
Abstract
Study Design
Systematic review.
Objective
This systematic review aims to identify prognostic factors, encompassing biomedical and psychosocial variables, linked to outcome of fusion surgery for chronic low back pain (CLBP) in single or two-level lumbar degenerative spinal disorders. Identifying these factors is crucial for decision making and therefore long-term treatment outcome.
Methods
A systematic search (PROSPERO ID: CRD4202018927) from January 2010 to October 2022 was conducted, utilizing Medline, Embase, and the Cochrane Database of Systematic Reviews (CDSR, CENTRAL). Prognostic factors associated with various outcomes, including functional status, back and leg pain, health-related quality of life, complications, return to work, and analgesic use, were assessed. Risk of bias was determined using QUIPS, and the quality of evidence was evaluated using GRADE approach.
Results
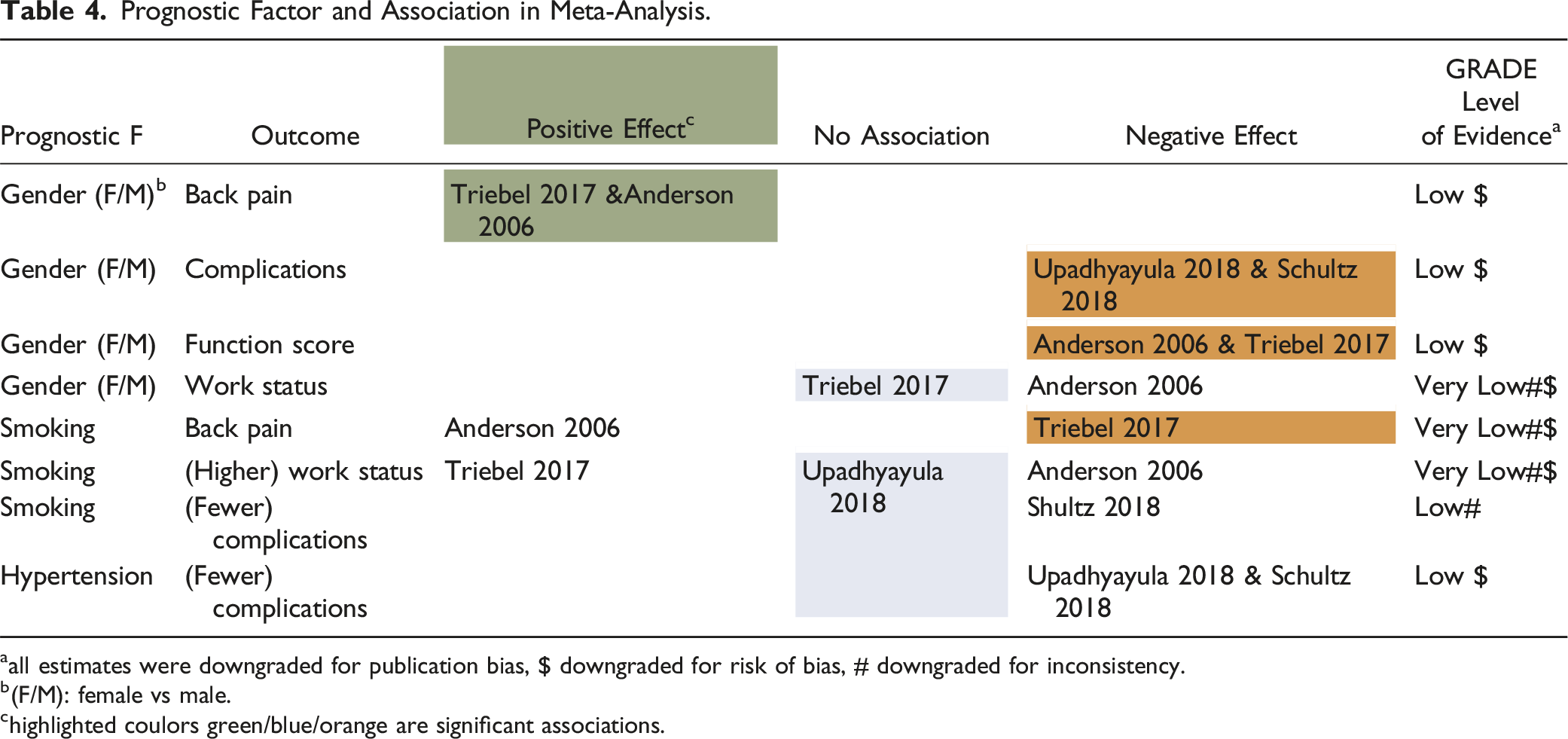
Of the 9852 initially screened studies, eleven studies (n = 16,482) were included in the analysis. In total, 161 associations were identified, with 67 prognostic factors showing statistical significance (P < 0.05). Thirty associations were supported by two or more studies, and only eight associations were eligible for meta-analyses: female gender remained statistically significant associated with decreased postoperative back pain, but negatively associated with complication rates and functional status, and smoking with increased postoperative back pain.
Conclusion
Only female gender and smoking were consistently associated with outcome of fusion for CLBP. Most of the included studies exhibited low to moderate methodological quality, which may explain the relatively weak associations identified for the assessed prognostic factors.
Keywords
Introduction
Low back pain (LBP) is the leading cause of years lived with disability worldwide and as such has a major financial impact on global health care and social security systems.1–5 As described by the Lancet Low Back Pain Series Working Group, management of the LBP population remains controversial and challenging.6,7 The population includes patients with persisting LBP, lasting over three months (chronic LBP or CLBP) due to degenerative spinal disorders. This is characterized by a biomedically focused and fragmented model of care, limited international and national guidelines, and the need for evidence-based treatment.8–11
It is suggested that carefully selected patients who have severe, lifestyle-limiting, CLBP may benefit from lumbar spine surgery.12–15 Selecting which patients may benefit from surgery is still difficult as clear-cut criteria are lacking. Some predictive factors for poor functional outcome of fusion surgery are known, such as older age, number of prior spine surgeries, duration of symptoms, lower scores on leg pain, opioid use, drug dependency (including tobacco) comorbid conditions, socio-economic circumstances, depression, and lower scores on the SF-36 MCS, but no reliable tests or prognostic tools have been identified so far.16–30 Most studies on prognostic factors for the outcome of spine surgery are not specific for CLBP due to degenerative spinal disorders. Furthermore, superiority of surgery over a cognitive-behavioural pain management program (CBPMP) is not evident for patients with CLBP.31–35 Most current international and national guidelines advice to primarily enroll patients with CLBP in specific exercise-based programs or a CBPMP and recommend to only perform fusion surgery for single level DDD if all conservative treatment has failed.36–41 Finally choosing for surgical treatment invokes the risk of complications which can result in lifelong debilitating consequences.(42-46)
A knowledge gap still exists on which patients might benefit from fusion surgery and for whom a negative outcome may be anticipated. Identification of the right prognostic factors may improve patient selection and long-term outcomes of fusion surgery for this population. This study aims to systematically review the literature to identify patient-related pre-operative prognostic biomedical and psychosocial prognostic factors that are associated with outcomes of single and/or two-level lumbar fusion procedures at a minimum of 12 months follow up for patients with CLBP due to degenerative spinal disorders.
Methods
A systematic review was conducted following the guidelines for systematic reviews for trials of interventions for neck and back pain, and related spinal disorders as published by the Cochrane collaboration.47,48 The protocol was registered and published in the online PROSPERO database (ID: CRD4202018927). Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed to conduct and report the systematic review as well as guidelines to systematic review prognostic factors, i.e. checklist for critical appraisal and data extraction for systematic reviews of prediction modelling studies (CHARMS-PF), Quality in Prognostic Factor Study (QUIPS), and Grades of Recommendation, Assessment, Development and Evaluation (GRADE).47,48 These checklists are used to evaluate (1) completeness of reporting, (2) risk of bias, (3) methodological conduct, and (4) appraisal and interpretation.
