
Abstract
Study Design
Systematic literature review.
Objectives
Posterior spinal fusion is the golden standard in the treatment of neuromuscular scoliosis. There are different views on whether pelvic fusion is necessary.
Methods
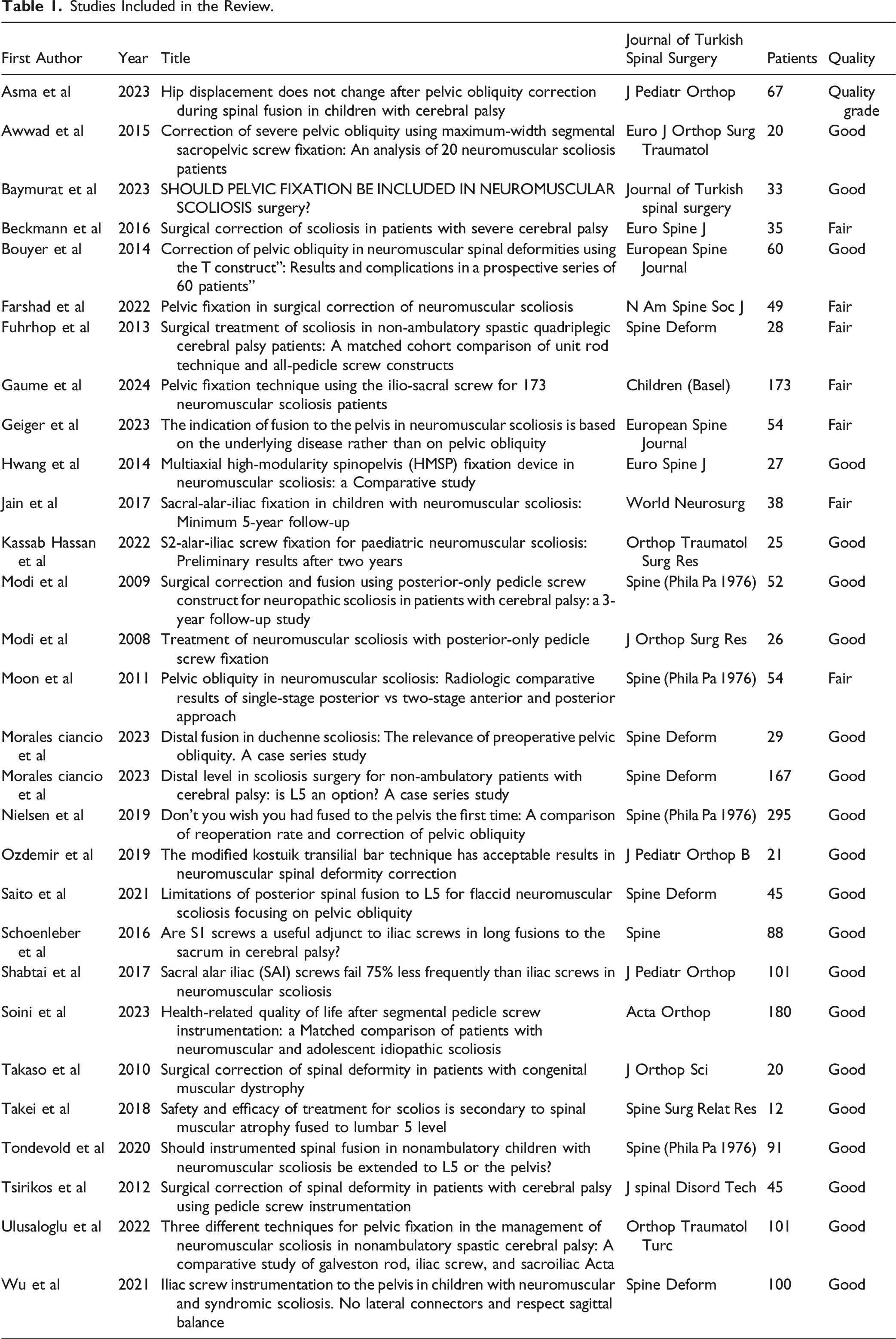
A systematic literature review according to PRISMA guidelines was performed. A total of 628 articles were screened. Original articles of neuromuscular scoliosis patients with reference to posterior spinal fusion in the population of ≤20 years of age were included. Operative technique with lumbar pedicle screws was required. Case reports, articles with missing data on pelvic parameters or with a postoperative follow-up of less than 2 years were excluded. A final of 29 original articles were included in the review.
