
Abstract
Study design
Systematic review.
Objective
To summarise the parameters available to measure horizontal gaze, provide their values in patients and/or asymptomatic individuals, and assess their reliability.
Methods
A literature search was conducted on 9/9/2023 using Medline and Embase, applying the following keywords: “horizontal gaze” or “gaze line”. Articles that reported on horizontal gaze were included.
Results
Twenty-six articles published between 2015 and 2023, were included, of which 15 reported on patients, 10 reported on asymptomatic individuals, and one reported on both. The three most reported horizontal gaze parameters were McGregor’s slope (n = 20 studies, asymptomatic individuals range: −8.8-10.2°), C0-C2 angle (n = 18 studies, asymptomatic individuals range: −32.0-101.5°), and chin brow vertical angle (CBVA) (n = 12 studies, asymptomatic individuals range: −5.9-12.7°). The most frequently reported correlations were between McGregor’s slope and C0-C2 angle (R,-0.390-0.676; P < 0.065; n = 4 studies), McGregor’s slope and CBVA (R, 0.679-0.862; P < 0.0001; n = 3 studies), as well as CBVA and slope of the line of sight (R, 0.592-0.996; P < 0.001; n = 3 studies).
Conclusion
The present systematic review identified 18 parameters used to measure horizontal gaze; however, there is no gold standard. Although parameters had good to excellent inter-observer reliabilities, there were large variations in measurements among asymptomatic individuals across studies, which may imply a limited clinical relevance. Therefore, there is a need for a gold standard parameter of horizontal gaze, which uses easily identifiable landmarks that are simple to measure (reliable), relates both orbital and cervical anatomical structures, and provides insight into compensatory mechanisms in deformative or degenerative conditions.
Keywords
Introduction
Bipedalism and maintaining an upright posture are crucial for achieving stable horizontal gaze, 1 which enables humans to walk, interact with their surroundings, and carry out daily tasks. 2 Horizontal gaze is frequently assessed using the chin brow vertical angle (CBVA) 3 and the McGregor’s slope. 4 The CBVA is defined as the angle formed by a line drawn from the brow to the chin and a line drawn from the brow to the vertical.3,5 The McGregor’s slope is defined as the angle formed by the line from the midpoint of the posterior aspect of the hard palate to the lower margin of the occipital bone and the horizontal plane. 4
The CBVA has easy to identify landmarks and provides repeatable measurements.2,6 However, it is often impossible to measure, as its landmarks (the chin and brow), are not always available on standard sagittal spine radiographs.1,7,8 Additionally, it may not be a reliable measure in cases of mandible protrusion or retraction and does not accurately reflect the relationship between cranial morphology and cervical position. 6 While, the McGregor’s slope has landmarks that are usually available on standard sagittal spine radiographs 1 and does consider head position and cervical morphology, its landmarks are difficult to locate on radiographs, especially the posterior aspect of the hard palate, the opisthion, and the most caudal point on the midline occipital curve.2,9
There have been several attempts to introduce new parameters to measure horizontal gaze,2,10-12 but none have been adopted on a large scale and there is no consensus regarding a gold standard parameter 8 ; in contrast to pelvic incidence, pelvic tilt, and sacral slope, which are known to describe spino-pelvic sagittal balance. 13 A recent narrative review 14 has explored the parameters available to measure horizontal gaze in patients with cervical deformities, but it did not provide average physiological values for this population, nor reported their reliabilities. Furthermore, the available parameters can be grouped into two categories: “de facto” parameters that evaluate horizontal gaze vs parameters that describe the compensatory mechanisms which affect horizontal gaze. Therefore, the purpose of this systematic review is to summarise all parameters available to evaluate or describe horizontal gaze, provide their values in patients and/or asymptomatic individuals, and assess their reliability.
Methods
The search strategy and methodological protocol for this systematic review is registered with PROSPERO (CRD42023456813). This systematic review follows the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines.
Search Strategy
The authors conducted a structured electronic literature search on 9 September 2023 using the Medline and Embase databases, applying the following keywords: “horizontal gaze” or “gaze line”. Duplicate records were removed, and two reviewers (AK,TB) independently screened the title and abstracts to determine eligibility using the following inclusion and exclusion criteria.
Inclusion Criteria:
Comparative or non-comparative studies reporting: • Normative and/or pathologic values of parameters to measure horizontal gaze. • Reliability of parameters to measure horizontal gaze. • Correlations between parameters to measure horizontal gaze, both among themselves and in relation to other spinal and hip parameters.
Exclusion criteria: • Articles that report on parameters of horizontal gaze where the individual was not in the upright position (magnetic resonance imaging, computed tomography, etc). • Articles that report on individuals who underwent measurements of their horizontal gaze following spinal surgery. • Articles written in languages other than English or French. • Reviews, editorial commentaries, conference proceedings, etc. • Cadaveric, laboratory, modelling, and animal studies.
Full-texts were retrieved for all articles that were deemed relevant or if the title and abstract provided insufficient information to establish eligibility. Full text screening was performed independently by three reviewers (AK,TB,DC), with one of the reviewers screening all articles, while the other two reviewers each screened half of the records. Screening decisions were compared between reviewers and disagreements were solved through review and consensus.
Data Extraction and Quality Assessment
The following characteristics were extracted from each eligible study independently by three reviewers (AK,TB,DC), with one of the reviewers extracting data from all articles, while the other two reviewers each performed data extraction on half of the records: lead author, journal, date of publication, article type, conflicts of interest, funding, country of study, cohort type (asymptomatic individuals or patients), pathology if any, cohort size, sex, age, parameters described, definitions of parameters, normative or preoperative pathologic values, inter- and intra-observer reliability, and correlation coefficients. The data extracted was compared and disagreements were solved through review and consensus.
