
Abstract
Study Design
Retrospective study.
Objective
This retrospective study primary focus is to investigate the relationship between the C-VBQ score and the occurrence of postoperative zero-profile anchored spacer (ROI-C) interbody fusion cage subsidence. Additionally, we aim to evaluate the predictive efficacy of the C-VBQ scoring system for subsidence in the context of ACDF with the ROI-C.
Methods
Patients who underwent ACDF with the ROI-C cage at our hospital between January 2016 and December 2022 were included in this study. Univariate analysis and multivariate logistic regression were employed to identify independent risk factors associated with ROI-C cage subsidence after ACDF. Pearson correlation analysis was utilized to assess the correlation between the C-VBQ score and the height of ROI-C cage subsidence.
Results
A total of 102 patients underwent ACDF with ROI-C in our hospital were included in this study. Univariate analysis showed that age (P = 0.021) and C-VBQ score (P < 0.001) were the influencing factors of cage subsidence. Pearson correlation analysis showed that there was a significant positive correlation between the subsidence height of ROI-C cage and C-VBQ (r = 0.55, P < 0.01). Multivariate binary logistic regression analysis showed that C-VBQ score was the only variable that could significantly predict the subsidence of ROI-C cage after ACDF. Higher C-VBQ score was significantly associated with cage subsidence (P < 0.001).The AUC was 0.89, and the cutoff value for C-VBQ was 2.70.
Conclusion
The findings indicate a significant correlation between a higher C-VBQ score before surgery and ROI-C cage subsidence after ACDF. The preoperative assessment of C-VBQ proves valuable for clinicians, enabling them to identify patients with low bone mineral density and predict the risk of zero-profile anchored spacer interbody fusion cage subsidence following ACDF.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) serves as an effective procedure for alleviating spinal cord compression and restoring the physiological curvature of the cervical spine. It has now become the standard surgical approach for treating cervical spine degenerative diseases.1-3 The interbody fusion cage combined with a titanium plate internal fixation system remains the classic and preferred method for ACDF in clinical practice. This approach effectively enhances the stability of fusion segments, contributing to an improved interbody fusion rate. However, with medium and long-term follow-up, it has been observed that this method may lead to surgery-related complications. These complications include loosening of screws or the titanium plate, injury to the anterior cervical soft tissue, hematoma formation, and postoperative issues such as hoarseness and dysphagia.4-7 Additionally, the use of titanium plates is associated with an increased risk of adjacent segment degeneration (ASD).8,9 In response to these concerns, the zero-profile anchored spacer (ROI-C) interbody fusion cage was created. This innovative approach primarily involves a fusion device crafted from polyether ether ketone (PEEK) material and 2 curved titanium wedge pieces.10,11 Through the implantation of 2 titanium inserts in the upper and lower adjacent vertebrae, the fusion cage is securely anchored within the intervertebral space, effectively minimizing the risk of movement. In contrast to traditional titanium plate fixation surgeries, the zero-profile anchored spacer (ROI-C) interbody fusion cage offers advantages such as a shorter operation time, a smaller exposure range, and a design that prevents the cage from protruding from the anterior edge of the vertebral body. This feature helps avoid interference with adjacent segments.12-14
In recent years, there has been a gradual increase in the utilization of zero-profile anchored spacer interbody fusion cages in cervical vertebra surgery. Despite achieving favorable clinical efficacy, the postoperative subsidence of interbody fusion cages has garnered attention from scholars both domestically and internationally.15,16 Studies have indicated that cage subsidence, internal fixation failure, and the development of pseudarthrosis following ACDF have emerged as primary reasons necessitating revision surgery.17-19 Fusion cage subsidence significantly influences clinical efficacy and biomechanics, leading to intervertebral height loss, cervical kyphosis, and, in severe cases, compression of the spinal cord with the recurrence of neurological symptoms.20-22 There are many factors that influence the cage subsidence after ACDF, and the severity of osteoporosis is 1 of the major factors.23,24 Therefore, it is particularly important to evaluate patients’ bone mineral density (BMD) before spinal surgery. In 2020, Ehresmand et al 25 introduced a novel Vertebral Bone Quality (VBQ) score based on MRI. Numerous clinical studies have since validated the significant correlation between the VBQ score and DXA T-score, as well as QCT BMD values. This scoring system proves effective in differentiating patients with bone loss from those with normal bone density.26-29
Currently, the majority of clinical studies on VBQ scores primarily focus on the lumbar spine. There are only 3 studys on C-VBQ score predicting cage subsidence after anterior cervical spine surgery. Soliman 30 found that patients with cage subsidence after ACDF had significantly higher C-VBQ score than patients without cage subsidence (2.83 ± 0.38 vs 2.22 ± 0.36). Li et al 31 found that a higher preoperative C-VBQ score was an independent risk factor for TMC subsidence after ACCF. Wang et al 32 found that the VBQ score was effective in predicting zero-profile cage subsidence after single-segment ACDF. The first 2 studies assessed the role of the C-VBQ score in predicting titanium cage subsidence after anterior cervical spine surgery. However, previous studies have shown that the subsidence rate varies between different materials of the cage. 33 Therefore, it is important to explore the prediction effect of C-VBQ score on the subsidence of different material cage after ACDF. We and Wang 32 all explored the role of the C-VBQ score in predicting zero-profile anchored spacer fusion cage subsidence after ACDF. Differently, our study is the first to assess the predictive role of the C-VBQ score on ROI-C cage subsidence after ACDF, and we considered the influence of different surgical segments on the cage subsidence. Exploring the predictive effect of C-VBQ score on different materials and different types of cage subsidence, which is helpful to improve the general applicability of C-VBQ score in clinic work. Therefore, this retrospective study, based on preoperative MRI, aimed to analyze the correlation between C-VBQ scores in patients undergoing ACDF with zero-profile anchored spacer (ROI-C) interbody fusion cage at our hospital and cage subsidence. Furthermore, the study evaluated the predictive value of C-VBQ scores for postoperative cage subsidence.
