
Abstract
Study Design
Prospective cohort study.
Objectives
To report the results for an alternative technique based on minimally invasive fusion-less surgery. This approach is original in that it corrects deformities by proximal and distal fixation, with reliable pelvic fixation through the use of iliosacral screws on osteoporotic bones.
Methods
Adult cerebral palsy patients requiring spinal correction surgery were included prospectively between 2015 and 2019. The technique involved the use of a double-rod construct anchored proximally by four clawed hooks and distally by iliosacral screws, in a minimally invasive approach. Cobb angle and pelvic obliquity were measured before and after initial surgery and at final follow-up. Complications and functional results were reviewed. This group (P) was compared with a second group (R) of patients who underwent surgery between 2005 and 2015, for whom data were collected retrospectively.
Results
Thirty-one patients were included in group P, and 15 in group R. The two groups were comparable for demographic data and deformity. At most recent follow-up (3 years for group P [2-6] and 5 years for group R [2-16]), neither correction nor surgical complications differed between the two groups. However, group P had 50% less blood loss and a lower medical complication rate than group R.
Conclusions
Our results confirm the effectiveness of this minimally invasive technique for neuromuscular scoliosis in adults. The results were similar to those obtained with the usual techniques, but with fewer medical complications. Confirmation of these results is now required for a longer follow-up period.
Keywords
Introduction
Scoliosis is frequent and significant in cerebral palsy,1,2 with discomfort, difficulty of treatment, and pain. The deformity continues to worsen into early adulthood, with growth often ending late, after 18 years of age. Life expectancy is reduced by the deformity in severe cases, 3 but is steadily increasing due to advances in treatment. 4 It is, thus, not uncommon for corrective surgery to be performed during adulthood, but with a rate of complications at least as high as that in children, especially with regard to medical complications and infections. 5
On the other hand, several observations and findings have led us to adopt an innovative surgical technique for treating adult spinal deformity.
First, using a graft increases the length of the surgery, increases blood loss and requires the entire spinal column to be exposed. Placing long, very rigid constructs with multiple implants causes stress peaks in certain areas: lumbosacral area, areas where rods are bent significantly, which is often necessary when a rod is being passed through several implants. Bone ankylosis is difficult to achieve because it must extend to the entire construct, without any continuity solution, in adults whose osteogenic potential is much less than in children (1.4% nonunion reported in children, 6.3% in adults). 6 Moreover, even a continuous graft can become deformed, and in itself does not ensure a lasting result.
Also, fusionless spine surgery is now a standard procedure in adults: percutaneous fixation of vertebral fractures7,8 or secondary tumors, 9 flexible instrumentation to prevent the development of junctional syndrome in cases of degenerative disc disease.10-13
Lastly, fusionless spine surgery is now a standard procedure for treating scoliosis in children when the child must be operated before the end of growth. 14 These solid, two-rod constructs are no longer protected by corsets since rod failure is much rarer given the more solid fixation. The bipolar constructs used no longer cross the apex of the curvature, which is difficult to access, but are limited to one approach and solid fixation at the extremities.14,15 A recent study of the Growing Study Group 16 showed it was unnecessary to carry out an additional procedure to fuse the spine; they found the spine becomes stiffer with instrumentation alone and that adding a graft at the end of the growth period was not beneficial. This concurs with other observations that scoliosis is not better corrected with a final surgical fusion procedure. 17
Six years ago, we started performing minimally invasive graft-free surgery for scoliosis in adults. 18 The hypothesis in this population is that this fusion-less bipolar construct can achieve ankylosis of the spine without the need for fusion. In an effort to improve our results and, in particular, reduce the complication rate, we decided to use this technique for the treatment of scoliosis due to cerebral palsy. We report here the comparison of this method with usual techniques.
Material and Methods
Study Design
This prospective study included all adult patients (>18 years of age) undergoing surgery for neuromuscular scoliosis due to cerebral palsy between 2015 and 2019, with a construct extending to the pelvis. All patients underwent surgery with a minimally invasive technique and without bone grafting. All the patients with scoliosis had an oblique pelvis and balance problems, necessitating this extension to the pelvis. All patients underwent a nutritional assessment, with correction of any deficiencies detected, and were checked for sites of infection, with a dental examination and treatment if necessary.
This prospective series was compared to a series of patients undergoing surgery between 2005 and 2015 for the same condition, but with classical arthrodesis, for whom the results were collected retrospectively.
This study was approved by the ethics committee of our establishment (IRB registration #: 00001072). Informed consent was obtained for all patients included in the prospective group through their legal representative.
Surgical Technique
The operation is performed without preoperative traction, with neurological monitoring based on motor and/or somatosensory evoked potentials depending on the preoperative signal obtained.
The patients were installed on an Allen® table with or without traction applied on the lower limbs depending on the stiffness of the curvature. The traction can be asymmetrical to help reduce an oblique pelvis. The head is fixed using a Mayfield clamp. Two posterior approaches are performed. The first incision was made in the lower lumbar area and two transmuscular approaches (as described by Wiltse) were made in order to insert the iliosacral screws and their connectors (TANIT®, Euros) (Figure 1). The iliosacral screws were implanted using a navigation system (O-Arm, Medtronic, Sofamor, Broomfield, CO).