The same three reviewers assessed the methodological quality of eligible studies according to the methodological index for non-randomised studies (MINORS). 15 The quality assessment was compared and any discrepancies in appraisal was resolved through discussion and consensus. “Question 6: Follow-up period appropriate to the aim of the study” and “Question 7: Loss to follow up less than 5%” were not completed as the present study only focused on preoperative measurements. Furthermore, questions relating to comparative studies were not completed, as there was no comparator group of interest. Therefore, the maximum score was 12 points which indicated high quality/low risk of bias, while the minimum score was 0 points which indicated low quality/high risk of bias.
Data Analysis
Parameters were grouped into two categories: “de facto” parameters that evaluate horizontal gaze vs parameters that describe the compensatory mechanisms which affect horizontal gaze. When available in the included articles, horizontal gaze parameters, their reliability, and their correlations were tabulated. Horizontal gaze parameters were reported as means and standard deviations, reliability was reported as intra- or inter-class correlation coefficients (ICC), and correlations were reported as Pearson’s’ or Kendall’s correlation coefficients. Intra- and inter-class correlation coefficients were interpreted using the thresholds defined by Cicchetti et al. 16 which are as follows: <0.40 is poor, 0.40-0.59 is fair, 0.60-0.74 is good, and 0.75-1.00 is excellent. A sub-analysis was performed on the three most commonly reported parameters (McGregor’s slope, CBVA, and C0-C2) to compare differences in these values between patients with deformity pathologies vs patients with degenerative pathologies.
Results
Literature Search
The electronic literature search identified 2075 references, 780 of which were duplicates (Figure 1). The remaining 1295 articles underwent title and abstract screening, and 1261 were excluded as they did not meet the inclusion criteria. The full text of the remaining 34 articles were screened, and a further 8 articles were excluded because: three took measurements from photographs instead of radiographs,5,17,18 two did not specify the parameters used to assess horizontal gaze,19,20 two did not report on horizontal gaze parameters,21,22 and one was a review.
23
This left a total of 26 articles, published between 2015 and 2023 eligible for data extraction, of which 15 reported on patients,1,2,7,24-35 10 reported on asymptomatic individuals,6,10,36-43 and one reported on both.
44
Flowchart of the study selection procedure.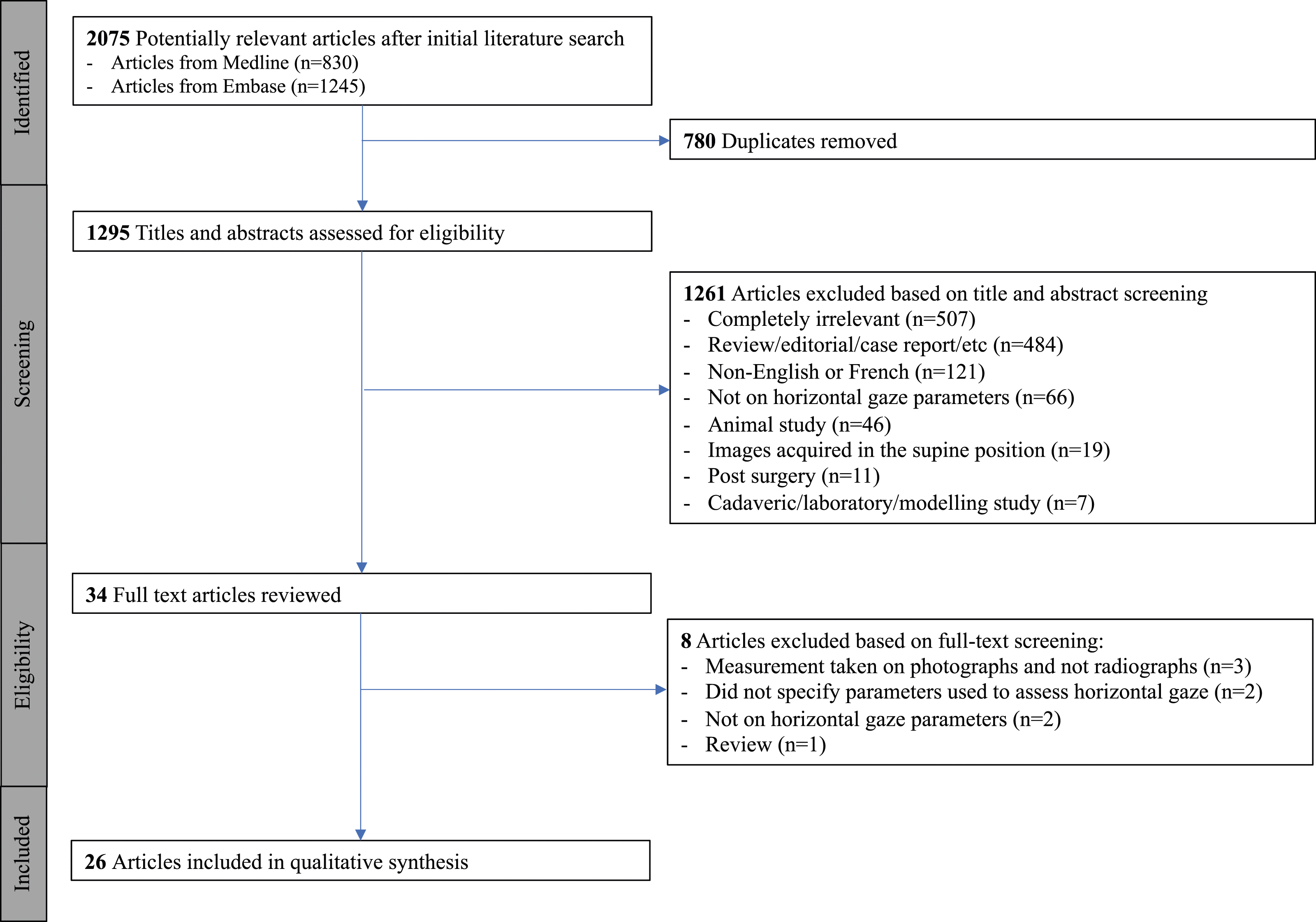
Characteristics of Included Studies and Quality Assessment
Study characteristics.
