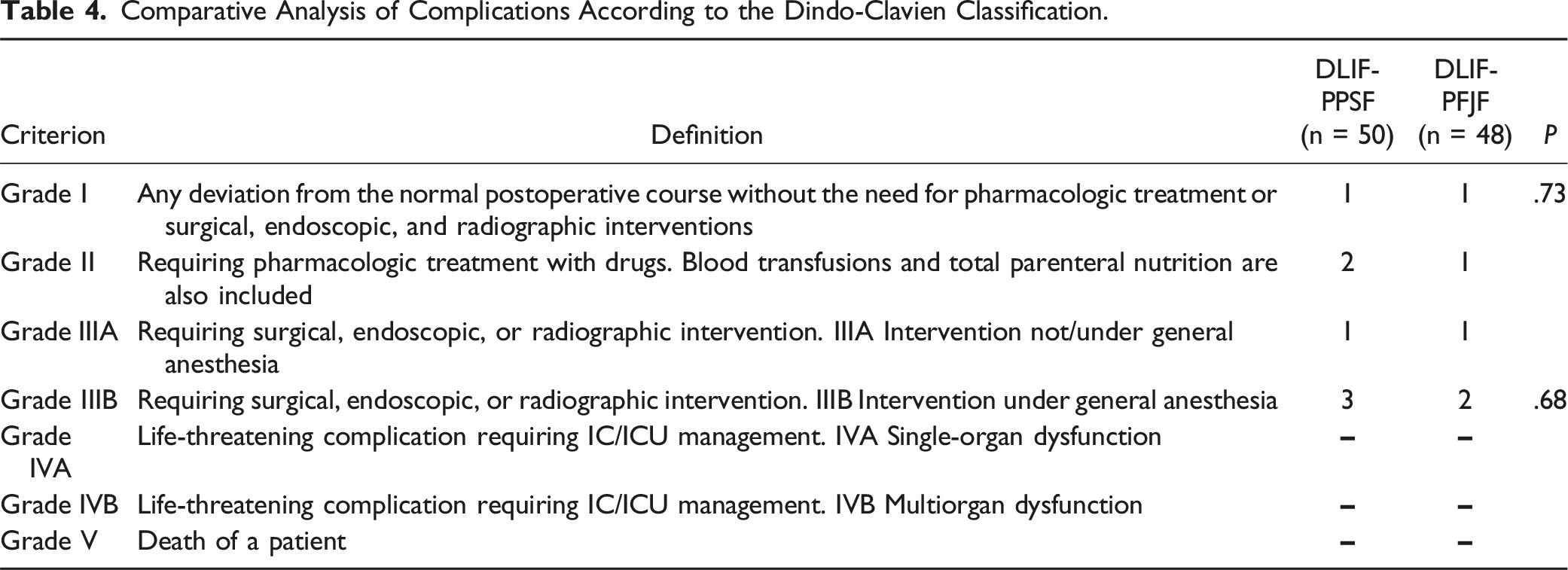
All surgical complications that caused re-admissions and revision interventions according to the Dindo-Clavien classification 15 were evaluated using medical cards and postoperative clinical notes.
Statistical Analysis
Statistical analysis was carried out on a personal computer using the Statistica 13.2 program. The necessary statistical power of the study and the number of cases in each group were calculated, and the ODI score was considered the main indicator of functional outcome. A minimum of 37 cases was needed in each group to achieve 80% statistical power, with P < .05 as the 2-tailed level of significance indicating achievement of the minimum clinically significant 10-point difference in ODI score (standard deviation = 15). The character of the distribution of signs was evaluated by the Shapiro — Wilk, Kolmogorov — Smirnov and Lilliefors tests for normality. Considering the presence of statistically significant differences according to these tests (P < .05), the distribution was considered to be different from normal. In this regard, the criteria of nonparametric statistics were used to assess the significance of the differences in the samples. The obtained results are presented by the median, the values of the 1st and 3rd quartiles — Me (Q25; Q75). For a comparative analysis of the obtained values, the Mann — Whitney U—test and the Wilcoxon criterion, the χ2 criterion for binomial signs were used. The differences were considered significant at the level of P < .05.
Results
Patient Features and Surgical Data.
