
Abstract
Study Design:
Retrospective cohort.
Objective:
To provide a national-level assessment of the short-term outcomes after spinal deformity surgery in pediatric patients with cerebral palsy.
Methods:
A national, prospectively collected database was queried to identify pediatric (≤18 years) patients with cerebral palsy, who underwent spinal fusion surgery from 2012 to 2017. Separate multivariate analyses were performed for the primary outcomes of interest including extended length of stay (>75th percentile, >8 days), and readmissions within 90 days after the index admission.
Results:
A total of 2856 patients were reviewed. The mean age ± standard deviation was 12.8 ± 2.9 years, and 49.4% of patients were female. The majority of patients underwent a posterior spinal fusion (97.0%) involving ≥8 levels (79.9%) at a teaching hospital (96.6%). Top medical complications (24.5%) included acute respiratory failure requiring mechanical ventilation (11.4%), paralytic ileus (8.2%), and urinary tract infections (4.6%). Top surgical complications (40.7%) included blood transfusion (35.6%), wound complication (4.9%), and mechanical complication (2.7%). The hospital cost for patients with a length of hospital stay >8 days ($113 669) was nearly double than that of those with a shorter length of stay ($68 411). The 90-day readmission rate was 17.6% (mean days to readmission: 30.2). The most common reason for readmission included wound dehiscence (21.1%), surgical site infection (19.1%), other infection (18.9%), dehydration (16.9%), feeding issues (14.5%), and acute respiratory failure (13.1%). Notable independent predictors for 90-day readmissions included preexisting pulmonary disease (odds ratio [OR] 1.5), obesity (OR 3.4), cachexia (OR 27), nonteaching hospital (OR 3.5), inpatient return to operating room (OR 1.9), and length of stay >8 days (OR 1.5).
Conclusions:
Efforts focused on optimizing the perioperative pulmonary, hematological, and nutritional status as well as reducing wound complications appear to be the most important for improving clinical outcomes.
Keywords
Introduction
A common manifestation of cerebral palsy is spinal deformity, which is known to be strongly associated with worse gross motor function (higher GMFCS [Gross Motor Function Classification System] levels) and can become quite severe as it is known to progress beyond skeletal maturity.1-3 Generally, spinal fusion in pediatric patients with cerebral palsy is considered when the curvature of the spine impairs sitting ability, bracing is intolerable or inadequately improves sitting posture, the magnitude of the deformity continues to progress despite conservative measures, and medical issues (eg, cardiopulmonary dysfunction, gastrointestinal issues, pain) attributed to the spine deformity become more apparent. 4 In comparison to idiopathic scoliosis, the treatment of spinal deformity in cerebral palsy is considerably more complex since spinal curves are often larger and more rigid, bone quality is poorer, and medical comorbidities are numerous and significant.2,5-8 Therefore, it is not surprising that complications are common in this high-risk population.
Prior literature suggests that the overall complication rate after spinal fusion in cerebral palsy patients is high, but variable (range: 17% to 80%).9-17 According to a meta-analysis on neuromuscular scoliosis surgery, the top complications include pulmonary issues (22.7%), implant failure (12.5%), and infections (10.9%). 16 The reported complication rates vary significantly in literature due to differences in follow-up periods (range = 2-14 years), the inclusion of cerebral palsy as a subgroup within neuromuscular scoliosis, single institutional analyses, and discrepancies in the definition of complications. Although a plethora of literature has been published on the surgical management of neuromuscular scoliosis, few have reported on strategies and potential modifiable risk factors to reduce adverse outcomes at a national level.
In comparison to prior literature, we use a multicenter registry to investigate both the inpatient and postdischarge outcomes up to 90 days after spinal fusion in pediatric patients with cerebral palsy. Specifically, we determine the incidence and risk factors associated with complications, extended hospital length of stay, and unplanned readmissions. We hypothesize that complication rates will be high but associated with potentially modifiable factors. To our knowledge, this is the first and largest study to provide national-level estimates of clinical outcomes, readmissions, and total hospital cost in this population.
Materials and Methods
Data Source
The Nationwide Readmission Database was developed for the Healthcare Cost and Utilization Project (HCUP) and includes prospectively collected data from 28 geographically dispersed States, accounting for 60% of the total US resident population. Discharge weights can be applied to each patient encounter to allow for the calculation of national estimates, such as those for total hospital charges and costs, and complication rates. In comparison to other publicly available databases, this registry is structured to allow for tracking of an individual’s hospital admission across different institutions and state lines within a given year. Therefore, readmissions up to 90 days after the index admission discharge date can be reliably reported using this database. Several perioperative factors such as patient demographics, comorbidities, insurance type, and hospital-level factors are included. The perioperative factors that were not predefined in this database were coded using the International Statistical Classification of Diseases 9th revision (ICD-9) and 10th revision (ICD-10) diagnosis and procedure codes. The publicly available HCUP tools and software facilitated the mapping of these variables as shown in the appendix. 18 This database contains de-identified patient information and was deemed exempt by the institutional review board.
