
Abstract
Study Design
Observational study
Objective
As an important consideration of surgery, cervical sagittal balance is believed to be better assessed using standing radiograph than supine magnetic resonance imaging (MRI). However, few studies have researched this. Our study aimed to observe the correlations and differences in cervical sagittal parameters between radiograph and MRI in patients with cervical spondylotic myelopathy (CSM), and evaluate whether the change of position affects them.
Methods
We analyzed 84 patients, measuring Cobb angle (CA), T1 slope (T1S), neck tilt (NT), and thoracic inlet angle (TIA). Inter- and intra-parameter analyses were performed to identify any difference between standing radiograph and supine MRI. Statistical correlations and differences between the parameters were compared.
Results
There were excellent inter-observer agreement for each parameter (interclass correlation coefficient >.75), and significant differences were observed in each parameter between radiograph and magnetic resonance imaging (P < .05). Strong correlations were noted between the same parameters in radiograph and MRI. Cobb angle, T1S, and neck tilt were significantly correlated with thoracic inlet angle on both radiograph and MRI, and CA was significantly correlated with T1S on both radiograph and MRI (r: −1.0 to −.5 or .5 to 1.0).
Conclusion
Supine MRI obviously underestimated the value of CA, T1S, and TIA. Therefore, standing cervical radiographs should be obtained in CSM patients to assess and determine surgical strategy, not only supine MRI. Moreover, we observed that NT and TIA were not constant morphological parameters.
Introduction
With the increasing incidence of cervical spondylotic myelopathy (CSM), more patients choose surgical treatment in recent years. As an important consideration of laminectomy and anterior cervical discectomy and fusion, spinal surgeons have paid much attention to cervical sagittal balance.1,2 The sagittal parameter of cervical spine has been a hot spot in spine surgery, these parameters include thoracic inlet angle (TIA), neck tilt (NT), and T1 slope (T1S), that were considered previously as important factors influencing cervical sagittal balance.3,4 Several studies reported that the postoperative changes of cervical sagittal parameters were closely related to the quality of life.5,6 Meanwhile, it was pointed out that the larger preoperative T1S significantly increased the kyphotic changes of posterior laminoplasty. 7 Therefore, sagittal balance must be considered before spinal surgery.
T1-related sagittal parameters are very valuable in evaluating sagittal balance, however, T1 vertebral body, sternal manubrium, and sometimes even the lower endplate of C7 vertebrae cannot be definitely identified on standing cervical radiograph due to the occlusion of bilateral shoulder joints.8,9 Qiao et al. 10 reported that only 21% of radiographs can clearly show T1 vertebra and upper sternum, which makes it difficult to measure T1-related sagittal parameters. However, those anatomic structures are clearly visible on supine magnetic resonance imaging (MRI), and it is of great significance to measure T1 sagittal parameters through MRI instead of radiograph. Therefore, some surgeons use only MRI for preoperative planning. However, it seems not deliberate and comprehensive enough. Nevertheless, as long as there is no evidence that weight-bearing radiograph is necessary for assessment of cervical sagittal alignment, we still have reason to argue that supine MRI is sufficient in preoperative work-up. 11
In addition, as is known to all, cervical radiographs are performed in standing position with skull weight adding a compressive force on the vertebrae, while supine position is taken for MRI with a counterforce from the bed affecting the vertebrae. Whether there are correlations or differences between those parameters obtained from the two examinations still need to be revealed. The purpose of our study was to analyze and compare the sagittal parameters measured on radiograph and MRI in patients with CSM, and evaluate whether the neck position affects these parameters.
Materials and Methods
Patient Case and Parameters
We obtained ethical approval exemption from our ethics committee to perform this study since we didn’t have direct contact with the participants. Database records of patients treated for CSM in our hospital were retrospectively included and analyzed since April 1, 2018, to March 31, 2020. All participants were required to have available clinical data and a full set of cervical radiographs and MRI images. The exclusion criterion was as follows: 1) T1 vertebral body and/or upper end of sternum were not clearly visible on lateral radiograph (obscured by overlapping soft and bony tissues); 2) Patients with history of cervical surgery, trauma, infection, and deformity were excluded, as well as those combined with tumor, tuberculosis, ankylosing spondylitis, and other systemic diseases (to avoid objective impacts on measurements). A total of 84 subjects were involved.