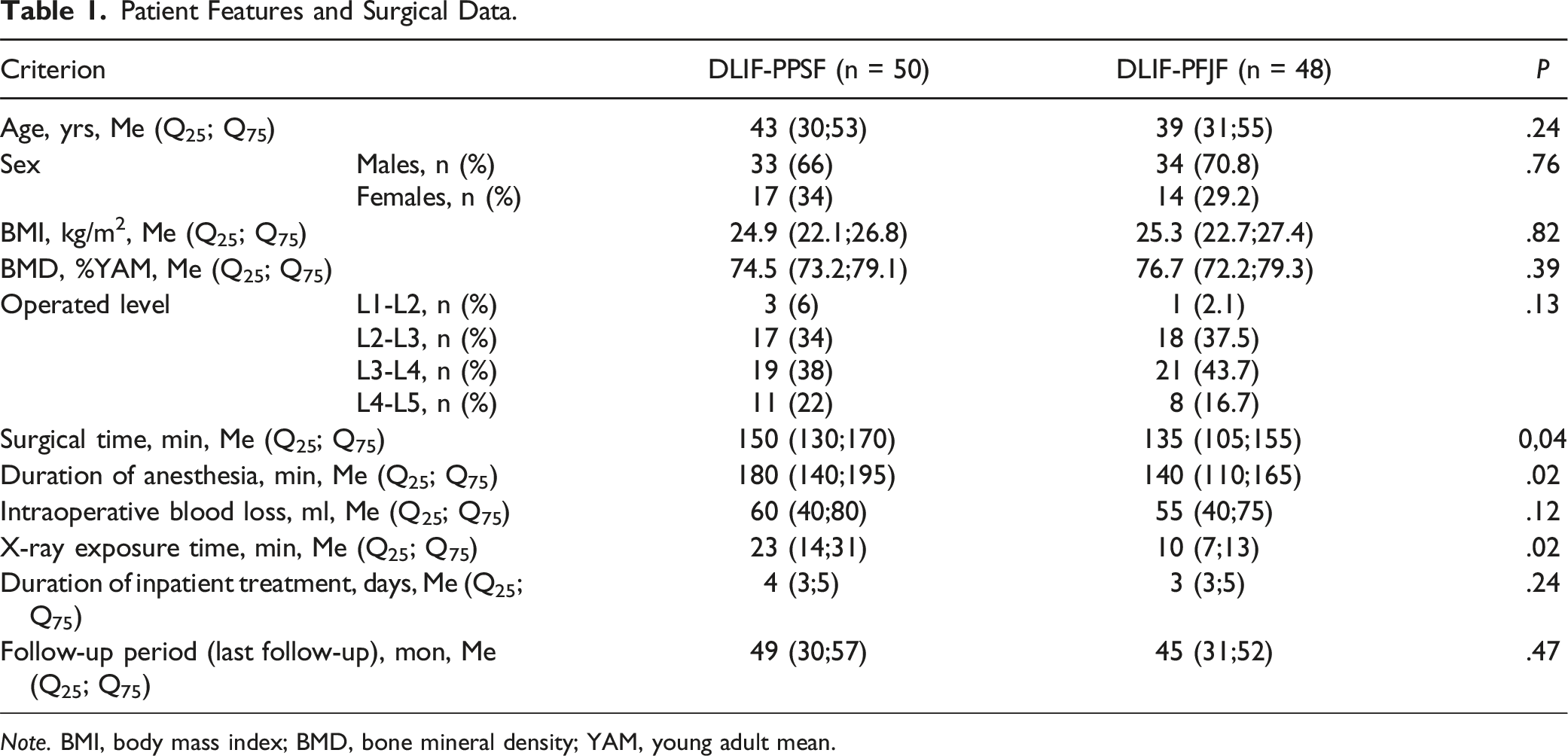
Note. BMI, body mass index; BMD, bone mineral density; YAM, young adult mean.
Clinical Results of the Studied Patients.
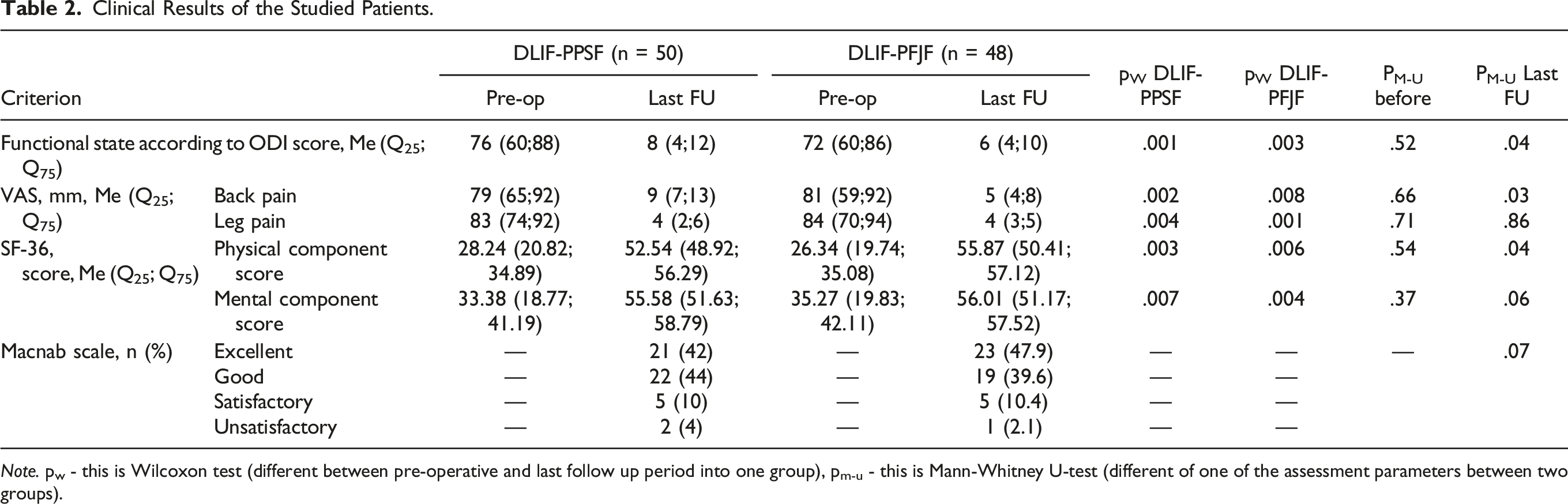
Note. pw - this is Wilcoxon test (different between pre-operative and last follow up period into one group), pm-u - this is Mann-Whitney U-test (different of one of the assessment parameters between two groups).