Patient Population
The 2012 to 2017 Nationwide Readmission Database was queried for all pediatric (≤18 years) patients with cerebral palsy, who underwent spinal fusion surgery. The specific diagnosis and procedure codes used to define cerebral palsy and spinal fusion surgery can be found in the appendix. The ICD-9 codes used to define this population are consistent with prior literature.19,20 Of note, ICD-10 codes were used in 2016 and 2017. HCUP tools and software were used to map these codes appropriately. Exclusion criteria included nonelective index admissions, missing data, and 4th quarter index admissions to account for possible 90-day readmissions (Figure 1).
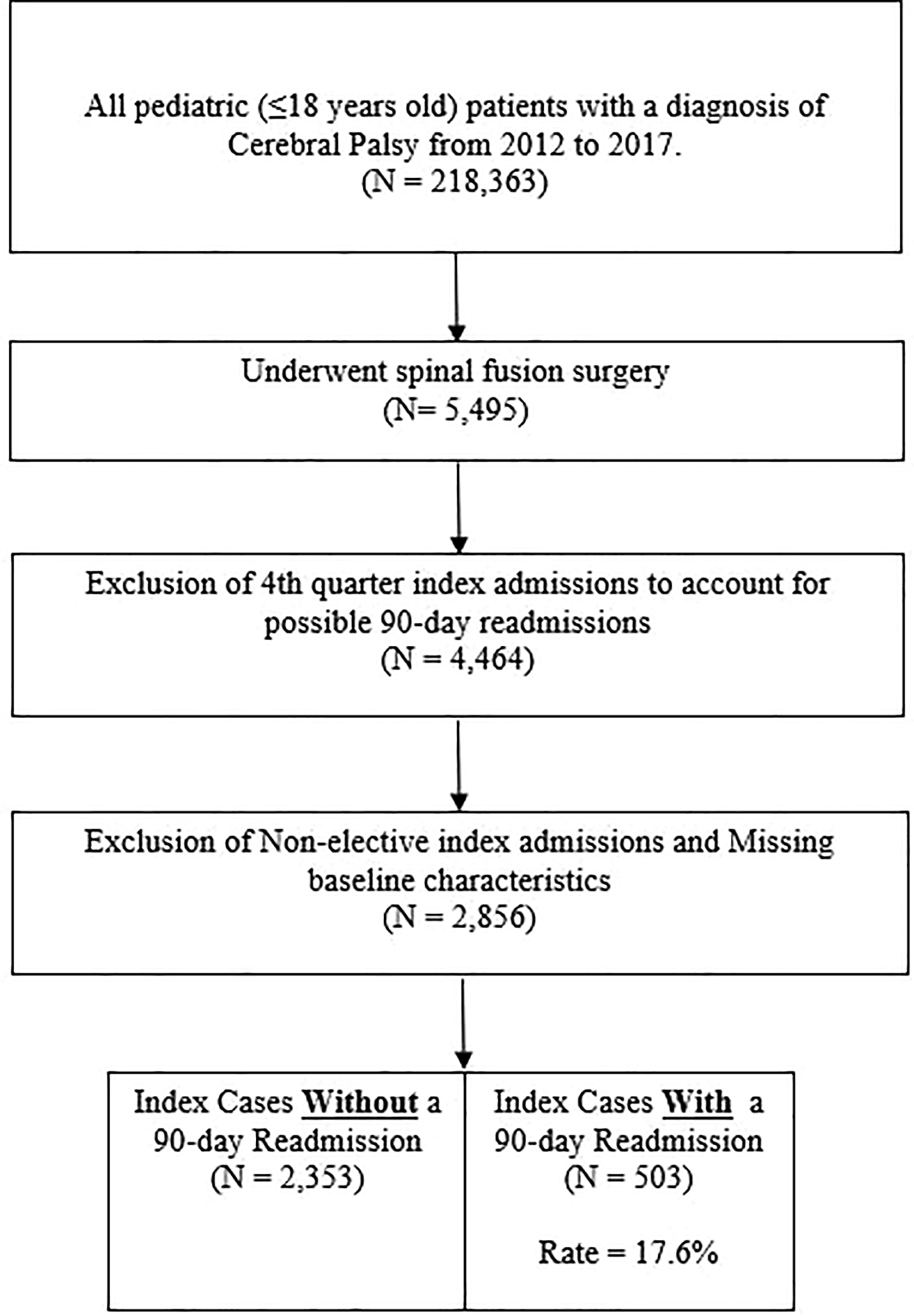
Selection criteria of the study’s patient population.
Perioperative Factors
Patient data included age, gender, insurance type, and income quartile. A comprehensive set of comorbidities was included as listed in Table 1 with corresponding ICD-9/-10 codes in the appendix. Surgical factors included surgical approach (posterior-only, anterior-only, and combined anterior-posterior) and fusion levels. There is a discrepancy in the coding for levels fused between ICD-9 and ICD-10 codes. Therefore, we defined “long-segment fusion” as >8 levels fused for years 2012 to 2015 and ≥8 levels fused for years 2016 to 2017. Hospital factors included hospital teaching status (metropolitan nonteaching, metropolitan teaching, and nonmetropolitan), hospital ownership (private nonprofit, private for-profit, government), and discharge disposition (routine/home, home with health care services, transfer to other than home).