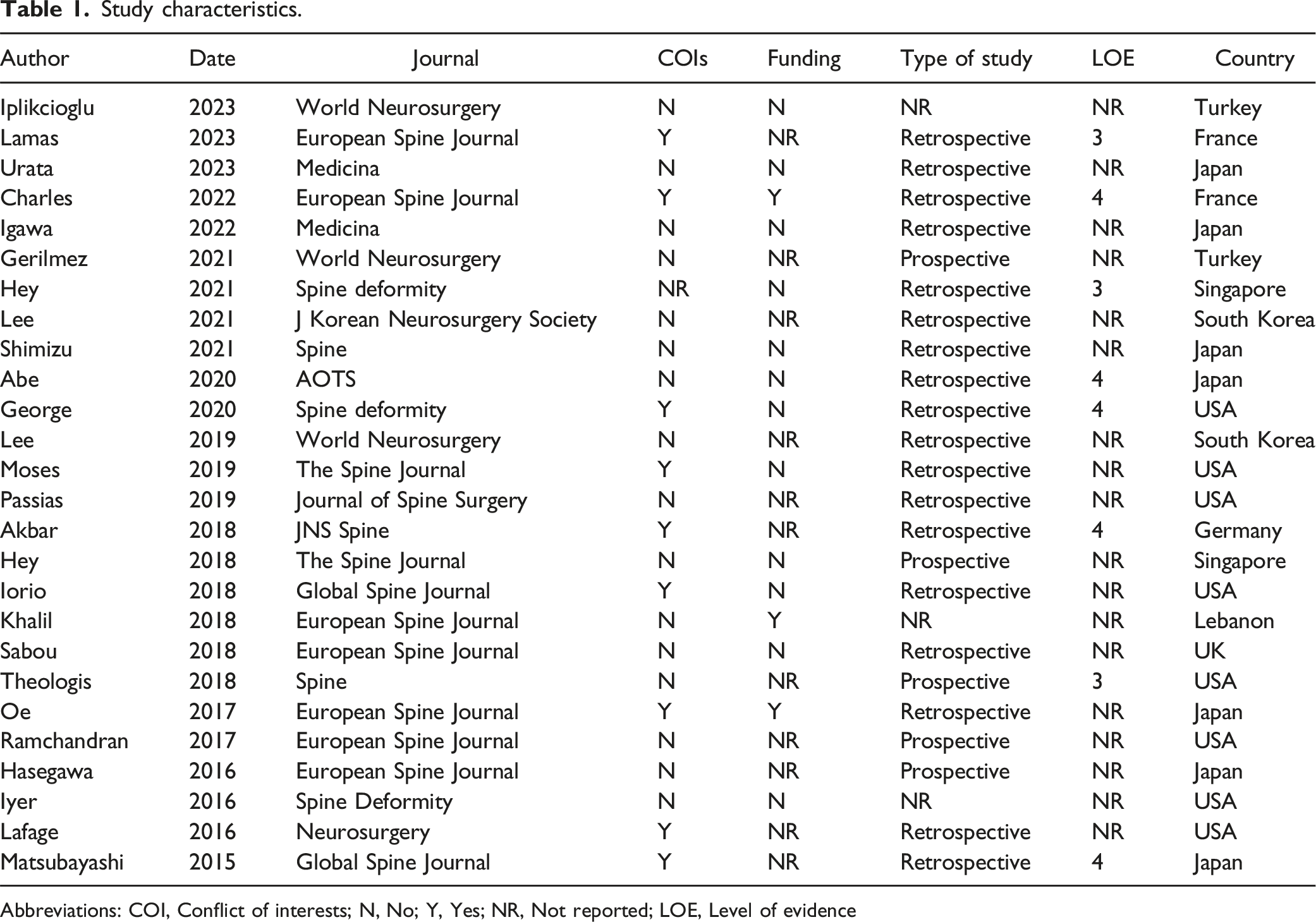
Abbreviations: COI, Conflict of interests; N, No; Y, Yes; NR, Not reported; LOE, Level of evidence
Risk of bias assessment according to methodological index for non-randomised studies (MINORS)*.
