
Abstract
Study Design
systematic review.
Objective
To evaluate risk factors associated with failure of non-operative management of isolated unilateral facet fractures of the subaxial cervical spine in neurologically intact patients.
Methods
A systematic review of the PubMed, Embase, LILACS, and Cochrane Library databases was conducted in order to determine risk factors associated with failure of non-operative management in isolated unilateral facet fractures of the subaxial cervical spine without facet and/or vertebral displacement, in neurologically intact patients. Our research was in line with the PRISMA Statement and registered on PROSPERO (CRD42023405699).
Results
A total of 1639 studies were identified through a database search on May 5, 2023. In total, 7 studies from the databases were included, along with 1 study found through a manual citation search. The evidence showed high clinical heterogeneity, a serious risk of bias according to the ROBINS-I tool, and a predominance of retrospective cohort studies. In comparison to less complex facet fractures, lateral floating mass fractures were found to have 5.41 times higher odds of failure of non-operative management (OR = 5.41; 95% CI = 1.32, 22.19). We calculated the potential association between lower absolute fracture height and non-operative treatment success [Fracture height (percentage) Mean Difference = −17.51 (−28.22, −6.79 95% CI); Absolute height Mean Difference: −0.46 (−0.60, −0.31 95% CI)]. Other risk factors were not included in the meta-analysis due to lack of data. The level of certainty was rated as “very low”.
Conclusions
Lateral floating mass cervical facet fractures and larger fracture fragment size (measured either in absolute terms or as a percentage) are significant risk factors for failure of non-operative treatment.
Introduction
Traumatic cervical facet injuries encompass a broad spectrum that can range from unilateral non-displaced facet fractures to bilateral facet fractures with joint dislocations with or without neurological injury. Traumatic unilateral non-displaced, as well as minimally subluxed cervical facet fractures are often underdiagnosed, even among trained surgeons. 1 In recent years, cervical facet fractures have been identified more frequently and at an earlier stage thanks to computed tomography (CT), which offers comprehensive imaging angles and multiplanar reconstructions, providing critical information during the initial assessment of trauma patients. 2
However, the management of isolated subaxial facet fractures remains a subject of debate, particularly when dealing with neurologically intact patients. This may be attributed to their relatively low frequency compared to other injuries, representing only 5% of all cervical spine injuries in traumatic case series, as well as the diversity in their morphological presentation.1,3-6 One of the primary challenges in the decision-making process for these cases is determining the presence of mechanical instability.7,8 Both unilateral non-displaced facet injuries and minimally subluxed injuries, particularly those without neurological deficits, are often treated with non-operative management using a cervical orthosis for several weeks. 1 Despite apparent mechanical stability during the initial assessment, subsequent symptomatic facet and/or vertebral displacement may develop, making surgical treatment necessary for these injurie.
Additionally, studies have shown that patients with unilateral cervical facet fractures involving 40% of the absolute height of the intact lateral mass, or those with an absolute height of 1 cm, are at an increased risk of failure of non-operative treatment. These criteria have since been incorporated into the AO Spine Subaxial Cervical Spine Classification System, which describes 4 morphological types of injuries to the facet component. 4 Despite its widespread use among spine surgeons, the potential instability of the so-called F2 and F3 fractures remains a topic of debate,9,10 as there is significant variability in the accuracy and reliability of the classification for these injuries. Therefore, this study aimed to evaluate risk factors associated with failure of non-operative management of isolated unilateral facet fractures of the subaxial cervical spine in neurologically intact patients. 11
Material and Methods
A systematic review of the literature was conducted to identify risk factors associated with failure of non-operative management in isolated unilateral facet fractures of the subaxial cervical spine without facet and/or vertebral displacement in neurologically intact patients. This systematic review was performed in accordance with the PRISMA 2020 Statement and registered in PROSPERO (CRD42023405699). 12
A clinical question was formulated using the PICO acronym to clarify the scientific problem and guide eligibility criteria.
Criteria for Study Inclusion in This Review
Studies Were Selected according to the following Criteria
- - - - - -
Search Methods for Study Identification
Data Sources
We conducted a search across several databases, including MEDLINE (PubMed), Embase (OVID), LILACS, and the Cochrane Library, as well as the reference lists of the included studies and relevant reviews identified during the search (snowballing).
Search Strategy
We formulated our literature search strategy by employing Medical Subject Headings (MeSH) and relevant entry terms pertaining to subaxial cervical facet fractures. The following search strategy was specifically created for the MEDLINE database: (facet OR zygapophyseal joint) AND (cervical) AND (spine OR vertebral column) AND (fracture OR injury). The search was not restricted by study design or language; however, due to resource limitations, only studies published in English, Portuguese, or Spanish were ultimately included. We searched from the earliest available date to May 5, 2023. The original MEDLINE search strategy was subsequently adapted to the syntax and subject headings of the other databases. After identifying relevant studies, the reviewers examined their references to find additional pertinent articles.
Data Management
The results of the literature search were uploaded to Zotero Reference Manager (Corporation for Digital Scholarship, 2023), a web-based application that facilitates collaboration among reviewers during the study selection process. Duplicates were removed, and prior to the formal screening process, training was provided to new members of the review team who were unfamiliar with citation management software.