Patient, Surgical, and Hospital Factors (2012-2017).
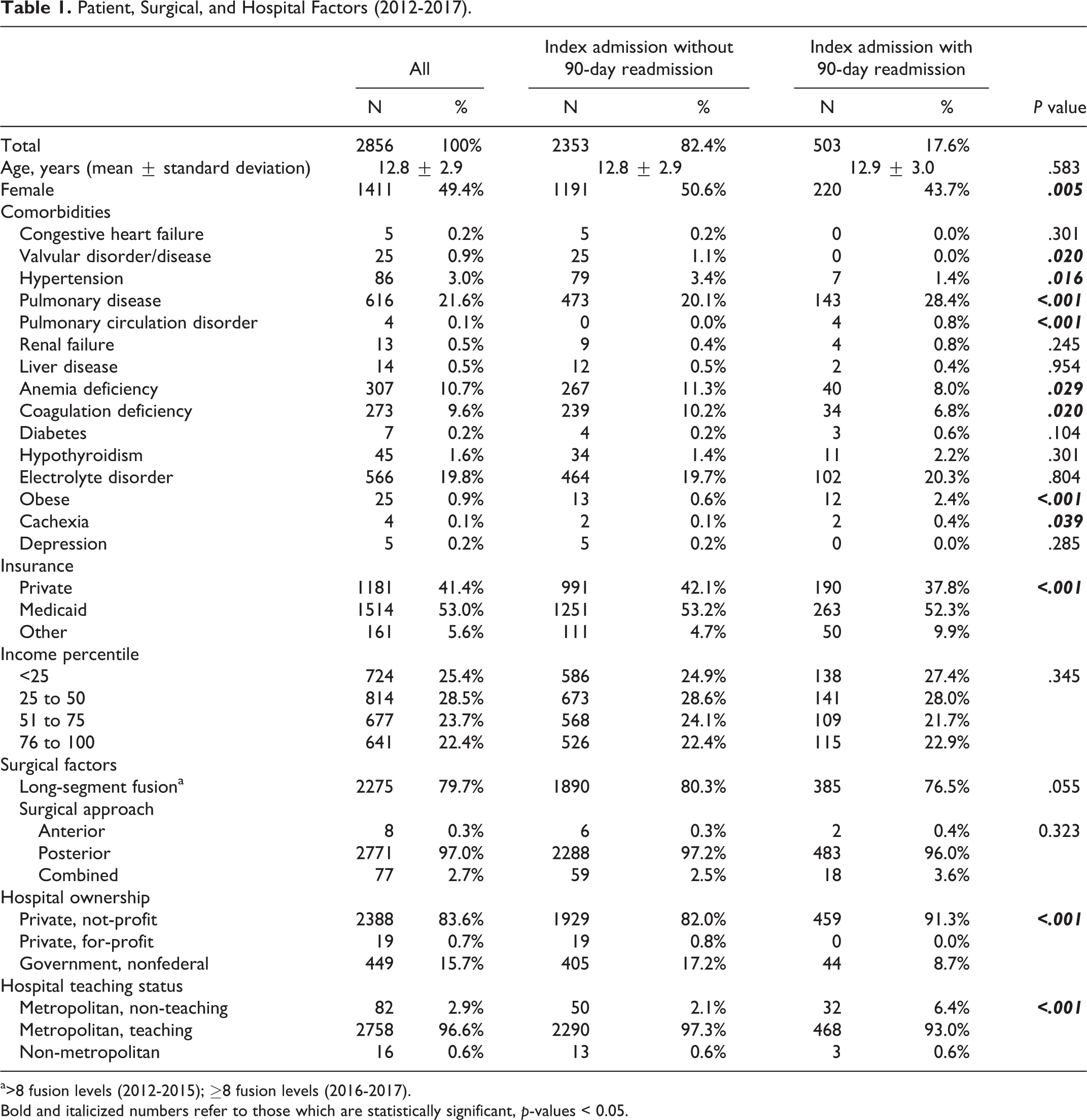
a>8 fusion levels (2012-2015); ≥8 fusion levels (2016-2017).
Bold and italicized numbers refer to those which are statistically significant, p-values < 0.05.
Outcomes of Interest
The primary outcomes of interest included index admission inpatient complications (medical and surgical), extended length of hospital stay (LOS >75th percentile: >8 days), and 90-day readmissions. A 90-day readmission was defined as any readmission within 90 days after the index admission discharge date. The reasons for 90-day readmissions were assessed by reviewing the primary and secondary diagnoses of each subsequent admission.
Statistical Analysis
Bivariate analyses were performed on perioperative factors for each outcome of interest. Chi-square or Fisher’s exact test (where appropriate) and t tests/ANOVA were used for categorical and continuous variables, respectively. Separate multivariate analyses were performed for inpatient medical complications, inpatient surgical complications, extended length of hospital stay, and 90-day readmissions. The multivariate analyses involved stepwise logistic regressions. The C-statistic was used to measure the goodness of fit for these logistic regressions. Statistical significance was defined as a P value <.05. SAS software (Version 9.3; SAS Institute Inc) was used for statistical analyses.
