
Abstract
Study Design
Cross-sectional, international survey.
Objectives
To evaluate the knowledge of spine surgeons regarding the use of electromyography (EMG) and nerve conduction studies (NCS) for degenerative cervical spine conditions (DCC).
Methods
All members of AO Spine International were emailed an anonymous survey to evaluate their clinical knowledge about the use of EMG and nerve conduction studies for DCC. Descriptive statistics were used to analyze the results, as well as to compare the answers among different groups of surgeons and assess demographic characteristics.
Results
A total of 402 participants answered the survey, 91.79% were men from the 5 continents. There were 221 orthopedic surgeons (55.39%) and 171 neurosurgeons (42.86%), more than a half of them with a complete spinal fellowship (56.44%). The most common reasons that surgeons obtain the test is to differentiate a radiculopathy from a peripheral nerve compression (88.06%). As a group, the responding surgeons’ knowledge regarding EMG-NCS was poor. Only 53.46% of surgeons correctly answered that EMG-NCS is unable to differentiate a C5 from a C6 radiculopathy. Only 23.47% of the surgeons knew that EMG-NCS are not able to diagnose a pre vs a post-fixed brachial plexus. Only 25% of the surgeons correctly answered a question regarding the test’s ability to diagnose other neurological diseases.
Conclusions
We found that our respondents’ knowledge regarding EMG-NCS for DCC was poor. Identifying the weak points of knowledge about EMG-NCS may help to educate surgeons on the indications for the test and the proper way to interpret the results.
Keywords
Introduction
Electromyography (EMG) and nerve conduction studies (NCS) are often used by spine surgeons to diagnose cervical radiculopathy, as well as to rule out other non-spinal conditions such as motor neuron diseases, plexopathies, compressive neuropathies, among others.1-3 However, many spine surgeons have no training in EMG/NCS and may not be aware of the advantages, disadvantages, and limitations of electrodiagnostic tests in diagnosing and differentiating cervical conditions from non-spinal pathologies. For the past couple of years, the senior author (KDR) has given numerous lectures regarding EMG/NCS use for cervical spine conditions using an audience-participation test format and noted that the vast majority of spine surgeons in both the US and abroad have minimal or incorrect knowledge regarding their use. We undertook this multi-national survey study of AOSpine members to evaluate the knowledge base of spine surgeons regarding EMG and NCS for degenerative cervical conditions.
Methods
We came up with a set of clinical questions and answers related to the use of EMG and NCS that we felt were appropriate for spine surgeons who treat cervical conditions. The answers were provided by an experienced neurophysiologist (CRM) using pertinent literature as well as his knowledge base from years of clinical practice.
Questions Emailed in this Survey.
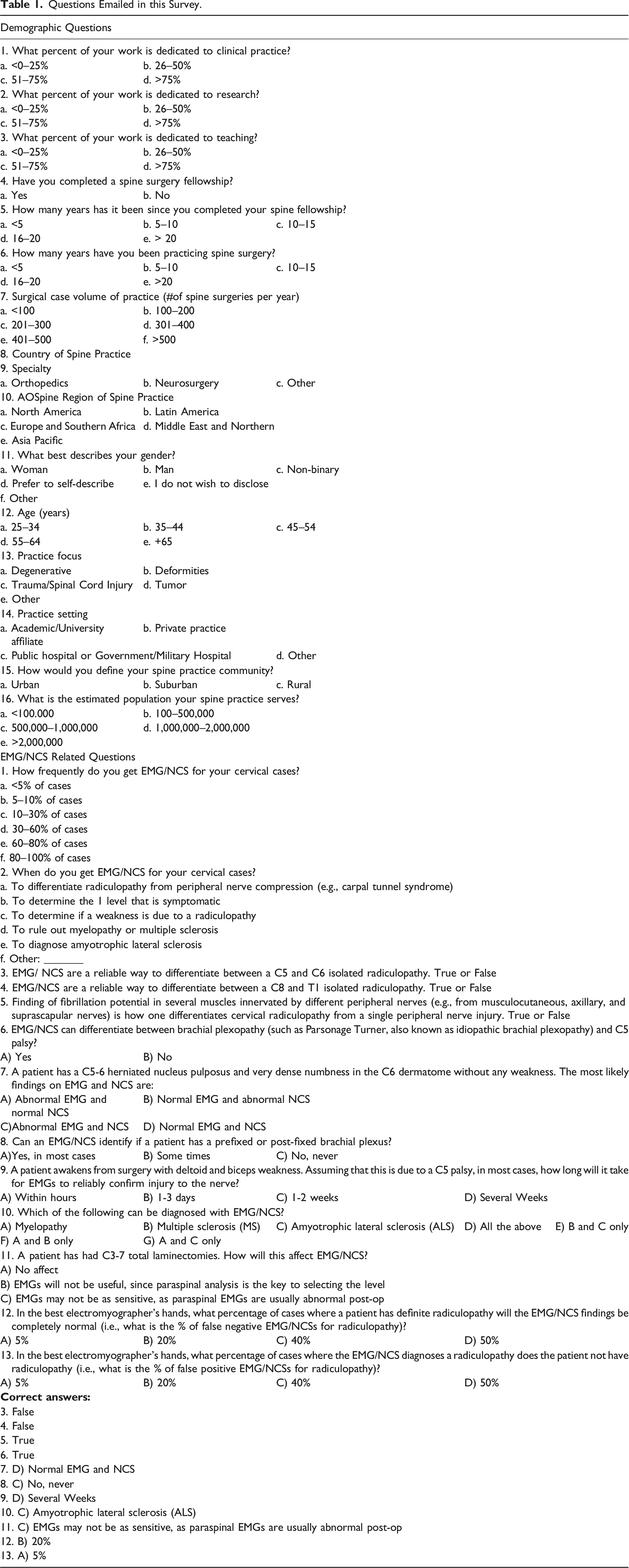
In addition, surgeons were asked, for each question, how sure they were about their answers, with a scale ranging from 0 (don´t know the answer), 1 (I think I know, but I’m not sure), 2 (I’m pretty sure, but I´m not positive) and 3 (I´m positive I know the answer).
Survey Distribution
The survey was distributed via email to AO Spine members between April 21 and April 29, 2021. It was estimated that over 6000 surgeons that were AO Spine members received the email. Among all those who received the email, 402 responded the survey. All questions were optional and those not answered were excluded from analysis.
Survey Analysis
The data was grouped in an Excel file and analyzed using descriptive statistics to describe overall responses. Subgroup analyses were performed comparing different group of respondents with the wrong or right answer using a Chi-square statistic test with a P value of <.05 for significance.
Results
Survey Demographics Responses.
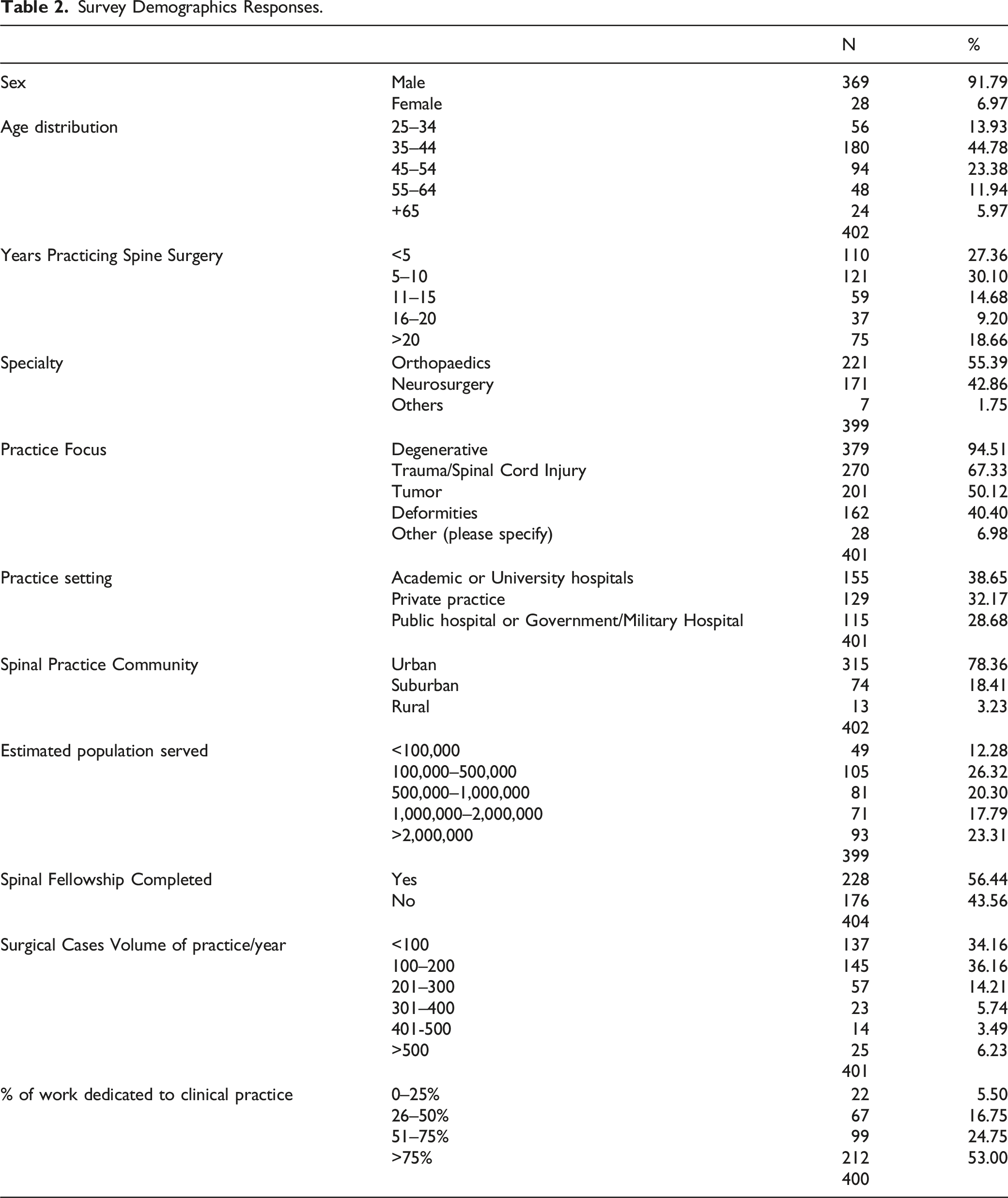
Considering their work characteristics, 53% of the participants dedicated more than 75% of their work to clinical practice; 85.21% dedicated less than 25% of their work to research, and, finally, 73.13% of the participants spend less than 25% of their time teaching.