Selection Process
The selection process was conducted by four reviewers, divided into two groups, who independently screened the titles and abstracts according to the inclusion criteria. Disagreements were initially addressed through discussion among the reviewers and, if unresolved, were settled by consultation with an expert researcher not involved in the screening process. Once articles were selected for full-text review, they were retrieved from their respective sources. Each group of reviewers then evaluated the full-text articles selected by the other group in a crossover design to minimize potential selection bias. During the review, the references in the selected articles were also checked for additional eligible studies (snowballing). Any conflicts that arose were initially resolved through discussion among the reviewers, and, if needed, by consulting a third-party expert.
Data Collection and Analysis
Data Extraction
Data extraction was also carried out in duplicate by independent reviewers. The data were organized into two separate tables: one containing the study characteristics and another summarizing the findings. The study characteristics included study design, diagnosis and selection criteria, participants, intervention and comparator, outcomes, follow-up period, as well as information on funding and potential conflicts of interest. The abstracted data focused on failure of non-operative management (defined by the rate of pseudarthrosis), posterior translation, new neurological injury (radicular or spinal cord injury), pain, and other relevant outcomes. Successful treatment was defined as the absence of any of these occurrences during follow-up. Disagreements between reviewers were resolved through discussion and, if necessary, by consulting a third-party reviewer.
Risk of Bias Assessment
Given the nature of the included studies, these were evaluated for risk of bias using the ROBINS-I tool for non-randomized exposure studies. 13
