
Abstract
Study Design
Retrospective cohort study.
Objectives
Proximal junctional kyphosis (PJK) is a postoperative complication in spinal deformity surgery causing pain, functional deterioration, and potential revision surgery, with challenges in the neuromuscular scoliosis (NMS) population. We investigated the incidence, risk factors, and clinical impact of PJK in nonambulatory pediatric NMS patients following spinopelvic fusion.
Methods
Seventy-two NMS patients who underwent spinopelvic fusion from the upper thoracic vertebra to the pelvis were reviewed, with a minimum 2-year follow-up. Radiographic measurements and clinical data were analyzed to identify PJK predictors and evaluate outcomes. PJK was defined as a proximal junctional angle (PJA) ≥10° and an increase of ≥10° from preoperative measurements. Statistical analyses included t-tests, ROC curve analysis, logistic regression, and linear regression.
Results
The incidence of PJK was 25%. Significant predictors included rod contour angle (RCA) (odds ratio [OR]: 1.11, P = 0.04), postoperative T2-T12 kyphosis (OR: 1.04, P = 0.043), and the difference between postoperative T2-T12 kyphosis and RCA (OR: 1.04, P = 0.021). A bidirectional relationship between pre- and postoperative PJA was observed. Lower preoperative PJA was associated with an increased risk of PJK (area under the curve [AUC]: 0.78, P < 0.001). Conversely, high preoperative PJA tended to decrease after surgery. No revision surgeries were performed for PJK.
Conclusion
This study reveals a 25% incidence of PJK in NMS patients undergoing spinopelvic fusion. Preoperative radiographic evaluation warrants particular attention in cases exhibiting decreased PJA values. Furthermore, meticulous intraoperative optimization of PJA, RCA, and thoracic kyphosis appears crucial for minimizing PJK occurrence.
Keywords
Introduction
Proximal junctional kyphosis (PJK) is characterized by kyphotic alteration above the upper instrumented vertebra (UIV) in spinal deformity surgery.1,2 It poses significant clinical challenges, with presentations ranging from asymptomatic radiographic changes to pain, functional deficits, and neurological symptoms.3,4
The etiology of PJK is multifactorial. Its prevalence varies with instrumentation type and level, patient population, and diagnostic criteria. 2 Neuromuscular scoliosis (NMS) patients frequently sustain scoliosis, pelvic obliquity, and hip deformity. 5 Spinopelvic fusion is recommended to maintain sitting balance, prevent respiratory complications, and improve the quality of life.6,7 Long fusion levels and pelvic fixation are known risk factors for PJK.1,8 Patients with NMS exhibit an elevated risk for PJK due to concurrent osteoporosis, muscle weakness, and neck control issues. 9 Despite this increased risk, research on PJK in NMS populations remains comparatively scarce, suggesting a significant knowledge gap.2,10,11
This study investigated PJK in nonambulatory pediatric NMS patients following spinopelvic fusion. Our objectives are to determine the incidence, identify potential risk factors, and evaluate the clinical impact of PJK in this cohort. We aim to develop better strategies to prevent PJK and improve long-term outcomes for these high-risk patients.
Materials and Methods
Study Participants and Surgical Procedures
Following institutional review board approval, we retrospectively reviewed NMS patients who underwent spinal deformity surgery between January 2013 and December 2022. The inclusion criteria included (1) diagnosis of NMS; (2) age at surgery under 18 years old; (3) posterior instrumented fusion from the thoracic vertebra (T1-T4) to the pelvis; and (4) a minimum 2-year follow-up. Exclusion criteria comprised incomplete medical and radiographic data.
At our institution, spinopelvic fusion is specifically indicated for nonambulatory NMS patients. The surgical procedure included posterior spinal fusion from the upper thoracic to the pelvis. We used sacral-alar-iliac screws for spinopelvic fusion. 12 Demographic data, intraoperative reports, and medical records were collected through the electronic health medical record (Epic Systems Corporation).
Radiographic Measurement
Radiographic assessments were conducted preoperatively, postoperatively, and at final follow-up. Major curve size, T2-T12 kyphosis, T5-T12 kyphosis, and T12-S1 lordosis were evaluated using the Cobb method. The Osebold method measured pelvic obliquity (PO).
13
We also measured the sacral slope (SS), pelvic tilt (PT), pelvic incidence (PI), and sagittal vertical axis (SVA) as previously described.14-16 Rod contour angle (RCA) was measured as the Cobb angle between the UIV and one vertebra caudal to the UIV (UIV-1) Figure 1.
17
Proximal Junctional Angle (PJA) and Rod Contour Angle (RCA) Measurements in Neuromuscular Scoliosis (A) Preoperative and (B) postoperative radiographs of a cerebral palsy patient with scoliosis after spinopelvic fusion. PJA is measured between the lower endplate of the upper instrumented vertebra (UIV) and the upper endplate of UIV+2. RCA is the Cobb angle between UIV and UIV-1.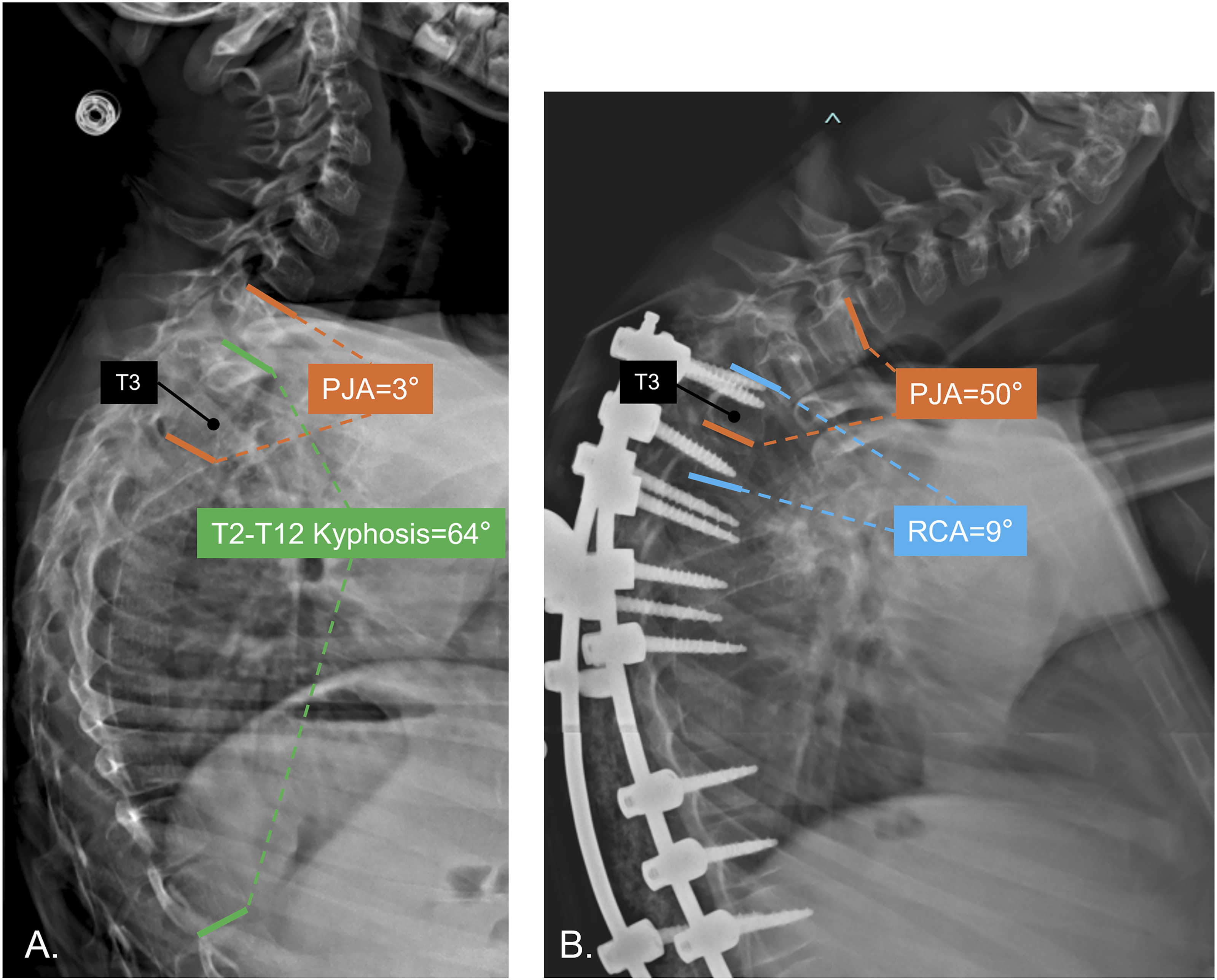
The proximal junctional angle (PJA) was defined as the angle between the lower endplate of the UIV and the upper endplate two levels above the UIV (UIV+2). 16 PJK was defined as a PJA ≥10° and an increase of ≥10° compared to the preoperative measurement.10,16
Statistical Analysis
We analyzed data using IBM SPSS Statistics (Version 25, SPSS Inc., USA) and R (version 4.3.2; R Core Team (2023), Austria). Categorical variables were analyzed using Chi-square or Fisher’s exact tests. Paired t-tests evaluated differences in paired continuous measures, while independent t-tests determined pairwise group differences when appropriate. Receiver operating characteristic (ROC) curve analysis evaluated the accuracy of factors predicting PJK after spine surgery. The optimal cutoff point was established by calculating the maximum Youden index. Logistic regression analysis examined the association between risk factors and PJK. The logistic regression table provided odds ratios and 95% confidence intervals. Linear regression analysis examined the relationship between postoperative T2-T12 kyphosis and reciprocal changes in RCA. The linear regression model results were presented via the ANOVA table and the reported slope estimate. A P-value less than 0.05 was considered statistically significant.
