
Abstract
Study Design
Retrospective analysis was performed of a multi-center Canadian Spine Outcomes and Research Network (CSORN) surgical database.
Objective
To determine the rate and time to return to work (RTW) based on workload intensity after elective degenerative lumbar spine surgery.
Methods
Patients working pre-operatively, aged greater than 18, who underwent a primary one- or two-level elective lumbar spine surgery for degenerative conditions between January 2015 and October 2020 were evaluated. The percentage of patients who returned to work at 1 year and the time to RTW post-operatively were analyzed based on workload intensity.
Results
Of the 1290 patients included in the analysis, the overall rate of RTW was 82% at 1 year. Based on workload there was no significant difference in time to RTW after a fusion procedure, with median time to RTW being 10 weeks. For non-fusion procedure, the sedentary group had a statistically significantly quicker time to RTW than the light-moderate (P < .005) and heavy-very heavy (<.027) groups.
Conclusions
The rate of RTW ranged between 84% for patients with sedentary work to 77% for patient with a heavy-very heavy workload. Median time to resumption of work was about 10 weeks following a fusion regardless of work intensity. There was more variability following non-fusion surgeries such as laminectomy and discectomy reflecting the patient’s job demands.
Introduction
Return to work (RTW) after elective lumbar spine surgery is an important post-operative outcome. 1 Time off work due to lumbar spine pathology can have a significant financial impact for patients, their families and society. 2 In addition to the socioeconomic effect, time off work can impact one’s mental and physical well-being. 3 Return to work can help restore a sense of independence and purpose. The motivation and expectation to resume regular duties are goals that both patients and surgeons share.
There is variability in the literature on both the predictive factors and the recommendations for returning to work.4-6 Important predictive factors for RTW after lumbar surgery have been summarized in a systematic review and include preoperative work status, presence of comorbidities, age, sex, and duration of preoperative symptoms. 4 In addition to patient factors, work factors such as type of work including more strenuous and physically demanding jobs are related to prolonged time and lower rates of resuming work following elective lumbar spine surgery.1,4
The preoperative expectations set by the surgeon are related to the patients’ expectations for returning to work after low back surgery. 6 A surgeon must understand the patient’s ability and the expectations of workload intensity. 1 Assessing the fitness in the workplace is a difficult task for surgeons. There is a gap in the literature on recommendations to return to work based on workload intensity.
Despite correlation between workload intensity and delayed return to work, 6 there is a gap in the literature directly assessing the impact of workload on the rate and timing. Using the prospectively collected data from the Canadian Spine Outcomes and Research Network (CSORN), the primary objective of this study was to describe the impact of workload (sedentary, light-moderate and heavy-very heavy) on the rate and time to return to work after elective lumbar spine surgery (one- or two-level laminectomy, discectomy, and fusion). The secondary objective, assessed by a survey sent to the participating surgeons, was to determine how a patients’ workload requirement influenced the surgeons’ recommendations.
Methods
Study Design
A retrospective analysis of prospectively collected data from the multicentered Canadian Spine Outcomes and Research Network (CSORN) surgical registry was performed. This is a national registry that includes 60 neurosurgical and orthopedic spine surgeons from 18 academic and non-academic hospitals across Canada. All data is collected in a standardized fashion peri-operatively at pre-specified time points. Data was collected by trained research assistants and patient identification was kept anonymized. All sites have obtained Research Ethics Board approval for data collection. (IRB approval number H12-01627-A029). Informed consent was not required as per IRB for CSORN.
Eligibility
Inclusion criteria for this study were patients older than 18 years of age, who underwent one- or two-level primary elective lumbar spine surgery for degenerative conditions between January 2015 to October 2020. Patients underwent either a non-fusion procedure (discectomy and/or laminectomy) or a fusion (with or without a decompression) procedure. We included all patients who were actively working pre-operatively, and completed baseline work status information and reached 1-year post surgery. Exclusion criteria were age less than 18 years, patients who were not working at baseline, patients who did not complete baseline work status information, emergency surgeries, non-degenerative spine conditions (tumor, infection and trauma), cervical or thoracic pathologies, revision surgeries, patients treated non-operatively and patients who underwent greater than a 2-level lumbar spine surgery.