Methods
Inclusion and Exclusion Criteria
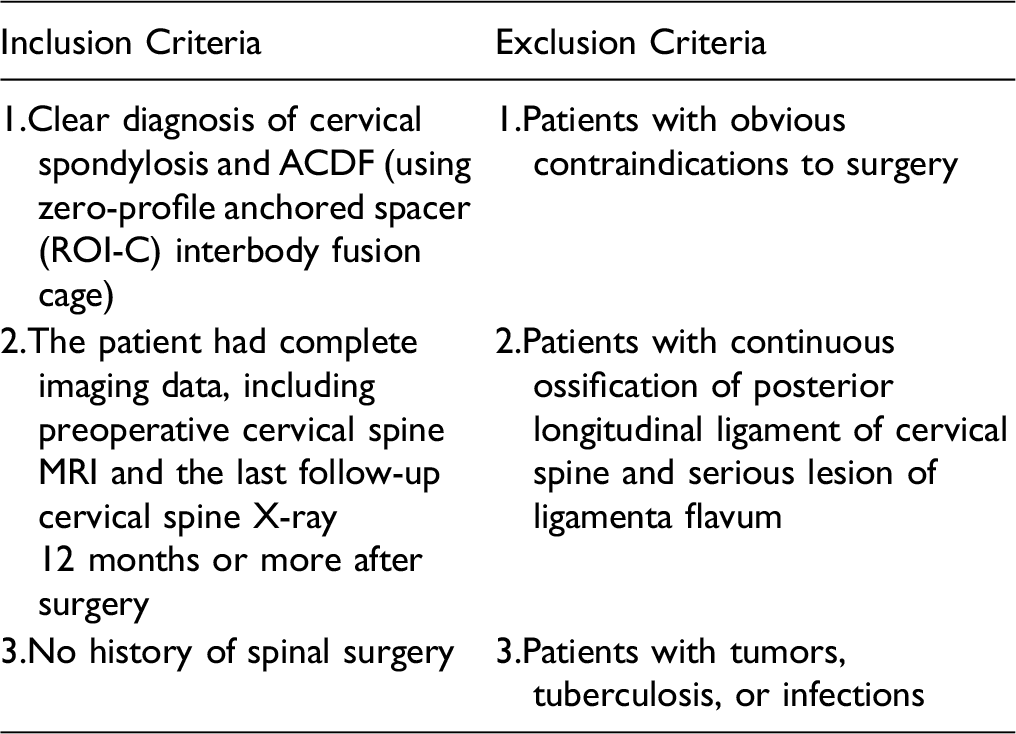
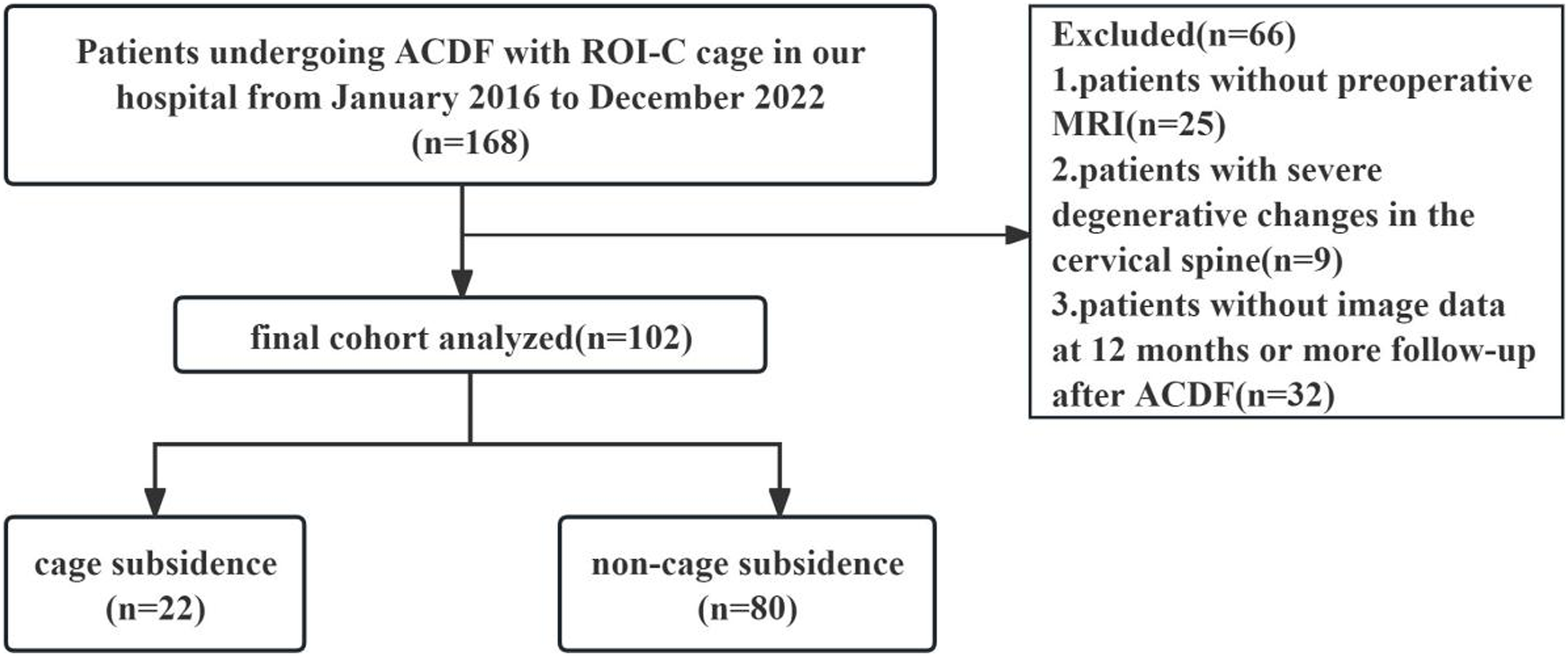
Flowchart of the inclusion of 102 patients in this study.
Clinical Data Collection
Collecting and summarizing clinical data of enrolled patients, including age, sex, body mass index, smoking history, and alcohol consumption history, diabetes and hypertension history, operation date, operation stage and follow-up time, etc. Preoperative scores of Visual Analogu Scale (VAS), Japanese Orthopaedic Association (JOA) and Neck Disability Index (NDI) were completed.
Cervical Vertebral Bone Quality (C-VBQ) Score Calculation
T1-weighted MRI images of patients’ cervical spine were selected in the PACS system. In the median sagittal position,the regions of interest (ROI) were placed within the medullary bone of the C3, C4, C5, and C6 vertebrae and in the cerebrospinal fluid portion of the C2 vertebrae. The mean signal intensity (SI) of C3-C6 vertebral and cerebrospinal fluid (CSF) at the C2 level were measured within the region of interest, and the C-VBQ score was calculated according to the formula. As shown in the figure, selecting cervical spine MRI T1-weighted images, in the mid-sagittal position, the SI of C3-C6 vertebral medullary bone and CSF in ROI was measured separately, C-VBQ score was calculated according to the formula. The C-VBQ score shown in this example is 1.99.

The VBQ scores were measured independently by 2 professional radiologists who were not associated with the patient’s treatment or the measurements. when the original scores of the 2 radiologists differed by more than 10%, the measurements were rerun by the third radiologist. 30 The final result is the mean value of the measurements obtained by the 2 physicians’ measurements.
Radiological Evaluation
Segment height (SH), that is, the distance between the midpoint of the upper endplate of the upper vertebra of the fusion segment and the midpoint of the lower endplate of the lower vertebra, was measured on neutral lateral plain radiographs of the patients within 1 week after surgery and at the last follow-up (Figure 3). Cage subsidence is defined as fusion segment height loss ≥3 mm, which has been fully verified in previous studies.
