
Abstract
Study Design
Retrospective study.
Background
Non-operative treatment for patients with spinal ankylosing disorders presenting with extension type fractures (AOSpine B3) has been disregarded due to reports of poor outcomes including secondary fracture displacement and unacceptably high mortality rates. Recent studies have questioned the prevailing recommendation for surgical management, advocating for reconsideration of non-operative treatment in appropriate cases. We aim to further identify patient and radiographic factors favoring successful non-operative management.
Methods
A retrospective analysis was conducted using data from Royal North Shore Hospital spine consult database. Patients with AOSpine B3 fractures treated non-operatively between 2021-2023 were included. Demographic, clinical, and radiographic data were collected and assessed, including outcome analysis of specific fracture patterns.
Results
A total of 40 patients were treated non-operatively. 30 were deemed appropriate for non-operative management based on initial imaging assessment. Complications and 6-month mortality occurred in 13% of patients in this group. No patients failed non-operative management and good clinical and radiologic outcomes were observed in all patients on follow up. An additional 10 patients required surgery but were deemed medically unfit. Patients in this group were found to have a mortality rate of 80%.
Conclusions
Non-operative management appears feasible for selected patients with DISH and AOSpine B3 fractures of an osseous or osseous-discal pattern, without posterior vertebral wall/annulus involvement and an anterior opening of up to 6 mm. These findings suggest non-operative treatment with close clinical and radiological follow up for specific patients is a viable treatment method in this patient group.
Introduction
Patients with ankylosing spinal disorders (SAD) presenting with vertebral column fractures are a population that has been on the rise in the past few decades. 1 The most common fracture pattern encountered is the extension type injury (AOSpine B3)2,3 with a prevalence of up to 93% 1 of patients. These injuries can be highly unstable, with patients often presenting with devastating neurological sequelae and unacceptably high rates of mortality.1,4 This has brought many to suggest surgical management with long fixation for these fractures while emphasizing the possible drawbacks of conservative management.1,2,5
Recently though, there has been an increase in studies suggesting the reassessment of non-operative treatment in this patient group.6-8 Some suggest better mortality rates in this group than previously reported whilst emphasizing a potential selection bias as patients deemed medically unfit to undergo surgery and those who were trialed non-operative management have been included in reported data without discrimination. 7 Furthermore, it has been somewhat overlooked that within a specific fracture type, a variety of different patterns can be present with a possibly different natural history amongst them.
This prompts investigation of outcomes not of non-operative management in general, but rather of the specific clinical characteristics and fracture patterns that harbour favourable outcomes for patients who undergo non-operative treatment. As such, this study assesses our non-operatively treated patient cohort and aims to shed light on patient factors and more specifically fracture patterns that can be deemed stable and be successfully treated non-operatively.
Materials & Methods
Approval from the institutional review board no. 2024/ETH00897 was obtained prior to data collection and analysis. Waiver of the requirement for consent was granted due to the nature of the study. This is a retrospective analysis of data from the computerized database of Royal North Shore Hospital, Sydney as well as the statewide database of New South Wales, Australia. Royal North Shore Hospital is a statewide referral center for spinal trauma. Patients were evaluated and treated by 3 fellowship trained, consultant spine surgeons. We retrospectively searched our spine consult database for correspondence regarding patients who presented with extension type vertebral fractures (AOSpine B3)9,10 between the years 2021-2023. Demographic data collected included- age, gender, patient comorbidities and functional status. Hospitalization data included neurological status, additional injuries, time of presentation, patient complications and length of stay. Data regarding patient mortality was collected using our government database as well as telephone communication to patient contacts. Patient mortality was considered a death secondary to a medical complication which occurred following the patient’s injury. Patient presentation was considered delayed if occurred more than a week after the patient’s injury.
