
Abstract
Study Design
Cross-sectional study.
Objectives
To assess global practices and preferences in the use of osteobiologics for anterior cervical discectomy and fusion (ACDF) and identify factors influencing the choice of specific osteobiologics.
Methods
An online survey developed by AO Spine was distributed to spine surgeons worldwide. The survey captured demographic characteristics, osteobiologic use and related information (i.e., previous training, practice patterns, etc.), and factors influencing osteobiologic choice in ACDF. Descriptive statistics, Chi-square tests, and multiple logistic regression were used to analyze responses, focusing on the associations between osteobiologic use and variables such as training, cost awareness, and regional practices.
Results
Responses from 458 surgeons revealed regional variability in osteobiologic preferences. Autologous iliac crest bone graft (AICBG) was predominant in Asia Pacific and Middle East, while allograft and demineralized bone matrix were favored in North America and Latin America (P < 0.0001). Over half of the respondents (79.7%) lacked formal training in osteobiologics, and 53.1% were unaware of related costs. Surgeons residing in the Asia Pacific region (OR: 0.47, 95% CI: 0.26-0.84, P = 0.0114), without formal training (OR: 0.53, 95% CI: 0.29-0.97, P = 0.0429), or using cages less often (OR: 0.15, 95% CI: 0.06-0.34, P < 0.0001) were less likely to utilize osteobiologics. Osteobiologic use was also more common when related costs were not an issue for the practitioner (OR: 2.32, 95% CI:1.47-3.70, P = 0.0004).
Conclusions
Significant variation exists in osteobiologic use in ACDF across global regions, influenced by surgeon training, cost awareness, and institutional resources. Enhanced training and guidelines could improve consistency in osteobiologic application.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed spine surgeries worldwide, with a high success rate ranging from 85 to 95%. 1 The primary objectives of ACDF are to relieve pain and restore neurological function, which are achieved through thorough decompression of neural structures. However, long-term success largely depends on achieving solid bony fusion. 2 This can be attained through various combinations of implants (e.g., cages and plates) and osteobiologics.
Osteobiologics are substances that can induce bone formation (osteoinduction), support bone ingrowth (osteoconduction), or directly generate new bone tissue (osteogenesis). 3 Autologous iliac crest bone graft (AICBG) has traditionally been considered the gold standard for achieving fusion due to its ready availability and excellent osteogenic, osteoinductive, and osteoconductive properties. Despite these advantages, AICBG is associated with significant donor site morbidity, including wound complications, persistent pain, infection, and hematoma. 4
The limitations of AICBG have prompted the development of a variety of osteobiologics to augment or replace autografts. These include allografts, bone morphogenetic protein (BMP)-2, demineralized bone matrix (DBM), hydroxyapatite (HA), beta tricalcium phosphate (β-TCP), bioglass, bioceramics, and synthetic peptides. While these materials offer potential advantages, their use is complicated by variability in clinical evidence supporting their efficacy and safety. Indeed, there is a lack of high-quality clinical evidence for the use of osteobiologics, which provides limited information to foster the knowledge and to support their use.5-7 Furthermore, there is ongoing debate whether the use of osteobiologics, either AICBG or other grafts, significantly affects fusion rates in revision ACDF cases, where the risk of pseudoarthrosis is substantially higher. 8 Additionally, regulatory differences across countries, including variations in reimbursement policies and market availability, contribute to inconsistent adoption among spine surgeons.9,10 From a global market perspective, this is particularly relevant since the economic potential of osteobiologics has been estimated >$9 billion in 2024. 11 These disparities highlight a critical need to standardize practices and evaluate the factors influencing clinical decision-making.
Given the limited clinical data available, there is no consensus among spine surgeons regarding the use of appropriate osteobiologics in specific clinical scenarios, whether for single- or multi-level ACDF. AO Spine recently developed an international guideline, the AO Spine Guideline for the Use of Osteobiologics (AOGO), to provide evidence-based recommendations. 12 The aim of the current study is to assess global practice patterns and preferences regarding the use of osteobiologics in ACDF, and to identify the factors influencing the selection of specific osteobiologics. This research addresses a critical gap by exploring how individual surgeon preferences, familiarity, and access to resources drive decision-making. Additionally, it seeks to evaluate whether cost-effectiveness and clinical evidence play a secondary role in the selection process. By elucidating these dynamics, this study aims to inform future research, enhance the applicability of guidelines, and promote consensus among spine surgeons.
Materials and Methods
Study Participants
An online questionnaire assessing the use of osteobiologics in ACDF was formulated by the AO Spine Knowledge Forum Degenerative working group within the AOGO project. AO Spine is a professional medical association of spine surgeons and a clinical division of the AO Foundation. AO Spine is the leading global academic community of spine surgeons dedicated to generating, distributing, and sharing knowledge through research, education and community development. Established in June 2003, the organization is led by the AO Spine International Board. The board guides and supports the AO Spine regions Asia Pacific, Europe and Africa, Latin America, Middle East, and North America. AO Spine fosters a global community of 30,000 members and associates from all over the world. Within the society, the Knowledge Forum Degenerative is one of five expert-driven working groups generating evidence-based knowledge on degenerative disorders of the spine. The survey was developed within the AO Spine Knowledge Forum Degenerative via iterative review cycles among the members of the group which are key opinion leaders in the field in the Degenerative Spine surgery field. No formal institutional review board approval was required for this study. The survey was sent out by email to approximately 6,000 spine surgeons between March 1 and 15, 2024. The link was kept accessible for 15 days with two reminders sent out during the period. All the participants signed a digital informed consent and agreed on the use of their anonymized responses for research purposes.
Study Questionnaire
The survey originally included 23 questions. General participants’ demographics included country and AO Spine region of practice, gender, age, years of practice in spine surgery, specialty, practice setting, information about spine surgery fellowship, number of spine surgery cases performed per year, and number of ACDF surgeries performed per year. Then, information regarding previous formal training in the use of osteobiologics, awareness of osteobiologic costs, use of implants in ACDF surgeries (i.e., cages and plates), frequency of osteobiologic use in ACDF, strategies to reduce complications and improve treatment outcomes, and factors influencing the use of osteobiologics in ACDF. These factors included cost, evidence base, historical practice, availability, education, and vendor support, and were rated by each participant from 1 (“most important”) to 6 (“not important”). The full questionnaire is available as a Supplemental Material.