20
All imaging data were separately measured by 2 radiologists and then averaged. In median lateral X-ray,segment height was defined as the distance between the midpoint of superior endplate of the superior fused vertebral body and the midpoint of the inferior endplate of the inferior fused vertebral body. The SH as shown in this example was 28.74mm.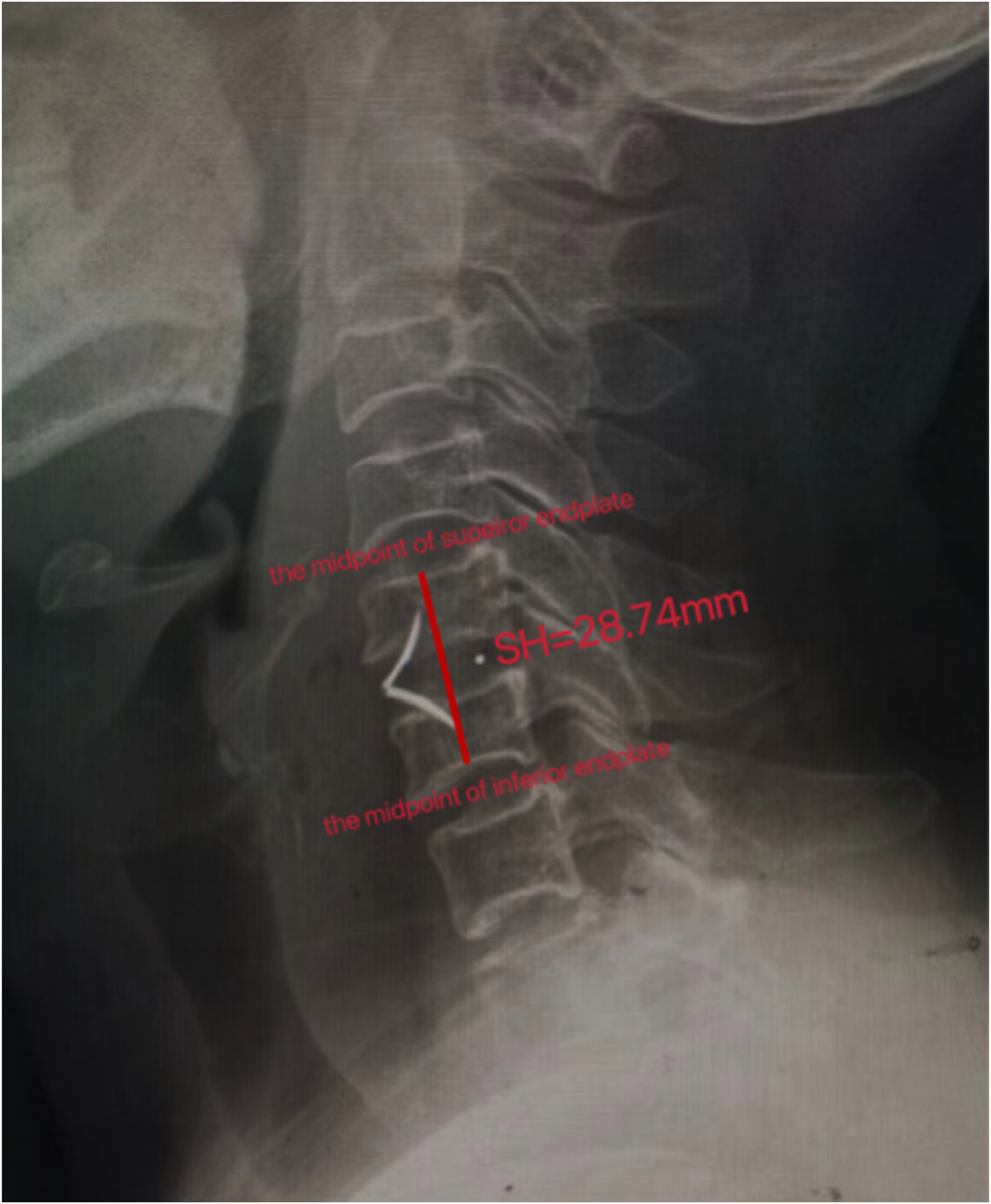
Data Analysis
SPSS 27.0 statistical software was used for analysis. All continuous variables in this study conformed to normal distribution and were expressed as Mean ± SD. And t test or rank sum test was used for univariate analysis. Categorical variables were reported as frequency and percentage, and single factor analysis was performed using Chi-square test or Fisher exact probability method. The variables with P < 0.05 in the univariate analysis were included in the multivariate analysis, and the multivariate analysis adopted Logistic regression model to screen the independent risk factors for the self-stabilizing cage subsidence. Pearson correlation analysis was used to determine the correlation between C-VBQ score and the subsidence height of the cage. Receiver operating characteristic curve (ROC) was plotted and Youden index was calculated to analyze the ability of C-VBQ score to predict the subsidence of ROI-C cage after ACDF. When P < 0.05, the difference was considered statistically significant.
