
Abstract
Study Design
Retrospective Cohort.
Objectives
The objective of this study was to analyze postoperative complications in different mFI-11 groups after surgery for odontoid fractures in a geriatric population.
Methods
A single center retrospective review of odontoid fractures surgery (between 2013 and 2022) in patients aged 65 years and older was conducted. The primary outcome was the occurrence of a major complication (Calvien-Dindo ≥4) within 30 days post-surgery. The secondary outcome was the occurrence of a major complication within 3 months after surgery, and death within 1-month post-surgery. Survival curve, multi-variate analysis was performed and adjusted receiver operating characteristic curves were generated.
Results
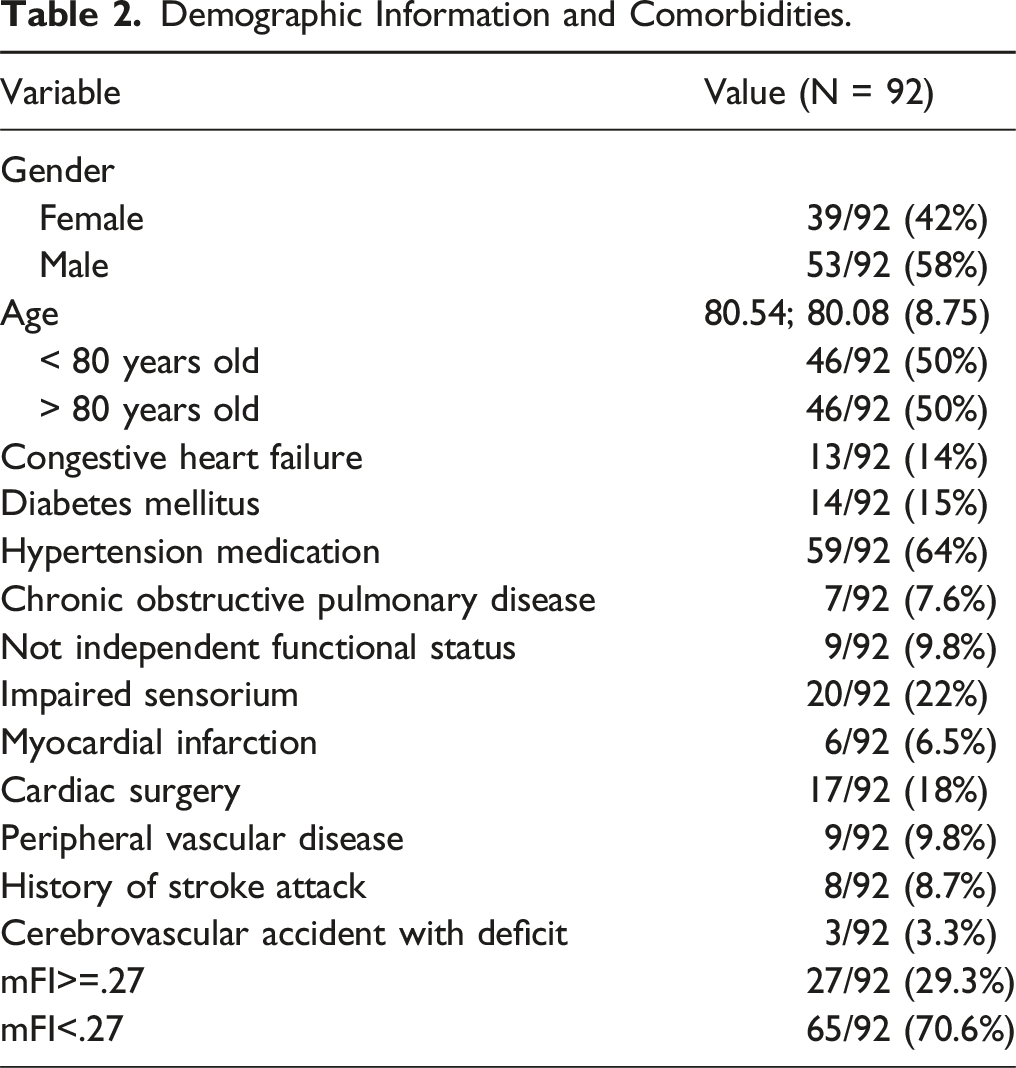
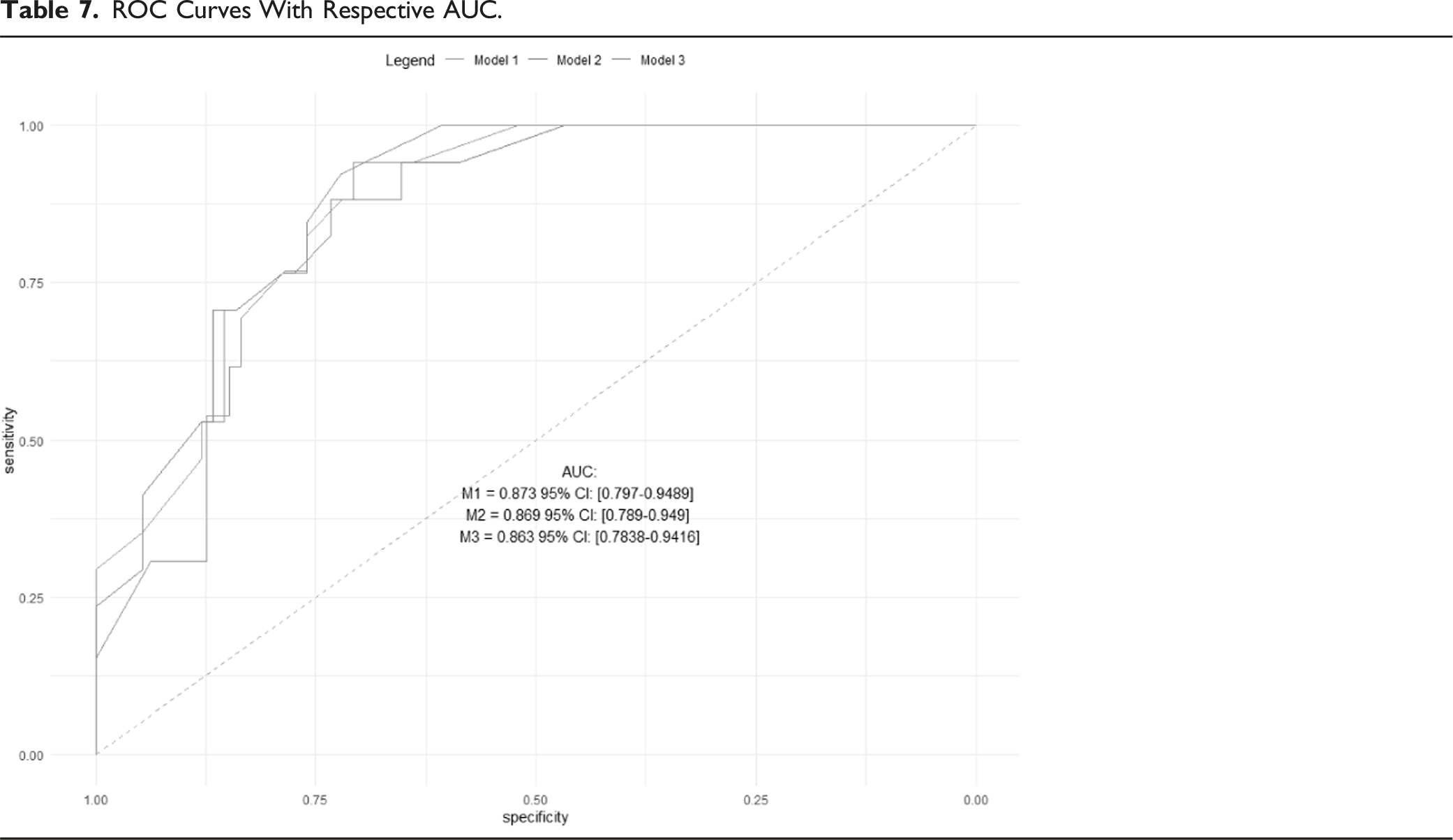
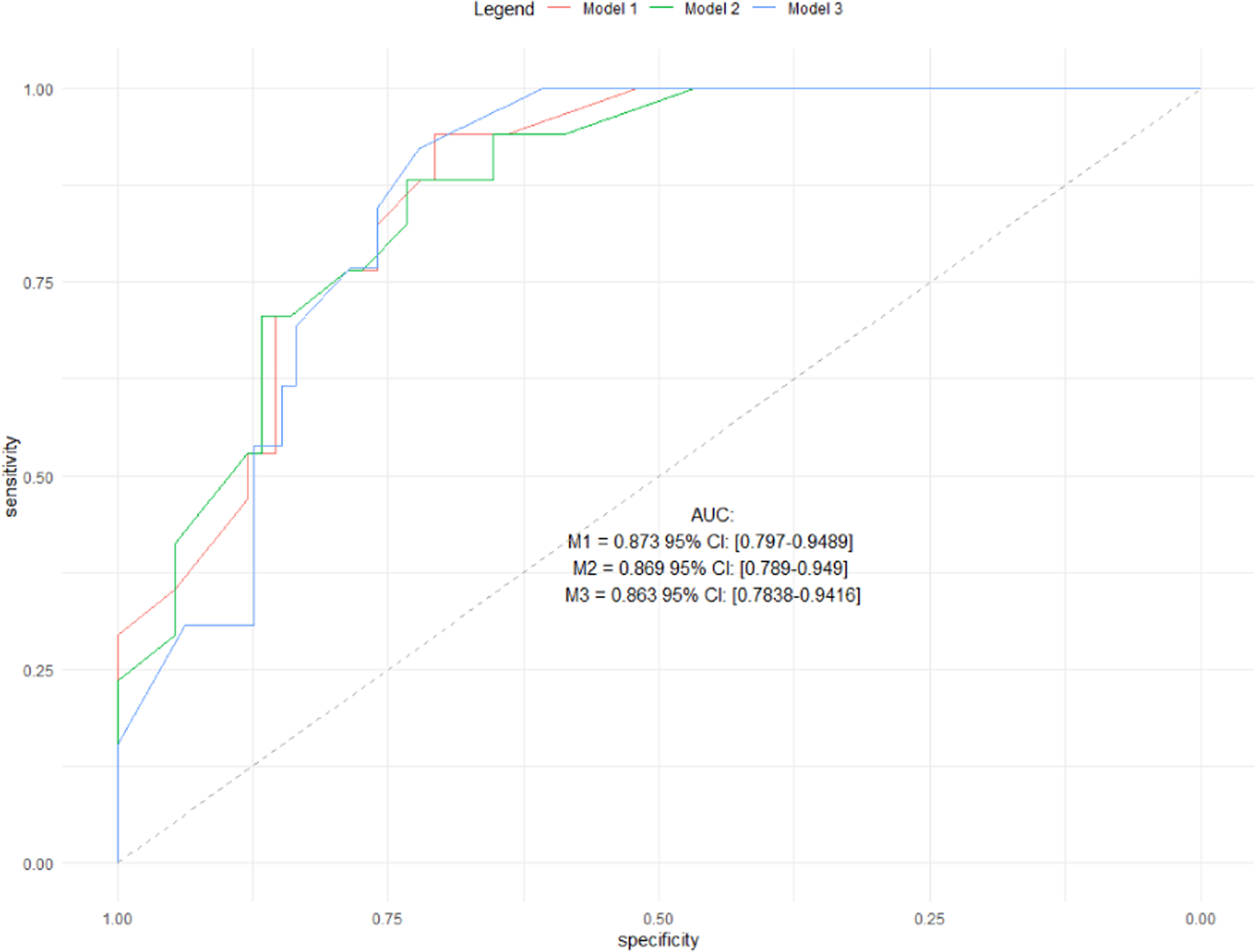
There were 92 patients included in this study, with a mean age of 80.5 years. Serious complication occurred for 16 patients (17%) during hospitalization. Multivariate analysis demonstrated an mFI 11 >.27 was strongly and independently associated with serious complications within 1-month post-surgery (OR = 16.7, 95% CI = 4.50-83), as well as serious complications within 3 months post-surgery (OR = 11.8, 95% CI = 3.48-49.1) and death within 1 month post-surgery (OR = 11.7; 95% CI = 3.02-60.4). The Receiver Operator Characteristics (ROC) curves for the three models all have an Area Under the Curve (AUC) value greater than 0.7.