Results
Demographic Result and Patient Characteristics.
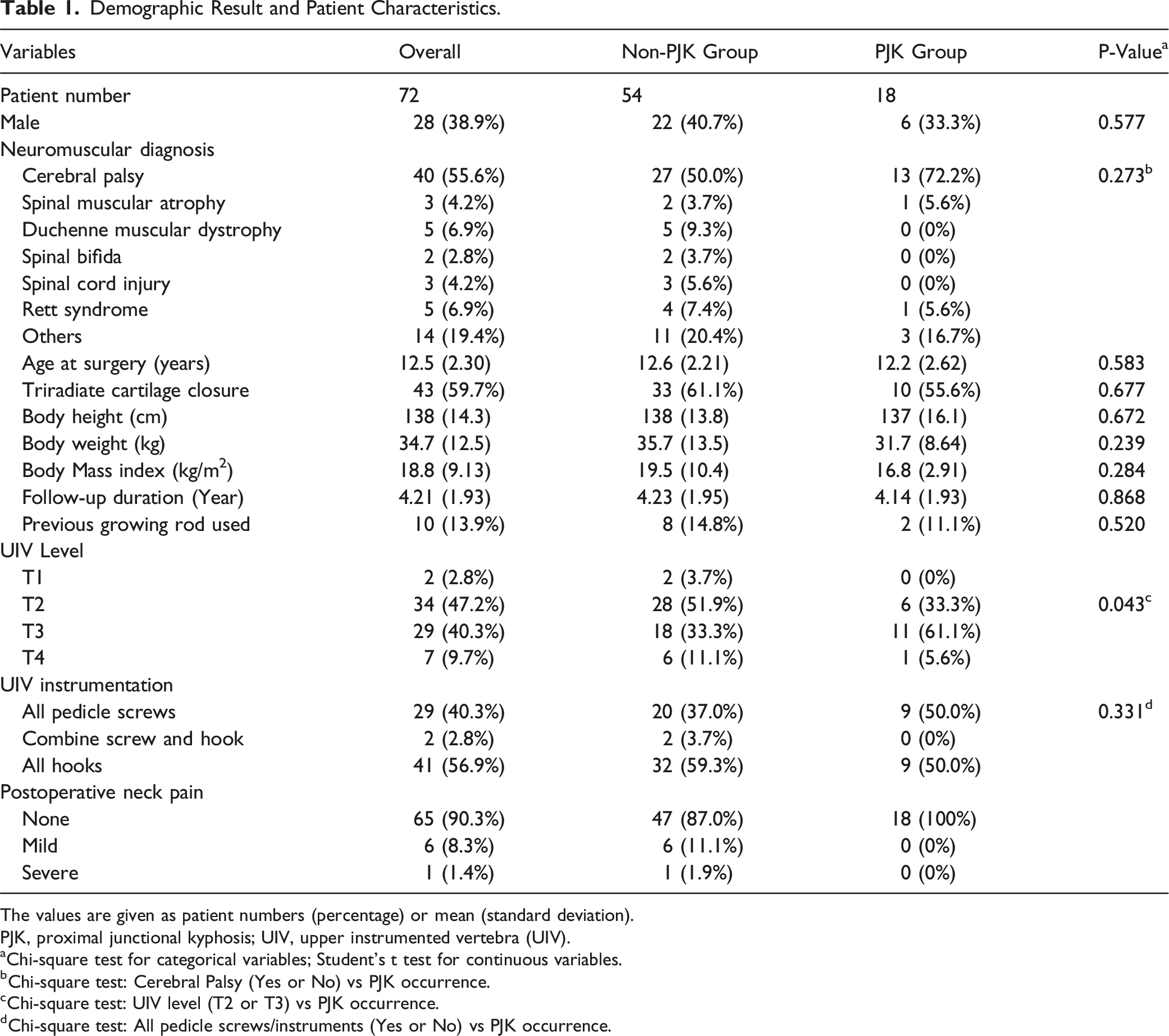
The values are given as patient numbers (percentage) or mean (standard deviation).
PJK, proximal junctional kyphosis; UIV, upper instrumented vertebra (UIV).
aChi-square test for categorical variables; Student's t test for continuous variables.
bChi-square test: Cerebral Palsy (Yes or No) vs PJK occurrence.
cChi-square test: UIV level (T2 or T3) vs PJK occurrence.
dChi-square test: All pedicle screws/instruments (Yes or No) vs PJK occurrence.
Result of Radiographic Measurement before and Initial after Surgery.