Cervical radiographs were performed using standing position, with upper extremities neutrally hanging down and eyes looking straight ahead. The projection range includes the orbit to the upper thoracic spine, and the center is at the level of C4-C5. Cervical MRI was with patient in supine neutral position using 1.5 T machine. MRI data was measured on the T2-weighted images. The radiograph and MRI of each case were performed within 2 months’ interval in order to avoid deviation caused by disease progression.
Data collection was performed by one of the managing team physician, who was not involved in the final data analysis. One spine surgeon and one radiologist were selected to be evaluators and performed the measurements with Picture Archiving and Communication System (PACS) as they blinded from the clinical data of the patients. The following cervical sagittal parameters were assessed on both radiographs and MRI images: 1) C2-7 Cobb angle (CA), measured as the angle between the tangents of the C2 and C7 lower endplates; 2) T1S, measured as the angle between the T1 upper endplate and horizontal reference line at the median sagittal cervical vertebra; 3) NT, defined as the angle between the vertical line and the line connecting the center of the T1 upper endplate and the sternum tip; and 4) TIA, defined as the angle between the perpendicular bisector of the T1 upper endplate and the line connecting the center of the T1 upper endplate and the sternum tip.4,12 The thoracic inlet angle was derived from the following formula: thoracic inlet angle = T1 slope + neck tilt (Figure 1).
12
Cervical sagittal alignment parameters.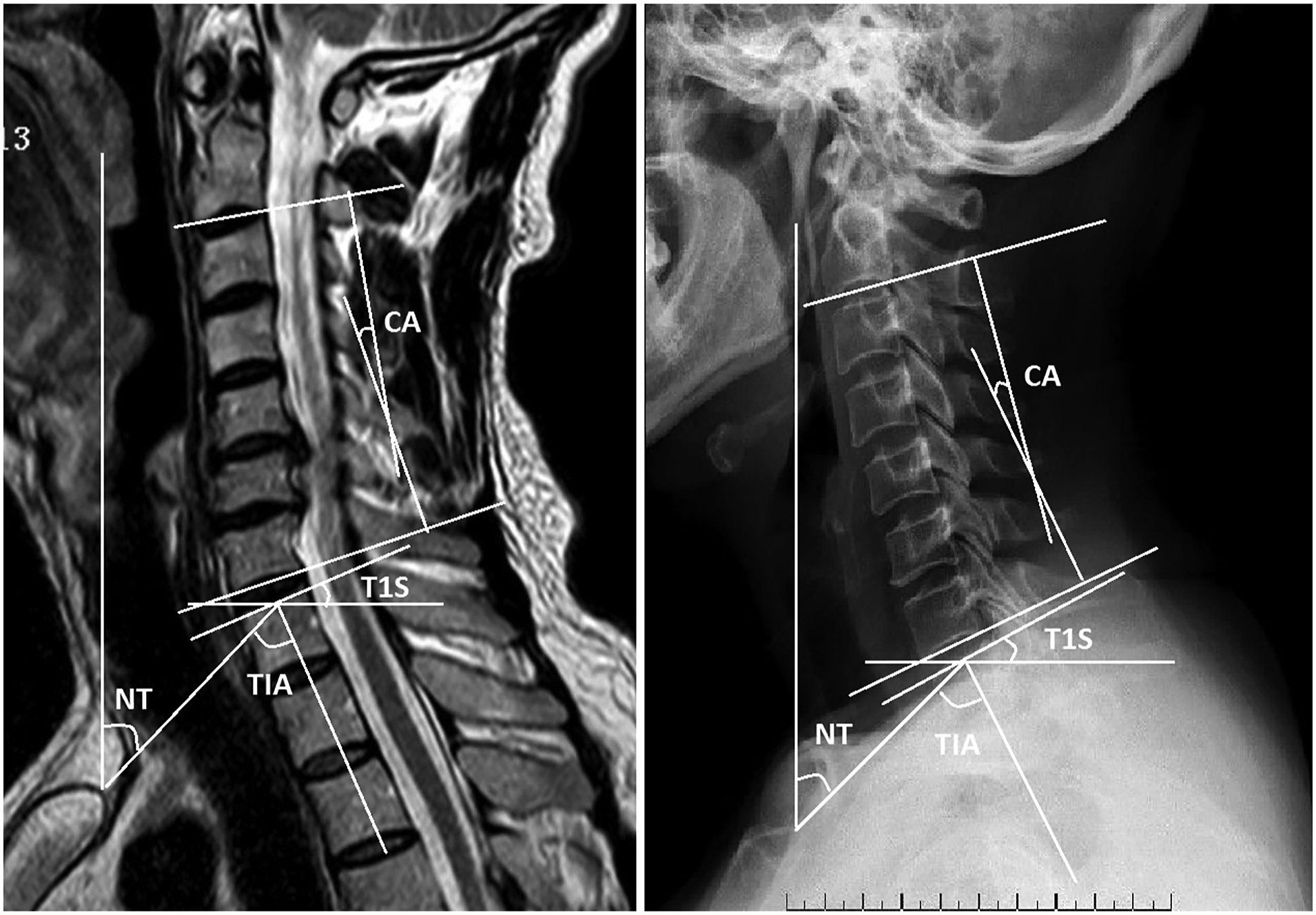
Statistical Analysis
Level of Agreement for ICC Values and Relationship for r Values.