Conclusions
The mFI-11 is a straightforward and validated tool that can be used during the preoperative period to identify the patient’s level of frailty and assess their risk of postoperative complications. Patients with mFI-11 ≥.27 are at greater risk of serious complications within 1 and 3 months’ post-surgery and death within 1 month post-surgery.
Introduction
Odontoid fractures are prevalent and account for 20% of all cervical fractures. Their incidence is estimated to be 14.9 cases per 100 000 people per year. 1 This injury is more prevalent among the elderly population. 2 Due to the increasing global aging population and advancements in diagnostic imaging, surgeons are increasingly encountering this condition and its management. This trend of increasing incidence is expected to continue.3,4
The Anderson and Alonzo classification is the most widely utilized in clinical practice. It categorizes odontoid fractures into three groups: 1, 2, and 3. Type 2 fractures refer to those in which the fracture line passes through the base of the odontoid process, and are considered unstable. 5
There are two possible therapeutic strategies: a conservative approach, which involves immobilization with a cervical collar, or a surgical approach, which can involve either an anterior or a posterior approach.6,7 Although surgical intervention for type 2 fractures is commonly accepted, there is no clear consensus. Surgery may reduce the rate of pseudoarthrosis, but it may also increase morbidity and mortality, particularly in the elderly population.6,8 However, it has been demonstrated that these pseudoarthroses are usually asymptomatic and that conservative treatment is effective and yields good functional outcomes in the elderly population as a first-line approach 9
Age, comorbidities, prior independence, and life expectancy are factors that influence morbidity and mortality as well as the outcome of surgical management.2,6-8 Therefore, it is crucial to identify a valid tool to objectively and quantifiably assess these factors in order to make an appropriate treatment decision.
Concept of frailty is increasingly used as a predictive factor of perioperative risk. It corresponds to a state of diminished physiological reserves necessary to overcome stress. It is not necessarily related to age. Its prevalence is estimated to be 4% among spinal surgery patients and 50% among the entire geriatric surgical population10,11 Standardized geriatric assessment is the gold standard for assessing frailty. However, due to its multidisciplinary and time-consuming nature, it is difficult to perform in the emergency setting. Alternative, more practical frailty assessment scores, such as the Charlson Comorbidity Index (CCI) 12 or modified Frailty Index (mFI-5 and mFI-11),13,14 have been developed for use in clinical practice. Among them, the modified frailty index 11 or five items is the most used in spine surgery. 15 It’s a simple form of the Canadian Study Of Health and Aging Index based on the theory of “accumulating deficits”. 13 Studies have shown that this score independently predicts the likelihood of adverse events post-spine surgery.10,16-20
To the best of our knowledge, there has not been a study that has evaluated the efficacy of the modified frailty Index 11
Materials and Methods
Study Design and Population
We conducted a retrospective analysis of 92 consecutive geriatric patients (over 65 years) who underwent stabilization surgery (LDCA005, LDCA004, LDCA006) for odontoid fractures or C2 pseudarthrosis from October 2013 to August 2022. All operated patients had a type 2 fracture according to the Anderson and D’Alonzo classification, diagnosed on a CT scan with indirect signs of instability (displacement or diastasis). The only exclusion criterion was being under 65 years of age. Data was collected from the medical records at Saint-Etienne University Hospital Center, including patient demographics (sex, date of birth), surgical details (duration, type), length of hospital stay, comorbidities, postoperative adverse events, and survival. The model variables were selected based on a prior literature review.