Effect Measures and Statistical Analysis
For continuous variables, the mean difference with a 95% CI was calculated, while for dichotomous outcomes, the odds ratio with a 95% CI was determined using the Mantel-Haenszel method. A random-effects model was employed, and statistical heterogeneity among studies was assessed using the Tau 2 test. A two-tailed P-value of less than 0.05 (P < 0.05) was considered significant. Data analysis and synthesis were performed using RevMan (Review Manager), v. 5.4.1 (The Cochrane Collaboration, 2020).
Strategy for Data Synthesis and Quality Assessment
The results from individual reviewers were consolidated into a single data table. The entire review team then discussed this table to reach a consensus on the findings. Additionally, the data was evaluated for its suitability for quantitative meta-analysis, and the GRADE approach was employed to assess the certainty of the evidence. 14
Results
We identified a total of 1639 studies during our search in May 2023. After removing duplicates, we screened 1567 studies based on their titles and abstracts, ultimately retaining 1544 for further consideration. A full-text assessment was conducted on 23 studies that potentially met the inclusion criteria,1-3,6,8,10,15-32 leading to the exclusion of 16 of them. Finally, after reviewing the full texts, 7 studies were included in the present systematic review.2,3,8,10,15,17,18 In addition, we identified 2 studies through manual citation search,16,33 of which only one was included.
16
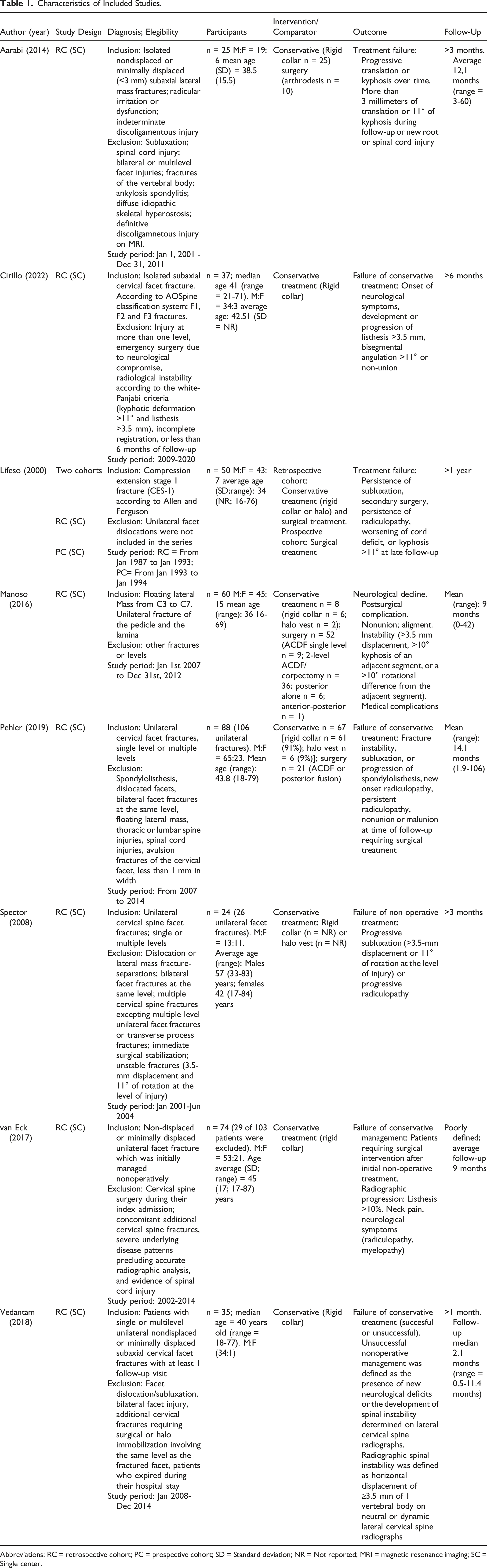
Therefore, we obtained a total of 8 articles for this review (Figure 1). Table 1 summarizes the characteristics of the studies. PRISMA flowchart. Characteristics of Included Studies. Abbreviations: RC = retrospective cohort; PC = prospective cohort; SD = Standard deviation; NR = Not reported; MRI = magnetic resonance imaging; SC = Single center.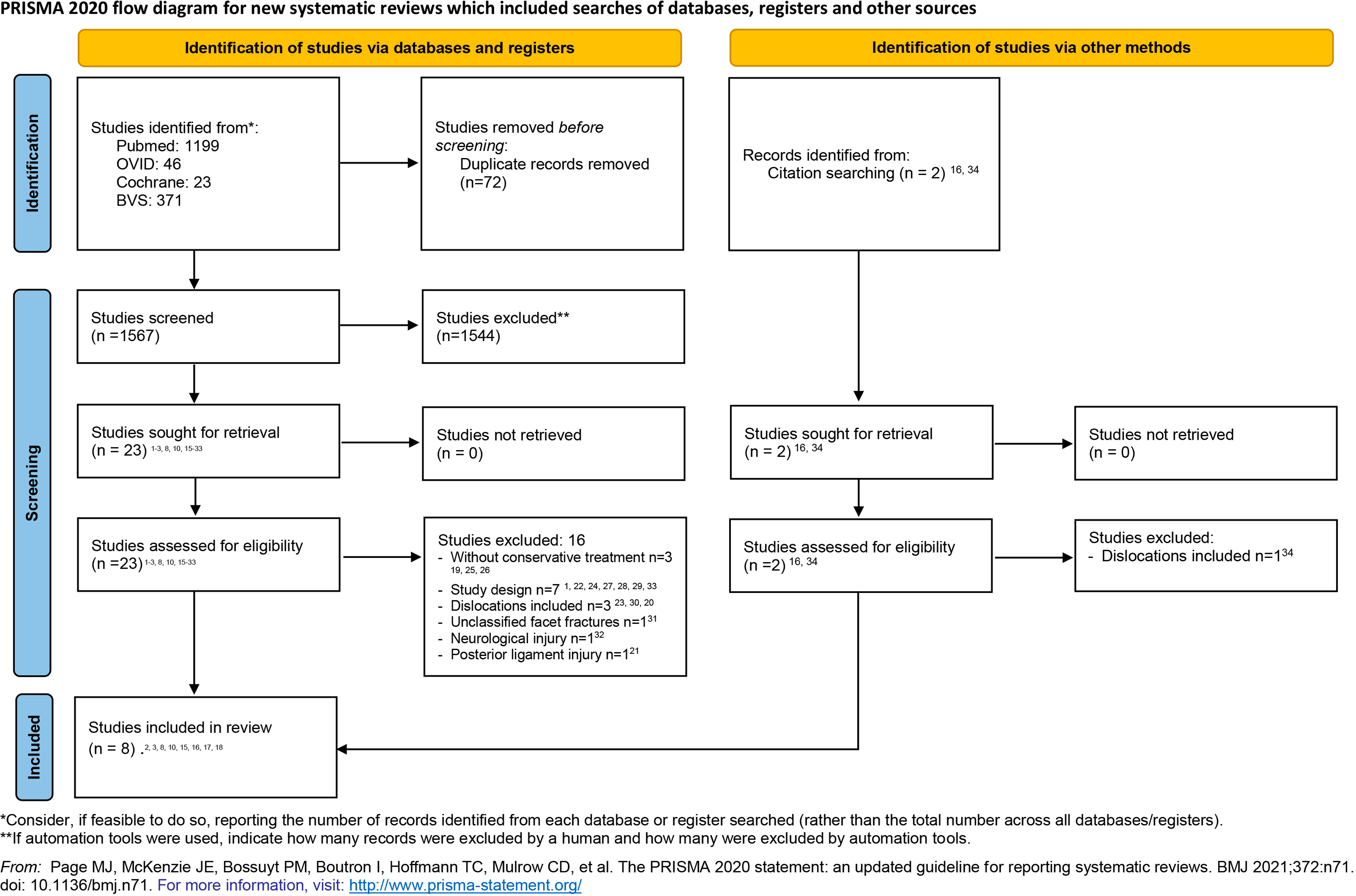
Risk of Bias Assessment
Risk of Bias (ROBINS-I).