Statistical Analysis
Categorical data were shown as absolute (n) and relative (%) frequencies. Statistical analysis of data was performed using the Chi-square test. Multiple logistic regression was performed to investigate the associations between the use of osteobiologics, related training, and different instrumentation with AO Spine region, hospital setting, community setting, surgeon’s age, years of surgical practice, overall spine surgery and ACDF case volume, specialty, fellowship, knowledge of osteobiologic costs, existence of institutional cost limitations, and use of local corticosteroids. These covariates were selected based on their statistical significance as per univariate analyses (Supplemental Tables). Answers reporting the use of multiple osteobiologics were removed from the analysis. Reference levels were selected based on their frequency or their relevance per each independent variable. Odds ratios (OR) and 95% confidence intervals (CI) were estimated for each reference category. Statistical significance was set at P < 0.05. Formal analysis was performed using Prism 10 (v. 10.1.1, GraphPad Software).
Results
Participants’ Demographics
A total of 458 surgeons completed the survey. Participants were from North America (12.2%), Latin America (14.4%), Europe & Southern Africa (35.2%), Middle East & North Africa (13.5%), and Asia Pacific (24.7%) regions. The majority of respondents were male (94.6%), aged between 35 and 44 (39.1%), and had been practicing for at least 5 years (79.7%). Among these, 57.6% were orthopaedic surgeons, 40.4% practiced in an academic hospital, 28.4% in a private setting, and 27.5% in a public or government/military hospital; most worked in urban areas (79.7%). The majority had completed a spine surgery fellowship (65.1%): of these, one-third finished their post-graduate training within the last 5 years, one-fourth within the last 5 to 10 years, and the rest more than 10 years ago. Regarding surgical volume, 26.9% performed fewer than 100 spine surgeries per year, 36.2% operated between 100 and 200 cases annually, and the remaining surgeons operated on more than 200 cases per year. Among these, 45.0% performed fewer than 20 yearly ACDFs, 36.7% performed between 20 and 50, and the rest performed over 50 ACDFs annually.
Use of Implants and Osteobiologics during ACDF Surgery
Univariate Analyses Assessing the Relationship Between Osteobiologic-related Training and Study Covariates.
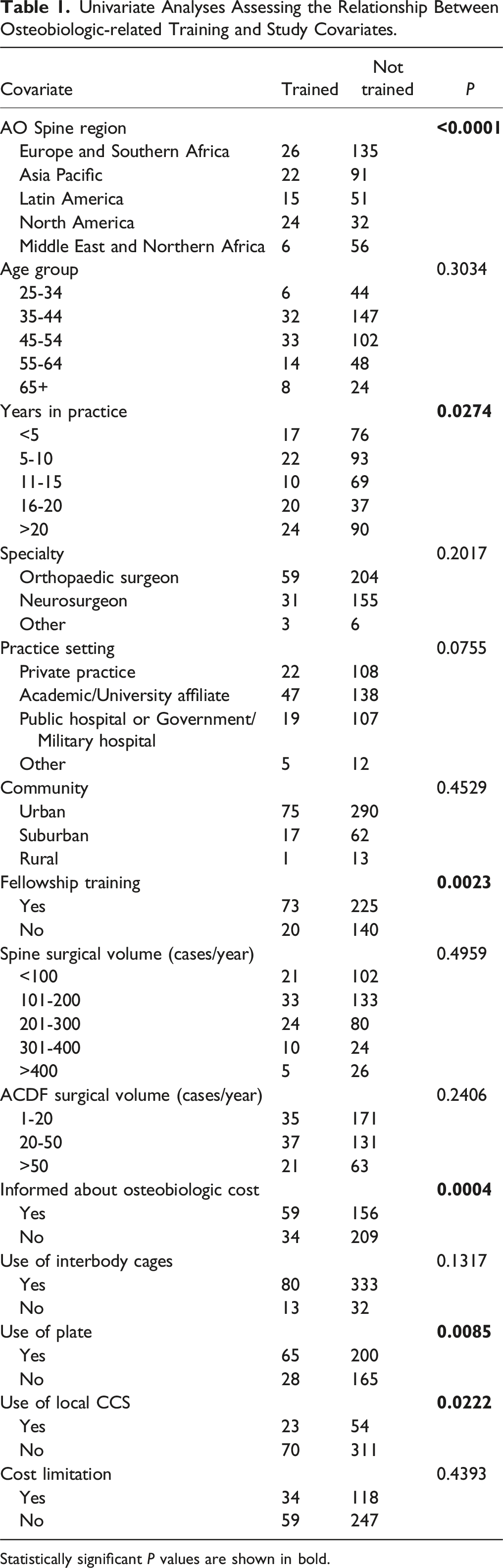
Statistically significant P values are shown in bold.
Univariate Analyses Assessing the Relationship Between the Use of Interbody Cages (>50% of Cases) and Study Covariates.
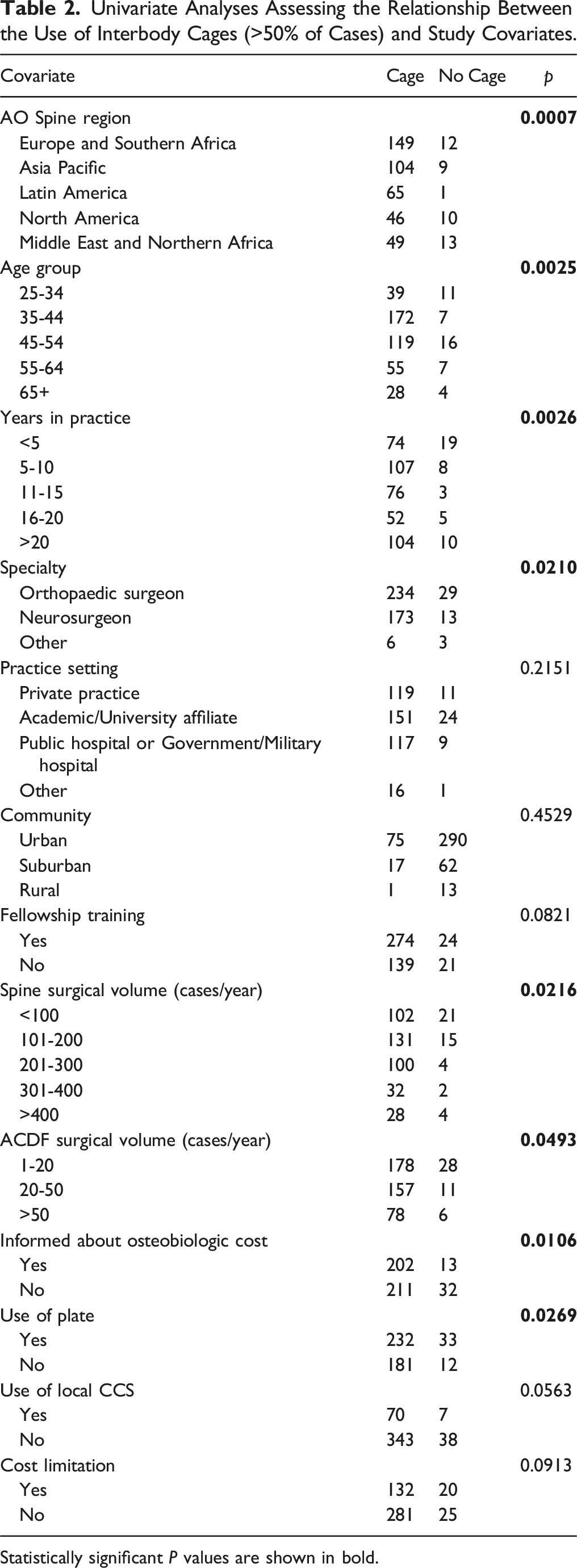
Statistically significant P values are shown in bold.
