
Abstract
Study Design
Retrospective study.
Objective
To investigate the relative curve correction of Proximal Thoracic (PT) and Main Thoracic (MT) scoliosis curves and their relationship with post-operative UIV tilt angle as well as post-operative shoulder imbalance.
Methods
151 AIS patients with Lenke type 1 and 2 curves who underwent PSF were reviewed. Relative PT/MT Correction Rate (RCR), Relative PT/MT Residual Cobb angle (RRCA) and Post-operative UIV Tilt Angle were investigated for their association with post-operative T1 tilt (medial shoulder balance), Cervical Axis (neck balance) and Clavicle Angle (Lateral Shoulder Balance).
Results
There were 107 patients with Lenke 1 curves and 44 patients with Lenke 2 curves. Overall, the prevalence of medial shoulder, neck and lateral shoulder imbalance was 27.8%, 23.2% and 9.9%, respectively. There was a significant association between RRCA and medial shoulder, lateral shoulder and neck balance but RCR had a significant association with lateral shoulder and neck balance. There was a significant and strong correlation (r = 0.708) between post-operative UIV tilt angle and post-operative T1 Tilt. Unlike RCR, RRCA had shown a statistically significant correlation to post-operative UIV tilt angle with an r-value of 0.406.
Conclusions
RRCA had shown a statistically significant correlation with the post-operative UIV tilt angle, and post-operative T1 tilt ie, medial shoulder balance. However, the post-operative UIV tilt angle showed the strongest strength of correlation with the post-operative T1 tilt (r = 0.708).
Keywords
Introduction
Shoulder balance plays a significant role in the overall cosmetic appearance among patients with adolescent idiopathic scoliosis (AIS). 1 Post-operative shoulder imbalance (PSI) is common following posterior spinal fusion (PSF) surgery. 2 The incidence of PSI among scoliosis patients post-operatively was reported to be up to 25%. 3 Shoulder imbalance which comprises the medial shoulder, lateral shoulder as well as neck are represented by radiographic parameters of TI Tilt, Clavicle Angle and Cervical Axis, respectively.3-8
Recently, 2 important risk factors of PSI have been reported, ie, relative curve correction of the proximal thoracic curve/main thoracic curve (PTC/MTC) and the upper instrumented vertebra (UIV) tilt angle. Lee et al had emphasized that PSI was associated with higher Risser grade, larger post-operative proximal wedge angle (PWA) and greater post-operative PTC/MTC ratio 4 in Lenke 2 curves. Yuan et al also highlighted the importance of harmonizing the correction rate ratio of the PTC, MTC and LC in their study. 6 As for the UIV tilt angle, this radiological parameter is an independent variable that significantly correlates with post-operative T1 Tilt and Cervical Axis measurement. 9 Patients with positive post-operative UIV tilt angle were 14.9 times more likely to experience positive medial shoulder imbalance (T1 tilt angle ≥+4°) and 3.3 times more likely to experience positive neck imbalance (cervical axis ≥+4°). 10 Therefore, achieving the optimal UIV tilt angle may prevent neck tilt with medial shoulder imbalance due to trapezial prominence but not lateral shoulder imbalance. 11
To date, the correlation between these 2 factors ie, Relative Curve Correction (RCC) and Post-operative UIV Tilt Angle is yet to be fully investigated. Therefore, the purpose of this study is to investigate the RCC and its relationship with Post-operative UIV Tilt Angle as well as post-operative shoulder imbalance.
Methodology
Statement
Informed consent was not required for this study as it is a retrospective study. The study was deemed exempt from the requirement for informed consent by the institutional Medical Research Ethics Committee (MREC).
Study Design
This was a retrospective study that was carried out in a single tertiary academic centre. 151 AIS patients with Lenke type 1 and 2 curves who underwent PSF between 2019 to 2021 were reviewed. The institutional ethical approval was obtained prior to the commencement of the study (MREC ID NO: 2023519-12466). The inclusion criteria included AIS patients with Lenke 1 and 2 curves, patients with sufficient clinical and radiological parameters with at least 24 months follow-up post-operatively. Patients with non-idiopathic scoliosis, juvenile scoliosis and congenital scoliosis and patients who underwent anterior spinal fusion surgery, two-staged surgery or revision surgery were excluded from the study.
The null hypothesis proposed that there was no significant association between relative curve correction, post-operative UIV tilt angle and post-operative medial, neck and lateral shoulder balance.
The objectives of this study were to investigate (comparing between Lenke 1 and Lenke 2): 1. The prevalence of radiological medial shoulder, neck and lateral shoulder imbalance at the final follow-up. 2. The association between medial shoulder, neck and lateral shoulder imbalance with Relative Curve Correction (RCC) and Post-operative UIV Tilt Angle. 3. The association between RCC and Post-operative UIV Tilt Angle.
Definition of Shoulder Balance Parameters
PSI is divided into 2 components which are lateral and medial shoulder balance. Medial shoulder balance is represented by T1 Tilt whereas lateral shoulder balance is represented by Clavicle Angle.
12
The Cervical Axis represents the neck tilt.8,13 The parameters14-17 were defined and illustrated as shown below (Figure 1): Illustration of T1 Tilt, Clavicle Angle, Cervical Axis and UIV tilt angle measurements.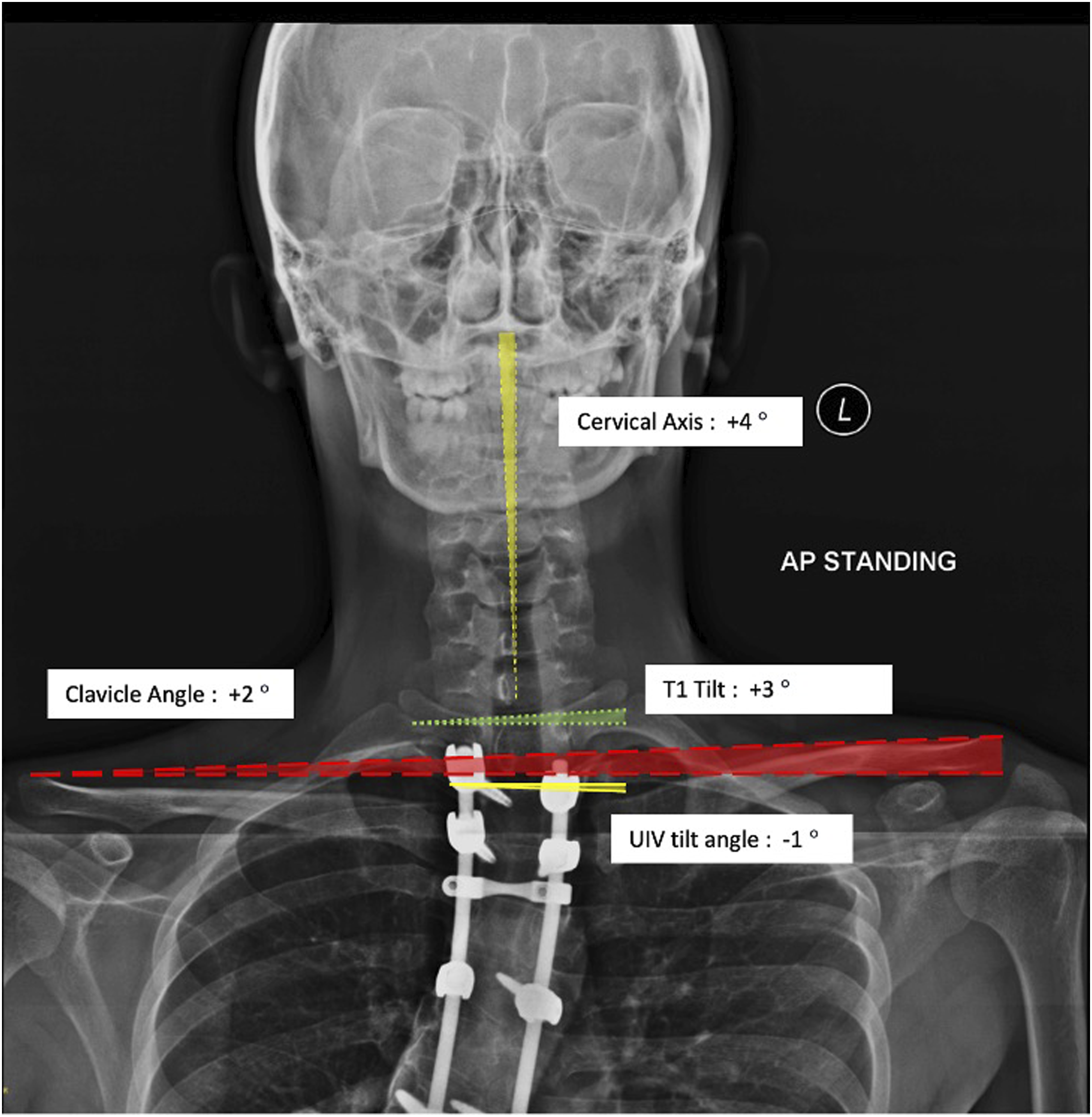
T1 Tilt
Angle (in degree) is formed between a horizontal line and a line drawn along the parallel to the superior end plate of the T1 vertebrae. This parameter is directional. When the T1 Tilt is tilted towards the right, it is regarded as a positive (+) value and vice versa.