19
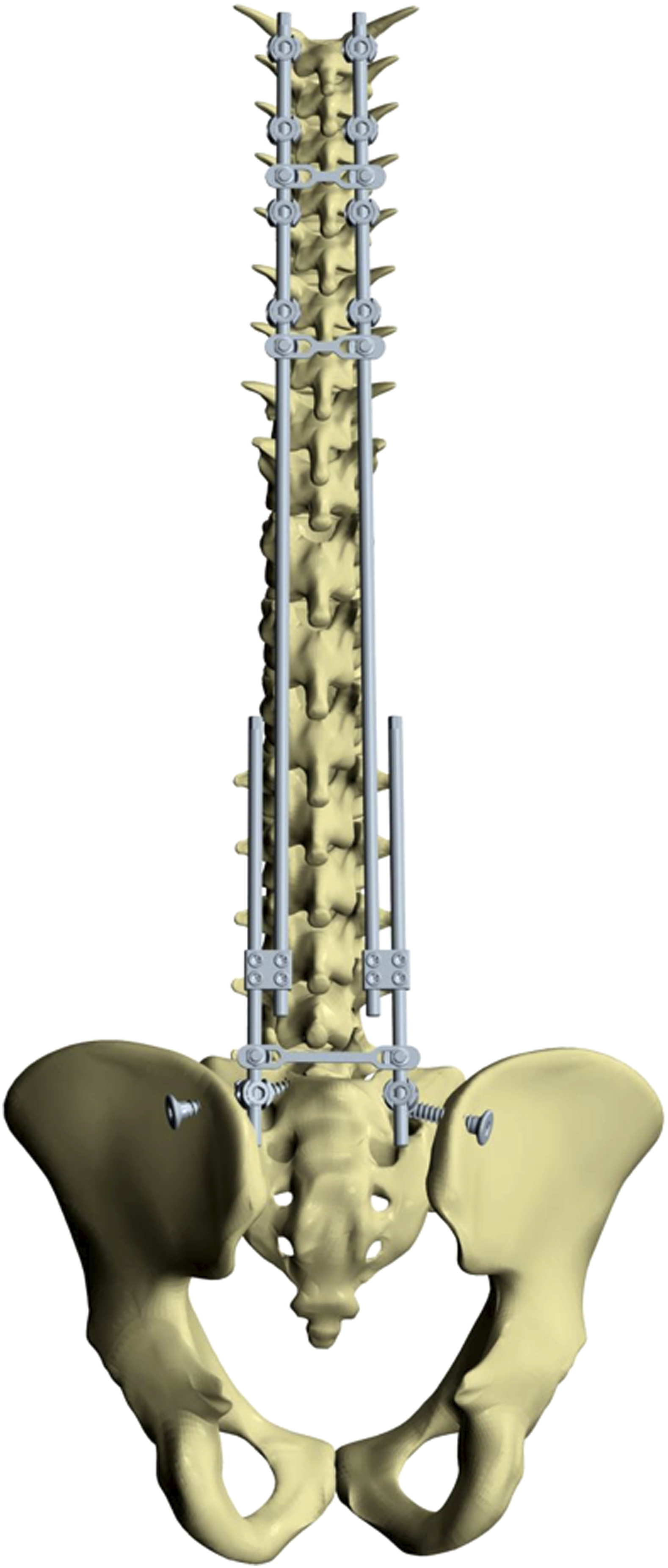
A second incision was made in the upper portion of the thoracic spine where hooks were implanted (supralaminar and pedicle hooks) to act as two pediculolaminar clamps on either side. The superior construct is made on 5 vertebrae. Cobalt-chrome rods were inserted under the fascia to join the upper hooks to the lower connectors with placement of a long rod and short rod joined by a domino. Rod curving, lever maneuver with lowering of rods in the lower connectors, distraction, compression and bending in situ were used to rebalance each patient’s spine. The pelvic obliquity is progressively corrected by a distraction maneuver at the level of the domino between the short and the long rod. The final construct was stabilized with three or four transverse linking devices. These devices were introduced in the standard manner from the upper portion and transmuscular to the lower portion to join the two approaches. No additional incisions were needed (Figure 2). A, The jig used to guide the iliosacral screw placement. B, The iliosacral screw. The bipolar construct anchored proximally by hooks in a double claw and distally by iliosacral screws through a minimally invasive approach.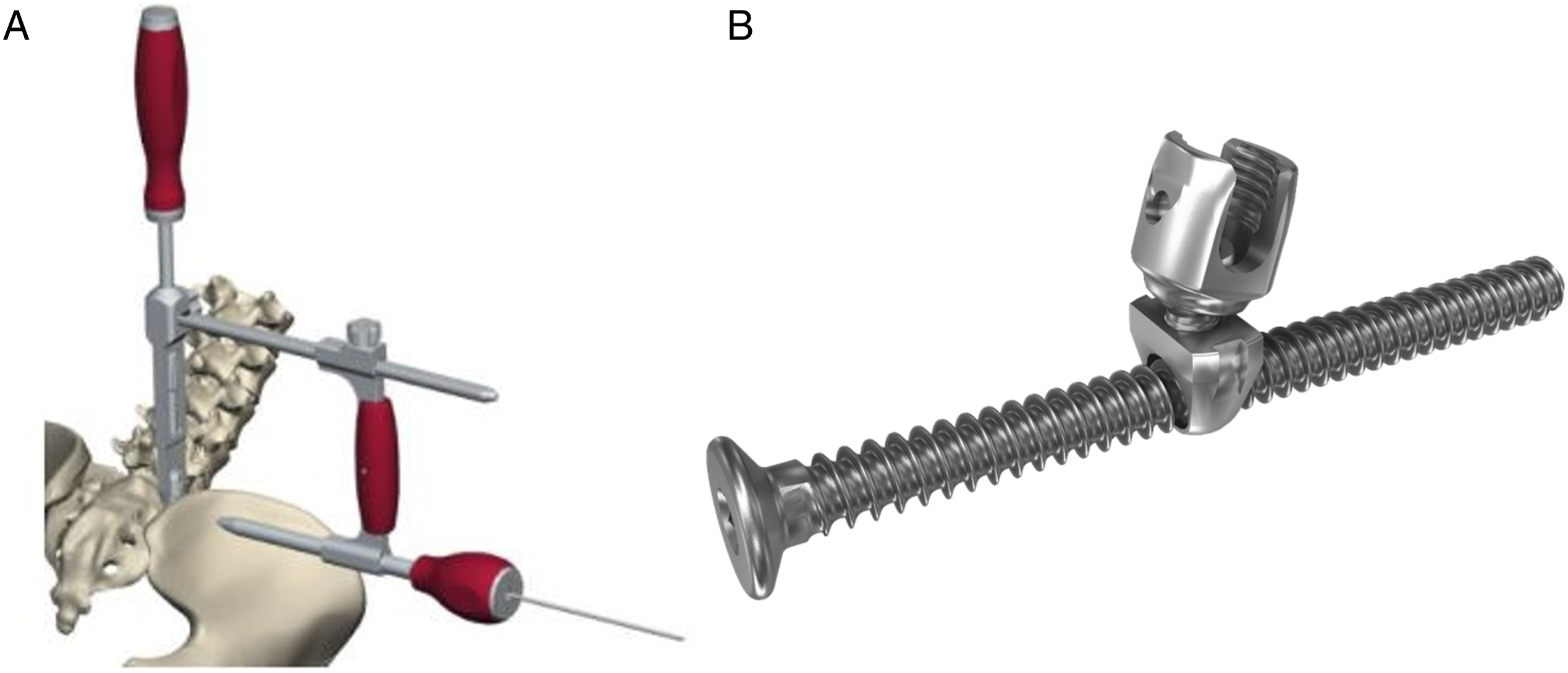
An x-ray image was taken with the O-Arm during the procedure to evaluate the balance and correction, allowing adjustments to be made as needed. In cases of very rigid deformity, this technique offers the possibility of performing the reduction in several stages: Indeed, it is possible to reoperate several months later and improve the correction of the spinal balance by manoeuvers through the distal incision only.
Post-operatively, patients are mobilized as quickly as possible. They is placed in a sitting position on D1 post-surgery. The urinary catheter is removed after 48 hours and the dressings are redone every 48 hours. Antibiotic prophylaxis with cephazoline is started at least 30 minutes before the surgery and continued during the 2 days following the procedure, according to the recommendations of the nosocomial infection control committee (NICC) at our establishment.