Result
Clinical Demographic Data
A total of 102 patients were included in this retrospective study, including 45 males and 57 females. All patients ranged in age from 35 to 84 years, with an average age of 60.8 ± 10.42 years. There were 22 patients with cage subsidence after ACDF, the subsidence rate was 21.57%. The age of patients in the subsidence group was 65.36 ± 9.43, and the age of patients in the non-subsidence group was 59.63 ± 10.39, which had statistical significance (P = 0.02; Figure 4). Bar charts of age and C-VBQ scores of patients in subsidence group and non-subsidence group. *: p< 0.05. ***: p<0.001.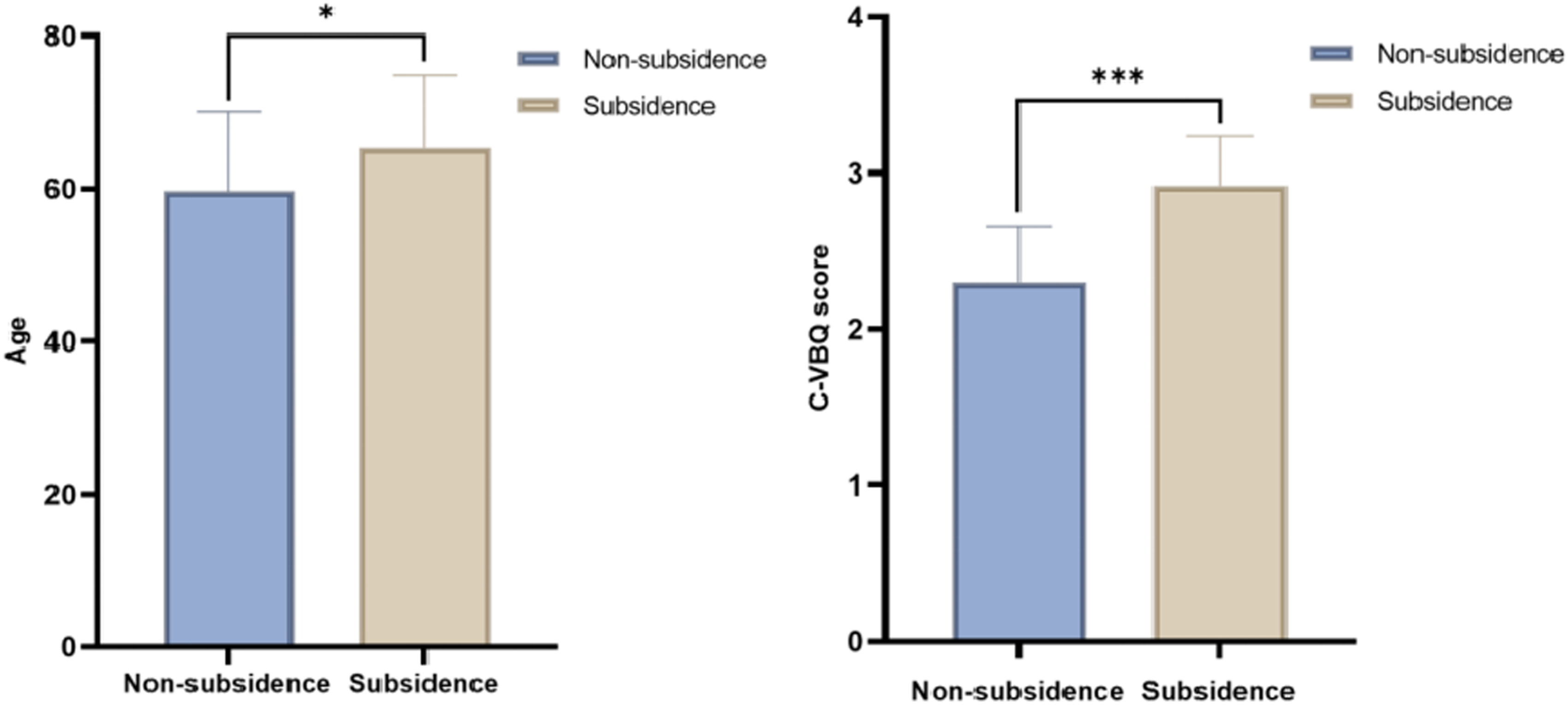
Basic Characteristics of Patients Undergoing ACDF With ROI-C Self-Stabilizing Cage.
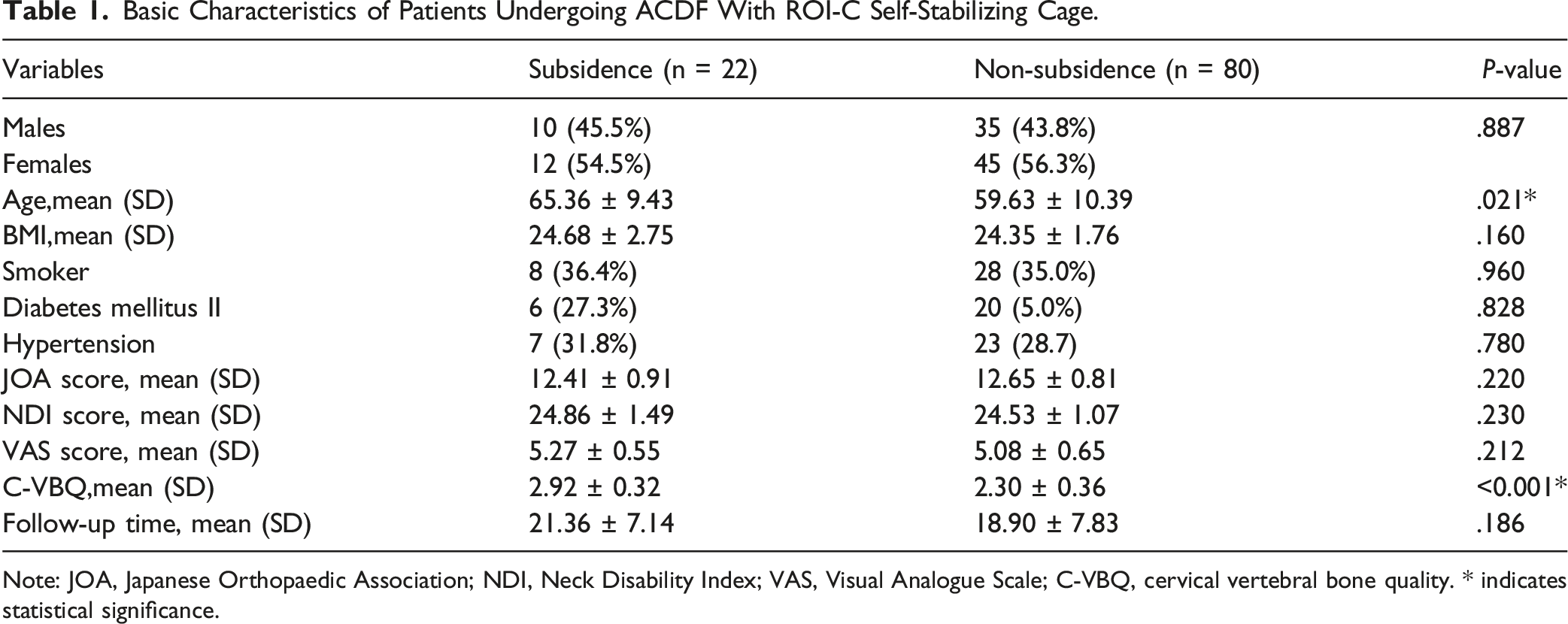
Note: JOA, Japanese Orthopaedic Association; NDI, Neck Disability Index; VAS, Visual Analogue Scale; C-VBQ, cervical vertebral bone quality. * indicates statistical significance.
Surgical Segment Distribution
Distribution of Surgical Segments in Patients.