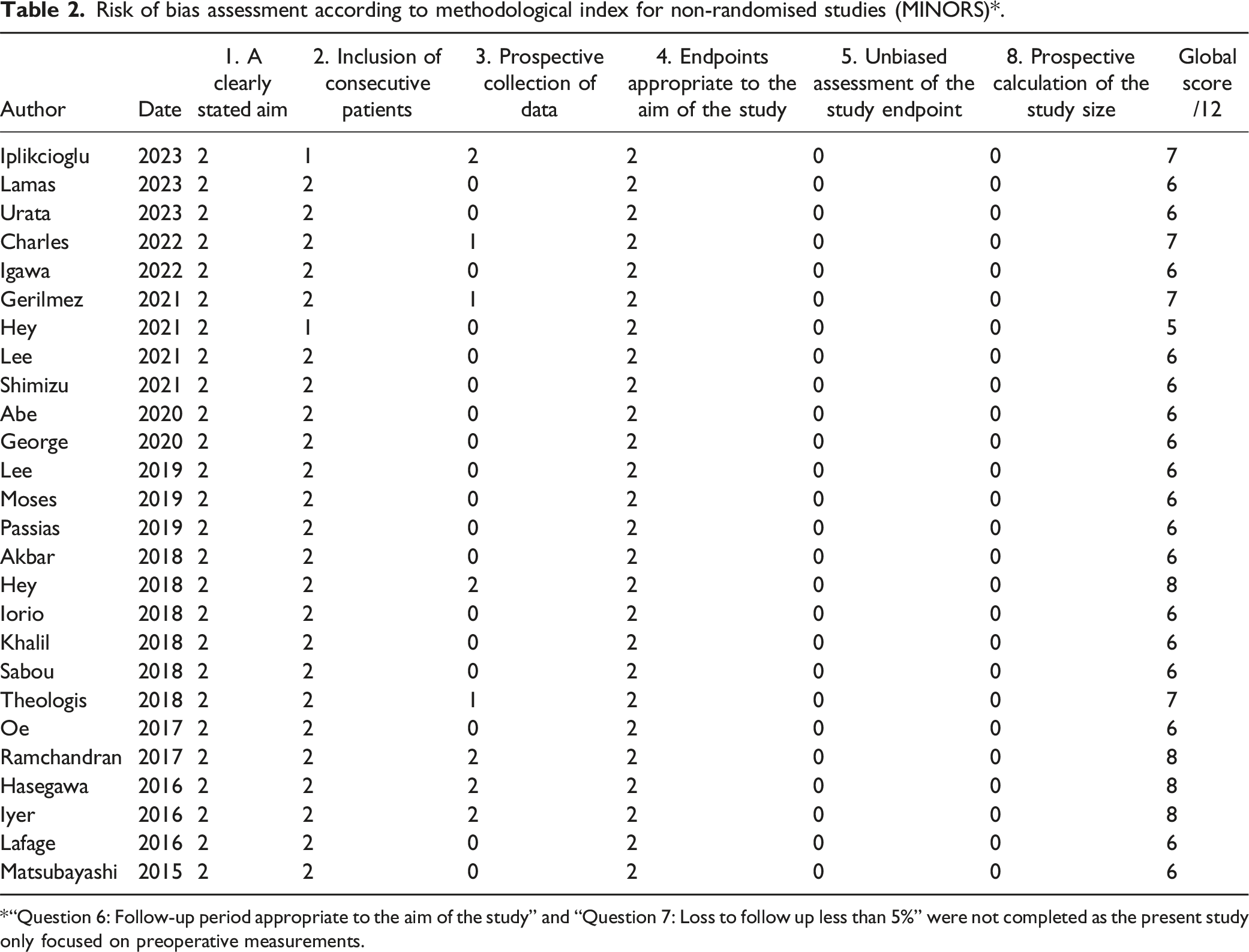
“Question 6: Follow-up period appropriate to the aim of the study” and “Question 7: Loss to follow up less than 5%” were not completed as the present study only focused on preoperative measurements.
Characteristics of Patients and Asymptomatic Individuals
Patient characteristics.
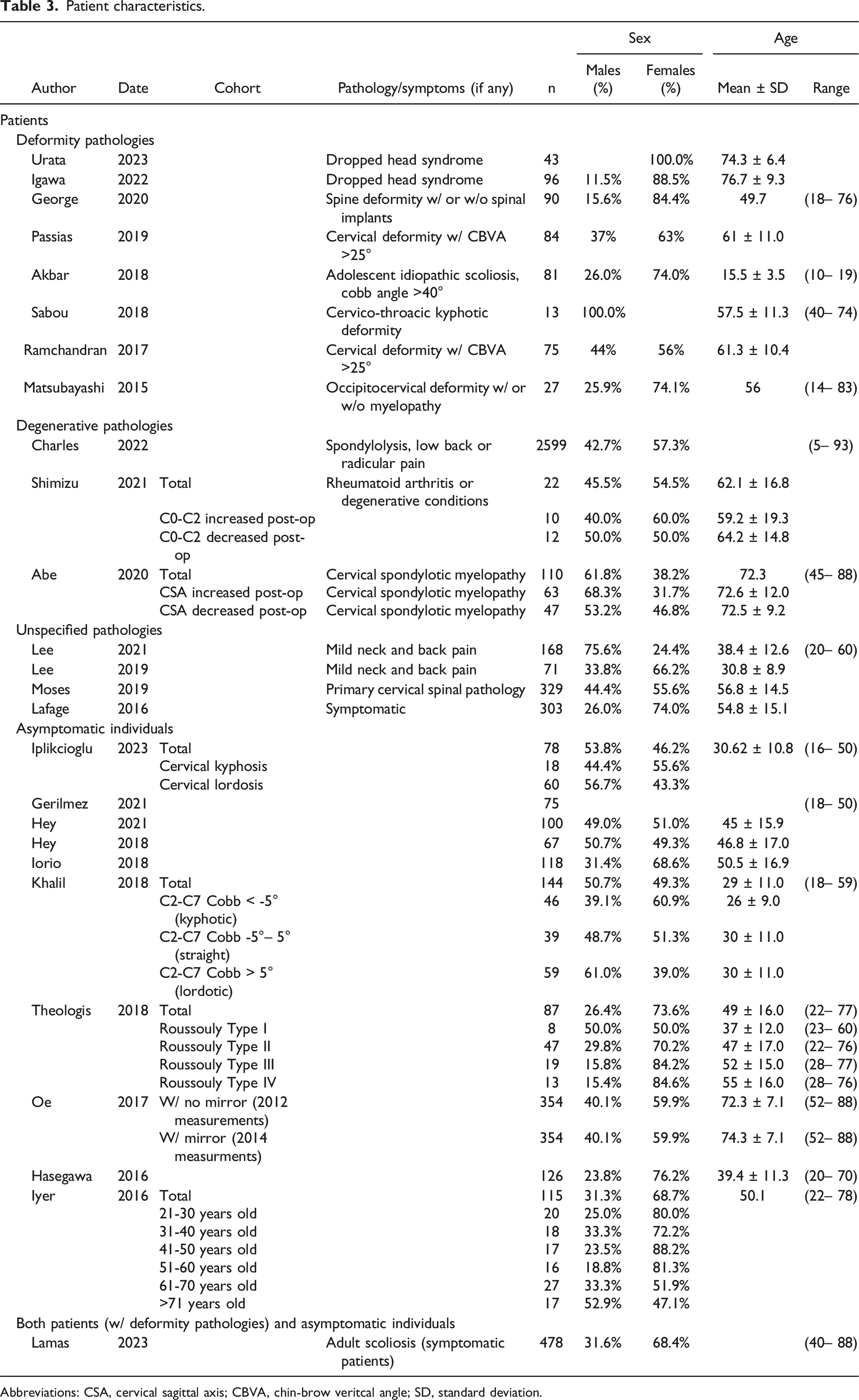
Abbreviations: CSA, cervical sagittal axis; CBVA, chin-brow veritcal angle; SD, standard deviation.