Radiologic Measurements of the Studied Patients.
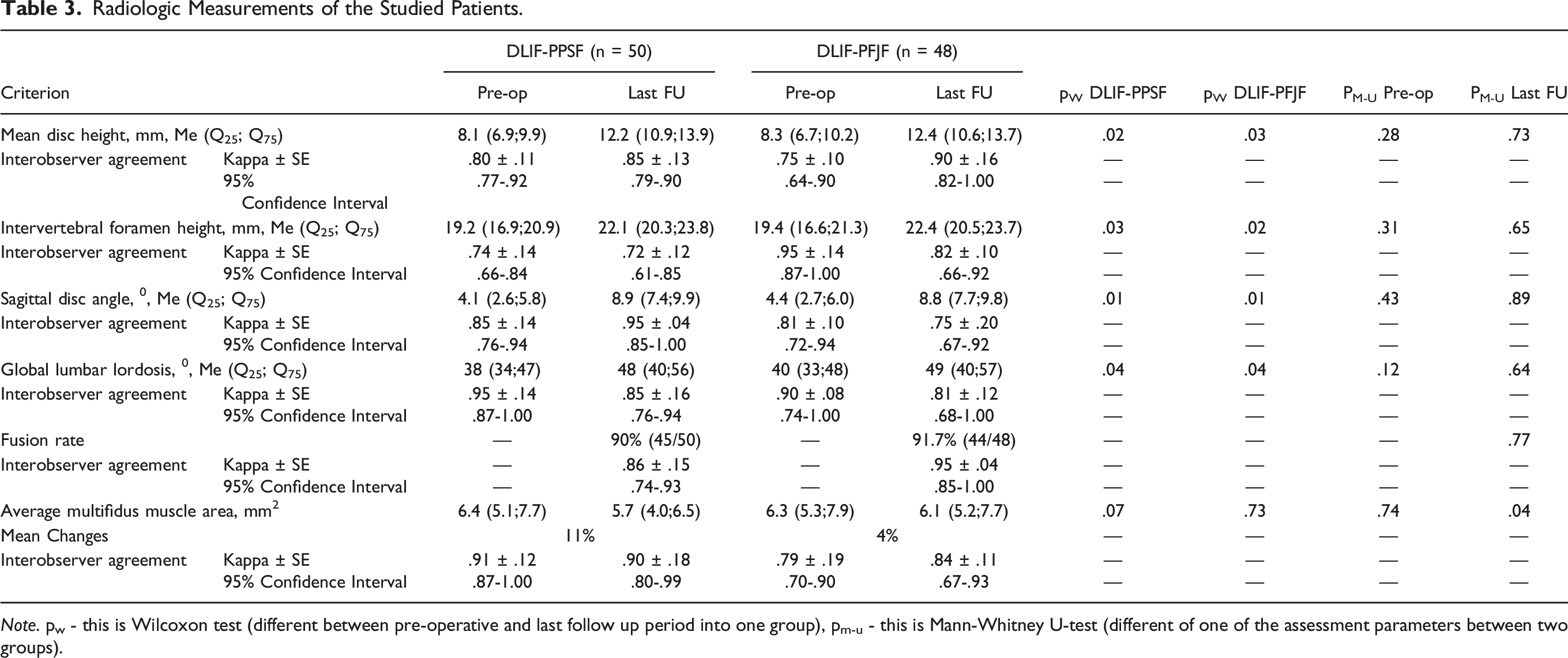
Note. pw - this is Wilcoxon test (different between pre-operative and last follow up period into one group), pm-u - this is Mann-Whitney U-test (different of one of the assessment parameters between two groups).
