
Abstract
Study Design
Cross-sectional Survey.
Objectives
The objective of this study was to describe clinicians’ decision-making regarding suitability of patient cases for lumbar fusion surgery or conservative care and the level of equipoise to randomise participants into a randomised controlled trial (RCT).
Methods
An online survey distributed via Australian professional networks to clinicians involved in low back pain care, collected data on clinical discipline, clinical experience, practice setting and preferred care of five patient case vignettes (ranging in age, pain duration, BMI, imaging findings, neurological signs/symptoms). Clinicians were asked about preferred clinical care and willingness to randomise each case.
Results
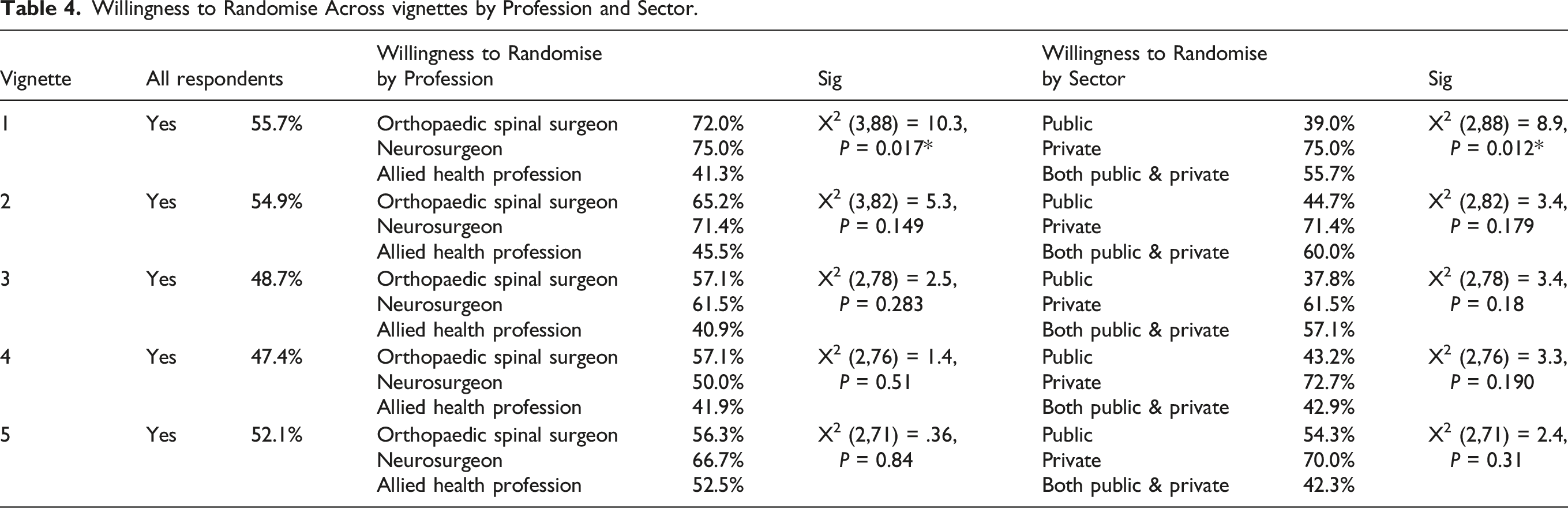
Of 101 respondents (31 orthopaedic surgeons, 17 neurosurgeons, 50 allied health professionals (AHPs), 1 pain physician, 1 nurse), 44% worked in public health services only, 36.4% in both public and private, 19.2% in private only. 46.5% had over 20 years clinical experience. Conservative care was preferred for all cases (83.1%–90.9%). Surgeons preferred an anterior approach to lumbar fusion (range 40.6%–68.4%). On average 51.9% (range: 47%–55%) indicated willingness to randomise cases, with orthopaedic (61.5%) and neurosurgeons (64.9%) more willing than AHPs (44.4%). Willingness to randomise was highest in younger cases with shorter pain duration, no neurological symptoms/signs and localised degeneration, and lowest when cases had high BMI, longer pain duration, and inadequate conservative management. Willingness to randomise was higher in those in private (70.3%) vs public health care services (43.6%).
Conclusions
Over half of respondents reported willingness to randomise cases, indicating sufficient clinical equipoise for a future RCT.
Introduction
Persistent low back pain (LBP) is the leading cause of disability worldwide. 1 It causes significant burden for individuals, communities and society more broadly, with an estimated $4.8 billion Australian dollars spent managing persistent LBP in Australia per year. 2 While most individuals will recover from an episode of acute LBP, 3 recurrence rates are high and around 33% will have another episode of LBP within 12 months.4,5 Many clinical guidelines around the world advocate education, physical and psychological interventions for persistent LBP, reserving invasive treatments for specific groups of patients such as those who do not respond to conservative care.6-8
While evidence supports the role of decompressive surgery in the management of LBP in the presence of neurological compromise including radicular leg pain following disc herniation9,10 or neurogenic claudication resulting from spinal canal stenosis, 11 the indication for stabilisation spinal surgery for LBP associated with degenerative findings on spinal imaging, in the absence of neurological compromise, is less clear. The uncertainty regarding the role of lumbar fusion surgery for treatment of degenerative LBP led to The National Institute for Clinical Excellence (NICE) guidelines recommending against it use unless as part of a randomised controlled trial (RCT). 6 Worldwide, only six RCTs have been conducted evaluating lumbar spine fusion surgery vs non-surgical care,12-17 summarised in several systematic reviews, with the most recent meta-analysis 18 showing a between group difference of 7.51 points on the Oswestry Disability Index (ODI) scores in favour of surgery at two years follow-up, a difference that was not statistically significant. Surgical complication rates are reported to be between 9%–18%. 19 Where longer term RCT follow-up data have been published (mean 12.8 years, range 9-22 years) these show similar outcomes in ODI scores between surgical and non-surgical groups. 16 Criticisms of previous trials include small samples, large cross-over, and varied non-surgical care. Where non-surgical care comprised more intensive physiotherapy and cognitive behavioural therapy approaches, results were similar to surgery. 20 Trials concluding surgery was superior to conservative care have tended to offer less intensive conservative interventions (eg, stretching and walking), 17 or physical therapy that was inadequately described, 21 in populations that have likely already undergone (and failed) these treatments. Despite the collective uncertainty about the place of lumbar spine fusion surgery for degenerative LBP, and the wide variation in rates of this type of surgery across Australia, 22 the overall rate has increased, particularly in the Australian private sector.23,24
Based on the above RCT evidence, the collective uncertainty is also reflected in clinical practice guidelines. The American Pain Society guidelines conclude that lumbar fusion surgery is no better than intensive rehabilitation combined with cognitive behavioural therapy, but slightly superior to standard, non-intensive conservative management. 25 In the UK, NICE released guidance on the management of LBP which stated that lumbar spinal fusion surgery should not be offered for the management of degenerative low back pain except as part of a clinical trial. 6 This prompted calls in 2021 from the National Institute for Health Research (NIHR) Health Technology Assessment (HTA), and through collaboration with the Australian National Health and Medical Research Council (NHMRC), for new RCT evidence comparing lumbar fusion surgery with conservative care for persistent degenerative LBP.