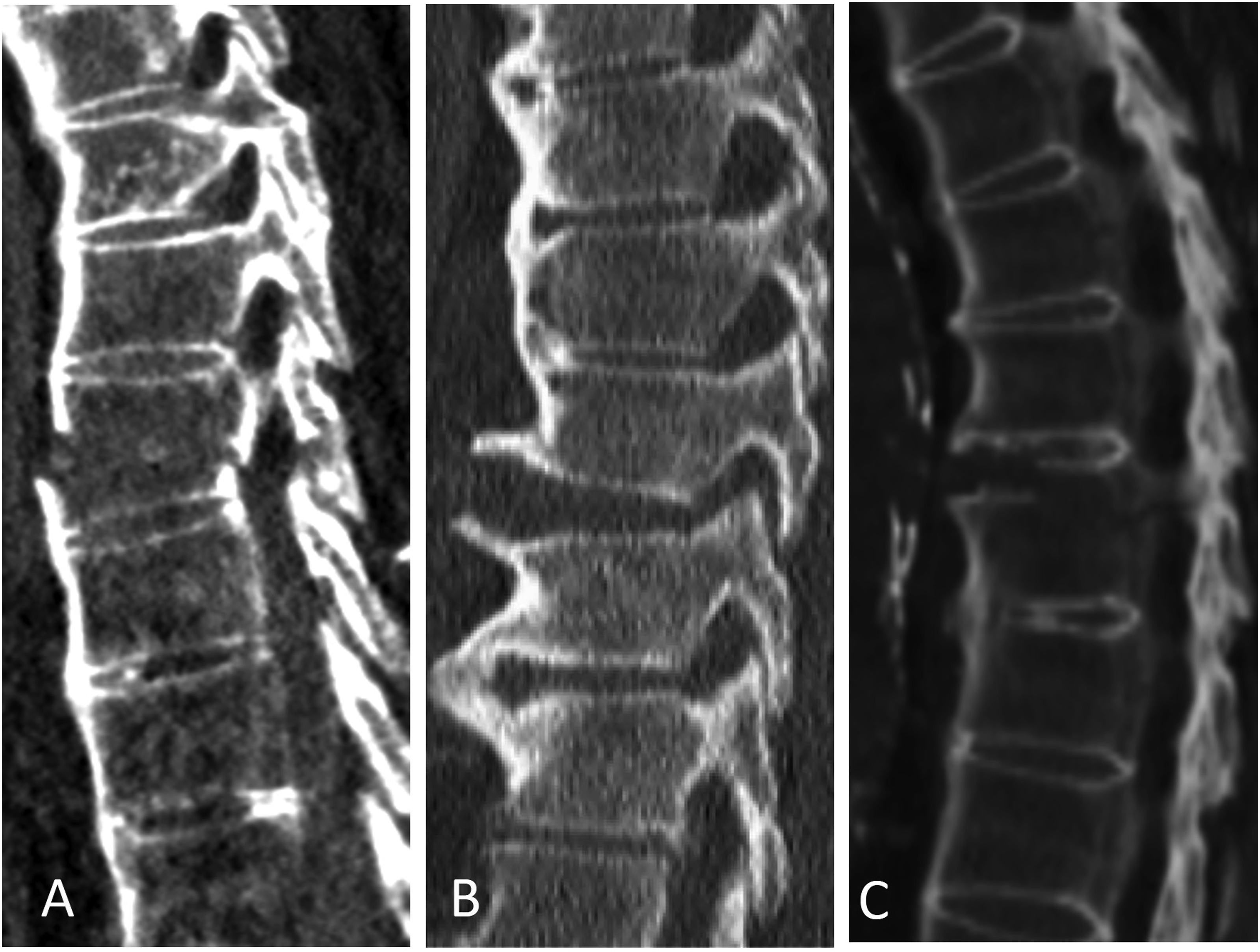
Fracture pattern on initial consult was assessed using CT imaging and MRI when available. Parameters assessed were the posterior extent of the fracture, whether the fracture was trans-osseous, trans-discal or combined and the anterior cortical widening of the fracture. Fracture patterns are portrayed in Figures 1 and 2. Anterior cortical widening of the fracture was the largest anterior cortical gap measurement on the sagittal recumbent CT. Additional radiographic factors collected were the fracture level and the classification of the patient’s spinal ankylosing disorder (SAD) [ankylosing spondylitis (AS) or diffuse osseous skeletal hyperostosis (DISH)].
11
Radiographic assessment on follow up was done with upright radiographs and CT when available. Radiographic parameters assessed on follow up were maintenance of spinal alignment, segmental kyphosis and fusion of the fracture. Imaging assessment was performed by a fellowship trained spine surgeon. Fractures treated non-operatively. (A)-Trans-osseous pattern, (B)-combined osseous-discal pattern. Examples of fracture patterns rendered unstable due to involvement of the posterior elements and/or posterior vertebral wall/annulus. (A)-Trans-osseous pattern, (B)-trans-discal pattern, (C)-combined pattern.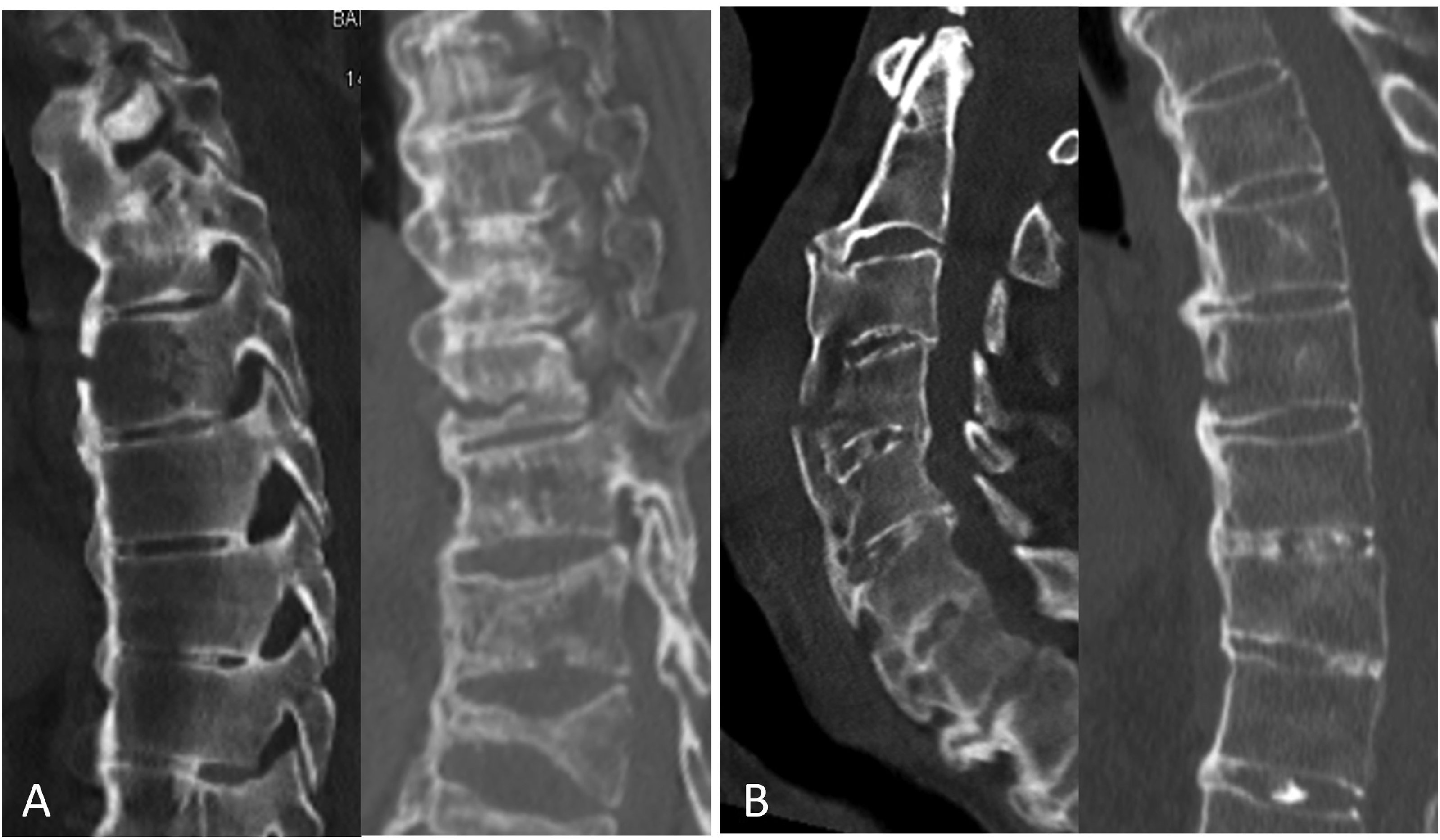
Included in the study were patients presenting with an extension type fracture (AOSpine B3) who underwent non-operative management. All patients underwent CT imaging for fracture pattern assessment. At the consultant surgeon’s discretion, additional MRI studies including a STIR sequence was obtained to further assess the fracture pattern and involvement of the ligamentous structures. When considering non-operative management, additional upright X-rays