Results
A total of 1611 patients undergoing posterior spinal fusion for neuromuscular scoliosis were included in the analysis with a mean age of 14.0 ± 1.0 years and a mean number of 15.5 ± 0.8 levels fused. Spinal fusion was extended to the pelvis in 1222 cases, while in 389 patients had fusion limited to the lumbar spine. The percentage of main curve correction was slightly higher in pelvic fusion patients 63 ± 10% compared to 58 ± 9% in lumbar fusion group, P < 0.001. Pelvic obliquity correction was superior in the pelvic fusion group, 58% compared to 42% in the spinal fusion group, P < 0.001. Operative time, complication rate and perioperative bleeding were greater in the pelvic fusion group.
Conclusions
Pelvic fusion in posterior spinal fusion for neuromuscular scoliosis results in small but statistically significant differences in curve correction and pelvic obliquity but increases the risk for perioperative bleeding and other complications. The impact on quality of life should be addressed in future research.
Background
In neuromuscular scoliosis (NMS), the abnormal curvature of the spine affects ambulation, sitting balance and posture, and can lead to back and costopelvic pain and severe respiratory, gastrointestinal, or skin problems.1-3 Progressive NMS often requires operative treatment, and once growth has ceased and sufficient spinal growth has been achieved, instrumented spinal fusion is the golden standard of the treatment. Scoliosis in NMS patients is often characterised by pelvic obliquity (PO), where the pelvic balance is compromised by the scoliosis and the contractures and weakness of hip muscles. 4 This can be addressed by extending the fusion to the pelvis. Indications for pelvic fusion are controversial, although pelvic obliquity >15° and Lonstein & Akbarnia type 2 NMS curves are the most commonly accepted indications.5,6
Most surgical techniques currently used for pelvic fusion involve iliac or sacral-alar-iliac (S2AI) screws. In previous publications, the benefits of these methods have been controversial. Pelvic instrumentation in neuromuscular scoliosis has been shown to improve radiological outcomes and subsequently facilitate patient management in non-ambulatory individuals. 7 Extension of fusion to the pelvis has not affected the walking ability in ambulatory NMS patients.8,9 However, a recent publication has reported an inferior health-related quality-of-life outcomes in patients with pelvic fusion compared those without pelvic fixation. 10 Mobility of the lumbosacral junction may facilitate transfers and weight shifts. 11 On the other hand, lumbar fusion alone can lead to progression in PO requiring revision surgery to extend the fusion to the pelvis. This has been shown to be associated with an increased risk of complications including a doubled reoperation rate (excluding the revision itself) and an increased risk of infection, implant failure, pseudarthrosis, and pain compared with initial pelvic fusion.12-14
Due to the lack of consensus on pelvic fusion, practice varies between centres. The literature suggests that non-ambulatory patients may benefit from pelvic fusion7,15-17 with improved main curvature and correction of pelvic obliquity (PO). 7 In ambulatory patients, pelvic fusion has only been indicated for more severe pelvic obliquity (>15°). 18
The aim of this study was to evaluate the clinical, radiological, and social impact of pelvic fixation in spinal fusion for NMS patients. The main interest was the role of pelvic fixation on walking ability in ambulatory patients, and the need for revision surgery and impact on pelvic obliquity in the non-ambulatory group. Secondarily we wanted to compare the outcomes of iliac vs S2AI screw techniques. We hypothesised that pelvic fixation would not have negative effect on ambulation, and an improving effect on correction of scoliosis, pelvic obliquity, and risk of revision surgery without an increased risk of perioperative complications.
Materials and Methods
A systematic literature review according to the PRISMA guidelines encompassing the published literature on the outcomes of short of pelvis vs pelvic fusion was performed.