Of the 10 studies that reported on asymptomatic individuals, the cohort size ranged from 67 to 354 subjects per study, with a proportion of males ranging from 23.8% to 50.7%. The mean age ranged from 29.0 to 72.3 years.
In the study that reported on both patients and asymptomatic individuals, there were 243 patients with adult scoliosis and 235 asymptomatic individuals, with an overall proportion of males of 31.6% and age ranging from 40 to 88 years.
“De facto” Parameters that Evaluate Horizontal Gaze
Horizontal gaze parameters.
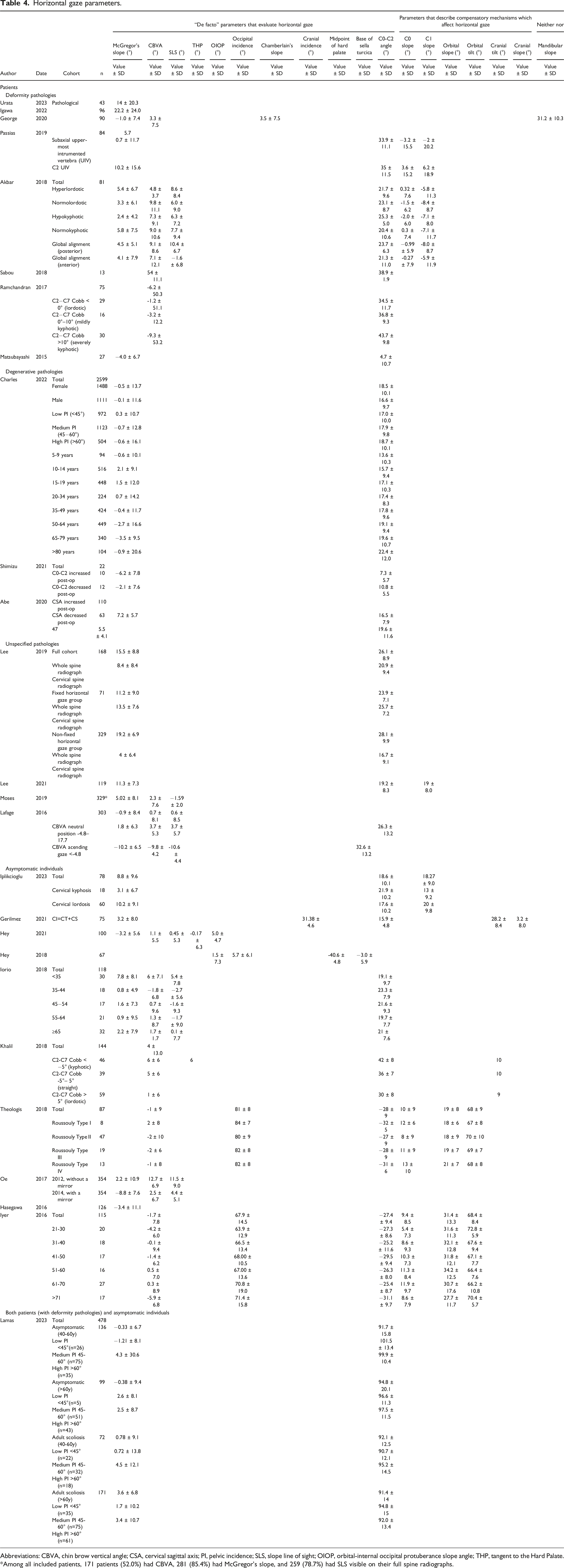
Abbreviations: CBVA, chin brow vertical angle; CSA, cervical sagittal axis; PI, pelvic incidence; SLS, slope line of sight; OIOP, orbital-internal occipital protuberance slope angle; THP, tangent to the Hard Palate.
Among all included patients, 171 patients (52.0%) had CBVA, 281 (85.4%) had McGregor's slope, and 259 (78.7%) had SLS visible on their full spine radiographs.