In response, two, soon-to-commence RCTs - FusiOn veRsus bEst coNServatIve Care (the FORENSIC-UK and FORENSIC-Australia trials) will compare lumbar fusion surgery vs continued best conservative care in individuals with persistent severe LBP and who have imaging evidence of lumbar spine degenerative changes. In advance of these trials being conducted, it is important to better understand i) which clinical features of patients mean that health care professionals are more likely to consider lumbar fusion surgery or conservative care to be the most appropriate treatment, and ii) whether the necessary equipoise (ie, collective clinical uncertainty) exists amongst health care professionals for randomisation of cases into either intervention arm. A recent cross-sectional survey concluded that the necessary equipoise exists amongst UK health care professionals. 26 The aims of this study were to describe Australian health care professionals’ decision-making about the suitability of case examples of patients for either lumbar fusion surgery or best conservative care, and to determine if there is sufficient equipoise to randomise participants into each arm of the future FORENSIC-Australia trial.
Materials and Methods
Design and Setting
A cross-sectional electronic survey was developed and distributed to health care professionals in Australia involved in the management of patients with LBP, between June-July 2023. Ethics approval was obtained from the University of Queensland Human Research Ethics Committee (2023/HE000438). Consent was assumed if individuals completed and submitted survey responses.
Questionnaire Sampling and Mailing Process
The sampling frames comprised relevant professional bodies in Australia (Spine Society of Australia, Australian Pain Society, Neurosurgical Society of Australasia, Australian Physiotherapy Association) in addition to Australian email distribution lists accessible to the authors (Queensland Neurosurgical/Orthopaedic Physiotherapy Screening Clinic and Multidisciplinary Service, Queensland Directors of Physiotherapy) and through highlighting the survey at scientific conferences in Australia (Spineweek 2023, Queensland Orthopaedic Research Foundation 2023).
Survey
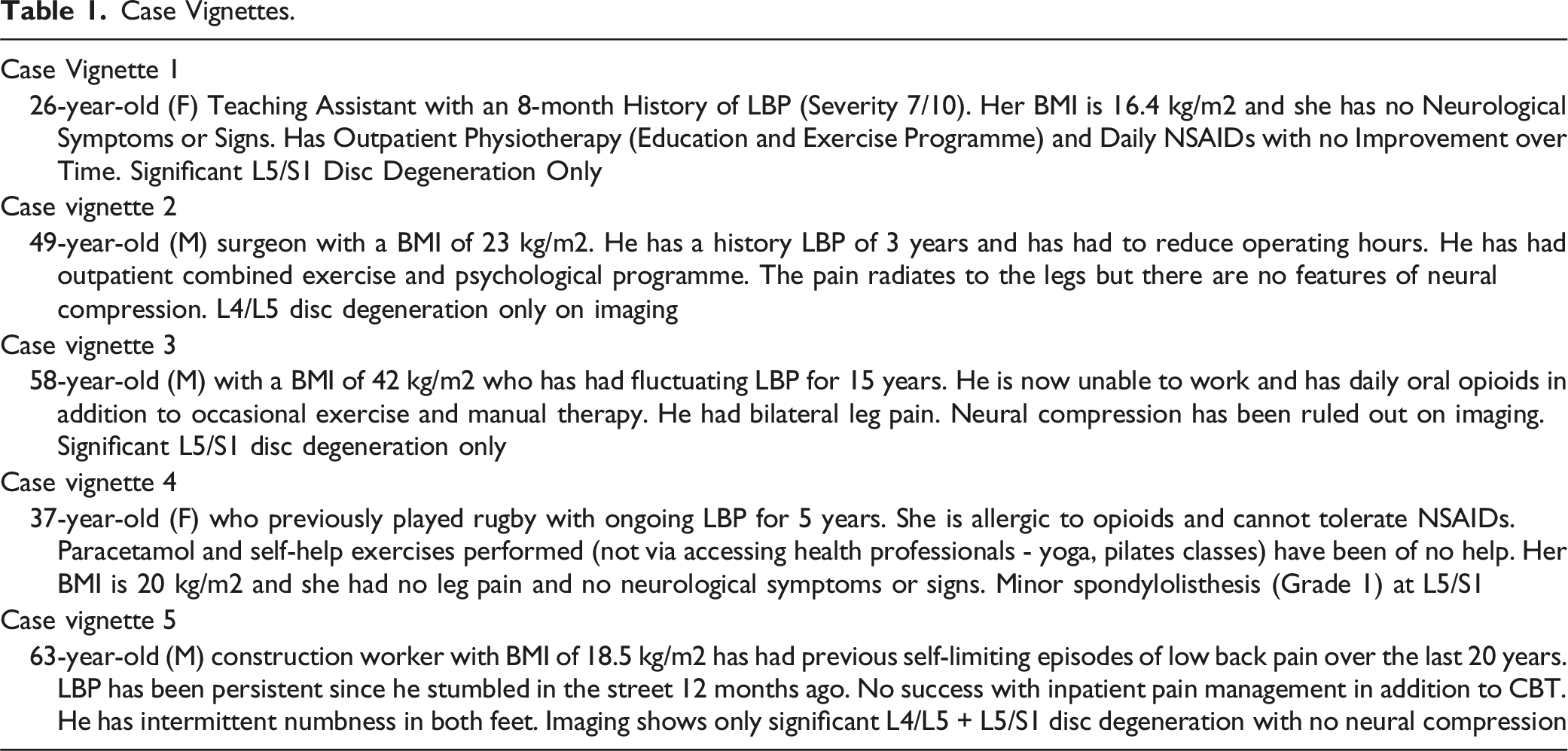
Case Vignettes.