were obtained to assess for signs of dynamic instability. A decision that a patient was appropriate for a trial of non-operative management was made by the consultant surgeon following assessment of imaging studies as well as clinical exam. Prior to the study our service did not implement a uniform treatment algorithm for this patient population which takes into account the specific fracture pattern and additional patient characteristics. A distinction was made between patients who were found appropriate for non-operative management following radiographic assessment of their fracture pattern and those whose fracture pattern warranted surgical intervention but were clinically assessed as too sick or frail to undergo surgery. The latter patients were proclaimed such only if it was clearly specified in the medical note that this was the reason for non-operative treatment. This decision was made based on each surgeon’s personal assessment if the benefits of surgery would outweigh the possible risks for the patient, without specific criteria. Patients excluded were those who underwent surgical intervention following their initial presentation. Also excluded were patients who presented with a suspected extension type fracture of the anterior vertebral osteophyte that does not extend posteriorly into the vertebral body or disc as determined by CT or MRI when needed. Due to the nature of our service, radiology reports for imaging studies were not readily available and hence were not included in the study. Patient comorbidities were assessed and scored using the Charlson comorbidity index. 12 Patient’s preoperative functional status was defined as independent, device assisted and non-ambulant. Minimum patient follow up for radiographic analysis was 3 months and mortality at 6 months.
