
Abstract
Study Design
Retrospective cohort study.
Objectives
To determine the incidence and identify independent predictors of incisional hernia following anterior lumbar interbody fusion (ALIF).
Methods
The PearlDiver national database was queried to identify patients who underwent ALIF. Patients were stratified based on the presence or absence of an incisional hernia diagnosis. Chi-squared and Student’s t-tests were used to identify demographic and comorbidities between the 2 cohorts. Multivariate logistic regression analysis was performed to identify independent risk factors for incisional hernia development.
Results
A total of 165,110 patients underwent ALIF during the study period, of whom 4164 (2.52%) developed an incisional hernia. The mean and median time to diagnosis were 1093 ± 1030 days and 728 days, respectively. Independent risk factors for incisional hernia included obesity (aOR: 1.19), smoking (aOR: 1.09), chronic obstructive pulmonary disease (COPD) (aOR: 1.25), ascites (aOR: 2.16), surgical site infection (SSI) (aOR: 1.96), malnutrition (aOR:1.56), and two-level ALIF (aOR: 1.12) (all P < 0.05).
Conclusion
The incidence of incisional hernia following ALIF is 2.52%, with obesity, smoking, COPD, ascites, SSI, malnutrition, and two-level surgeries identified as independent risk factors. Spine surgeons should implement risk mitigation strategies including weight loss, smoking cessation, and nutritional support. Future research should explore the impact of surgical techniques on hernia risk such as open vs minimally invasive ALIF, incision type, and suture methods, on hernia prevention, as well as evaluate the efficacy of targeted rehabilitation protocols in reducing hernia risk.
Introduction
Anterior lumbar interbody fusion (ALIF) is a widely accepted treatment for both spinal deformity and degenerative spine pathology. ALIF offers distinct advantages compared to other lumbar fusion techniques, including enhanced restoration of lumbar lordosis, increased fusion rates compared to some posterior-only techniques, and improved correction of coronal and sagittal imbalance.1-3 The anterior approach also enables direct visualization of the anterior spinal column, facilitates extensive discectomy, allows placement of the largest interbody devices, and achieves indirect decompression of neural structures while avoiding trauma to the posterior paraspinal muscles.4-6
However, ALIF is also associated with several well-documented risks and complications, including but not limited to: iliac vessel injury, deep venous thrombosis, retroperitoneal hematoma, and retrograde ejaculation.1,6 Unique to ALIF is the potential development of incisional hernias, a complication that can impact morbidity. Incisional hernias require surgical management in up to 70% of cases and are associated with recurrence rates as high as 40%.4,7 While preoperative consultations often emphasize the risks of revision spine surgery secondary to instrumentation failure, pseudoarthrosis, and/or adjacent segment disease, the potential need for future surgery to address incisional hernias is often overlooked.
A recent study reported a 2.7% incidence of incisional hernia following ALIF, and identified gender, hospital length of stay, and history of abdominal surgery as potential risk factors but was limited by small sample size, with only 20 cases of this complication. 4 To date, no large database studies have comprehensively examined this complication, leaving its true incidence and the influence of other broader demographics and comorbidities unclear. Identifying the incidence and predictors of hernia development is critical for enhancing preoperative patient education and implementing targeted risk mitigation strategies. Therefore, this study aims to characterize the incidence and identify the predictors of incisional hernia following ALIF.
Methods
Study Population
We queried the PearlDiver database (PearlDiver Technologies, Fort Wayne, IN, USA), a national database containing records from 170 million patients to identify patients who underwent ALIF. PearlDiver is a de-identified database, thus, informed consent was waived and Institutional Board Review (IRB) approval was not required.
Identification of Study Cohorts
Current Procedural Terminology (CPT) codes were used to identify patients who underwent one- or multi-level ALIF from 2010 to 2022 Q3 (Supplemental Table 1). Using International Classification of Disease (ICD) 9th (ICD-9) and 10th (ICD-10) edition codes, patients were further stratified based on the presence or absence of a subsequent incisional hernia diagnosis (Supplemental Table 1). Continuous variables were reported as mean values with standard deviations, while categorical variables were reported as percentages. Differences between patient demographics and comorbidities were compared between the cohorts.