Univariate Analyses Assessing the Relationship Between the Use of an Anterior Plate (>50% of Cases) and Study Covariates.
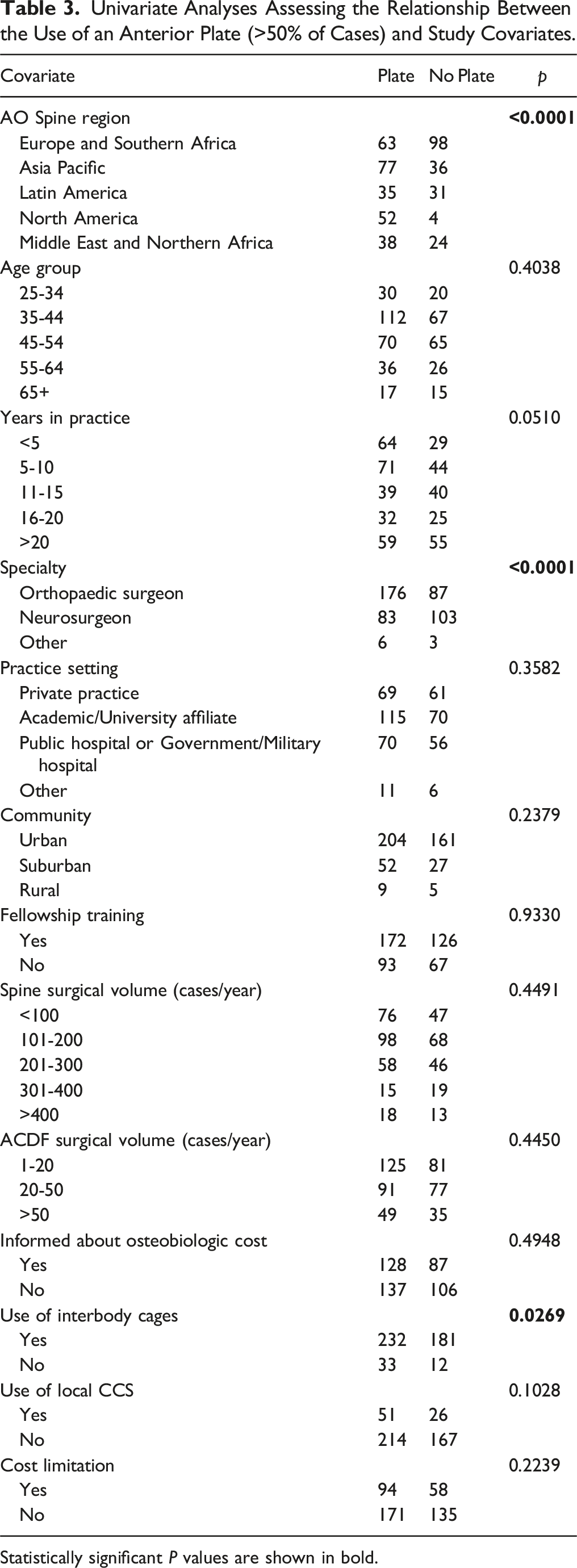
Statistically significant P values are shown in bold.
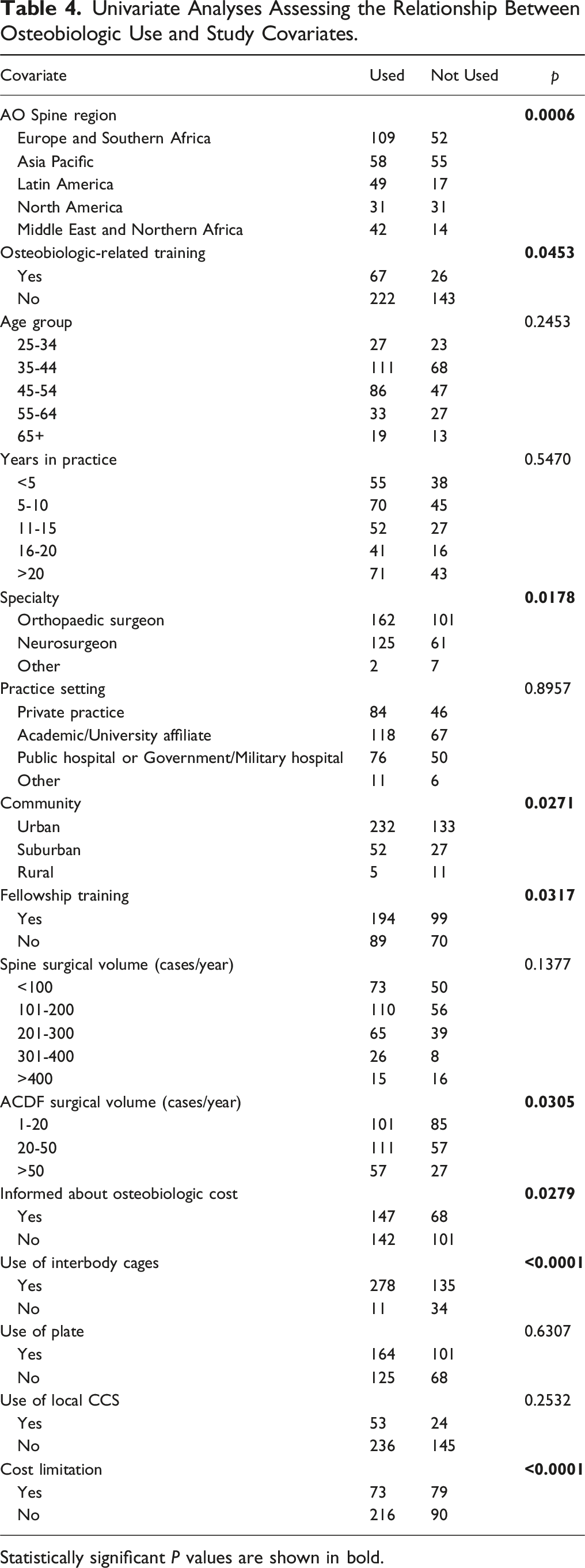
In terms of using osteobiologics as a supplement to autologous local bone, 38.0% of the surgeons always used some form of osteobiologic, 17.3% used them most of the time, 7.9% used them half of the time, while 22.5% and 14.4% used them rarely or never, respectively. As an alternative to autologous local bone graft, 28.0% reported using a tricortical bone graft, 27.3% used DBM, 22.7% used allograft, 12.7% used HA, 9.4% used cancellous AICBG, 7.7% used cellular bone graft, 7.4% used bicalcium phosphate, 6.6% used BMP-2, 1.3% used ABM/P-15 peptide, and a small percentage used other grafts including tibial (0.2%) and fibular grafts (0.2%), unspecified synthetic materials (0.2%), bone marrow aspirate (0.2%), β-TCP (0.2%), collagen matrix (0.2%), bioactive glass (0.8%), or no graft at all (1.0%). When subgrouping the three most common osteobiologics by regions, AICBG was the most popular in Asia Pacific (58.5%) and Middle East and Northern Africa (45.3%), allograft was primarily employed in Latin America (35.8%) and North America (33.3%), and DBM was mostly used in North America (39.6%) and Europe and Southern Africa (20.3%). All these differences were statistically significant (P < 0.0001; Figure 1). The use of osteobiologics (Table 4) showed statistically significant differences when considering geographical distribution (P = 0.0006), osteobiologic-related training (P = 0.0453), specialty (P = 0.0178), community (P = 0.0271), fellowship training (P = 0.0317), ACDF case volume (P = 0.0305), knowledge of osteobiologic costs (P = 0.0279), use of interbody cages (P < 0.0001), and limitations related to osteobiologic use (P < 0.0001). Regional distribution of the three most common osteobiologics. Abbreviations: AICBG = autologous iliac crest bone graft; DBM = demineralized bone matrix. Univariate Analyses Assessing the Relationship Between Osteobiologic Use and Study Covariates. Statistically significant P values are shown in bold.