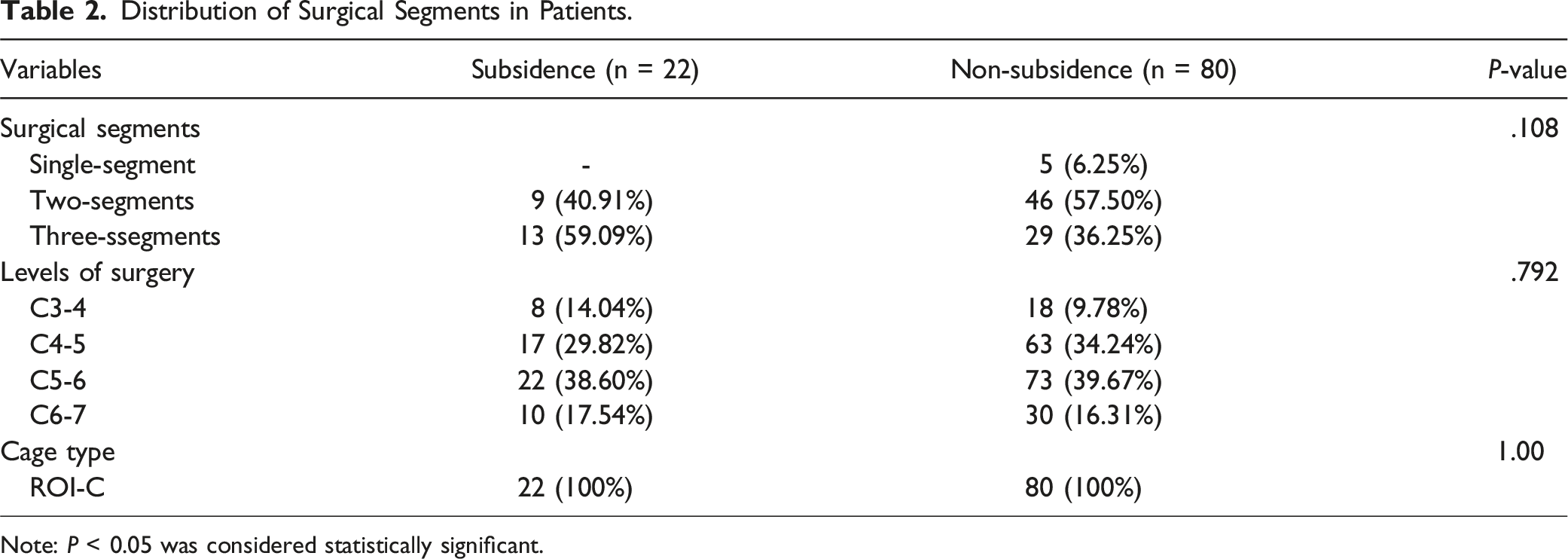
Note: P < 0.05 was considered statistically significant.
Imaging Parameters
Zero-profile anchored spacer (ROI-C) interbody fusion cage subsidence occurred in 22 patients enrolled in the study after ACDF, with segmental height loss of 3.66 ± 0.32 mm in the subsidence group and 1.89 ± 0.53 mm in the non-subsidence group. The C-VBQ score increased significantly from 2.30 ± 0.36 to 2.92 ± 0.32 (P < 0.001; Figure 4).
C-VBQ Score Predicts Zero-Profile Anchored Spacer (ROI-C) Interbody Fusion Cage Subsidence after ACDF
Binary Logistics Regression Analysis to Identify the Influence Factors of ROI-C Self-Stabilizing Cage Subsidence After ACDF.
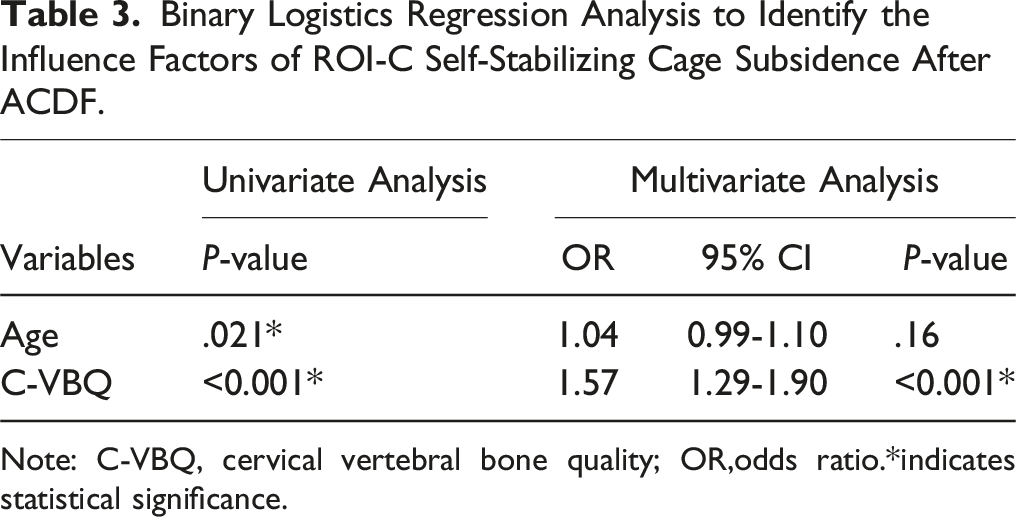
Note: C-VBQ, cervical vertebral bone quality; OR,odds ratio.*indicates statistical significance.
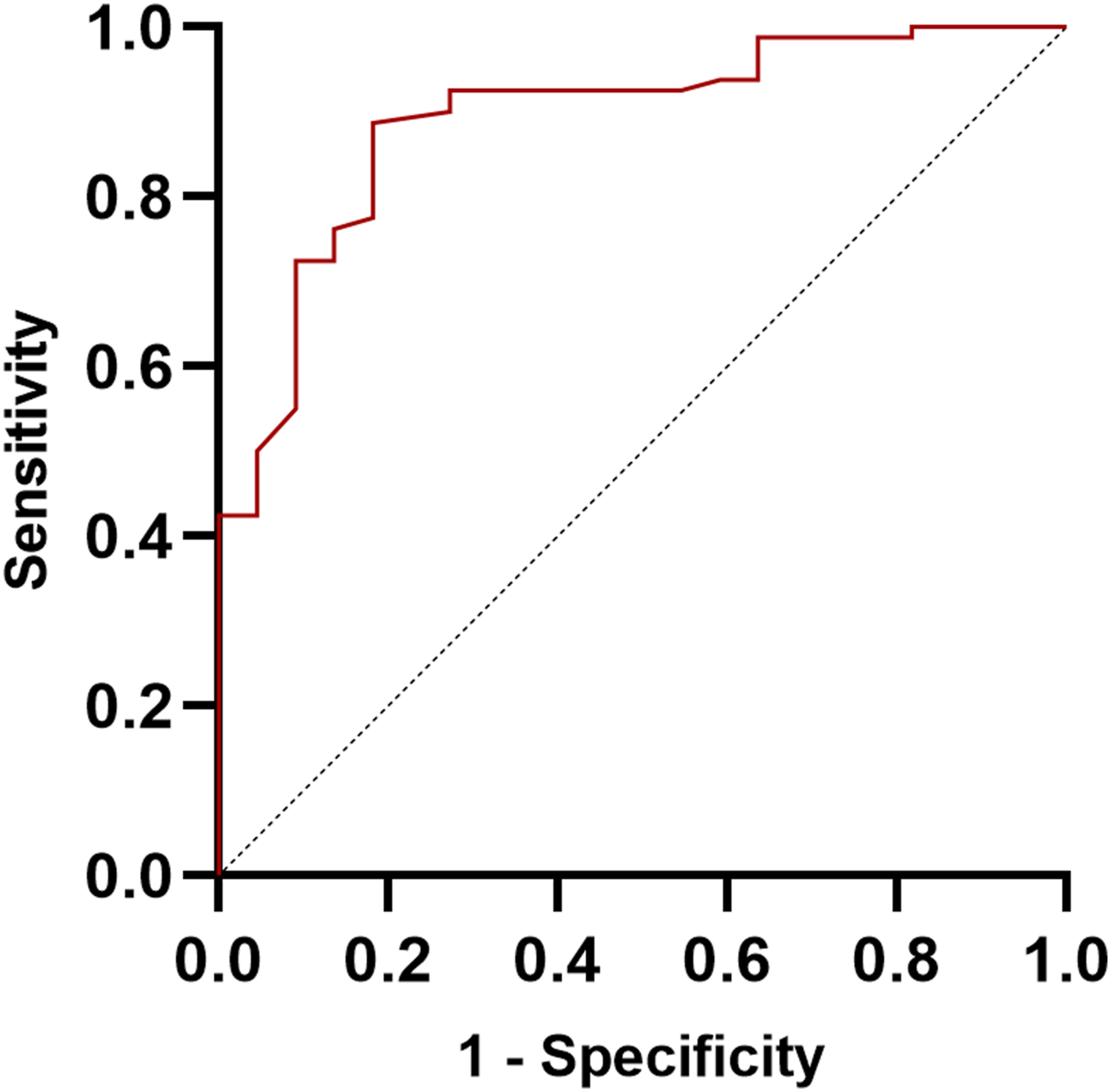
ROC curves of sensitivity and specificity for C-VBQ score in predicting ROI-C cage subsidence after ACDF. The AUC was 0.89.