19
PubMed, Embase, and Medline databases were searched using the terms “neuromuscular scoliosis” in combination with “spinal fusion” or “pelvic fixation” as keywords. All articles published before 12th of April 2024 were included in the review. After removing duplicates, the articles were screened based on the title and abstract. Original articles of neuromuscular scoliosis patients with reference to posterior spinal fusion in the population of ≤20 years of age were included. Non-English papers, studies on adult populations (>20 years of age), case reports (<3 patients), review articles, technical notes, expert opinions, articles on surgeries other than spinal fusion, articles on other types of scoliosis and other unrelated articles to the topic were excluded. After that a more detailed full-text review of the relevant articles was carried out, and articles were excluded if they lacked information on pre- and post-operative data on major curvature and pelvic obliquity, or if they had a follow-up of less than 24 months post-operatively. In addition, only studies in which pedicle screw instrumentation in the lumbar spine was performed were included. PRISMA flow chart diagram was created to illustrate the process (Figure 1). PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.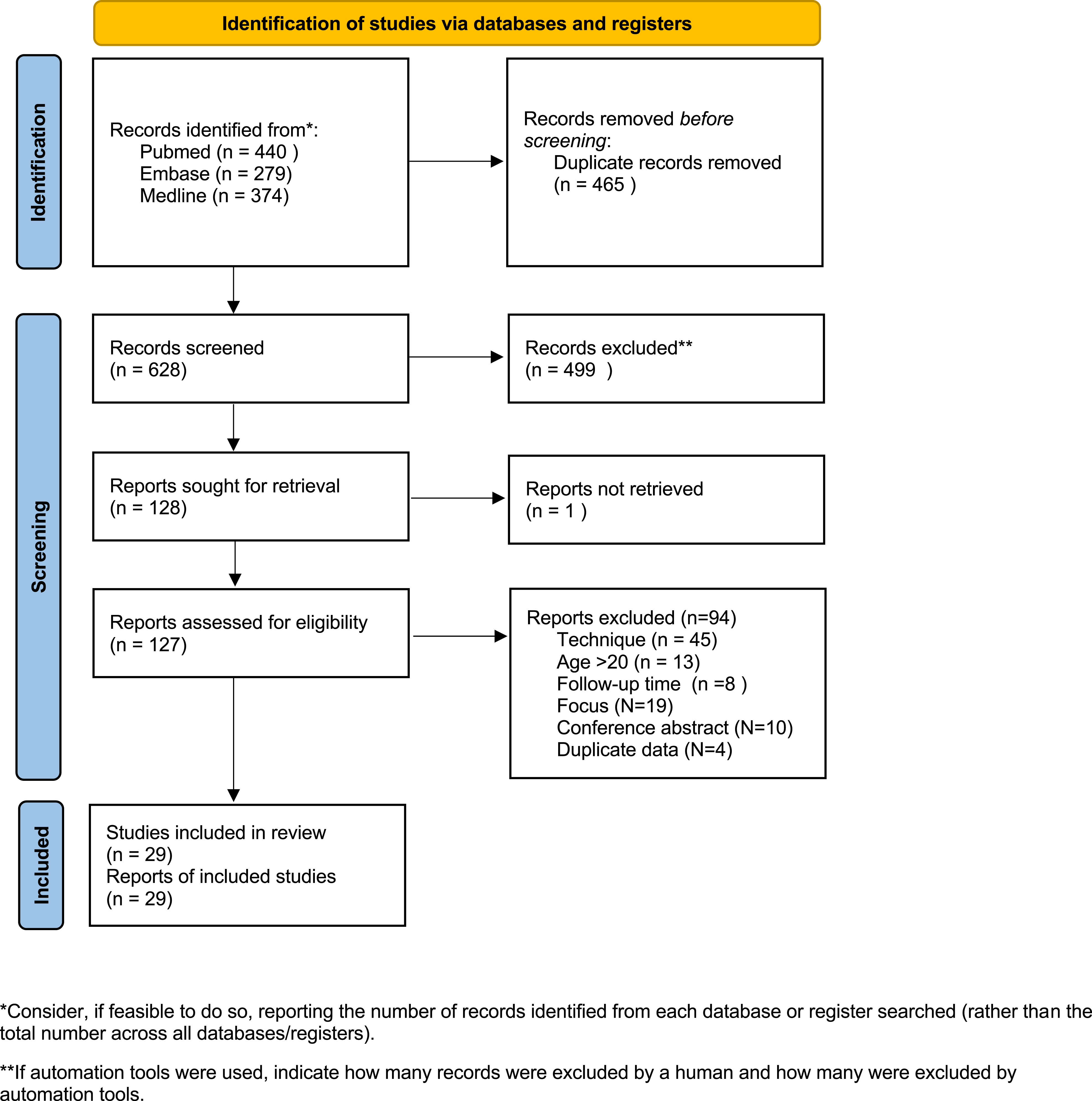
Studies Included in the Review.