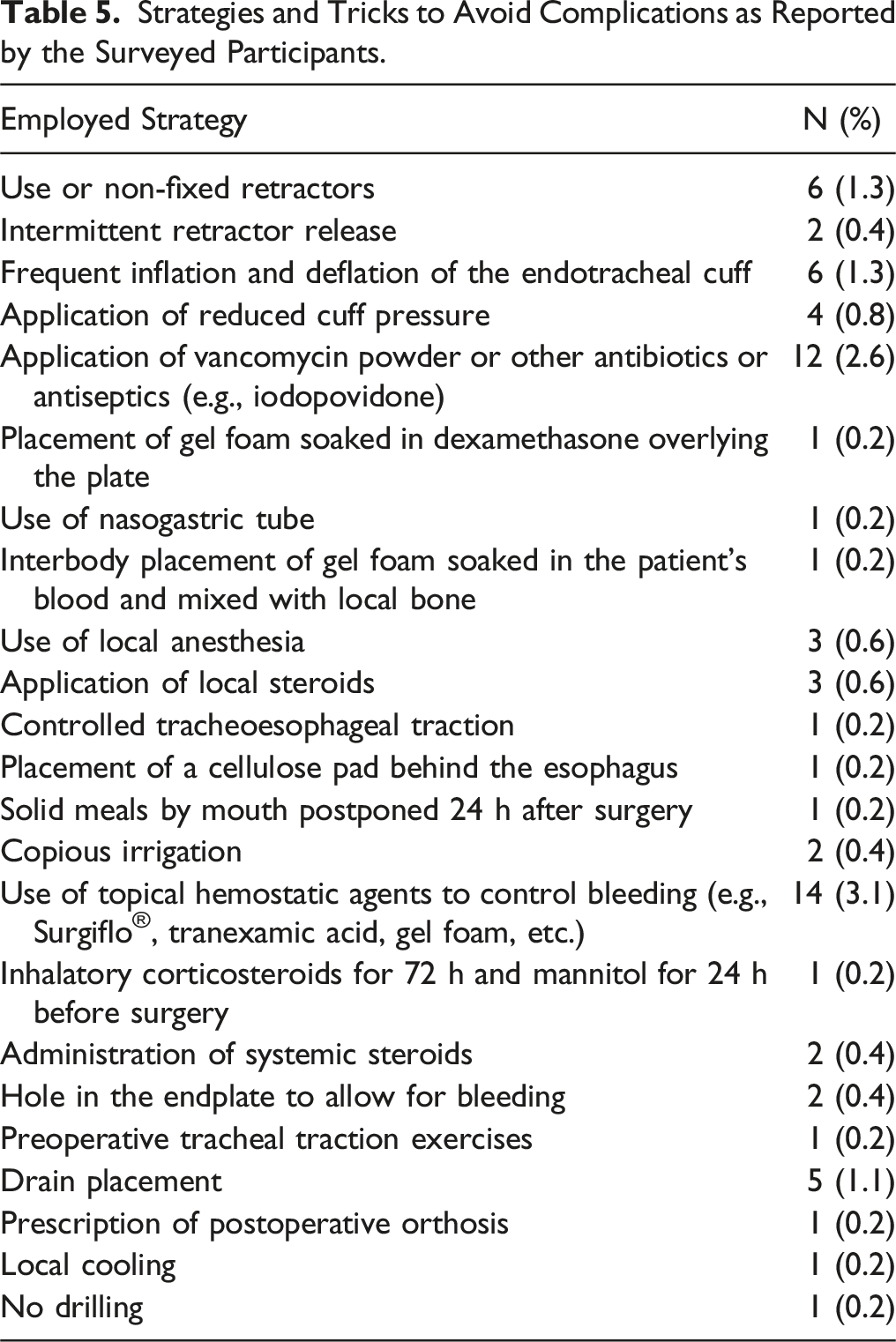
Strategies and Tricks to Avoid Complications as Reported by the Surveyed Participants.