Frailty was assessed using the Modified Frailty Index-11 (mFI-11), which is an 11-item index that assesses comorbidities to stratify patient risk. The simplified frailty index is calculated as the number of present comorbidities divided by the total number of 11 items used in the mFI-11 assessment, which include diabetes mellitus, not independent functional status, chronic obstructive pulmonary disease, congestive heart failure, myocardial infarction, percutaneous coronary intervention or cardiac surgery or angina, hypertension medication, peripheral vascular disease, impaired sensorium, transient ischemic attack, and cerebrovascular accident. 13 The resulting score ranges from 0 to 1. According to literature, patients are considered frail if the score is above .27. 21
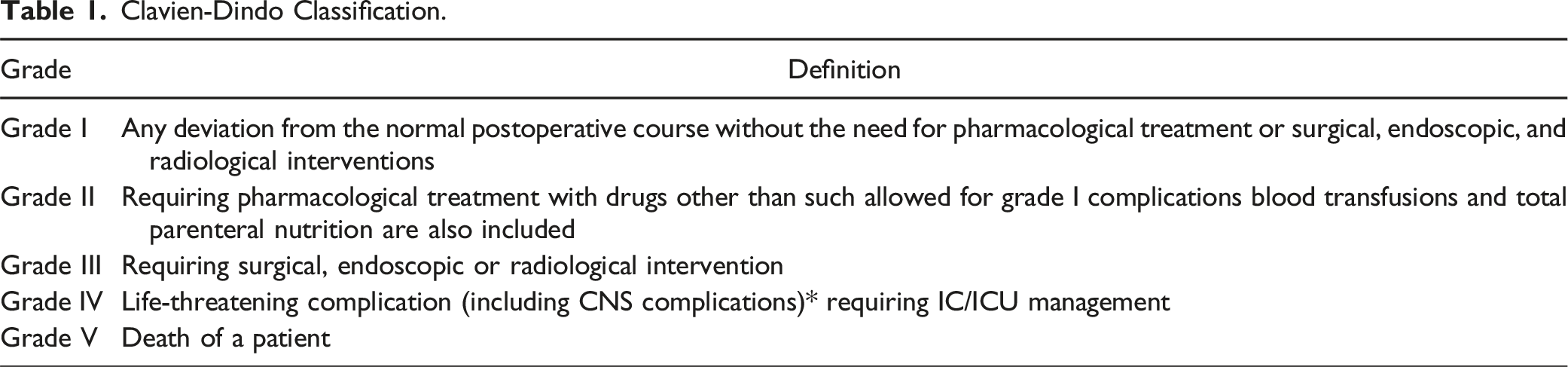
Clavien-Dindo Classification.
Statistical Analysis
The primary outcome was the occurrence of a major complication within 30 days post-surgery. A serious adverse event was defined as a life-threatening complication requiring ICU/ICU management or death as per the Clavien-Dindo classification. 22 The secondary outcome was the occurrence of a major complication within 3 months after surgery, and the third endpoint was death within 1-month post-surgery.
Categorical variables were summarized as frequencies (percentage) and continuous variables as means, medians and standard deviations. In order to study this association, multivariate logistic regression models were built. The models were constructed a-priori, before accessing the data. Potential confounders were included and selected based on previous knowledge from scientific literature, clinical knowledge and expert’s opinions on the subject. Variables selected as adjustment variables were age, sex, type of surgery (HARMS or non-HARMS), and length of surgery.
The first logistic regression model (model 1) evaluated the severity of the outcome as death occurring less than 1 month after the surgery and/or the presence of Clavien-Dindo 4 or higher post-operative complications.
The second model (model 2) evaluated the severity of the outcome as death occurring in less than 3 months after the surgery and/or the presence of Clavien-Dindo 4 or higher post-operative complications.
The third model (model 3) evaluated the severity of the outcome as death occurring less than 1 month after the surgery.
Results of models were presented as Odds Ratios with their respective 95% confidence intervals, as well as their P-values.
In addition, to validate and assess the capability of the mFI-11 cut-off to predict the severe outcome, the Area Under Curve (AUC) of the Receiver Operator Characteristics (ROC) curve of the model and its 95% confidence interval were calculated. An AUC >.6 would be considered as satisfying, an AUC >.7 as optimal, and an AUC close to 0 as unusable.
All statistical tests were two-sided, with P < .05 considered as statistically significant. Analyses were performed using the R software for statistical computing, version 4.2.2 (with packages “gtsummary” version 1.6.2, “ggplot2” version 3.4.0 and “pROC” version 1.18.0).
Ethical Review
This study was approved by the Institutional Review Board of the participating institution with a waiver of informed consent (IRBN182023/CHUSTE).
Results
Demographic Information and Comorbidities.