Clavicle Angle
Angle (in degree) is formed by the intersection of a horizontal line and a line connecting the highest 2 points of each clavicle. This parameter is directional. When the Clavicle Angle is tilted towards the right, it is regarded as a positive (+) value and vice versa.
Cervical Axis
Angle (in degree) between the longitudinal axis of cervical spine (centre of C2 odontoid process and centre of C7) and the vertical axis. This parameter is directional. When the Cervical Axis is tilted towards the right, it is regarded as a positive (+) value and vice versa.
Upper Instrumented Vertebra (UIV) Tilt Angle
Angle (in degree) is formed by the intersection between a horizontal line and a parallel line drawn to the upper end plate of the UIV. This parameter is directional. When the UIV tilt angle is tilted towards the right, it is regarded as a positive (+) value and vice versa 10
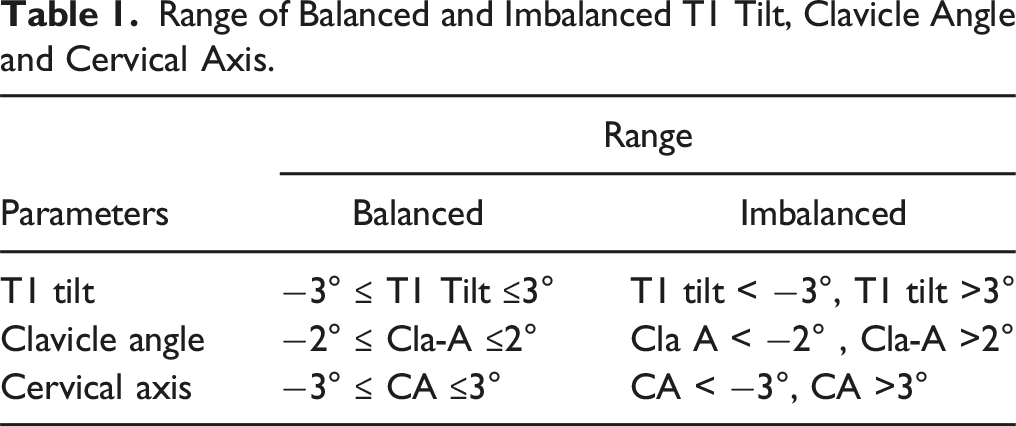
Range of Balanced and Imbalanced T1 Tilt, Clavicle Angle and Cervical Axis.
Relative curve correction was assessed using these radiological parameters:
(1). Relative PT/MT Correction Rate (RCR): This parameter is the ratio of the Correction Rate (CR) of the PT curve to the MT curve. This parameter is reported as a percentage whereby a value of 100% indicates the RCR is equal.
(2). Relative PT/MT Residual Cobb angle (RRCA): This parameter is the ratio between the post-operative Cobb Angle of the PT to the MT curve. This parameter is reported as a percentage whereby a value of 100% indicates the RRCA is equal.
Data Collection
Participating surgeons measured the PT Cobb angle, MT Cobb angle, PT side bending Cobb angle, MT side bending Cobb angle, UIV tilt angle, T1 Tilt, Clavicle Angle as well as Cervical Axis pre-operatively and post-operatively. Then, the PT correction rate, MT correction rate and RCR and RRCA percentages were calculated. RCR, RRCA and UIV tilt angle were correlated with PSI parameters while RCR and RRCA were correlated with UIV tilt angle.
Surgical Strategy
All patients underwent PSF using pedicle screws construct. Alternate level pedicle screw placement was implemented. Correction maneuver consisted of rod translation technique and direct vertebral derotation. Radical facetectomies were performed to increase spinal flexibility prior to correction as well as to augment the fusion process. Autogenous bone grafts obtained from the spinous processes, laminae, facet joints and transverse processes were processed and distributed over the fusion bed. The UIV in Lenke 1 curves were at T3, T4, or T5 when the right medial shoulder was high or when the medial shoulder was balanced. Fusion to T2 was performed when the left medial shoulder was high. In Lenke 2 curves, the UIV were T1 or T2 when the left medial shoulder was high and T3 when it was level or the right medial shoulder was high. The optimal UIV tilt angle can be calculated from the Supervised Supine Side Bending radiographs preoperatively (11) and confirmed during surgery using the crossbar method (17).
Statistical Analysis
SPSS Version 27.0 (SPSS Statistics for Windows, IBM Corp, Armonk, NY, USA) was utilised for data analysis. Pearson chi-squared test and Fisher’s exact test were used to analyse the categorical parameters. Shapiro-Wilk tests of normality were run for continuous parameters. Normally distributed parameters were analysed using Independent sample t-test and reported in mean and standard deviation or percentages. Non-normally distributed parameters were analysed by Mann-Whitney U Test non-parametric test and reported in median and interquartile range. 0.05 was the cut-off point of statistical significance applied. Pearson correlation analysis was used to determine the correlations and relationships between variables.
Results
Patient Demographics and Pre-operative Parameters.