Comprehensive data analysis was performed using Excel and JMP Pro 17.0.0. Data-analyses included subgroup analyses, considering pelvic fixation and different pelvic techniques (S2-Alar-Iliac and Iliac Screws). The normal distribution assumption was tested visually and statistically with the Shapiro-Wilkins test, and as the data were not normally distributed, non-parametric tests were used for the analysis of continuous data. Wilcoxon rank-sum test and Kruskal-Wallis test were used respectively.
The main outcome measures were postoperative major curve and pelvic obliquity angles. Secondary outcome measures included but were not limited to pre- and postoperative kyphosis and lordosis curve angles, ambulatory status and complications.
Results
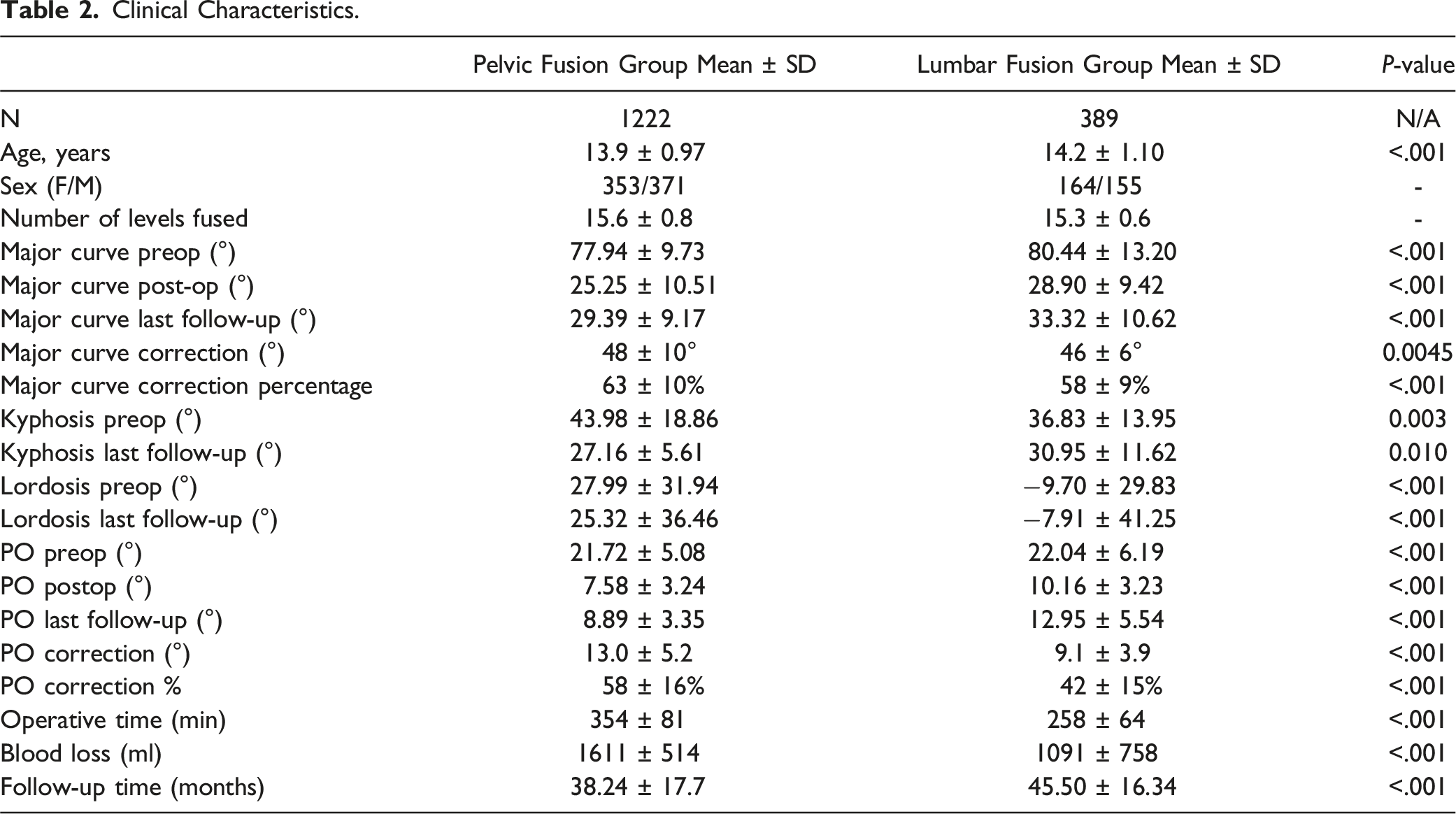
Clinical Characteristics.