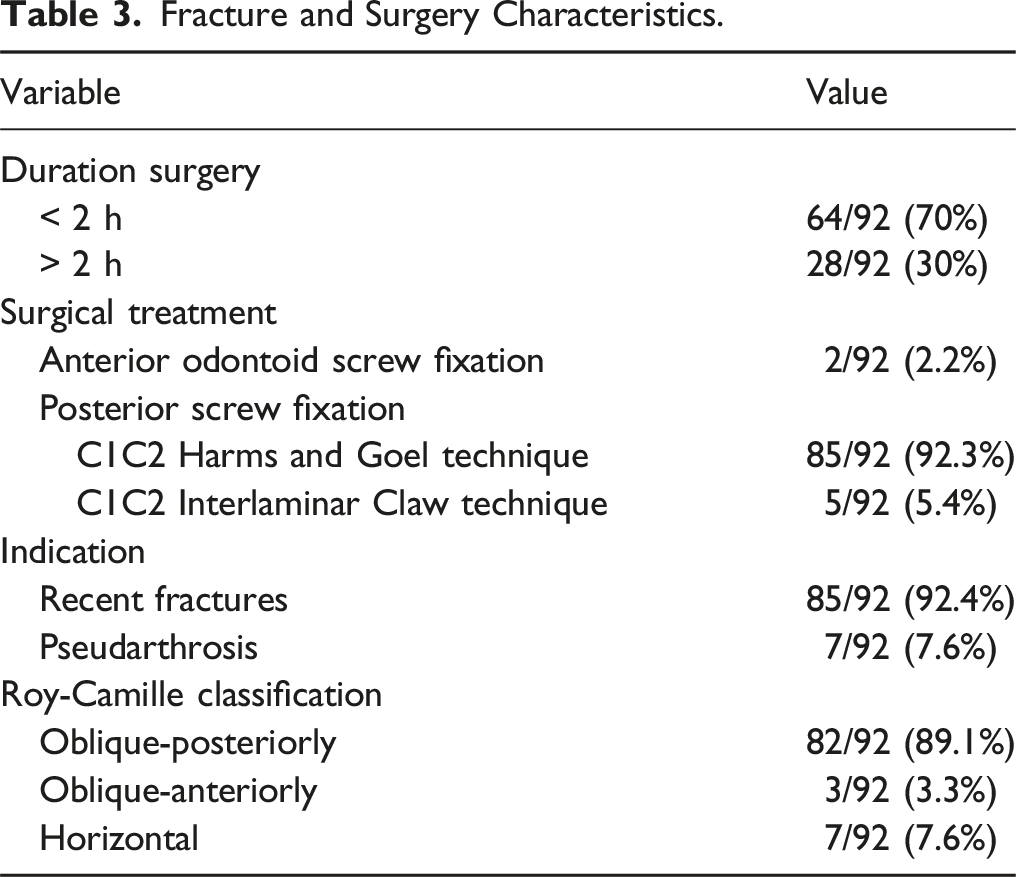
Fracture and Surgery Characteristics.
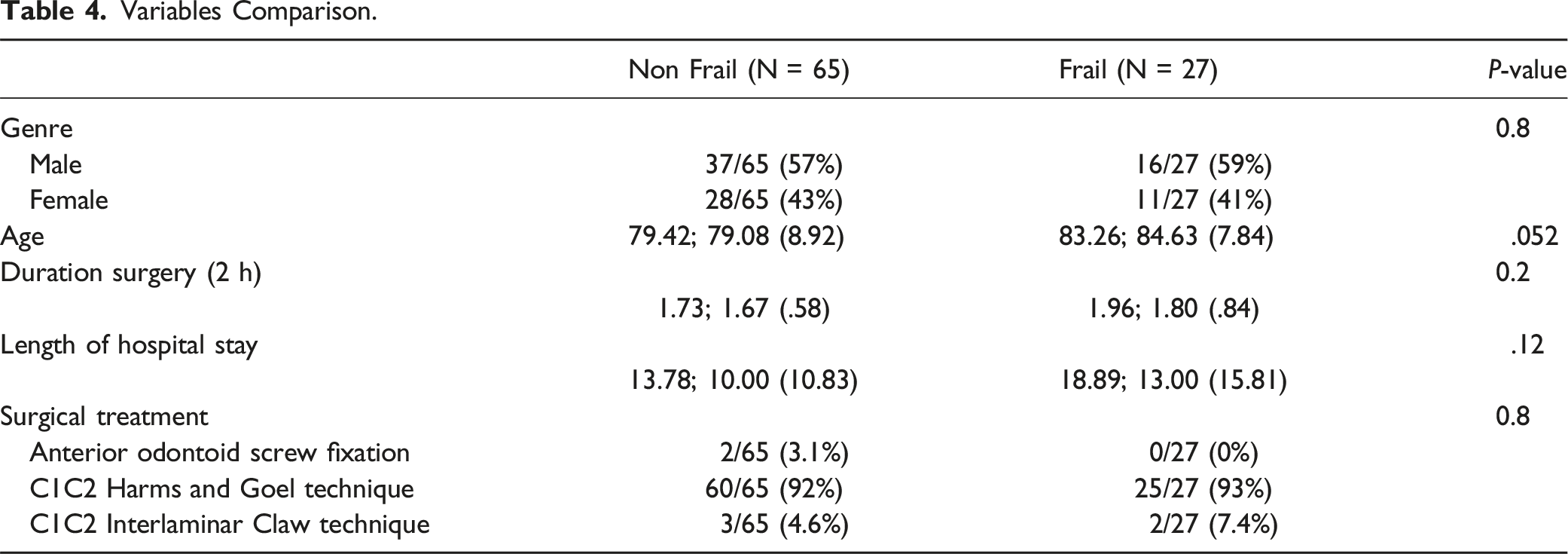
Variables Comparison.
Survival Curve According to Frailty.