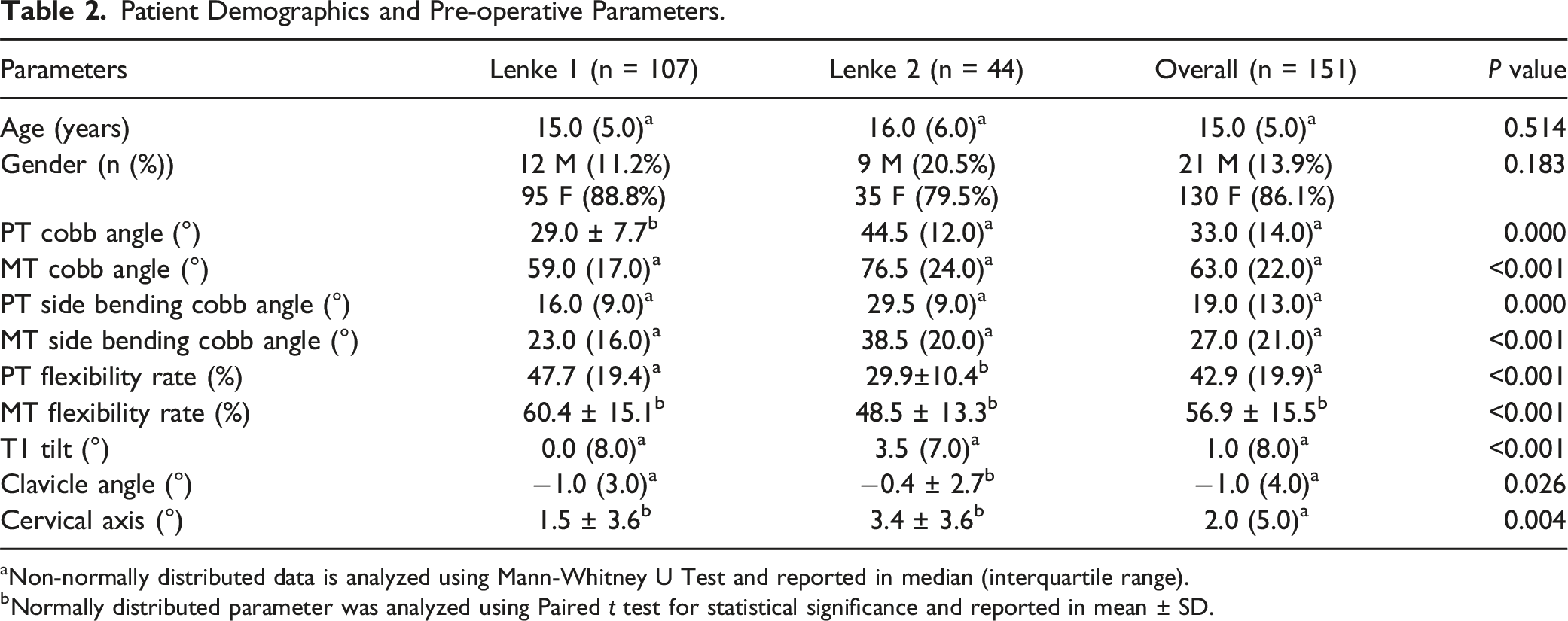
aNon-normally distributed data is analyzed using Mann-Whitney U Test and reported in median (interquartile range).
bNormally distributed parameter was analyzed using Paired t test for statistical significance and reported in mean ± SD.
Patient Post-operative Parameters.
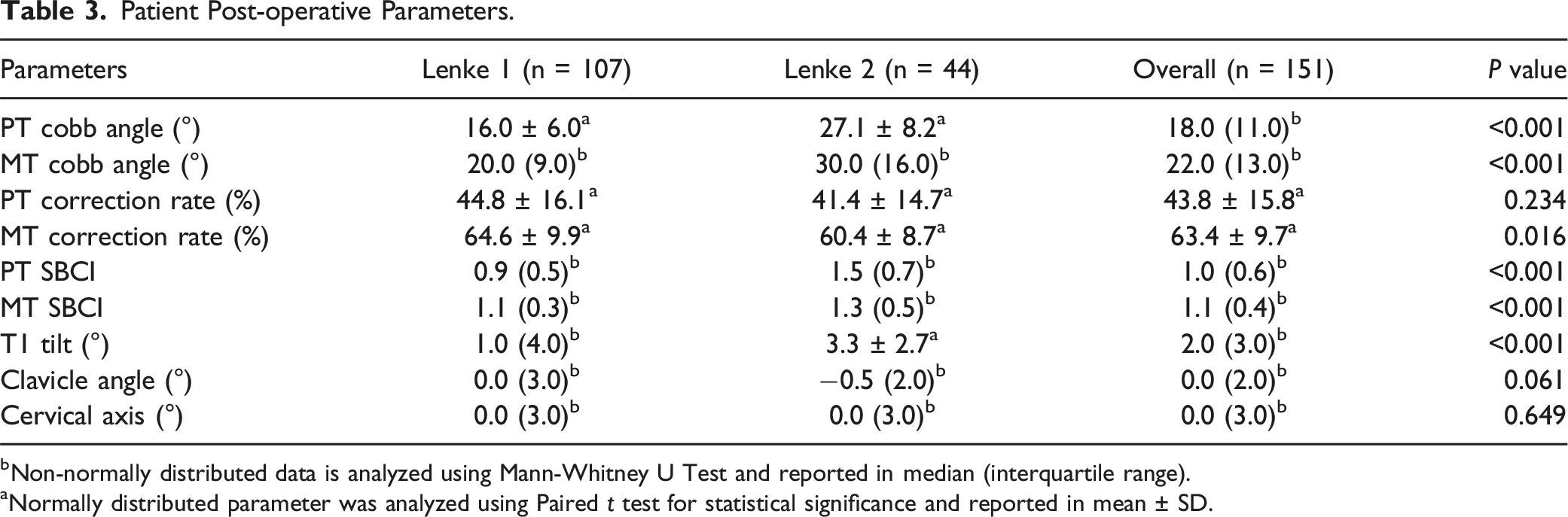
bNon-normally distributed data is analyzed using Mann-Whitney U Test and reported in median (interquartile range).
aNormally distributed parameter was analyzed using Paired t test for statistical significance and reported in mean ± SD.
Post-operative Medial Shoulder (T1 Tilt), Lateral Shoulder (Clavicle Angle) and Neck (Cervical Axis) Balance.