Patient and Surgical Data
Age, gender, comorbidities, marital status, living arrangement, education level, BMI, tobacco use, pain medication use, narcotic use, symptom duration, diagnosis, province of surgery, and active workers’ compensation claims were collected prospectively. Outcome measures were patient reported outcomes (numerical rating scale (NRS) for back and leg pain, the SF-12 physical (PCS) and mental component summary (MCS), the EuroQol 5D (EQ-5D) general health care score, the Patient Health Questionnaire-9 (PHQ9) and the Oswestry Disability Index (ODI)). Surgical information recorded included the type of surgery (non-fusion or fusion) and whether it was performed open or minimally invasively (MIS).
Workload Definition
Baseline workload was self-reported at baseline in the pre-operative patient questionnaire and was categorized as sedentary to very heavy based on lifting pattern as defined by the dictionary of Occupational Title (https://occupationalinfo.org). Sedentary work involves lifting no more than 10 pounds and occasionally lifting or carrying small tools. Light work is defined as lifting no more than 20 pounds at a time with frequent lifting or carrying of objects weighing up to 10 pounds. Medium work involves lifting no more than 50 pounds at a time with frequent lifting or carrying of objects weighing up to 25 pounds. Heavy work is defined as lifting no more than 100 pounds at a time with frequent lifting or carrying of objects weighing up to 50 pounds. Very heavy work involves lifting objects weighing more than 100 pounds at a time with frequent lifting or carrying of objects weighing 50 pounds or more. This study divided workloads into 3 categories: sedentary, light-moderate and heavy-very heavy.