Questions Specifically Addressing EMG/NCS
Question 1: How frequently do you get EMG/NCS for your cervical cases?
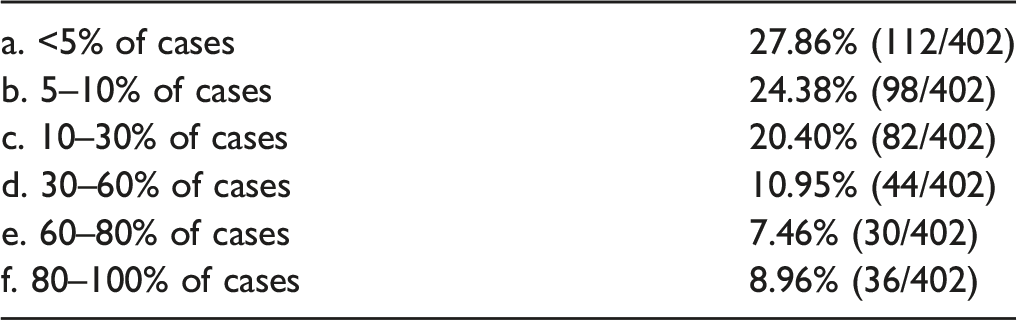
27.86% (112/402) requested in < 5% of the cases, 24.38% (98/402) in 5–10%, 20.40% (82/402) in 10–30%, 10.95% (44/402) in 30–60%, 7.46% (30/402) in 60–80% and 8.96% (36/402) in 80–100% of the cases. Grouping these answers, over 50% of the surveyed surgeons obtained EMG/NCS in less than 10% of their cervical cases. On the other hand, 16.42% obtained them in the majority (>60%) of their cases.
Question 2: When do you get EMG/NCS for your cervical cases?
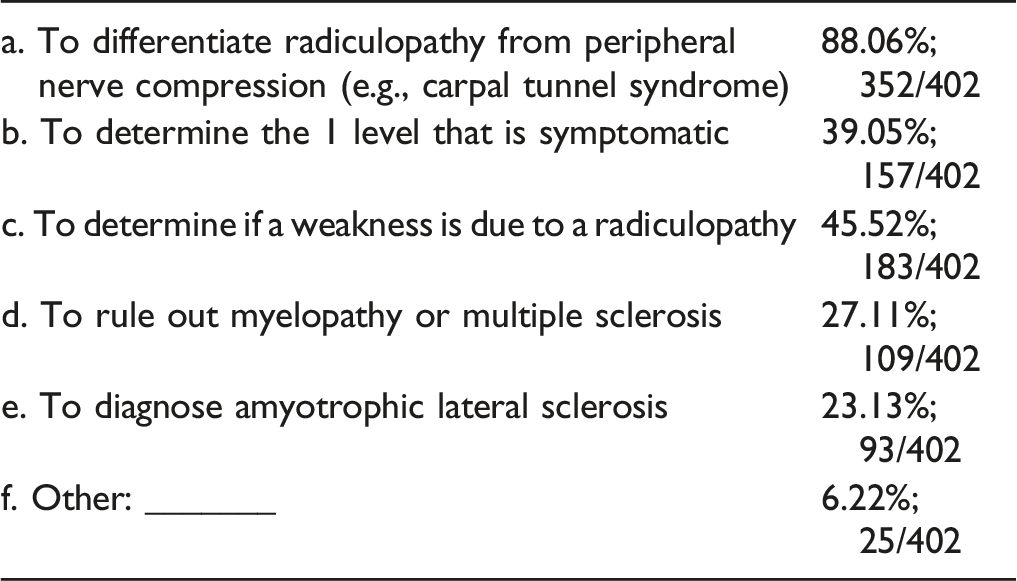
The most common reason to request an EMG-NCS was to differentiate a radiculopathy from a peripheral nerve compression (88.06%; 352/402), then, to determine if a weakness is due to a radiculopathy (45.52%; 183/402), both of which are valid reasons to obtain EMGs. However, EMGs cannot determine the one level that is symptomatic, which 39.05%; (157/402) ordered the tests for or to rule out myelopathy or multiple sclerosis, which 27.11% (109/402) said that they ordered the tests for.
Note that EMG/NCS is not useful to rule out myelopathy or multiple sclerosis, as well as to determine the level that is symptomatic (see comments below).
For the rest of the questions, we will display the results starting with the question with the most correct answers. The percentage of correct answers was, respectively: 82.8% (question 6), 64.95% (question 5), 60.76% (question 4), 53.46% (question 3), 50% (question 12), 49.21% (question 9), 47.12% (question 13), 45.86% (question 11), 23.47% (question 8), 23.35% (question 10), and 16.56% (question 7). In addition, we looked at the percentage of answers that were correct where the respondent was positive that they knew the answer. From highest to lowest percentage, these were: 21.3% (question 6), 20.3% (question 9), 15.4% (question 5), 12.9% (question 3), 12% (question 4), 9.8% (question 11), 7% (question 13), 6% (question 10), 5.4% (question 7), 4.5% (question 8), 2.5% (question 12).
Question 6: EMG/NCS can differentiate between brachial plexopathy (such as Parsonage Turner, also known as idiopathic brachial plexopathy) and C5 palsy?
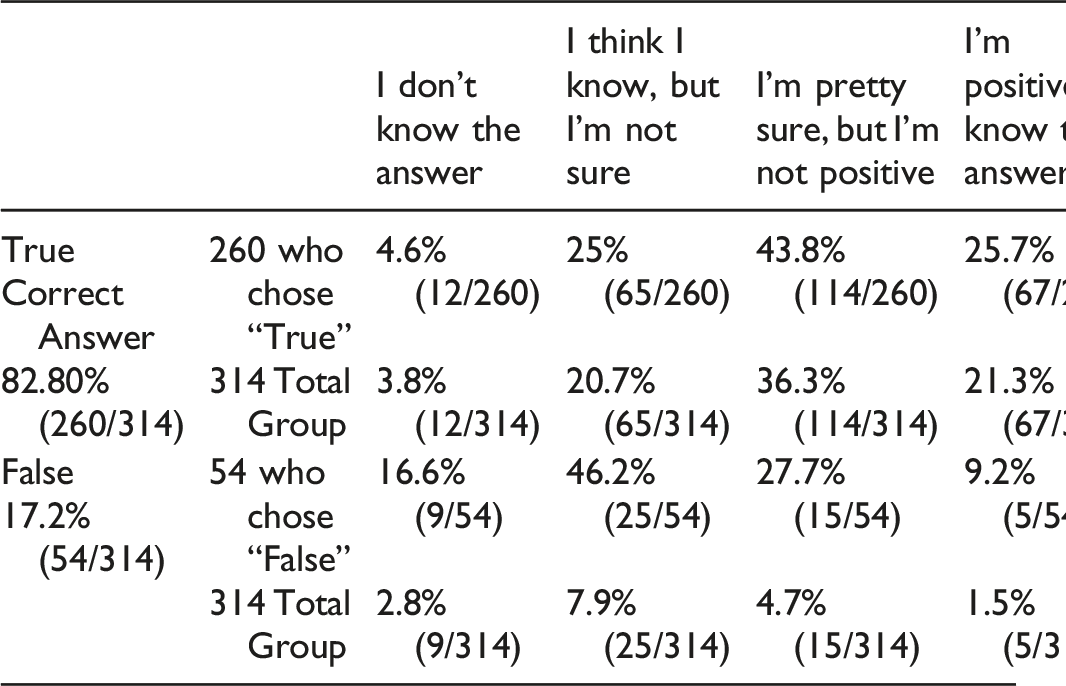
Of the 314 participants who answered this question, 82.80% (260/314 answers) correctly answered that it was true and 17.2% (54/314) were incorrect. However, only 67/314 (21.3%) of the total respondents got the question right and were positive about the answer. Of those who answered incorrectly, 9.2% (5/54) were nevertheless positive they knew the answer.