Correlation Between C-VBQ and the Subsidence Height of Zero-Profile Anchored Spacer (ROI-C) Interbody Fusion Cage
Since C-VBQ score was the only significant predictor of ROI-C cage subsidence after ACDF, we performed linear regression on the correlation between C-VBQ score and subsidence height. Pearson correlation analysis showed that there was a significant positive correlation between the C-VBQ score and the subsidence height of the ROI-C cage after ACDF (r = 0.55, P < 0.001,95% CI 0.45-0.73; Figure 6). Pearson correlation plot of C-VBQ and ROI-C self-stabilizing cage segmental height loss after ACDF.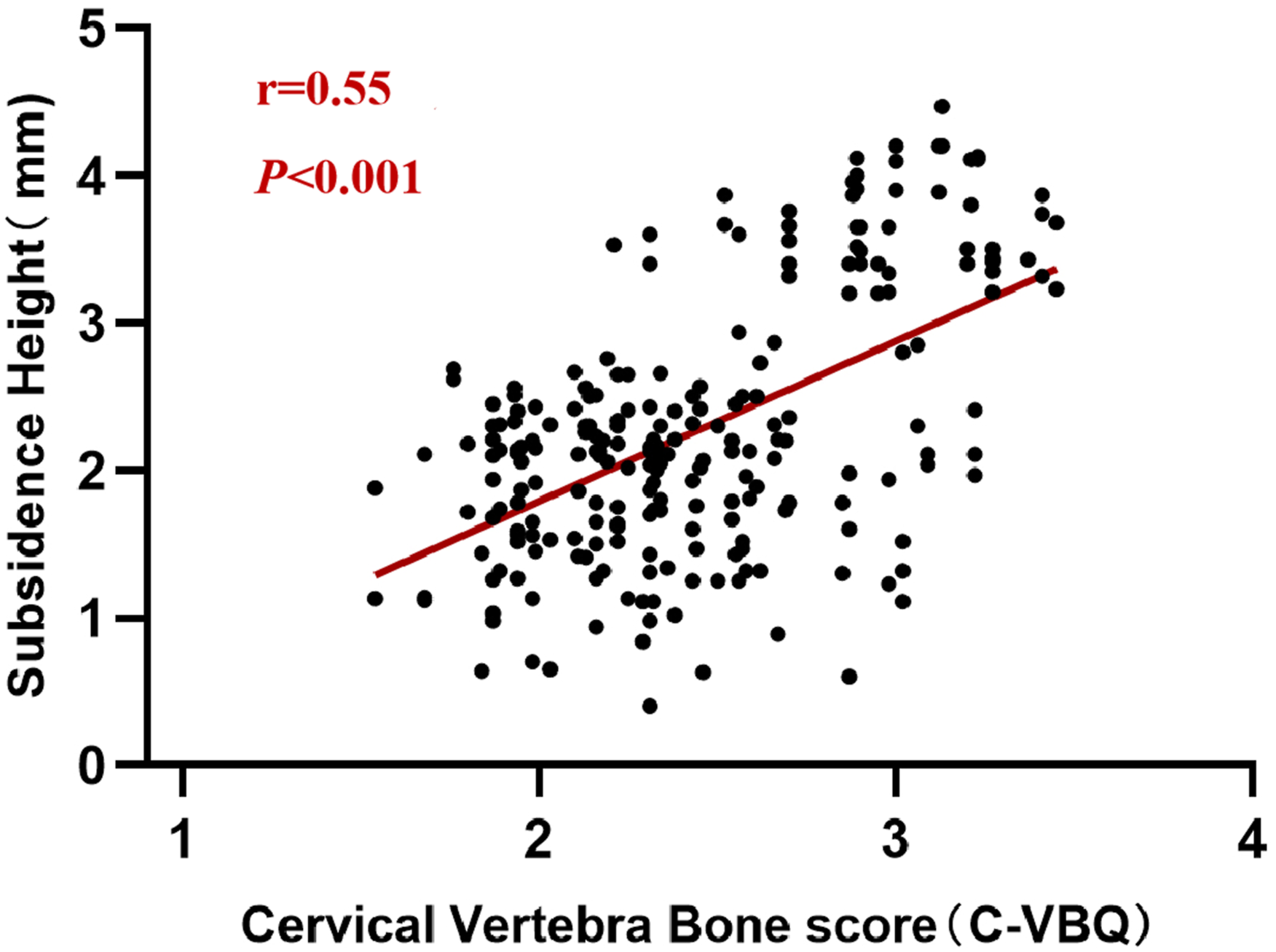
Typical Cases
Case 1: Bi XX, female, 69 years old, complained of “intermittent pain in the neck and shoulders with numbness in both upper limbs for 5 years.” The patient underwent C5/6 and C6/7 ACDF using zero-profile anchored spacer (ROI-C) interbody fusion cage under general anesthesia on 2019-11-15. The last follow-up time was 2021-04-13, and the imaging data of the patient were shown in Figure 7. 1a-1e: follow-up imaging data of Bi XX. 1a: postoperative C5/6 segment height 34.0mm; 1b: postoperative C6/7 segment height 34.5mm; 1c: C5/6 segment height 30.6mm at last follow-up; 1d: C6/7 segment height was 30.7mm at last follow-up. 1e: the VBQ score of the patient’s preoperative cervical spine MRI was 3.39. 2a-2g: follow-up imaging data of Zhao X. 2a: postoperative C4/5 level height 35.5mm; 2b: postoperative C5/6 segment height 34.3mm; 2c: postoperative C6/7 segment height 34.7mm; 2d: C4/5 segment height 31.4mm at the last follow-up; 2e: C5/6 segment height 29.4mm at last follow-up; 2f: C6/7 segment height was 30.7mm at last follow-up. 2g: the VBQ score of the patient's preoperative cervical spine MRI was 2.89.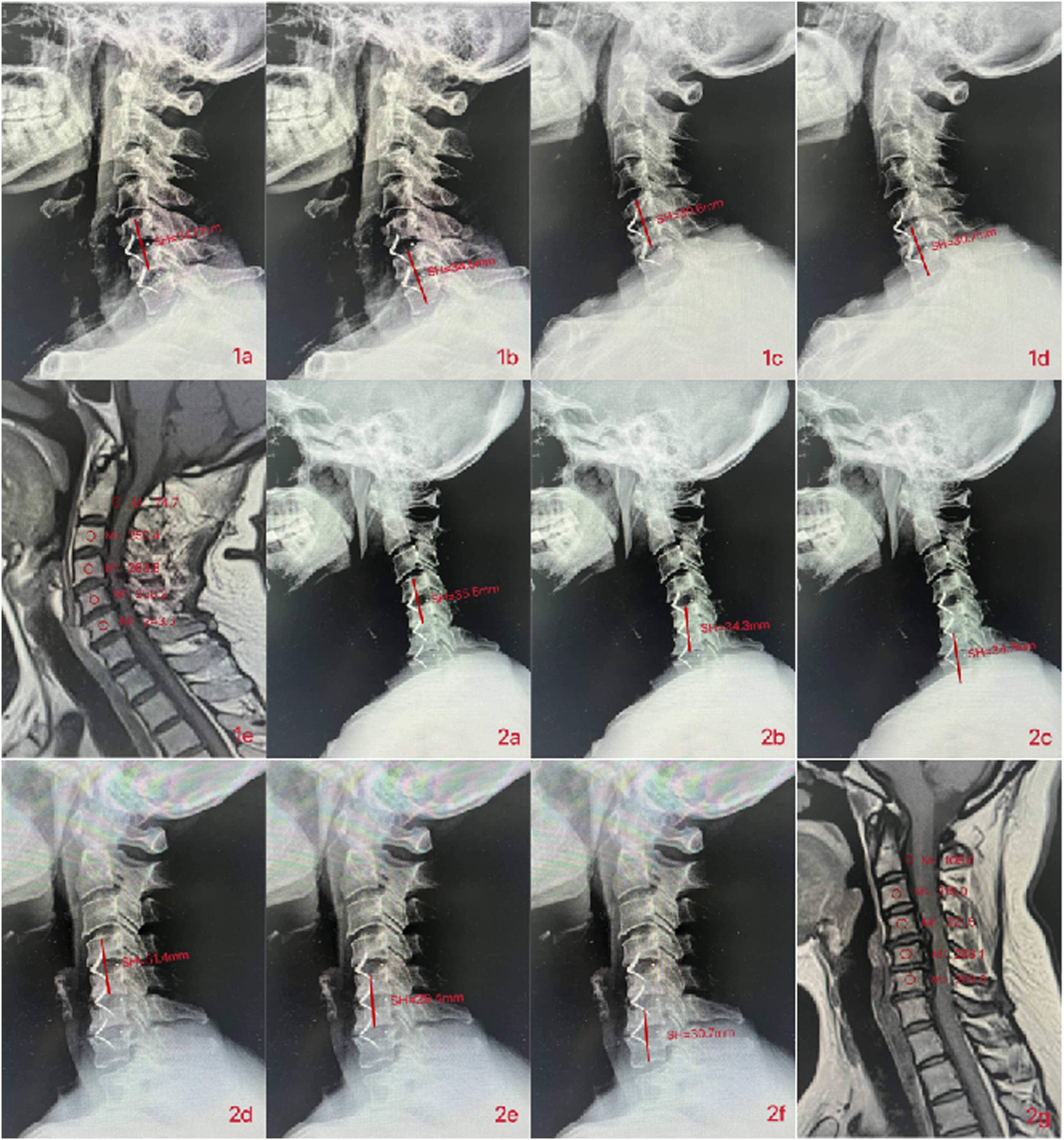
Case 2: Zhao X, female, 53 years old, complained of “walking instability for 3 years, aggravated with weakness of both lower limbs for 1 month.” The patient underwent C4/5, C5/6, and C6/7 ACDF using zero-profile anchored spacer (ROI-C) interbody fusion cage under general anesthesia on 2020-01-06. The last follow-up time was 2021-04-22, and the imaging data of the patient were shown in Figure 7.