When asked about the main factors influencing their choice of a specific osteobiologic, the most important was the evidence base, followed by availability, cost, historical practice, education, and vendor support (Figure 2). In 66.8% of cases, respondents were not limited by the costs of osteobiologics. However, most of the remaining surgeons (23.6%) were burdened by the high costs of these products, especially when practicing in low-to-middle-income countries and under healthcare systems in which insurances do not cover for osteobiologics, thus requiring patients to pay out of their own pockets. Additional factors limiting the utilization of these products were the lack of strict necessity for their use given acceptable outcomes with other approaches (3.5%), local hospital policies (3.9%), and product availability (1.3%). Finally, 91.5% of surgeons were not aware of specific guidelines regarding the use of osteobiologics in ACDF. Conversely, the remaining surgeons mentioned guidelines from AO Spine (5.0%), NASS (0.7%), or other sources (2.8%). Main factors influencing the choice of a specific osteobiologic among participants rated between 1 (“most important”) and 6 (“not important”).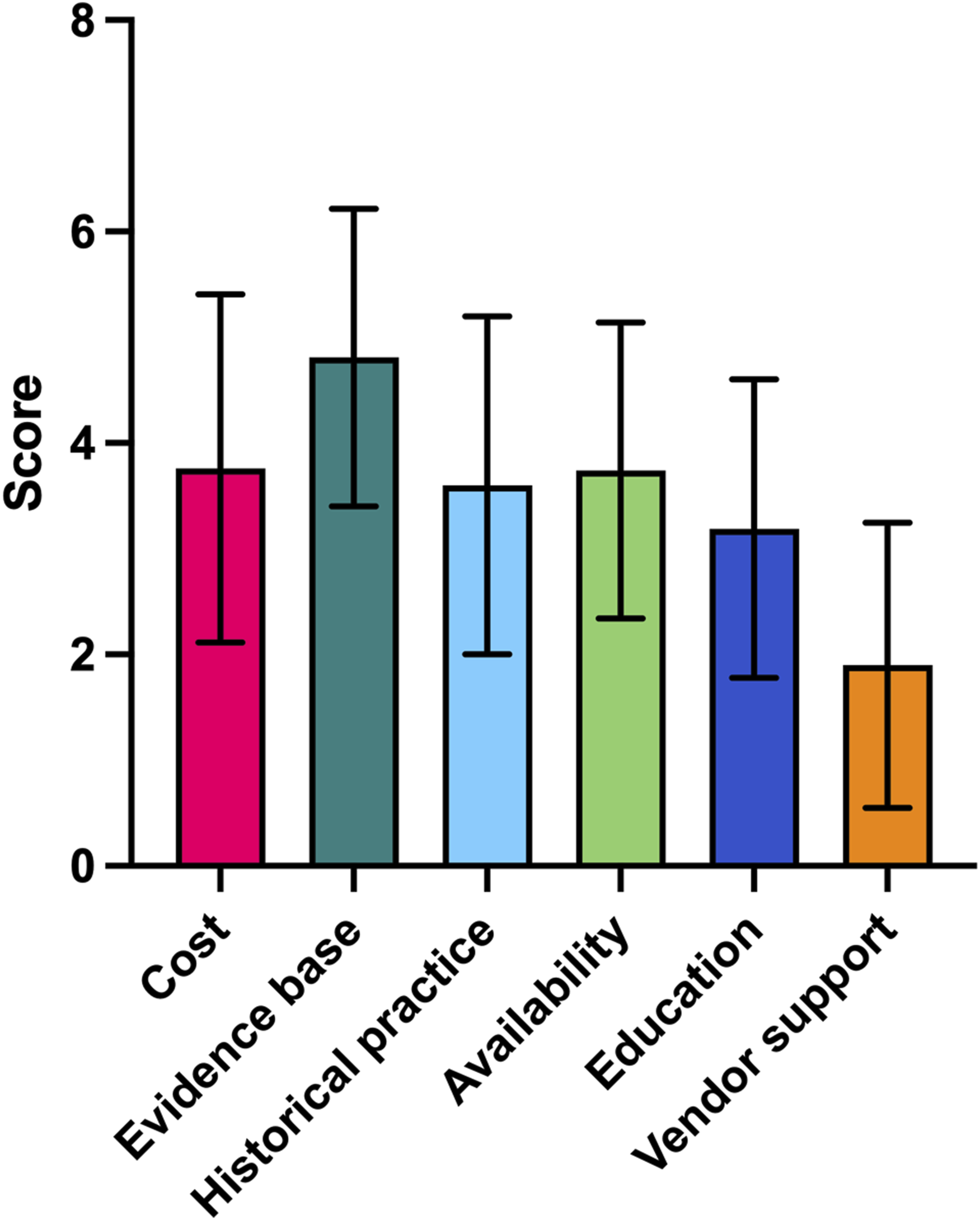
Factors Associated with the Use of Osteobiologics
Multivariate Logistic Regression Model Showing the Association Between Osteobiologic Use in ACDF and Study Covariates.
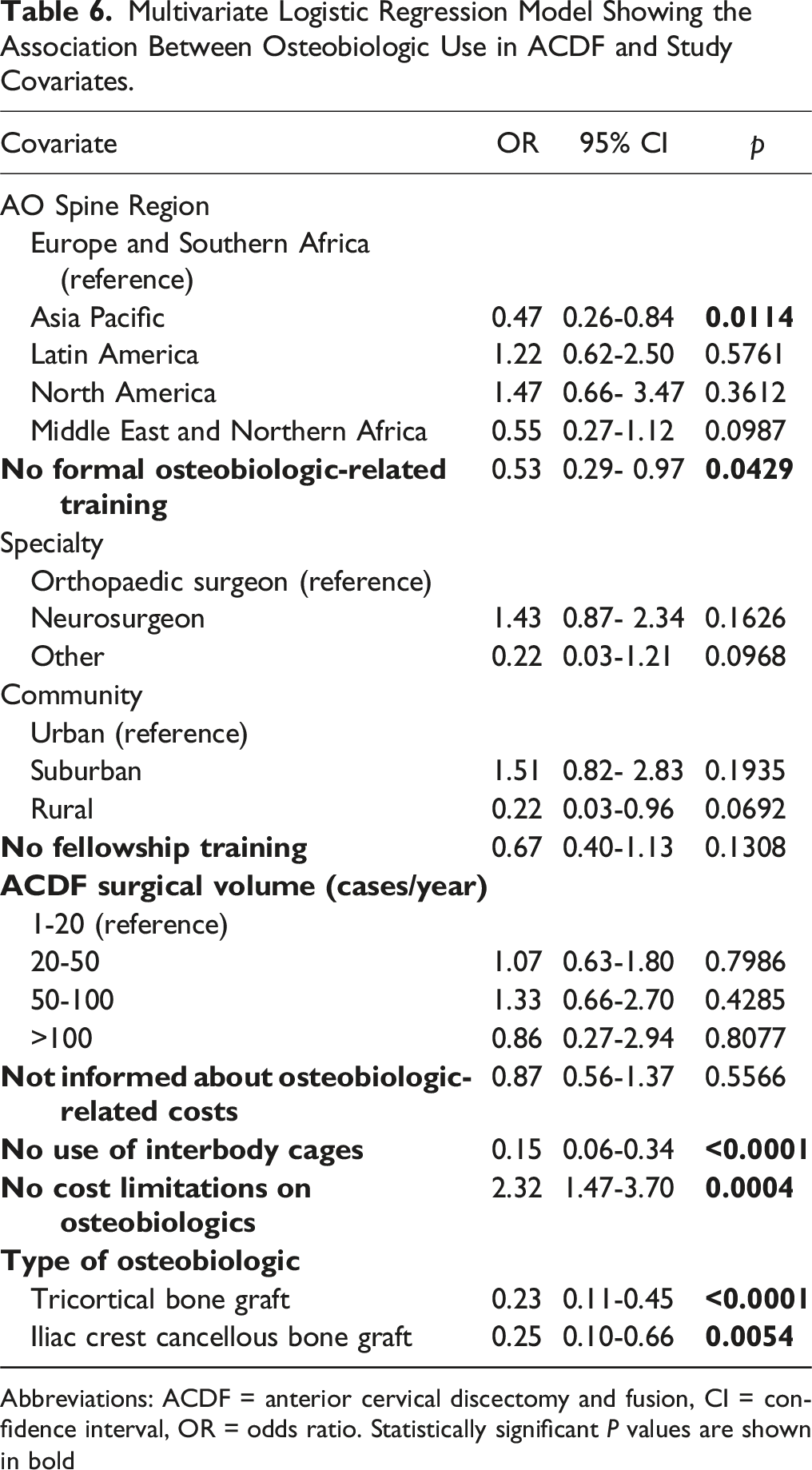
Abbreviations: ACDF = anterior cervical discectomy and fusion, CI = confidence interval, OR = odds ratio. Statistically significant P values are shown in bold
Multivariate Logistic Regression Model Showing the Association Between Osteobiologic-related Training and Study Covariates.