There were no significant differences in any of the preoperative radiological parameters (P > .05). In each group, mean disc height, facet height, and sagittal disc angle were statistically significantly increased at last follow-up compared to preop (all P < .05). There were no differences between the groups at last follow-up in the mean disc height (P = .73), facet height (P = .65), sagittal disc angle (P = .89) and global lumbar lordosis (P = .64). The fusion rate at last follow-up was 90% (45/50) in the DLIF-PPSF group and 91.7% (44/48) in the DLIF-PFJF group, respectively, with no significant difference. There was no significant difference in muscle atrophy between preoperative and last follow-up for either group (P = .07 for PPSF; P = .73 for PFJF). However, at last follow-up, the pedicle fixation group had significantly greater muscle atrophy than the Facet fixation group (P = .04).
Comparative Analysis of Complications According to the Dindo-Clavien Classification.
Return to Work Rate at Mean 45 months Stratified by Workload and Surgical Procedure.
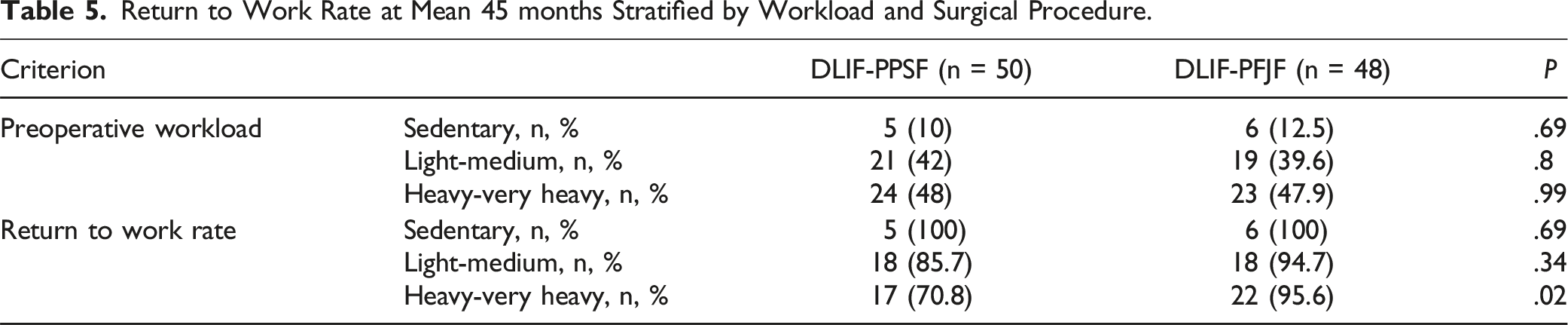
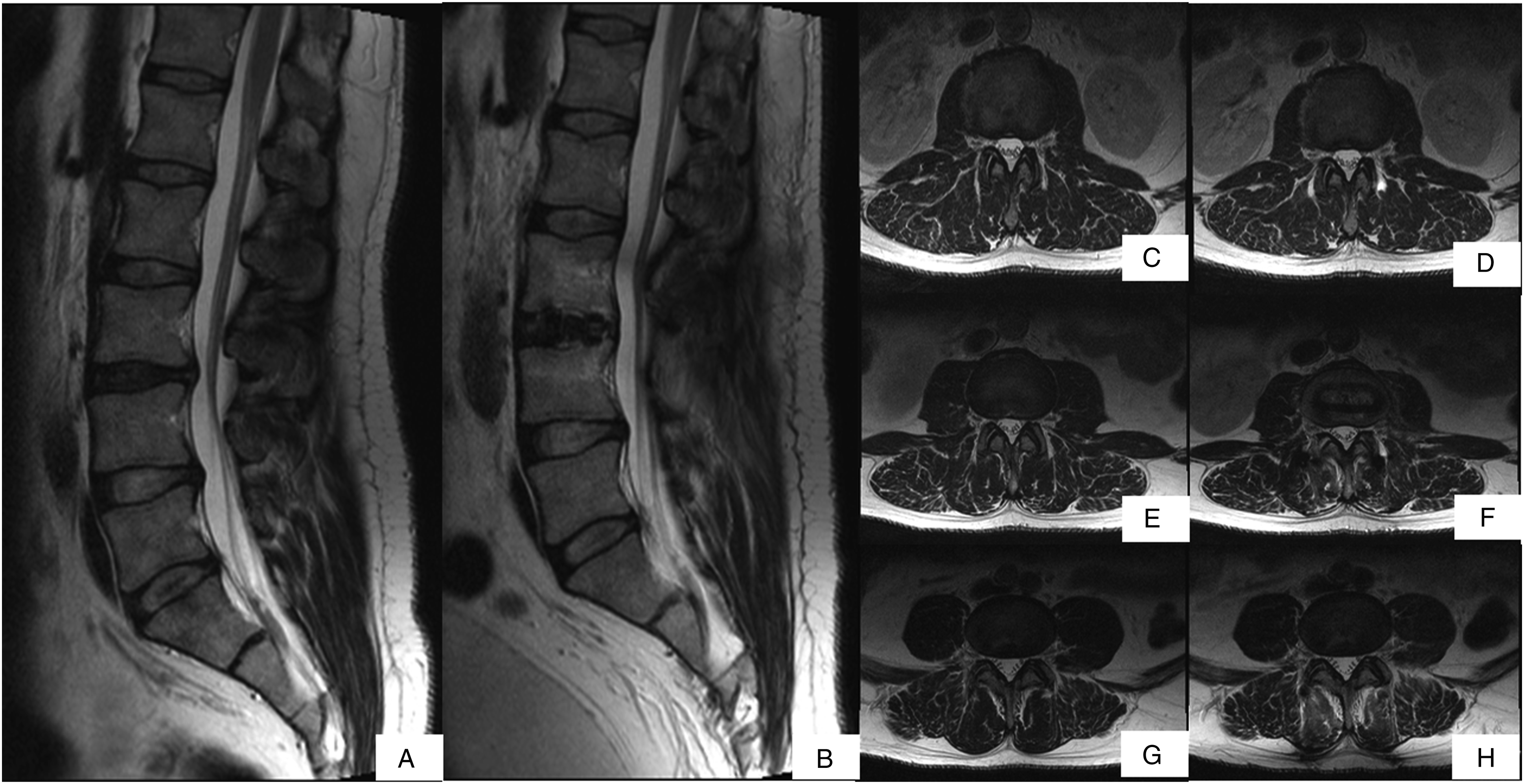
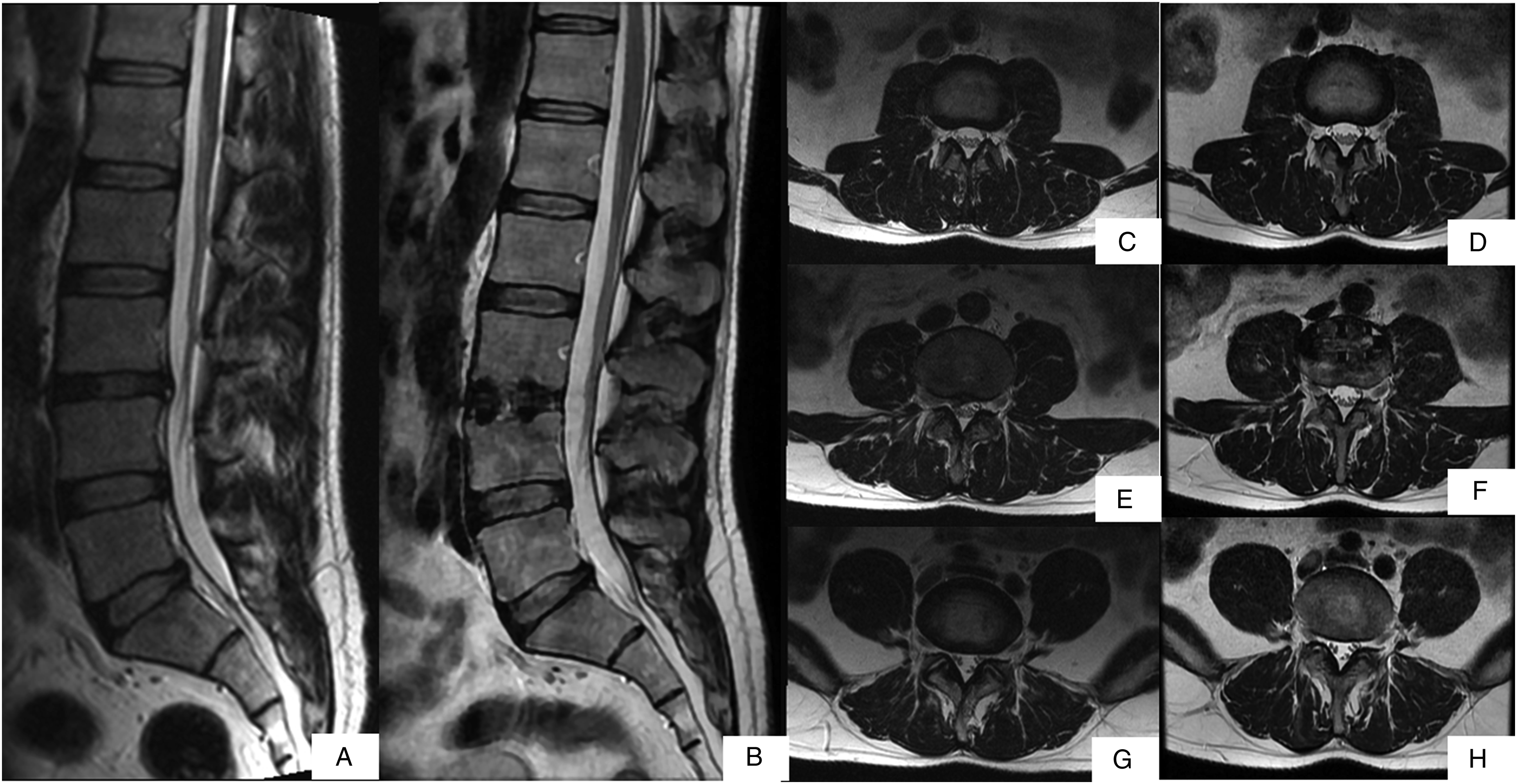
Figure 2 shows standing anterior-posterior and lateral X-rays of patients after DLIF with percutaneous pedicle screw fixation (a,b) and percutaneous facet joint fixation (c,d). Figures 3 and 4 present MRI clinical cases of patients who underwent DLIF with percutaneous pedicle screw fixation and facet joint fixation, respectively. Postoperative standing anterior-posterior and lateral X-rays: (A, B) – after DLIF with percutaneous pedicle screw fixation; (C, D) – after DLIF with percutaneous facet joint fixation. Clinical case, Male, 39 yo, underwent DLIF with percutaneous pedicle screw fixation, MRI T2w: (A) — preoperative sagittal MRI; (B) — postoperative sagittal MRI; (C) — preoperative axial MRI at L2-L3 (overlying segment); (D) — postoperative axial MRI at L2-L3 (overlying segment); (E) — preoperative axial MRI at L3-L4 (operation level); (F) — postoperative axial MRI at L3-L4 (operation level); (G) — preoperative axial MRI at L4-L5 (underlying segment); (H) — postoperative axial MRI at L4-L5 (underlying segment). Postoperative change in multifidus muscle area was 16%. Clinical case, Male, 40 yo, who underwent DLIF with facet joint fixation, MRI T2w: (A) — preoperative sagittal MRI; (B) — postoperative sagittal MRI; (C) — preoperative axial MRI at L2-L3 (overlying segment); (D) — postoperative axial MRI at L2-L3 (overlying segment); (E) — preoperative axial MRI at L3-L4 (operation level); (F) — postoperative axial MRI at L3-L4 (operation level); (G) — preoperative axial MRI at L4-L5 (underlying segment); (H) — postoperative axial MRI at L4-L5 (underlying segment). Postoperative change in multifidus muscle area was 2%.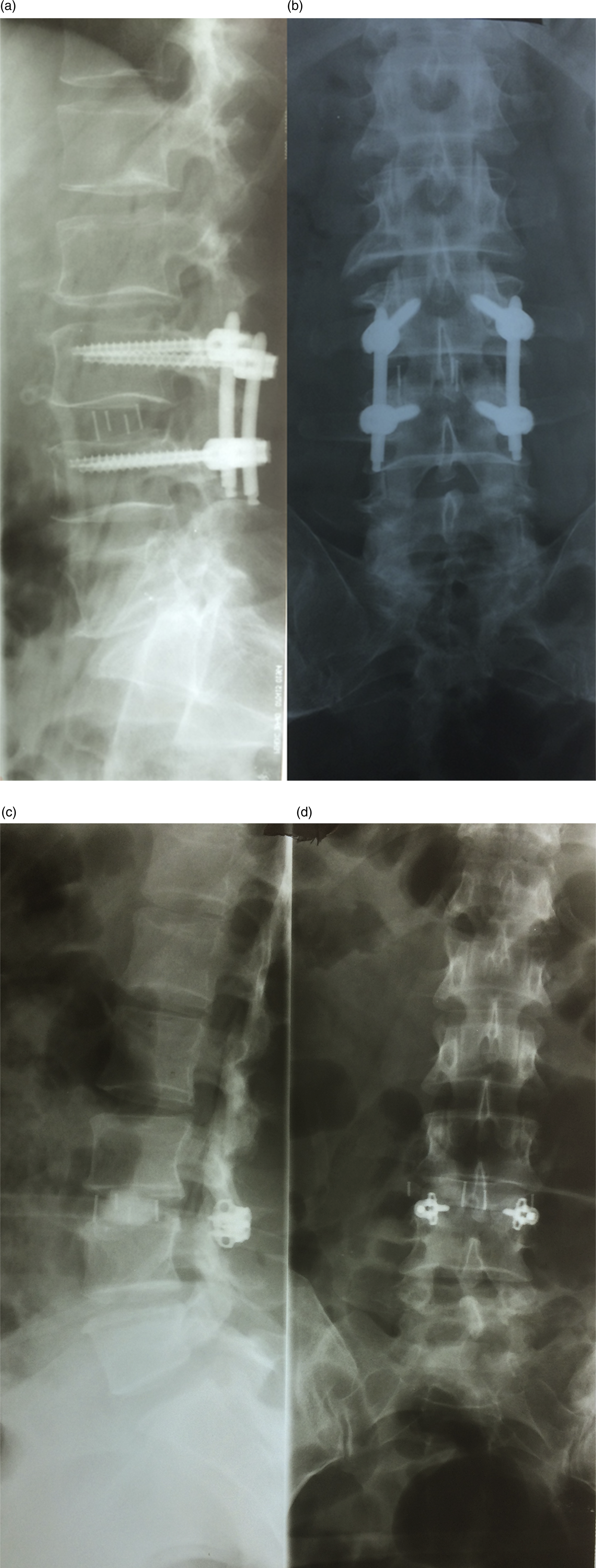