Answer and Comments: This sentence is also true and 82.80% marked the correct answer. Brachial plexopathy has abnormal sensitive conduction in NCS.1,4,5 Radiculopathies have normal sensitive conduction (NCS).4,5 In patients with radiculopathy, nerve conduction studies typically are normal, and the electrodiagnosis is established with needle EMG.4,5 Although some motor abnormalities are occasionally seen in radiculopathy, the more important reason to perform nerve conduction studies is to exclude other conditions that may mimic radiculopathy, especially entrapment neuropathy and plexopathy.1,4,5
Question 5: Finding of fibrillation potential in several muscles innervated by different peripheral nerves (e.g., from musculocutaneous, axillary, and suprascapular nerves) is how one differentiates cervical radiculopathy from a single peripheral nerve injury True or False.
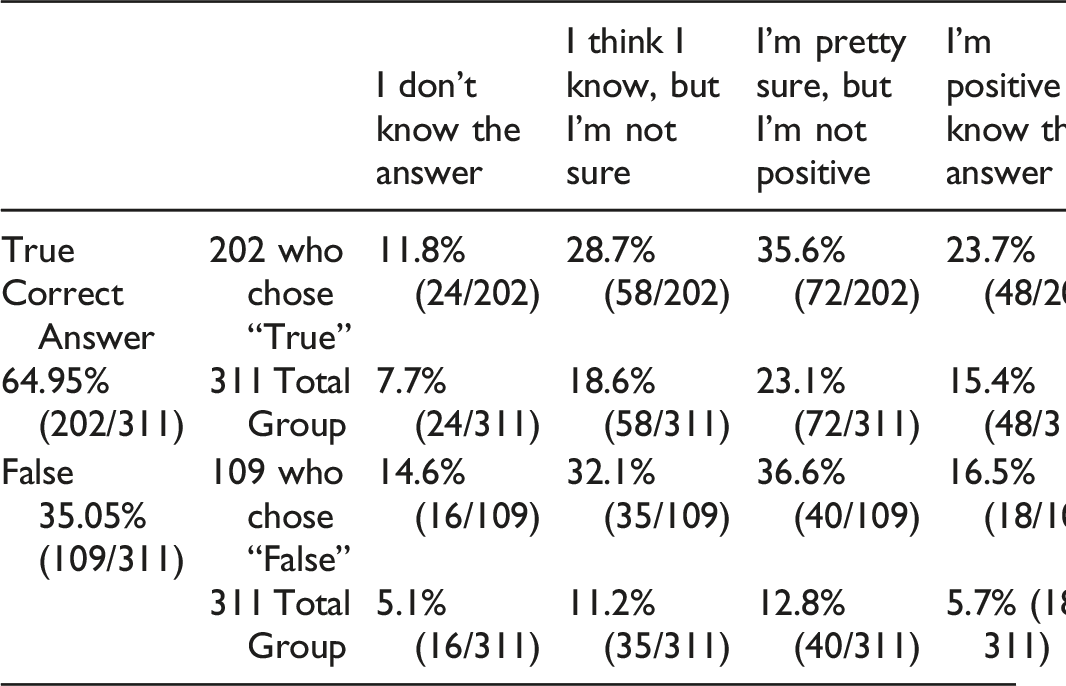
Of the 311 participants who answered this question, 64.95% (202/311) correctly answered that it was true and 35.05% (109/311) were incorrect. However, only 23.7% (48/202) of those who answered correctly were positive they knew the answer. Therefore, only 15.4% (48/311) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 16.5% (18/109) were nevertheless positive they knew the answer.
Answer and Comments: Finding of fibrillation potential in several muscles innervated by different peripheral nerves (e.g., from musculocutaneous, axillary, and suprascapular nerves) is how one differentiates cervical radiculopathy from a single peripheral nerve injury.1,3-5 Answer: True.
Question 4: EMG-NCS are a reliable way to differentiate between a C8 and T1 isolated radiculopathy? True or False.
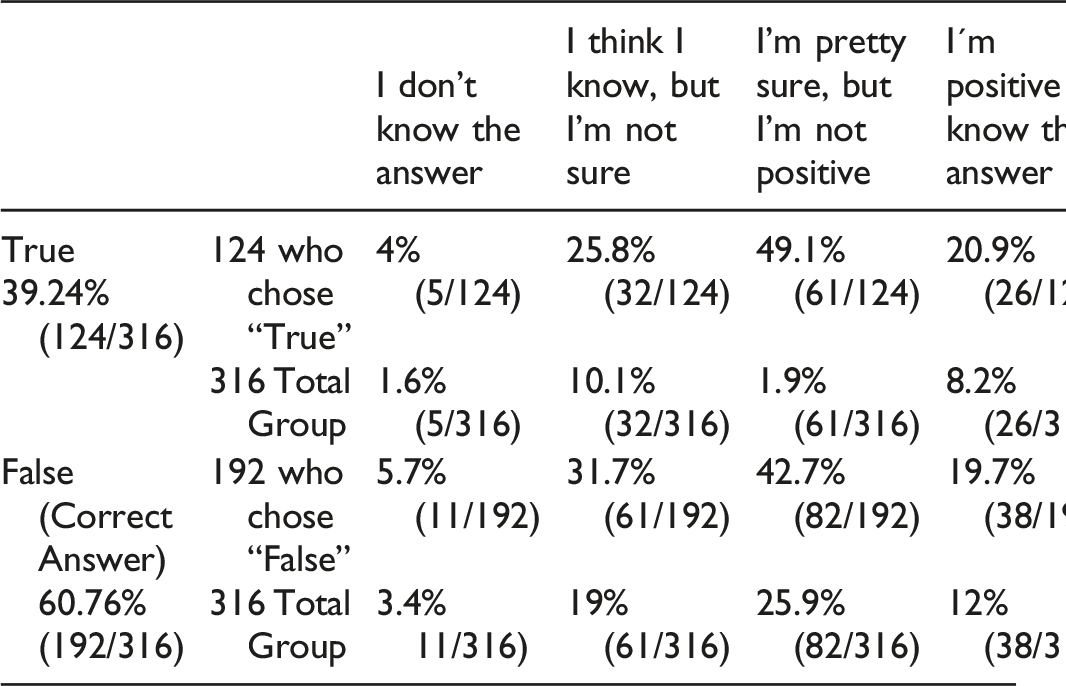
Of the 316 participants who answered this question, 60.76% (192/316) correctly answered that it was false and 39.24% (124/316) were incorrect. However, only 19.7% (38/192) of those who answered correctly were positive they knew the answer. Therefore, only 12.0% (38/316) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 20.9% (26/124) were nevertheless positive they knew the answer.