All the parameters were expressed as mean ± standard deviation since they belonged to measurement data. Paired t tests were used to analyze the differences between plain radiographs and MRI studies if the parameters conformed to normal distribution. The correlation analysis of these parameters between the two imaging studies were performed by Pearson correlation test and expressed by r coefficient which was divided into 4 grades, with -1.0 to -.5 or .5 to 1.0 considered strong, -.5 to -.3 or .3 to .5 considered moderate, -.3 to -.1 or .1 to .3 considered weak, and -.1 to .1 considered none or very weak (Table 1). Meanwhile, P values of <.05 were considered statistically significant for all the above.
Result
237 patients were reviewed with CSM within the study period, and 153 were excluded. The current study totally involved 84 consecutive cases, including 49 males (58.3%) and 35 (41.7%) females with a mean age of 53.7 ± 8.1 years (range from 36 to 75 years). For there were two evaluators measuring the four sagittal parameters, respectively, on radiographs and MRI studies, we obtained a total of 1344 measurements.
Inter-observer Reliability
Inter-observer Reliability and Pairwise Difference of Each Parameter between observers.
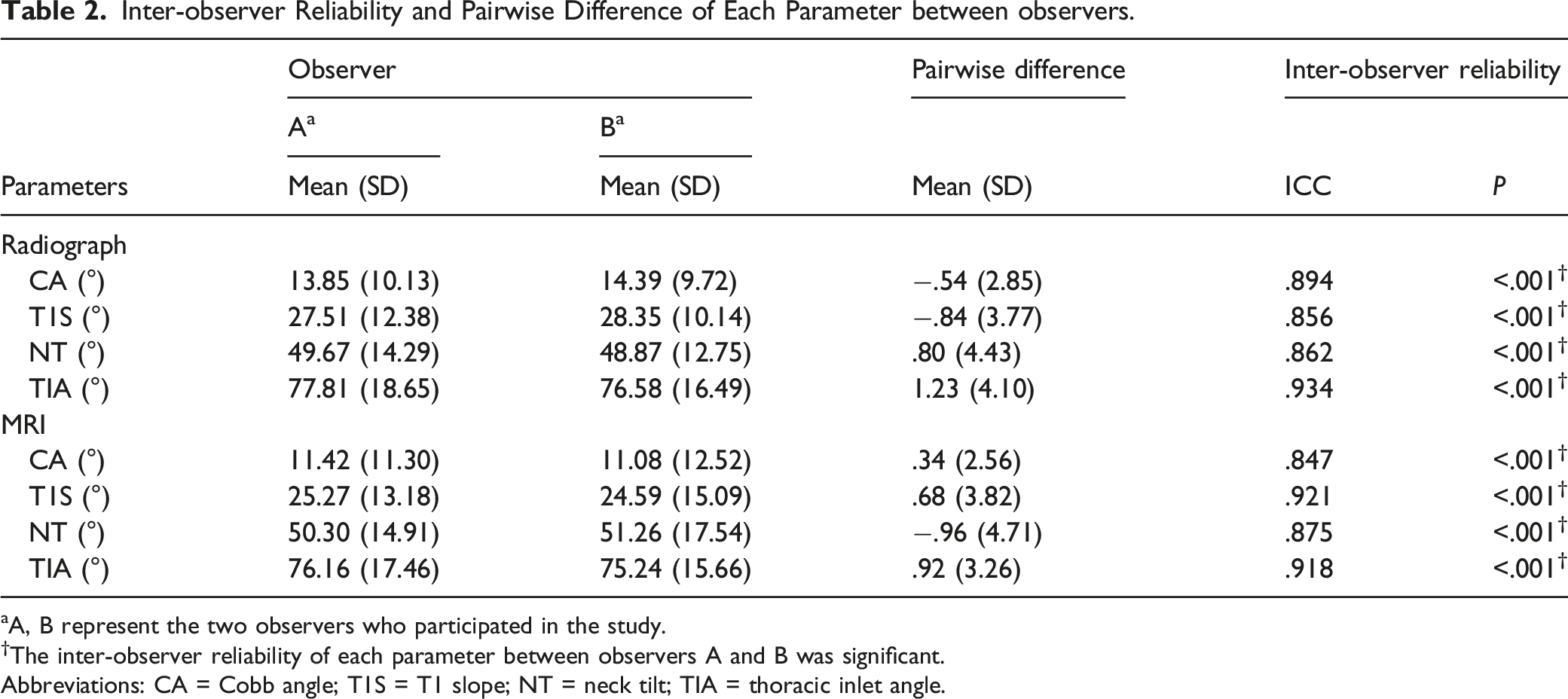
aA, B represent the two observers who participated in the study.