Discussion
Treatment of degenerative disc disease with LLIF can result in improvement in axial and sagittal canal diameter, cross-sectional area of the spinal canal, back and lower extremity pain and increased disk and foramina height. 16 DLIF is a minimally invasive alternative to traditional lumbar interbody fusion techniques that provides indirect decompression with access through the retroperitoneum and psoas muscle that avoids major vessels and visceral organs. 17 Moreover, the effectiveness of indirect decompression during DLIF is reduced in the presence of severe arthropathy of the facet joints, which may constitute a relative contraindication for its implementation. 18 Transpedicular fixation after lumbar interbody fusion is the gold standard for restoring the stability of the posterior support complex. 19 Significant surgical trauma, severe pain and postoperative muscle atrophy associated with open pedicle screw fixation led to the widespread use of percutaneous stabilization techniques.20,21 However, percutaneous pedicle screw fixation increases the risk of intra-canal (dural tear, nerve root damage), extra-canal (vascular and visceral), as well as infectious complications.22-24 In comparison to transpedicular screws, facet-joint stabilization does not carry significant risks of damage to intra-or extra-canal structures, with comparable fixation.25,26 We undertook this study to determine if the two supplemental fixation techniques (PPSF – percutaneous pedicle screw fixation and PFJF – percutaneous facet joint fixation) yielded comparable radiographic and clinical results. To our knowledge, our analysis of clinical and radiographic outcomes, postoperative muscle atrophy, return-to-work rates with DLIF supplemented with two different posterior fixation techniques in a large population of manual laborers with a mean 45 months follow-up has not been conducted before.
The DLIF technique preserves the anterior and posterior longitudinal ligaments, as well as the facet joints, so some consider standalone cages as adequate stabilization without additional posterior instrumentation. Marchi noted that the use of osteoinductive material and large custom cages resulted in acceptable fusion rates without the need for additional posterior fixation. 27 On the other hand, biomechanical studies indicate better stability of the operated segments when combining DLIF with transpedicular stabilization. 28 In addition, according to some authors, standalone cages without additional posterior instrumentation may be associated with implant subsidence, pseudoarthrosis, and worse indirect decompression.29,30 This may be due to the continued presence of micromotion and decreased mechanical rigidity at the operated level. 31 Clinically significant benefits were noted with a lower rate of revision surgery and adjacent level degeneration when using additional posterior instrumentation. 32