Data Management and Analysis
Upon completion of the survey period, data were exported into Microsoft Excel (Microsoft, Redmond, Washington US) for cleaning prior to exporting to SPSS (version 28) for analysis. Presence of bot activity was evaluated from mean reCaptcha scores, with scores <0.5 considered to be likely a bot. Possible duplicate responses were flagged for consideration. Respondent demographics were analysed using descriptive statistics. Continuous data was reported as either means (standard deviation) or medians (inter-quartile range) while categorical data were presented as n (%). Management decisions for each vignette were evaluated using descriptive statistics, with equipoise regarding willingness to randomise patients to best conservative care or lumbar fusion surgery determined a priori and deemed sufficient if at least 50% of respondents were willing to randomise. Differences in choice of management across different disciplines (eg, orthopaedic spine surgeon, neurosurgeon, allied health professional (AHP), pain specialist), time in practice, and practicing sector (public, private) were analysed using descriptive statistics and chi-square tests. Significance level was set at α = 0.05 for all analyses.
Results
Survey Respondent Demographics.
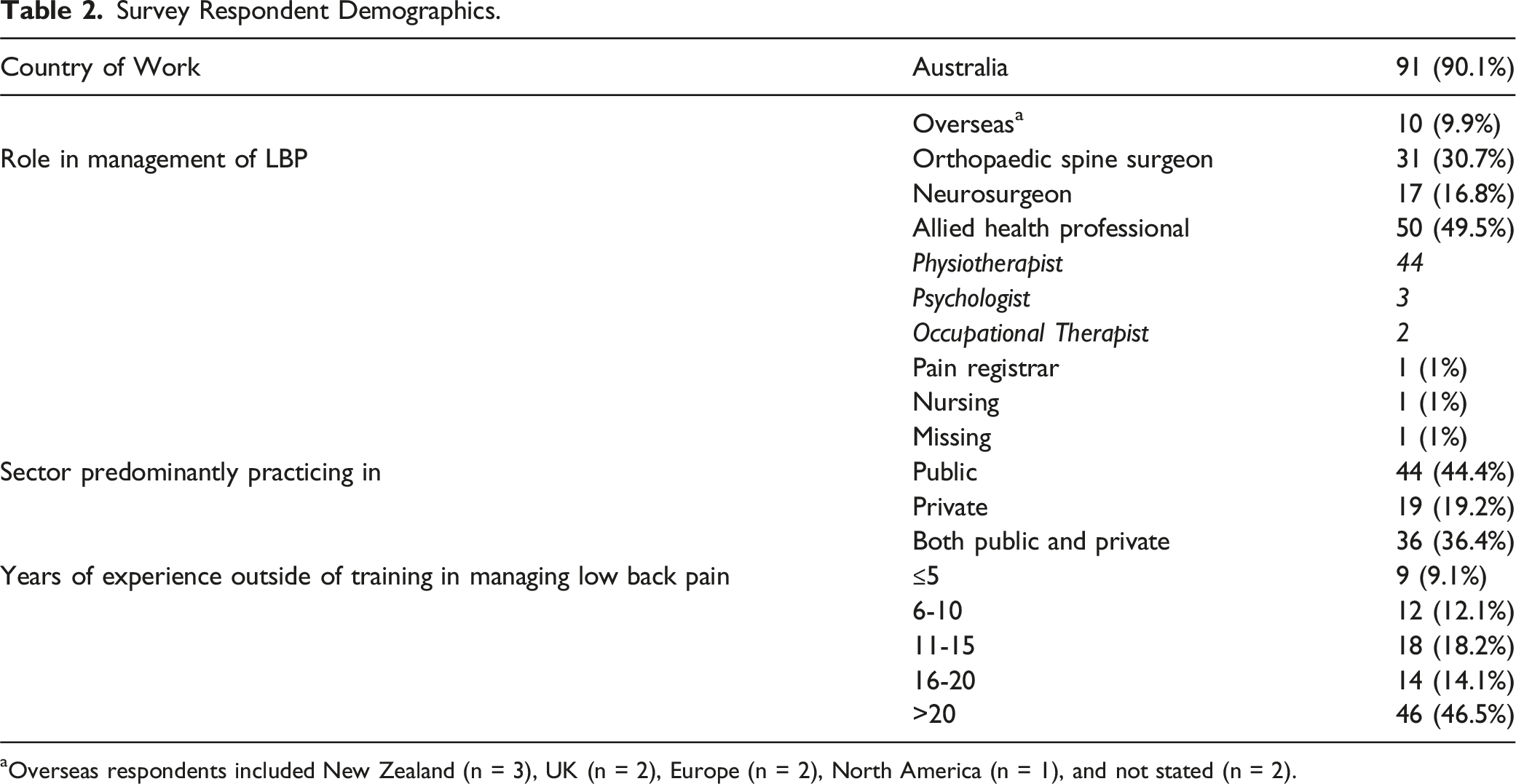
aOverseas respondents included New Zealand (n = 3), UK (n = 2), Europe (n = 2), North America (n = 1), and not stated (n = 2).