Search Strategy
A search of Medline, Embase, Cochrane Database of Systematic Reviews (CDSR, CENTRAL), and Web of Science (Science and Social Science Citation Index) from January 2010 to October 2022 was performed for studies on prognostic factors for single or two-level fusion procedures for chronic low back pain (CLBP) due to lumbar degenerative spine disorders. Appropriate references from January 2000 to December 2009 found in the systematic reviews identified in the search were added. (Supplement 1. Search strategy) Prognostic factors for the following outcomes were included: functional status, back and leg pain, health-related quality of life, complications, return to work and analgesic use (Supplement 2. Potential prognostic factors and outcome definitions).
Selection Criteria
Studies with the following criteria were included: (1) study type: randomized controlled trials (RCTs) and observational studies with at least 12 months follow-up, (2) population: adults, aged ≥18 years, with CLBP and with one or two level lumbar degenerative disorders (DDD, post-discectomy, degenerative spondylolisthesis without lumbar spinal stenosis, non-specific and or chronic low back pain, segmental pain), (3) single or two-level lumbar fusion procedures of any type, (4) multivariable analysis of prognostic factors for beneficial or detrimental outcome in functional status (Oswestry Disability Index [ODI v.2.1a], Roland-Morris Disability Questionnaire [R-MDQ]), back and leg pain (Numeric Rating Scale [NRS], Visual Analogue Scale [VAS]), health-related quality of life (36-item Short Form Health Survey [SF-36], EuroQol 5Dimensions [EQ-5Dutility] and VAS [EQ-VAS]), complications (surgical site infection [SSI], implant failure, revision surgery, vascular complications, neurologic deficit, cauda syndrome or spinal cord injury), return to work and analgesic use, and (5) sample size was at least 100 patients (fusion cases).
Exclusion criteria were (1) wrong study type (case series, case reports, animal study, in-vitro studies, bio-mechanical study, simulation study), (2) publication date before 2000, (3) population with age <18 years and diagnosis lumbar disc herniation with radiculopathy, high grade spondylolisthesis, lumbar spinal stenosis, predominantly radicular complaints, neurogenic claudication, failed back surgery after fusion, adult spinal deformity, fractures, malignancies, ankylosing spondylitis and cauda equina syndrome, mixed population (indication) or treatment (non-fusion, cervical and or thoracic procedures), (4) no prognostic variable/other outcome measure and or no multivariable analysis for the prognostic factor, and (5) insufficient sample size, incomplete baseline information, or impossibility to verify data based on language.
All criteria were applied independently to the titles, abstracts and full text versions of the articles by two review authors independently (W.C.H.J. and R.J.M.). A consensus meeting was planned to resolve disagreements. If disagreements persisted, a third review author (M.L.v.H) was consulted for a final decision.
Risk of Bias and Level of Evidence
The QUIPS tool was used to examine the risk of bias (RoB) across six domains: (i.e. study participation, study attrition, prognostic factor measurement, outcome measurement, adjustment for other prognostic factors, and statistical analysis and reporting).48,49 The overall score of the methodological quality of a paper was based on the following criteria: If all domains were classified as having low RoB, or ≤1 moderate RoB, then the paper was classified as ‘high quality’. If one or more domains were classified as having high RoB, or ≥3 moderate RoB, then the paper was classified as ‘low quality’. All papers in between were classified as moderate quality. Methodological quality of included studies was evaluated by the two reviewers, with referee if necessary.
The clinical relevance was scored at three levels ‘low’, ‘moderate’, and ‘high’ scoring 0 items, 1-2 items and 3 items, respectively on the following three questions: (1) “Are the patients described in detail so that you can decide whether they are comparable to those that you see in your practice?” (2) “Are the interventions and treatment settings described well enough so that you can provide the same for your patients?” (3) “Are all clinically relevant outcomes and prognostic factors measured and reported?”
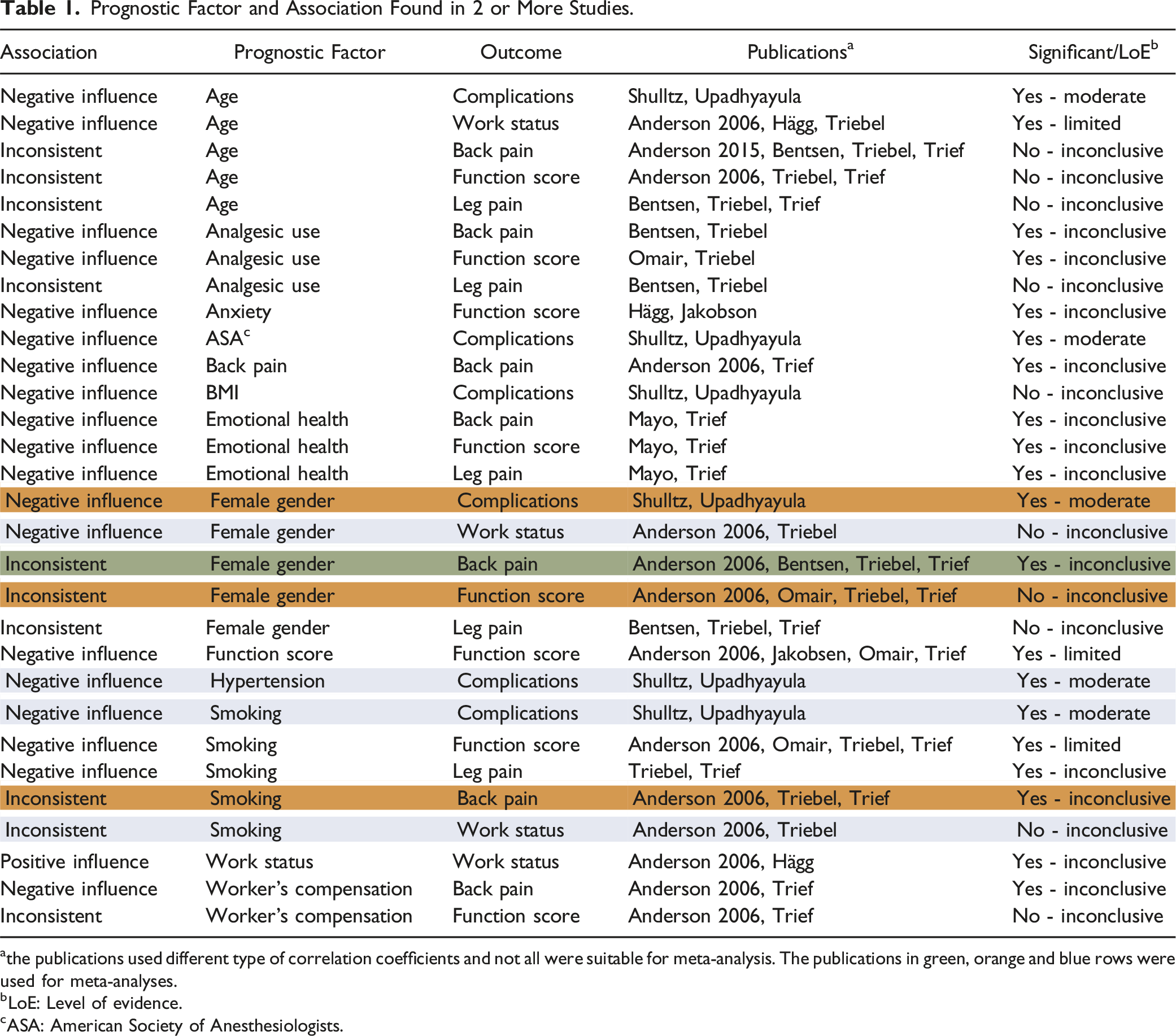
For every prognostic value analyzed in two or more articles, we defined a level of evidence: strong, moderate, limited or inconclusive (Table 1):
50
• Strong evidence: consistent findings (80%) in at least two high-quality cohorts. • Moderate evidence: one high-quality cohort and consistent findings (80%) in one or more low-quality cohorts. • Limited evidence: findings of one high-quality cohort or consistent findings in three or more low-quality cohorts. • Inconclusive evidence: inconsistent findings irrespective of study quality. Prognostic Factor and Association Found in 2 or More Studies. athe publications used different type of correlation coefficients and not all were suitable for meta-analysis. The publications in green, orange and blue rows were used for meta-analyses. bLoE: Level of evidence. cASA: American Society of Anesthesiologists.