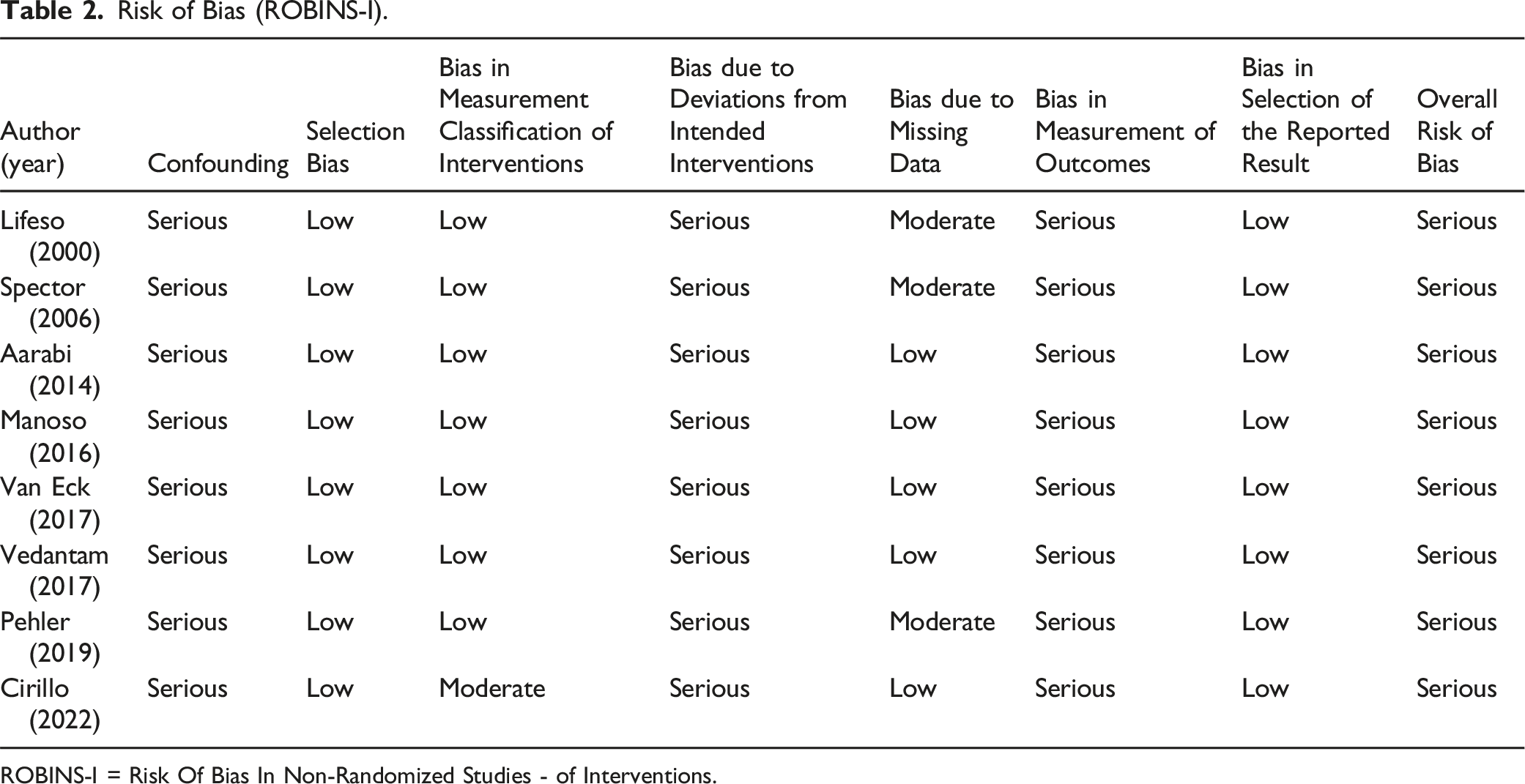
ROBINS-I = Risk Of Bias In Non-Randomized Studies - of Interventions.
Data Extraction and Synthesis
Failure of non-operative management was analyzed based on the presence or absence of the following risk factors:
Facet Fracture Subtype
Our review identified only two studies that considered fracture subtype as a risk factor for unsuccessful non-operative management, specifically distinguishing floating lateral mass fractures from other simpler subtypes.3,16 Both studies employed a similar definition of unsuccessful non-operative management, defined as a translation of more than 3.5 mm of the vertebral body. Despite using different facet injury classifications (A3 from Dvorak,
20
and F3 from AOSpine
4
), both papers compared floating lateral mass fractures with less complex fractures. Unsuccessful non-operative management was categorized into two types: floating lateral mass fractures and other types (F1/F2 or A1/A2). The analysis included data from two studies with a total of 72 participants who underwent non-operative management. Individuals with a floating lateral mass fracture were estimated to have 5.41 (OR = 5.41; 95% CI = 1.32, 22.19) times higher odds of experiencing unsuccessful non-operative management compared to those with less complex facet fracture subtypes (P = 0.02) (Figure 2). No heterogeneity was detected among the results (Tau2 = 0.00). Forest plot of failure of non-operative management according to the morphology of cervical facet fractures (“floating lateral mass” in comparison to other subtypes).
Height of the Cervical Facet Fracture as a Percentage
The height of the cervical facet fracture was expressed as a percentage of the remaining intact facet height. Two studies measured this height as a percentage of the intact facet height: Spector et al
2
(the original author who proposed this method) and Pehler et al.
17
Data from these two studies were summarized, which included 93 participants who received non-operative treatment for F1 or F2 facet fractures. The inverse variance method with random effects model was applied to calculate the mean difference, which was determined to be −17.51 (95% CI = −28.22, −6.79). This indicates a significant reduction in the mean height of facet fractures among individuals who underwent successful non-operative management. Furthermore, there is a potential association between the percentage reduction in fracture height and the effectiveness of non-operative management (Figure 3). High heterogeneity was detected among the results (Tau2 = 34.23). Forest plot of cervical facet fracture height (in percentage) according to non-operative management.