Outcome Measures
The primary outcomes measures were the number of patients who returned to work at 1 year following their surgery and the number of days after surgery it took for patients to resume working. The date of the return to work was self-reported in the follow-up questionnaires. Specifics such as part-time vs full-time work and workplace restrictions were not captured.
Survey of Enrolling Surgeon Recommendations
Twenty questions were distributed to the 60 enrolling surgeons. They were asked to respond to 3 case studies (Supplemental Appendix 1) with respect to how they would counsel patients about delaying a return to work, based on the type of surgery and the job requirements. Workload was stratified as sedentary, light-moderate, and heavy-very heavy workload. The operations were one- or two-level lumbar discectomies, laminectomies, and fusions. Additional questions queried practice patterns (community vs academic), years into practice, surgical subspecialty and whether the procedure was open or vs MIS.
Statistical Analysis
Baseline patient characteristics and surgical characteristics were evaluated with descriptive statistics: t tests for continuous variables (means and standard deviations) and chi-square test for categorical variables (numbers and frequencies). Kaplan-Meier tests were used to assess differences in time across the various levels of workload intensity. An a priori level of 5% was used to determine statistical significance. Analyses were conducted using SPSS (IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp.)
Results
In total, 1484 patients met the inclusion criteria. Of these 194 patients were lost to follow-up before 1 year, leaving 1290 patients for the final analysis (Figure 1). The follow up in each workload group was over 80%. There were no statistically significant differences in baseline demographics between the study cohort and those lost to follow up for: sex, living status, symptom duration, active worker’s compensation claims, medication use, province of surgery, BMI and number of comorbidities. Those lost to follow up had significantly more patients who were smokers (P < .001), unmarried (P < .037), had less than a high school education (P<.006), had increased narcotic use (P < .028) and were of younger age (P < .007). (Supplemental Appendix 1) Patient flow diagram.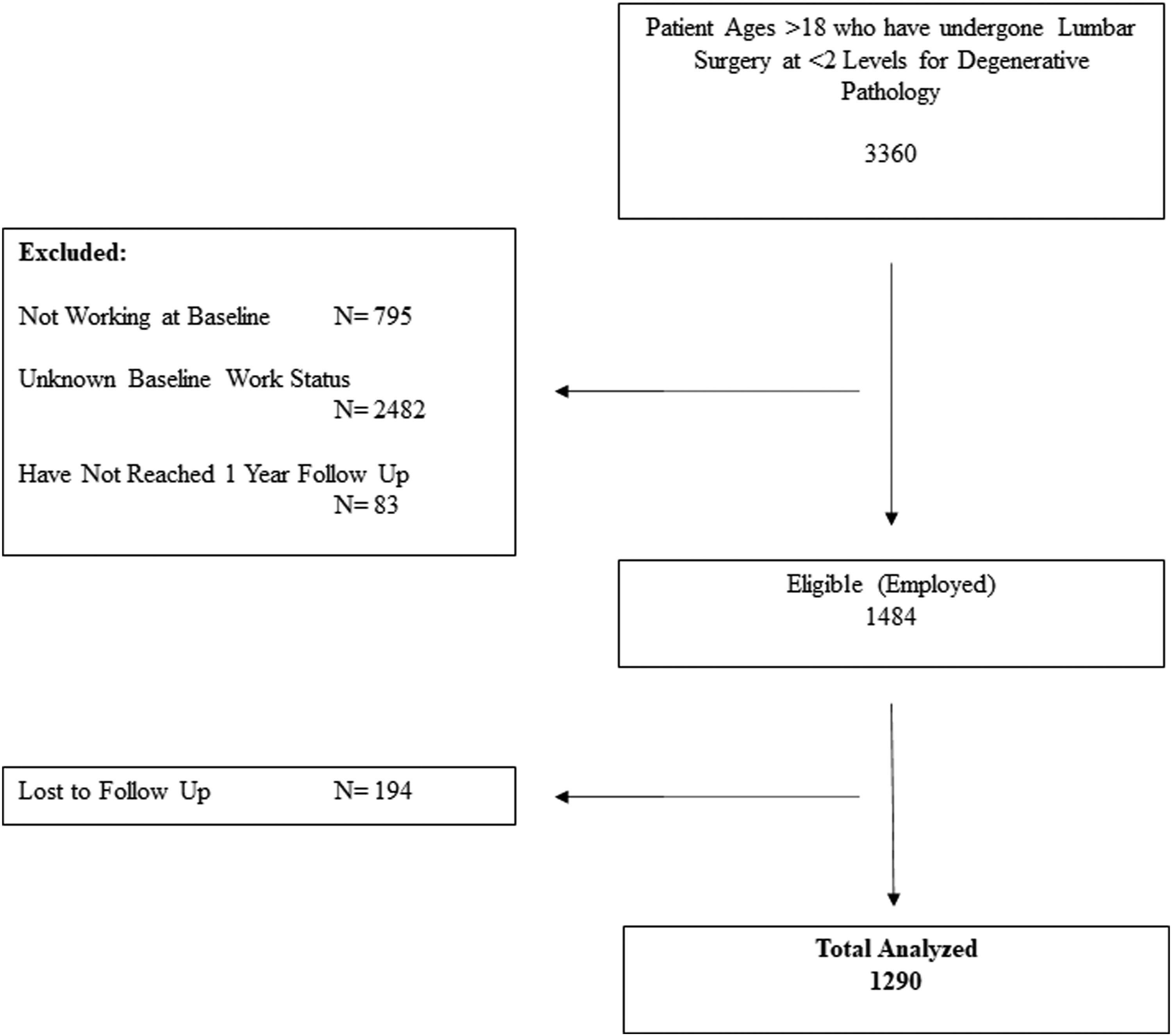
Study Population
Fifty seven percent of the cohort was male with a mean age of 50 (SD 12) years. The most common diagnosis was disc herniation (36%) followed by stenosis (27%) and spondylolisthesis (26%). Forty-two percent of the patients underwent a fusion procedure and 58% had a non-fusion procedure (18% laminectomy and 40% discectomy).
Comparison of baseline characteristics between Workload Groups.
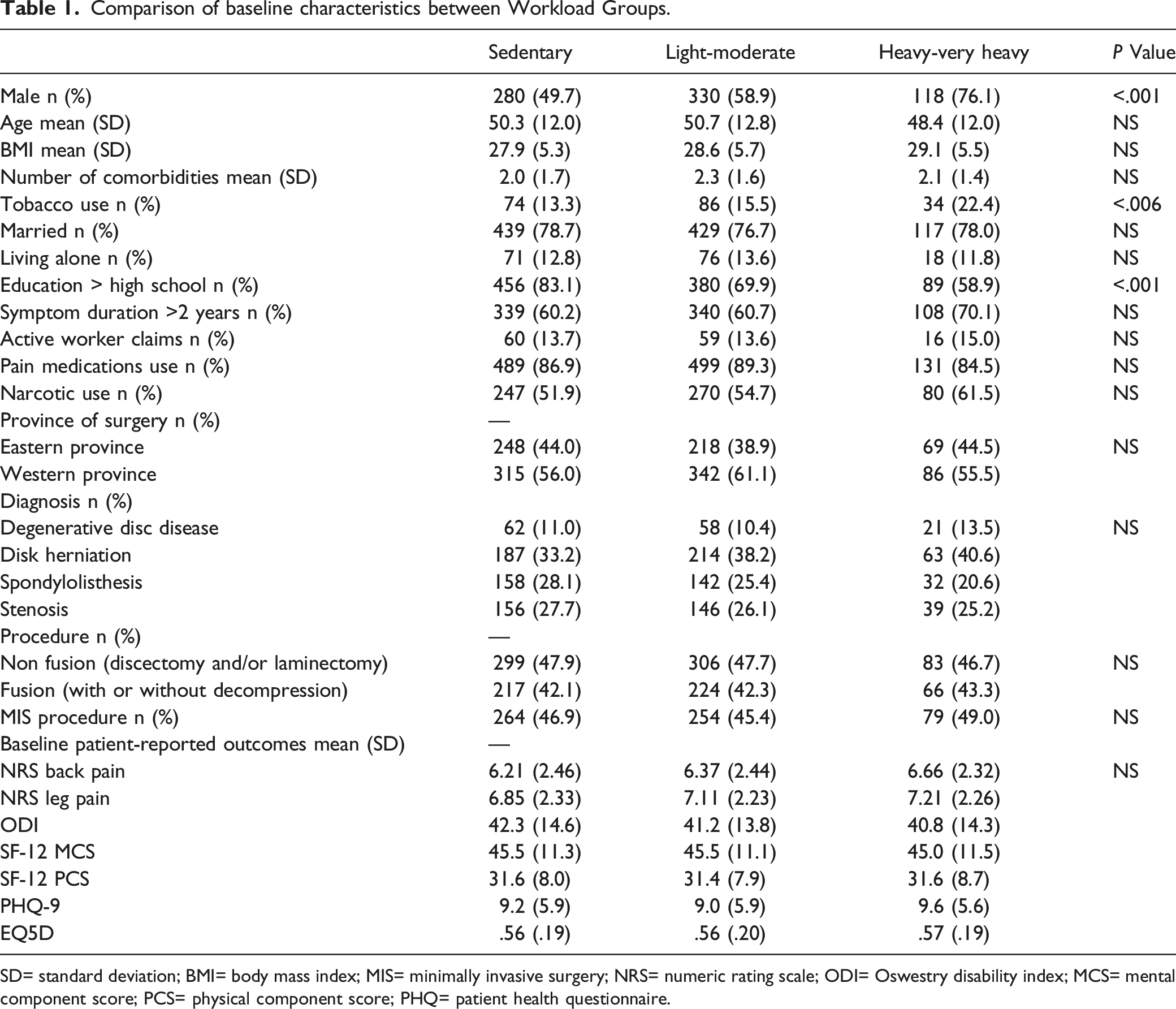
SD= standard deviation; BMI= body mass index; MIS= minimally invasive surgery; NRS= numeric rating scale; ODI= Oswestry disability index; MCS= mental component score; PCS= physical component score; PHQ= patient health questionnaire.
Return to Work Rate
RTW rate at 1 year stratified by workload and procedure.
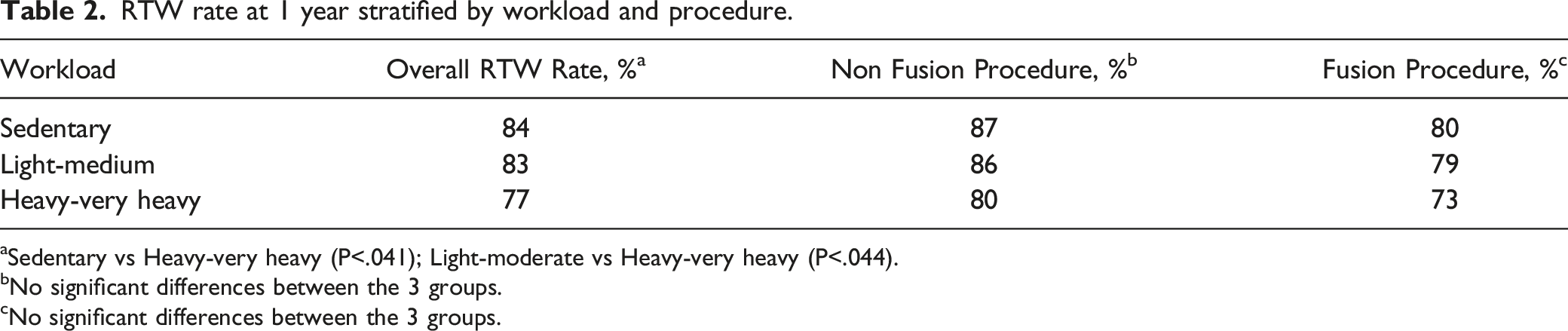
aSedentary vs Heavy-very heavy (P<.041); Light-moderate vs Heavy-very heavy (P<.044).
bNo significant differences between the 3 groups.
cNo significant differences between the 3 groups.