The level of evidence of any meta-analysis was scored as “high”, “moderate”, “low”, or “very low” with the GRADE method using RoB, inconsistency, indirectness, imprecision, and publication bias. 47
Data Extraction
Study characteristics extracted from eligible papers were study type, group description, sample size, recruitment (region and type of hospital), inclusion period, informed consent, inclusion and exclusion criteria, baseline demographics (e.g. age, gender, work status, education, litigation, social support, BMI, smoking, analgesics use, ASA, BMI >30, yellow flags, red flags, duration of symptoms, previous surgery, indication for surgery, type of surgery, number of levels fused, complications, all prognostic factors investigated and all outcomes as described under Selection criteria, duration and completeness of follow-up, type of analysis, and summary of results.
Data extracted for analysis were the type of prognostic factor and the associated outcome. The type of correlation efficient was specified as Odds ratio or Beta, with 95% confidence interval and P-value. We used standardized forms for data extraction to facilitate comparison.
A ‘positive influence’ was defined as ‘decrease in post-operative pain scores’, ‘less analgesic use’, ‘improvement of functional status’, ‘improvement in health-related quality of life’, lower risk of complications, and ‘higher return to work’.
The data extraction was performed by the first author and was cross-checked and analyzed by the second author. When interpretation of data differed the third author was consulted.
Analysis
The meta-analysis was performed using Stata 14 for prognostic variables that had two or more estimate for the same outcome parameter. Beta and Odds ratios were pooled separately. Odds ratios were pooled using log transformed estimates, and back converted.
Results
Selection of Studies
The initial search yielded 9852 articles (Medline, 4096; Embase, 4766; Cochrane Database, 955; 35 systematic reviews 2000-2009). Duplicates were removed and 7416 articles remained (Figure 1) and 1649 additional references from systematic reviews 2010-2022 were screened for relevant articles from 2000-2009. A total of 547 full-text articles were analysed (including 11 articles from 2000-2009). Conflicts occurred in less than 10% of the full text articles mostly as minor differences in reason for exclusion. All articles on chronic low back pain in spondylolisthesis were excluded due to mixed populations (with neural compression), and thus a better prognosis in outcome of surgery. In 3 articles both review authors doubted the clinical relevancy for inclusion and the third author was consulted; these articles were finally excluded. Of the 547 full-text articles, 11 fulfilled all inclusion criteria (n = 16,482) and were included in our review.14,51-60 One RCT was included, the other articles consisted of prospective (n = 3) and retrospective cohort studies (n = 7). Of these 11 studies, four studies were included for meta-analyses. Prognostic factors - outcome of lumbar fusion for chronic low back pain.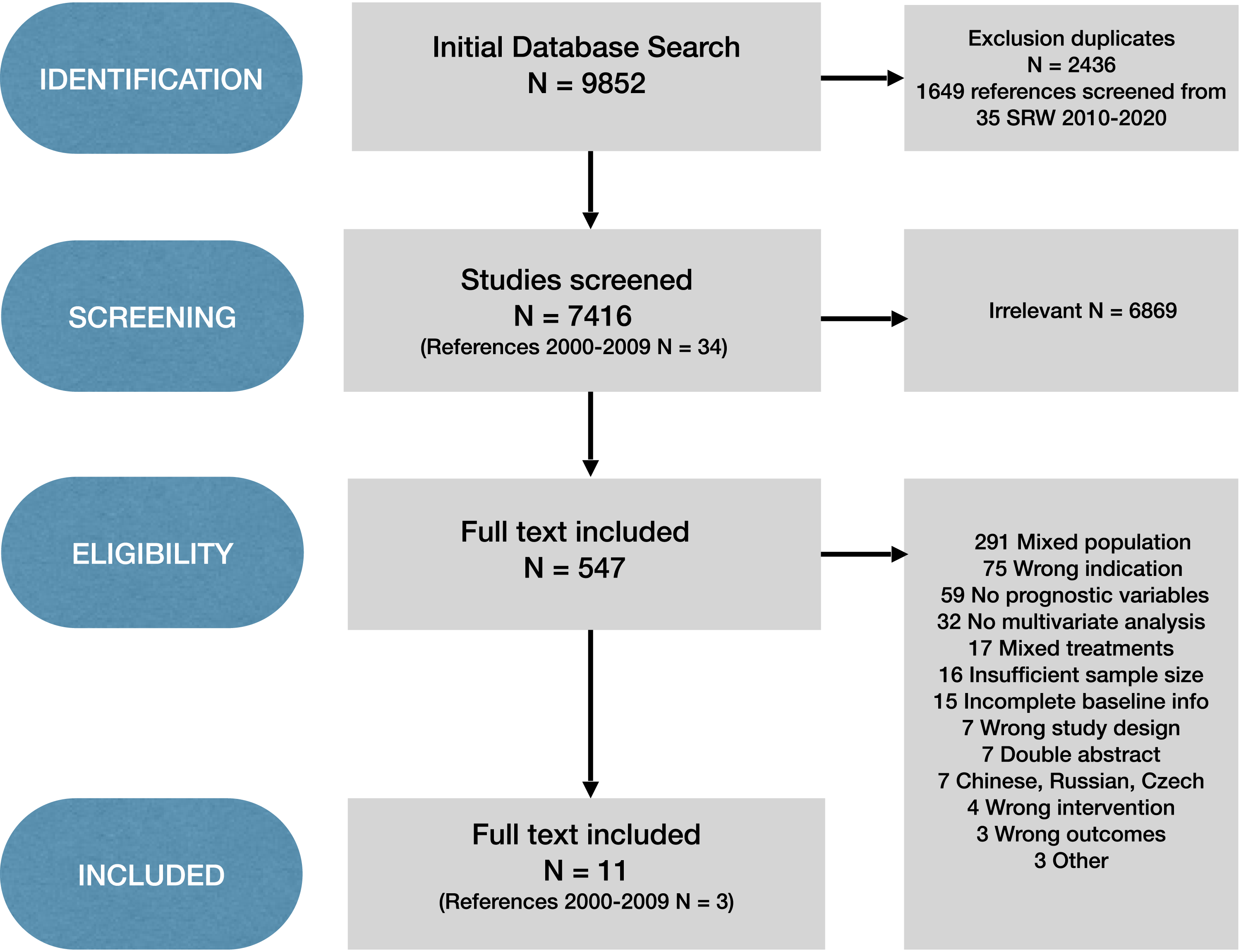
Characteristics of Included Studies
Study Characteristics.