Absolute Cervical Facet Fracture Height
Based on the results of two studies,2,17 the meta-analysis of cervical facet fracture height (in cm) in relation to treatment outcomes (successful vs unsuccessful non-operative management) reveals a mean difference of −0.46 (calculated using the inverse variance method with random effects model) and a 95% confidence interval of [-0.60, −0.31]. This result indicates a statistically significant decrease in the absolute height of facet fractures among individuals with successful non-operative management compared to those with unsuccessful non-operative management. The negative mean difference demonstrates a notable reduction in fracture height and an association between lower absolute fracture height and success in non-operative treatment. No heterogeneity was observed among the results (Tau2 = 0.00) (Figure 4). Forest plot of cervical facet fracture height (absolute) according to non-operative management.
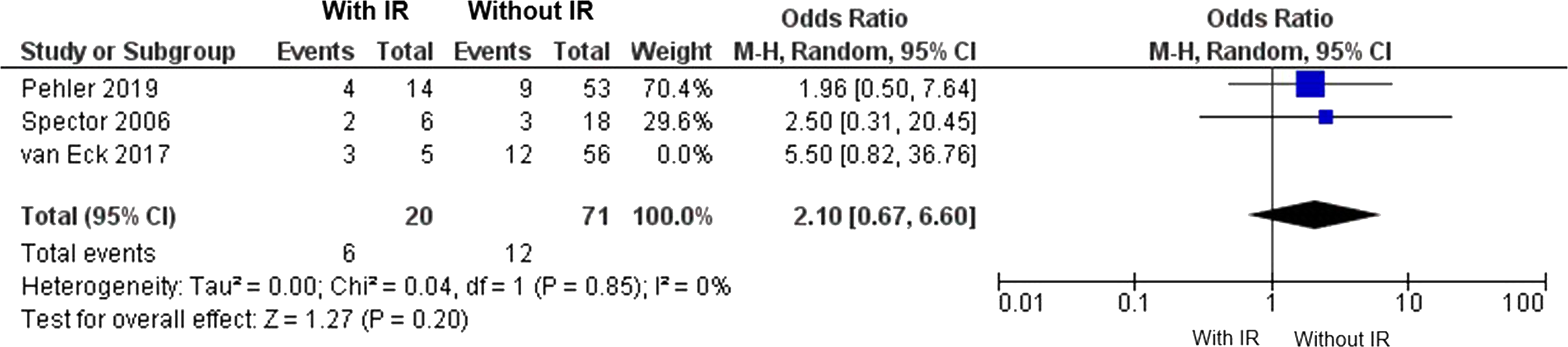
Presence of Radiculopathy on Admission
Three studies2,17,18 involving 111 patients reported the presence of irritative radiculopathy upon admission in patients with isolated cervical facet fractures. The pooled analysis evidenced an odds ratio of 2.72 (M-H, random effect) [95% CI = 1.02, 7.24]. The analysis of the confidence interval reveals a lower limit of 1.02, which is very close to 1 (no effect), suggesting a very weak association (Figure 5). Additionally, because the study population in van Eck et al
18
included floating lateral mass fractures (unlike the studies by Pehler
17
and Spector
2
), we conducted a second pooled analysis that excluded the van Eck study.
18
In this analysis, the effect size decreased, and the confidence interval included 1, indicating no significant differences between groups based on the presence or absence of associated irritative radiculopathy (Figure 6). Forest plot of failure of non-operative management according to the presence of irritative radiculopathy (IR) on arrival. Forest plot of failure of non-operative management according to the presence of irritative radiculopathy (IR) on arrival, excluding patients from the van Eck study.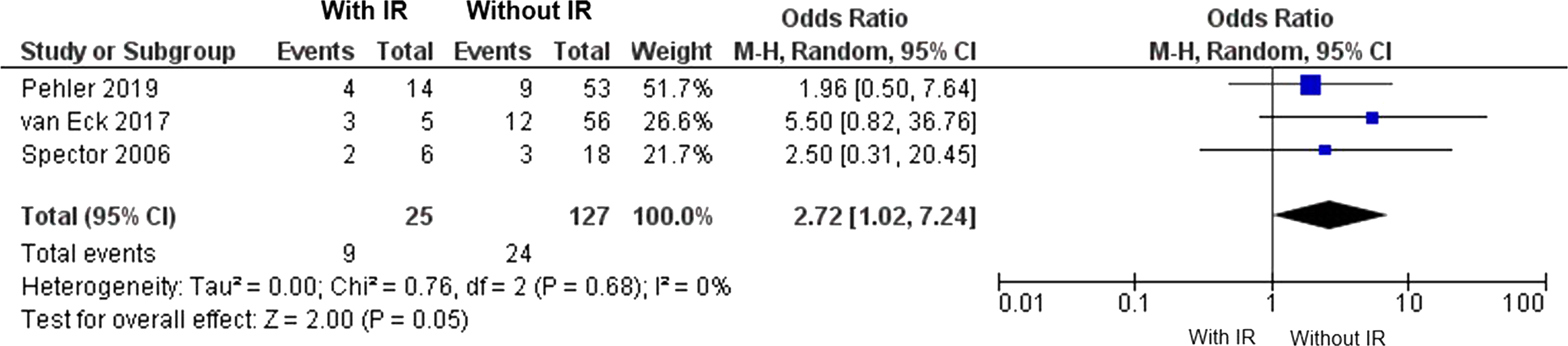
Other Documented Risk Factors
Additional risk factors were identified through this systematic review. However, due to their isolated description in the literature, insufficient data, or significant clinical heterogeneity in their definitions, a pooled analysis was not feasible. These other documented risk factors include acute disc injury,10,16 comminution,17,18 and patient weight and body mass index.17,18
Summary of Findings: Risk Factors for Failure of Conservative Treatment in Cases of Isolated Unilateral Subaxial Cervical Facet Fractures Without Displacement or Neurological Injury.