In the retrospective group, patients were operated on using a conventional midline approach with exposure of the entire spine from T1 to the pelvis. Conventional instrumentation was performed using pedicle screws, hooks at the top and iliac screws in the pelvis (Figure 3). Radiographs of a patient operated on according to the conventional technique.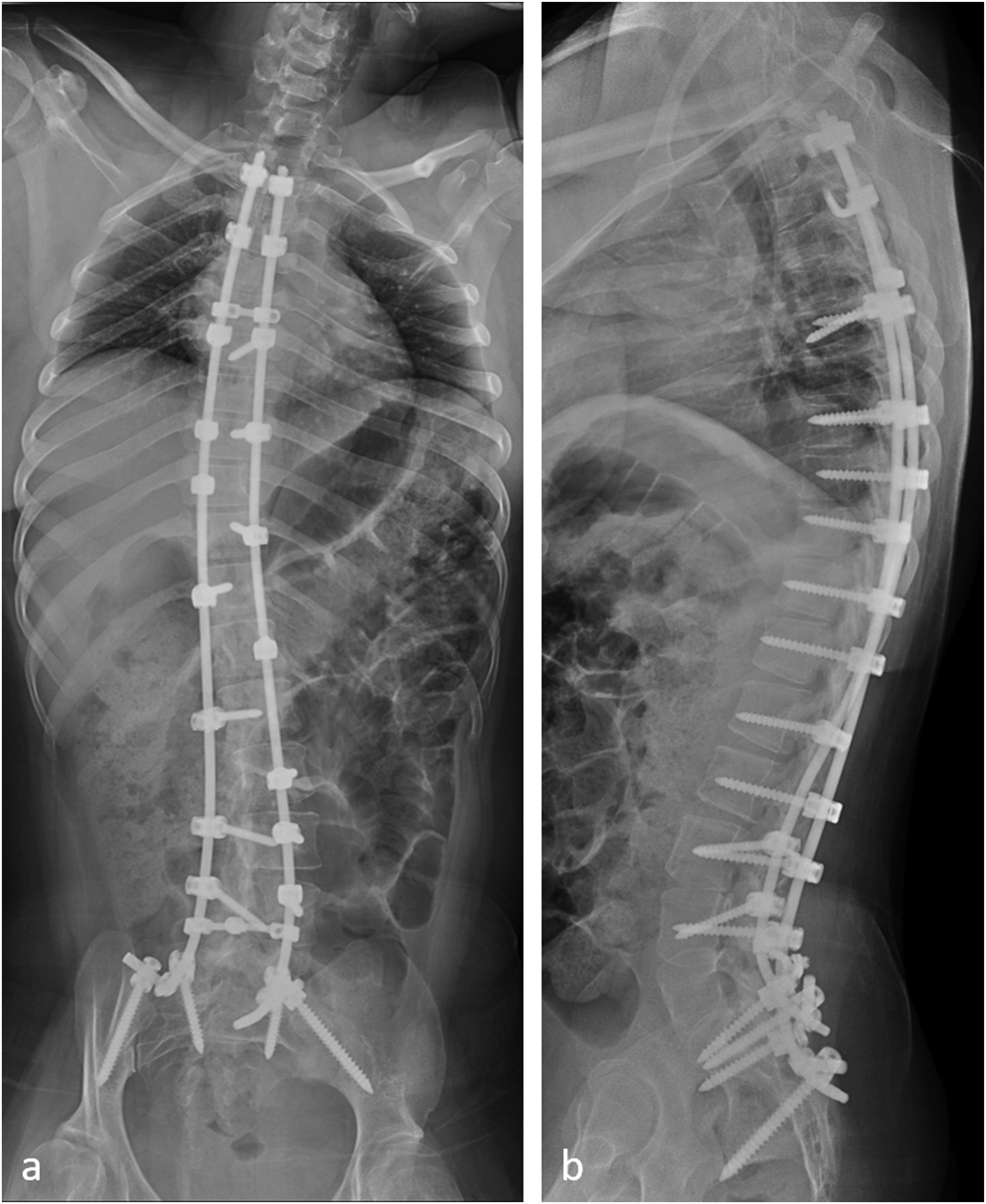
Data Collection
The following preoperative clinical data were collected for all patients in each group: age, weight, height, and body-mass index (BMI). The main antecedents and comorbidities were also collected. Motor skills were assessed with the gross motor function classification system (GMFCS) score for cerebral palsy. 20
The following data were recorded during surgery: operating time and blood loss. Blood loss was assessed with the formula of Rosencher et al, 21 which quantifies peri- and postoperative blood loss in the first 48 hours.
All patients underwent X-ray imaging, before surgery, after surgery, and at last follow-up visit. The following data were collected for each image: angulation of the main curvature (defined frontally or sagittally, depending on whether scoliosis predominated or the patient presented pure hyperkyphosis) and pelvic obliquity.
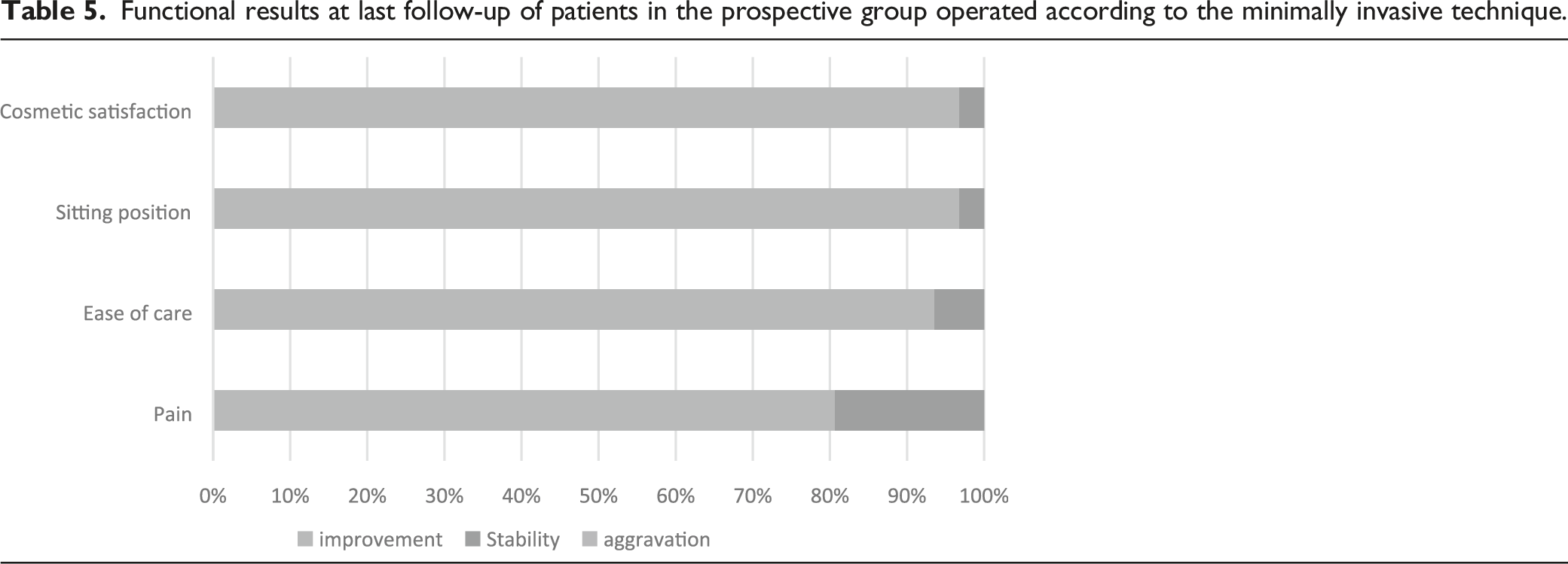
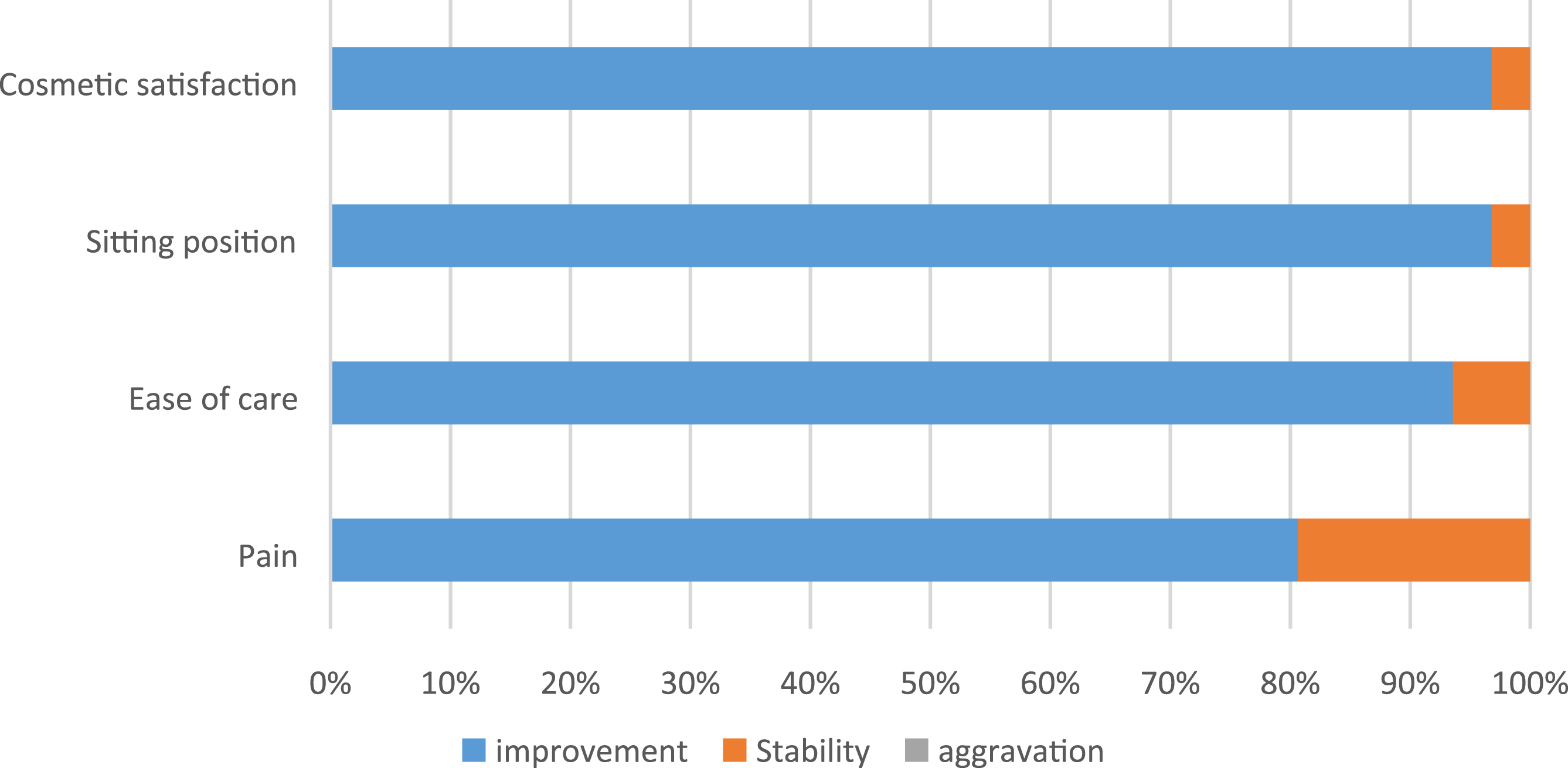
For the patients included in the prospective group, a simplified questionnaire based on the evaluation questionnaire for children with cerebral palsy (CPCHILD) was used to evaluate the functional result. Four items were evaluated by the patient’s parents and caregivers, when possible: pain, ease of care, comfort in the sitting position, and cosmetic satisfaction. For each question, three answers were possible: improvement, stability, or worsening.