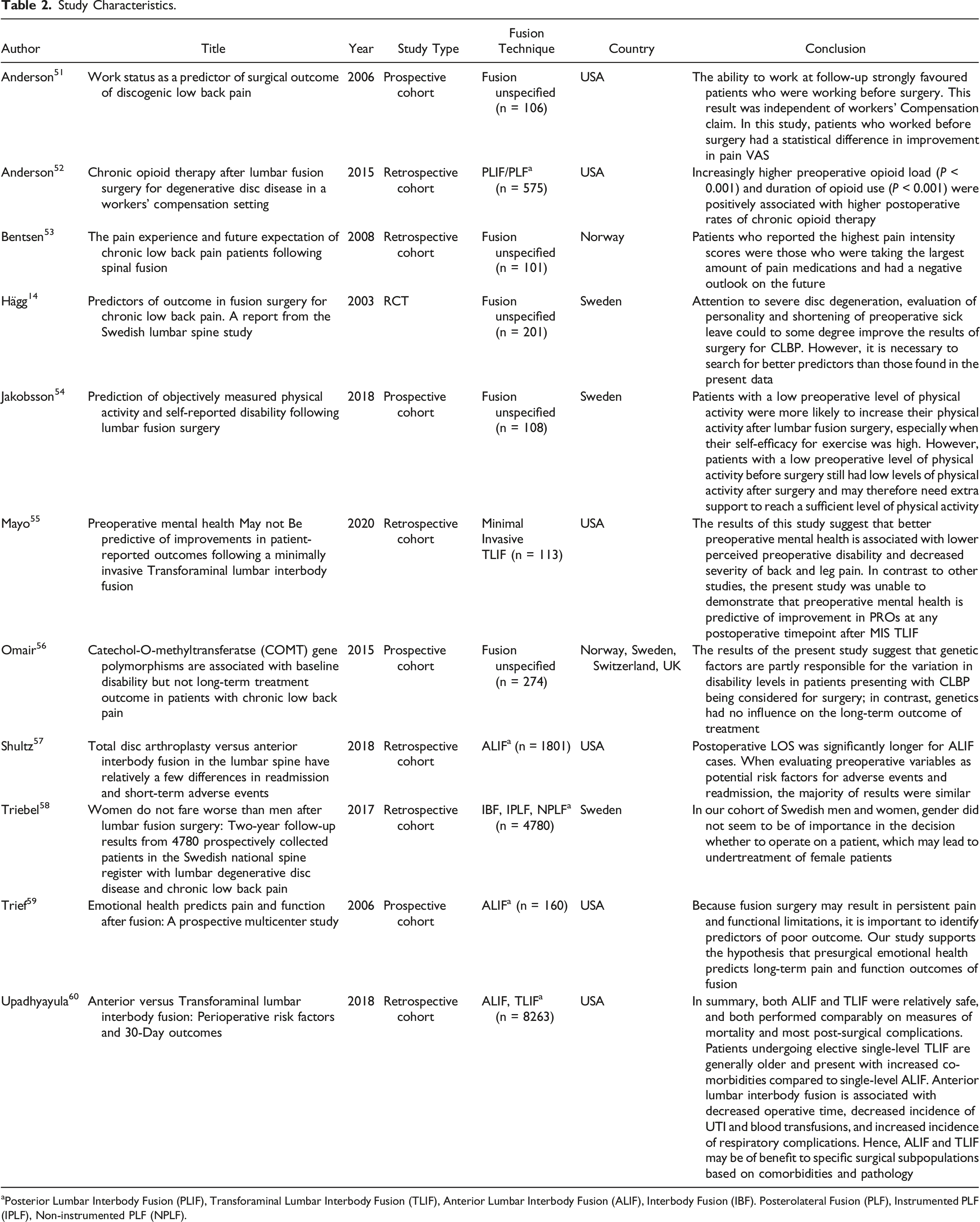
aPosterior Lumbar Interbody Fusion (PLIF), Transforaminal Lumbar Interbody Fusion (TLIF), Anterior Lumbar Interbody Fusion (ALIF), Interbody Fusion (IBF). Posterolateral Fusion (PLF), Instrumented PLF (IPLF), Non-instrumented PLF (NPLF).
Risk of Bias.
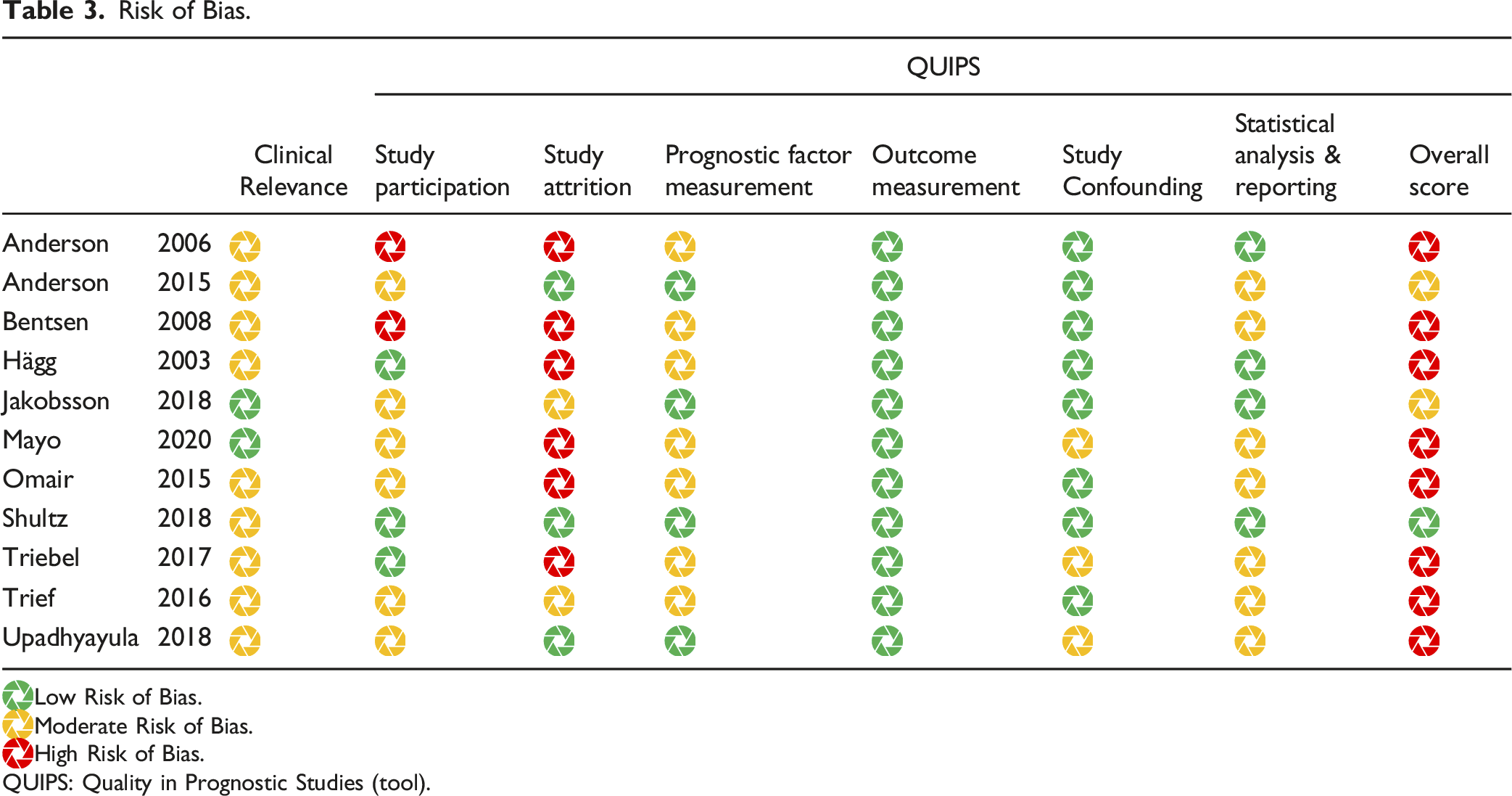
 Low Risk of Bias.