Non-operative management consisted of inpatient mobilization with our physical therapy team and obtaining baseline upright X-rays for assessment. If a patient was unable to mobilize due to pain, surgical intervention was reconsidered. At the treating surgeon’s discretion, the patient was advised to wear a brace in the form of a semi-rigid collar such as a Miami-J for cervical fractures or a molded thoraco-lumbo-sacral orthosis (TLSO) for thoracolumbar fractures. When prescribed, the TLSO was custom fitted and manufactured by our institution’s orthotics department. Outcome measures were failure of nonoperative management defined as secondary fracture displacement, neurologic decline or pain requiring surgery as well as improvement of patient pain and function on follow up. Outpatient clinic follow up with upright X-rays was performed at 6 weeks and 3 months. As per our service protocol, patients with good clinical and radiographic outcomes at this point were exempt from further follow up. Further clinic follow up and advanced CT imaging was performed at the treating team’s discretion following discussion with the patient. Patient pain and function on follow up with relation to pre-injury levels was subjectively reported and recorded by the examining physician.
Statistical analysis was performed with Graphpad Software (2024) Boston, MA, USA. Categorical variables were summarized as frequency and percentage. Continuous variables were evaluated for normal distribution using histogram and summarized and reported as median and inter quartile ranges (IQR). Categorical variables were compared using chi square or fishers exact test and continuous variables were compared using student t test. All statistical tests were 2 sided and P < .05 was considered statistically significant.
Results
A total of 63 patients with a radiographic diagnosis of AOSpine B3 fractures were consulted on by our service during the research timeframe. Non-operative treatment was found appropriate in 30 patients following assessment of their initial imaging. 63% of patients in this group were male with a Median age of 81 (IQR 76-87). CCI was found to have a median of 5 (IQR 4-7) in this group. An additional 10 patients were treated non-operatively due to their physical state. These patients warranted surgical intervention following initial assessment of their imaging but were deemed medically unfit or too frail to undergo surgery. 80% of patients in this group were male with a Median age of 91 (IQR 88-95). CCI in this group was found to have a median of 5 (IQR 2-7). A significant difference in age was found between the 2 groups (P = .022). There was no difference found between the groups with regard to sex (P = .69) and CCI (P = .631).
Non-Operative Treatment Appropriate Patients
Summary of Patient Mortality and Complications-Non-Operative Appropriate Patients.
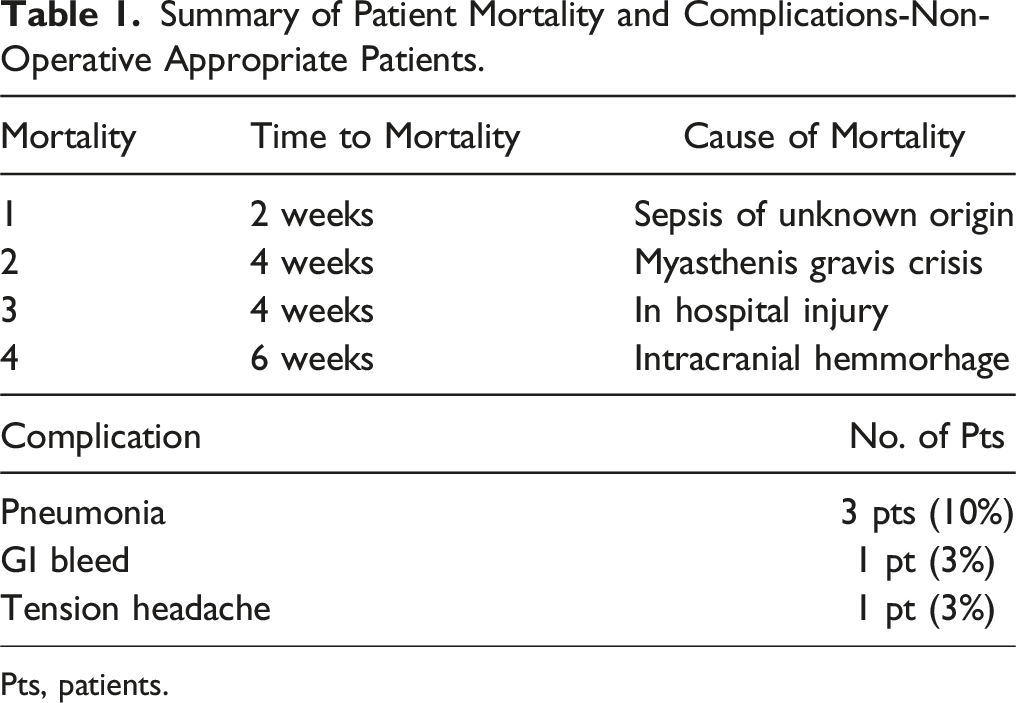
Pts, patients.
Summary of Patient Mortality and Complications-Patients Medically Unfit for Surgery.