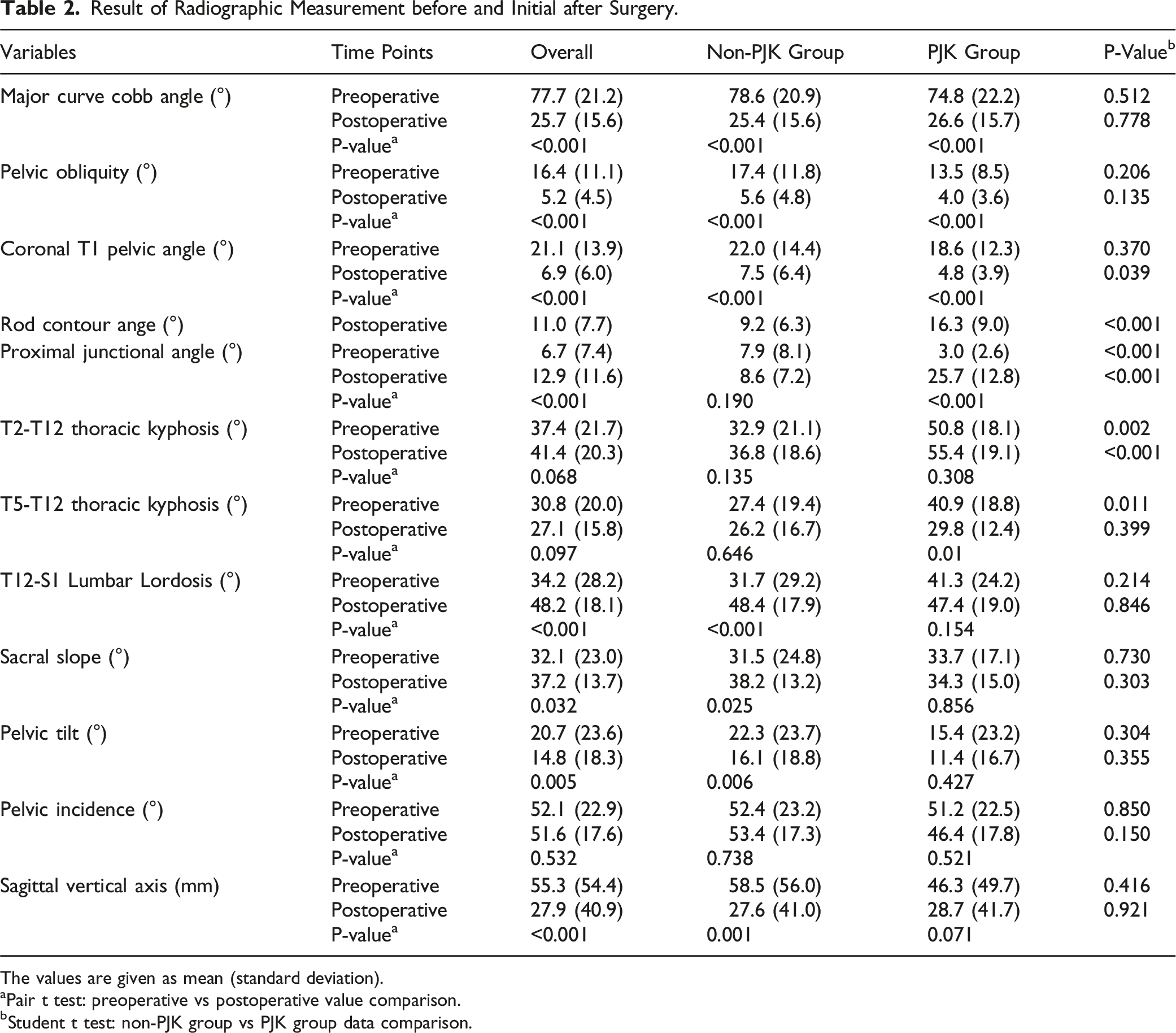
The values are given as mean (standard deviation).
aPair t test: preoperative vs postoperative value comparison.
bStudent t test: non-PJK group vs PJK group data comparison.
Result of Radiographic Measurement at Final Follow-Up.
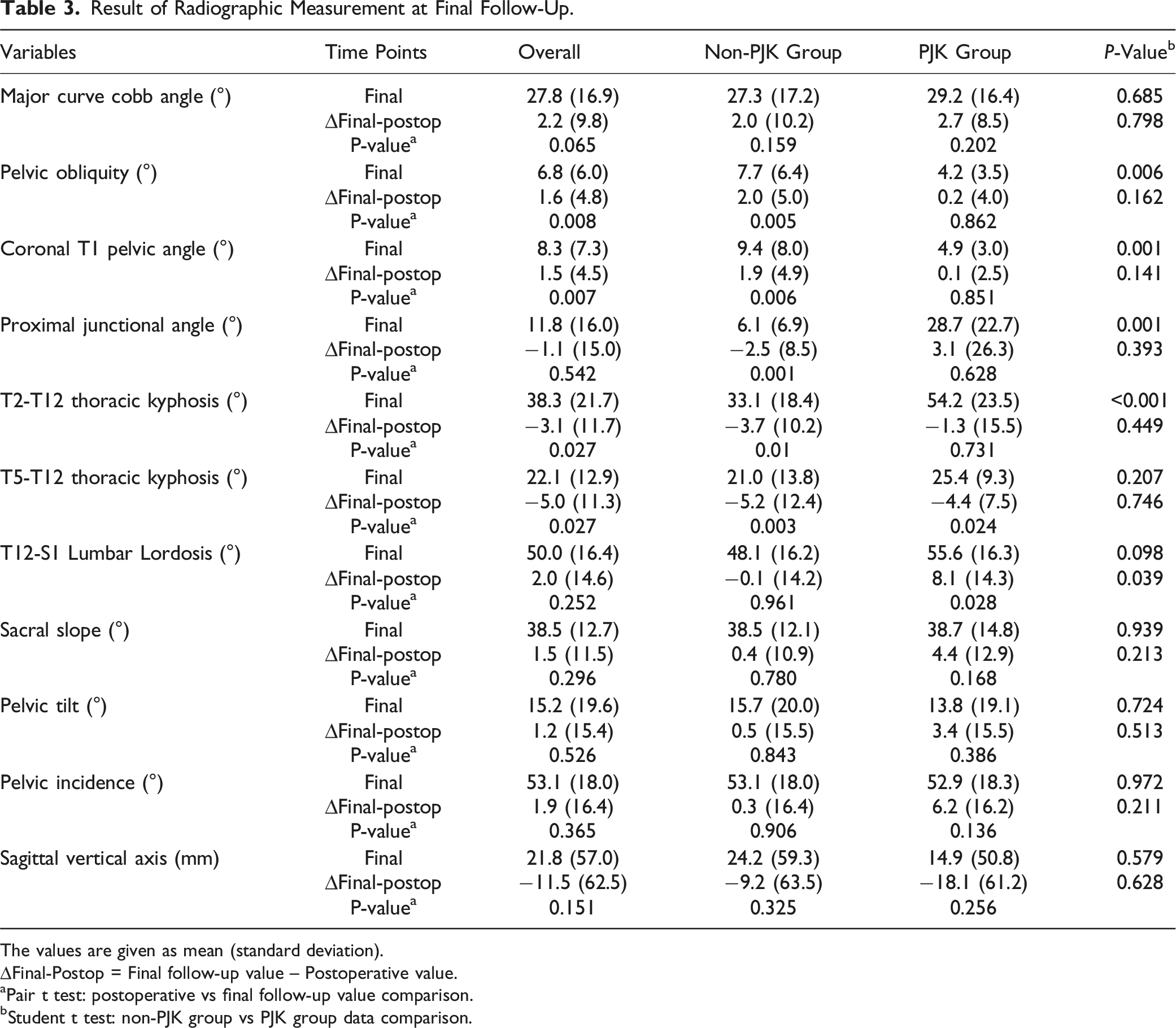
The values are given as mean (standard deviation).
∆Final-Postop = Final follow-up value – Postoperative value.
aPair t test: postoperative vs final follow-up value comparison.
bStudent t test: non-PJK group vs PJK group data comparison.
Logistic Regression Analysis for Predicting Proximal Junctional Kyphosis at Final Follow-Up.