Comparing outcomes between patients who had fusions that those who did not, there was no statistical significance for the rate of return to work between the sedentary and light-moderate groups There was a statistically significant difference between the sedentary and heavy-very heavy workload groups (odds ratio =1.57, P < .041), as well as for the light-moderate and heavy-very heavy cohorts (odds ratio= 1.56, P < .044).
Time to Return to Work
For the entire group the median time to RTW was 56 [IQR = 68] days. By workload cohort, the median [IQR] time to RTW was 47 [70] (sedentary); 61 [74] (light-moderate); 73 [56] (heavy to very heavy). Kaplan-Meier log-rank testing revealed that the sedentary group had a statistically significantly quicker time to return to work than the light-moderate (P < .001) and the heavy-very heavy (P < .014) groups; there was no statistically significant difference between the light-moderate and heavy-very heavy groups. In the whole cohort, a fusion was associated with a significantly longer time to return to work than a non-fusion (median 77 days vs 48 days, P < .001). Figure 2 illustrates time to RTW stratified by workload and procedure. Time to return to work distribution stratified by workload. A) in the whole cohort B) following a fusion procedure C) following a non-fusion procedure.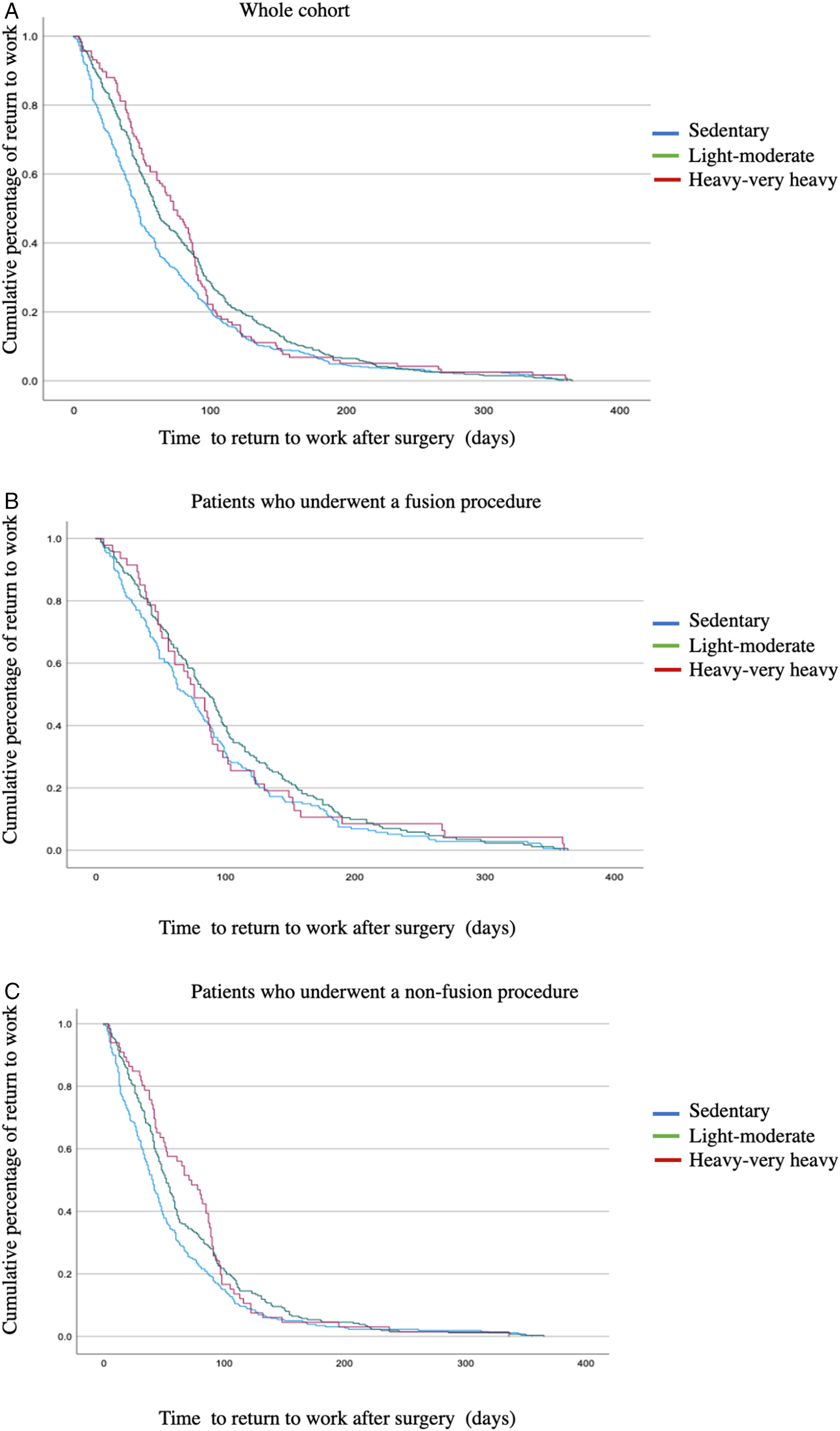
Median and mean time to RTW (in days) stratified by workload and procedure.