Discussion
ACDF proposed by Smith 35 and Cloward 36 in the 1950s, stands as the most frequently employed surgical procedure for addressing degenerative cervical spine diseases. The latest advancement in this field is the zero-profile anchored spacer interbody fusion cage, which can ensures segmental stability, reduces the incidence of dysphagia, and minimizes adjacent disc degeneration.37,38 However, during follow-ups, an increasing incidence of fusion cage subsidence into the adjacent vertebral endplates after ACDF. Studies have indicated that factors contributing to the risk of fusion cage subsidence primarily include the type and material of the fusion cage, patient age, and the stage of fusion, among other variables.39-42 Previous studies have shown that there is a difference in subsidence rate between titanium cages and polyether ether ketone cage. 33 However, most of the current studies on VBQ score to predict the subsidence of the fusion cage after cervical surgery focus on titanium cage. Our study is the first to investigate the predictive effect of C-VBQ score on zero-profile anchored spacer interbody fusion (ROI-C) cage subsidence. The results show that C-VBQ score can also predict the subsidence of polyether ether ketone cage after ACDF. Moreover, the recognized severity of the patient’s osteoporosis is also a factor influencing the subsidence of the fusion cage after cervical surgery.43,44 The mean age of the patients included in this study was 60.86 ± 10.42 years old, and they may be accompanied by different degrees of preoperative osteoporosis. The decrease of BMD often affects the choice of surgical method and leads to the postoperative osteoporosis complications. Therefore, preoperative assessment of BMD is critical to the patient’s surgical outcome.
Correlation of VBQ Score With Bone Mineral Density and Summary of Cutoff Value for Predicting Osteoporosis.