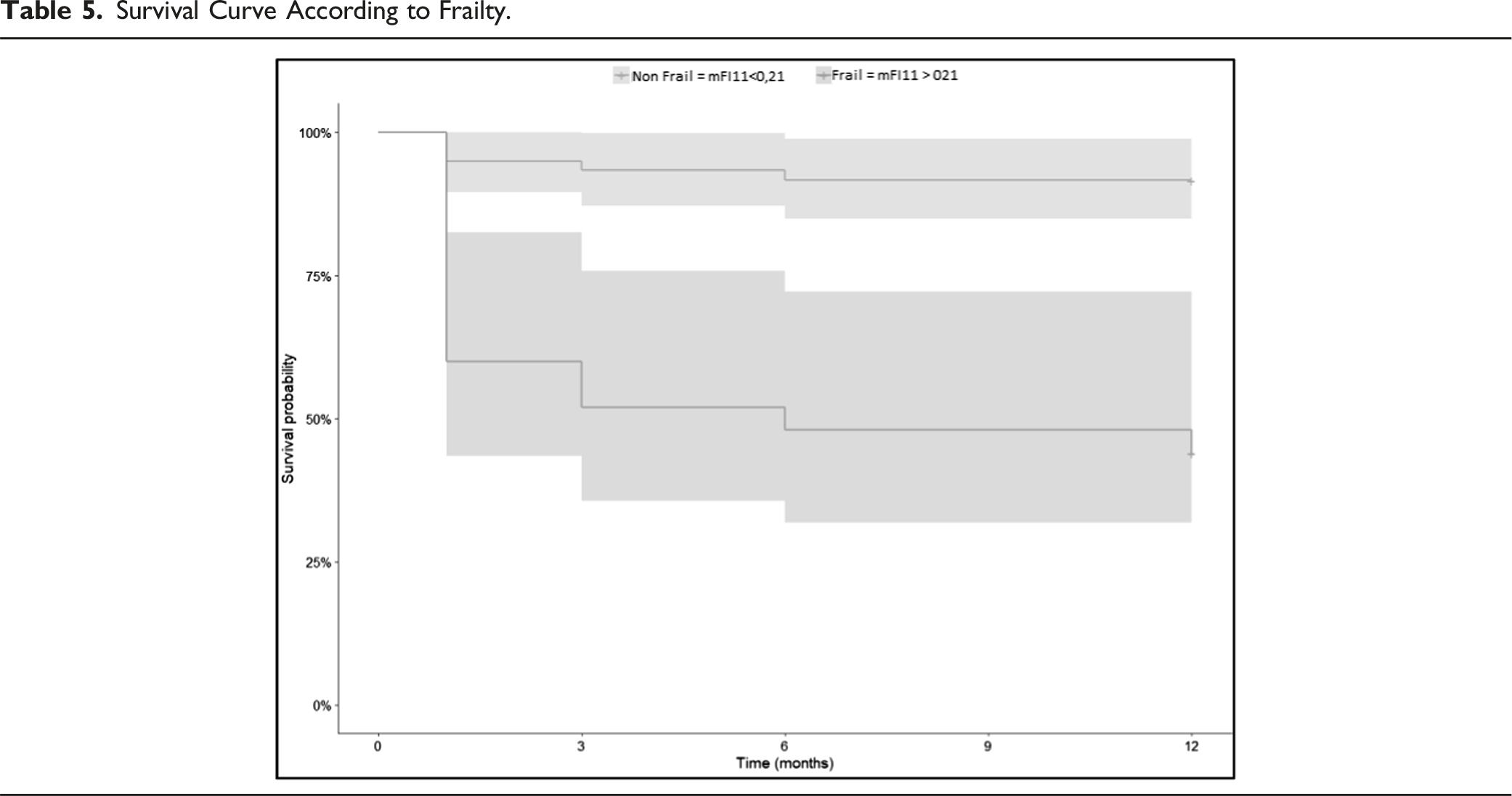
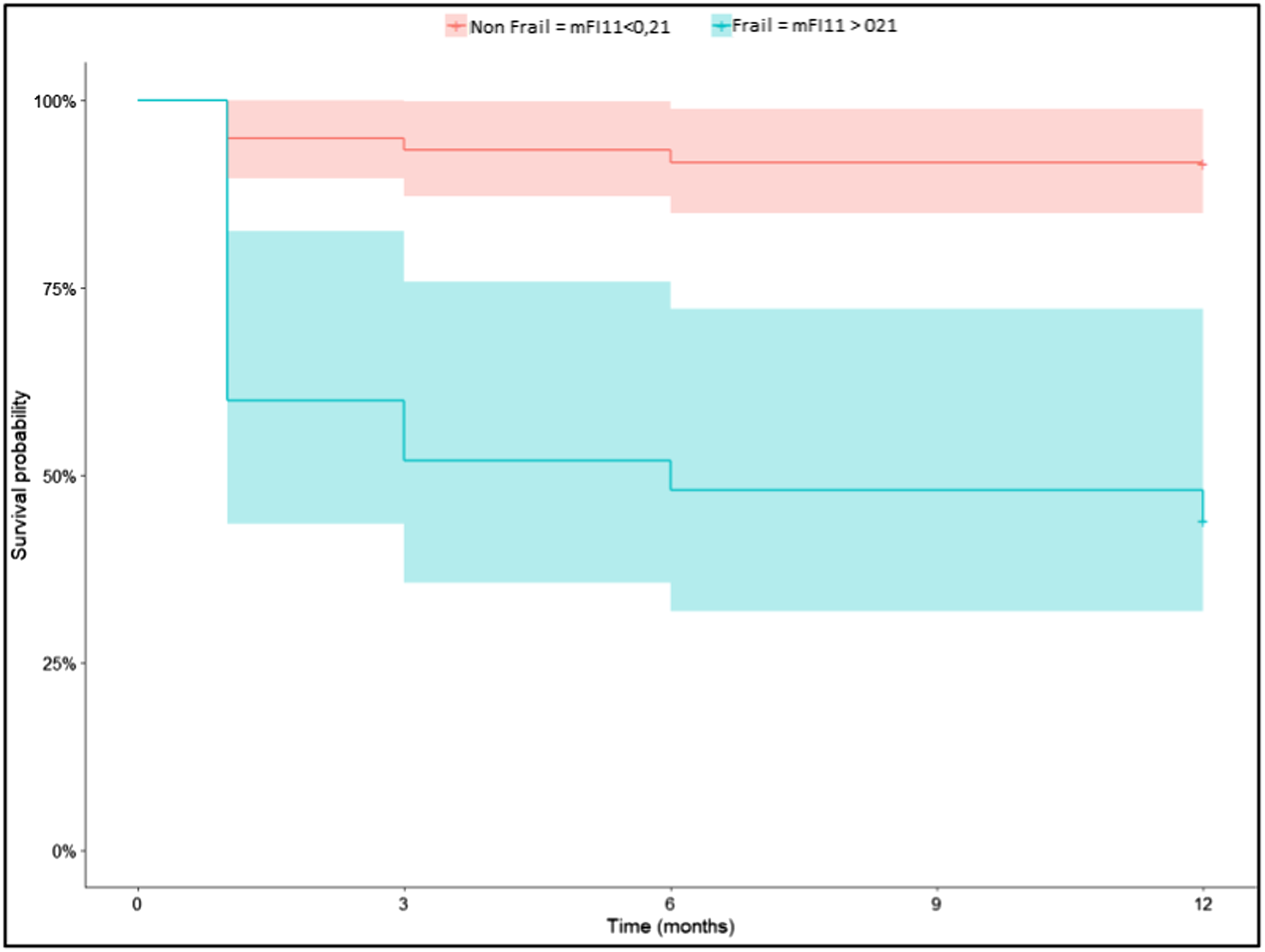
At least one complication occurred in 39% of the patients (n = 36). Among these complications that occurred during hospitalization, 16 (17%) were considered serious according to the Clavien-Dindo classification system, with a grade of IV or V. These serious complications included one case of pulmonary embolism, three cases of sepsis, two cases of acute respiratory failure, one case of acute renal failure, one case of rectum rectorrhagia, one case of anesthesia induction drug shock, and seven deaths without a known cause.
Logistic Regression Results.
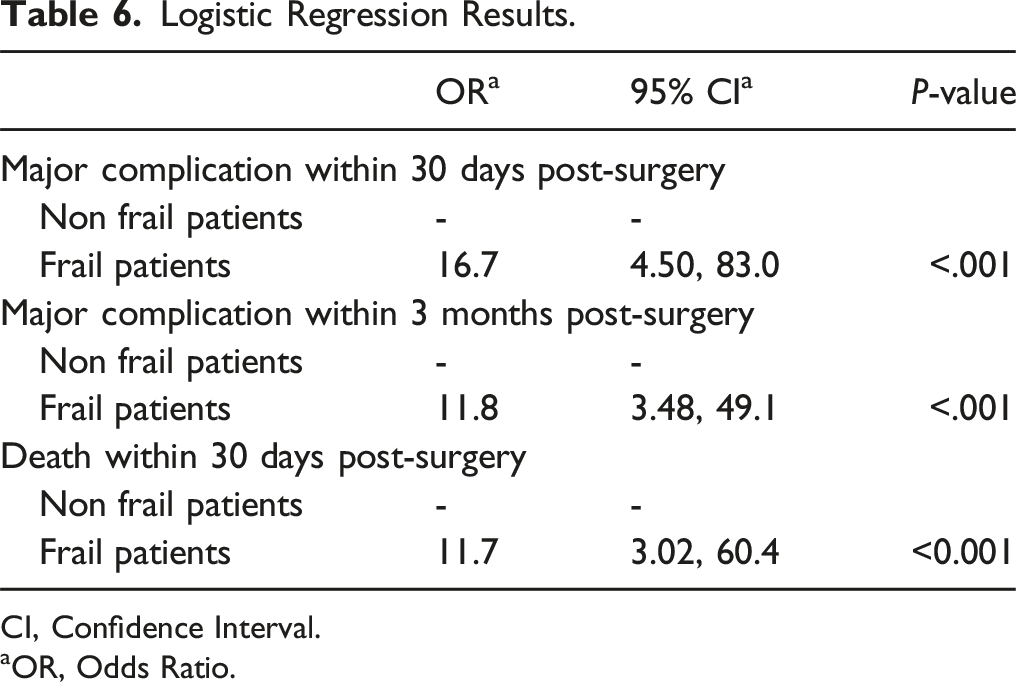
CI, Confidence Interval.
aOR, Odds Ratio.
ROC Curves With Respective AUC.
Discussion
The findings of our study indicate a substantial association between frailty and unfavorable outcomes following surgery for odontoid fractures in the geriatric population.
Type 2 fractures of the odontoid are frequently encountered by spine surgeons in clinical practice. This type of injury is common and often leads to unfavorable outcomes, particularly in the geriatric population. Additionally, the elderly demographic is one of the fastest growing segments of society. For instance, the number of individuals aged 75 years and above in France is projected to increase by 240% in 2040 compared to 1995. 23 As the population ages, there is still much debate regarding the surgical indication vs conservative management of type II odontoid fractures. Although these fractures are traditionally considered unstable, there is heterogeneity in indications depending on the medical teams. Some teams are increasingly questioning the dogma of surgical intervention in geriatric patients with a displaced type II odontoid fracture, due to the high morbidity and mortality associated with the surgery.9,24 They have reported the development of fibrous unions as a result of conservative treatment, which led to clinical functional outcomes that were either comparable to or better than those of surgery.25-27 However, conservative management also results in significant morbidity and mortality over the long term.28,29 Precisely predicting how geriatric patients will tolerate elective odontoid stabilization surgery presents a significant challenge for spine surgeons. It is important for surgeons to have knowledge of outcomes after odontoid fracture surgery for preoperative counseling and guiding treatment decisions. For these reasons, it is necessary to find practical prognostic tools for routine clinical practice to better select geriatric patients who may benefit from surgical management of type 2 odontoid fractures.