†The inter-observer reliability of each parameter between observers A and B was significant.
Abbreviations: CA = Cobb angle; T1S = T1 slope; NT = neck tilt; TIA = thoracic inlet angle.
Cervical Sagittal Parameters
Pairwise Differences of Cervical Sagittal Parameters between Radiograph and MRI.
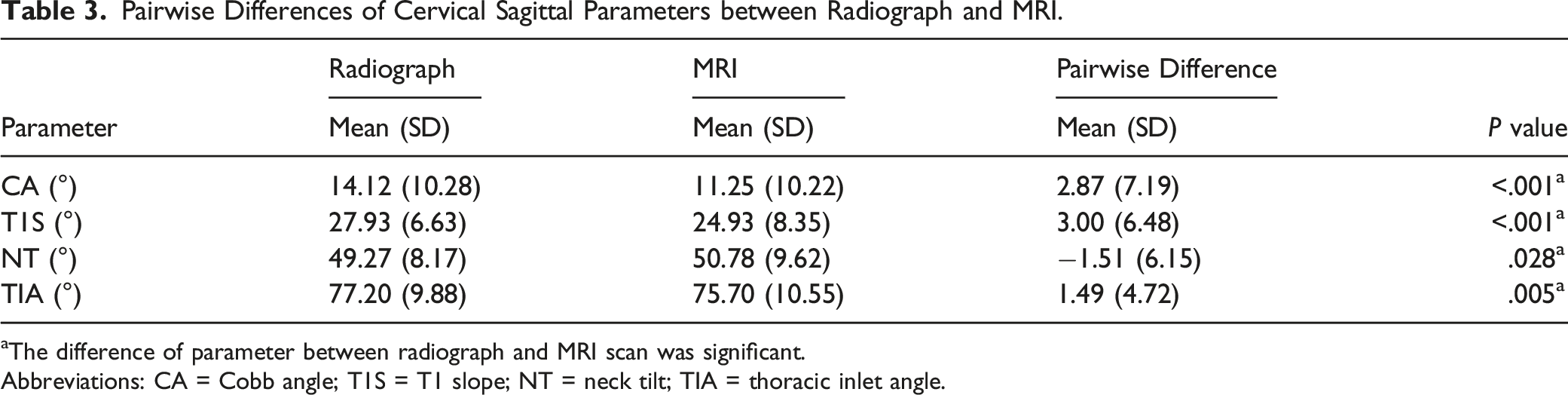
aThe difference of parameter between radiograph and MRI scan was significant.
Abbreviations: CA = Cobb angle; T1S = T1 slope; NT = neck tilt; TIA = thoracic inlet angle.
Correlations of Parameters
Correlations of Parameters in Radiograph and MRI.