Results
In the United States, a total of 218 363 pediatric patients had a diagnosis of cerebral palsy from 2012 to 2017. About 2.5% (N = 5495) of these patients underwent spinal fusion surgery. After exclusion criteria, a total of 2856 patients remained (Figure 1). The mean age ± standard deviation of the final population was 12.8 ± 2.9 years, and 49.4% (N = 1411) of patients were female. The most common comorbidities included pulmonary disease (21.6%, N = 616), electrolyte disorder (19.8%, N = 566), anemia deficiency (10.7%, N = 307), and coagulation deficiency (9.6%, N = 273). The majority of patients underwent a posterior spinal fusion (97.0%, N = 2771) and long-segment fusion (79.9%, N = 2275) at a nonprofit (83.6%, N = 2,388), teaching hospital (96.6%, N = 2758; Table 1).
The inpatient morbidity and mortality of the index admission were 53.5% (N = 1528) and 0.2% (N = 5), respectively. Top medical complications (24.5%, N = 699) included acute respiratory failure requiring mechanical ventilation (11.4%, N = 326), paralytic ileus (8.2%, N = 233), other respiratory issue (6.2%, N = 176), and urinary tract infections (4.6%, N = 130). Top surgical complications (40.7%, N = 1162) included blood transfusion (35.6%, N = 11 017), wound complication (4.9%, N = 140), and mechanical complication (2.7%, N = 77). About 4% (N = 109) of patients required a return to the operating room during the same index admission for either wound drainage/debridement (1.5%, N = 42) or removal of implants (2.3%, N = 67). The majority of patients were discharged home (92.1%, N = 2630). The mean LOS and total hospital costs for the index admission were 7.7 ± 7.6 days and $78 828 ± 59 414 (Table 2).
Inpatient Complications, Disposition, and Cost for Index Admissions.
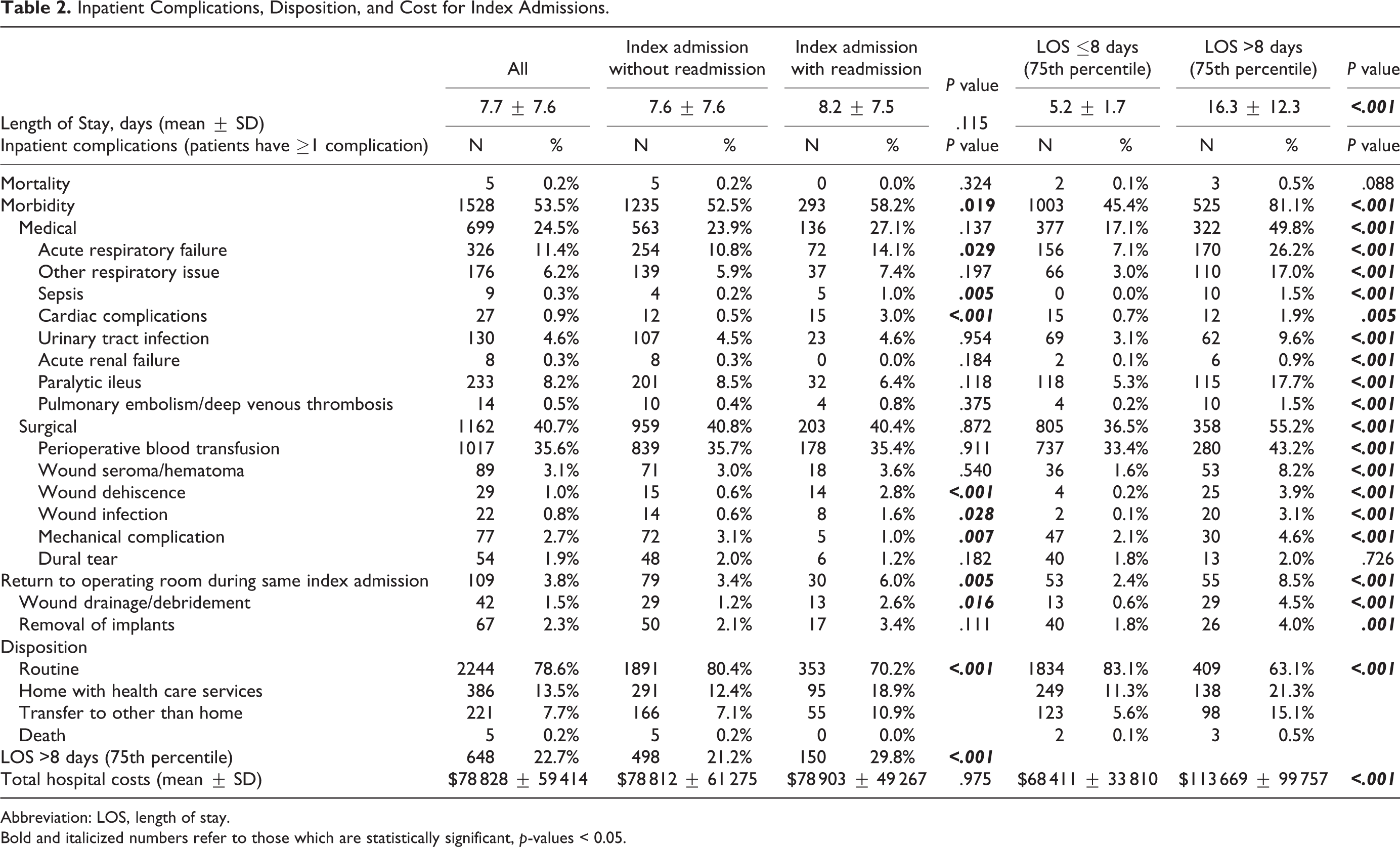
Abbreviation: LOS, length of stay.