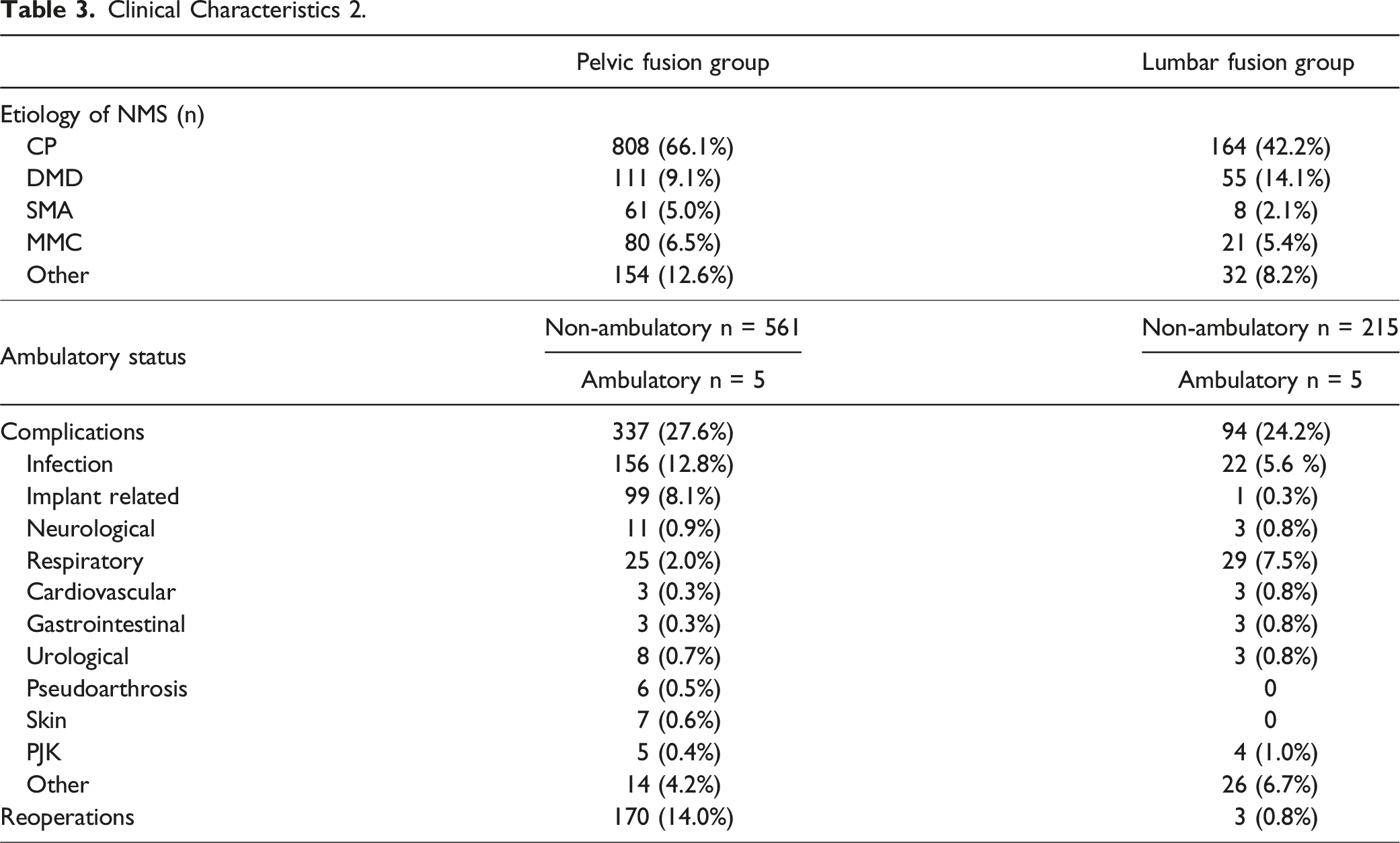
Clinical Characteristics 2.