aSedentary vs Light-moderate (P < .005), Sedentary vs Heavy-very heavy (P < .027), Light-moderate vs Heavy-very heavy (P < .680)
bNo significant differences in time to RTW between the 3 groups.
Enrolling Surgeon Recommendations for Time to RTW
A questionnaire was sent to the participating surgeons and 52 surgeons, 86.7%, responded. There were 35 (67%) orthopedic and 17 (33%) neurosurgeons. Thirty-eight (73%) had an exclusively spine practice, while 10 (25%) identified spine surgery as constituting the majority of their practice. Years of experience varied between early (0-5 years) (23.5%) to mid (6-15 years) (50%) to late career (>16 years) (27.5%). Most surgeons, 50 (96%) practiced at an academic center.
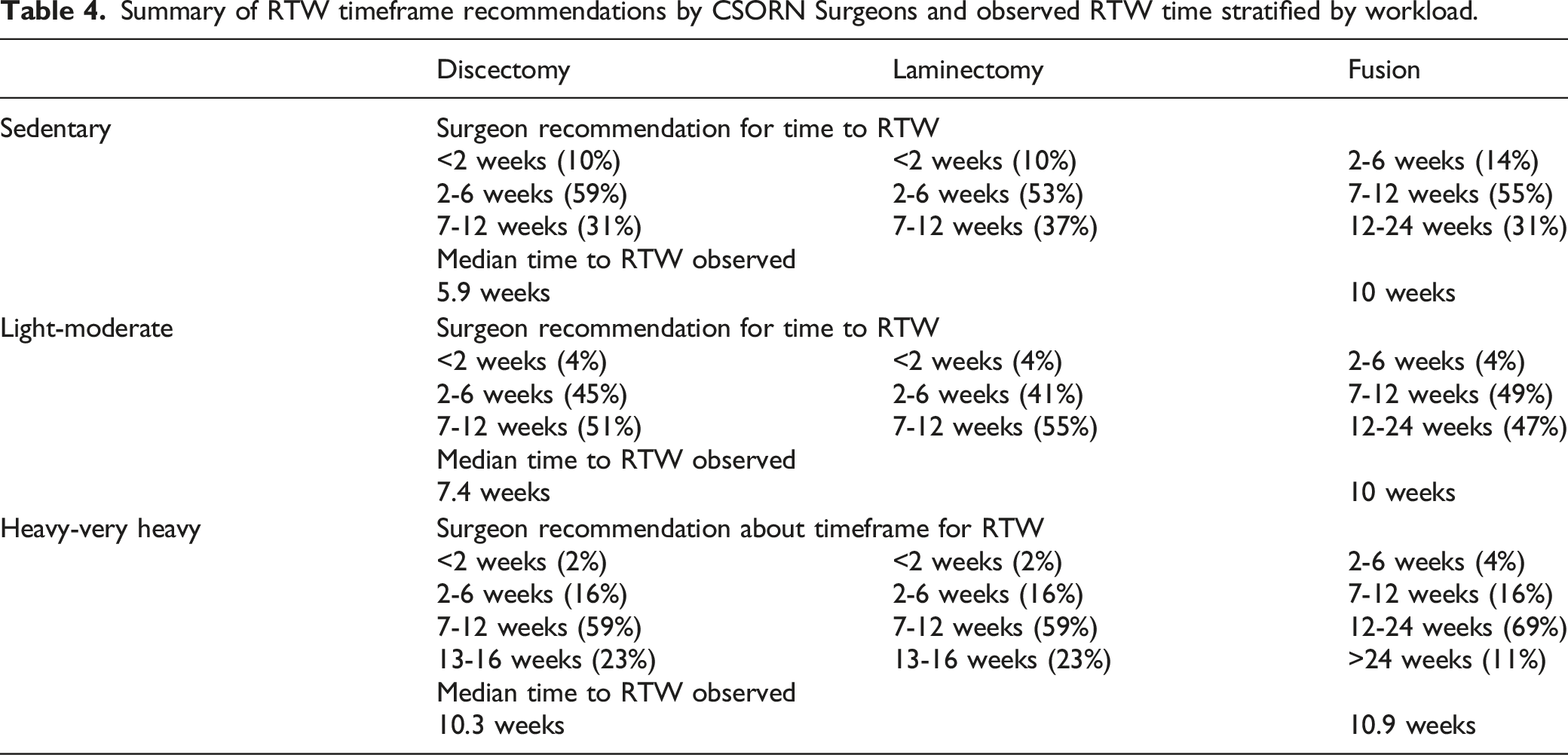
Summary of RTW timeframe recommendations by CSORN Surgeons and observed RTW time stratified by workload.