Bold and italicized numbers refer to those which are statistically significant, p-values < 0.05.
The mean LOS for those requiring more than 8 days was 16.3 ± 12.3 days versus those with ≤8 days (5.2 ± 1.7 days). The total hospital cost for patients with a prolonged LOS ($113 669 ± 99 757) was nearly double than that of those with a shorter length of stay ($68 411 ± 33 810; Table 2). Significant predictors for extended LOS included preexisting pulmonary disease (odds ratio [OR] 1.9), anemia deficiency (OR 2), coagulation deficiency (OR 1.8), electrolyte imbalance (OR 2.1), lowest income quartile (OR 2.6), discharge to other than home (OR 5.5), inpatient medical complications (OR 3.8), inpatient surgical complications (OR 1.8), and inpatient return to operating room (OR 4). The risk factors for inpatient medical complications of the index admission included female (OR 1.3), pulmonary disease (OR 1.7), anemia deficiency (OR 2.3), electrolyte imbalance (OR 1.8), Medicaid insurance (OR 1.1, reference: private insurance), and long-segment fusion (OR 1.5). Predictors for inpatient surgical complications of the index admission included older age (OR 1.1), pulmonary disease (OR 1.3), anemia deficiency (OR1.9), electrolyte imbalance (OR 1.5), and Medicaid insurance (OR 1.3; Table 3). Comorbidities, which were not significant for any multivariate regression, were not included in Table 3.
Independent Risk Factors for Selected Outcomes Based on Stepwise Multivariate Logistic Regressions.
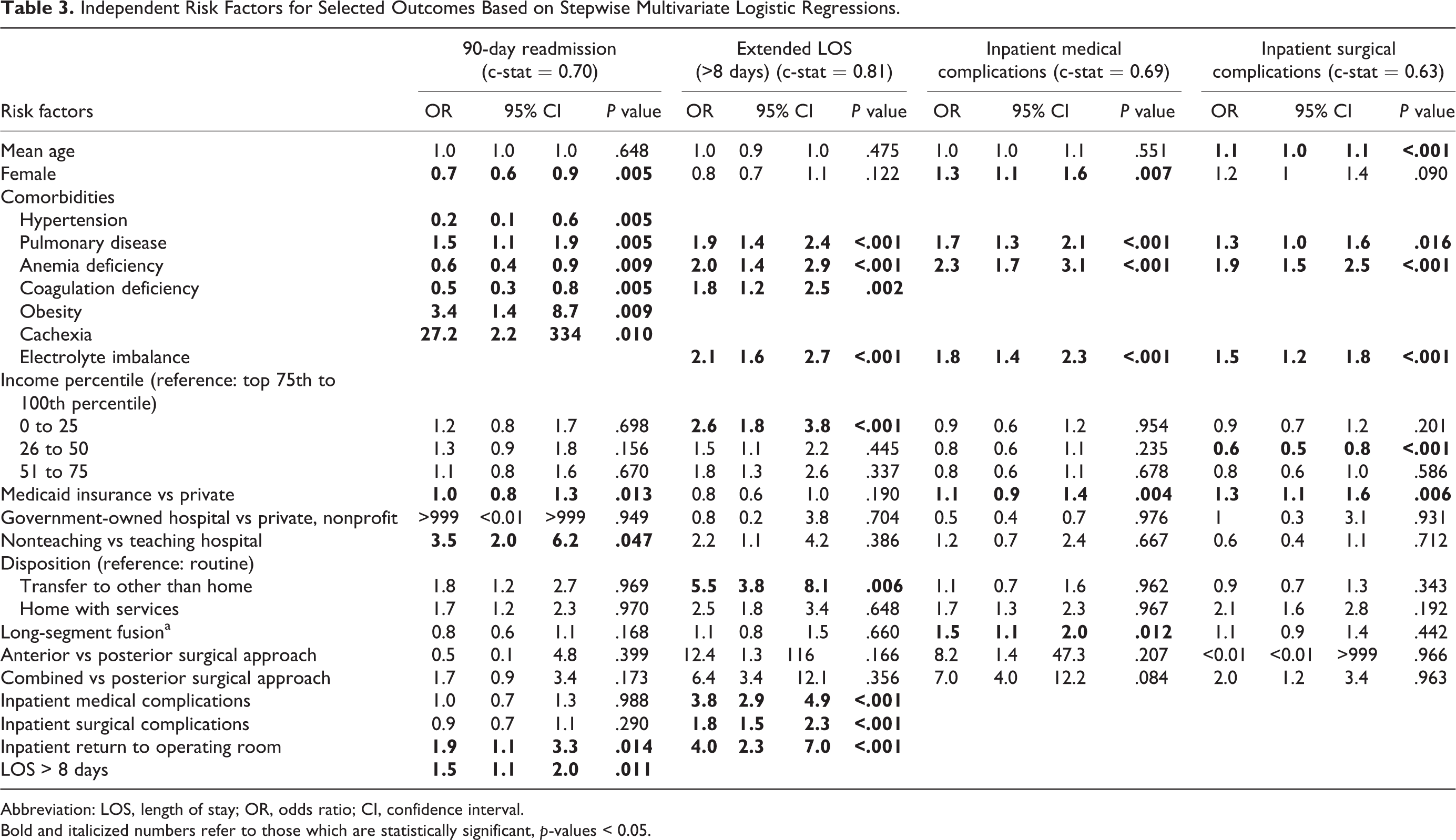
Abbreviation: LOS, length of stay; OR, odds ratio; CI, confidence interval.