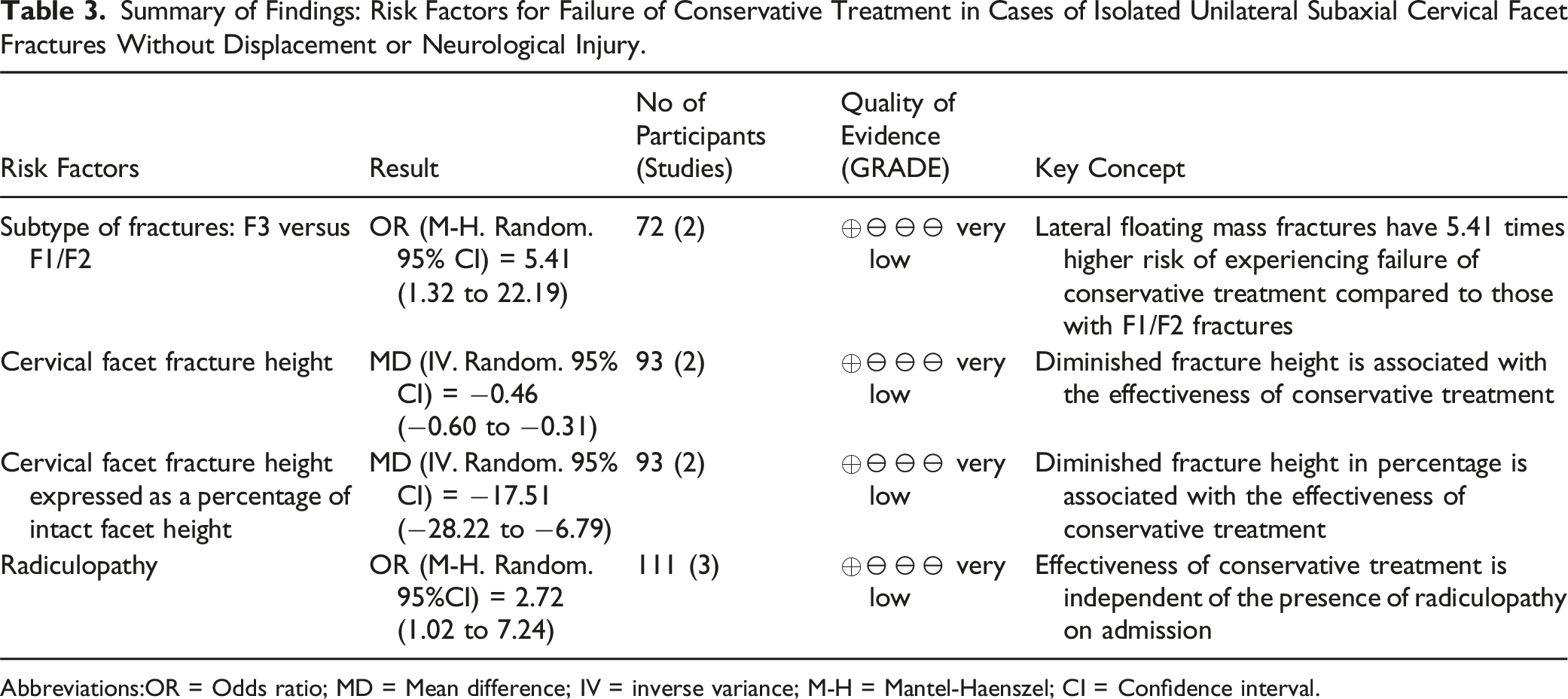
Abbreviations:OR = Odds ratio; MD = Mean difference; IV = inverse variance; M-H = Mantel-Haenszel; CI = Confidence interval.
Publication Bias
The assessment of publication bias in a meta-analysis with fewer than 10 studies is inherently limited and requires a combination of approaches. Standard statistical tools cannot be relied upon exclusively, making a qualitative assessment essential. The various comparisons made in the present paper involved results from only 2 or 3 trials, which adds to the challenge. A funnel plot is a common tool for detecting publication bias; however, with only two studies, it is not useful, as it does not provide enough information to assess symmetry. Additionally, specific tests, such as Egger’s test for funnel plot asymmetry, are not applicable with just two studies. A qualitative assessment of the studies may provide indications of publication bias. It should be noted that cervical facet fractures are frequently overlooked, which leads to their prevalence and publication being underrepresented in the literature. Moreover, the spine medical specialty is predominantly surgical, likely resulting in fewer publications on non-surgical treatments compared to innovative surgeries, which may have industry support. Finally, the low quality of the studies, particularly the high selection bias, could further justify suspicion of potential publication bias.