Preferred Management
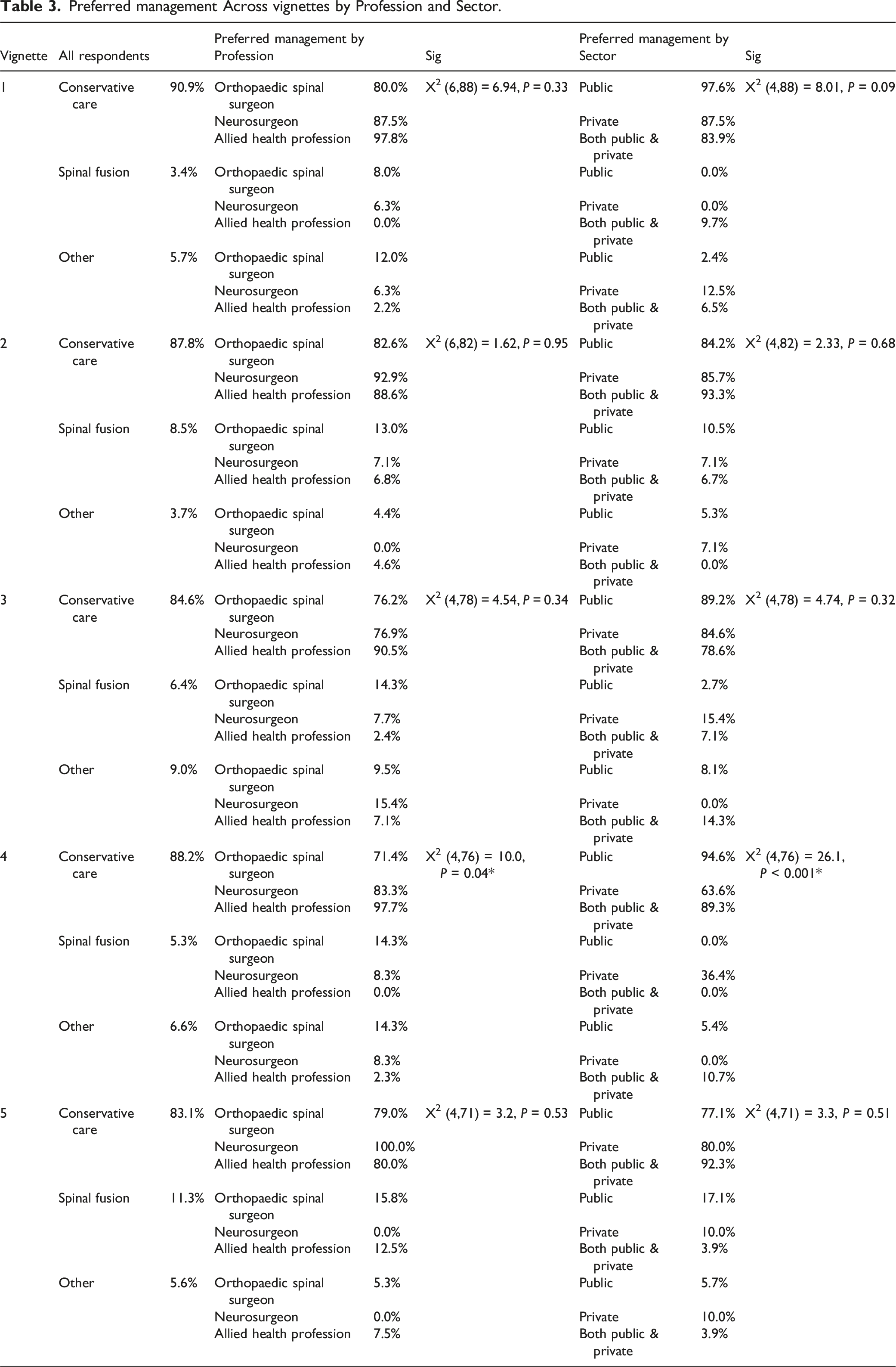
Preferred management Across vignettes by Profession and Sector.
Factors associated with respondents’ decisions regarding clinical management are displayed in Figure 1. Radiological appearance was the strongest factor across vignettes 2-5 (23.2%–30.8% of all responses), with age being the most significant factor in vignette 1 (26 year old female). Body mass index was a strong factor in vignette 3 (22.8% of all responses, BMI of 42 kg/m2). Factors influencing decision-making regarding preferred management for vignettes. Examples of ‘Other’ responses included duration and severity of symptoms, lack of neurological symptoms, psychological factors, and need for further investigations/work up.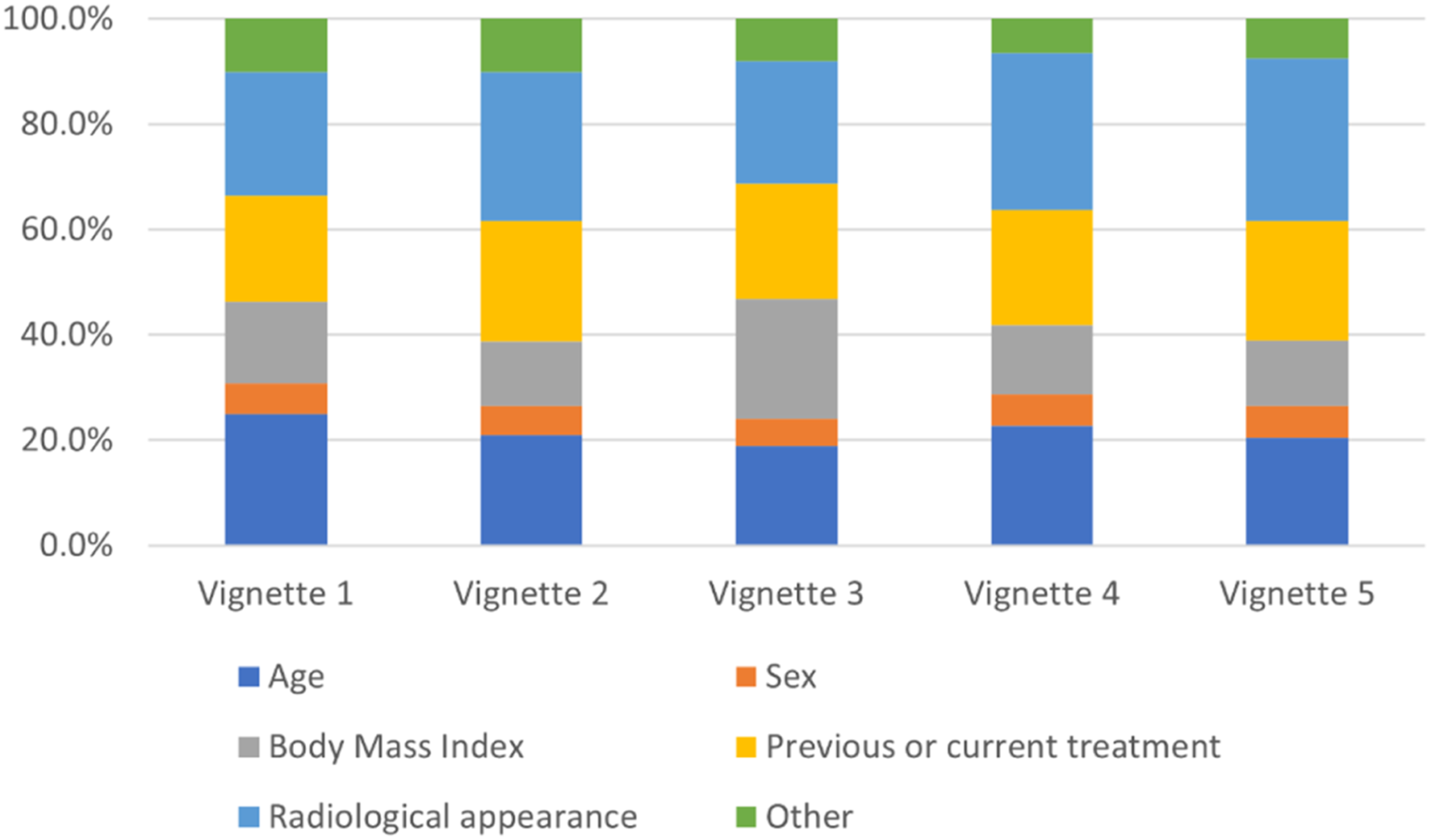
Willingness to Randomise
Willingness to Randomise Across vignettes by Profession and Sector.