Bold and italicized numbers refer to those which are statistically significant, p-values < 0.05.
The 90-day readmission rate was 17.6% (N = 503; mean days to readmission: 30.2 ± 22.7). The total hospital costs for the index admission did not differ significantly between those who required a readmission versus not (P = .975). However, the mean total hospital cost of a readmission was $19 658 ± 23 384. Readmissions which involved a return to the operating room were associated with significantly higher readmission costs ($34 229 ± 22 771) than those who did not ($16 781 ± 22 444, P < .001). The most common reason for readmission included wound dehiscence (21.1%, N = 106), surgical site infection (19.1%, N = 96), other infection (18.9%, N = 95), dehydration (16.9%, N = 85), feeding issues (14.5%, N = 73), and acute respiratory failure (13.1%, N = 66). Other infection included pneumonia (6.4%, N = 32), sepsis (7.2%, N = 36), and urinary tract infection (5.4%, N = 27). Of those readmitted, 14.1% (N = 71) required a wound debridement and 5.8% (N = 29) required the removal of implants (Table 4). Notable independent predictors for 90-day readmissions included preexisting pulmonary disease (OR 1.5), obesity (OR 3.4), cachexia (OR 27), nonteaching hospital (OR 3.5), inpatient return to operating room (OR 1.9), and LO S>8 days (OR 1.5; Table 3).
Reasons for Readmissions and Reoperations Within 90 Days of Index Hospital Stay.
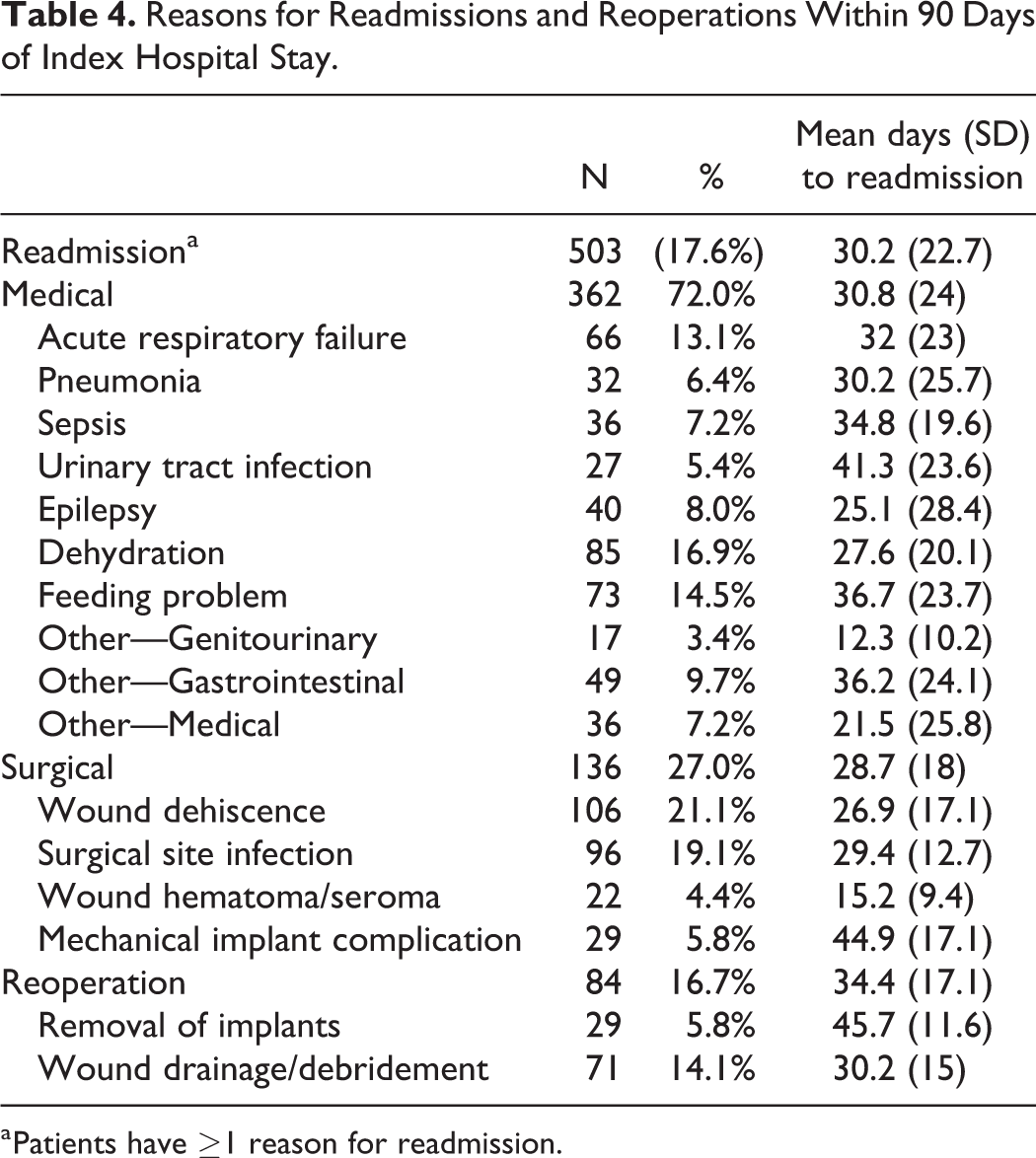
a Patients have ≥1 reason for readmission.
Discussion
The decision to undergo spine surgery can be daunting for the patient, caregiver, and surgeon as most patients with cerebral palsy have complex medical issues that increase the risk for surgery. Recent literature suggests, however, that in comparison to untreated scoliosis, pediatric patients with cerebral palsy who undergo spinal arthrodesis are able to achieve a substantial improvement in the overall health-related quality of life by 2 years.21,22 In fact, most caregivers report that spinal fusion is the most beneficial intervention in their children’s lives, secondary to only gastrostomy tube placement. 23 Despite the potential benefit of spinal fusion surgery, complications are significant and costly, which present significant opportunities to improve the care for these high-risk patients.
In our study, more than half of our patients experienced at least one complication during the same index admission (52.4%). Interestingly, patients with pulmonary disease, hematological deficiencies, and electrolyte disorders were at particularly higher risk for both inpatient medical and surgical complications. Surgical factors such as the length of fusion and surgical approach appeared to have less influence on the early postoperative course for these patients. As expected, the management of these inpatient complications resulted in a substantially longer LOS and higher index admission hospital costs. The major determinants for extended LOS included discharge disposition to other than home (OR 5.5), return to operating room during the same index admission (OR 4.0), inpatient medical complications (OR 3.8), and inpatient surgical