Parameters that Describe Compensatory Mechanisms which Affect Horizontal Gaze
The most frequently reported parameter that describes compensatory mechanisms which affect horizontal gaze was C0-C2 angle (n = 18 studies)1,6,10,25,28-35,39-41,43-45 (Table 4), with a mean value of 4.7-95.2° for patients (n = 12 studies)1,25,27-35,44 and −32.0-101.5° for asymptomatic individuals (n = 7 studies).6,10,39-41,43,44 Furthermore, 6 other parameters that describe compensatory mechanisms which affect horizontal gaze were described, including C0 slope (n = 4 studies; also known as occipital slope and McRae slope),6,28,32,43 C1 slope (n = 4 studies),28,29,32,40 orbital slope (n = 2 studies),6,43 orbital tilt (n = 2 studies),6,43 cranial tilt (n = 2 studies),10,41 and cranial slope (n = 1 study). 10
One additional parameter was identified from the literature: the mandibular slope (n = 1 study) 2 (Table 4), which is neither a “de facto” parameter that evaluates horizontal gaze nor a parameter that describes compensatory mechanisms, but it still provides useful information regarding horizontal gaze.
Sub-analysis to Compare Patients with Deformity Pathologies vs Degenerative Pathologies
Mean McGregor’s slope was −4.0-22.2° for patients with deformity pathologies (n = 6 studies) and −6.2-7.2° for patients with degenerative pathologies (n = 3 studies); there was a trend of lower McGregor’s slope in patients with degenerative pathologies (Table 4). Mean CBVA was −9.3-9.8° for patients with deformity pathologies (n = 4 studies), while no CBVA values were reported for patients with degenerative pathologies (n = 0 studies). Mean C0-C2 was 4.7-43.7° for patients with deformity pathologies (n = 5 studies) and 7.3-22.4° for patients with degenerative pathologies (n = 3 studies); there was a trend of lower C0-C2 in patients with degenerative pathologies.
Observer Reliability
Only two studies reported observer reliability for horizontal gaze parameters (Appendix I). George et al 2 reported excellent inter-observer reliabilities for McGregor’s slope (0.90, P < 0.001), Chamberlain’s slope (0.81, P < 0.001), and mandibular slope (1.0, P < 0.001). Iyer et al 6 reported excellent inter-observer reliabilities for CBVA (0.98, p = not reported (NR)), C0-C2 angle (0.91, p = NR), orbital slope (0.80, p = NR), orbital tilt (0.97, p = NR), and C0 slope (0.95, p = NR), but good reliability for occipital incidence (0.69, p = NR).
Correlations
Horizontal gaze parameters and their correlations with other horizontal gaze or spinal parameters.
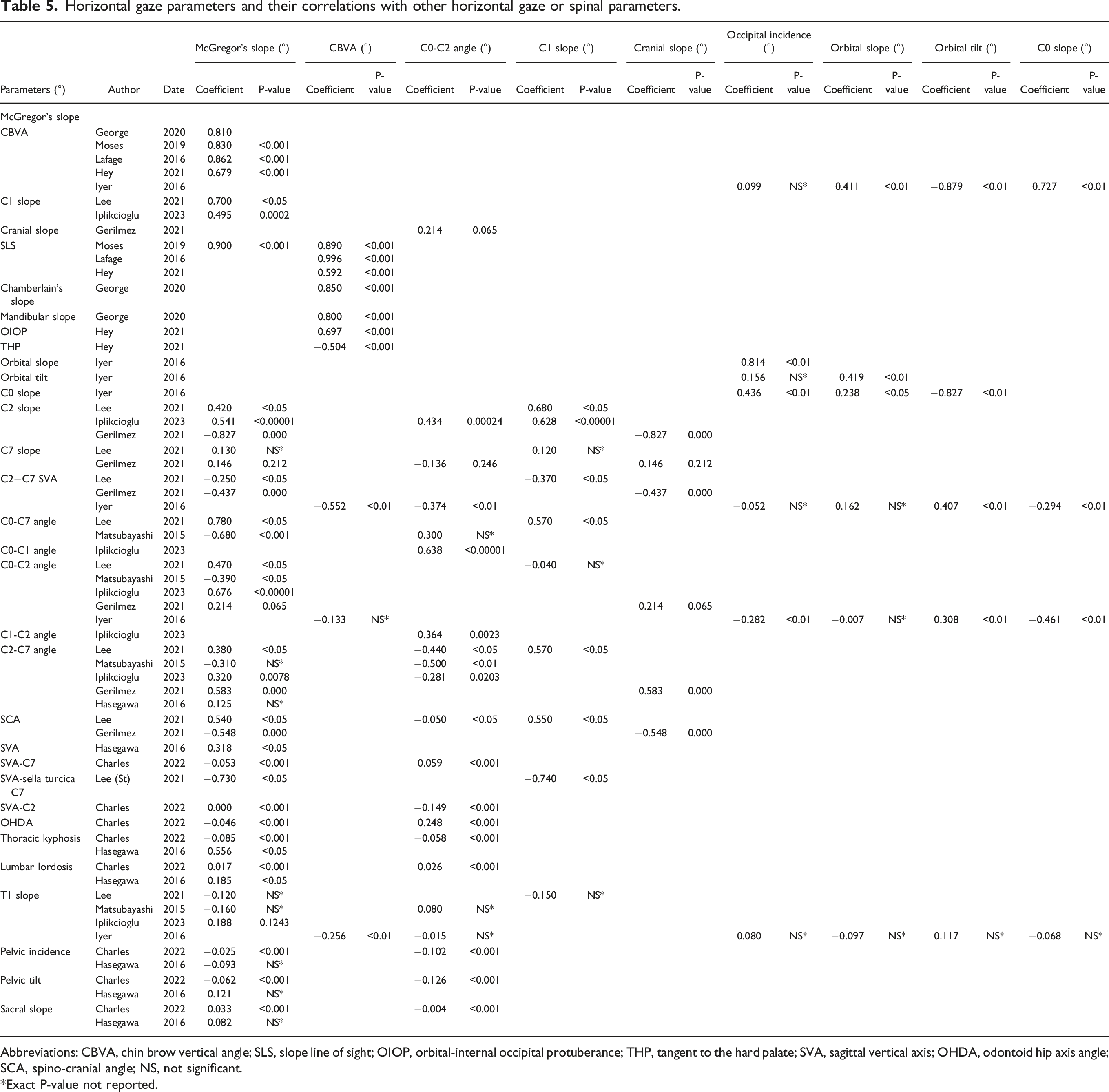
Abbreviations: CBVA, chin brow vertical angle; SLS, slope line of sight; OIOP, orbital-internal occipital protuberance; THP, tangent to the hard palate; SVA, sagittal vertical axis; OHDA, odontoid hip axis angle; SCA, spino-cranial angle; NS, not significant.