Low Risk of Bias.
 Moderate Risk of Bias.
Moderate Risk of Bias.
 High Risk of Bias.
High Risk of Bias.
QUIPS: Quality in Prognostic Studies (tool).
Population
The diagnosis of Chronic Low Back Pain (CLBP) and Degenerative Disc Disease (DDD) was the primary indication for fusion surgery in all studies. Four studies used MRI to confirm the diagnosis of DDD.14,51,52,58 Hagg et al used CT and or MRI to confirm the diagnosis. 14 Anderson et al. used additional discography to decide on a symptomatic level or non-symptomatic level. 51 In most studies this was not further specified.53,54,56,57,59,60 Five studies used operation codes to perform a retrospective analysis.52,53,57,58,60
In all included studies patients were operated for single level DDD. In the following studies this was further specified: in Anderson et al. 2006 82% of the operated patients had single level DDD and 18% two level DDD, 51 in Anderson et al. 2015 of the operated patients 58% had single level DDD and 42% two level DDD, 52 in the study of Jakobson et al. 59% had single level DDD and 36% two level DDD and <5% multi-level DDD, 54 and in the study of Upadhyayula et al. 72% had single level DDD and 23% two level DDD and <5% multi-level DDD. 60
None of the studies showed complete baseline information on all predefined aspects of demographics, pre-operative clinical status, and pre-operative scores of functional status, back and leg pain, or health related quality of life.
Prognostic Factors
In the included studies 161 associations were evaluated between 28 prognostic factors and 10 surgical outcomes (Supplemental file 3). Of the 161 associations, 67 prognostic factors were statistically significantly (P < 0.05) and were associated with the following surgical outcomes: back pain (13 statistically significant estimates), leg pain (12), analgesic use (6), functional status (18), post-operative complications (9), change in activity level (2), readmission (1), and work status (6). All studies used a multivariable regression analysis for included prognostic factors, but the studies did not all correct for the same factors (not all relevant confounders). In Table 1 an overview is given of the 30 associations between prognostic factors and outcomes that were found in two or more studies. The last column describes qualitatively whether these findings are significant and the level of evidence.
Finally, eight combinations of a prognostic factor (gender, smoking, and hypertension) and an outcome (back pain, complications, functional status, and work status) were suitable for meta-analysis.
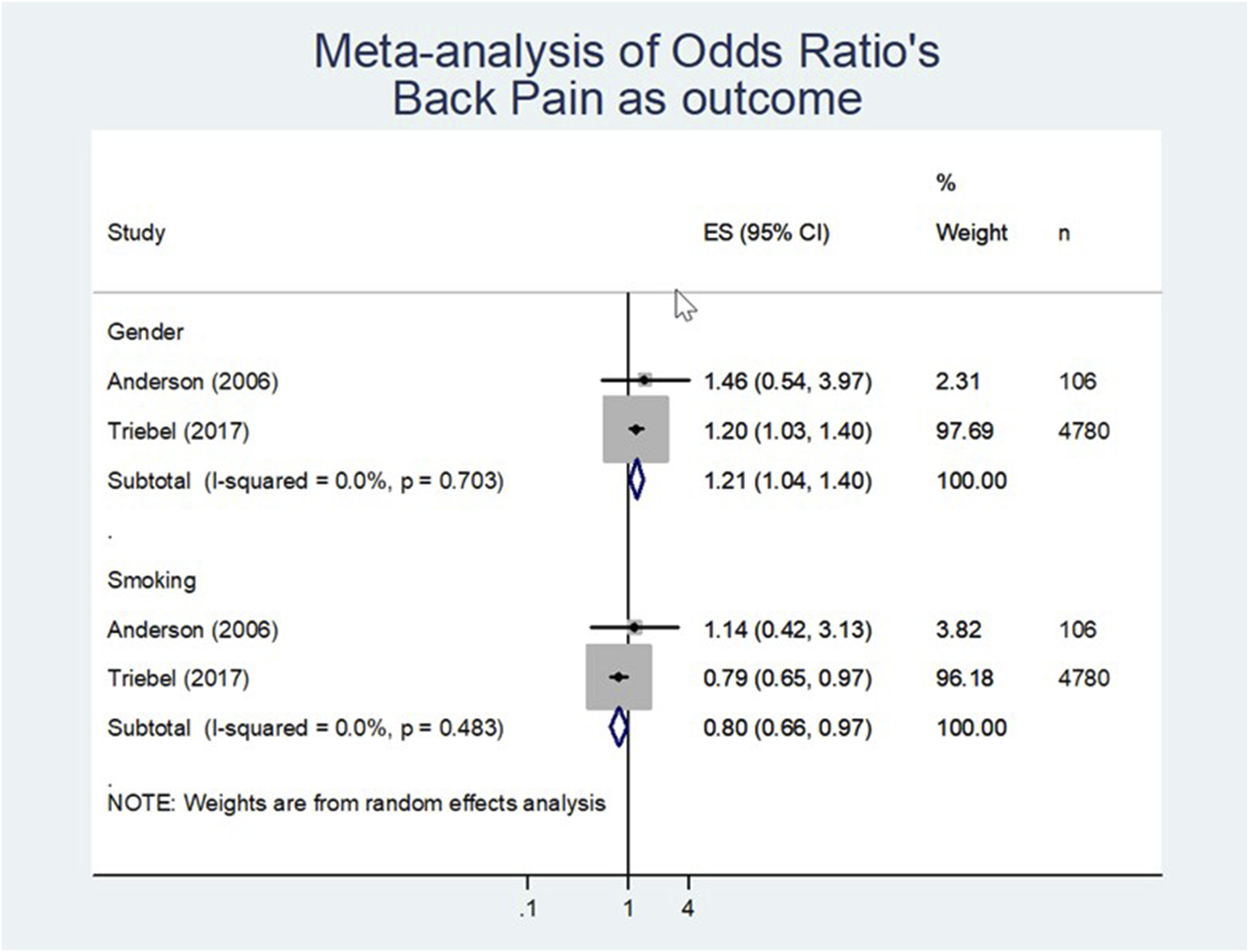
Back pain
• Low level of evidence (LoE) exists that female gender positively influences post-operative outcome in back pain (effect size 1.21; 95% CI 1.04 to 1.40 [n = 4886; Figure 2, Table 4]). • Very low LoE that smoking negatively influences post-operative outcome in back pain (effect size of 0.80; 95% CI 0.66 to 0.97 [n = 4886; Figure 2, Table 4]). Meta-analysis of odd’s ratio back pain as outcome. Prognostic Factor and Association in Meta-Analysis. aall estimates were downgraded for publication bias, $ downgraded for risk of bias, # downgraded for inconsistency. b(F/M): female vs male. chighlighted coulors green/blue/orange are significant associations.