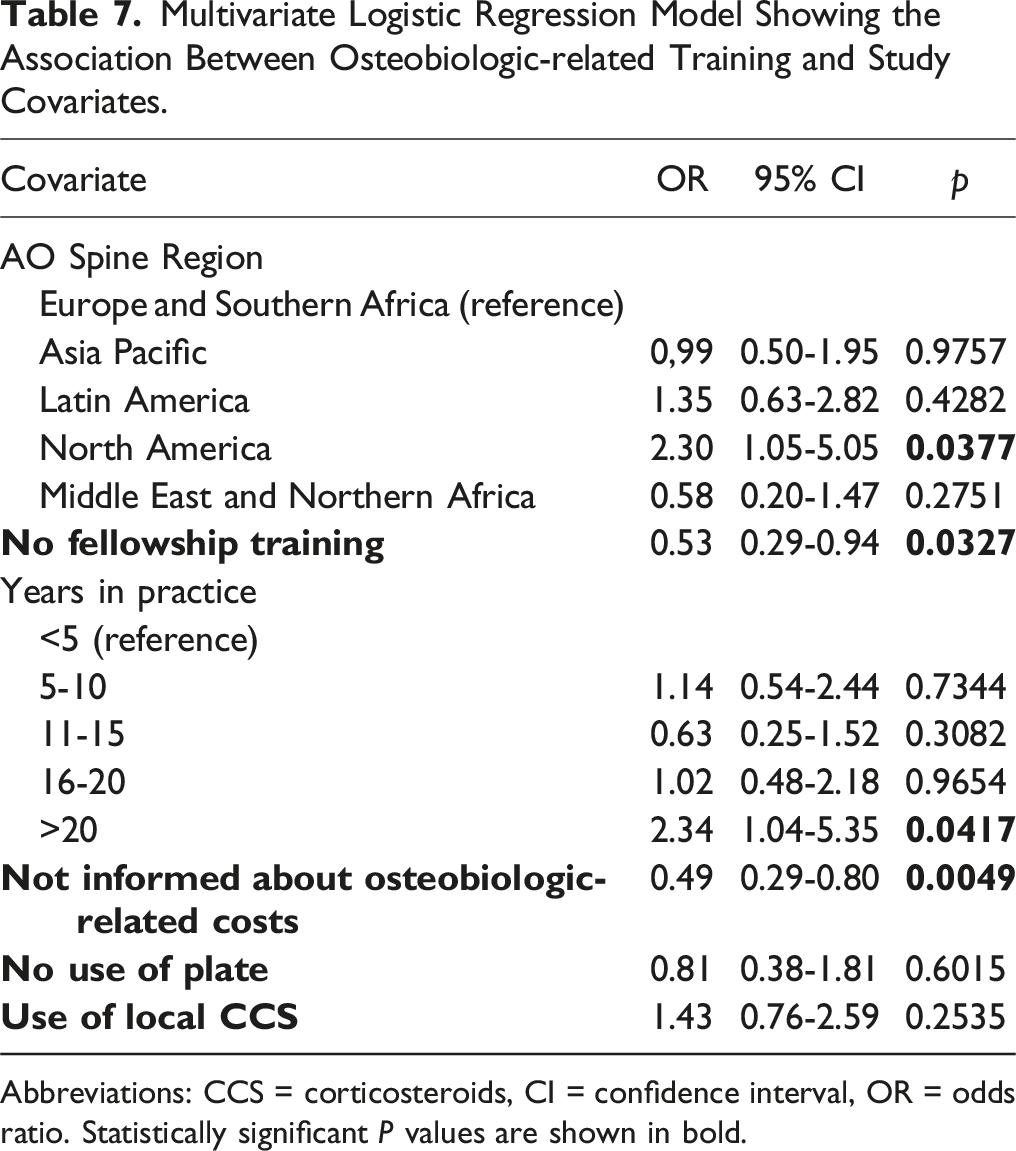
Abbreviations: CCS = corticosteroids, CI = confidence interval, OR = odds ratio. Statistically significant P values are shown in bold.
Multivariate Logistic Regression Model Showing the Association Between the Use of Interbody Cages (>50% of Cases) and Study Covariates.