We found that the two groups had a statistically similar and significant improvement in radiological parameters with an increase in mean disc height, intervertebral foramen height, sagittal disc angle, global lumbar lordosis, as well as a high fusion rate. Both groups demonstrated high fusion rates that were statistically similar (DLIF-PPSF: 90%, DLIF-FJF: 91.7%). DLIF-PPSF exhibited a slightly lower fusion rate. Hartensuer et al, 33 noted that pedicle screws provide the highest and most consistent stability across all planes of motion. Although our data did not reveal a statistically significant difference, the high fusion rate after DLIF-PFJF compared to DLIF-PPSF may be due to a combination of various factors (gender, age, BMD, smoking, body mass index, degree of physical activity, concomitant pathology, phosphorus-calcium metabolism, etc.). In addition, the presence and degree of muscle atrophy both before and after surgery may also influence the fusion rate and requires further research. DLIF with facet joint fixation in the lateral decubitus position resulted in reduced surgical time, duration of anesthesia and X-ray exposure time compared with DLIF with percutaneous pedicle screw fixation, which was done in a prone position. With intraoperative computed tomography or robotic navigation, percutaneous pedicle screw fixation in the lateral position is possible, which reduces surgical time and radiation hazards.34,35 Our results do not show the intra-operative “time lost” when repositioning the patient to a prone position for pedicle screw placement. Those who do this “single position” save this intra-operative time. Therefore, it is possible to overstate the significance of shorter operating and anesthesia times without taking into account the “time lost” when transferring the patient, which requires further study. Importantly, there was significantly less postoperative multifidus muscle atrophy after DLIF-PFJF compared to DLIF-PPSF. In our opinion, despite the fact that placement of the facet fixation involves muscle splitting, the technique is much less invasive compared to placing two pedicle screws and a rod on each side. This explains the lower muscle atrophy in the PFJF subgroup compared to PPSF. It is also possible that muscle atrophy is affected by a larger number of dorsal fixation elements in the PPSF subgroup (screws and rods) compared to PFJF. As to whether it is advisable to explant instrumentation once a solid fusion is attached, additional studies are needed to test such a hypothesis. However, it is our opinion that the added trauma to the muscles required to do so may potentially