Answers for Questions 3 and 4 and Comment: Both are false. EMG-NCS cannot reliably differentiate a C5 from a C6 isolated radiculopathy, nor a C8 from T1, in the vast majority of the cases.1,3-6 To diagnose radiculopathy in the needle study, one must evaluate muscles from different nerves, but from the same myotome.1,4,5 Thus, to differentiate C5 from a C6 radiculopathy, the electromyographer must evaluate the biceps brachii (C5-C6) and the pronator teres (C6).1,4,5 To differentiate C8 from a T1 radiculopathy, one must study the intrinsic hand muscles (C8-T1) and the forearm (mostly C8).1,4,5 However, it is not easy to differentiate. EMG-NCS is not always able to differentiate isolated radiculopathies, involving only one root, as muscles are innervated by more than one myotome. Although the EMG-NCS study is a sensitive test for identifying radiculopathy, it may still be difficult to identify the specific segmental level, because most muscles are innervated by more than one myotome.1,4,5 For instance, the finding of fibrillation potentials with decreased recruitment of MUAPs (motor unit action potential) in the biceps, deltoid, infraspinatus, and mid-cervical paraspinal muscles is consistent with a C5–C6 myotomal pattern. In such a case, one can be certain that the lesion is not due to a single peripheral nerve injury because abnormalities are present in muscles innervated by the dorsal rami as well as by the musculocutaneous, axillary, and suprascapular nerves. However, it is more challenging and sometimes impossible to differentiate between a C5 and C6 radiculopathy. One would next sample muscles that belong to one but not the other myotome. For example, it would be helpful to sample muscles with partial C5 but without C6 innervation, as well as muscles with partial C6 but without C5 innervation. For instance, if the rhomboids (C4–C5) were sampled and found to be normal while the pronator teres (C6–C7) showed fibrillation potentials, then a C6 lesion would be more likely than a C5 lesion. The same approach is used to identify radiculopathies at other levels. One can see that it is just as important to identify which muscles are normal as which are abnormal to try to identify the specific root level involved. Often, multiple muscles must be sampled to try to define the level of the involved myotome.
In studies of patients who had a surgically defined single-level radiculopathy, the correct level often could be deduced from extensive needle EMG. However, not infrequently, there is significant overlap between adjacent segments, making a single root localization difficult. The most difficult level to differentiate is C6 from C7.1,3
Question 3: EMG-NCS are a reliable way to differentiate between a C5 and C6 isolated radiculopathy? True or False.
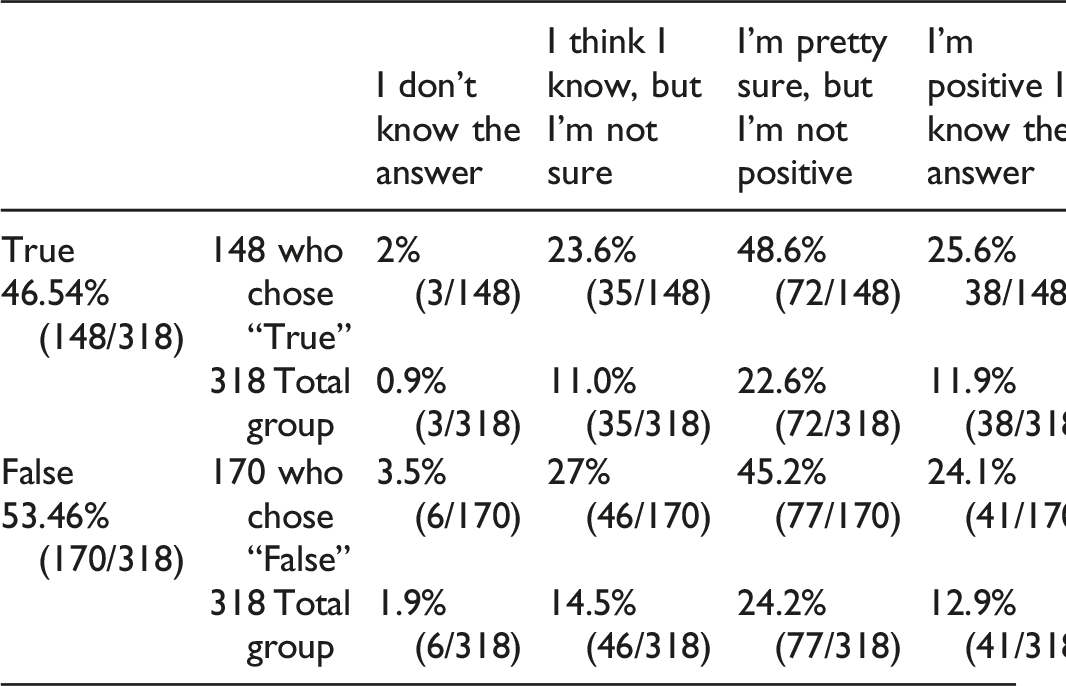
From 318 participants who answered this question, 53.46% (170/318) correctly answered that this was false, whereas 46.54% (148/318) incorrectly answered that EMG-NCS were a reliable to differentiate between a C5 and C6 isolated radiculopathy. However, only 24.1% (41/170) of those who answered correctly were positive about the answer. Therefore, only 12.9% (41/318) of the total respondents got the question right and were positive about their answer. Another 24.2% got the answer correct and were “pretty sure but not positive.” Of those who answered incorrectly, 25.6% (38/148) were nevertheless positive they knew the answer and another 48.6% were incorrect but were “pretty sure but not positive” that they knew the answer.
See comments above with question 4.
Question 12—In the best electromyographer’s hands, what percentage of cases where a patient has definite radiculopathy will the EMG/NCS findings be completely normal (i.e., what is the % of false negative EMG/NCSs for radiculopathy)?
A) 5% B) 20% C) 40% D) 50%
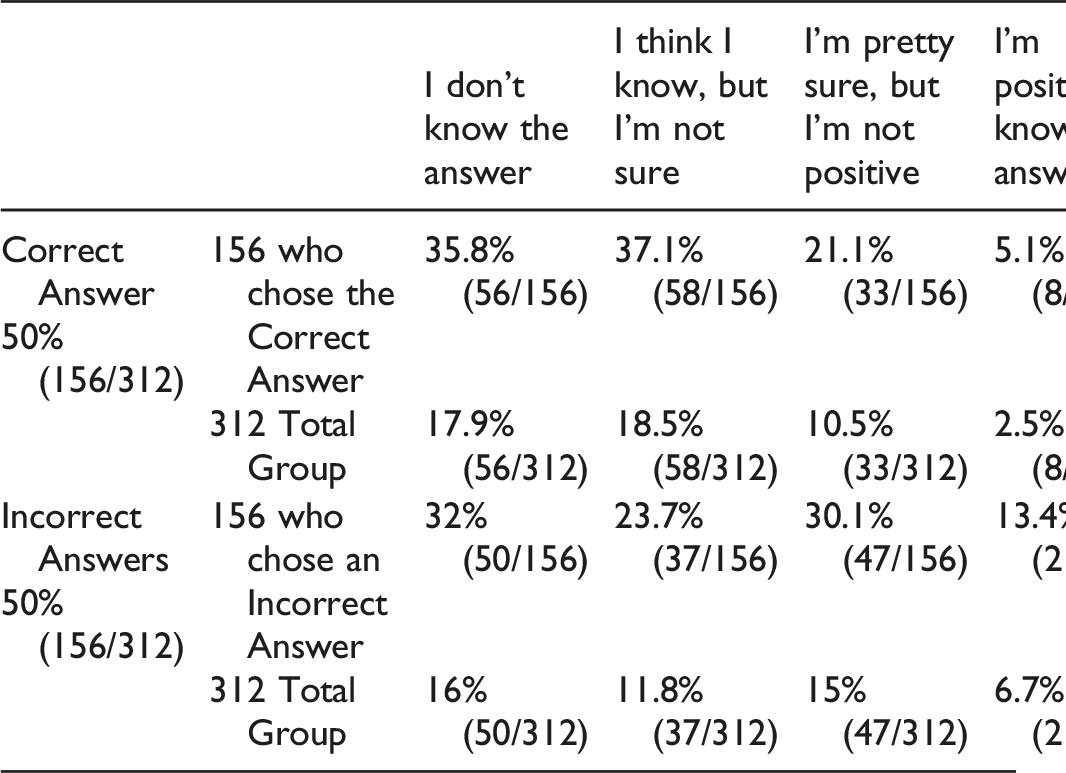
Of the 312 participants who answered this question, 50% (156/312) correctly answered that it was 20% and 50% (156/312) were incorrect. However, only 5.1% (8/156) of those who answered correctly were positive they knew the answer. Therefore, only 2.5% (8/312) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 13.4% (21/156) were nevertheless positive they knew the answer.
Answer and Comments of question 12 and 13: In the best of hands, the false negative rate is 20%, but the false positive rate is only 5%.5,7 However, some series reported lower rates of false negative for distal peripheral nerve diseases such as carpal and cubital tunnel syndrome.1,5,7 In the best of hands, it has been shown that the false negative rate is ∼20%. Therefore, even with a negative test, up to 20% can have a true radiculopathy. In the best of hands, it has been shown that the false positive rate is 5%. Therefore, with a positive test, 95% actually have a radiculopathy.
Question 9: A patient awakens from surgery with deltoid and biceps weakness. Assuming that this is due to a C5 palsy, in most cases, how long will it take for EMGs to reliably confirm injury to the nerve?
A) Within hours B) 1–3 days C) 4–7 days.
D) 1–2 weeks E) Several Weeks.