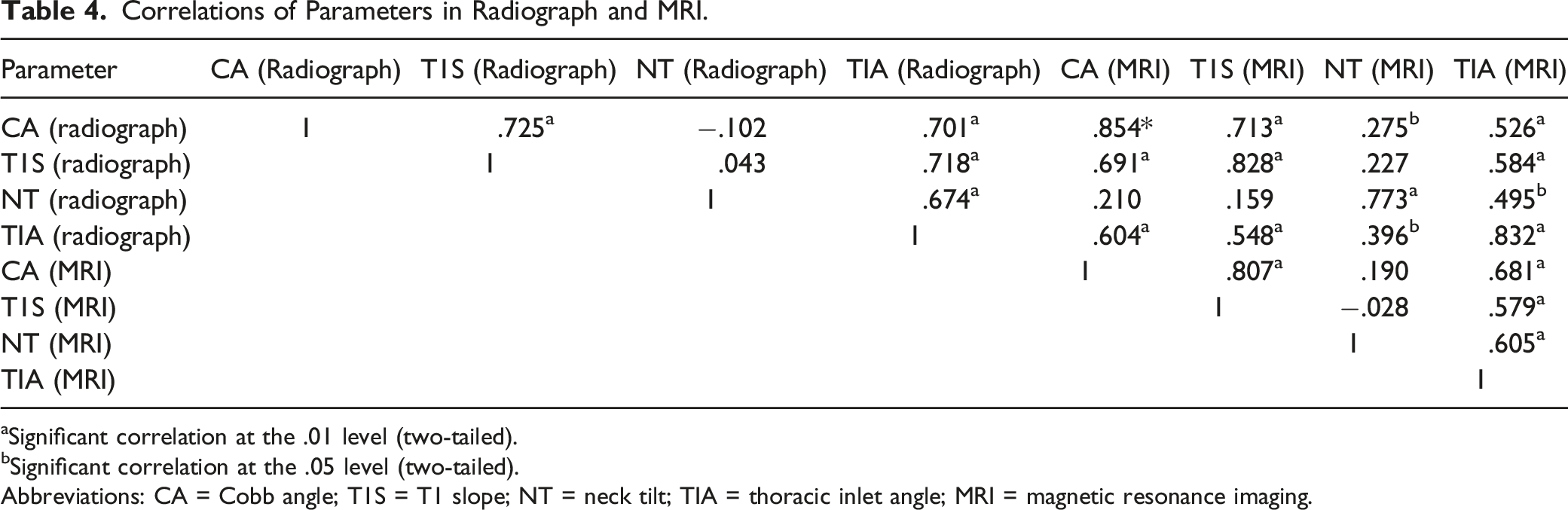
aSignificant correlation at the .01 level (two-tailed).
bSignificant correlation at the .05 level (two-tailed).
Abbreviations: CA = Cobb angle; T1S = T1 slope; NT = neck tilt; TIA = thoracic inlet angle; MRI = magnetic resonance imaging.
Discussion
Since it is related to the cervical sagittal alignment, the position of neck must be considered in imaging examination. Spine surgeons should notice the weight of the skull which adds compressive force to cervical spine in standing radiograph, while supine MRI is not affected by body weight. 16
Based on our results, we discovered two controversial findings that NT on radiograph was significantly smaller than on MRI, and TIA on radiograph was significantly larger than on MRI. These findings meant that both NT and TIA were influenced by positional change. Most of previous studies considered NT and TIA to be constant in different positions.11,16-18 Oshina et al. 11 believed that NT was relatively constant because the relationship between the sternal tip and the center of the T1 upper endplate did not change much with the position. Similar to pelvic incidence, Lee et al. 12 and Jun et al. 8 indicated that each individual had a specific TIA which remained constant whether changing position or increasing thoracic kyphosis. To find the reason for the new discoveries, we analyzed the detailed case history of our subjects, and found that 27.4% of them suffered severe neck pain, stiffness, and even myotonia. These clinical symptoms prompted the patients to keep a compulsive position of forward direction of skull and neck, which was more obvious in standing position. When the patients took supine position to perform MRI, their necks extended (backward) and the compulsive position was slightly relieved. At that time, the distance from the sternum tip to the center of T1 upper endplate was increased, and the cervical anteversion was corrected (which reduced T1 vertebra rotation). Thus, the NT became larger and TIA became smaller on MRI.
In our study, CA, T1S, and NT were significantly positively correlated with TIA on both radiograph and MRI. Lee et al. 12 pointed out that the physiological NT was around 44°, and proposed the geometric relationship, TIA = T1S + NT. According to the formula, while preserving physiological NT which maintained normal cervical lordosis, large TIA increased T1S and vice versa. 11 Therefore, for CSM patients undergoing anterior or posterior approach surgery with a high TIA due to a high position of the sternum tip or a thick thoracic cage, sufficient correction angle (T1S) related to suitable fusion cage and cervical lordosis restoration is essential for sagittal balance. In addition, CA was also positively correlated with T1S on both radiograph and MRI. This could be explained by the fact that the T1 vertebra rotation directly affected the cervical curvature, that was, larger T1S usually associated with greater CA. In a few cases, as we mentioned above, when the patients’ skull and neck were tilted forward because of the pain or stiffness, CA did not change significantly with the increase of T1S since cervical spine was in the hyperflexion position (tended to kyphosis). However, this kind of situation had little influence to the correlation between CA and T1S according to our results.