The preoperative main curve angle was significantly smaller in pelvic fusion group, 77.9 ± 9.7, in comparison to 80.4 ± 13.2 in lumbar fusion, mean difference −2.5, 95% CI [-3.75 to −1.29], P < 0.001. Also, the postoperative main curve was significantly lower in the PF group than in the LF group at the last postoperative follow-up (29.3 ± 9.2 vs 33.3 ± 10.6, mean difference −4.9, 95% CI [-6.0 to −3.8], P < 0.001). Similarly, the percentage of main curve correction was significantly better in the PF group than in the LF group (63% vs 58%, score mean difference 4.9% [95% CI 3.7%–6.0%], P < 0.001). Concerning sagittal markers, preoperative lumbar lordosis and kyphosis angles were greater in the PF group. However, the change from preoperative to last follow-up kyphosis angle was similar between the groups. The deviation of lordosis values was vast and lordosis change was minimal between the groups. There was a minor difference in preoperative pelvic obliquity degree, 21.7 ± 5.1 in PF group in comparison to LF group, 22.0 ± 6.2 (mean difference −0.32, 95% CI [−0.92 – 0.29, P < 0.001]. Postoperative pelvic obliquity was significantly lower in the PF group, 8.9 ± 3.4 than in the LF group, 13.0 ± 5.5 (mean difference – 4.1, 95 % CI [−4.5 to −3.6], P < 0.001]). Correction of pelvic obliquity was significantly greater in the pelvic fusion group: 58% vs 42% (mean difference 16.0%, 95% CI [14.3%–17.9%] P < 0.001). The operative time was significantly longer in the PF group, 354 min compared to 258 min in the LF group, which was statistically significant (Mean difference 97 min, CI 95% [87-106], P < 0.001. There was also a major difference in the intraoperative blood loss between the groups, 1611 mL in PF and 1091 mL in LF groups (Mean difference 519 mL, CI 95% [435 – 603], P < 0.001. (Table 2).
Complications occurred in 28% of the pelvic fixation group and 24% of the spinal fusion group (RR 1.14, 95% CI [0.94-1.34]). The most common complications related to pelvic fusion were surgical site infection (12.8%, RR 2.26, 95% CI [1.82-2.69]) and implant related complications (8.1%, RR 31.5, 95% CI [29.5 – 33.5]), while in the lumbar fusion group the most common complications were respiratory complications (8.3%, RR 0.27 95% CI [0-0.80]) and surgical site infections (6.3%). Other complications, such as neurological complications including dural tear and neurological deficits, urological complications (urinary tract infection or haematuria), pseudoarthrosis, proximal junctional kyphosis and skin issues, were rare. Revision surgery was required in 14% of the cases in the pelvic fusion group and in 0.8% of the cases in the lumbar fusion group. (Table 3).