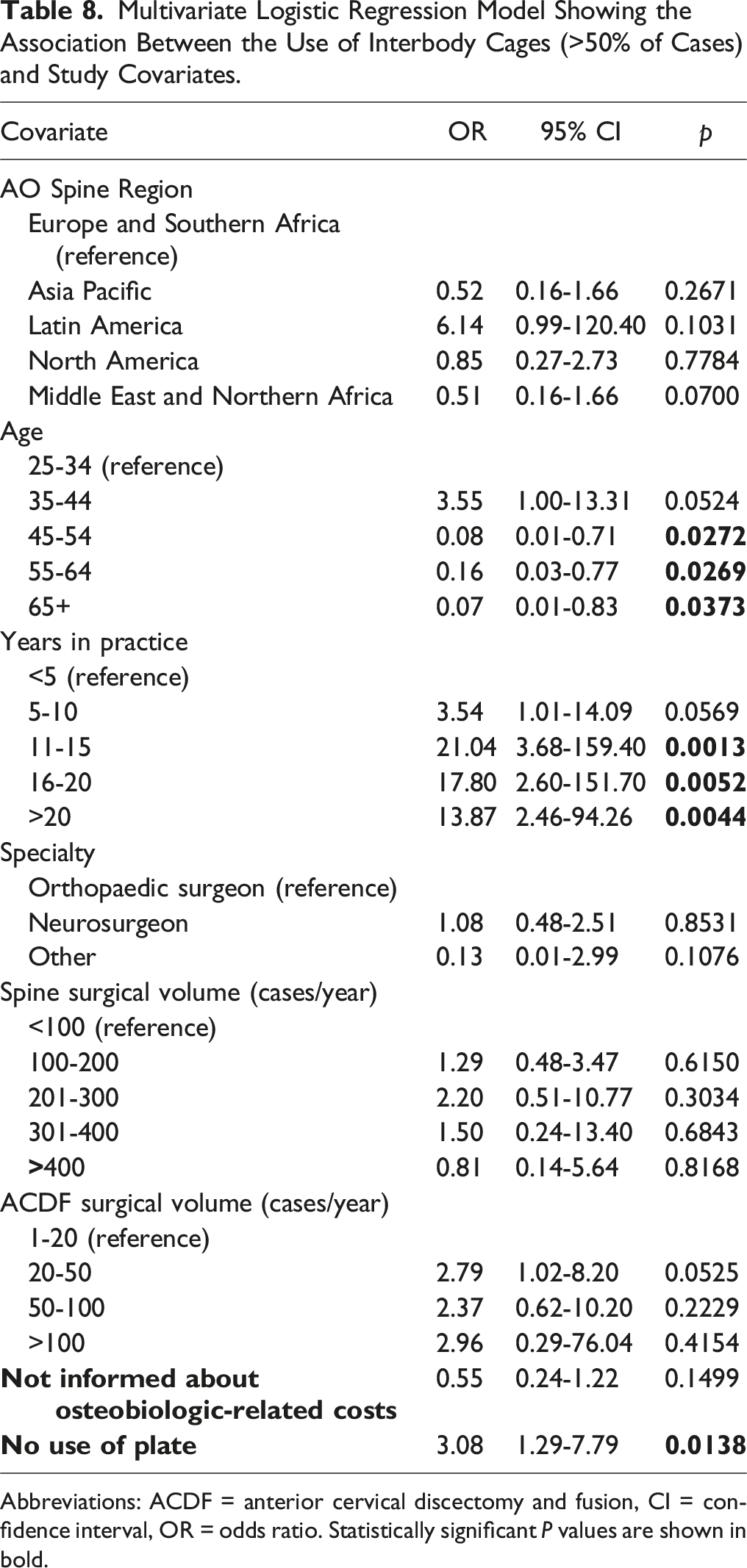
Abbreviations: ACDF = anterior cervical discectomy and fusion, CI = confidence interval, OR = odds ratio. Statistically significant P values are shown in bold.
Multivariate Logistic Regression Model Showing the Association Between the Use of an Anterior Plate (>50% of Cases) and Study Covariates.
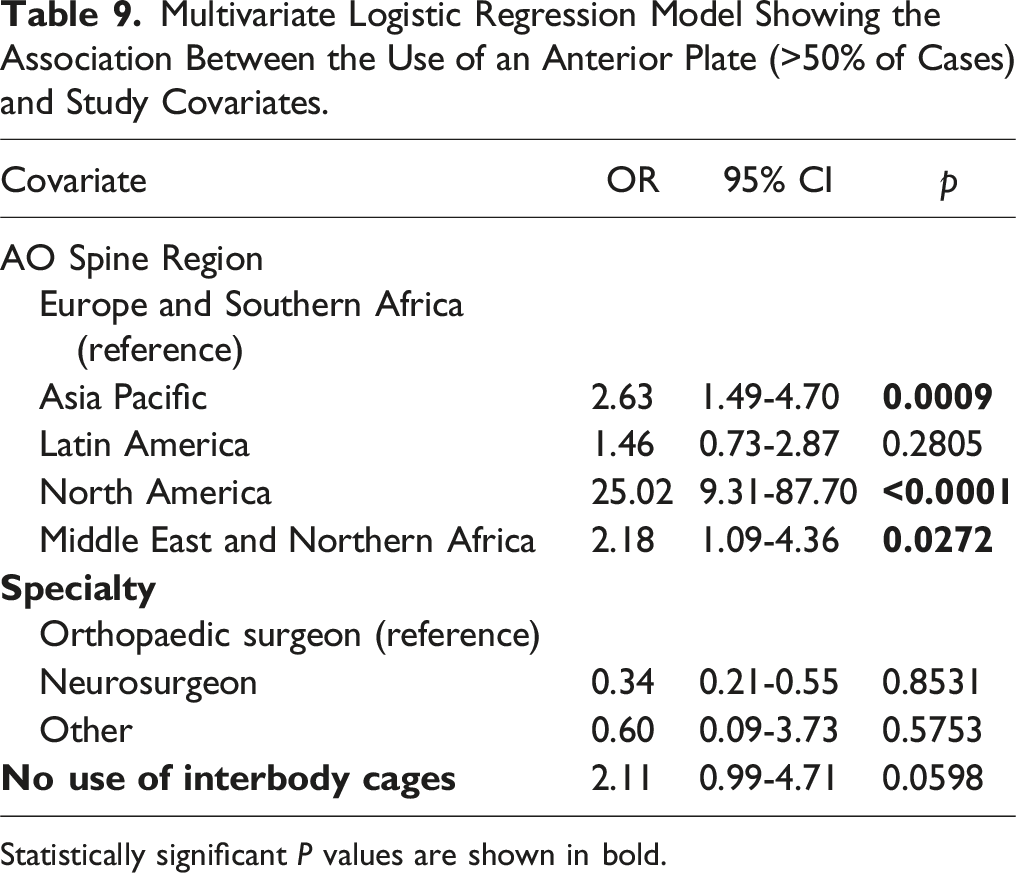
Statistically significant P values are shown in bold.
Discussion
The findings of this study reveal important insights into the global practices and preferences for osteobiologics in ACDF surgery. The high variability in the use of osteobiologics, both in terms of types and frequency, underscores the lack of a universally accepted standard in clinical practice. This variability is influenced by multiple factors including regional differences, surgeon training, and economic considerations.
One of the main observations is the significant proportion of surgeons who have not received formal training in the use of osteobiologics. This highlights a critical gap in spine surgery education, suggesting that despite the availability of osteobiologics and their potential benefits, many surgeons may be underprepared to effectively utilize these materials. Given that the effectiveness and safety of each osteobiologic are closely linked to its underlying mechanisms and specific biological pathways, a deep understanding of how these materials function in vivo is essential. 13 Overlooking these nuances may potentially cause undesired effects and severe adverse events, which might even be life-threatening. 14 Furthermore, whether osteobiologics significantly improve ACDF clinical outcomes and fusion rates is still to be determined, as recently highlighted by a systematic review. 15
The reliance on unregulated learning platforms such as courses, webinars, and industry-sponsored events may contribute to the inconsistent use of osteobiologics, as these methods do not always provide the comprehensive training necessary for informed clinical decision-making. Furthermore, over relying on industry-organized educational events may skew perceptions of efficacy towards the products being promoted, increasing the risk of conflicts of interest.