Finally, data concerning all complications occurring during surgery and/or during the follow-up period were collected for each patient. Complications were classified into two main categories: surgery-related complications divided into 3 subgroups (neurological, site infections, mechanical) and general complications (death, cardiopulmonary, thrombo-embolic, infectious, iatrogenic).
The minimum follow-up period was 2 years. All data were recorded in a dedicated Keops database (SMAIO®, Lyon, France).
Statistical Analysis
Quantitative variables are expressed as means ± standard deviations or medians and interquartile range [Q1; Q3], and were compared in Student’s t or Wilcoxon tests, depending on their distributions. Qualitative variables are expressed as numbers (proportions) and were compared in Chi-squared or Fisher’s exact tests, depending on the application conditions.
Analyses were performed with R software (R Core Team, 2021. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/). All tests were two-tailed and a P-value <.05 was considered significant.
Results
Description of the Cohort
Minimally invasive bipolar construct group: Thirty-one patients, with a mean age of 22 years (18-36 years), underwent surgery with the minimally invasive technique described above. Mean BMI was 18.14-26 According to GMFCS score, the series included two patients at stage 3 (walking), 10 at stage 4 (wheelchair with a little autonomy), and 19 at stage 5 (totally dependent). Mean follow-up was three years (2-6 years).
Traditional instrumented fusion group: Fifteen patients underwent surgery with the classic technique from 2003 to 2013 at a mean age of 22 years (18-35 years). Mean BMI in this group was 18.7.16-27 This group included five patients at GMFCS stage 4 and nine at GMFCS stage 5. The last evaluation of this group occurred after a mean follow-up of five years (2-16 years).
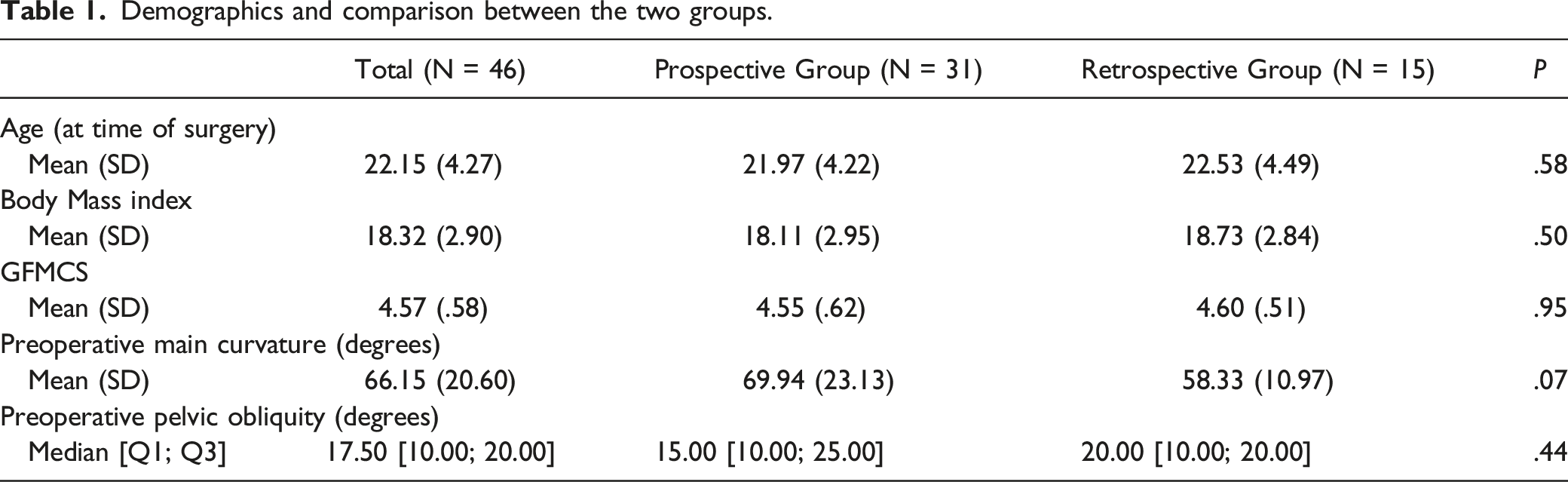
Demographics and comparison between the two groups.