*Exact P-value not reported.
Discussion
The present systematic review aimed to summarise the parameters available to measure horizontal gaze, provide their values in patients and/or asymptomatic individuals, and assess their reliability. The most important findings are that, though there are 18 parameters to measure horizontal gaze, there is no gold standard. The present review found 10 “de facto” parameters that evaluate horizontal gaze, seven parameters that describe the compensatory mechanisms which affect horizontal gaze, and one parameter that does neither of the above but still provides useful information regarding horizontal gaze. Furthermore, although the parameters have good to excellent inter-observer reliabilities (0.69-1.0), there are large variations in means among asymptomatic individuals across studies, which implies they may have limited clinical relevance. The findings of this systematic review highlight the need for a gold standard parameter for horizontal gaze, which uses easily identifiable landmarks that are simple to measure (reliable), relates both orbital and cervical anatomical structures, and provides insight into compensatory mechanisms in deformative or degenerative conditions. Furthermore, future studies should investigate the pathologic values of these parameters, as well as their variability among an asymptomatic population and across different spine pathologies.
A recent narrative review 14 that summarised the different measurements of horizontal gaze in patients with cervical deformities included 41 articles, of which the following parameters were described: CBVA (21 studies), McGregor’s slope (19 studies), SLS (6 studies), C0-C2 slope (3 studies), orbital-internal occipital protuberance slope angle (1 study), THP (1 study), mandibular slope (1 study), Chamberlain’s slope (1 study), and the 3-6–12 rule derived from the base of the sella turcica and OIOP (1 study). The review concluded that there is no ideal measurement of horizontal gaze and emphasised that new methods should be studied in order to improve clinical practice. This is in line with the findings of the present systematic review; however, the present review also highlights the need for a novel parameter that considers both orbital and cervical anatomical structures.
Although the literature states that a number of parameters are used to measure horizontal gaze, the present systematic review has grouped these parameters into three categories: “de facto” parameters that evaluate horizontal gaze, parameters that describe the compensatory mechanisms which affect horizontal gaze, and parameters that are neither of the two but still provide useful information regarding horizontal gaze. “De facto” parameters were taken as those that are fixed or are considered fixed, such as the CBVA. In contrast, there are other parameters, such as the C0-C2, which capture partial or complete compensatory mechanisms of the spine. In patients with spinal pathologies, compensatory mechanisms may take place in the trunk to maintain an upright position, which could produce large variations in the compensatory parameters, but not in the “de facto” parameters. There was only one parameter that did not fit either group: the mandibuar slope, which can vary with mouth opening. Interestingly, the sub-analysis to compare patients with deformity pathologies vs those with degenerative pathologies showed that the latter had lower McGregor’s slope and C0-C2. CBVA could not be compared across groups because it was not reported for patients with degenerative pathologies.
The CBVA and McGregor’s slope are the most frequently used to measure horizontal gaze, however, there is no gold standard parameter. While, the CBVA is easy to measure and highly repeatable, it does not consider the relationship between cranial morphology and cervical position and it cannot be consistently measured due to relevant landmarks (the chin and brow) often being unavailable on radiographs.1,7,8 Furthermore, the CBVA is distorted in cases of mandible protrusion or retraction and is dependent on mouth opening. 6 McGregor’s slope, on the other hand, accounts for cranial morphology and cervical position but relies on the correct identification of difficult-to-find landmarks (the posterior aspect of the hard palate and the opisthion) that are not always visible on radiographs.2,9 Other parameters such as the C0-C2 angle1,6,10,25,28-35,39-41,43-45 and SLS1,7,28,36,37,39,42 have also been used to measure horizontal gaze. These parameters also exhibit high variability across studies in the asymptomatic population. The present systematic review found that asymptomatic individuals had mean CBVA that ranged from −5.9-12.7°, mean McGregor’s slope that ranged from −8.8-10.2°, mean C0-C2 that ranged from −32.0-101.5°, and mean SLS that ranged from −2.7-11.5°. Several studies have also reported high variability in SLS among a healthy population.1,46 Nonetheless, inter-observer reliabilities were excellent for McGregor’s slope (0.90), CBVA (0.98), and C0-C2 angle (0.91), 2 indicating that the discrepancy across studies does not stem from difficulty in performing measurements. Furthermore, Oe et al 42 performed imaging in asymptomatic individuals with and without the use of a mirror and found considerable differences in measurements of McGregor’s slope (−8.8 vs 2.2), CBVA (2.5 vs 12.5), and SLS (4.4 vs 11.5), which may be due to the position of the head.