Pelvic obliquity was corrected with iliac screws in 42% of the pelvic fusion patients (N = 517) and the S2AI method was used in 8% of the cases (N = 101). In the remaining pelvic fusion cases, the methods could either not be divided into S2AI and iliac screw groups or were not reported. Major curve correction was statistically significantly improved by 66% in the iliac and 61% in the S2AI subgroups (Mean difference, 4.4%, 95 % CI [−6.6 to −2.1%], P < 0.0002). There was a clear difference in pelvic correction results between these two subgroups, pelvic obliquity correction angles of 15.1 ± 6.1 for iliac and 8.6 ± 4.7 for S2AI groups, (mean difference 6.0, 95% CI [−7.2 to −4.7], P < 0.001), correction percentages of 61% for iliac and 43% for S2AI methods, mean difference of 18%, 95% CI (−22 to −14.4%), P < 0.001. There was no difference in complications between the two methods.
The most common GMFCS scores were IV and V, but this was not reported individually in most reports. There was very limited data on previous GFSI implantation (no articles), blood transfusions (3 articles), hip status (no articles), and quality of life outcomes (4 articles).
Discussion
Based on the current systematic literature review, pelvic fixation in posterior spinal fusion for neuromuscular scoliosis patients results in slightly superior curve correction and pelvic obliquity compared to lower lumbar fusion only, but it increases operative time, complication rate, and intraoperative blood loss. Iliac screw method seems to be associated with better correction of pelvic obliquity correction compared to the S2AI method.
To the best of our knowledge, there are no recent systematic reviews that address the question of advances of pelvic fixation for posterior spinal fusion in patients with neuromuscular scoliosis. Ravindra et al observed the effectiveness of the S2AI screw technique in their systematic review. They suggested that this technique is effective for pelvic fusion in patients with neuromuscular scoliosis and has a reasonable safety profile. However, they did not address the question of whether or not to fuse the pelvis or show a comparison with other types of pelvic fusion. 48 Douleh et al. conducted a narrative review and found that pelvic fusion may result in better curve and PO correction but may increase the blood loss and operative time. However, their review did not include any data-analyses. 49 The results of the current review support these previous findings, and add to the literature by presenting statistical analyses and addressing the issue of complication rate. The fusion to pelvis group had more implant related complications (8%), some of which were loosened screws, in comparison to lumbar fusion group, in which only one patient (0,3%) had an implant related complication. However, this may also be partly explained by chance or limited reporting, as the pelvic fusion group was much larger than the other group.
The Harms Study Group compared the outcomes of lumbar vs pelvis fusion groups in CP associated neuromuscular scoliosis. 11 The most significant predictors of an unsatisfactory outcome included a pelvic obliquity ≥17° and dependent sitting status. The absence of both predictors conferred a 10% probability of unsatisfactory correction, compared with a 27% to 44% probability when 1 predictor was present and a 72% probability when both predictors were present. Patients with a satisfactory outcome reported better health-related quality of life (CPCHILD scores) in the lumbar fusion group than in the pelvic fusion group. Tondevold et al. observed better correction of both major curve and pelvic obliquity when instrumentation was extended to the pelvis in non-ambulatory children with neuromuscular scoliosis. 7 In contrast to this systematic review, there were no significant differences in the intraoperative blood loss and complications between the lumbar and the pelvic fusion groups.
Coronal and sagittal balance were variably reported in the reviewed papers. As an indicator of coronal balance we used the pelvic obliquity and found a clear difference between the groups, in favor to pelvic fusion. It must be considered that although the pelvic fixation method was associated with superior pelvic obliquity and curve correction, for an individual neuromuscular patient, a few degrees more correction, even with a statistically meaningful difference, may not be clinically relevant. As lumbosacral mobility provides functional advantages in transfers and ambulation, the benefits of the mobility may outweigh the risk of revision surgery. For clinical outcome and quality of life after fusion/no fusion to the pelvis, HRQoL would have been a meaningful outcome measure, but there were very few studies reporting this. Recent studies have shown improved quality of life in NMS patients after spinal fusion, but the reported HRQoL outcomes may be inferior when comparing patients with pelvic fusion to those without.10,50 Due to the limited data on HRQoL, we analysed secondary situational variables for clinical outcomes; risk of reoperation, ambulatory status, and pelvic and spinal parameters. Again, there was heterogeneity in the trials regarding risk of reoperation and walking status, which did not allow for reliable statistical analyses. Similarly, the preservation of walking ability could not be analysed, as almost all the patients in both study groups were non-ambulatory already before surgery; however, the ambulatory status remained unchanged for all patients after surgery. The literature on the influences of pelvic fixation on ambulatory status in NMS patients is limited but based on the current knowledge pelvic fixation does not affect the ambulatory status of the patients. 51 A more detailed comparison of different etiologies for neuromuscular scoliosis, i.e. cerebral palsy, would have been clinically useful. However, most of the reviewed papers did not provide subgroup data comparing the outcomes of underlying etiology for neuromuscular scoliosis.