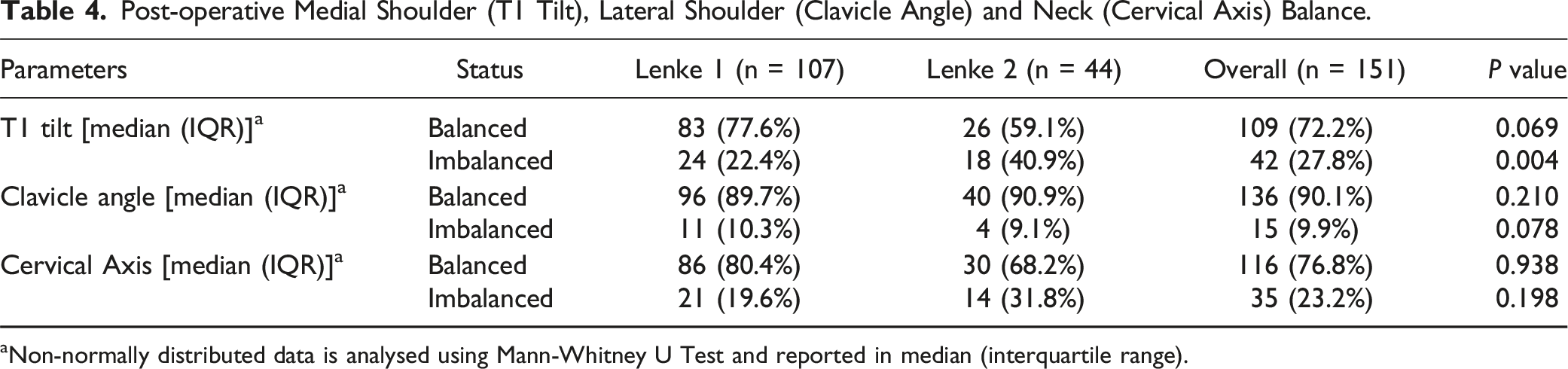
aNon-normally distributed data is analysed using Mann-Whitney U Test and reported in median (interquartile range).
RCR and RRCA in the Balanced and Imbalanced Medial Shoulder (T1 Tilt), Lateral Shoulder (Clavicle Angle) and Neck (Cervical Axis).
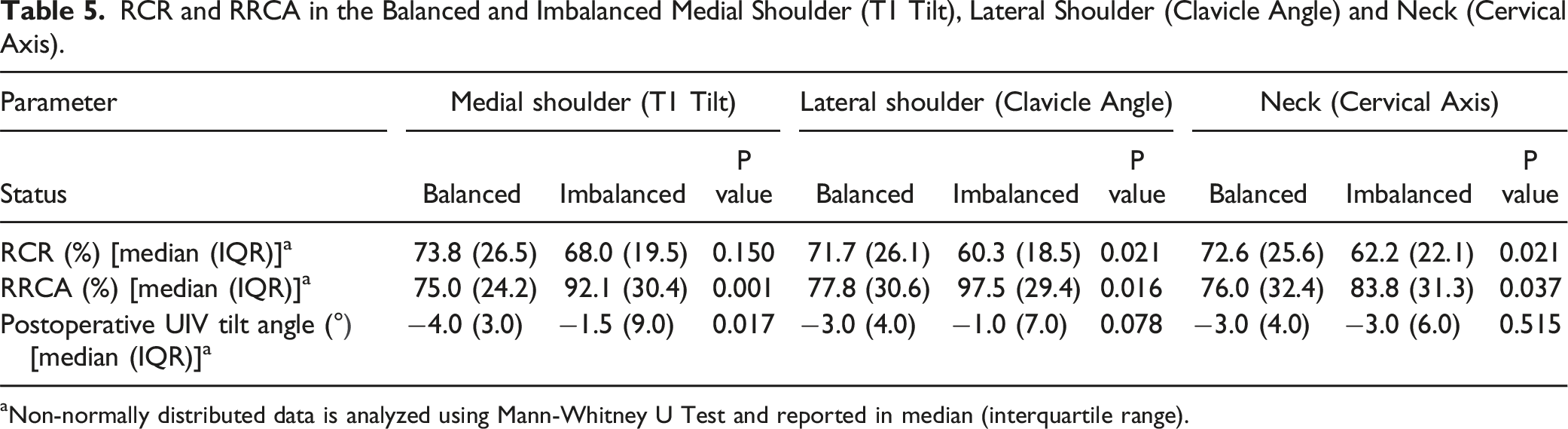
aNon-normally distributed data is analyzed using Mann-Whitney U Test and reported in median (interquartile range).
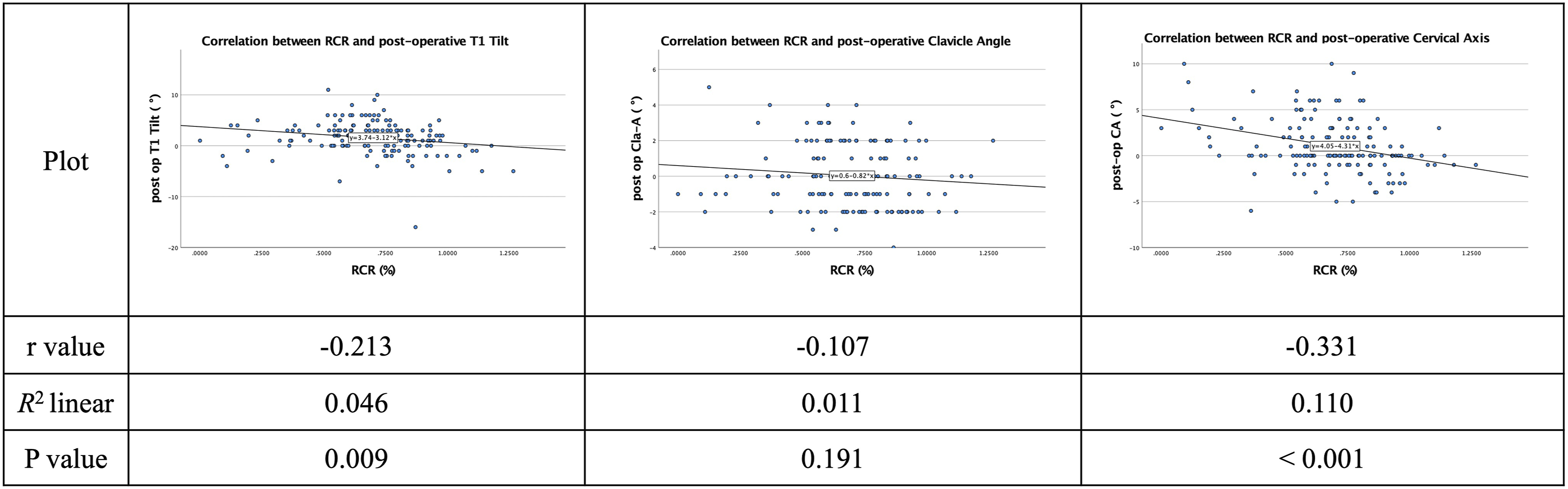
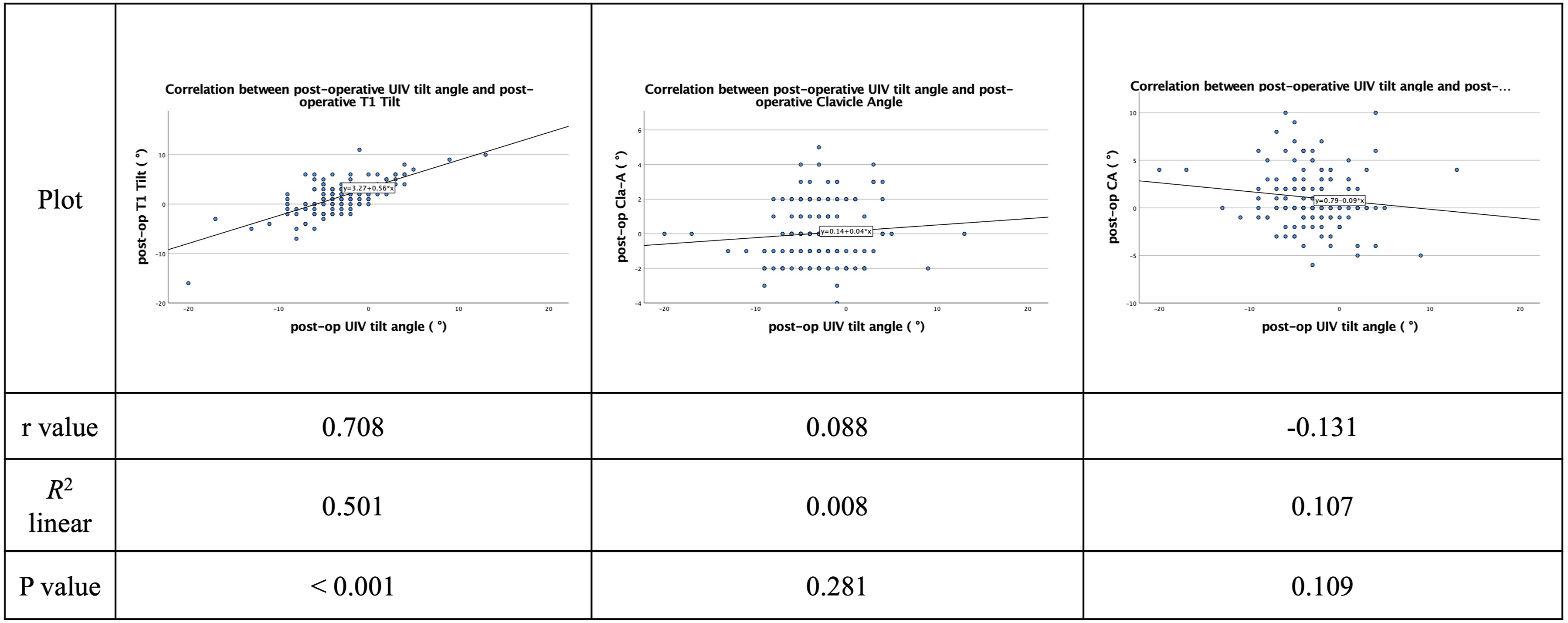
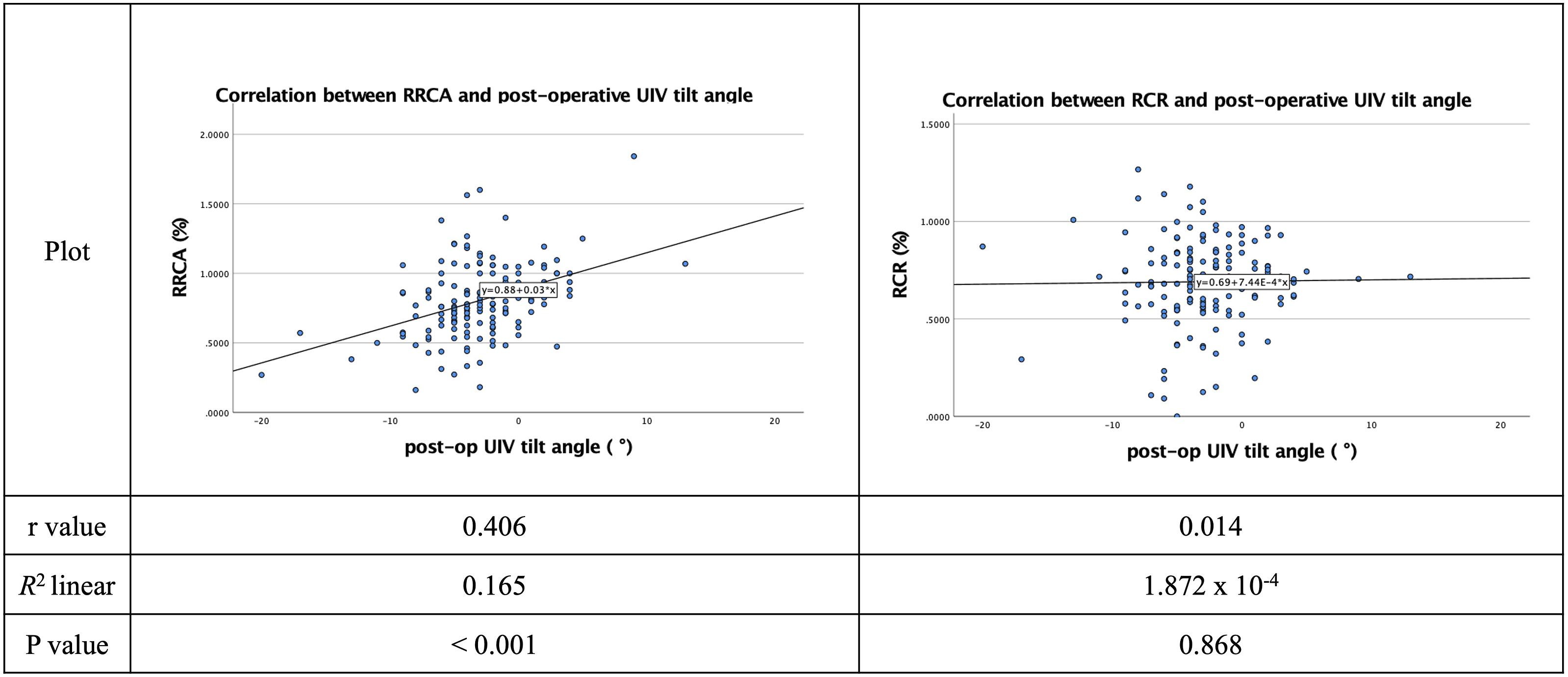
Post-operative T1 Tilt had a significant correlation (P < 0.001) with RRCA with a moderate strength of correlation (R = 0.628) (Figure 2). RCR was found to have a significant correlation with post-operative T1 Tilt (P = 0.009) and post-operative Cervical Axis (P < 0.001). However, all parameters had shown a