Complications
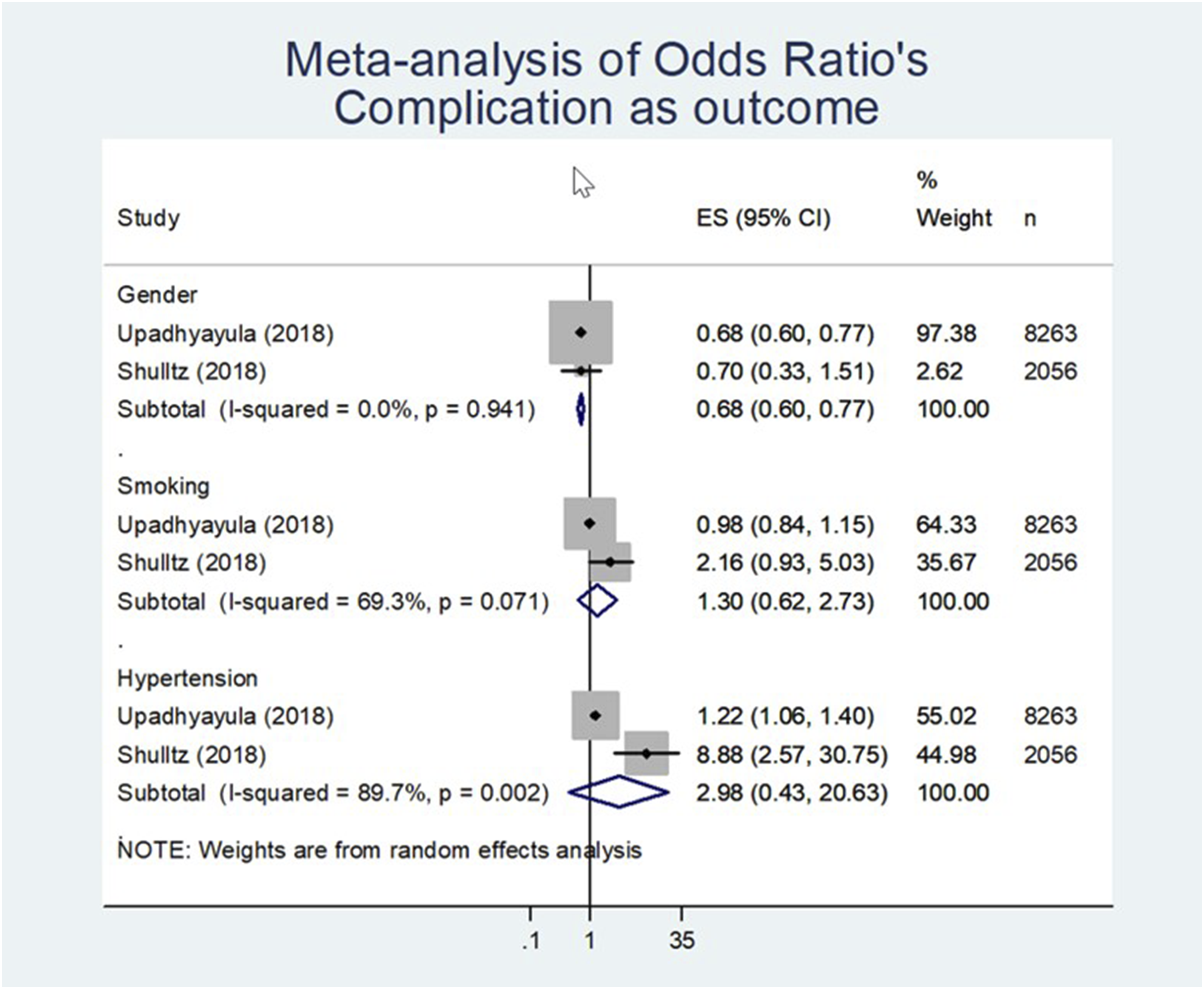
• Low LoE exists for female gender negatively influences post-operative complications (effect size of 0.68; 95% CI 0.60 to 0.77 [n = 10319; Figure 3, Table 4]). • Very low LoE that smoking negatively influences post-operative complications (effect size of 1.30 [n = 10319; Figure 3, Table 4]), but the effect was not statistically significant (95% CI 0.62 to 2.73). • Low LoE is shown for hypertension that negatively influences the risk of complications (i.e. less complications) (effect size of 2.98 [n = 10319; Figure 3, Table 4]). However, the effect was not statistically significant (95% CI 0.43 to 20.63). The complications that were analysed in the studies of Shultz et al.
23
and Upadhyayula et al.
60
are: stroke, peripheral nerve injury, unplanned intubation, prolonged ventilator time, thromboembolic event, wound infection, cardiac arrest, myocardial infarction, death, return to OR, renal failure, wound dehiscence, blood transfusion, urinary tract infection, pneumonia and progressive renal failure. Meta-analysis of odd’s ratio complication as outcome.
Return to work
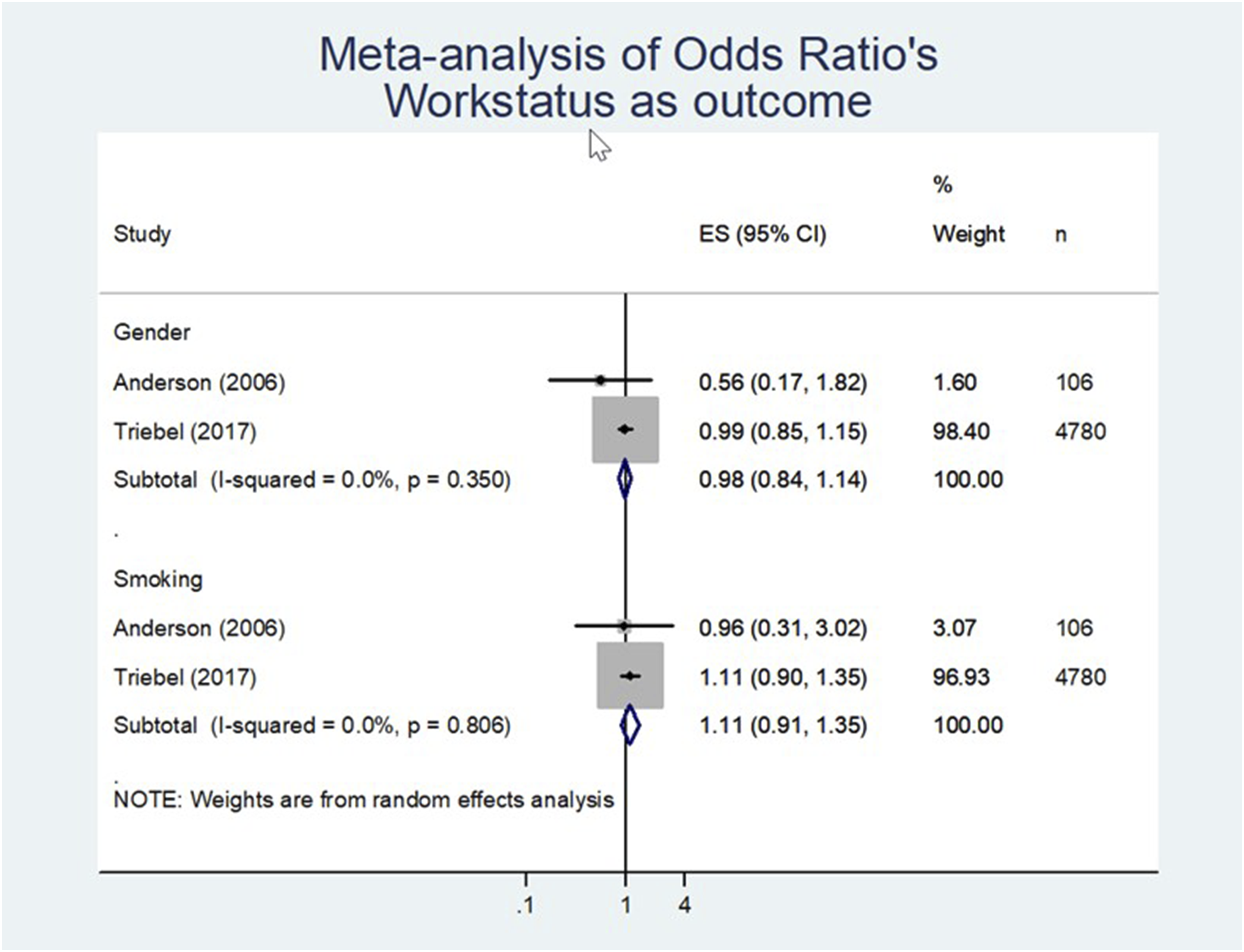
• There is very low LoE that gender negatively influences return to work: (effect size of 0.98 [n = 4886; Figure 4, Table 4]). However, the effect was not statistically significant (95% CI 0.84 to 1.14). • Very low LoE evidence that smoking negatively influences return to work (effect size 1.11 [n = 4886; Figure 4, Table 4]). However, the effect was not statistically significant (95% CI 0.91 to 1.35). Meta-analysis of odd’s ratio workstatus as outcome.