Perioperative Data
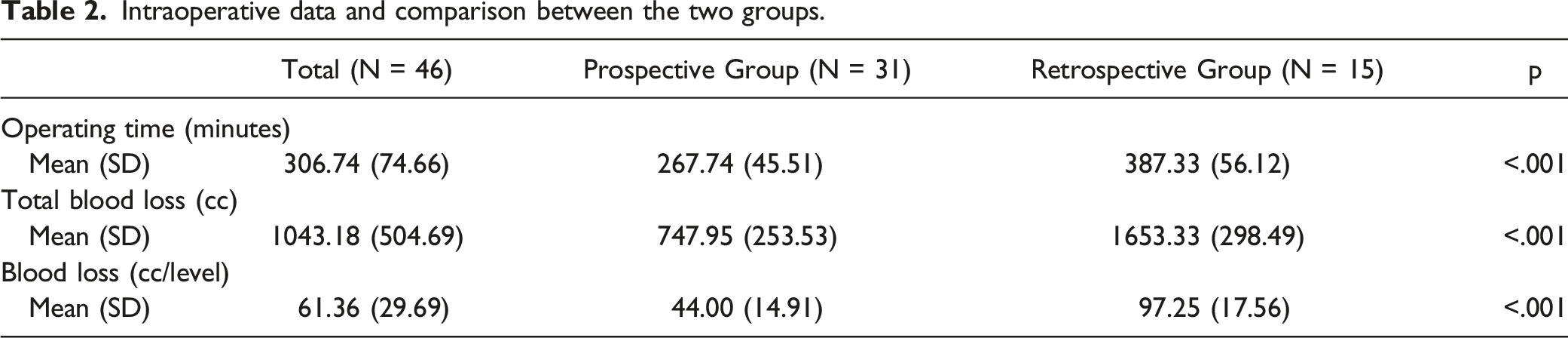
Intraoperative data and comparison between the two groups.
Radiological Results
Minimally invasive bipolar construct group: Mean preoperative Cobb angle was 70° (10-130°). It was reduced to 36° (10-70°) after surgery, corresponding to a mean correction of 51%. Mean preoperative pelvic obliquity was 18° (0-40°). It was reduced to 7° (0-26°) after surgery, corresponding to a mean improvement of 62% (Figure 4). Radiographs of a non-walking patient. A/B, Preoperative x-rays with a 100°curve. C/D, X-rays after surgery at 5 years of follow-up.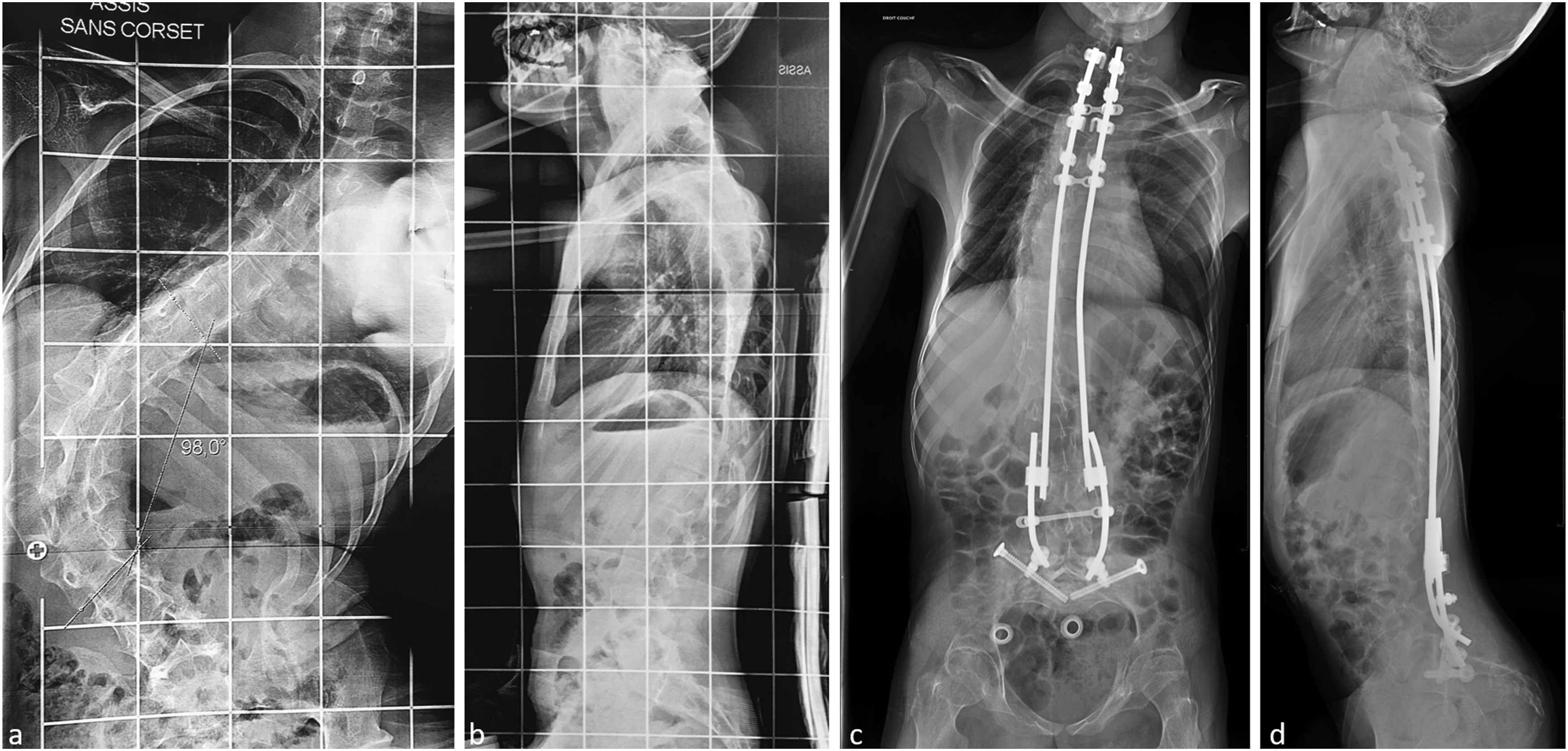
Traditional instrumented fusion group: Mean preoperative Cobb angle was 58° (45-80°). It was reduced to 30° (15-50°) after surgery, corresponding to a mean correction of 51%.
Pelvic obliquity was improved by 57%, from 14° (0-30°) before surgery to 6° (0-20°) after surgery.