Various studies have introduced alternative parameters to measure horizontal gaze. Hey et al 38 proposed four novel parameters: the midpoint of the hard palate, the base of the sella turcica, THP, and OIOP. The study concluded that the midpoint of the hard palate and THP were poor measures of horizontal gaze as the sloped and curved structure of the hard palate may lead to inaccurate results. Instead, they recommended the use of the base of the sella turcica and OIOP, which may more accurately measure horizontal gaze and help determine gaze direction, potentially serving as an indicator for C0 functional alignment in the measurement of cervical angles. The authors of the present study believe that it is also difficult to identify the base of the sella turcica in standard sagittal radiographs.
The same authors further investigated the use of THP and OIOP in determining gaze direction 37 by comparing them to existing measures of horizontal gaze. The study found that OIOP (standard deviation (SD), 4.66) exhibited lowest variability in a population of healthy subjects compared to CBVA (SD, 5.48°), McGregor’s slope (SD, 5.63°), and THP (SD, 6.27°). Among the studied parameters, the authors concluded that OIOP is the most appropriate parameter for measuring horizontal gaze as it is less prone to variations in anatomy and has easy to identify landmarks. However, the OIOP does not relate the orbit to the cervical spine.
George et al 2 proposed the use of the mandibular slope, defined as the angle created by the inferior edge of the mandibular body and the horizontal. Mandibular slope (1.0, P < 0.001) has a higher interobserver reliability compared to McGregor’s slope (0.90, P < 0.001) and Chamberlain’s slope (0.81, P < 0.001) and is moderately correlated with CBVA (0.80). Unlike the McGregor’s slope and Chamberlian’s slope that rely on the identifcation of the posterior aspect of the hard palate, which is difficult to locate on low-quality radiographs2,9; the mandibuar slope uses the inferior edge of the mandibule, which is easily identifiable on most radiographs. However, it can yield inaccurate results in patients with fixed coronal plane deformities as both far and near edges of the mandible would be visible on lateral radiographs. The authors suggest using the average slope of both lines in such cases. Furthermore, variations in mandibular morphology, as well as slight mouth opening may also lead to inaccuracies.
The parameters proposed by Hey et al 38 and George et al 2 do not use any landmarks that relate the cranium to the cervical spine, and therefore cannot be used to explain compensatory mechanisms between the head and the spine in the framework of degenerative and deformative conditions. Thus, morphometric parameters that provide deeper insights into cervical spine mechanisms might be preferable to measure horizontal gaze. Gerilmez et al 10 introduced the cranial slope (CS) defined as the angle between the McGregor’s line and the horizontal line; the cranial tilt (CT) defined as the angle between the line connecting the sella turcica and centre of McGregor’s line and the vertical line; and the cranial incidence (CI) defined as the angle between the line perpendicular to the centre of McGregor’s line and the line connecting the sella turcica and centre of McGregor’s line, where CI = CS + CT. Though CS had a strong correlation with McGregor’s slope (0.900, P < 0.001), 7 it had a weak correlation with C0-C2 angle (0.214, P = 0.065). 10 The study did not report correlations between CI and CT and other horizontal gaze parameters, nor did it report correlations between the three introduced parameters. The inter and intra-observer reliability of these parameters was also not reported.
Iyer et al 6 measured the C0 slope (named occipital slope (OS) in the article); the orbital tilt (OrT), defined as an angle between the vertical and a line extending from the center of the orbit to the center of McRae’s line; and the occipital incidence (OI), which is a morphometric parameter where OI = OS + OrT. All three parameters showed good to excellent inter-observer reliabilities (OS = 0.80, OrT = 0.97, and CI = 0.69). Furthermore, only OrT had a strong correlation with CBVA (−0.879, P < 0.01), while OS and OI had a weak correlation with CBVA (0.411, P < 0.01 and 0.099, P > 0.05, respectively). Additionally, none of the three parameters had strong correlations with other sagittal spine parameters such as C0-C7 angle, C0-C2 angle and T1 slope. OS, OrT, and OI rely on the McRae line, which requires correct identification of the foramen magnum, which can be challenging to locate. Moreover, OS uses the C0 vertebra as a landmark, which is immobile and may not fully capture the relationship between the cervical spine and the cranium.
The present systematic review has several limitations. First, it was difficult to directly compare studies, as most studies stratified the cohort into different subgroups; therefore, meta-analyses could not be performed. Second, it was not possible to compare horizontal gaze values in pathologic patients due to different pathologies being reported across studies. Furthermore, two studies included patients with a CBVA >25°.32,33
Conclusion
The present systematic review has identified 18 parameters used to measure horizontal gaze; however, there is no gold standard. Although the identified parameters have good to excellent inter-observer reliabilities, there are large variations in measurements among asymptomatic individuals across studies, which may imply a limited clinical relevance. Therefore, there is still a need for a gold standard parameter for horizontal gaze, which uses easily identifiable landmarks that are simple to measure (reliable), relates both orbital and cervical anatomical structures, and provides insight into compensatory mechanisms in deformative or degenerative conditions.
Supplemental Material
Supplemental Material - Parameters Used to Define Horizonal Gaze: A Systematic Review
Supplemental Material for Parameters Used to Define Horizonal Gaze: A Systematic Review by Féthi Laouissat, MD, Sonia Ramos-Pascual, MEng, PhD, Ankitha Kumble, BSc, Theo Broussolle, MD, Danilo Casasola, MD, Mo Saffarini, Meng, MBA, FRSM, and Alexis Nogier, MD in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ‘Clinque Trenel’, which provided funding for data analysis and manuscript writing.
Data Availability Statement
Data is available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.