weak correlation to RCR (Figure 3). There was a significant and strong correlation (r = 0.708) between post-operative UIV tilt angle and post-operative T1 Tilt (P < 0.001). (Figure 4). Unlike Relative Correction Rate (RCR), Relative Residual Cobb Angle (RRCA) had shown a statistically significant correlation (P < 0.001) to post-operative UIV tilt angle with an r-value of 0.406 (Figure 5). Correlation between Relative Residual Cobb Angle (RRCA) and post-operative T1 Tilt, Clavicle Angle and Cervical Axis in Lenke 1 and Lenke 2 patients. Correlation between Relative Correction Rate (RCR) and post-operative TI Tilt, Clavicle Angle and Cervical Axis in Lenke 1 and Lenke 2 patients. Correlation between post-operative UIV tilt angle vs post-operative T1 Tilt, Clavicle Angle and Cervical Axis in Lenke 1 and Lenke 2 patients. Correlation between Relative Residual Cobb Angle (RRCA) and Relative Correction Rate (RCR) vs post-operative UIV tilt angle in Lenke 1 and Lenke 2 patients.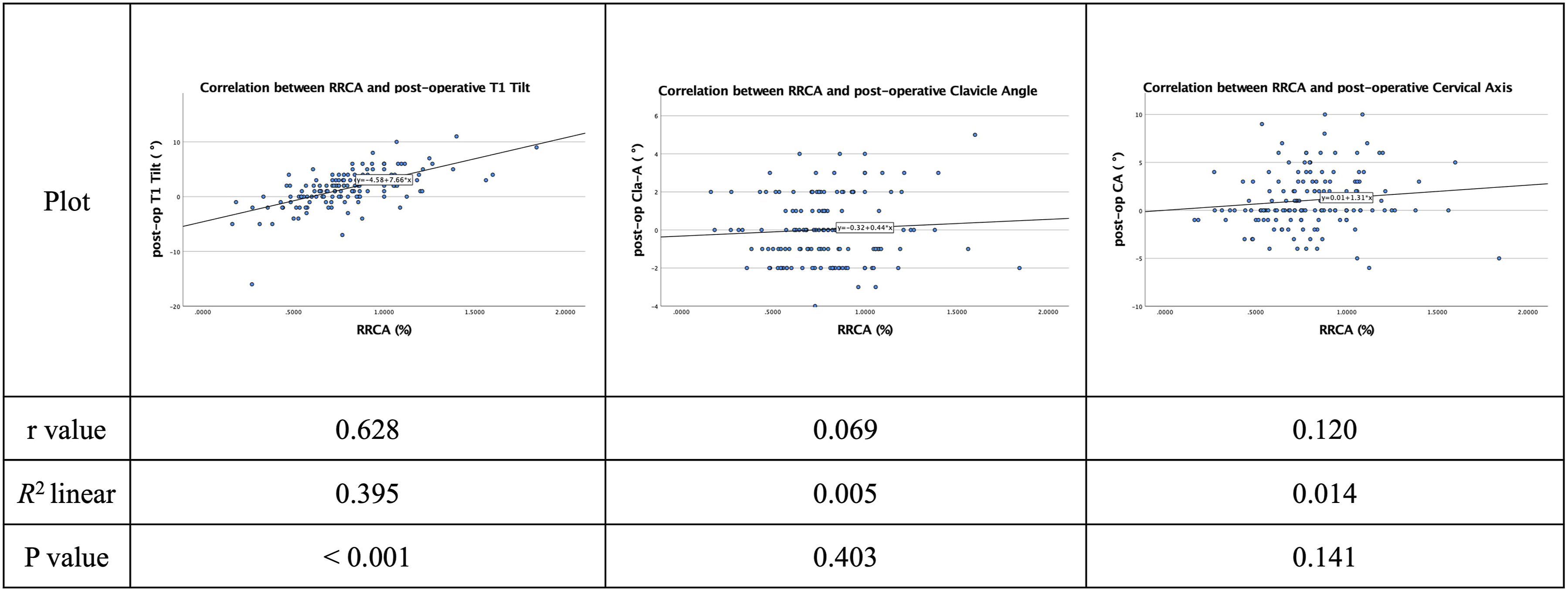
The correlation analysis among the 3 factors (T1 tilt, clavicle angle, and cervical axis) showed no significant difference: T1 tilt and clavicle angle (r = 0.140, P = 0.087), T1 tilt and cervical axis (r = 0.114, P = 0.162), and cervical axis and clavicle angle (r = 0.132, P = 0.105).
ROC Analysis of RCR and RRCA for Medial Shoulder (T1 Tilt), Lateral Shoulder (Clavicle Angle) and Neck (Cervical Axis) Balance.
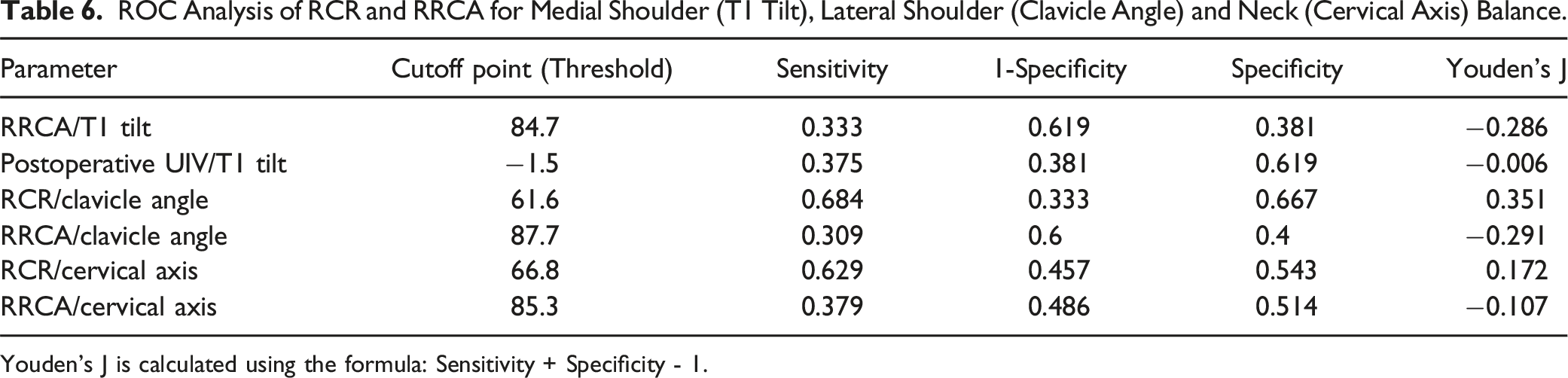
Youden’s J is calculated using the formula: Sensitivity + Specificity - 1.
Cut-Off Point of RCR and RRCA for Medial Shoulder (T1 Tilt), Lateral Shoulder (Clavicle Angle) and Neck (Cervical Axis) Balance.
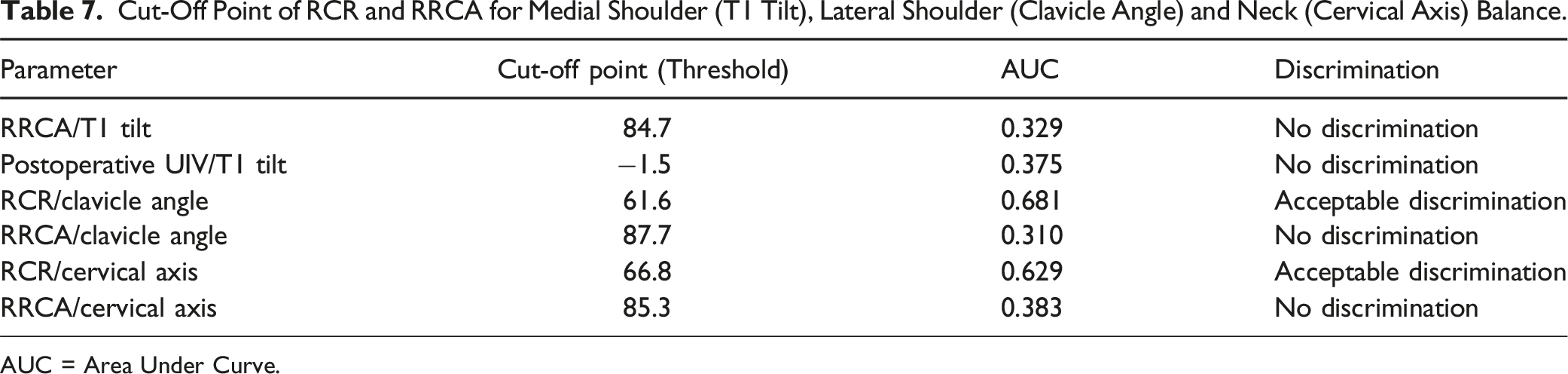
AUC = Area Under Curve.