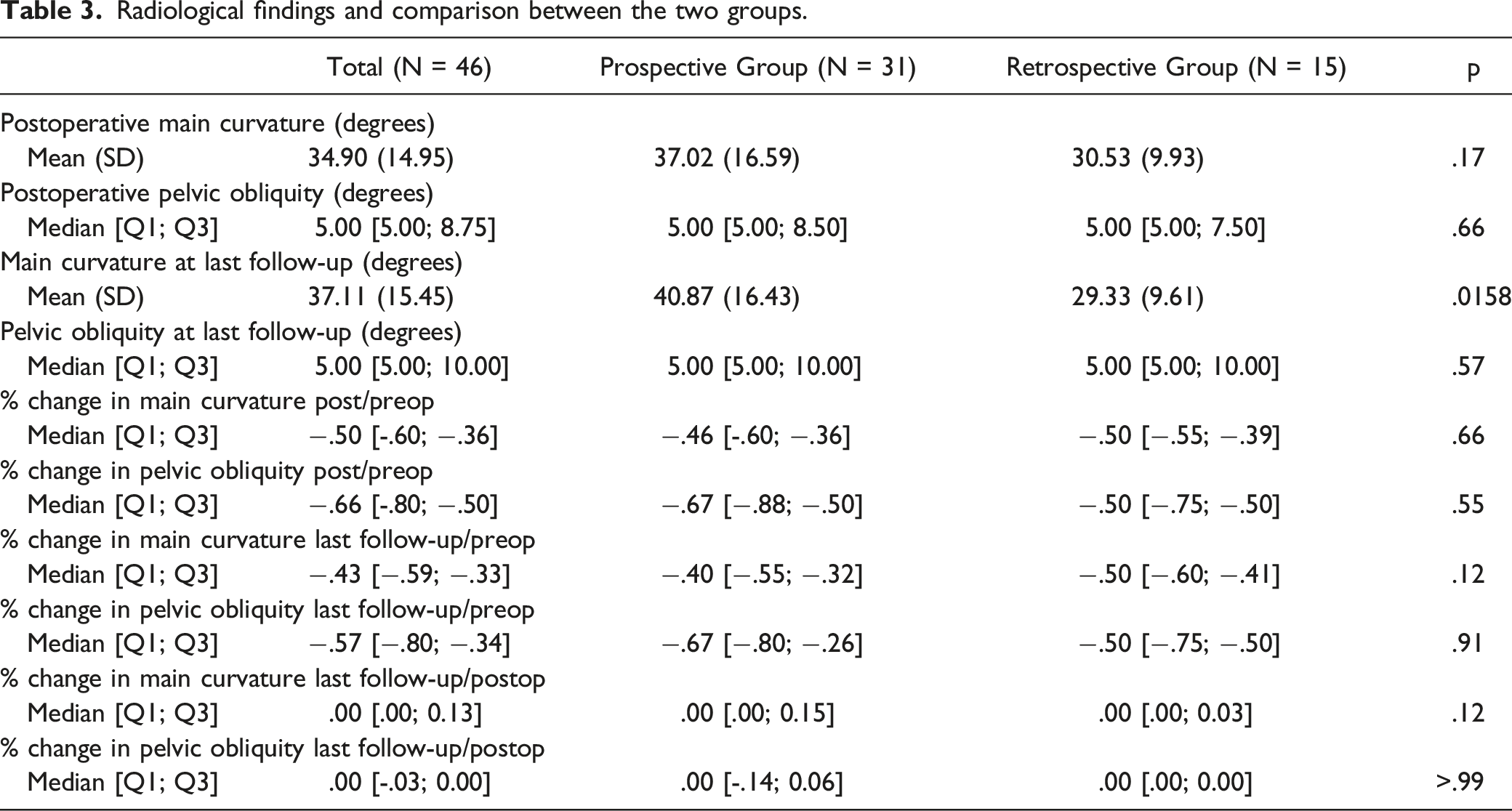
Radiological findings and comparison between the two groups.
Complications
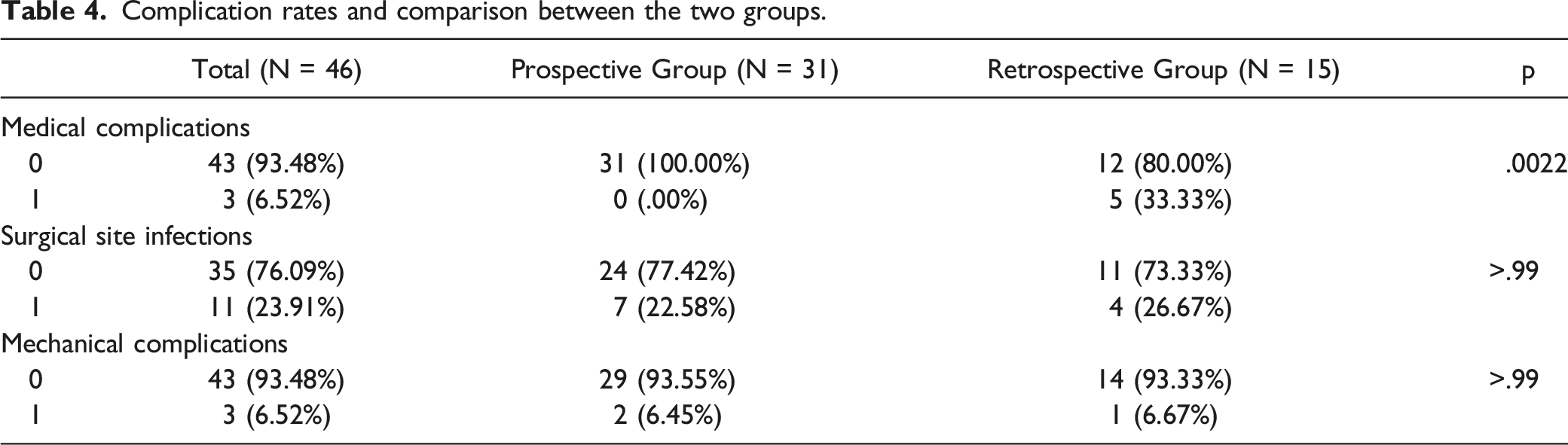
Minimally invasive bipolar construct group: There were no major medical complications in this series.
There were two mechanical complications (6%): one disconnection, which were repaired with a favorable outcome and one rod rupture associated with a disconnection. This walking patient was reoperated using the same technique: the two long rods were removed and replaced with a 4 rods construct. Iliac screws have also been added in order to protect the iliosacrall connectors from a recurrence of disconnection. No conversion to a traditional fusion was required after 4 years of follow-up of the revision surgery (Figure 5). No patient needed a revision surgery for a proximal junctional kyphosis. Seven patients presented surgical site infection (SSI) (23%), including one late infection requiring the removal of the material. These infections occurred a mean of 19 days after surgery. Half these infections were multi-microbial. Staphylococci were the microorganisms most frequently identified (S. epidermidis or S. aureus, either methicillin-sensitive [30%], or methicillin-resistant [5%]). The other microorganisms identified were Propionibacterium acnes (10%), Proteus (10%), Enterococcus (5%), and Escherichia coli (10%). Radiographs of a walking patient. A/B, Preoperative x-rays with a 80°curve and important coronal imbalance. C/D, X-rays after surgery at 2 years of follow-up. E/F, X-rays showing the rod breakage occurring the third year after surgery. G/H, X-rays after revision at 4 years of follow-up.
Traditional instrumented fusion group: We identified five major medical complications (33%): one case of acute lower limb ischemia, three pulmonary infections, one pulmonary embolism and a serious mechanical complication (7%), in which the fixation system failed, necessitating surgical revision. Finally, four patients presented SSI (27%).