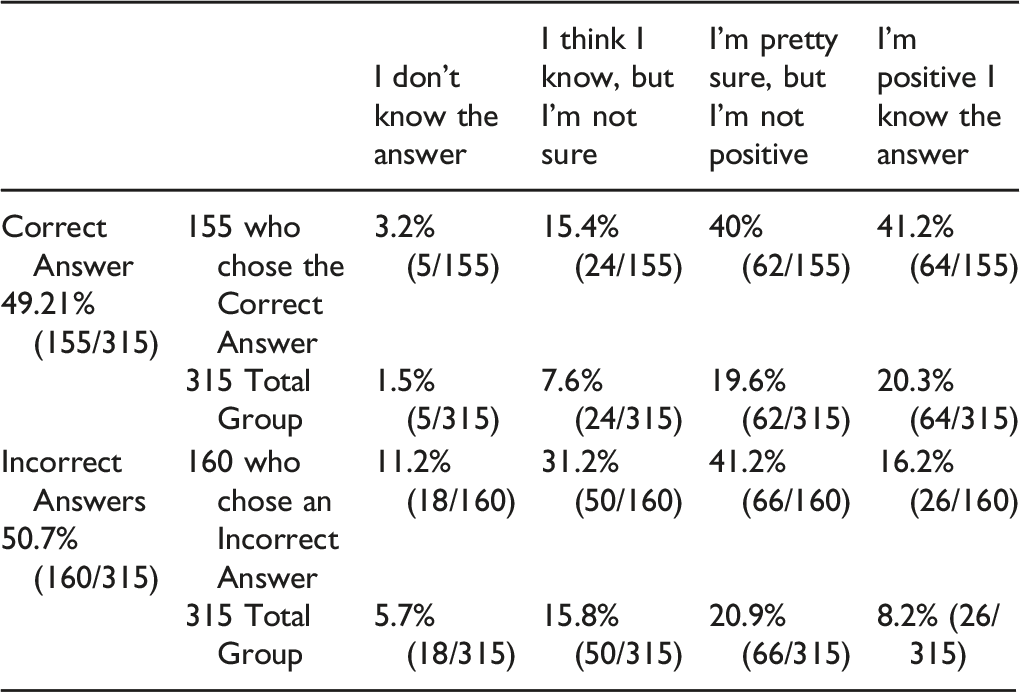
Of the 315 participants who answered this question, 49.21% (155/315) correctly answered that it takes several weeks and 50.7% (160/315) were incorrect. However, only 41.2% (64/155) of those who answered correctly were positive they knew the answer. Therefore, only 20.3% (64/315) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 26 of 160 (16.2%) were nevertheless positive they knew the answer.
Answer and Comments: Correct answer is several weeks. Between days 3 to 10, the process of Wallerian degeneration occurs: the nerve or root distal to the lesion undergoes degeneration, resulting in a low amplitude potential. The process of Wallerian degeneration is earlier for motor fibers (typically between days 3–5) compared to sensory fibers (typically between days 6–10). Once Wallerian degeneration is complete, the typical pattern of axonal loss will be seen on the exam. During the first 10 to 14 days after the onset of an acute radiculopathy, there are no needle EMG abnormalities except for decreased recruitment of MUAPs in weak muscles.1,3,6 Because it is unusual to find significant weakness in radiculopathy, the EMG study often is completely normal in the acute setting. Fibrillation potentials take several weeks to develop in the more distal limb muscles; therefore, it often is best to wait several weeks before sending a patient for an EMG study, unless one is willing to repeat a normal study after several weeks to look for new changes.1,5,6
Question 13—In the best electromyographer’s hands, what percentage of cases where the EMG/NCS diagnoses a radiculopathy does the patient not have radiculopathy (i.e., what is the % of false positive EMG/NCSs for radiculopathy)?
A) 5% B) 20% C) 40% D) 50%
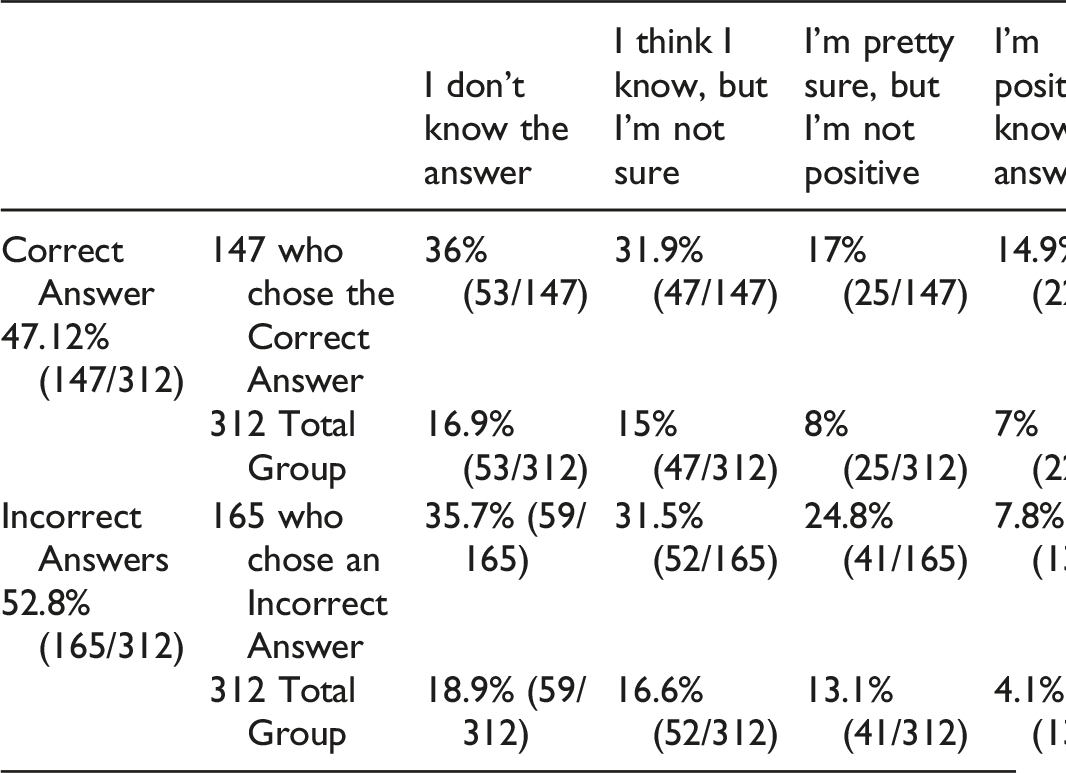
Of the 312 participants who answered this question, 47.12% (147/312) correctly answered that it was 5% and 52.8% (165/312) were incorrect. However, only 14.9% (22/147) of those who answered correctly were positive they knew the answer. Therefore, only 7% (22/312) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 7.8% (13/165) were nevertheless positive they knew the answer.
See comments above with question 12.
Question 11: A patient has had C3-7 total laminectomies. How will this affect EMG/NCS?
A) No affect
B) EMGs will not be useful since paraspinal analysis is the key to selecting the level.
C) EMGs may not be as sensitive, as paraspinal EMGs are usually abnormal post-op.
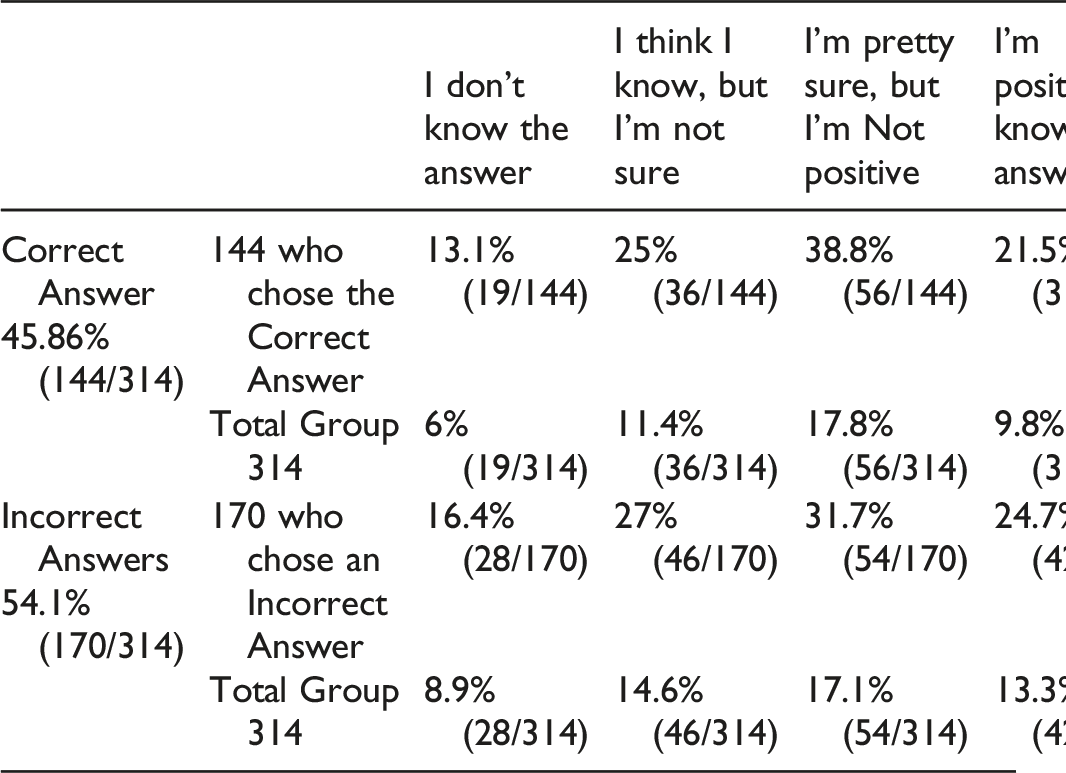
Of the 314 participants who answered this question, 45.86% (144/314) correctly answered that it may not be as sensitive and 54.1% (170/314) were incorrect. However, only 21.5% (31/144) of those who answered correctly were positive they knew the answer. Therefore, only 9.8% (31/314) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 24.7% (42/170) were nevertheless positive they knew the answer.