complications (OR 1.8). Patients with a LOS >8 days resulted in nearly double the total hospital costs ($113 669 vs $68 411) and were significantly more likely to be readmitted within 90 days after hospital discharge (OR 1.5). The 90-day readmissions were common (17.6%) and associated with an additional $19 658 of hospital cost. This 90-day readmission rate is consistent with prior literature (16.1%), and substantially higher than what is reported for adolescent idiopathic scoliosis (3.4%). 24 The distribution of postdischarge complications appeared different from that of inpatient complications. While perioperative blood transfusion (35.6%), pulmonary complications (17.6%), and paralytic ileus (8.2%) were the major inpatient issues, the most common postdischarge complications were wound-related issues (eg, wound dehiscence, surgical site infections), nutritional concerns (eg, feeding problems, dehydration, other gastrointestinal), and other infection (eg, pneumonia, sepsis, and urinary tract infection). Furthermore, high-risk groups for inpatient complications, extended LOS, and readmissions appeared similar and suggest that optimizing perioperative pulmonary, hematologic, and nutritional status should be a priority.
Pulmonary complications are common after spinal fusion in neuromuscular scoliosis, and known to be associated with other poor clinical outcomes. In a recent case-series, Luhmann and Furdock reported an incidence of 15.3%, which included pneumonia, pleural effusion, pneumothorax, need for reintubation, respiratory status requiring return to the intensive care unit, and prolonged mechanical ventilation. 25 Similarly, our study found that 17.6% of patients suffered a pulmonary complication, with most of these patients requiring a mechanical ventilation. In a multicenter study of 217 pediatric patients at GMFCS level V, LaValva et al reported that 27% of patients required a prolonged intubation (at least 3 days after surgery), which was significantly associated with increased ICU (intensive care unit) stays, longer hospitalization lengths, and other medical complications (particularly gastrointestinal and other respiratory issues). 26 A multidisciplinary effort to minimize postoperative intubations, when possible, should be a priority. Another important consideration is the preoperative pulmonary function, which is a major determinant of postoperative lung function. Prior literature report that worse preoperative lung function (eg, FEV1 < 40%) is significantly associated with higher postoperative pulmonary complication rates and increases the risk for prolonged postoperative mechanical ventilation.27,28 Delaying surgery can worsen preoperative lung impairment as the deformity becomes more severe. As an alternative to early fusion in skeletally immature patients, growing rods have been shown to effectively preserve thoracic cavity growth while slowing the progression of scoliosis and pelvic obliquity; however, in the pediatric cerebral palsy patient, its use has been associated with a high rate of deep wound infections (30%). 29 The optimal timing for spinal fusion in this patient cohort remains somewhat controversial.