Preferred Surgical Approach
The preferred surgical approach if choosing lumbar fusion is displayed in Figure 2. Of respondents performing spinal surgery, Anterior Lumbar Interbody Fusion (ALIF) was most preferred across all vignettes (Mean 54%, range 40.6%–68.4%). Posterior Lumbar Interbody Fusion (PLIF, Mean 11.3%, range 5.0%–15.7%) and Transforaminal Lumbar Interbody Fusion (TLIF, Mean 10.3%, range 3.1%–15.1%) showed similar rates. Preferred surgical approach for individual vignettes (for respondents who perform lumbar fusion surgery). Respondents were asked ‘How will you perform the surgery if you choose spinal fusion surgery?’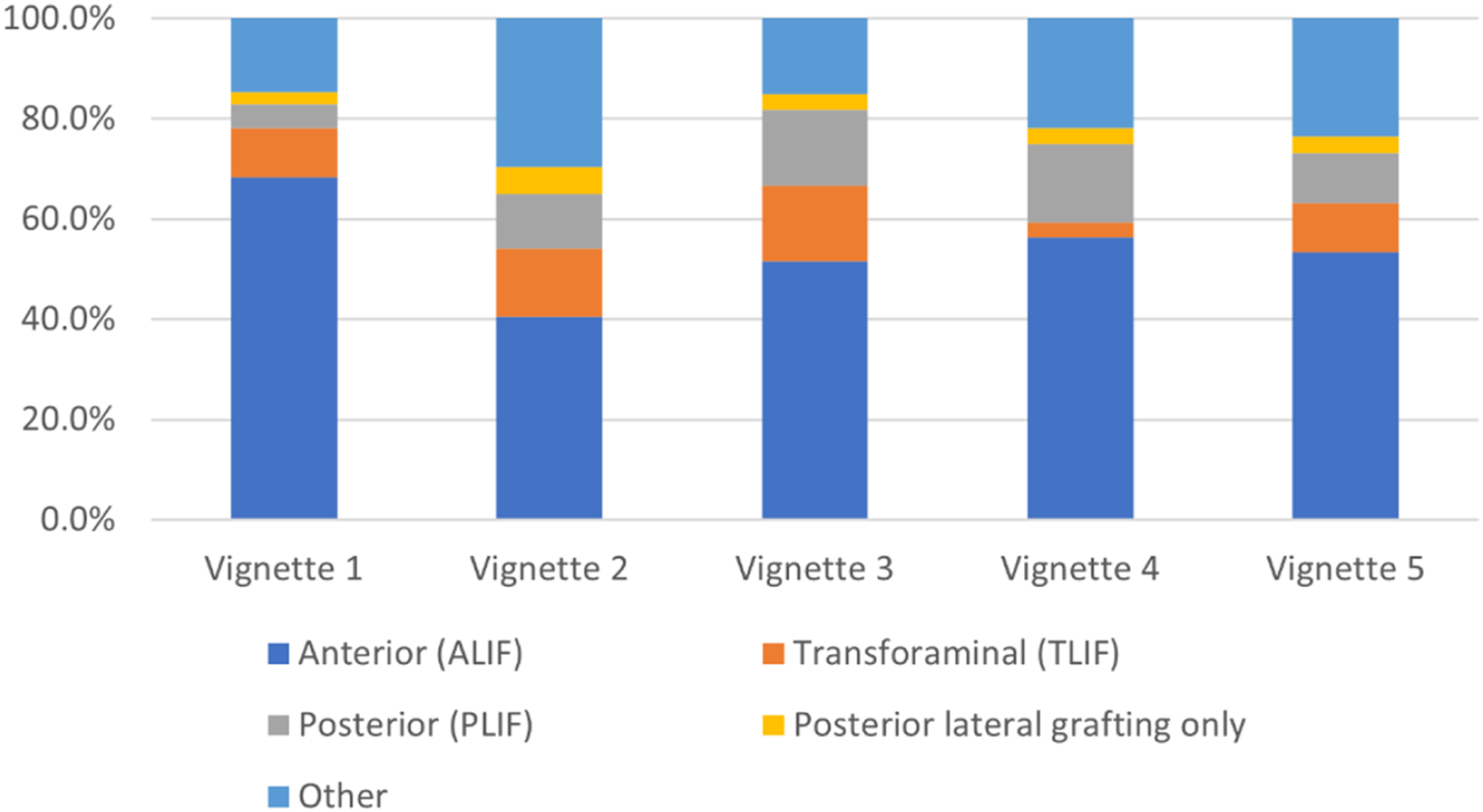
Preferred Conservative Care and Analgesia
Preferred conservative care across vignettes is demonstrated in Figure 3. Advice and self-management (range 17.2%–20.8% of all responses) was most commonly selected, followed by education (14%–18% of all responses), a combined physical and psychological programme (13.5%–20.5%), and exercise (14%–18%). Preferred conservative care for individual vignettes. Respondents were asked ‘If choosing the best conservative care for this patient, what will you offer?’. Examples of ‘other’ responses include cognitive functional therapy, specific exercises, and weight loss/dietetics.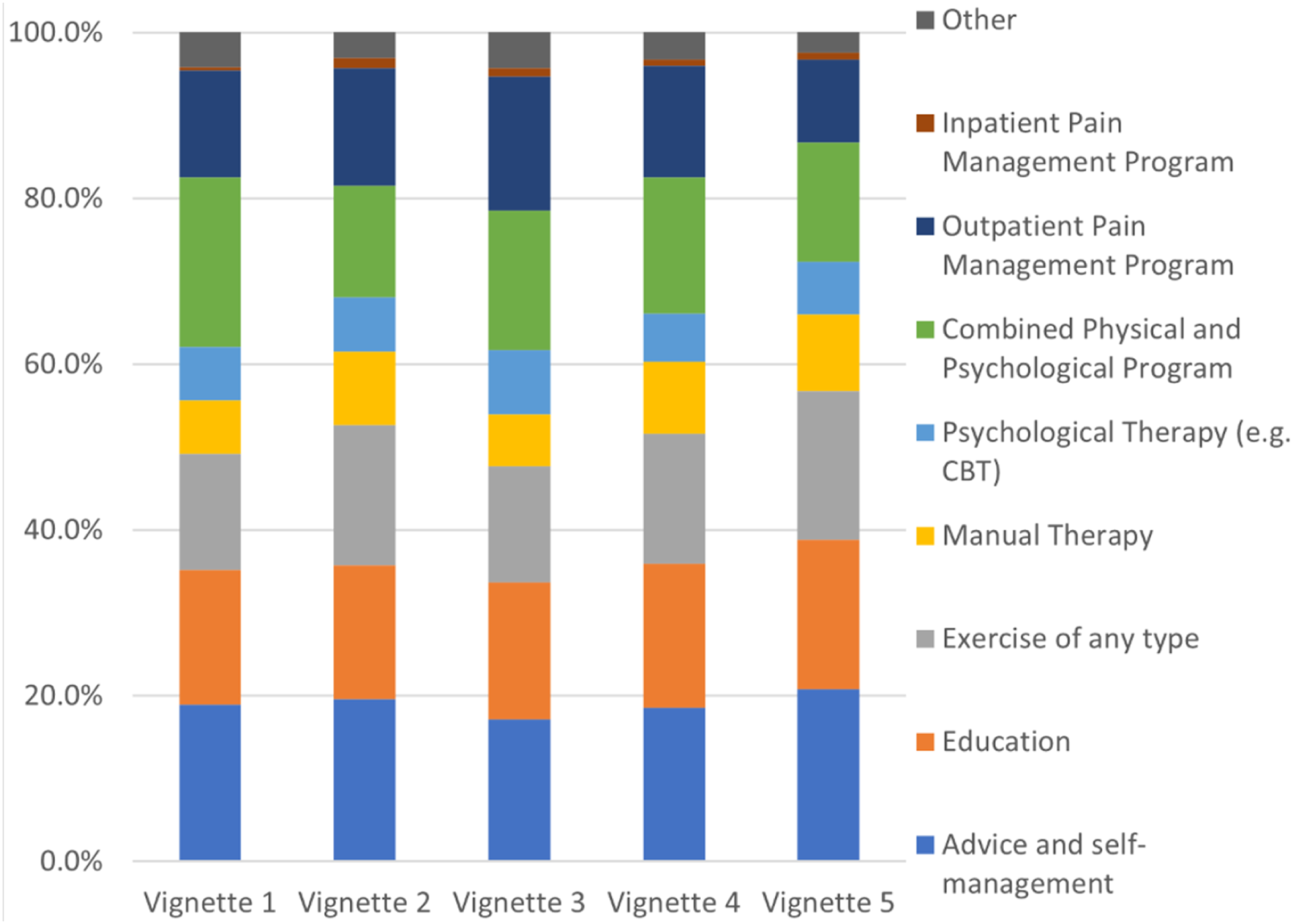
Figure 4 demonstrates respondents’ preferred analgesia for the case vignettes. Simple analgesia was the preferred option across all vignettes (range 53.1%–71.3%). Higher rates of pregabalin/gabapentin were noted for vignettes 2 (13.5%), 3 (15.8%), and 5 (15.2%), where leg pain or numbness was mentioned in the case description. Preferred analgesia for individual vignettes. Respondents were asked ‘What medication will you use for best conservative care?’ Examples of ‘other’ responses included Amitriptyline, baclofen, duloxetine, and referral to pain specialist.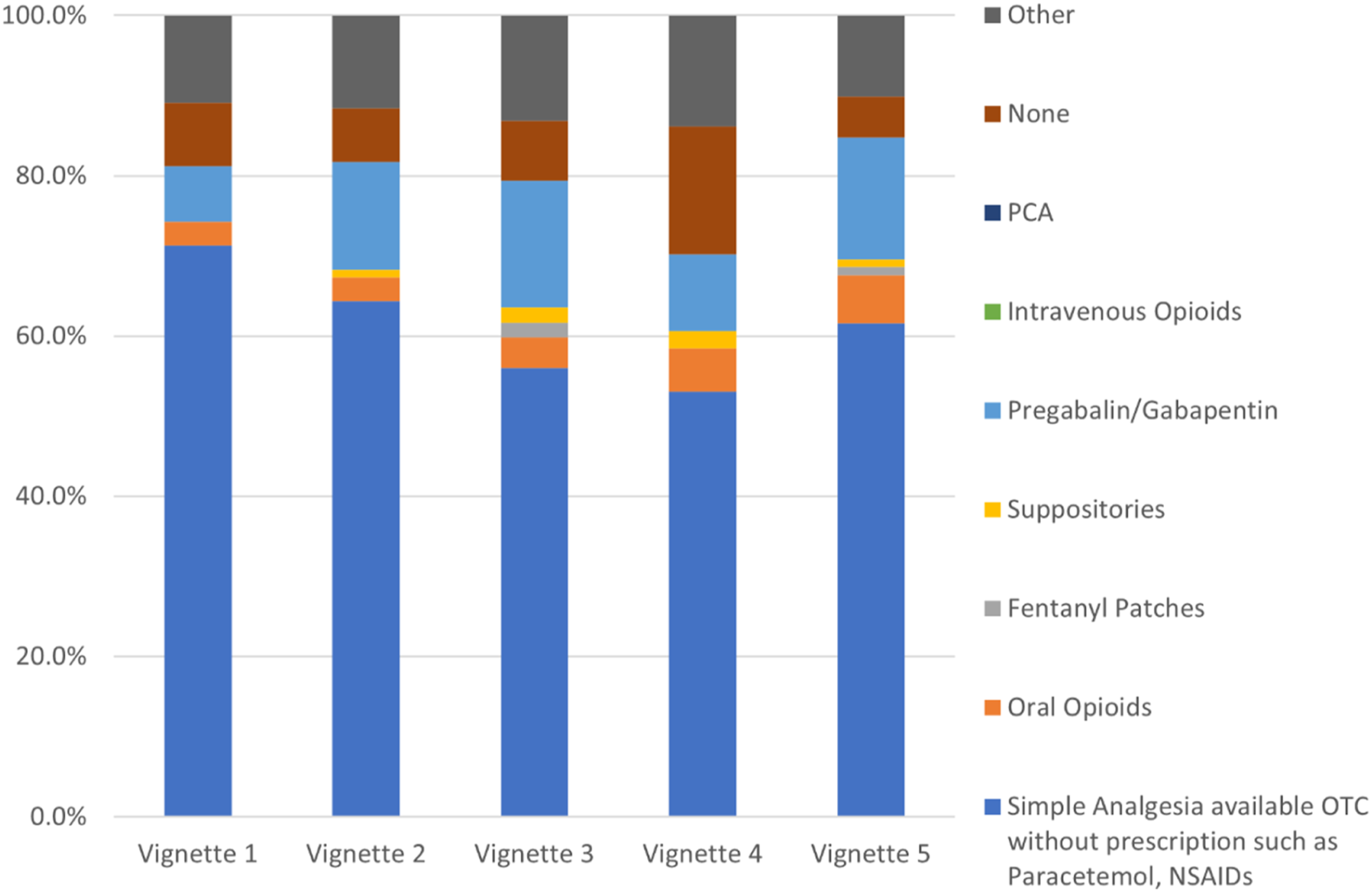
Discussion
This is the first Australian descriptive survey of health care professionals’ decision-making regarding suitability of patient cases for lumbar fusion surgery or conservative care. This study demonstrated that best conservative care was seen as the preferred option in all hypothetical vignettes. Over half of surveyed clinicians reported being willing to randomise patients with back pain without features of neurological compromise to either lumbar fusion surgery or best conservative care, indicating that there is clinical equipoise (collective uncertainty) required for RCT recruitment. However, willingness to randomise differed by profession and by sector, with lower willingness to randomise amongst AHPs and respondents working in the public sector only.