Answer and Comments: In this case, a needle study cannot be performed in the paraspinals, as the muscles will show signs of denervation (false positive). 1 In this case, there is no way to infer denervation due to cervical radiculopathy.4,5 EMG will be performed normally, but without the paraspinal analysis. Patients with recurrent or persistent pain after posterior spine surgery often are referred to the EMG laboratory. However, the interpretation of fibrillation potentials in the paraspinal muscles of such patients is not straightforward.
Patients who have undergone successful posterior spine surgery and no longer have symptoms or signs of radiculopathy have been demonstrated to have persistent fibrillation potentials in the paraspinal muscles, often for several years.2,6 It is not clear why this occurs, but it may be related to the surgical scar through the paraspinal muscles. For this reason, the paraspinal EMG examination no longer assumes the same diagnostic importance in postsurgical patients, and it is questionable whether sampling the paraspinals is worthwhile in such patients (i.e., the absence of denervation cannot exclude a radiculopathy, and the presence of denervation may be a “normal” finding many years after spinal surgery and is of no clinical significance). 6
Question 8: Can an EMG/NCS identify if a patient has a prefixed or post-fixed brachial plexus?
A) Yes, in most cases B) Sometimes C) No, never.
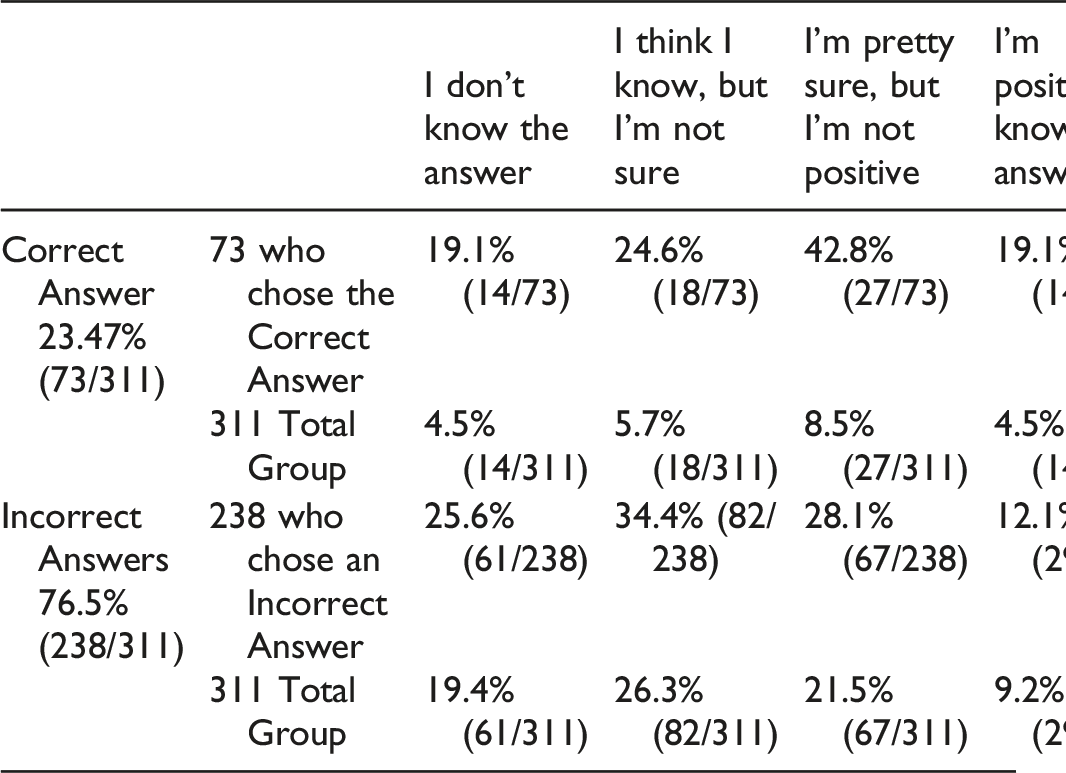
Of the 311 participants who answered this questions, 23.47% (73/311) correctly answered that this was false and 76.5% (238/311) were incorrect.
However, only 19.1% (14/73) of those who answered correctly were positive that they knew answer. Therefore, only 4.5% (14/311) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 12.1% (29/238) were nevertheless positive they knew the answer.
Answer and Comments: It is not possible to identify if the plexus is pre or post-fixed.1,4 Only 23.47% of the participants marked the correct answer. EMG tells us nothing about what a given patient’s anatomy is like. It relies on an abnormal finding with a muscle, for example, deltoid. We then assume that the deltoid is a C5 myotome but there is no way to know if in any given individual, the C4 root contributes (prefixed brachial plexus). So an EMG/NCS gives no information about the presence of a prefixed or post-fixed brachial plexus.
Question 10: Which of the following can be diagnosed with EMG/NCS? (a) myelopathy; (b) MS; (c) ALS; (d) all the above; (e) B and C only; (f) A and B only; (g) A and C only.
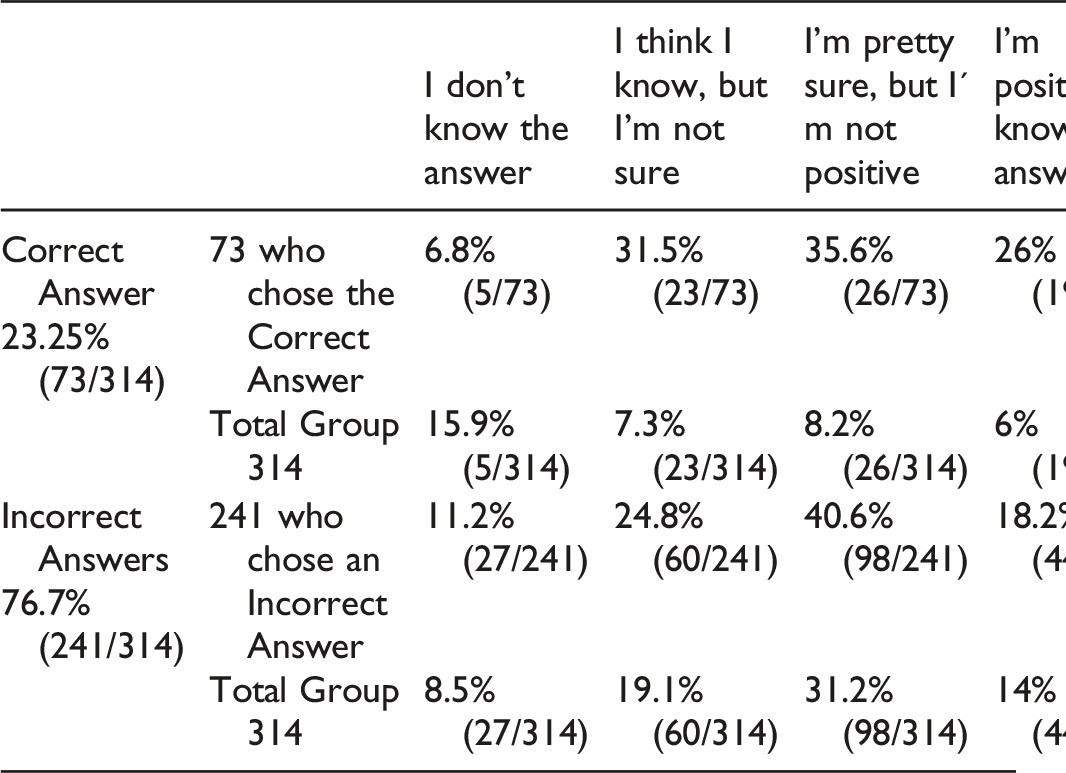
Of the 314 participants who answered this question, 23.25% (73/314) correctly answered that it was only ALS and 76.7% (241/314) were incorrect. However, only 26% (19/73) of those who answered correctly were positive they knew the answer. Therefore, only 6% (19/314) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 18.2% (44/241) were nevertheless positive they knew the answer.