worsen, rather than improve muscle function. DLIF-FJF had better post-operative ODI and SF-36 scores and a higher return to work rate for heavy / very-heavy workload workers (P = .02). Considering the long-term minimal clinical difference between the subgroups in ODI scores of 8 (4;12) for DLIF-PPSF vs 6 (4;10) for DLIF-PFJF, as well as a P value close to statistically insignificant (P = .045), it is possible that in this case there is an initial imbalance between the preoperative ODI values, indicating a more pronounced baseline functional impairment in the DLIF-PPSF subgroup. The clinically minimal difference between the subgroups in the SF-36 PCS results (P = .044) revealed in the study potentially does not have true clinical significance and may be beyond the limits of statistical significance. Minor and major complication rates were comparable. Our clinical results are comparable to the literature on DLIF with facet joint fixation10,11 as well as with pedicle screw fixation.36,37
Iatrogenic paravertebral muscle damage has been shown to affect long-term clinical and radiological outcomes. Significant postoperative atrophy of paravertebral tissues is associated with poorer long-term clinical outcomes, 38 screw loosening, 39 adjacent-segment degeneration, 40 local and global malalignment, 41 pseudarthrosis 42 and reoperations. 43 Various techniques have been developed to reduce iatrogenic muscle damage after PLIF and TLIF, including bilateral percutaneous transpedicular stabilization, 44 unilateral pedicular fixation, 45 facet cage fixation,2,14 and minimally invasive pedicle fixation with cortical bone trajectory. 46
The Limitations and Strengths of the Study
The limitations of the study include: (1) retrospective nature of the data collection and the impossibility of blinding; (2) nonrandomized sample of examined patients without using an electronic patient data management system; (3) lack of analysis of results in the early and intermediate postoperative period; (4) unique, relatively homogeneous population of railway workers with risk, strenuous labor responsibilities; (5) the use of multicomponent structurally different implants; (6) the use of 1.5 T MRI and T2w imaging exclusively without additional software modules; (7) the use of percent change of muscle area as the sole factor in assessing muscle atrophy; (8) including only patients who were working preoperatively.