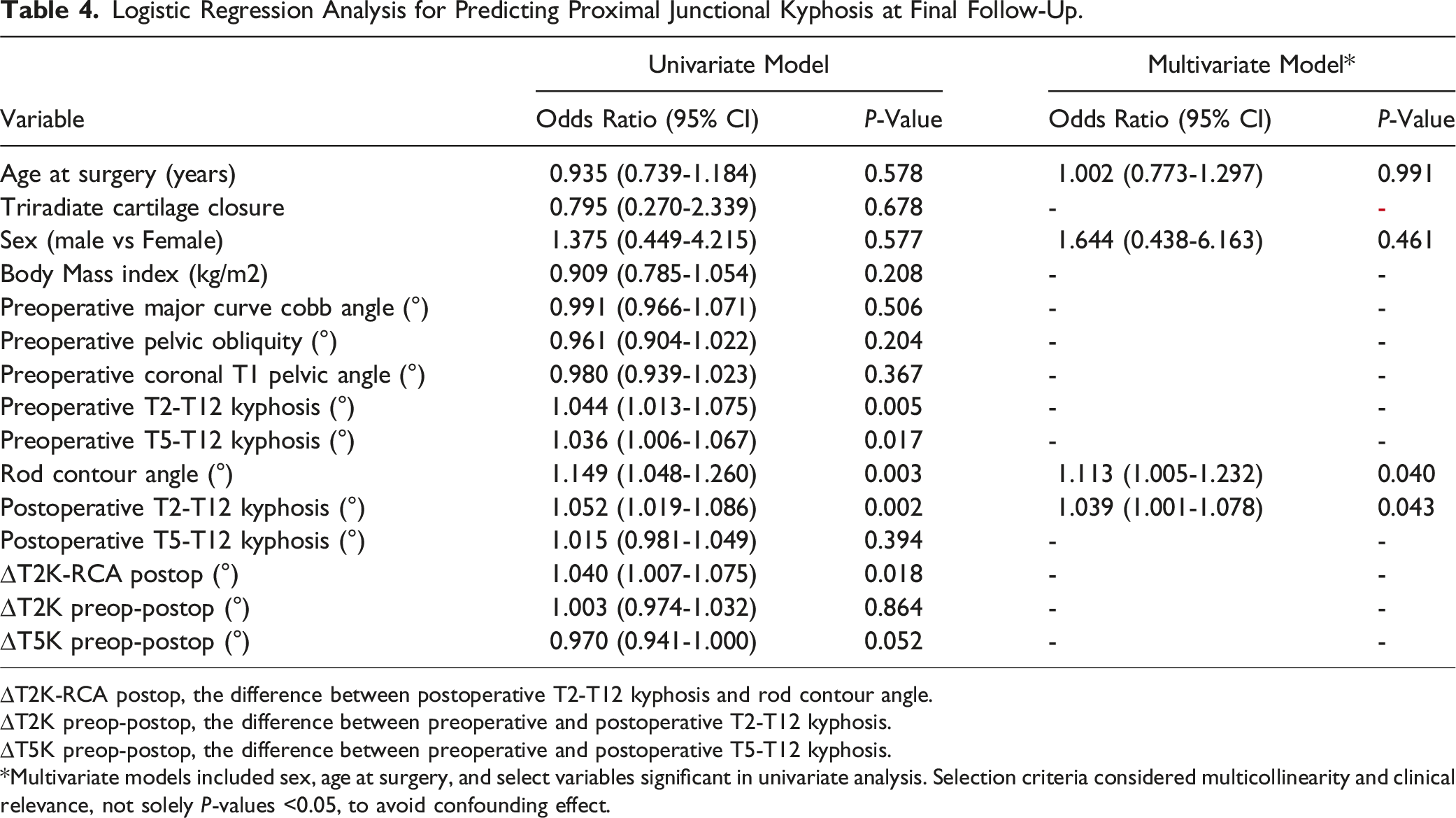
∆T2K-RCA postop, the difference between postoperative T2-T12 kyphosis and rod contour angle.
∆T2K preop-postop, the difference between preoperative and postoperative T2-T12 kyphosis.
∆T5K preop-postop, the difference between preoperative and postoperative T5-T12 kyphosis.
*Multivariate models included sex, age at surgery, and select variables significant in univariate analysis. Selection criteria considered multicollinearity and clinical relevance, not solely P-values <0.05, to avoid confounding effect.
ROC Curve Analysis of Predicting Proximal Junctional Kyphosis at Final Follow-Up.
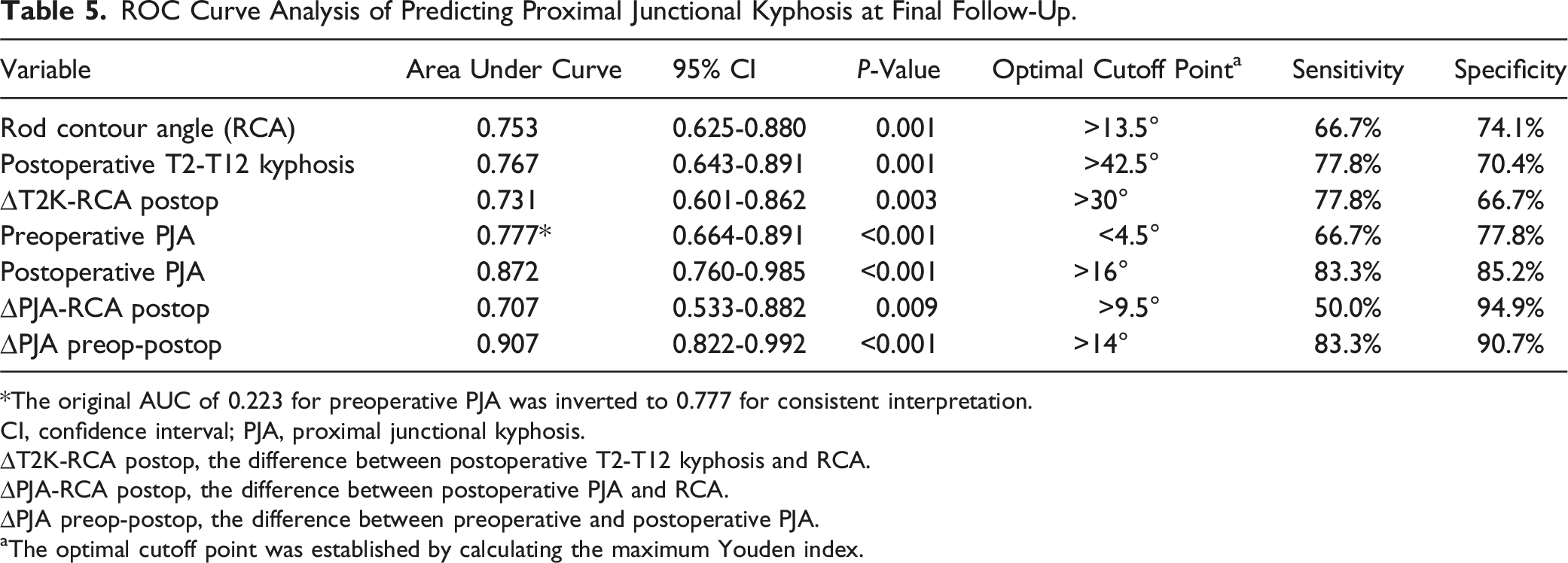
*The original AUC of 0.223 for preoperative PJA was inverted to 0.777 for consistent interpretation.
CI, confidence interval; PJA, proximal junctional kyphosis.
∆T2K-RCA postop, the difference between postoperative T2-T12 kyphosis and RCA.
∆PJA-RCA postop, the difference between postoperative PJA and RCA.
∆PJA preop-postop, the difference between preoperative and postoperative PJA.
aThe optimal cutoff point was established by calculating the maximum Youden index.