Answer and Comments: Only ALS can be diagnosed in some cases. EMGs cannot diagnose myelopathy.7-9 Needle examination can only infer injury to the central nervous system by reducing activation.7-9 Multiple Sclerosis (MS) is a pathology of the central nervous system (CNS), so EMG is normal. ALS affects motor neurons so EMGs can look identical to a radiculopathy in the early stages. However, as ALS progresses, it will begin to affect multiple myotomes and in different limbs.1,7-9
Multiple Sclerosis (MS) is a pathology of the central nervous system (CNS), so EMG is normal. 1 Amyotrophic Lateral Sclerosis (ALS) is an axonal pathology. 10 Unfortunately, it is not possible to differentiate ALS and radiculopathy, as both have normal sensitive conduction. Only in forms of ALS with bulbar involvement, EMG is able to confirm the diagnosis. 10 If the nerve root is compressed, resulting in demyelination without axonal loss, the needle EMG study may be completely normal.
Diagnosing radiculopathy with EMG usually rests on the identification of denervation and reinnervation, signs of axonal loss. If there is no axonal loss, the study usually is normal. Only if demyelination results in significant conduction block, with accompanying weakness, will MUAP recruitment be diminished. This situation, however, is rarely seen in radiculopathy. Although EMG cannot differentiate between a disorder of the nerve roots and a disorder of the motor neurons, there are clear and unequivocal clinical differences that allow the distinction to be made.
For example, there likely would be no difference between the EMG of a patient with motor neuron disease, such as ALS, and that of a patient with malignant lymphoma diffusely infiltrating multiple nerve roots and cranial nerves. The F responses (one of several motor responses which may follow the direct motor response evoked by electrical stimulation of peripheral motor nerves) might be abnormal in polyradiculopathy, in contrast to motor neuron disease, but otherwise the studies could be identical (normal SNAPs, diffuse denervation and reinnervation). 5 However, the clinical presentation and neurologic examination certainly would be markedly different. In motor neuron disease, there are no sensory signs or symptoms.
In contrast, pain and paresthesias are prominent in polyradiculopathy. Deep tendon reflexes usually are depressed or absent in polyradiculopathy, whereas they are increased or present in ALS (although they may be depressed in the progressive muscular atrophy variant of ALS). These points once again underscore that EMG and nerve conduction studies can be properly interpreted only in the context of the clinical history and physical examination. 1
Question 7—A patient has a C5-6 herniated nucleus pulposus and very dense numbness in the C6 dermatome without any weakness. The most likely findings on EMG and NCS are.
A) Abnormal EMG and normal NCS B) Normal EMG and abnormal NCS.
C) Abnormal EMG and NCS D) Normal EMG and NCS.
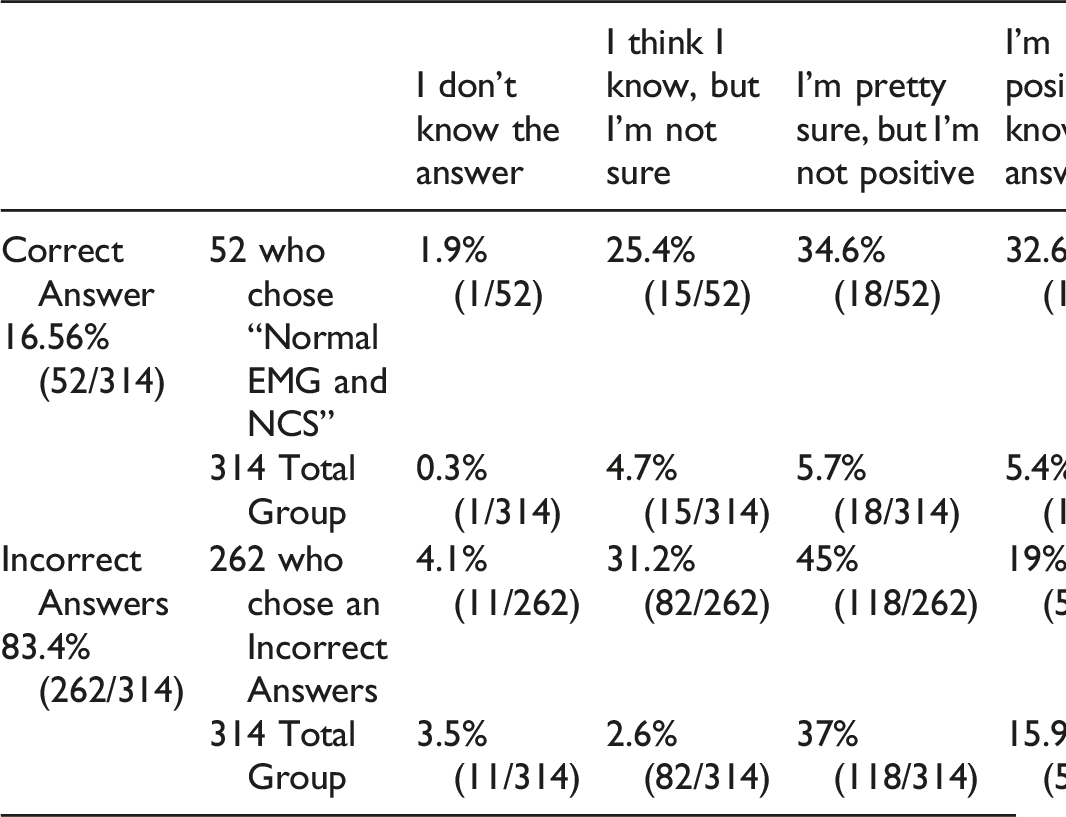
Of the 314 participants who answered this question, 16.56% (52/314) correctly answered and 83.4% (262/314) were incorrect. However, only 32.6% (17/52) of those who answered correctly were positive they knew the answer. Therefore, only 5.4% (17/314) of the total respondents got the question right and were positive about their answer. Of those who answered incorrectly, 50 of 262 (19%) were nevertheless positive they knew the answer.