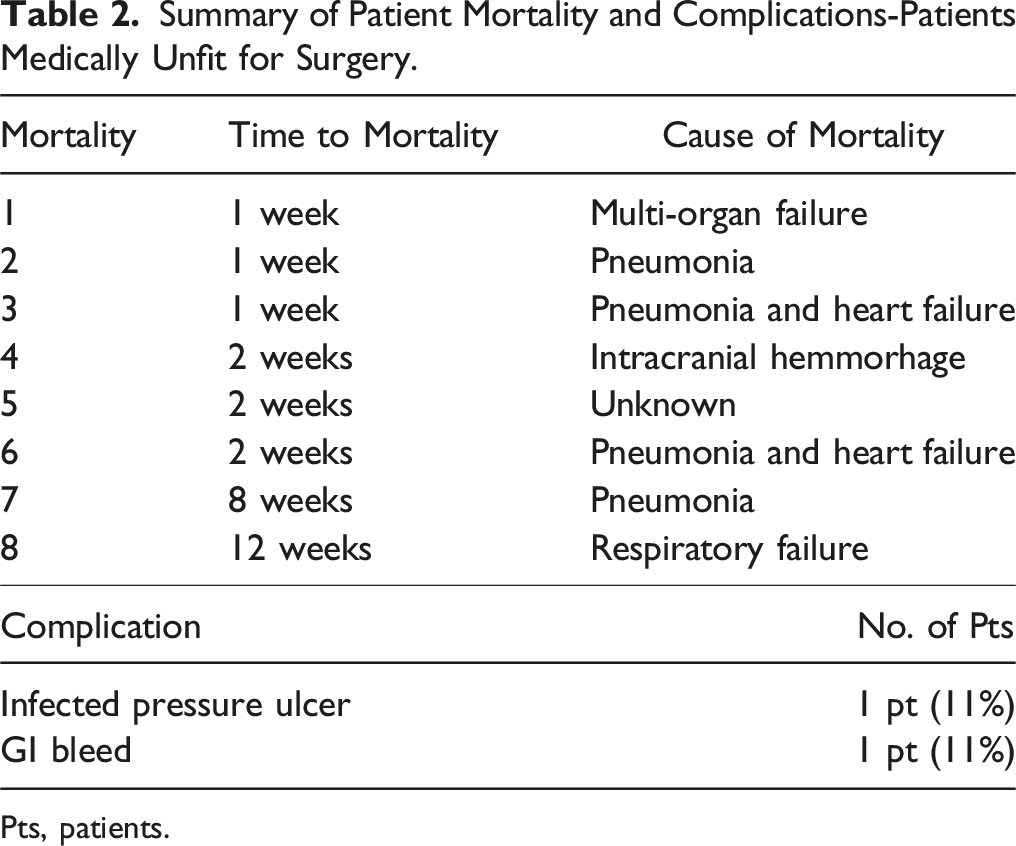
Pts, patients.
Summary of Fracture Characteristics and Radiologic Follow Up-Non-Operative Appropriate Patients.
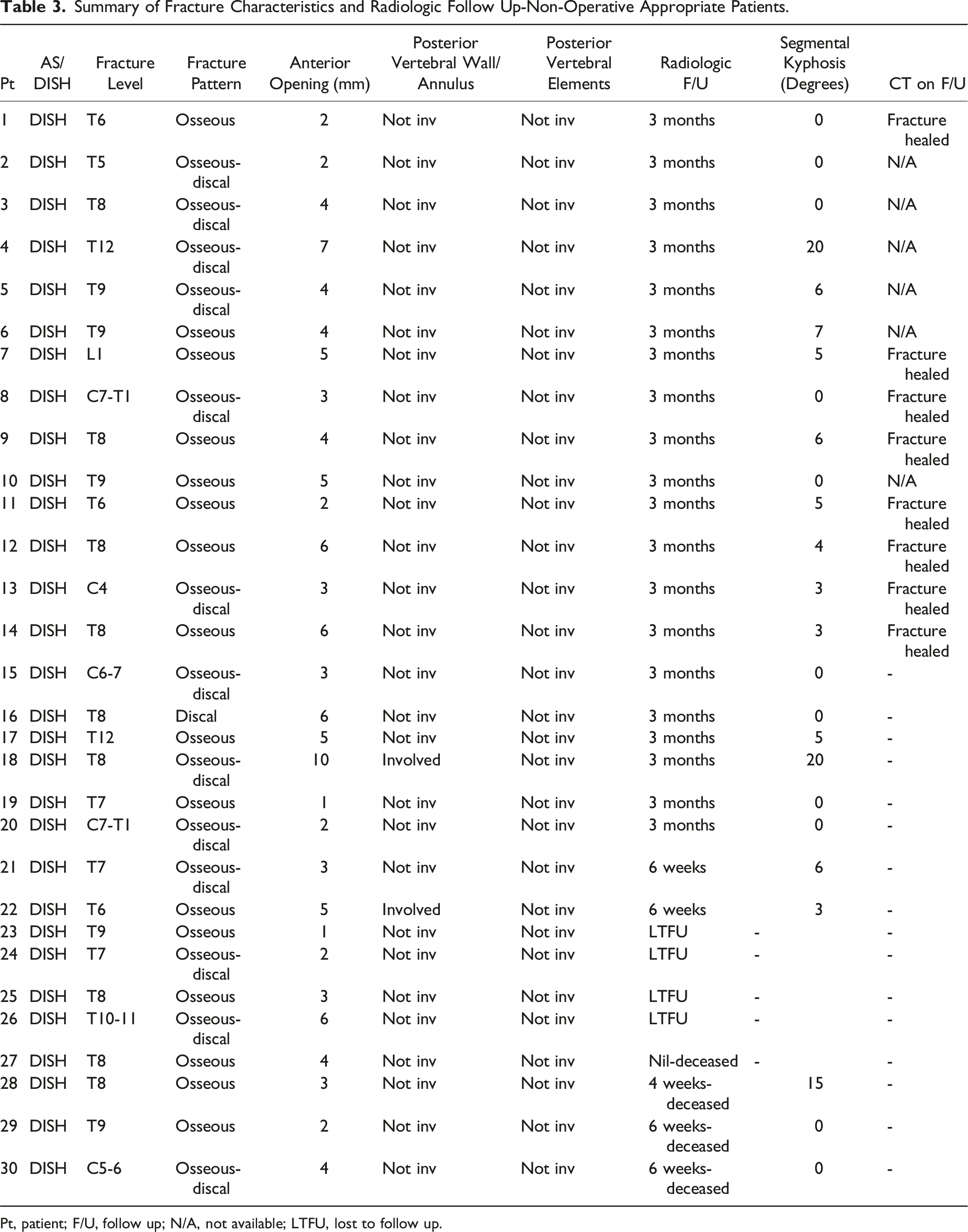
Pt, patient; F/U, follow up; N/A, not available; LTFU, lost to follow up.