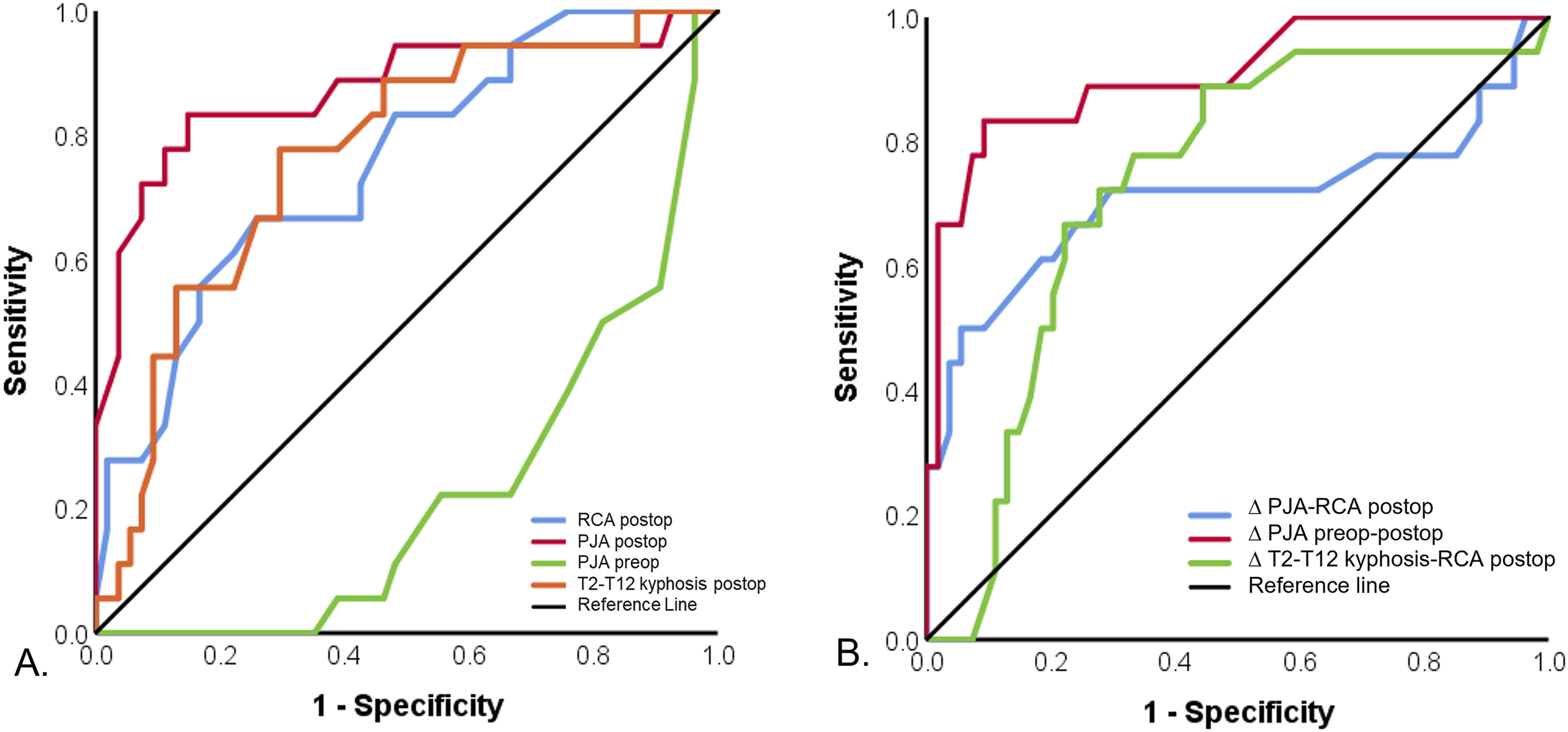
ROC Curve Analysis of Radiographic Parameters for Assessing Proximal Junctional Kyphosis (PJK) (A) Comparison of individual radiographic parameters, including rod contouring angle (RCA), postoperative proximal junctional angle (PJA postop), preoperative PJA (PJA preop), postoperative T2-T12 kyphosis (T2-T12 kyphosis postop). (B) Comparison of derived radiographic parameters, including the difference between postoperative PJA and RCA (∆PJA-RCA postop), preoperative and postoperative PJA (∆PJA preop-postop), and between postoperative T2-T12 kyphosis and RCA (∆T2K-RCA postop).
Scatter plots illustrated the distinct patterns between PJK-positive and PJK-negative cases. Reference lines indicated potential thresholds for each parameter, as determined by ROC curve analysis (Table 5). Our findings revealed a bidirectional impact of surgery on PJA. (Figure 3) While surgery generally decreased PJA in patients with higher preoperative measurements, patients with lower preoperative PJA, specifically those with values <4.5°, experienced a marked increase postoperatively. Patients with preoperative PJA <4.5° exhibited significantly higher rates of PJK (P = 0.001), greater postoperative T2-T12 kyphosis (P = 0.04), and increased T2-T12 kyphosis (∆T2K preop-postop, P = 0.04) after surgery. (Table 6) Relationship between Preoperative (Preop) and Postoperative (Postop) Proximal