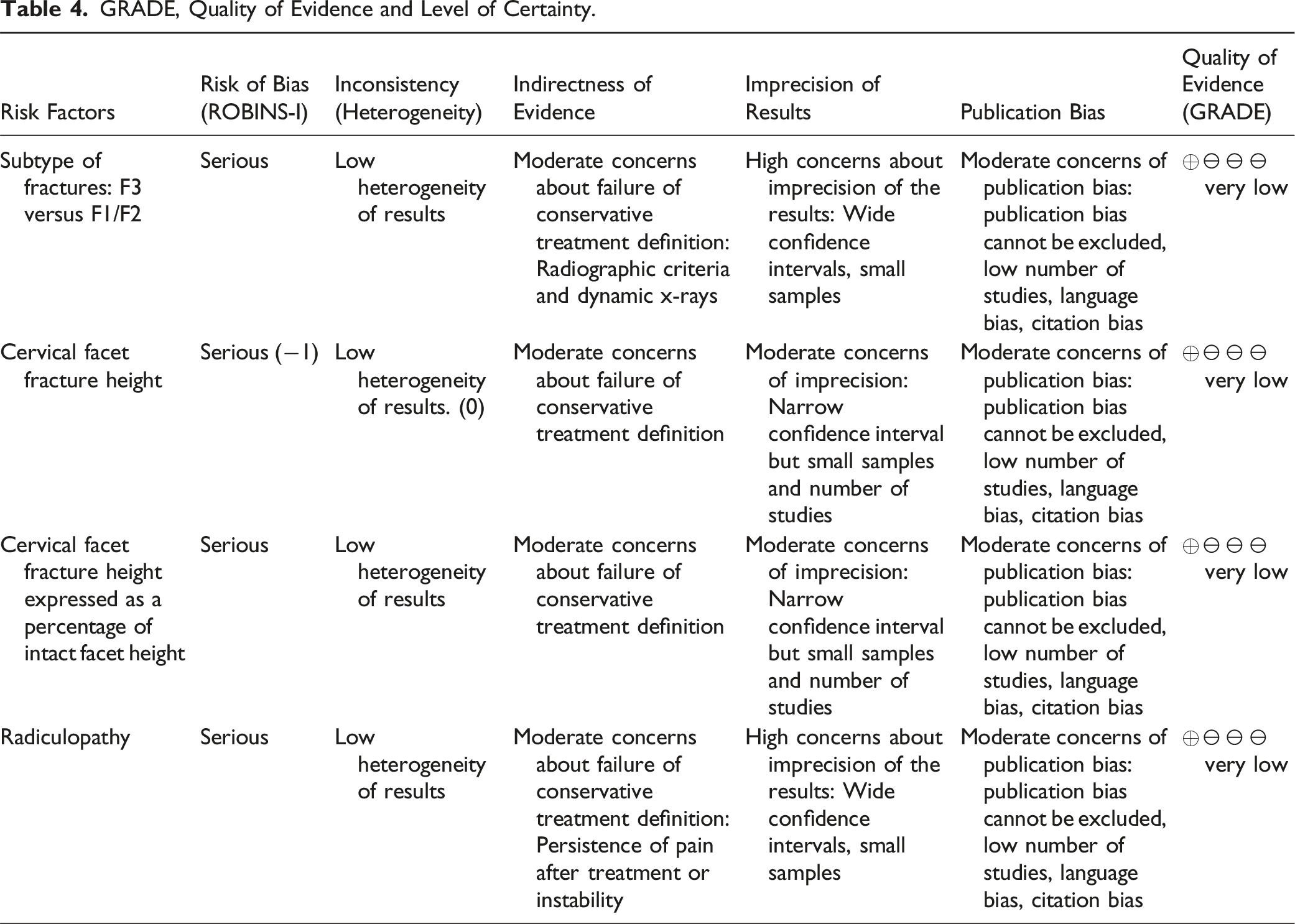
Level of Certainty
GRADE, Quality of Evidence and Level of Certainty.
Discussion
Several classification systems have been proposed to assess cervical facet injuries.4,7,20,25,33 However, aside from clearly unstable fracture-dislocations, many facet injury patterns remain uncertain in their potential for mechanical instability.