Summary of Fracture Characteristics and Radiologic Follow Up-Patients Medically Unfit for Surgery.
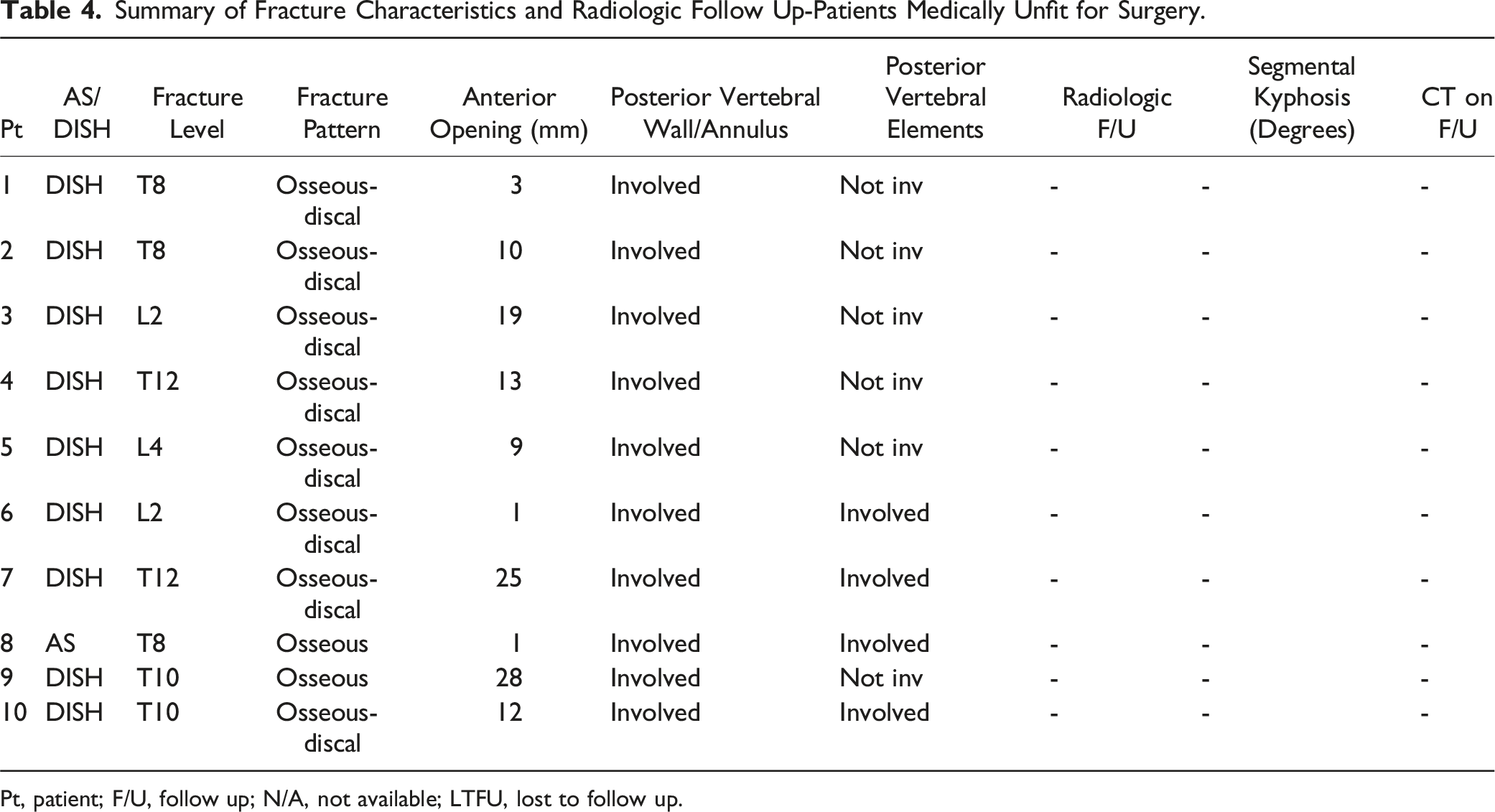
Pt, patient; F/U, follow up; N/A, not available; LTFU, lost to follow up.