Functional Status
•Low LoE is shown for female gender that negatively influences the post-operative functional status (effect size of 1.24; 95% CI 1.05 to 1.46 [n = 4886; Figure 5, Table 4]). Meta-analysis of odd’s ratio function score as outcome.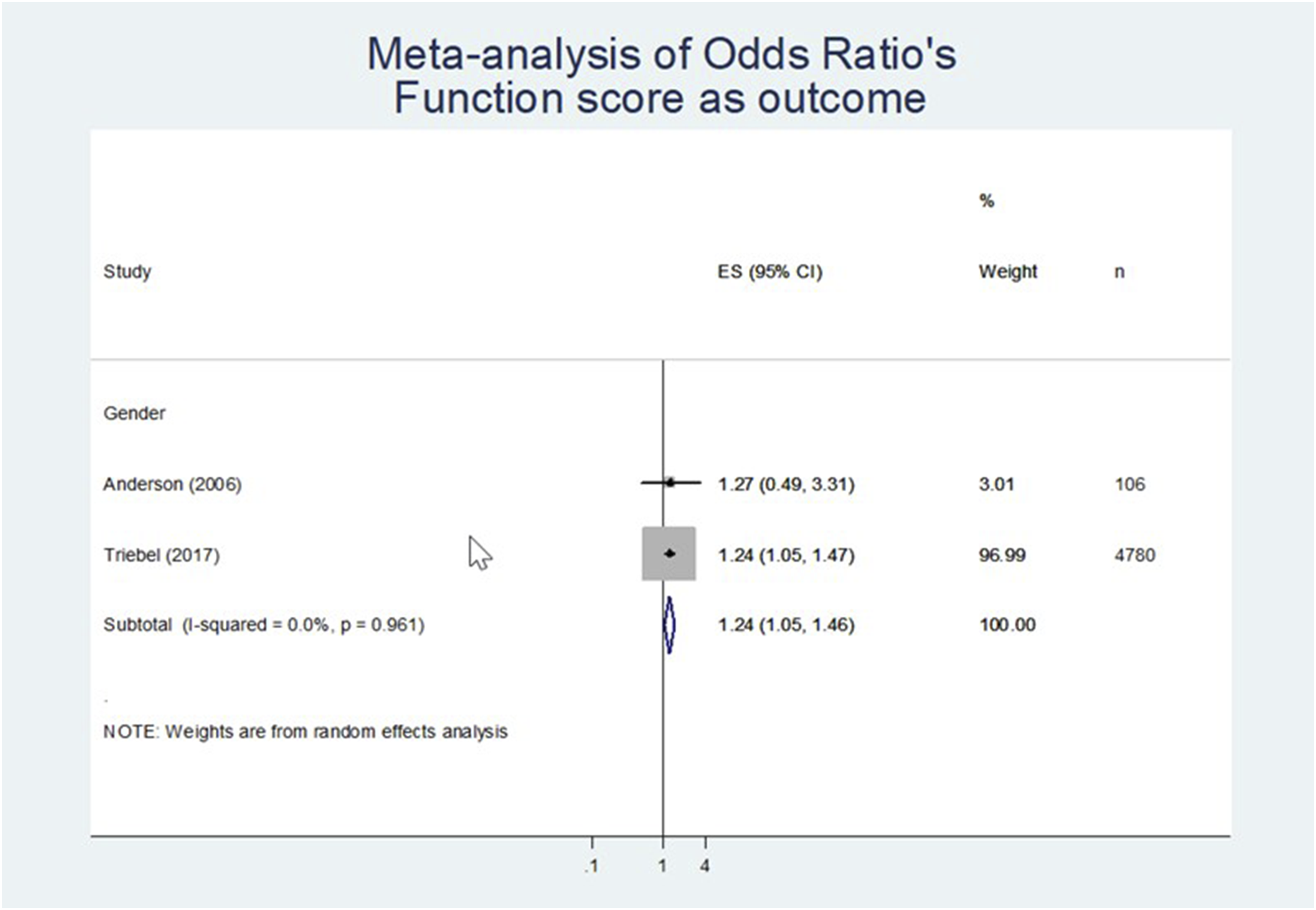
Discussion
In this systematic review eleven studies of low to high methodological quality, with at least one year follow-up, were included to identify pre-operative prognostic factors that are associated with outcomes of lumbar fusion surgery for patients with chronic low back pain (CLBP) due to degenerative disc disease (DDD). Overall, we found 161 associations, with 67 prognostic factors that were statistically significant (P < 0.05) associated with outcomes (pain, functional status, work status, health-related quality of life, and complication). Of these, 30 associations occurred in two or more studies and only eight associations were suitable for meta-analysis. In the meta-analyses, female gender remained statistically significant and positively associated with postoperative back pain and negatively associated with complication rates and functional status. For the remainder, only smoking remained statistically significant associated with increased postoperative back pain. The negative associations of smoking and hypertension with complication risk were not statistically significant.
Based on our findings, we do not recommend advising against surgery solely due to gender, as the odds ratios indicate small effect sizes. Previous meta-analyses have shown worse outcomes for women in terms of pain, functional status, ICU admission, readmission rates, and adjacent segment disease following lumbar spine fusion surgery. 61 These differences may however be partially influenced by higher prevalence of anxiety disorders and greater pain sensitivity in women.62,63 Informing female patients about the potential for reduced functional improvement, and providing tailored pain management and support strategies may improve peri operative care. We would strongly advise all patients to stop smoking before undergoing lumbar spinal fusion surgery. Smoking is associated with less improvement in back pain, delayed wound healing, delayed bone growth and fusion, and increased complication rates.64–71
Most studies on prognostic factors for the outcome of spine surgery are not specific for CLBP due to DDD, superiority of surgery over a cognitive-behavioural pain management program (CBPMP) is not evident,31–35 and thus the advice from international and national guidelines is to primarily enroll patients with CLBP in specific exercise-based programs or a CBPMP. Our recommendation remains to only perform fusion surgery for single level DDD if all conservative treatment has failed.36–41
Only carefully selected patients who have severe, lifestyle-limiting, CLBP may benefit of lumbar spine surgery.12–14 The core outcome set for this type of surgery includes post-operative pain scores, functional status, health-related quality of life, complications and return to work. 72 The clinical criteria guiding the selection of patients are: mechanical low back pain, specific findings of single or two-level degenerative disc disease with loss of disc height or Modic changes or vacuum sign or angulation on radiological imaging, Oswestry Disability Index (ODI)>40, failed conservative treatment of more than six months, psychosocially or mentally or physically able to comply with the protocol, and informed consent.11,13
Previous systematic reviews discussed different prognostic factors guiding the possible outcome of lumbar spine surgery, such as prior spine surgery, 16 smoking, 73 multifidus fat infiltration, 74 and several psychological factors.18,75 However, none of the prognostic factors found in these studies are specific to fusion surgery for patients with CLBP due to DDD (the included study population in the current study) which makes any comparison impossible.