Comparing our findings with the UK survey results, 26 we found that similar rates were seen for preferred management, with best conservative care selected in 84.4% of cases in the UK data compared to 85.7% in this study. Willingness to randomise amongst health care professionals was very similar (50.7% in the UK study compared to 51.9%) although the data from this study demonstrated less variation across vignettes (47.4%–55.7% in Australia vs 37.0%–60.3% in the UK). These similarities were apparent despite a lower number of respondents from AHPs in the UK study (20.5% of respondents compared to 49.5% in this study), who tended to show higher preference for conservative care management and lower willingness to randomise. Two key differences between studies were apparent: firstly, with respect to best conservative care, UK survey respondents much more often preferred a combined physical and psychological program compared to our Australian respondents (48.5% vs 13.5%–20.5%). This is likely explained by the response options (the UK survey forced one response only to this question whereas the Australian survey allowed respondents to choose multiple conservative care interventions). Secondly with respect to preferred surgical approach, TLIF was the preferred approach in the UK (36.4% across vignettes) while in Australia ALIF was, by far, most preferred (54.0%), with TLIF comparatively lower (Mean 10.3%). The reasons for this disparity are unclear, however the preference for TLIF in the UK mirrors the findings of a UK cross-sectional survey of surgeons, with TLIF most frequently performed, 27 and database evidence in the United States also indicate a higher rate of TLIF to ALIF procedures. 28 No data relating to trends in surgical approach for lumbar fusion surgery were available in the Australian context. Discrepancies may reflect an economic driver in the UK, particularly as UK survey respondents were mostly currently practising in the NHS (91.7%). Anterior Lumbar Interbody Fusion approaches are significantly more costly than TLIF procedures, 29 while evidence to date suggests similar fusion rates and clinical outcomes between these approaches. 30
Results highlighted that across all professions and sectors, over half of respondents were willing to randomise the hypothetical vignettes to either lumbar fusion surgery or best conservative care, indicating sufficient equipoise for a future RCT in the Australian context. However, willingness to randomise was lower amongst AHPs (Mean 44.4%) and those working solely in the public sector (43.8%). These findings are consistent with the increasing rates of private lumbar fusion surgeries relative to the public sector in Australia,23,24 which may reflect over-servicing in the private sector (and potential under-servicing in the public sector). It is also likely that health care professionals will favour selection of treatments they have most experience with. For example, a pilot implementation of multidisciplinary case conferences including both surgical and non-surgical (including physiotherapy) health care professionals reduced recommendations for lumbar fusion surgery compared to surgical consultations alone. 31 Further, while over half of respondents were willing to randomise the vignettes to either approach, the preferred management option was overwhelmingly for best conservative care, perhaps indicating that although both interventions were considered appropriate, there is a preference to trial adequate conservative management (both in type and duration) prior to undergoing lumbar fusion surgery. Survey results also indicated potential differences between professions regarding their willingness to randomise, with AHPs favouring older patients with longer duration of pain and long-term conservative management, while surgeons favouring younger patients with shorter duration of symptoms. Our survey findings have potential implications for health care professional engagement with, and patient recruitment into, the FORENSIC-Australia RCT. Targeted strategies may be required to both explore and address potential barriers to recruitment 32 that may include differing health care professional views around preferred management approach and equipoise. 33
From a clinical perspective, these findings suggest the need for careful consideration in determining treatment options for individuals with LBP associated with degenerative findings. While younger patients with shorter duration of symptoms may be seen as more favourable candidates for lumbar fusion surgery, they may also be more amenable to appropriate conservative care, particularly if this has not already been tried. Conversely, individuals with longstanding low back pain that has been recalcitrant to appropriate conservative management may also present as higher risk of poor outcome following lumbar fusion surgery, and alternative pathways (eg, pain specialist review) should be considered. Finally, willingness to randomise was impacted by vignette features such as BMI and opioid use (vignette 3). These are factors known to impact treatment outcomes following lumbar fusion surgery for degenerative low back pain,34,35 and a wider multidisciplinary review including dietetics and pharmacy could be considered for individuals presenting as surgical candidates with these features.
This study has strengths and limitations. It had representation across multiple professions and sectors, enhancing the generalisability of findings to the wider Australian context. It comprised multiple sampling frames including relevant national professional bodies, advertisement at relevant conferences and through email distribution lists. However this also prevented us from accurately estimating a survey response rate. Although participation was also influenced by eligibility criteria (eg, currently involved in management of individuals with low back pain), given the membership of the Australian Physiotherapy Association (32 000 members), Spine Society of Australia (169 members), Neurosurgical Society of Australasia (>200 members) and Australian Pain Society (>800 members), it represents a low response rate, likely introducing an unknown influence of responder bias. We believe those more interested in the topic are more likely to have responded to this online survey. There were also limited responses from pain specialists (one pain registrar, one pain nurse) preventing any meaningful description of these health care professionals’ decision-making. We also acknowledge that our analysis included multiple statistical tests, without adjustment in the alpha level to identify statistically significant findings. Finally, hypothetical case vignettes were used in the survey. While vignettes have demonstrated validity and reliability in evaluating clinical decisions36,37 they may not provide a true representation of the real world but rather an approximation of it. However, the vignettes in this study were developed to reflect realistic case descriptions consistent with the real-world environment, a necessary feature of vignette-based surveys. 37
Conclusion
This is the first Australian descriptive survey of clinicians’ decision-making regarding suitability of cases for lumbar fusion surgery or conservative care. This study demonstrated that conservative care was the preferred management, however clinical equipoise (collective uncertainty) exists regarding willingness to randomise individuals with severe, persistent low back pain into an RCT investigating lumbar fusion surgery vs best conservative care. Willingness to randomise was higher amongst orthopaedic surgeons and those working in the private sector, and targeted recruitment strategies may need to be considered for recruitment through AHPs and clinicians in the public sector.
Footnotes
Acknowledgments
We would like to thank all the survey participants for taking the time to complete the survey.
Author Contributions
P. Window: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Validation, Visualization, Writing – original draft.
E. S. Bada: Conceptualization, Data curation, Methodology, Writing – Writing – review & editing.
M. Stovell: Methodology, Writing – review & editing.
S. Ahuja: Conceptualization, Methodology, Writing – review & editing.
D. J. Beard: Conceptualization, Methodology, Writing – review & editing.
A. C. Gardner: Conceptualization, Methodology, Writing – review & editing.
N. E. Foster: Conceptualization, Formal analysis, Methodology, Project administration, Visualization, Writing – review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
DB, SA, AG and NEF have funding from the National Institute for Health Research UK [NIHR134859], NEF, DB and SA have funding from the Australian National Health and Medical Research Council (NHMRC) [GA268233] and NEF is funded through an Australian National Health and Medical Research Council (NHMRC) Investigator Grant (ID: 2018182). AG has funding from Orthopaedic Research UK (combined with British Association of Spine Surgeons and British Scoliosis Society) and Innovate UK.