Complication rates and comparison between the two groups.
Functional Results
Functional results at last follow-up of patients in the prospective group operated according to the minimally invasive technique.
Discussion
Our series was unique in the use of a recent technique on adults with cerebral palsy. The aim was to use a minimally invasive technique, with the hope of ensuring results similar to those obtained with the classic technique, but with fewer complications. This minimally invasive technique has already proved effective in children. 22 We focused on its application in patients older than 18 years. No other study has focused on scoliosis surgery specifically in adults with cerebral palsy or on the use of this new technique in these patients.
Most authors have reported favorable results for arthrodesis, as shown by the meta-analysis of Legg et al. 23 After a mean follow-up of three years, the functional results obtained with this minimally invasive technique are similar to those of the conventional technique,23,24 with lower blood loss and fewer medical complications. Indeed, perioperative blood loss was 44 cm3 per level in our study. According to Shapiro and Sethna, 25 the mean blood loss for this population is 150 cm3 per level and 97 cm3 in our retrospective group.
The radiological results of frontal correction were slightly lower than those usually obtained with the conventional technique, with a mean correction of 51%, and no significant difference between our two series. Pediatric and mixed series gave results ranging from 54% 26 to 68% 27 correction. Pelvic obliquity was most often strongly improved, to a degree similar to that reported by other teams (62% here and an average of 60% for the series mentioned above). Although not done here with this particular technique, it is possible to improve correction thanks to domino connectors if the initial reduction does not sufficiently correct pelvic obliquity. This possibility was described by Miladi et al, 22 explaining why pelvic obliquity was improved compared to the postoperative state. No loss of correction was observed during the follow-up period.
Given the follow-up data currently available, the durability of the reduction obtained and of the results over time remain uncertain. For this graft-free surgery to work, the spine must become progressively stiffer or undergo ankylosis. Such spontaneous evolution of the spine has been reported in children operated on early for scoliosis, in whom definitive arthrodesis was, finally, not performed. 16 Several authors have reported successful graft-free surgery in patients after the end of growth: Gazzeri et al for spondylolisthesis, with fusion occurring without a graft after percutaneous osteosynthesis, 28 Maruyama et al for scoliosis, with a mean follow-up of eight years. 29 But the most important study supporting this hypothesis is the one published by Gaume et al reporting the results of the same technique as the one we describe in this work applied to a population of pediatric neuromuscular scoliosis and reviewed after a minimum follow-up of 5 years. 30
The absence of major medical complications is highly encouraging. In the past, there were concerns about such procedures at our hospital due to the high frequency of medical complications. The rate of major medical complications was 40% over a period of 10 years. Knowledge of these risks was a barrier for the medical team and the patient’s family, due to a legitimate lack of confidence in this type of surgery. These difficulties can be found in other published series with a medical complication rate of more than 10%,5,31,32 and all included deaths.
Mechanical complications were limited to one patient in this prospective series. Thus, in the short and medium term, we experienced no more problems than in our previous series. In a meta-analysis, Sharma et al.
5
found an overall mechanical complication rate of 10%. The series with the longest follow-up had mechanical complication rates that could exceed 40%.
33
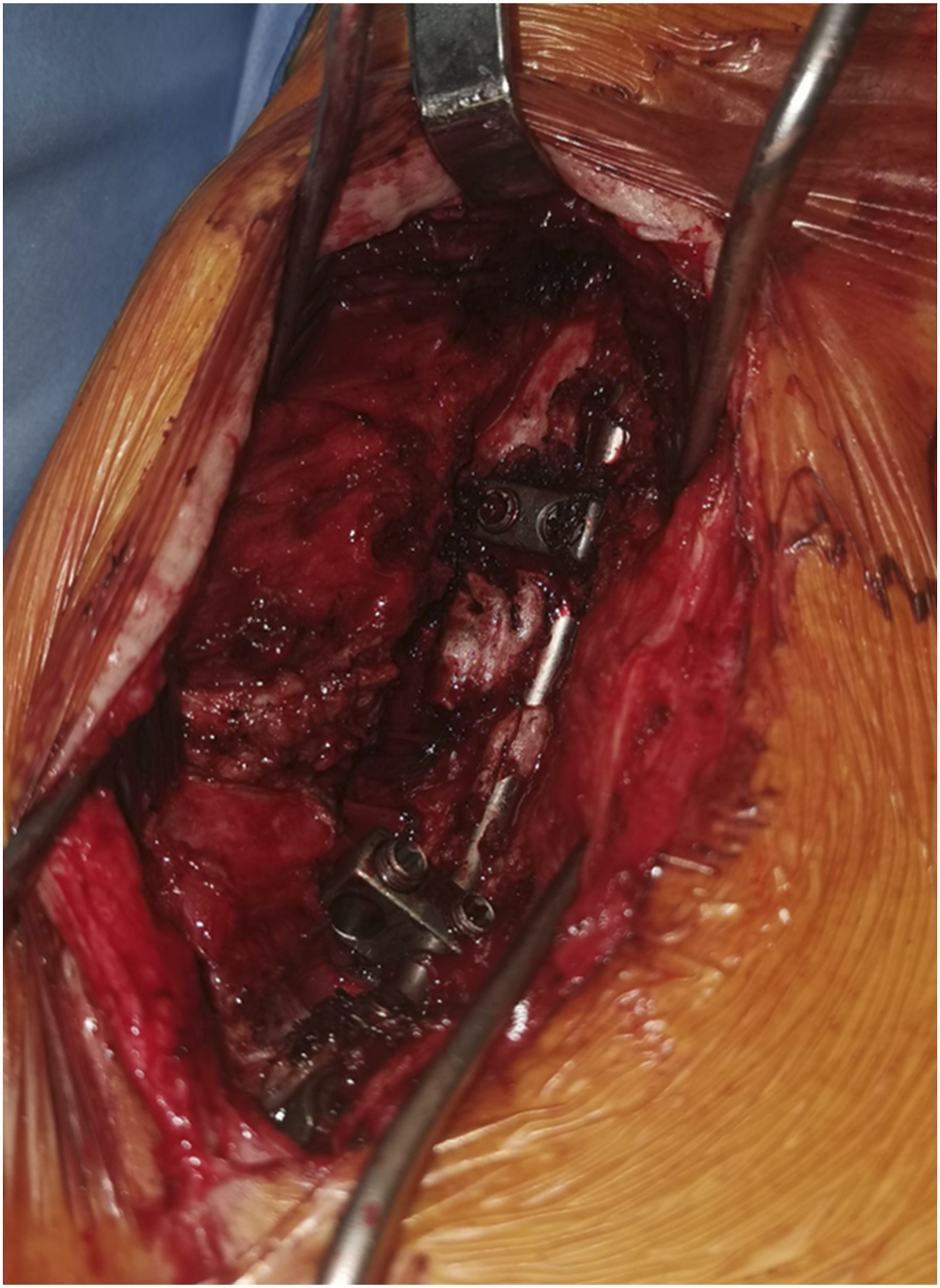
In addition, the iliosacral screw has proven to be effective in the long term in spinal constructs, leading to a low rate of mechanical complications.34,35 The hypothesis underlying this research is that progressive ankylosis can be achieved with this fixation. We were able to obtain proof of the reality of this hypothesis with control scans performed at 5 years’ follow-up in some of the patients in this series (Figure 6), and also by noting the presence of bone fusion during revision surgery (Figure 7). This hypothesis has already been verified in children
30
and it therefore appears to be true in adults as well. Indeed, in the children’s series, none of the patients underwent reoperation to obtain a definitive fusion.