Our results cannot be extrapolated to what might happen with multi-level degenerative disease and other forms of the degenerative pathologies. The study cohort consisted of patients with specific workloads with all patients operated on by a single surgeon in one hospital, potentially limiting its external applicability. Therefore, the generalizability of the findings needs to be confirmed by others, as patients in different settings may have different outcomes. Given that a very specific population was studied, the results of this study may not be generalizable to the majority of patients who require DLIF surgery for DDD. Given the limited methodological framework of the study, the findings can not be considered definitive or prescriptive. Further research is needed to draw definitive conclusions.
Despite these limitations, the strengths of the study include its mean 45 month follow-up on a large population of patients with a single diagnosis, treated by a single team without numerous confounding variables.
Conclusion
Our results suggest that DLIF in combination with pedicle screw fixation or facet joint fixation are highly effective in improving clinical results in railway workers at a mean 45 month follow-up period. Both minimally invasive methods have comparable blood loss, hospital stay, complications, leg pain, SF-36 MCS and Macnab scores, and radiological outcomes, including mean disc height, intervertebral foramen height, sagittal disc angle, global lumbar lordosis and fusion rate. However, DLIF with percutaneous facet fixation using bilateral titanium wedge-shaped plate-cage in the lateral decubitus position had statistically significant advantages in surgery time, duration of anesthesia, X-ray time, back pain, and quality of life, compared to DLIF with bilateral percutaneous pedicle screw fixation. In addition, after DLIF with facet joint fixation, there was less atrophy of the multifidus muscle area compared to DLIF with pedicle screw fixation and higher return to work rate in heavy/very-heavy workload groups at last follow up period. Given the minimal difference found between the subgroups for ODI and SF-36 PCS results, further studies on a larger number of cases are needed to make a final determination on the clinical significance of these parameters.
Footnotes
Author Contributions
Each author made significant individual contributions to this manuscript. V.A.B. (0000-0003-4349-7101)*, A.A.K. (0000-0002-6059-4344)*, Y.Y.P. (0000-0001-7076-571X)* and K.D.R. (0000-0003-2083-9375)* were the main contributors to the drafting of the manuscript. V.A.B., A.A.K., Y.Y.P., M.A.A. (0000-0002-3190-2395)*, R.M.Y. (0009-0002-7165-5373)*, and Y.K.D. (0000-0002-5245-0797)* evaluated the data from the statistical analysis. V.A.B., A.A.K., Y.Y.P., M.A.A. and K.D.R. performed the literature search and review of the manuscript, and contributed to the intellectual concept of the study. *ORCID (Open Researcher and Contributor ID).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
The study was approved by the Ethics Committee of FSBEI HE “Irkutsk State Medical University” of the Ministry of Health of the Russian Federation - No. 1, dated February 14, 2023.