Surgical Candidates Deemed Unfit for Surgery
A total of 10 patients sustained fractures that warranted surgery but were deemed unfit for surgery by their treating surgeon. 4 patients were deemed medically unfit and 6 patients too frail to undergo surgery. Mortality was 66% (6 pts) at 2 weeks and 80% (8 pts) at 3 months. These included the patient with AS. The remaining 2 patients were alive at 6 months from injury. 2 patients had passed due to concomitant injuries and 6 due to secondary medical complications.
Fractures diagnosed were in the thoracic spine in 70% of patients and the lumbar spine in 30% of patients. 90% of patients had a radiographic diagnosis of DISH and 10% of AS. Fracture pattern was combined osseous and discal in 80% of patients and purely discal in 20%. All patients had involvement of the posterior vertebral wall or annulus on initial imaging. Further extension of the fracture to the posterior elements was found in 40% of patients. None of the patients in this group were treated with a brace.
Discussion
Several arguments have been suggested to explain the rise in incidence of patients with SADs presenting with extension type fractures. Some of these include population ageing as well as an increase in comorbidities such as type 2 diabetes and obesity which may predispose the appearance of DISH(1). Furthermore, the possibility arises that in the past these patients went undiagnosed and the increase in incidence is partially due to implementation of mandate CT screening protocols in emergency department scenarios. This could lead to the notion that although in the past more severe injuries were missed, more patients with stable injuries also went undiagnosed and did well. Still, surgical management is the mainstay of treatment for this patient population. Those advocating against non-operative management describe higher rates of medical complications and mortality of up to 51%1,2 as well as progressive deformity and neurologic decline. 5 Furthermore, a failure rate of up to 50% has been described for non-operative management due to secondary displacement or intolerance of bracing.13,14 As non-operative treatment has been considered an option for patients with clinically stable fractures, 15 interest arises though as to what subgroup of patients in this population can in fact do well when managed non-operatively and what fracture can be considered stable given the irregular force acting on the fracture in the ankylosed spine. In a recent study of 167 patients with spinal ankylosing disorders treated for fractures of all patterns, Chen et al 6 endorsed a reappraisal of operative indications and a larger role for non-operative management in this patient population. In their cohort, 38% of patients had type B fractures with non-operative treatment selected in 44% 10 of patients diagnosed with DISH and 36% 15 of those with AS. Mortality rates for non-operative patients were found to be 8.8% and 15.7% at 30 and 90 days respectively. No difference between patients managed surgically and non-surgically was found in mortality rates, length of stay or loss of mobility. These results however did not differentiate between fracture patterns making it difficult to draw conclusions on specific patient management. Bäcker et al 7 also suggested that previous reports may overestimate the mortality rates in non-operatively treated patients. 29 patients in their cohort presented with AOSpine B3 type fractures and were treated non-operatively. They found a mortality rate of 10.3% at 6 weeks from their injury and a total of 27.5% mortality at follow up with a mean of 157.1 ± 158.1 days. As with Chen et al, they do not provide results for different fracture patterns within the AOSpine B3 category. Our study agrees with these and finds perioperative morbidity of 13% and a mortality of 13% at 6 weeks for patients found appropriate for non-operative care. Furthermore, Functional outcomes in our cohort are acceptable with a decline in functional status of 33% with none of these being wheelchair bound on follow up. This is comparable with data presented by Chen et al 6 who found loss of mobility in 33% of patients treated non-operatively and 27% of those treated surgically.