Revision pelvic surgery after index lumbar fusion is associated with a high risk of complications. The neurological disease with medical comorbidities may also limit the additional procedures. 13 Matsumoto et al. found several risk factors associated with a higher risk of surgical site infection (SSI), with non-ambulatory status, neuromuscular etiology, pelvic instrumentation and operative time having the highest relative importance. 52 Many of these risk factors apply to the NMS patient population. Nielsen et al presented a study with almost twice as many reoperations after revision surgery and extension to the pelvis compared to those patients who received pelvic fusion at the time of the index surgery. 13 Revision pelvic fusion also has a similar operative time and blood loss compared to the index lumbar fusion. Due to the even higher risk of complications in this patient population in the revision surgery, it is necessary to consider the risks and benefits of pelvic fixation during the index surgery.
Ahonen et al. describe in their recent publication, that operative treatment of neuromuscular scoliosis reduces mortality in children with cerebral palsy. 53 Traditionally, NMS fusions in children with CP include pelvic fusion nationwide in Finland. Tsirikos et al state that the estimated survival time after NMS spinal fusion in children with CP averages 11 years, 9 but Ahonen et al describe significantly longer survival rates. 47 Revision surgery after spinal fusion is often challenging and carries a greater risk of complications. 13 For this reason, not all children can tolerate a revision, which argues in favor of pelvic fixation during the first operation. However, considering postoperative functional capacity and quality of life, pelvic fixation is not trouble-free. According to the literature, quality of life after lumbar fusion is superior in comparison to pelvic fusion. 10 This makes our inquiry relevant and topical.
We fully acknowledge that this review is inherently limited by the heterogeneity of the available literature. Not all studies reported complete data on several parameters such as ambulatory status, complications, and pelvic fixation techniques. In addition, most of the data were not normally distributed so non-parametric statistical analyses were performed. Our study protocol and review criteria were tight in order to address this specific issue. A strict 2-year follow-up period was chosen, as loss of correction during the first two postoperative years has been described previously. 7 This excluded many reports, in which the range of follow-up time was insufficient. In addition, a strict limitation in terms of instrumentation (instrumentation with lumbar pedicle screws) and patient age was also applied to reliably assess the outcomes of modern treatment methods for NMS surgery in the paediatric population.
Conclusions
With reference to the current literature, posterior spinal fusion in neuromuscular scoliosis patients extending to the pelvis appears to provide small improvements in radiological measures of curve correction and pelvic obliquity compared to fusion extending to the lumbar vertebrae only. The complication rate, operation time and perioperative bleeding also increase with extended surgery. However, the impact on quality of life, ambulation, and risk of revision surgery due to latter continuation of the fusion to the pelvis remains still unknown. Further research is needed to address these clinically important issues.
Footnotes
Author Contribution
VS has received personal research grants from Vappu Uuspään säätiö, Finnish Pediatric Research foundation and Turku University research funding. SK has received personal research grants from Vappu Uuspään säätiö, Finnish Cultural Foundation and the Finnish Research Foundation for Orthopaedics and Traumatology. SK has received personal travel grants from Stryker and DePuy Synthes. SK has served as a consultant for Stryker. AR reports research grants from Päivikki and Sakari Sohlberg Foundation. IH has received Finnish State Funding via Helsinki and Turku University Hospitals, grants from Päivikki and Sakari Sohlberg Foundation and Finnish Paediatric Research Foundation, Research Grants from Medtronic, Stryker, Nuvasive, and Globus to Institution. IH has served as a consultant for Medtronic, Stryker, and Globus. IH has received Research Grants from Medtronic, Stryker, Nuvasive, and Globus to Institution. IH has served as a consultant for Medtronic, Stryker, and Globus. SK has served as a consultant for Stryker.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.