Junctional Angle (PJA). This scatter plot illustrates preoperative (preop) vs postoperative (postop) PJA for PJK-negative (blue) and PJK-positive (red) cases. The horizontal dashed line at 4.5° represents the significant preop PJA cutoff point determined by ROC curve analysis. The light blue shaded ellipse encompasses patients with large preop PJA who experienced effective PJA reduction after surgery and did not develop PJK at the final follow-up. Conversely, the light red shaded ellipse includes patients with low preop PJA who developed PJK at the final follow-up. Kyphosis Measurements in Patients With Different Preoperative PJA. *Fisher’s exact test for categorical variables; Student's t test for continuous variables. PJA, Proximal junctional angle. ∆T2K preop-postop, difference between preoperative and postoperative T2-T12 kyphosis.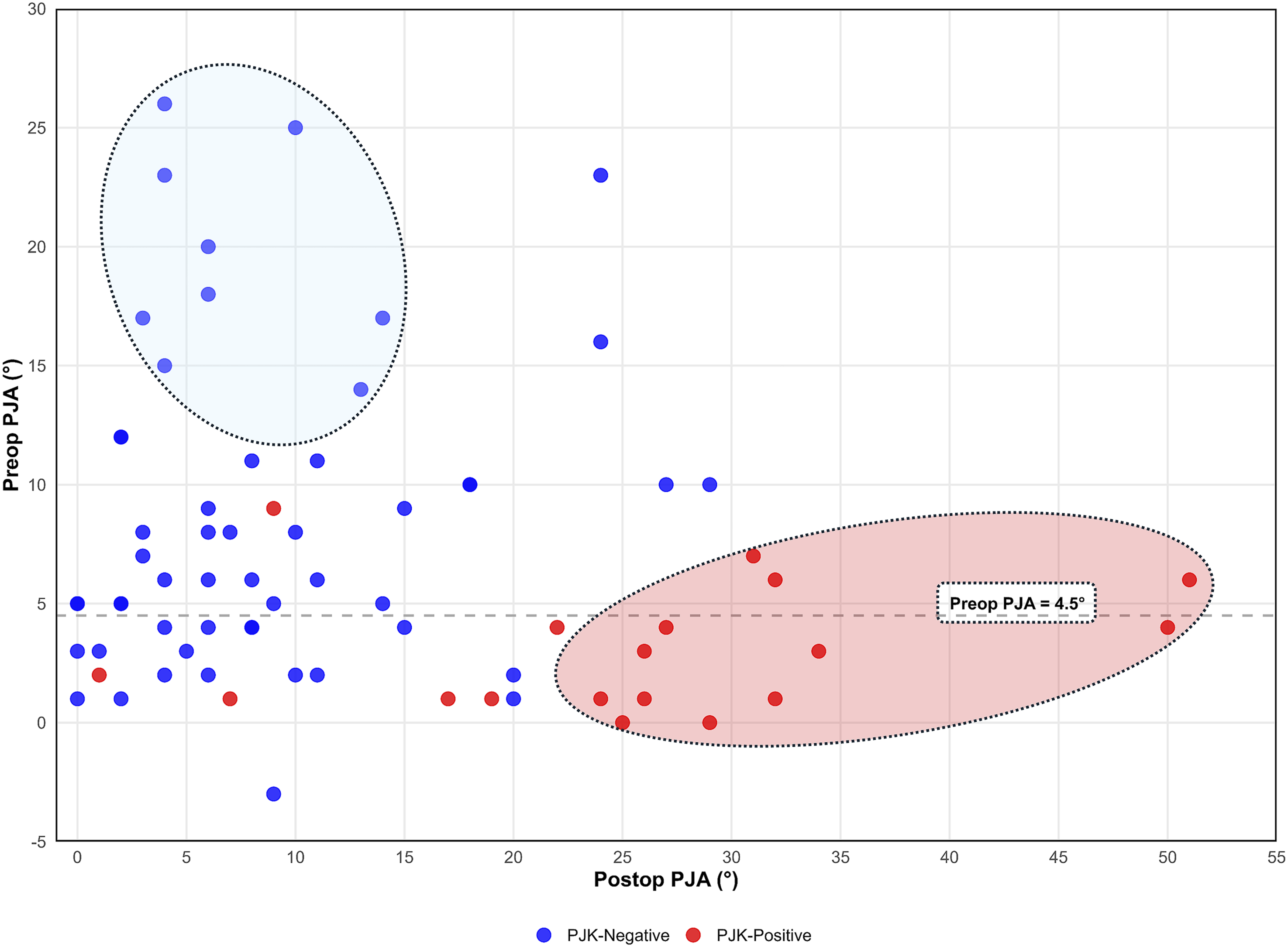
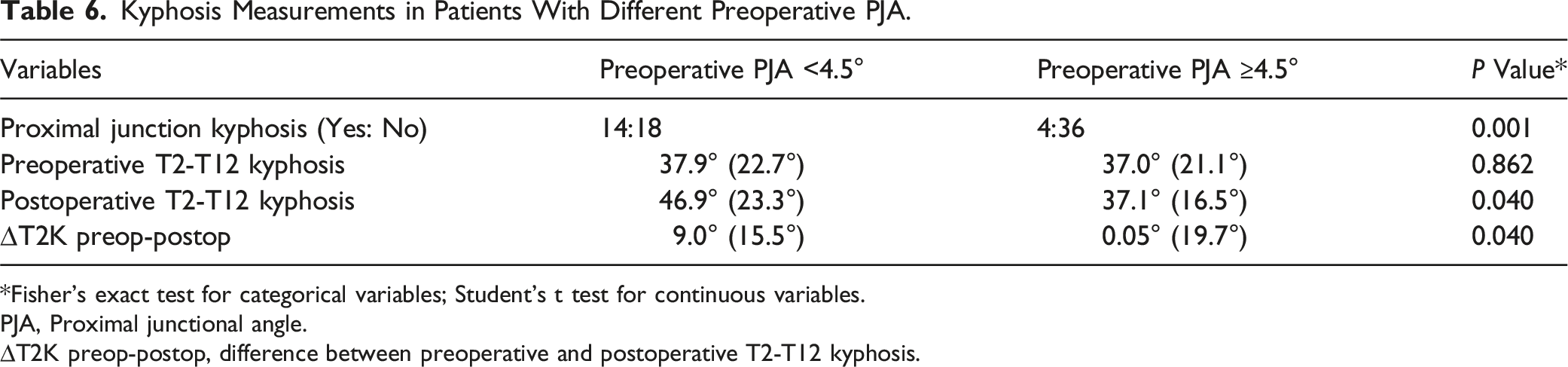
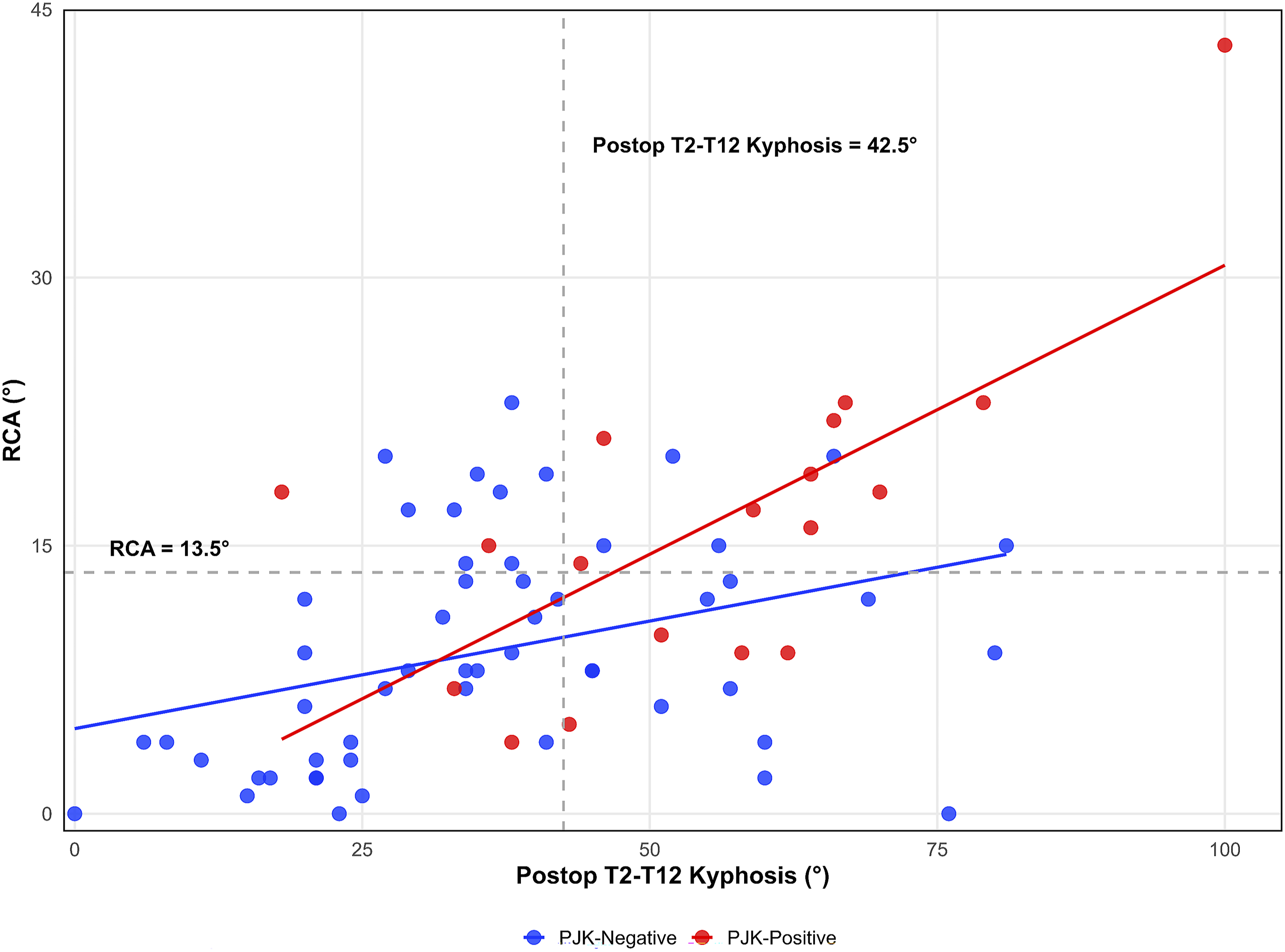
Figure 4 illustrated the association between RCA and postoperative PJA. The pink shaded area (∆PJA-RCA <9.5°) predominantly contains PJK-positive cases, with 75% (9/12) falling within this region. Cases with postoperative PJA ≥30° were all PJK-positive. Figure 5 showed the association between RCA and postoperative T2-T12 kyphosis. Most PJK-negative cases had RCA <13.5° and postoperative T2-T12 kyphosis <42.5°, possibly suggesting these thresholds may predict