30
We therefore believe that it is the achievement of this ankylosis that prevents mechanical complications. CT-scan control at 5 years of follow-up. A, coronal reconstruction. B, sagittal reconstruction. Intraoperative view of spontaneous bone fusion during revision surgery.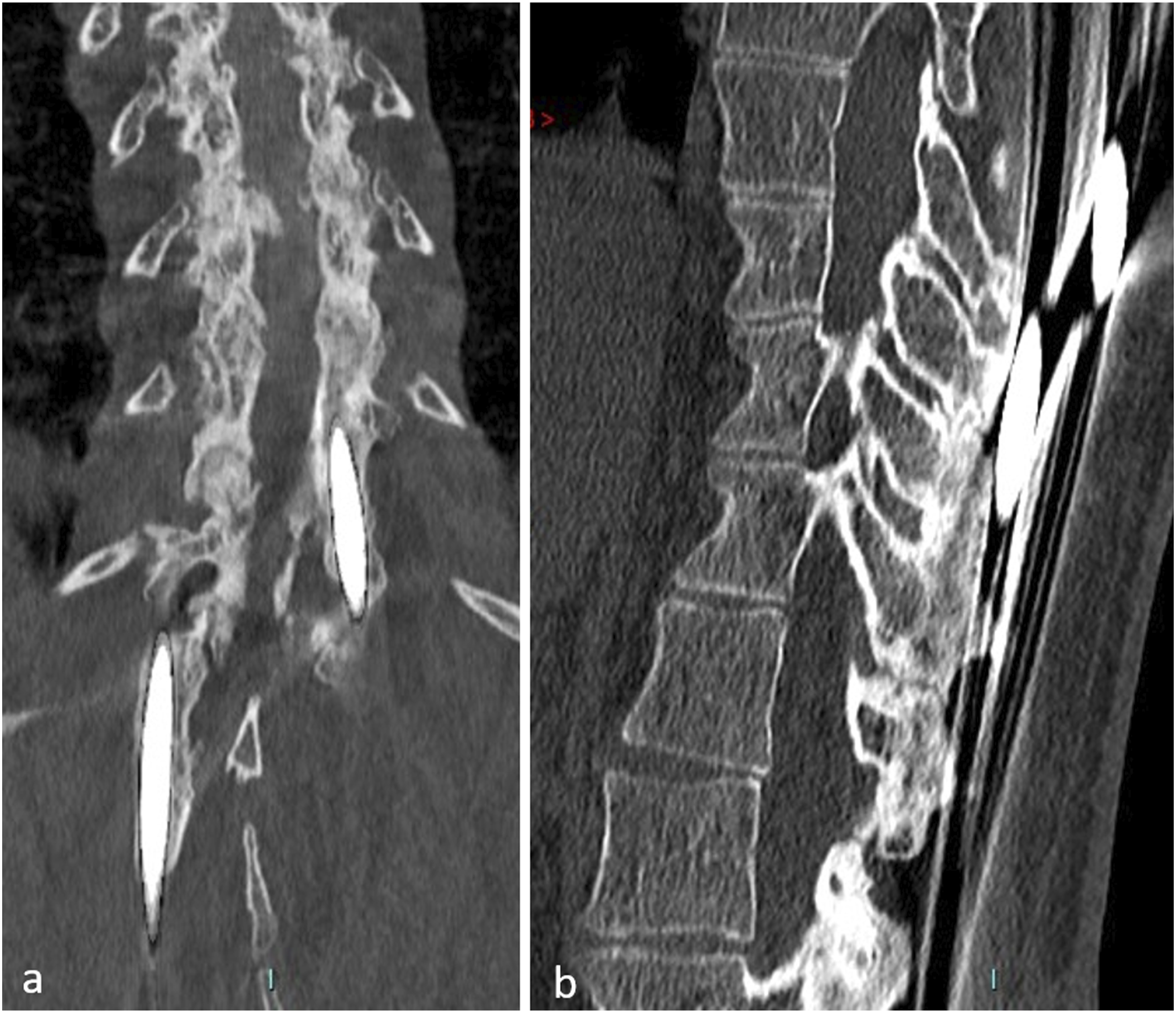
However, the infection rate of 18% was disappointing. We had hoped to reduce this complication rate by using a minimally invasive technique, but no improvement was observed. The mean infection rate was 11% (0-46%) in the meta-analysis by Sharma et al, 5 whereas Legg et al 23 reported infection rates ranging between 2 and 56%. The recent multicenter series of the Scoliosis Research Society 32 reported a 10% infection rate. The mechanism of contamination is difficult to establish. Contamination by bacteria on the skin may occur during the operation or during the first few days, when the scar is not an impenetrable barrier. Infections with urinary bacteria probably result from bacteremia. Intestinal infections may occur through contamination of the perineal region or bacteremia.
Despite the recommendations of the nosocomial infection control committee (NICC) at our establishment, the infection rate remained high. It is known that hypoalbuminemia must be corrected and it is recommended to perform surgery only on patients with normal lymphocyte levels. Patients with cerebral palsy have a body lower weight and BMI than the general population, proportional to the severity of their motor impairment. Patients below the 10th percentile have a higher risk of medical complications, and the risk of infection increases considerably for those below the 20th percentile, 36 ie, a weight of 28 kg for an adult patient. Kobayachi et al. 37 reported a threshold BMI of 20, below which the infection rate increases considerably.
This raises the question of whether to operate on patients with a BMI below 20. Weight gain following gastrostomy is often only moderate. In our series, we found no association between BMI and the occurrence of SSI. Some groups use broader-spectrum antibiotic prophylaxis. Others use antibiotic prophylaxis of longer than several days’ duration. Finally, some groups recommend the use of antibiotic therapy in situ (vancomycin powder) but this practice remains controversial.
After a multidisciplinary consultation, we decided to change our practices for such surgery. As most of the infections involved staphylococci, we are continuing to use cefazoline, but have extended its administration to the second day after surgery. However, it should be noted that, apart from one case of late sepsis requiring the complete removal of the material, without consequences and without loss of correction, all cases of infection progressed favorably under appropriate, prolonged antibiotic therapy.
This study, inevitably, has several limitations. Given the mean follow-up of three years, a study period of six years, and a series of only 31 cases, the results should be interpreted with caution, especially for spinal fixation without a graft. The continuing follow-up of this prospective cohort will make it possible to assess the durability of the results over time.
Conclusion
This study confirms the effectiveness of the minimally invasive bipolar technique for treating neuromuscular scoliosis in young adults. In the medium term, this approach yields results similar to those obtained with the usual techniques, but with fewer medical complications. These results require confirmation after a longer period of follow-up.
Footnotes
Acknowledgments
To Emmanuelle Sacco from the clinical research center of the Paris Saint-Joseph Hospital Group for the technical support.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: State: fees for consulting from Euros company for Dr L. Miladi and G. Riouallon.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study sponsor is the “Groupe Hospitalier Paris Saint-Joseph”. The cohort protocol has been approved by the institutional ethics committee (IRB number IRB00012157).