Answer and Comments: The correct answer is most likely a Normal EMG and Normal NCS. Only 16.56% marked the proper answer. If a patient only has radicular numbness and pain and no motor deficits, NCS will be negative, since NCS only examines the status of peripheral nerve dysfunction.1,5 EMGs also will likely be negative, if there is no motor root involvement. Therefore, a “normal” EMG-NCS in a patient with numbness with no motor deficits suggests a cervical etiology. Radiculopathies are preganglionic diseases, so they do not alter sensory conduction. Most patients with radiculopathy have prominent sensory symptoms, including pain and parasthesias, indicating dysfunction of the sensory nerve root. If the sensory nerve root is preferentially affected and the motor nerve root is spared, the EMG study will be normal.1,5
Unfortunately, there is no good way to assess the proximal sensory segments using routine nerve conduction studies. Somatosensory evoked potentials are often used to assess the proximal segments, but they share many of the limitations of the F response (a late response that follows the motor response and is elicited by supramaximal electrical stimulation of a motor nerve).1,5 Most areas of skin are innervated by multiple dermatomes. Accordingly, although a single spinal nerve root may be severely damaged with resultant slowing, the somatosensory evoked latencies may be normal because the adjacent nerve roots (and the overlapping dermatomes they innervate) are not affected.1,5
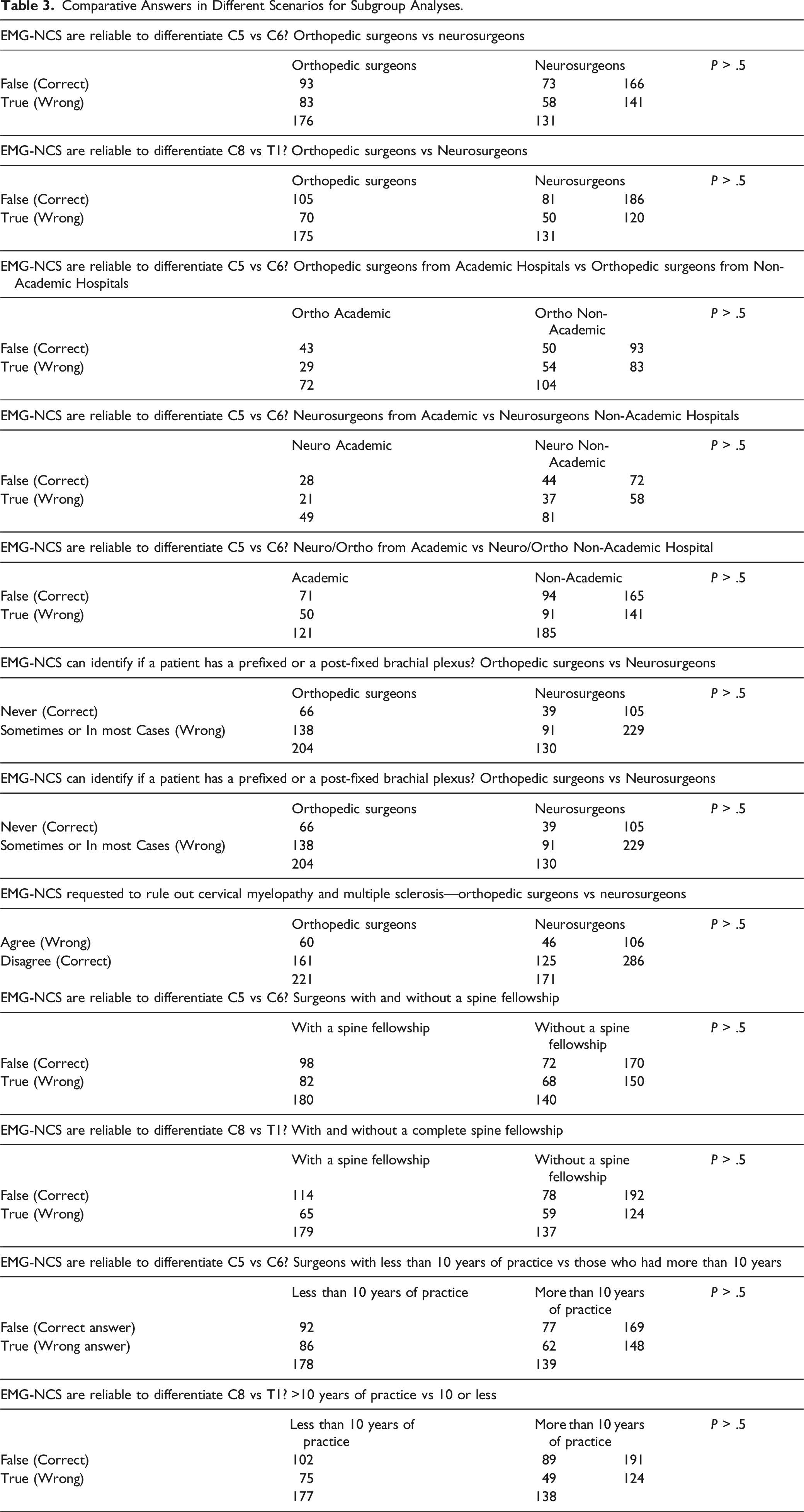
Comparative Answers in Different Scenarios for Subgroup Analyses.
Discussion
Electromyography (EMG) and nerve conduction studies (NCS) are important adjunct exams useful for evaluating the peripheral nervous system and neuromuscular abnormalities. They can be useful in diagnosing motor neuron diseases, compressive neuropathies, muscle disorders such as dystrophy or polymyositis, as well as radiculopathy.1,11,12 Despite the frequent use of EMG and NCS by spinal surgeons, there is no study evaluating how knowledgeable surgeons are about these procedures.
This international survey demonstrated that surgeons have relatively poor knowledge regarding the indications for and limitations and interpretation of these tests. Of the 11 questions regarding these tests, only 3 had a clear majority of respondents choosing the correct answer. These were: 82.8% for question 6 (EMG/NCS can differentiate between brachial plexopathy such as Parsonage Turner, also known as idiopathic brachial plexopathy and C5 palsy? Answer: True); 64.95% for question 5 (Finding of fibrillation potential in several muscles innervated by different peripheral nerves, for example, from musculocutaneous, axillary and suprascapular nerves, is how one differentiates cervical radiculopathy from a single peripheral nerve injury. Answer: True); 60.76% for question 4 (EMG-NCS are a reliable way to differentiate between a C8 and T1 isolated radiculopathy? Answer: False).
The responses to the rest of the questions suggest that surgeons need further education regarding EMG/NCS. Five questions had a close to 50% correct response rate. These were: 53.46% for question 3 (EMG-NCS are a reliable way to differentiate between a C5 and C6 isolated radiculopathy? Answer: False); 50% for question 12 (In the best electromyographer’s hands, what percentage of cases where a patient has definite radiculopathy will the EMG/NCS findings be completely normal; that is, what is the % of false negative EMG/NCSs for radiculopathy? Answer 20%); 49.21% for question 9 (A patient awakens from surgery with deltoid and biceps weakness. Assuming that this is due to a C5 palsy, in most cases, how long will it take for EMGs to reliably confirm injury to the nerve? Answer: several weeks); 47.12% for question 13 (In the best electromyographer’s hands, what percentage of cases where the EMG/NCS diagnoses a radiculopathy does the patient not have radiculopathy; that is, what is the % of false positive EMG/NCSs for radiculopathy? Answer: 5%); 45.86% for question 11 (A patient has had C3-7 total laminectomies. How will this affect EMG/NCS? Answer: EMGs may not be as sensitive, as paraspinal EMGs are usually abnormal post-op).
Three questions were missed by the vast majority of the respondents. These were: 23.47% for question 8 (Can an EMG/NCS identify if a patient has a prefixed or post-fixed brachial plexus? Answer: No, never); 23.35% for question 10 (Which of the following can be diagnosed with EMG/NCS? (a) myelopathy; (b) MS; (c) ALS; (d) all the above; (e) B and C only; (f) A and B only; (g) A and C only. Answer: ALS); 16.56% for question 7 (A patient has a C5-6 herniated nucleus pulposus and very dense numbness in the C6 dermatome without any weakness. The most likely findings on EMG and NCS are. Answer: Normal EMG and normal NCS).
While the above numbers are bad enough, the reality is likely to be even worse, in terms of surgeons’ knowledge regarding electrodiagnostic tests. For each question, respondents were also asked how positive they were about their answers, in order to determine if they were guessing or knew the answers. If we look at the percentage of answers that were correct where the respondent was positive that they knew the answer, no question even reaches the 25% threshold. From highest to lowest percentage, these were: 21.3% (question 6), 20.3% (question 9), 15.4% (question 5), 12.9% (question 3), 12% (question 4), 9.8% (question 11), 7% (question 13), 6% (question 10), 5.4% (question 7), 4.5% (question 8), 2.5% (question 12).
One question that also deserves specific comment has to do with the diagnostic capability of EMG-NCS (Question 10: Which of the following can be diagnosed with EMG/NCS? (a) myelopathy; (b) MS; (c) ALS; (d) all the above; (e) B and C only; (f) A and B only; (g) A and C only. Answer: ALS). A high percentage of surgeons (more than 75%) answered this question incorrectly. Neither multiple sclerosis nor cervical myelopathy can be diagnosed with EMG-NCS. The lack of knowledge regarding the appropriate indications for EMG-NCS may result in unnecessary tests that increase the cost of health care or cause unnecessary delay in proper diagnosis of the patient’s condition.
An interesting finding of our study is that no demographic group scored better than any other group: neurosurgeons vs orthopedic surgeons, years of practice or even the fact of having completed a spinal fellowship. This suggests that education regarding EMG-NCS for cervical conditions is necessary for all spine surgeons, regardless of their specialty, fellowship-training status, years in practice or degree of experience.
Limitations
This study is limited by its design: a small number of survey respondents, comprehension by some non-English speaking surgeons, respondents’ fatigue with answering questions towards the end of the survey, and, finally, clinically relevant questions formulated by one spine surgeon and answered by one neurophysiologist.
Despite these limitations, we believe that this paper provides useful and practical information for spine surgeons utilizing many different scenarios to better understand and utilize EMG and NCS. Given that no question scored higher than 25% correct where the respondents were positive about their answers, we believe that this study has the potential to educate surgeons about the indications for and limitations and benefits of EMG and NCS.
Conclusions
EMG and NCS are powerful tools for excluding compressive entrapments and brachial plexopathies from cervical radiculopathies. However, they have very limited ability to diagnose mild cervical radiculopathies with only sensory findings, as well as other central nervous system diseases such as cervical myelopathy and multiple sclerosis. EMG are also poor in identifying the exact site of cervical compression, which requires supplementary radiological and clinical evaluation.
Finally, specific programs designed to educate surgeons about the limitations and utility of EMG/NCS in clinical practice are necessary, as demonstrated by this survey.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
“This survey was organized and funded by AO Spine. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization.”