Classical systems have traditionally focused on the mechanism of injury extrapolated from static X-rays, as proposed by Allen et al, in 1982. 7 Kotani et al introduced a new classification of lateral mass fractures based on a retrospective case series analysis. This classification incorporates the use of X-rays and magnetic resonance imaging (MRI) of soft tissue. They identified four subtypes of lateral mass fractures: separation fracture (also known as “floating lateral mass”), comminution type, split type (characterized by a vertical fracture line on the coronal plane), and traumatic spondylolysis. The rates of anterior translation were high in separation fractures (91%), split type fractures (80%), and traumatic spondylolysis fractures (100%). Additionally, 76% of lateral mass fractures showed MRI signal changes of the anterior longitudinal ligament and disc in the caudal segments. 25 Lee et al modified Kotani’s classification by adding two types of facet fractures: articular process fractures with and without dislocations, thereby differentiating them from articular mass fractures. 33
Dvorak et al published a descriptive tomographic classification with three types: A, B, and C. Type A includes isolated facet fractures without dislocation, such as fractures of the superior facet (A1), inferior facet (A2), or floating lateral mass injuries (A3). Types B and C encompass subluxated-dislocated facet fractures, with or without facet injury. 20
The AOSpine subaxial cervical spine injury classification system defines four types of facet fractures, arranged hierarchically by complexity in ascending order from F1 to F4. Type F4 includes the most severe and mechanically unstable injuries, such as subluxated, perched, or dislocated facets. Type F3 includes floating lateral mass fractures. Finally, isolated facet fractures are classified into two types based on the tomographic instability risk factors proposed by Spector et al. These types are characterized by the fragment height exceeding either 1 cm or 40% of the intact contralateral lateral mass. 4
As outlined above, several classifications have been proposed. However, most of the factors that define the various subtypes of facet injuries are based on results from retrospective single-center cohort studies. 34 In our systematic review, we sought to estimate the strength of association between the specific injury subtypes and the likelihood of failure of non-operative management, and to indicate which of these features should be considered in an evidence-based decision-making process.
We found that floating lateral mass injuries are a more severe subtype of isolated facet fracture compared to less complex facet fractures, with a 5.41 times higher risk of failure of non-operative management. This injury is typically classified as a different subtype (F3 in the AO Spine classification, separation fractures in Kotani’s classification, and A3 in Dvorak’s classification). There are moderate concerns regarding the descriptions of injury patterns among the studies included in the meta-analysis.3,16 Therefore, our results support differentiating F3 fractures as a more hierarchically complex injury than F1/F2, and primary surgical treatment should be considered.
The tomographic risk factors included in the AO Spine classification system were summarized based on data from two available studies, which show that reduced fracture height, both absolute and as a percentage, is associated with successful non-operative management. These results support the AO Spine criteria for differentiating F1 from F2 fractures. 4
The presence of irritative radiculopathy was considered a risk factor for failure of non-operative management in patients with non-displaced or minimally displaced facet fractures who did not exhibit neurological symptoms at the time of presentation. 18 However, after conducting a meta-analysis of data from three studies, we found the results to be uncertain.2,17,18 Other predictive factors were reported in isolation. Cirillo et al proposed acute disc injury as a risk factor for failure of non-operative management of isolated subaxial cervical facet fractures. 16 They assessed all patients with cervical facet fractures of subtypes F1 to F3 using CT and MRI, finding that acute disc injury was significantly associated with unsuccessful non-operative management. Nevertheless, magnetic resonance imaging was not routinely performed in most cervical facet injury studies included in our systematic review, making a pooled analysis of this variable unfeasible. Manoso et al mentioned the association between floating lateral mass facet fractures and acute disc injury in 84% (n = 26) of patients evaluated using MRI. Furthermore, Spector et al used MRI for only seven patients (29%), three of whom were subsequently diagnosed with foraminal stenosis due to disc herniation. In a retrospective series, Lifeso et al indirectly noted a significant number of apparent associated disc injuries (n = 8 patients out of 18 receiving non-operative management), which manifested during follow-up as late disc space collapse. 8 Aarabi et al 15 excluded patients with documented acute disc injury, considering this as a sign of instability. 15 Pehler et al. did not routinely perform MRI scans on patients with cervical facet fractures and may have neglected associated acute disc injuries with potential instability. 17
According to Pehler et al, comminution and patient weight greater than 100 kg may be risk factors for failure of non-operative management in F1/F2 fractures. 17 Van Eck et al also found that higher body mass index was a risk factor for failure of non-operative management.17,18 Due to lack of data, a meta-analysis of these variables was not possible.
The recommendations of this systematic review have several limitations due to the very low quality of evidence. This is because all articles included in the review are retrospective, single-center cohorts with a serious risk of bias. The articles did not adequately describe cointerventions such as analgesia, physiotherapy, and activity restrictions, and they also failed to provide information on patient adherence to the intervention. Additionally, many of the articles included the use of hard collars or halo vest immobilization as part of non-operative management. The heterogeneity in the definition of failure of non-operative management made it impossible to summarize the results of some of the included studies.
Nevertheless, evidence-based medicine principles dictate that clinical decisions should be based on the best available evidence and integrated with our experience and patient preferences. The main strength of our study is that it summarizes the best available evidence on risk factors for failure of non-operative management for isolated cervical facet fractures. We believe in the necessity of conducting large multicenter prospective cohort studies to provide higher-quality evidence to guide our clinical decisions on this matter.
Conclusion
The evidence from this review indicates that the morphology of isolated floating lateral mass cervical facet fractures and greater fracture fragment size (measured either in absolute terms or as a percentage) are risk factors associated with failure of non-operative treatment. Other factors identified in the literature were not included in the meta-analysis due to lack of data, including the presence of acute disc injury, high degree of fracture comminution, body weight exceeding 100 kg, and high body mass index. The low certainty of the evidence precludes the formulation of recommendations.
Footnotes
Acknowledgments
This study was organized by the AO Spine Latin America Trauma Study Group. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Spine Latin America regarding data collection, data analysis, and proofreading. The authors would like to thank Idaura Lobo and Carla Ricci (AO Spine) for their administrative assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.