Poor nutritional status is common (46% to 90%) in children with cerebral palsy and known to be associated with postoperative infection after scoliosis surgery.30-33 Specific risk factors include patients with gastrostomy tube dependence, serum albumin <3.5mg/mL, and total lymphocyte count <1500 cells/mL.34,35 In our study, cachexia was an independent risk factor for 90-day readmissions, which included surgical site infections. Electrolyte imbalance, which was also a strong predictor for inpatient complications and readmissions, may be related to poor hydration status and other factors such as respiratory acidosis/alkalosis. This is difficult to determine since specific laboratory markers are not included in the Nationwide Readmissions Database. Nevertheless, dehydration, feeding problems, and infection were among the most common reasons for readmissions. The use of parenteral nutrition in the acute perioperative phase should be considered if enteral or other access is not possible. 5
Reducing blood loss is a major concern during neuromuscular scoliosis surgery. When controlling for perioperative factors such as preoperative hematocrit, platelet count, and levels fused, neuromuscular patients are nearly 7 times higher risk of excessive blood loss (>50% of their estimated total blood volume) in comparison to non-neuromuscular patients. 36 This may be partly due to the depletion of clotting factors, particularly factor VII, which occurs to a greater extent in patients with underlying neuromuscular disease than idiopathic patients who undergo scoliosis surgery. 37 In our study, a substantial percentage of patients (35.6%, N = 1017) required at least one unit of red blood cell transfusion, which is considerably more than what has been reported in prior idiopathic scoliosis literature. 38 Several strategies have been shown to minimize blood loss in this patient population. These include meticulous hemostasis and intraoperative hypotension during surgical dissection, the use of antifibrinolytics (eg, tranexamic acid), use of a bipolar sealant device, and a 2-attending surgeon team.39-42
Wound complication was the most common reason (dehiscence—21.1%, surgical site infection—19.1%) for 90-day readmission in our study. 5 In a recent multicenter study on pediatric patients with cerebral palsy, Eguia et al found that among other major complications after spinal fusion surgery, wound infection was an independent predictor for less improvement in CPCHILD total scores at 2 years postoperative. 43 Strategies to reduce the risk of infection may include adequate perioperative nutritional support, meticulous surgical technique, and appropriate perioperative intravenous and local antibiotics.34,44 If infection occurs, aggressive operative debridement, antibiotics, and wound care should be performed. Although wound complications can be a significant and costly burden to the patient and caregiver, recent literature suggests that recurrence of infection is low after appropriate comprehensive management. 45
There are several limitations for this study. First, the Nationwide Readmissions Database is an administrative database, which was designed to study all hospital readmissions and queried based on ICD coding; therefore, it lacks other spine specific variables (eg, exact number of levels fused, operative time) which may influence clinical outcomes. Second, the follow-up period is limited to 90 days after the index hospital admission discharge date. Surgical decision making relies not only on short-term complications, but also long-term outcomes. Third, it was impossible to determine the relative severity of cerebral palsy, both the neurologic impairment and the spinal deformity using this database. A large, prospective study that can control for the degree of spinal deformity and other perioperative factors such as pulmonary function would be helpful in determining the ideal timing of surgery for these patients.
Conclusion
In this largest multicenter study of spinal deformity surgery in pediatric cerebral palsy patients, we found a 54.2% inpatient complication rate and a 17.6% 90-day readmission rate. It is important to recognize that there is a substantial opportunity for quality improvement in this high-risk cohort as both medical and surgical complication rates are substantially high in the early perioperative period, which can lead to prolonged LOS and costly hospital admissions. Continued efforts focused on optimizing the perioperative pulmonary, hematological, and nutritional status as well as reducing wound complications appear to be the most important for improving clinical outcomes.
Supplemental Material
sj-docx-1-gsj-10.1177_2192568220960075 – Supplemental Material for Spinal Deformity Surgery in Pediatric Patients With Cerebral Palsy: A National-Level Analysis of Inpatient and Postdischarge Outcomes
Supplemental Material, sj-docx-1-gsj-10.1177_2192568220960075 for Spinal Deformity Surgery in Pediatric Patients With Cerebral Palsy: A National-Level Analysis of Inpatient and Postdischarge Outcomes by Nathan J. Lee, Michael Fields, Venkat Boddapati, Justin Mathew, Daniel Hong, Zeeshan M. Sardar, Paulo R. Selber, Benjamin Roye, Michael G. Vitale and Lawrence G. Lenke in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.