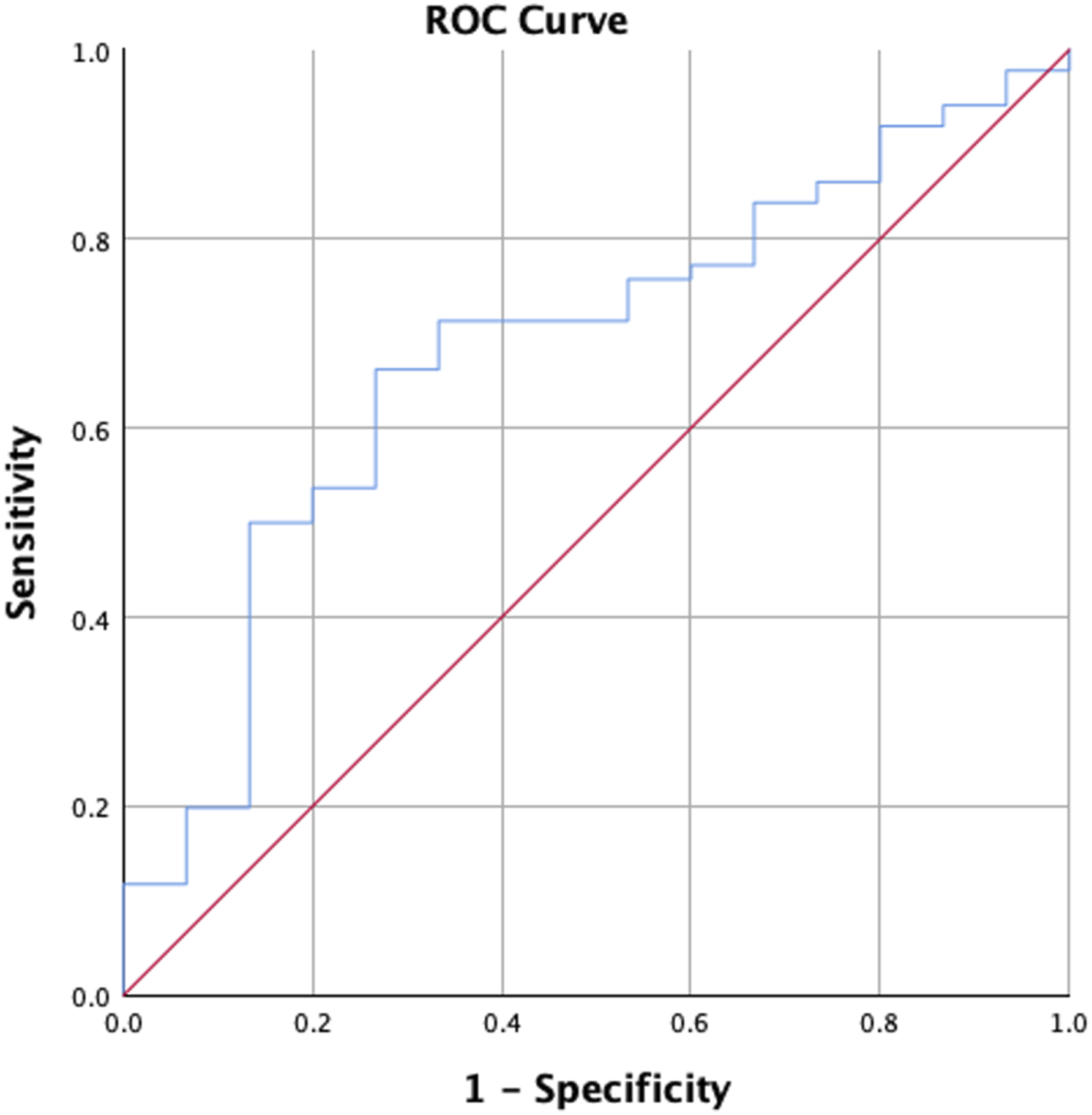
Receiver-operating-characteristic (ROC) of RCR/clavicle angle analysis showed acceptable discrimination of area under the curve (AUC) of 0.681 (P = 0.68). The cut-off value 61.6% had a sensitivity of 0.684 and specificity of 0.667.
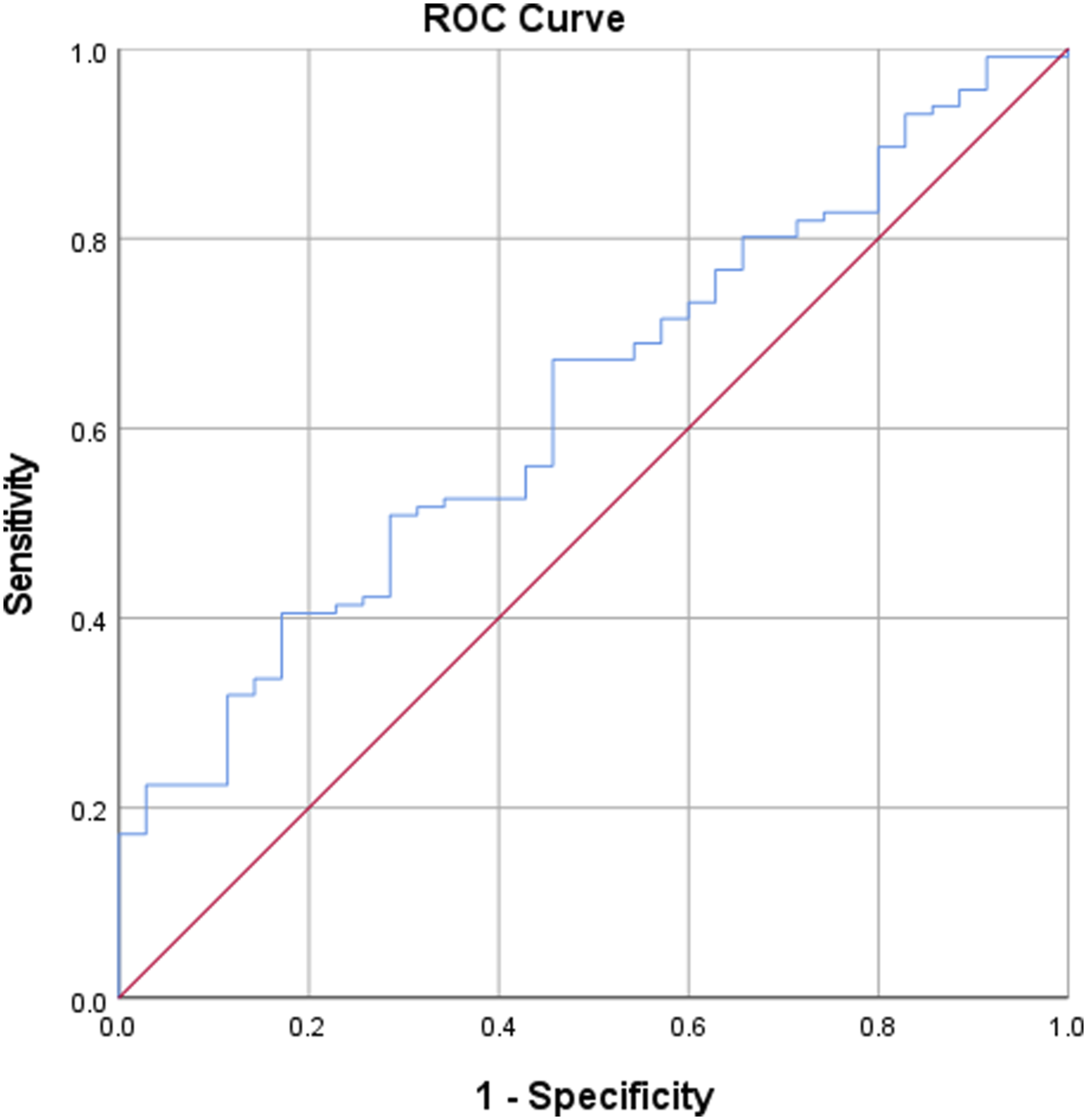
Receiver-operating-characteristic (ROC) of RCR/cervical axis analysis showed acceptable discrimination of area under the curve (AUC) of 0.629 (P = 0.50). The cut-off value 66.8% had a sensitivity of 0.629 and specificity of 0.543.