Primary Endpoints
The primary outcome of the study was to determine the incidence of incisional hernia following ALIF. Secondary outcomes included the average time from surgery to hernia diagnosis and the risk factors associated with its development. Patient characteristics included age, Elixhauser Comorbidity Index (ECI), gender, diabetes, obesity, tobacco use, peripheral vascular disease (PVD), malnutrition, chronic steroid use, surgical site infection (SSI), caesarean section, abdominal aortic aneurysm (AAA), ascites, anemia, and chronic obstructive pulmonary disease (COPD). Procedural characteristics included one- and two-level ALIF.
Statistical Analysis
Student’s t-test was used to compare continuous variables, while Pearson’s chi-squared test was used for categorical variables to assess demographic and comorbidity differences between the 2 cohorts. Univariate logistic regression was performed to identify predictors of incisional hernia following ALIF. Multiple logistic regression was conducted to account for covariates, including age, gender, ECI, and two-level ALIF. Due to the small number of 3+ level ALIFs, we did not add this factor as a covariate. All statistics were completed using RStudio (Version 4.4.2). A P-value of <0.05 was considered statistically significant.
Results
A total of 165 110 patients underwent ALIF during the study period, of which 4164 (2.52%) developed an incisional hernia following the procedure with a mean and median time to diagnosis of 1093 ± 1030 days and 728 days, respectively.
Patient Characteristics
Patient Characteristics. Continuous Variables are Presented as Mean Values + Standard Deviation.
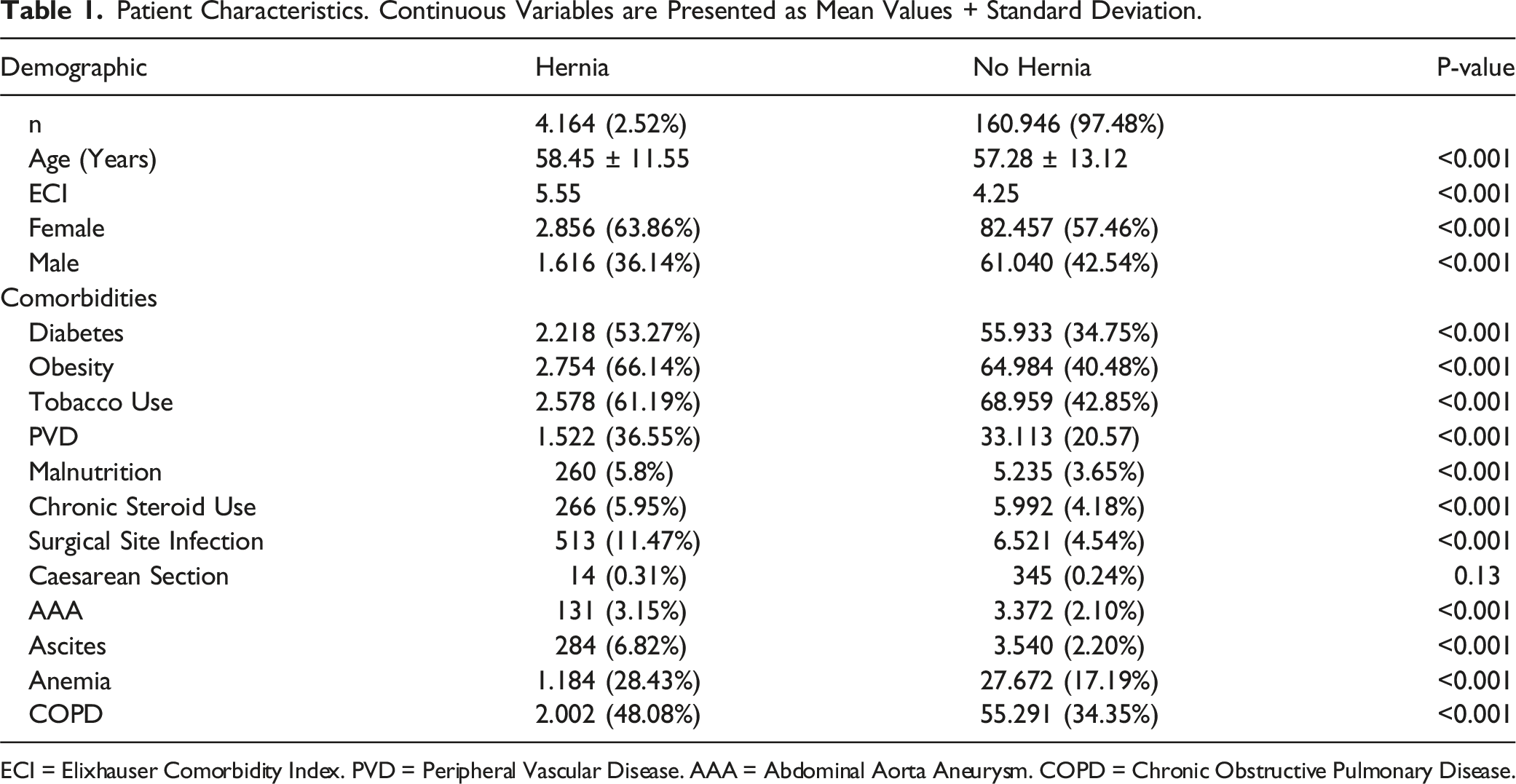
ECI = Elixhauser Comorbidity Index. PVD = Peripheral Vascular Disease. AAA = Abdominal Aorta Aneurysm. COPD = Chronic Obstructive Pulmonary Disease.
Predictors of Incisional Hernia following ALIF
Univariate Analysis of Risk Factors for Incisional Hernia Following ALIF.
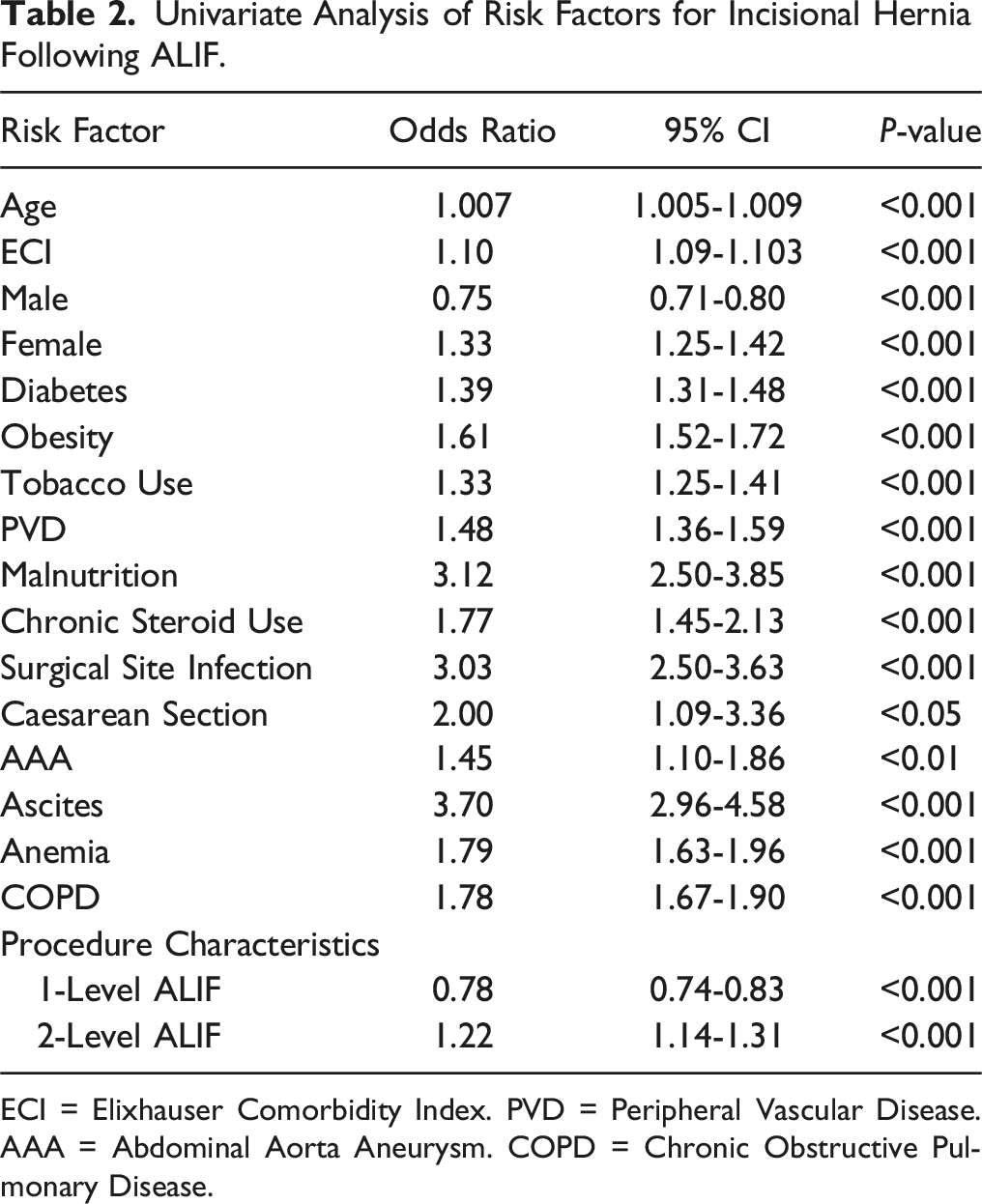
ECI = Elixhauser Comorbidity Index. PVD = Peripheral Vascular Disease. AAA = Abdominal Aorta Aneurysm. COPD = Chronic Obstructive Pulmonary Disease.
Multivariate Analysis of Risk Factors for Incisional Hernia Following ALIF.
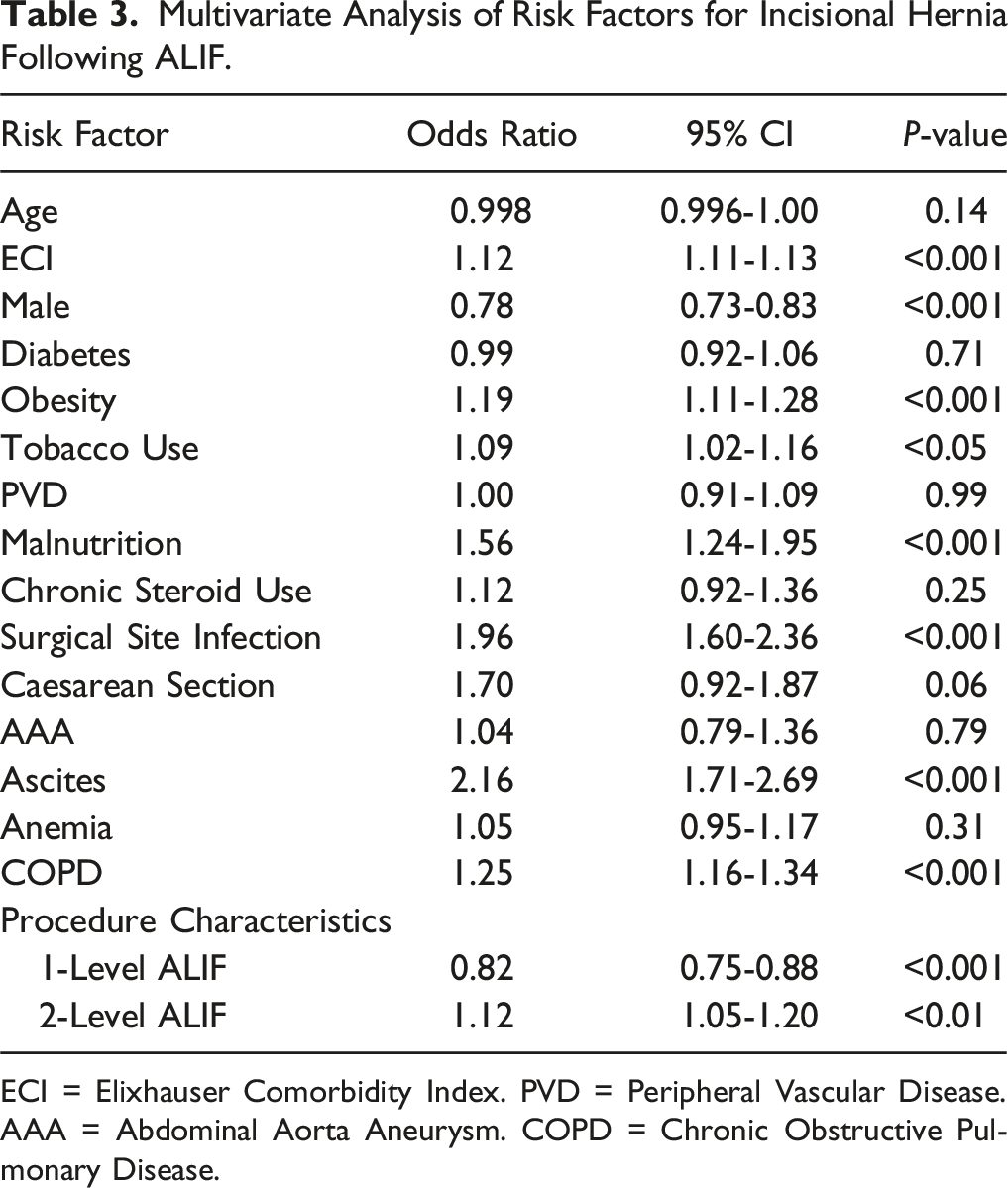
ECI = Elixhauser Comorbidity Index. PVD = Peripheral Vascular Disease. AAA = Abdominal Aorta Aneurysm. COPD = Chronic Obstructive Pulmonary Disease.