Discussion
To our knowledge, this is the first study to report the rate and the time to return to work based on workload intensity in patients who have undergone elective one- or two-level lumbar spine surgery. In patients who were actively working pre-operatively, the return was highest for the sedentary group and lowest for the heavy-very heavy workers; this cohort was least likely to resume employment (P < .05). Despite this, the rate of return to work remained high for all groups (84, 83 and 77%). Median time to return to work was between 70-97 days (10-14 weeks) following a fusion and did not vary significantly based on the anticipated workload. Following non-fusion spine surgery, patients with sedentary or light-moderate work resumed working faster than those with a heavy-very heavy jobs. On average this group remained off work nearly twice as long as sedentary workers.
A previous investigation by Toshiyui et al found following lumbar fusion that the difference in the rate of return to work between sedentary and heavy manual labour jobs was 48%. 7 In our study, we observed only a 7% difference. This may be the result of a difference in the patient populations; the Toshiyuki, et al. study focused on 21 patients with lumbar discogenic pain limiting generalizability of the study. In addition, our study only included patients who were pre-operatively working whereas 15 of the 21 patients included in Toshiyuki study were unable to work prior to the surgery. Although it is intuitive that the ability to return to work would be greater for less physically demanding jobs, this study suggests that despite having a strenuous occupation, the rate of success is still quite high in patients who were working prior to their surgery.
A study by Ziegler, et al. evaluating time to work 2 years after a 1 level lumbar discectomy showed a median time of 105 days (15 weeks) and a return rate of 62%. 8 This study showed that after one- or two-level lumbar discectomies the median time to start working was 41, 52 and 72 days for sedentary, light-moderate and heavy-very heavy workers, respectively. The difference may be that Ziegler included all patient whether they were employed or unemployed. Our previous work has shown that pre-operative work status is an important predictor of RTW. 9
There was a statistically significant difference between the speed with which sedentary workers returned to work and that of the other groups. Following non-fusion surgery, the difference between sedentary and heavy-very heavy-duty workers reached 30 days. The relationship between the intensity of the workload and the time to return to the job appears to be attenuated after a lumbar fusion. There was only a slight, non-statistical difference between the 3 groups.
There may be other factors contributing to the ability to return to work. The heavy-very heavy workers were more likely to be male, smokers and have less than a high school diploma education. Smoking status has been associated with a negative job return while higher education is associated with a positive outcome.4,10
Krause, et al. identified over 100 different determinants of RTW outcomes after injury or illness. 11 They list patient characteristics including sociodemographic factors, psychological factors, attitudes, beliefs, expectations and clinical measures of health and function. They enumerate characteristics of the injury/illness/surgery that affect the resumption of work, highlighting back pain and back injuries. They describe work characteristics that are barriers to returning to work including high physical and psychologically stressful jobs. These are 2 major factors in those seeking disability. 11 Heavy physical work prolonged the time to return to work and the duration of work disability.11-13
Spine surgeons adapt their recommendations for return to work based on the type of surgery and the demands of the workplace. Most surgeons surveyed in this study play a role in setting these expectations. For non-fusion surgeries, most surgeons suggested a return to work between 2-12 weeks, depending on the job demands (2-6 weeks for sedentary workers and 7-12 weeks for heavy-very heavy workers). For fusion surgeries, most surgeons recommended 7-12 weeks off work before returning to a sedentary to light-moderate workload job, and 12-24 weeks off work for a heavy-very heavy workload job. This study shows that the median time to return to work for fusion procedure regardless of workload was around 10 weeks. This suggests that surgeons may be advising longer time off work for this procedure than what we observed.