PJK. Relationship between Rod Contour Angle (RCA) and Postoperative Proximal Junctional Angle (Postop PJA) This scatter plot revealed the relationship between RCA and postop PJA for proximal junctional kyphosis (PJK)-negative (blue) and PJK-positive (red) cases. The pink shaded area indicates where the difference between postop PJA and RCA (ΔPJA-RCA postop) >9.5° was the significant cutoff point from our ROC curve analysis. The vertical dashed line at 16° represents the significant postoperative (postop) PJA cutoff point determined by ROC curve analysis. Relationship between Rod Contour Angle (RCA) and Postoperative T2-T12 Kyphosis (Postop T2-T12 Kyphosis) This scatter plot revealed the relationship between RCA and postop T2-T12 kyphosis for proximal junctional kyphosis (PJK)-negative (blue) and PJK-positive (red) cases. Linear trend lines are shown for each group. Linear regression analysis revealed a significant interaction between RCA and postop T2-T12 kyphosis in the PJK-positive group (red line, P = 0.028). Dashed lines indicate ROC-derived critical values: RCA (13.5°, horizontal) and postoperative T2-T12 kyphosis (42.5°, vertical).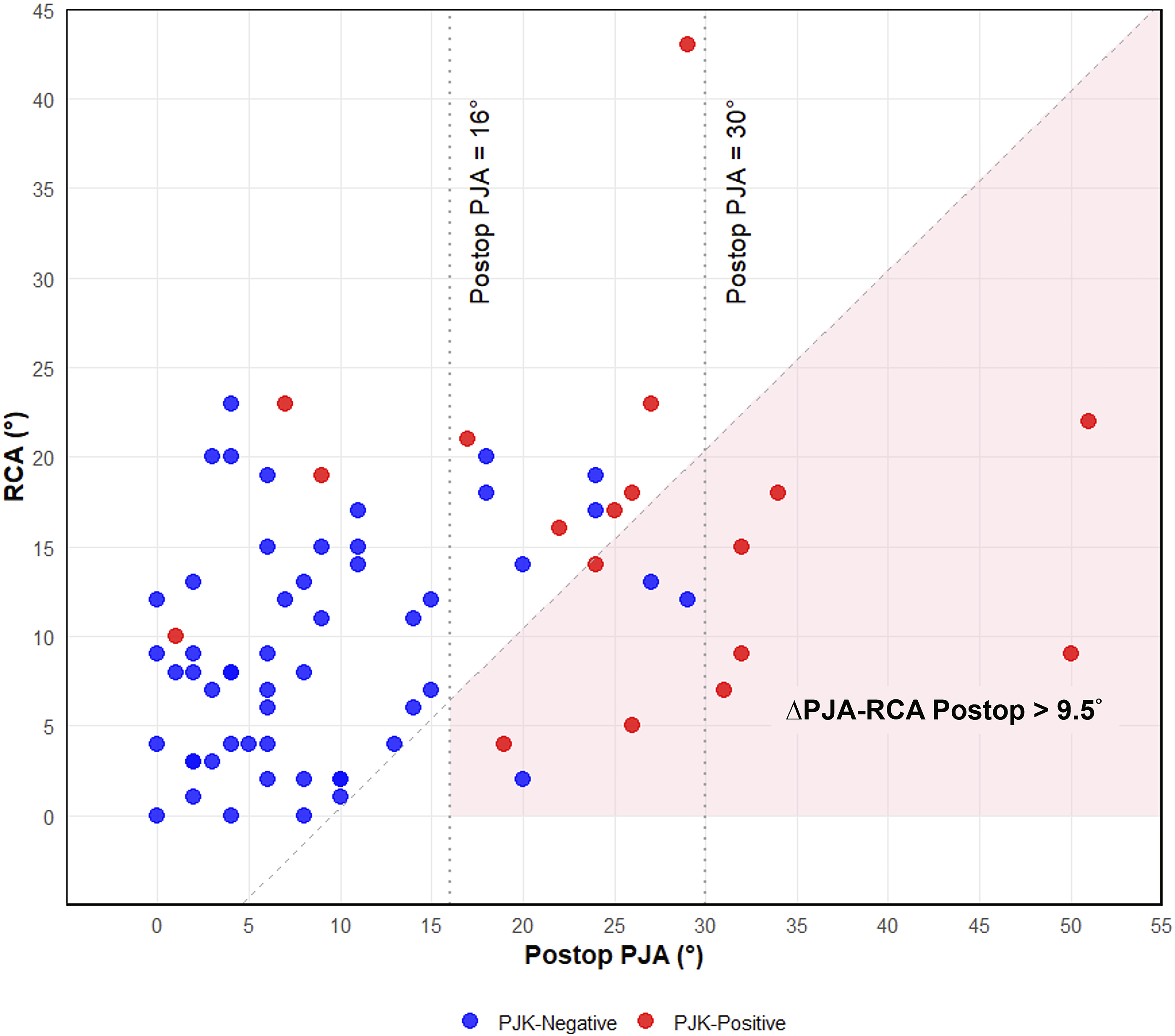
ANOVA Table: Factors Affecting Rod Contour Angle (RCA).
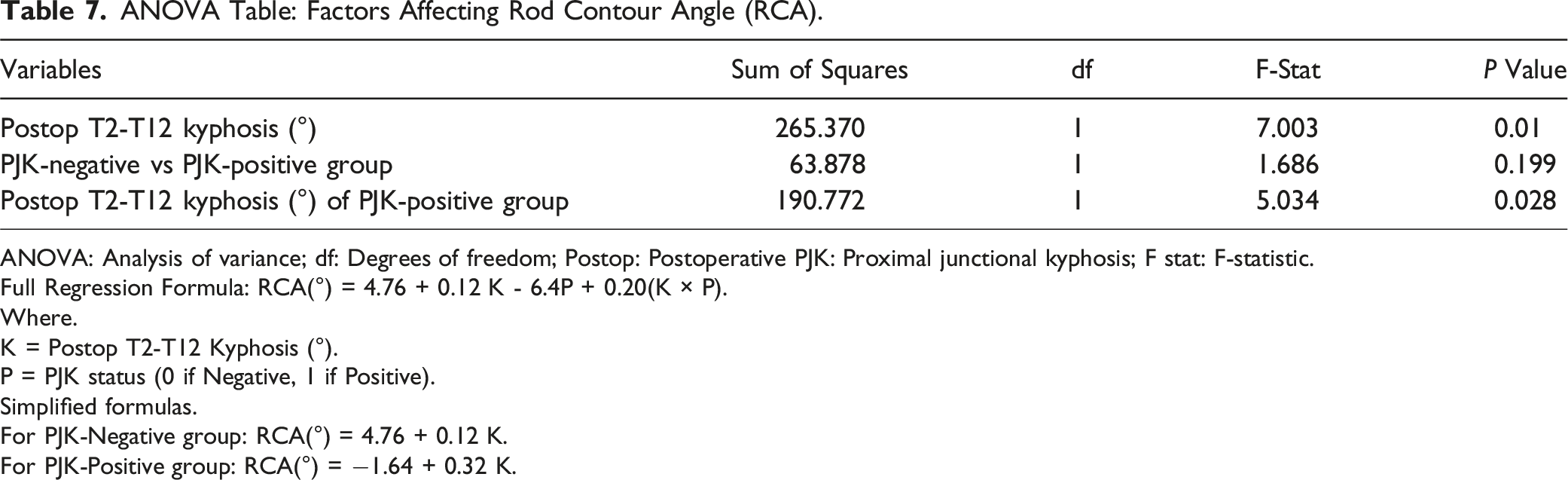
ANOVA: Analysis of variance; df: Degrees of freedom; Postop: Postoperative PJK: Proximal junctional kyphosis; F stat: F-statistic.