Discussion
In this study we aimed to characterize the incidence and risk factors for incisional hernia following ALIF. Using a large national database, we found that 2.52% of patients who underwent ALIF developed an incisional hernia, with the diagnosis occurring, on average, just under 3 years of the surgery. Additionally, we identified several independent patient-specific factors such as comorbidity index, obesity, tobacco use, malnutrition, surgical site infection, ascites, and COPD that significantly predict the development of this complication. While incisional hernia is a recognized complication of ALIF, this study is the first large-scale study to quantify its incidence, providing valuable data to enhance preoperative discussions, better inform patients about this complication, and emphasize the importance of risk mitigation strategies.
The 2.52% incidence of incisional hernia following ALIF observed in this study closely aligns with the 2.7% incidence reported by Luu et al. 4 It is however notably lower than the rates observed in other forms of abdominal surgery, likely due to differences in incision length and type. For instance, a large meta-analysis of 14,618 patients reported a 12.18% incidence of hernia following midline laparotomy. 8 This disparity is likely attributable to the shorter incision lengths used in ALIF, as prior research has established a clear association between longer incision lengths and increased hernia risk.9,10 ALIF is typically reserved for the L4-5 and/or L5-S1 spinal segments, requiring only a 2-3-inch incision, which is significantly smaller than those employed in laparotomies. Our study further supports this relationship, as we found that two-level ALIF was associated with increased incisional hernia risk where incision length is typically longer compared to single-level ALIF. Additionally, the type of incision used in ALIF likely contributes to the lower hernia rates. Surgeons may utilize a transverse Pfannenstiel incision to access the retroperitoneum during ALIF, which has significantly lower hernia rates compared to midline incisions. This is because transverse incisions align with the natural orientation of the abdominal muscles, promoting better wound closure. 11 These unique incision characteristics may explain the relatively lower incidence of hernia observed in our study compared to other abdominal surgeries.