We investigated the effectiveness of the modified frailty index with 11 items in predicting perioperative morbidity in geriatric patients undergoing surgery for odontoid fractures. Our multivariate analysis revealed that this index had a significant level of accuracy in predicting post-surgery morbi-mortality.
There are several surgical techniques available for managing a type 2 odontoid fracture, including anterior screw fixation of the odontoid, C1C2 Harms and Goel Technique, and C1C2 Interlaminar Claw Technique. While the anterior approach appears to result in fewer complications, it is associated with a higher incidence of pseudoarthrosis when compared to the C1C2 Harms and Goel Technique.30-32 Most of the patients in our series underwent surgery using the Harms and Goel Technique. Similarly to Faure et al, 33 we believe that this technique has several advantages, including its applicability regardless of the type of fracture line, ability to achieve better fusion (particularly in elderly patients with osteoporotic bone), and alignment with the local surgeon’s experience.
The mortality during the follow-up in our series is similar to what has been reported in the literature, which ranges from 10% to 20% at 1 month and 10% to 40% at 1 year, irrespective of the therapeutic approach employed (surgical or immobilization).28,29,33-35 The overall rate of complications (39%) in our series is consistent with that reported in the literature.33,36
Some suggest that the decision to perform surgery or conservative treatment should be based on age due to varying results related to the rate of pseudarthrosis, mortality, and cost-effectiveness.32,34,37-39 We chose to include patients aged 65 years and older in our study, which is in line with previous studies on this topic.26,40,41 The average age of our study population (80.54 years) is similar to that of other studies.25,33 While we believe that the decision to pursue surgical or conservative treatment of a type 2 odontoid fracture in the geriatric population should be based on the patients’ frailty rather than their chronological age, we acknowledge that this hypothesis requires verification through a multicenter randomized clinical trial that compares conservative and surgical treatments in both frail and non-frail populations.
Although frailty is often correlated with age, it is a much broader concept that encompasses the principle of deficit accumulation and reduced physiological reserves to overcome stress. The modified frailty index score has already been shown to predict morbidity and mortality in many types of spine surgery.42-46 Numerous frailty scores have been developed and validated. While these scores have demonstrated their ability to predict morbidity and mortality in spine surgery, there is no consensus in the spine literature on the optimal frailty index for risk stratification. Some frailty indices have even been specifically developed for spine surgery.47,48 The American Society of Anesthesiologists (ASA) score has been shown to have similar or better discriminative abilities for perioperative adverse outcomes than the modified frailty index in posterior lumbar fusion. 49 However, the modified frailty index is still the most widely used frailty index in the spine surgery literature. 15
A few other studies have also shown the usefulness of preoperative frailty assessment for surgical management of C2 fractures.28,29,39,50 Carlstrom et al 50 evaluated mFI-5, CCI and Davies (Stokes) scores and found that increasing scores for all frailty indices were significantly associated with mortality. They also found that the predictive value of patient frailty status as an indicator of clinical outcome was preserved independent of initial management via operative or non-operative strategy. However, the study population in this series included only 11 surgical patients out of the 97 included, and they did not test mFI-11. Chapman et al 29 published a retrospective multicenter geriatric odontoid fracture cohort with 165 surgical cases, but their objective was to assess differences in short- and long-term mortality between operative and nonoperative treatment for elderly patients with type II odontoid fractures. They did not specifically test the capability of frailty indexes to predict post-surgery morbi-mortality. Shafafy et al 28 focused on a non-surgically treated cohort. Hamrick et al 39 treated a mixed cohort (surgical and conservative), but they found no statistically significant correlation between mFI-11 and mortality between their two groups on multivariate analysis. These results can be explained by their small sample size.
Our results should be interpreted in light of the strengths and weaknesses of our study. To the best of our knowledge, this study is comprised of the largest cohort of frail geriatric patients undergoing odontoid fracture surgery. We also benefitted from a relatively long follow-up period. Additionally, the choice of a simple and objective primary endpoint (occurrence of a serious adverse event during the first 30 days) helped to reduce the study’s vulnerability to systematic errors.
However, our study also has several limitations that should be acknowledged. First, it is a retrospective single-center study, which limits the generalizability of our findings to other settings. Second, we did not assess functional outcomes or quality of life, which are important outcomes in geriatric patients. Additionally, we only assessed outcomes predicted by one frailty index, which may reduce the strength of our conclusions. Moreover, mFI-11 doesn’t consider the severity of its elements, potentially resulting in single-item patients not being labeled as frail. This approach might overlook a patient with a severe single comorbidity that would still be fragile. Finally, we found that frailty was associated with increased postoperative serious complications, we were not able to compare our results with the outcomes of frail patients undergoing conservative treatment, as Hamrick et al 39 did. Future studies should ideally use a randomized controlled design and include a larger sample of patients across multiple institutions to further investigate the relationship between frailty and surgical outcomes in the geriatric population.
The widespread use of neuronavigation is expected to lead to a reduction in perioperative morbidity in elderly patients undergoing surgery for this type of fracture. The use of this technology is expected to reduce the incidence of implant malposition, minimize intraoperative bleeding, and expedite reverticalization.
Conclusion
The mFI-11 is a straightforward and validated tool that can be used during the preoperative period to identify the patient’s level of frailty and assess their risk of postoperative complications. This information can guide the surgeon in the decision-making process and facilitate informed discussions with the patient about the potential risks and benefits of the surgical procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.