Discussion
Despite various recommendations and strategies to achieve post-operative shoulder balance, PSI is still a common occurrence among AIS patients.18-21 The occurrence of PSI post-PSF surgery is 1 of the factors that contributes to poor satisfaction among AIS patients, especially in those with left shoulder elevation pre-operatively.22,23 Bram et al revealed that severe PSI could be predicted by pre-operative PT Cobb angle >34.5° in which 44.4% of patients would develop severe PSI after 2 years. 23 Earlier studies had focused mainly on UIV selection and advocated the fusion of the proximal thoracic curve to reduce the incidence of PSI.24,25
However, recent studies had shown that PSI might stem from over-correction of the MT curve and under-correction of the PT curve. Sielatycki et al reported that 59% of patients developed shoulder imbalance when the correction of the MT curve was more than 54% while the correction of the PT curve was less than 52%. 26 Berlin et al had also concluded that MT correction of more than 64.9% and lumbar correction of more than 93.2% had resulted in PSI in 51.9% of AIS patients with Lenke 2 curves. 27 This was further supported by Landrum et al who had proposed the idea of Thoracic Curve Correction Ratio (TCCR) which was the PT/MT correction rate divided by pre-operative PT/MT Cobb angle. 28 TCCR had a significant correlation with post-operative T1 Tilt. 28 In a retrospective study involving 104 Lenke 1 patients, Banno et al found that PSI was associated with a higher MT correction. 29
Therefore, we postulated that relative correction of the PT curve to the MT curve would ultimately affect the position of the upper instrumented vertebrae, and this could be associated with the UIV tilt angle. The concept of UIV tilt angle was introduced in 2016. 11 Patients were reported to have lower risk of clinical neck tilt with medial shoulder imbalance if their UIV tilt angle was within their UIV’s reserve motion. 11 Besides that, they also discovered that the difference in UIV tilt angle (UIVDiff) had a strong correlation with medial shoulder balance (represented by T1 Tilt) and a moderate correlation with neck balance (represented by Cervical Axis). 11 Subsequent published literature had shown that post-operative UIV Tilt Angle was an independent variable that significantly correlated with post-operative T1 Tilt (r = 0.76) and Cervical Axis measurement (r = 0.42). 9
Patients with positive post-operative UIV tilt angle were also at higher risk (14.9x) of having medial shoulder imbalance. 10 Among 136 AIS patients with Lenke 1 and 2 curves, there were 51.6% of patients with positive post-operative UIV tilt angle and medial shoulder imbalance. 10 Zhang et al introduced a formula to predict the ideal post-operative UIV tilt: ideal post-operative UIV tilt = pre-operative UIV tilt - the flexibility between T1 and UIV – pre-operative CA. 30 The importance of UIV tilt angle was also investigated by Deng et al who reported that 69.2% of Lenke 2 AIS patients suffered from medial shoulder imbalance post-operatively even though lateral shoulder balance had been achieved. 31 They concluded that the significant predictors for medial shoulder imbalance were post-operative UIV tilt angle (P < 0.001), PT correction rate (P < 0.001), ratio of PTC/MTC (P < 0.001) and T2 vertebra rotation ratio (P = 0.008). 31 To date, no studies have been carried out to investigate the association between PT/MT relative curve correction and post-operative UIV tilt angle.
In this study, the relative curve correction of the PT/MT segment based on the Relative Correction Rate (RCR) and the Relative Residual Cobb angle (RRCA) was assessed. Higher RCR would indicate a higher correction rate of PT curve than MT curve whereas higher RRCA would indicate a higher post-operative PT Cobb angle than MT Cobb angle. The results of this study showed that RRCA had a stronger correlation with medial shoulder balance compared to RCR. UIV tilt angle and medial shoulder balance had the strongest correlation (r = 0.708). There was also a significant correlation between RRCA and UIV tilt angle (r = 0.406) but not with RCR. This is the first study to elucidate the association between RRCA, RCR and post-operative UIV tilt angle. From a practical point of view, surgeons must be cognizant of the importance of PT segment correction as this segment is inherently stiffer than the MT segment.32-35
Therefore, relative under-correction of the PT segment in relation to the MT segment is common and this could lead to medial PSI. RRCA illustrates a concept whereby PT correction should be optimised to avoid PSI. However, the post-operative UIV tilt angle offers the surgeons an objective target and this can be determined pre-operatively. The formula to calculate the optimal UIV tilt angle based on the supervised supine side bending films; Optimal UIV tilt angle = - ((RSB angle + LSB angle) / 2). 11 Furthermore, this target can be confirmed intra-operatively using the crossbar method. 36 As it is a highly objective measurement, understanding this radiological parameter is imperative to prevent medial PSI.
This study however has several limitations. The assessment of the medial, neck and lateral shoulder balance are represented by radiological parameters. Additional clinical assessment could strengthen the study despite these radiological parameters had been previously validated.7,16,37-39 The final assessment of the radiological outcome was carried out at minimum 2 years follow-up. Longer follow-up duration could reflect the final outcome more accurately. Although the concept of RRCA is important, it is difficult to predict it pre-operatively and to quantify and execute during the surgery. More studies would be needed to validate the concept of RRCA and its association with PSI.
Conclusion
In conclusion, the prevalence of post-operative medial shoulder, neck and lateral shoulder imbalance was 27.8%, 23.2% and 9.9%, respectively. RRCA and post-operative UIV tilt angle had shown a significant correlation with medial shoulder balance, but post-operative UIV tilt angle had shown the strongest strength of correlation (r = 0.708). RRCA had shown a statistically significant correlation with post-operative UIV tilt angle with a r-value of 0.406.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.