Nonetheless many articles focus on fusion surgery for low back pain and discuss mixed effects of psychological disorders,14,55,75 and obese status,29,30,76 but still, all of these have a mixed population of surgical indications. None of the larger studies are solely fusion surgery for CLBP and DDD and are therefore not included in our meta-analysis.29,30
Achttien et al and Halicka et al conclude that the use of leg pain (higher scores) and pre-operative working may be valuable predictors of outcome to inform clinical decision-making and advice regarding lumbar fusion surgery.24,25 Most of the articles included have a mixed indication for surgery or have less than 100 patients included. In this study, for the population we have evaluated back pain scores appeared higher than leg pain scores and we found inconclusive evidence that ‘work status’ positively influences ‘return to work’ and didn’t have sufficient data to meta-analyse this association.
Yap et al concludes that low educational attainment and low-income status attribute to poorer outcomes following lumbar spine surgery, and that occupational factors and work context are likely to be influential. Gender (male vs female sex) associated outcomes however were equivocal. 28 Although their meta-analysis was focused on low back pain the 23 included studies either had mixed indications for surgery, different indications for surgery (other than our definition such as decompression surgery, herniated disc, lumbar stenosis, isthmic spondylolisthesis, microdiscectomy, total disc arthroplasty), high number of multilevel fusions, or too little patients. The only comparable study was that of Hägg et al, which was also used in our analyses. 14 In the current systematic review we found low quality of evidence (QoE) that pre-operative working status predicts less post-operative disability both at one and at two-year follow-up in lumbar spine fusion surgery in general. 24
Strengths and Limitations
A strength of this study is that we set clear selection criteria on the reason for fusion: CLBP due to degenerative lumbar disc disease. No mixed populations were included. This provides the best possible homogenous group for meta-analysis. Additionally, we focused on single and two-level fusion surgery and the population size had to be at least 100 patients, providing sufficient patient data for multivariable analysis within the study population. As it is unlikely that the prognosis of CLBP due to degenerative spinal disorders is dependent on only one factor, study results had to be derived from multivariable prognostic models. In the included studies of this systematic review multivariable regression analyses on prognostic factors were performed.
Several limitations need to be acknowledged. Despite identifying 30 associations between prognostic factors and outcomes across multiple studies, meta-analysis potential was limited due to significant heterogeneity. This heterogeneity encompassed variations in prognostic factors, outcomes, ratios, populations, surgical techniques, postoperative protocols, definitions, and threshold values. Consequently, this affected the overall level of evidence and the strength of associations.
Female gender was found to be statistically significant and positively associated with postoperative back pain and negatively associated with functional status, while smoking was a significant predictor of increased postoperative back pain. Meta-analyses for these associations were performed using studies by Anderson and Triebel (Figures 2 and 4). These studies exhibited heterogeneity in study populations (incomplete baseline data), interventions (ALIF vs mixed fusion techniques), outcome measures (VAS, Roland Morris Score, work status vs VAS, ODI, EQ-5D, return to work), study designs (university cohort vs national registry), and various biases, including imprecise effect estimates, inconsistency, selection bias, and publication bias. Subgroup analysis was not feasible.
Female gender also showed a significant negative association with complication rates (Figure 3), with meta-analysis performed on studies by Upadhyayula and Shulltz. These studies presented heterogeneity in study populations (incomplete baseline data), interventions (ALIF & TLIF vs unspecified ALIF levels), lack of threshold values for prognostic relevance, short follow-up (1 month), and biases in study participation and selection. Therefore, the generalizability of these findings is limited.
This is reflected by the overall level of evidence of the potential prognostic factors and the strength of the association.
Furthermore, the measured estimates are limited and vary among the 11 included studies, which hampers any pooling and comparison using meta-analyses. Secondly, only one of the studies used threshold values for the prognostic factor to determine the relationship with the relevant outcome. This made it impossible to compare the confidence interval to the threshold value and with that an interpretation of the strength of that prognostic factor. 47 Third, larger patient samples are more reliable than small samples with normal distribution. 64 Only four out of the ten included studies were performed on large patient samples.52,57,58,60 Fourth, to estimate a success rate assessed by a patient-reported outcome measure (PROM), Austevoll et al. recommends using a percentage change score. 77 This score is more accurate as clinical important outcome than the change score such as minimal clinical important difference. None of the studies we have included worked with a percentage score for improvement of an outcome measure. Fifth, the overall number of included studies is low. This is potentially due to the necessary strict selection criteria to perform this systematic review and is related to the required number of included patients, population composition, fusion surgery for degenerative lumbar disorders without stenosis, lysis/listhesis and or dominant radiculopathy, and obligatory multivariate analysis for the predictive value of the prognostic factor.
To improve the quality and reliability of future research preferably prospective cohort studies are performed with comprehensive baseline information (including psychological factors and socioeconomic status), a robust methodological framework, and clearly defined beneficial and detrimental surgical outcomes (supplement 2). 78
Conclusion
Literature on fusion surgery for chronic low back pain (CLBP) due to degenerative disc disease (DDD) is heterogeneous and marked by mixed findings, superiority of surgery over a cognitive-behavioural pain management program (CBPMP) is not evident, and thus the advice from international and national guidelines is to primarily enroll patients with CLBP in specific exercise-based programs or a CBPMP. Our recommendation remains to only perform fusion surgery if all conservative treatment has failed.
Thirty prognostic factors associated with postoperative outcomes following fusion surgery in patients with CLBP and single or two-level lumbar DDD were supported by two or more studies. Only eight prognostic factors met the criteria for inclusion in meta-analyses. Female gender remained a statistically significant factor, positively linked to postoperative back pain and negatively associated with complication rates and functional status. Additionally, smoking remained a statistically significant predictor of increased postoperative back pain. Most of the included studies exhibited low-moderate methodological quality, which may explain the relatively weak associations identified for the assessed prognostic factors.
Considering all relevant literature concerning prognostic factors in this context, there is sparse evidence and guidance for clinical practice. Consequently, future research of high methodological quality may contribute to determine which patients will derive the greatest benefit from fusion surgery.
Supplemental Material
Supplemental Material - Prognostic Factors for Outcome of Fusion Surgery in Patients With Chronic Low Back Pain - A Systematic Review
Supplemental Material for Prognostic Factors for Outcome of Fusion Surgery in Patients With Chronic Low Back Pain - A Systematic Review by Rinse J. Meester, Wilco C. Jacobs, Maarten Spruit, Robert-Jan Kroeze, and Miranda L. van Hooff in Global Spine Journal
Footnotes
Author Contributions
All authors were involved in the following two contributions: (1) drafting the article or revising it critically for important intellectual content; (2) final approval of the version to be published. (3) The conception and design of the protocol was primarily done by the third and fifth (last) author and (4) the acquisition, analysis and interpretation of the data primarily by the first and second author. All authors discussed the results, reviewed drafts of the manuscript, and approved the final submitted version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.