The study also reveals a lack of awareness regarding the costs of osteobiologics among many surgeons, which could influence their adoption and utilization. This is particularly relevant considering that the costs associated with ACDF widely vary from hundreds to several thousand dollars based on the specific implants and osteobiologics employed, 16 as well as due to local reimbursement policies and insurance coverage. 17 In regions where healthcare systems do not cover the cost of these materials, surgeons may be hesitant to use them, particularly if patients must bear the financial burden. 18 This economic barrier could lead to disparities in the quality of care provided, with patients in lower-income regions potentially receiving less optimal or more invasive treatments (i.e., due to the higher use of AICBG) because of cost constraints.
Another critical factor influencing osteobiologic use is the evidence base supporting their efficacy. Surgeons were more likely to adopt osteobiologics when there is strong, evidence-based support for their use. However, this study shows that in the absence of robust evidence, historical practices, and surgeon familiarity often guide clinical decisions. This also applies to some of technical tricks employed by surveyed participants, such as the use of inhalatory corticosteroids, retroesophageal padding, or the use of vancomycin powder, which has not been validated in ACDF neither proven definitively safe and effective in other spine regions.19,20 This reliance on tradition over evidence can perpetuate the use of less effective, outdated, or even harmful techniques, further contributing to the variability in ACDF outcomes.
The regional differences in osteobiologic use observed in this study also raise important considerations. For instance, surgeons in the Asia Pacific region were less likely to utilize osteobiologics, and reported a substantially more frequent use of AICBG, either in the form of a tricortical or cancellous bone graft. Conversely, osteobiologic-related training was significantly more common in North American surgeons, which further highlights regional discrepancies in training pathways. These variable practice patterns may be due to differences in access to certain medical technologies, variations in healthcare infrastructures, or cultural and educational differences in surgical training. Such regional discrepancies highlight the need for more standardized global guidelines and improved access to training and resources. 21
The lack of awareness and use of guidelines related to the use of osteobiologics in ACDF is another concerning finding. Indeed, 9 out of 10 participants were unaware of the existence of any specific documentation, and the remaining sparingly mentioned guidelines from NASS and AO Spine. Over the years, NASS has issued evidence-based coverage recommendations for various materials, including allograft and DBM (2017), BMP-2 (2014), and synthetics (2023). 22 However, a comprehensive guideline has yet to be released. In this context, the AOGO guideline marks a significant milestone being the first to offer recommendations for the use of osteobiologics in ACDF. 12 Interestingly, the results of the present survey align closely with AOGO recommendations. The widespread use of structural AICBGs or cages with cancellous AICBGs or other osteobiologics such as allograft, DBM, HA, and β-TCP reflects the guidance advocating for either autograft or allograft vs. cages with osteobiologics, both of which are associated with comparable outcomes. 12 However, the low awareness of these guidelines suggests that more efforts are needed to disseminate and implement them across the global spine surgery community. Given that these guidelines were only recently introduced, it is likely that they will reach a broader audience over time, leading to greater implementation of the recommended practices in the near future. Therefore, the authors plan to repeat the survey after a designated period to evaluate the extent of guideline adoption and track changes in practice over time following their implementation.
This study has some limitations. First, the overall low response rate (458 respondents out of approximately 6,000 recipients) may have limited the reliability of the collected data. Although providing valuable insights, the reliance on self-reported data within this investigation may introduce response bias. Additionally, some regions, particularly North America, were significantly underrepresented compared to others, such as Europe and Southern Africa and Asia Pacific. The limited data from these regions could skew the results toward the small sample of surgeons who responded to the questionnaire. Altogether, these confounders may impact the reliability of our analyses and affect data interpretation. Therefore, a more comprehensive survey in these underrepresented areas is necessary to better understand their practice patterns and enhance the generalizability of our findings. Furthermore, as a cross-sectional study, this research cannot establish causality or track changes in practice over time.
Conclusions
In conclusion, the findings of this study highlight the variation in practice patterns and surgeon attitudes regarding use of osteobiologics in ACDF surgery. The data of the survey reveal the need for more formalized and comprehensive training, better awareness of the costs and evidence supporting osteobiologic use, and the dissemination of standardized guidelines. Addressing these issues could lead to improved patient outcomes in ACDF surgeries.
Supplemental Material
Supplemental Material - Global Practices and Preferences in the Use of Osteobiologics for Anterior Cervical Discectomy and Fusion: A Cross-Sectional Study
Supplemental Material for Global Practices and Preferences in the Use of Osteobiologics for Anterior Cervical Discectomy and Fusion: A Cross-Sectional Study by Luca Ambrosio, Viswanadha Arun Kumar, Pieter-Paul A. Vergroesen, Zorica Buser, Hans Joerg Meisel, Nancy Santesso, Jason P. Y. Cheung, Hai V. Le, Gianluca Vadalà, Amit Jain, Andreas K. Demetriades, Sam K. Cho, Patrick C. Hsieh, Ashish D. Diwan, Christopher Martin, Tim Yoon, Sathish Muthu, and AO Spine Knowledge Forum Degenerative in Global Spine Journal
Footnotes
Acknowledgments
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine degeneration experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: European Association of Neurosurgical Societies (immediate past-president), Global Neuro Foundation (vice-president); AO Spine Knowledge Forum Degenerative (steering committee and associate members); Depuy Synthes Spine (consulting work); Globus Medical (consulting work, fellowship education support to institution, royalties); Medtronic (consulting fees, royalties, support for attending meetings and/or travel, support to institution); 3M Science (educational consulting), SI Bone (support to institution, royalties), ATEC (support for attending meetings and/or travel, consulting fees), AO Foundation (contracts, support for attending meetings and/or travel), SeaSpine (support to institution), Next Science (support to institution), Motion Metrics (support to institution), NIH SBIR (support to institution), Cerapedics (consulting fees, fellowship education support to institution), AO Spine (consulting fees, support for attending meetings and/or travel, fellowship education support to institution), The Scripps Research Institute (consulting fees), Xenco Medical (consulting fees), North American Spine Society (support for attending meetings and/or travel, committee member, board of directors and executive committee), AO Spine North America (research committee member), Lumbar Spine Research Society (co-chair educational committee), Fehling Instruments GmbH (royalties), Stayble Therapeutics (consulting fees), Mundipharma (consulting fees), Spinplant GmbH (stock options), NC Biomatrix (stock options), Stryker (consulting fees), Carlsmed (consulting fees), Alphatec (consulting fees, stock options), Zimvie Spine (royalties), American Orthopaedic Association (committee member), Cervical Spine Research Society (committee member), Scoliosis Research Society (committee member), Empirical Spine (support to institution), International Society for the Study of the Lumbar Spine (support for attending meetings and/or travel, board member), Medyssey (stock options).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.