Although we have found positive correlations between CA and T1S, CA and TIA, and these parameters were mainly used in perioperative period, according to the feedback from our spine surgeon and radiologist, we believed that it was difficult to accurately determine the position of sternum tip and the center of T1 upper endplate when assessing the patients with unclear or thick or irregular manubrium sterni, arched T1 endplate, and severe degeneration. That was a common problem in almost all studies. Meanwhile, the correlation regression coefficients and constants summarized in domestic and foreign literatures are quite different. Therefore, the linear relationship and regression formula between these cervical parameters were still controversial.
As other scholars previously reported, there were significant differences in CA and T1S between standing and supine positions. Oshina et al. 11 showed that CA on radiograph was 2.37° larger than CA on MRI, and T1S on radiograph was 3.64° larger than T1S on MRI. That meant supine MRI underestimating the parameters. Besides, for each parameter, the measurements on MRI and radiograph had significantly correlations. Study by Xing et al. 18 also indicated that compared with standing radiograph, CA and T1S values were significantly lower on supine MRI. Our results were similar to these findings. When the neck was in flexion position, C4/5 and C5/6 segments had the largest range of motion, which made the measurements susceptible to posture changes and weight-bearing, even under axial load.19,20 Compared with supine MRI, this might be the reason for the significant increase of CA in standing radiograph. For most middle-aged and elderly patients, due to daily bad postures and cervical degeneration, the skulls were already displaced in the forward direction in a standing position. When performing supine MRI, the neck leant back and corrected the forward direction. Besides, the skull touched the table and exerted a reaction force of kyphosis tendency on neck. Thus, the decrease of T1 vertebra rotation produced smaller T1S on MRI.
Our findings have clinical implications that performing only MRI of CSM patients is not sufficient for surgeries, standing radiograph is also essential. Different positions have an important impact on cervical sagittal parameters. Considering that MRI can more clearly show the intervertebral disc, nerve root, spinal cord, and soft tissue, standing MRI is recommended, though it is not widely used.
The current study has several limitations. Firstly, we didn’t perform full-length radiographs which could help observing the whole sagittal alignment and make the analysis more comprehensive. Secondly, the relatively small sample size. Contrary to the widely accepted view, we found that NT and TIA changed with positions, and explained that the forward direction of skull and neck might be the influence factor. However, further expanding our sample population will eliminate coincidence as much as possible, or even obtain a definite subversive result. Finally, we acquired all measurements under static conditions and didn’t take dynamic adjustments into consideration. We should notice that in standing position, gravity may change the correlation between cervical parameters through a potential adaptive mechanism. Therefore, high-quality, large sample, and multicenter studies should be performed in our future clinical work to provide spine surgeons with the best evidence-based information.
Conclusion
There were significant differences between standing radiograph and supine MRI in CA, T1S, NT, and TIA. Supine MRI obviously underestimated the value of CA, T1S, and TIA. Therefore, standing cervical radiographs should be obtained in CSM patients to assess and determine surgical strategy, not only supine MRI. Moreover, we observed that NT and TIA were not constant morphological parameters. However, higher-quality studies should be performed to improve the accuracy and reliability of the findings, and further clinical correlation should be evaluated in future works.
Footnotes
Authors’ Contributions
XCQ, SQX and XJH are co-first authors of this manuscript. XCQ, SQX and XJH designed the study and collected the data. XJH and MJM did the data analysis. XCQ wrote the manuscript. YJ and MW revised the manuscript and decided to submit the manuscript for publication. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
All authors read and approved the final manuscript and declare that they have no competing interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The case was reviewed by the Longhua Hospital Ethics Committee and ethical approval was waived as written consent was obtained from the patient.; Consent for publication
Consent to Participate
Written patient consent was obtained for publication of all aspects of the case including personal and clinical details and images, which may compromise anonymity.
Availability of Data and Material
All supporting data can be provided upon request to the authors.