This study cannot determine whether the surgeon recommendations affected the actual time the patients required to start working again but the literature shows that patient-physician communication and physician recommendations influence return to work. 14 Positive reinforcement reduces short- and long-term disability status.11,15 This highlights the importance of surgeons’ setting appropriate and realistic expectations about RTW for patients undergoing lumbar spine surgery based on patient, surgical and work factors. Based on this study, surgeons can recommend that for a non-fusion procedure, an average return to work is reasonable within 6, 7.5 and 10 weeks for sedentary light-moderate workload and heavy-very heavy workloads workers, respectively. On the other hand, following a fusion procedure, most patients will return to work roughly 10 weeks after the surgery, regardless of their workload.
This study has several limitations. The CSORN database captures self-reported patient workload but the exact type of work performed by the patient is not reported and thus cannot be included in this study. The high rate of return to work reflects the selection bias: we included only patients who were working before surgery since this was the only group for which we could obtain the workload information needed to stratify the 3 cohorts. Our results may not be applicable to patients who were not working pre-operatively. This study examined the time and rate of return to work based on workload intensity. We recognize there are many other factors, including intrinsic and extrinsic motivation for working, job satisfaction, flexibility in the workplace for modified duties or hours and workplace environment, which can be considered. Return to work strategies such as gradual resumption of full activities or part time hours could not be collected and cannot be assessed. Financial incentives and socioeconomic status that may also play a role were not studied. Information on post-operative rehabilitation and overall post-operative management were not available so the effect of rehabilitation could not be included. Additionally, compliance and engagement of the patient toward such post-operative rehabilitation programs could not be determined.
Conclusion
Return to work following a one-or-two level elective lumbar spine surgery for degenerative conditions in patients who were working pre-operatively is usually successful. The rate of RTW ranged between 84% for patients with sedentary work to 77% for patient with a heavy-very heavy workload. Median time to resumption of work was about 10 weeks following a fusion regardless of work intensity. There was more variability following non-fusion surgeries such as laminectomy and discectomy reflecting the patient’s job demands.
Supplemental Material
Supplemental Material - Effects of Workload on Return to Work After Elective Lumbar Spine Surgery
Supplemental Material for Effects of Workload on Return to Work After Elective Lumbar Spine Surgery by Supriya Singh, Greg McIntosh, Nicolas Dea, Hamilton Hall, Jerome Paquet, Edward Abraham, Christopher S. Bailey, Michael H. Weber, Michael G. Johnson, Andrew Nataraj, R. Andrew Glennie, Najmedden Attabib, Adrienne Kelly, Y. Raja Rampersaud, Neil Manson, Philippe Phan, Maria Rachevitz, Ken Thomas, Charles Fisher, and Raphaële Charest-Morin in Global Spine Journal
Supplemental Material
Supplemental Material - Effects of Workload on Return to Work After Elective Lumbar Spine Surgery
Supplemental Material for Effects of Workload on Return to Work After Elective Lumbar Spine Surgery by Supriya Singh, Greg McIntosh, Nicolas Dea, Hamilton Hall, Jerome Paquet, Edward Abraham, Christopher S. Bailey, Michael H. Weber, Michael G. Johnson, Andrew Nataraj, R. Andrew Glennie, Najmedden Attabib, Adrienne Kelly, Y. Raja Rampersaud, Neil Manson, Philippe Phan, Maria Rachevitz, Ken Thomas, Charles Fisher, and Raphaële Charest-Morin in Global Spine Journal
Footnotes
Acknowledgments
The authors would like to thank all of the subjects who participated in the study, as well as the dedicated data collection and entry efforts of the support/research coordinator staff and investigators from the Canadian Spine Outcomes and Research Network (CSORN) contributing sites: Canada East Spine Centre: Saint John NB; Eastern Health: St John’s, NF; Foothills Medical Centre: Calgary AB; Hopital de L’enfant Jesus: Quebec City QC; Hopital General de Montreal: Montreal, QC; Hopital St Francois: Quebec City, QC; Ottawa Hospital: Ottawa, ON; Queen Elizabeth Health Sciences Centre: Halifax, NS; Sault Area Hospital: Sault Ste Marie, ON; St Michael’s Hospital: Toronto, ON; Sunnybrook Health Sciences Centre: Toronto, ON; Toronto Western Hospital: Toronto, ON; University of Alberta Hospital: Edmonton, AB; Vancouver General Hospital: Vancouver, BC; Vancouver Island Health Authority: Victoria, BC; Victoria Hospital - London Health Sciences Centre: London ON; Winnipeg Health Sciences Centre: Winnipeg, MB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.