As demonstrated, our study ratifies the findings of Chen et al and Bäcker et al while further assessing the fracture patterns and additional radiologic parameters which could suggest what patient may be appropriate for non-operative treatment. We found that none of the patients had fractures that involved the posterior vertebral wall or annulus. This with the exception of 2 patients that had a delayed presentation and continued non-operative management successfully. We believe the contiguity of the posterior vertebral body margin has a key role in preventing distraction of the vertebral column and displacement of these fractures. This notion gives rise to the question of how it is possible for the fracture to distract anteriorly if the posterior vertebral body wall is continuous. A possible explanation is that the flexible properties of bone and of the posterior longitudinal ligament allow it to withstand distraction forces, this in a similar fashion to the posterior ligamentous complex. In a bone that is more brittle or in a fully ossified posterior longitudinal ligament we might expect that the fracture would therefore continue beyond the posterior vertebral body margin causing further instability. This could possibly explain why patients with AS whose vertebrae bear these qualities more so than those of DISH patients are more susceptible to unstable fractures. This should be further investigated with biomechanical studies. All but one patient in our cohort had fracture patterns that were entirely osseous or combined osseous-discal. The single patient with a trans-discal injury is a testament to our practice of treating purely discal injuries surgically given the presumably low union rate of a non-osseous injury. When healing does occur, it may rely on the formation of bridging osteophytes to stabilize the injury which can be unpredictable. The majority of patients in our cohort had an anterior opening of their fracture of 6 mm or under. Interestingly, the 2 patients who had a larger anterior opening of their fracture of 7 and 10 mm presented at follow up with increased segmental kyphosis of 20°. This could possibly be a testament to poor bone quality, spinal rigidity or general spinal alignment, although a conclusion cannot be drawn from such a small number of patients. Furthermore, These patients did not undergo MRI scans following their injury which could have possibly demonstrated involvement of the PLC that went undetected on CT imaging. An additional radiographic parameter studied was the type of ankylosing disorder the patient had. All patients in this group had DISH and not AS. This suggests that patients with AS could be prone to more unstable patterns as perceived by the treating surgeon such as fractures involving the posterior elements or trans-discal fractures. As such, we believe a more surgically aggressive approach should be applied for AS patients as opposed to those with DISH where nonoperative treatment is can be considered in certain cases.
Different methods of bracing have been previously described for the treatment of extension type fractures. For the cervical or cervicothoracic spine, a semi rigid collar with a possible additional chest extension or halo immobilization has been recommended.15-17 As poor outcomes of halo treatment in the elderly population have become more apparent, we refrain from utilizing halo stabilization in this patient population and have found good results with collar immobilization. In the thoracolumbar spine, an individualized fitted brace has been described as being needed in order to incorporate the patient’s existing deformity. 15 Furthermore, standard “off the shelf” 3-point fixation braces most commonly apply an extension force which could possibly distract the fracture further. We found the use of custom fitted braces an appropriate treatment option in our cohort for certain patients. However, some patients have been found unsuitable for brace immobilization due to breathing difficulties, associated pain and lack of comfort or a large body habitus. This consideration is particularly relevant to polytrauma patients where a brace could further comprehend breathing and mobility. Subsequently, 75% of patients in our cohort with thoracolumbar fractures were not immobilized with a brace and had good results. As brace fixation has been found to have questionable utility with other injuries such as burst fractures, 18 additional research regarding it’s utility in treatment of extension type fractures should be conducted.
Special attention should be paid to the patients whose fracture pattern warranted intervention but were deemed medically unfit to undergo surgery. This group’s exceptionally high mortality rate of 80% suggests that previous reports possibly underestimate the detrimental outcomes of non-operative management in this population. As stated previously, this could possibly be because studies have failed to differ between patients undergoing non-operative treatment due to their poor physical state or due to them being appropriate candidates for non-operative treatment. This finding warrants reevaluation of the benefits of pain relief and early mobilization provided by surgical intervention albeit the high surgical risk for this population.
This study has several limitations that bear mention. First, the retrospective design of the study harbours inherent limitations. An example of this is the bias of patient selection by the treating surgeons. A randomized control trial assessing outcomes between similar patients that were treated operatively and non-operatively would be more powerful in drawing conclusions regarding the utility of this treatment method. Furthermore, although we believe that a radiologic follow up of 3 months is sufficient for assessment of outcomes and clinical decision making, longer follow up with CT imaging for the entire cohort could be beneficial in understanding the natural history of these fractures. Given our institution’s patient catchment which includes rural and remote areas, this follow up is difficult to obtain, especially for patients who feel well and are hesitant to travel. Regarding clinical outcomes, we do not routinely use pain and functional scores in our clinic follow ups. This could allow better quantification of patient outcomes and thus yield stronger and more specific conclusions.
Conclusions
This study ascertains the need to reevaluate the role of non-operative management in patients with spinal ankylosing diseases presenting with an extension type fracture (AOSpine B3). We found that non-operative treatment is a valid treatment option for a patient with DISH that presents with a fracture which does not involve the posterior vertebral wall or annulus, is of an osseous or osseous-discal pattern and opens anteriorly up to 6 mm. These patients can be clinically assessed for pain and mobility and followed up closely with upright x-rays. Exceptionally high mortality rates in patients deemed medically not appropriate for surgical intervention warrants reevaluation of the benefits of early pain relief and mobilization despite the surgical risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.