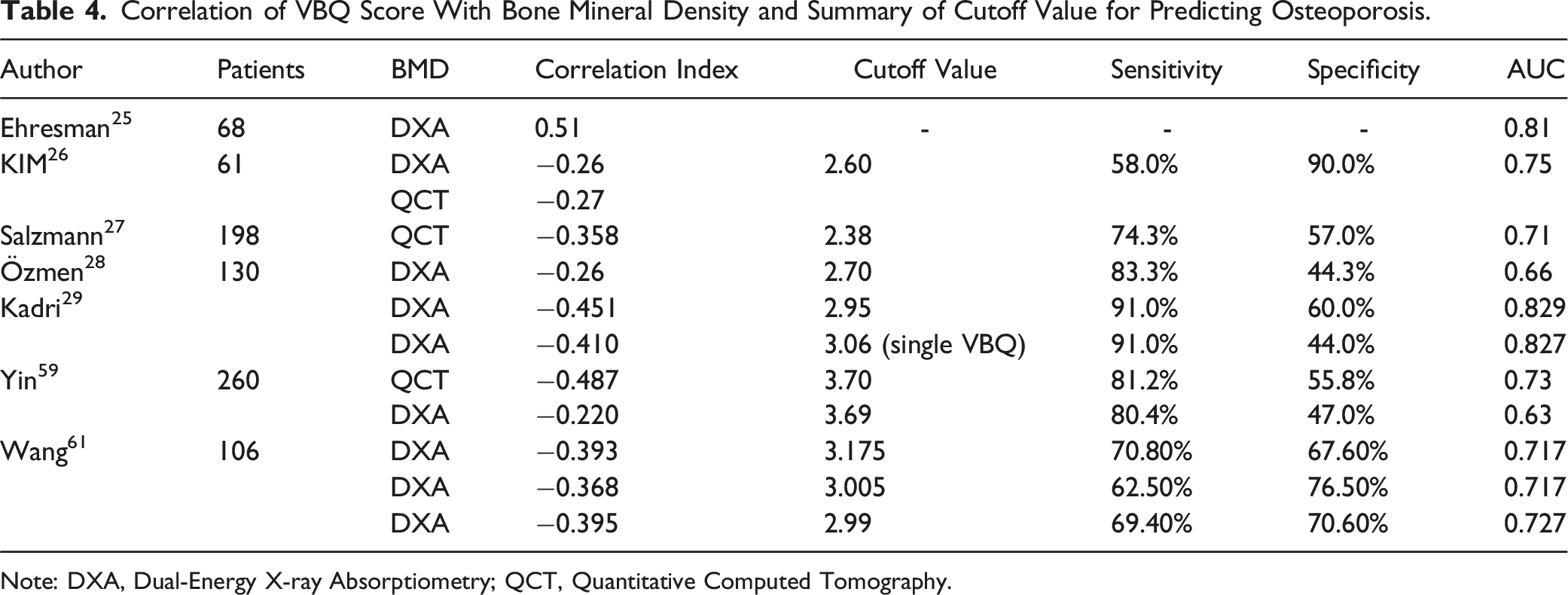
Note: DXA, Dual-Energy X-ray Absorptiometry; QCT, Quantitative Computed Tomography.
Our study investigated the predictive effect of C-VBQ score on the subsidence of zero-profile anchored spacer (ROI-C) interbody fusion cage after ACDF. A total of 102 patients who underwent ACDF using the ROI-C cage were included in the study. Among them, 5 patients were single-segmental, 55 patients were two-segmental and 42 patients were three-segmental. It has been shown that the incidence of fusion cage subsidence after ACDF is 17.7%.62,63 In this study, ROI-C self-stabilizing cage subsidence occurred in 22 patients after ACDF, the cage subsidence did not lead to adverse clinical outcomes, and none of the 22 patients underwent revision surgery. Compared with conventional titanium plate surgery, there were no serious instrument-related complications such as screws, loosening or breakage of titanium plates. We believe that it may be related to the young average age of patients and insufficient follow-up time. Meanwhile, surgical method, surgical procedure, and the choice of cage, which also affects the postoperative clinical outcome of the patients. Therefore, the absence of adverse clinical outcomes within a short time after surgery does not negate the significance of predicting cage subsidence in clinical practice, which requires longer follow-up time to verify.
There were no significant differences between the 2 groups in gender, BMI, smoking history, hypertension and diabetes history, preoperative VAS, NDI, JOA score, follow-up time, and surgical segments. The results of univariate analysis showed that the C-VBQ score of the patients with ROI-C cage subsidence after ACDF was significantly higher than that of the patients without subsidence (2.30 ± 0.36 VS 2.92 ± 0.32; P < 0.001). Although there was a statistical difference in age between the 2 groups (65.36 ± 9.43 VS 59.63 ± 10.39; P = 0.021), age was not an independent risk factor for cage subsidence after ACDF. This may be related to the wide age range of patients included in this study, some of whom were younger. The results of the Pearson correlation analysis showed a significant positive correlation between the C-VBQ score and the height of ROI-C cage subsidence, which was the only significant predictor of ROI-C cage subsidence after ACDF. The optimal cutoff C-VBQ value based on Youden index mining was 2.70 (sensitivity = 81.8%, specificity = 88.7%). MRI belongs to the preoperative routine examination of spinal surgery patients, and the measurement of VBQ score is simple and easy to operate, and clinicians can quickly obtain the results. For patients requiring spinal surgery, VBQ score can preliminatively evaluate preoperative bone mineral density and predict the risk of cage subsidence after ACDF. For patients with low bone mineral density identified by C-VBQ score or at risk of cage subsidence, the surgical method should be carefully selected, the patients should be actively treated with anti-osteoporosis during perioperative period and encouraged to strengthen the neck and shoulder function exercise after surgery.
Limitation
Our study has some limitations. First, this was a retrospective study, and not all of the included patients had preoperative cervical MRI and final follow-up cervical spine X-ray, resulting in a small sample size for this study. Future prospective randomized controlled trials with larger sample sizes are needed to confirm the current findings. Second, there was no preoperative DXA examination in the patients of this study, although this emphasizes our point that DXA results are usually not easily available to spine surgeons. However, the lack of correlation analysis between C-VBQ score and DXA T-value remains 1 of the limitations of this study. Future studies will further improve the correlation analysis between C-VBQ score, DXA T value and QCT bone mineral density value.
Conclusion
The C-VBQ score demonstrated a significant correlation with zero-profile anchored spacer (ROI-C) interbody fusion cage subsidence after ACDF. Furthermore, a higher C-VBQ score before surgery may be an independent factor influencing cage subsidence after ACDF. The preoperative measurement of C-VBQ proves valuable in not only assessing bone mineral density but also predicting the incidence of cage subsidence after ACDF.
Supplemental Material
Supplemental Material - Cervical Vertebra Bone Quality Score Predicts Zero-Profile Anchored Spacer Interbody Fusion Cage Subsidence after Anterior Cervical Diskectomy and Fusion: A Retrospective Study
Supplemental Material for Cervical Vertebra Bone Quality Score Predicts Zero-Profile Anchored Spacer Interbody Fusion Cage Subsidence after Anterior Cervical Diskectomy and Fusion: A Retrospective Study by Ningning Feng, Wenhao Li, Xing Yu, He Zhao, Ziye Qiu, Jianbin Guan, Guozheng Jiang, and Kaitan Yang in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.