Differences in surgical settings may also play a role in the incidence disparity. Basta et al. reported an almost five-fold increased hernia risk for emergency laparotomies compared to elective laparotomies. 12 ALIFs are almost exclusively performed for pre-planned, elective indications, such as degenerative spine disease and spinal deformity, and are rarely used in emergency settings. Another contributing factor may be postoperative course. Our findings, along with prior research, highlight SSI as a strong predictor of incisional hernia risk. 13 Most studies report an SSI incidence of less than 1% following ALIF, whereas midline laparotomies have been associated with SSI rates as high as 16.3%, further explaining the disparity in hernia incidence between these procedures.14-17
Regarding predictors of hernia following ALIF, obesity emerged as a significant risk factor, consistent with findings from prior studies.18,19 Walming et al reported a 2.63-fold increase in postoperative hernia risk in patients with a BMI of 30-35 compared to those with a BMI of <25, and an almost five-fold increased risk in those with a BMI >35. 18 This increased risk likely results from increased intra-abdominal pressure and weakened abdominal wall musculature caused by excess adipose tissue, predisposing these patients to hernia formation. 20 For similar reasons, ascites and COPD were significant risk factors. Ascitic fluid increases intra-abdominal pressure through the accumulation of fluid in the abdominal cavity, while chronic coughing associated with COPD further exacerbates pressure, increasing the likelihood of hernia development. 21
SSIs were among the strongest predictors of incisional hernia. These infections compromise wound integrity through localized inflammation, delayed healing, and tissue necrosis, weakening the abdominal fascia and increasing hernia risk. 22 Consistent with our findings, Murray et al. reported a two-fold increase in hernia risk following abdominal surgery in patients with SSIs. 23 Tobacco use was another significant predictor, likely due to its detrimental effects on wound healing. Nicotine-induced vasoconstriction, peripheral tissue hypoxia, reduced fibroblast proliferation, and impaired wound contraction all contribute to delayed wound healing and tissue repair.24,25 Sorenson et al also found a nearly four-fold increased incisional hernia risk among smokers. 26 Malnutrition furthers these risks, as nutrient deficiencies impair tissue repair and collagen synthesis, predisposing patients to wound complications such as SSIs and fascial dehiscence.27,28 Previous research has shown an association between patients with a nutritional disorder, characterized by an albumin level <3.5 g/dl, with the risk of incisional hernia. 29
Preoperative consultations with spine surgeons often focus on complications related to spinal pathology, such as hardware failure, pseudoarthrosis, and adjacent segment disease, as potential drivers of future revision surgeries. However, our analysis emphasizes incisional hernia as an additional surgical complication that warrants discussion. These hernias frequently require surgical correction and are associated with recurrence rates as high as 40%, even after repair.7,12,30 Of the 20 hernia cases following ALIF that Luu et al. found, 14 (70%) underwent surgical repair, with 21% requiring a bowel resection. 4 Recognizing this risk allows surgeons to better prepare patients for the postoperative period following ALIF.