Full Regression Formula: RCA(°) = 4.76 + 0.12 K - 6.4P + 0.20(K × P).
Where.
K = Postop T2-T12 Kyphosis (°).
P = PJK status (0 if Negative, 1 if Positive).
Simplified formulas.
For PJK-Negative group: RCA(°) = 4.76 + 0.12 K.
For PJK-Positive group: RCA(°) = −1.64 + 0.32 K.
Discussion
Our study found that 25% of NMS patients developed PJK following spinopelvic fusion. We observed a bidirectional relationship between pre- and postoperative PJA relationships. Surgery generally decreased PJA in patients with higher preoperative values. However, many PJK patients had preoperative PJA <4.5°. Significant predictors of PJK included RCA, postoperative T2-T12 kyphosis, and ∆T2K-RCA postop. The complex interplay between these parameters offers potential targets for preventing PJK in NMS surgical planning.
Toll et al. reported a 27% incidence of PJK in NMS using the definition of PJK as a >10° increase. 2 Despite variations in PJK definition, neuromuscular condition distribution, ambulatory status, and pelvic fixation rates, we observed a similar PJK prevalence. Our findings corroborate their observation regarding the PJK incidence and risk factors for PJK, including lower preoperative PJA and increased lumbar lordosis at the final follow-up in the PJK group. Figure 3 demonstrated that patients with higher preoperative PJA typically experienced reduction post-surgery, while those with PJK often presented with preoperative PJA <4.5°. We propose three potential explanations for the association between lower preoperative PJA and increased PJK risk. First, a lower initial PJA could more easily reach the 10° increase criterion for PJK diagnosis. Second, our patients with preoperative PJA <4.5°exhibited significantly higher postoperative T2-T12 kyphosis and greater kyphosis increases. (Table 6) They simultaneously presented two conditions associated with PJK risk. The interplay between these factors warrants further study. Third, poor cervical muscle control might cause unintended neck hyperextension during radiographic positioning, resulting in artificially lower preoperative PJA measurements. The increased lumbar lordosis observed in the PJK group was consistent with Toll et al's findings. The underlying mechanisms for this phenomenon remain unclear, but we hypothesize that it may indicate compromised bone quality, potentially affecting screw fixation. Further studies are needed to elucidate these factors in PJK etiology.
Larger postoperative PJA is a significant risk factor for PJK in adolescent idiopathic scoliosis (AIS) and adult spinal deformity (ASD) surgery.18-20 Sakuma et al. reported that postoperative PJA >15.5° and changes in postoperative PJA >14.5° predicted PJK in ASD surgery. 21 Our findings corroborate these results, with significantly higher PJK risk in patients with postoperative PJA >16°. (Table 5) While some patients’ PJA decreased at final follow-up, this was uncommon in those with postoperative PJA >16°. (Table 3) Given the increased risk when postoperative PJA exceeds 16°, intraoperative strategies to mitigate PJK risk are crucial. Beyond extending fusion levels, our findings suggest adjusting parameters like RCA and postoperative thoracic kyphosis may reduce risk, especially with high PJA values.
RCA and its relationship with postoperative PJA are significant predictors of PJK across various patient populations.17,19,20,22-25 Previous studies found that ∆PJA-RCA post >5° predicted PJK in AIS and early-onset scoliosis (EOS)20, 26. We observed that RCA >13.5° and ∆PJA-RCA postop >9.5
Our findings did not indicate that the preoperative and postoperative thoracic kyphosis change was a significant PJK predictive factor as previous literature described.19,24,26,27 Instead, we observed that postoperative thoracic kyphosis and ∆T2K-RCA postop were associated with PJK. Figure 5 demonstrates the interaction between RCA and postoperative T2-T12 kyphosis in predicting PJK. Non-PJK patients predominantly clustered in the lower left quadrant (RCA <13.5
Spinopelvic fusion and long-level fusion are known as PJK risk factors.17,28 In our study, while the absence of a control group precluded direct comparisons, we observed that the PJK rate falls between EOS and AIS, two distinct pediatric spinal deformities.18,26,29,30 Notably, no revision surgery was performed, possibly due to reduced functional demands, complex comorbidities, and wheelchair adjustments compensating for PJK deformities. However, this should not diminish PJK’s significance in NMS. Prevention remains crucial to avoid additional surgeries. Considering these patients’ unique clinical characteristics and functional requirements, reevaluating the PJK definition for this population may be necessary.
Our investigation of risk factors was informed by both AIS and ASD literature, as these populations share important characteristics with our NMS cohort. While AIS patients are similar in age to our population, ASD patients often share compromised bone quality issues. Regarding instrumentation, while transverse process hooks at UIV have been associated with decreased PJK risk in AIS, we found no significant differences between pedicle screws and hooks in our NMS cohort (P = 0.331). 31 This warrants careful interpretation due to selection bias in our surgical approach, where pedicle screws were preferentially used when anatomically feasible. While other fixation techniques such as transitional rods, hybrid constructs, and sublaminar bands have shown promise but were not evaluated in our cohort, their effectiveness in NMS patients requires further investigation due to several patient-specific factors.32,33 Age-related effects differed from AIS literature, where younger age is a known risk factor for PJK development. In our NMS cohort, neither age nor skeletal maturity (triradiate cartilage closure) showed significant association with PJK development (P = 0.583 and P = 0.746, respectively). Additionally, disease-specific growth patterns in our heterogeneous cohort may have confounded our ability to detect age-related effects on PJK development, as these conditions can have markedly different impacts on skeletal growth and maturation.
Osteoporosis, a well-established risk factor in ASD, that warrants further investigation in NMS patients. We did not routinely perform DXA scans for patients without fracture history, as there is no consensus on bone quality assessment protocols in NMS patients undergoing spinal surgery. 34 Future prospective studies are needed to elucidate the unique considerations in NMS patients. These should systematically assess bone quality, spasticity levels, and detailed postoperative protocols - factors that may significantly influence surgical outcomes in this population.
Our study had several limitations. (1) The generalizability may be limited as a single-center retrospective study. (2) Our radiographic analysis was confined to preoperative, initial postoperative, and final follow-up. Intraoperative and longitudinal postoperative assessments were lacking. Comprehensive temporal evaluations could provide critical insights into PJK’s dynamic progression and improve surgical decision-making. (3) We did not assess patients’ spasticity or motor control capabilities of the head, neck, and upper extremities—crucial neuromuscular parameters influencing postoperative functional outcomes. (4) Some patients were excluded due to inadequate imaging quality in the cervicothoracic junction region, attributed to poor bone quality, positioning difficulties during radiographic examination, and severe spinal deformities. Advanced imaging techniques and patient-specific protocols are essential to improve future investigations' reliability. Despite these limitations, our strengths include a relatively large sample size for NMS, extended follow-up duration, and a homogenous patient cohort with similar surgical procedures and fusion levels.
This study reveals a 25% incidence of PJK in NMS patients undergoing spinopelvic fusion, highlighting the need for effective preventive strategies. Our findings highlight the importance of careful preoperative assessment, particularly for patients with lower preoperative PJA values. Intraoperative optimization of PJA, RCA, and thoracic kyphosis emerged as key factors in mitigating PJK risk. The complex interplay between these parameters necessitates further research to refine surgical goals, ultimately reducing PJK incidence and enhancing outcomes in this vulnerable population.
Footnotes
Author Contributions
PCS: Writing – original draft, Investigation, Data curation, Conceptualization. CK: Statistical analysis, Visualization, Software. TS: Project administration, Conceptualization. NHM: Supervision, Conceptualization. MAE: Supervision, Conceptualization. Review and editing
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.