Based on the identified risk factors in this study, surgeons should emphasize preoperative optimization strategies. Smoking cessation should be strongly encouraged, as smoking not only impairs fusion rates, but also increases the risk of incisional hernias. This is particularly critical for patients with COPD, who already have an elevated risk. Moreover, nutritional status should be addressed for patients with albumin levels <3.5 g/dl in preoperative lab assessments. In a randomized clinical trial, Xu et al. outlined a multimodal nutritional management (MNM) protocol for patients with poor nutritional status undergoing primary lumbar spine surgery, showing that it reduced postoperative complications. 31 This protocol may also serve as a strategy to reduce hernia risk. For obese patients, preoperative weight loss should be emphasized. In a study of 922 patients, Pernar et al demonstrated a stepwise increase in hernia recurrence risk following abdominal surgery with increasing BMI class, with the highest risk observed in patients with BMI >40 kg/m2. 32 Even small amounts of weight loss in the preoperative period can significantly reduce hernia risk. Surgeons should also remain vigilant for hernias during postoperative physical examinations, especially in patients who developed an SSI. As physical examinations often focus on the spine, abdominal evaluations may be overlooked. Proper evaluation includes palpation of the surgical scar to detect abdominal wall defects, with confirmatory imaging such as CT scans ordered when necessary. These measures can help ensure early detection and management of incisional hernias, improving patient outcomes.
Limitations
This study is not without limitations. The PearlDiver database relies on accurate coding during the billing process, introducing a potential source of human error that may have impacted the reported incidence of incisional hernia. Due to this limitation, the incidence may have been over- or under-represented. For instance, in addition to incisional hernias, other types of hernias exist, including inguinal, femoral, epigastric, and diaphragmatic. If incorrect hernia codes were used during billing, the database might inaccurately capture the incidence of incisional hernias. Another limitation is the inability to differentiate between ALIF and LLIF, as these procedures share the same CPT codes. However, the incidence reported in our study closely aligns with the findings by Luu et al, reducing the likelihood of significant discrepancies due to coding errors. 4 This consistency also applies to the risk factors identified in our study.
Additionally, the database precluded us from accounting for variables such as suture type and length, post-operative activity restrictions, surgeon experience, incision length and type, or whether access was performed by a spine surgeon vs a vascular or general surgeon. For example, our study found that multi-level ALIF increases hernia risk, likely due to longer incisions. However, there are no standardized guidelines for optimal incision length during ALIF, potentially leading to variability across institutions. Similarly, we were unable to control for post-operative activity restrictions and hospital length of stay, which vary by institution, and may also contribute to hernia risk. By not being able to control for these factors, these limitations may affect the generalizability of our findings, and the incidence of hernia may vary by institution.
Furthermore, we were unable to control for previous abdominal surgeries, including but not limited to umbilical hernia repair, abdominoplasty, gastric bypass, etc.
Lastly, due to the retrospective nature of this study, causal relationships cannot be definitively established. However, our multivariate analysis, which controlled for confounding variables, provides strong evidence of associations with independent risk factors.
Despite these limitations, the study’s large sample size and use of a comprehensive national database represent major strengths, making this the first study to robustly report the incidence and risk factors for incisional hernia after ALIF, providing critical insights on how to mitigate the risks of this complication.
Conclusion
The incidence of incisional hernia following ALIF is 2.52%, with key risk factors including obesity, smoking, COPD, ascites, SSI, malnutrition, and two-level surgeries. To mitigate these risks, surgeons should emphasize preoperative optimization strategies, such as smoking cessation, nutritional support, and weight loss, while remaining vigilant for incisional hernias during postoperative physical examinations to ensure timely diagnosis. Future research should explore the impact of surgical techniques, such as open vs minimally invasive ALIF, incision type, and suture methods, on hernia prevention, as well as evaluate the efficacy of targeted rehabilitation protocols in reducing hernia risk.
Supplemental Material
Supplemental Material - Burden and Predictors of Incisional Hernia Following Anterior Lumbar Fusion: A National Study
Supplemental Material for Burden and Predictors of Incisional Hernia Following Anterior Lumbar Fusion: A National Study by Henry Avetisian, Marc Abdou, William Karakash, Brandon Yoshida, Jeffrey C. Wang, Raymond J. Hah, and Ram K. Alluri in Global Spine Journal.
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Henry Avetisian, Marc Abdou, William Karakash, and Brandon Yoshia have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccential Robotics for lectures and presentations.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.