
Abstract
Incisional hernias are a very common condition and they still are considered to be a surgical challenge due to their recurrence rate. Smoking, obesity and age are risk factors for developing these abdominal wall defects. Despite recent advances in hernia repairs, the recurrence rates of hernias did not significantly diminished, even after the introduction of meshes. The aim of this article is to report a case of a ventral incisional hernia in a 37-year-old man and its successful treatment with a procedure known as the Alcino-Lázaro technique repair. This procedure has been shown to be very effective in incisional hernias, especially in obese patients. Furthermore, it is as cheap as it is reliable, since it can be performed without technological aid or expensive materials (mesh); thus, patients in low-income countries can greatly benefit from this procedure.
Introduction
Ventral hernias are defects that can occur at the abdominal wall near the site of a prior surgical incision. They often originate due to poor wound healing or tissue healing failure. Incisional hernias are one of the most common complications after abdominal surgery, with an estimated incidence as high as 10%–20% following midline laparotomy. 1
Risk factors for developing incisional hernias include smoking, diabetes and older age. The morbidity and recurrence rates after surgery are significantly influenced by obesitiy.1,2
The surgical repair often depends on the size of the hernia and may use components separation, synthetic mesh overlay or even a biological mesh underlay to completely fix the defect. 3 Furthermore, the operative repair has to balance the ability to completely repair the defect without increasing the risk of post-operative complications, given its association with hernia recurrence. 4
We aim to report the case of a ventral incisional hernia in an obese 37-year-old male and discuss its treatment and outcomes.
Case presentation
The patient signed an informed consent form and no information presented herein was written without consent of the patient.
A 37-year-old patient victim of a motorcycle accident was presented to the emergency room with shortness of breath, pale and unstable, with a 155 bpm, 96% O2 saturation, a blood pressure of 90 × 60 mmHg and a Glasgow score of 12. 5 Furthermore, the patient presented a blunt abdominal trauma and advanced trauma life support (ATLS) was promptly initiated.
The patient was rushed to the operating room and submitted to an exploratory laparotomy. A considerable amount of blood was found inside the abdominal cavity. Lesions of the liver (grade 3), spleen (grade 5) and mesentery were also found. 6 Repairs of the liver and mesentery were performed together with an emergency splenectomy. During the surgery, the patient needed blood transfusion and vasoactive drugs.
After the surgery, the patient was moved to the intensive care unit (ICU) in a severe general state and clinically unstable, even though high doses of adrenaline were administered. After 3 weeks at the ICU, the patient did not improve and was put on a ventilator; however, his gut eviscerated and he was submitted to a peritoneostomy (Bogota bag technique). 7 Due to the severity of the case and his long hospital stay, the surgical team opted to close the abdominal wall by second intention, as the wound had a good amount of granulation tissue and a good overall aspect (Figure 1).

Granulation tissue before the skin graft.
Ten months after the initial trauma, the patient had a consult with the plastic surgery service for wound evaluation. The plastic surgery team performed a partial graft from the patient’s lumbar region. The surgery was uneventful and there was a good clinical outcome and scar evaluation showed improvement.
However, the patient presented an incisional ventral hernia (Figure 2) with a longitudinal diameter of 10.3 cm and a transverse diameter of 5.4 cm. It was necessary to use a compressive strap or elastic abdominal band in order to avoid hernia expansion and abdominal discomfort. The patient complained that the strap and the band were uncomfortable and he stated that “he wasn’t able to stay shirtless due to shame,” as well as “not performing any physical activities due to fear of increasing the size of the hernia or causing other injuries.”

The ventral incisional hernia.
The patient was sent to a surgical service and his hernia was evaluated for possible correction. He was then submitted to a herniorrhaphy according to the Alcino-Lázaro technique (Figure 3), since the public health service of Brazil does not cover the cost for mesh. 8 The surgery was uneventful and the hernia was successfully operated (Figures 4 and 5).
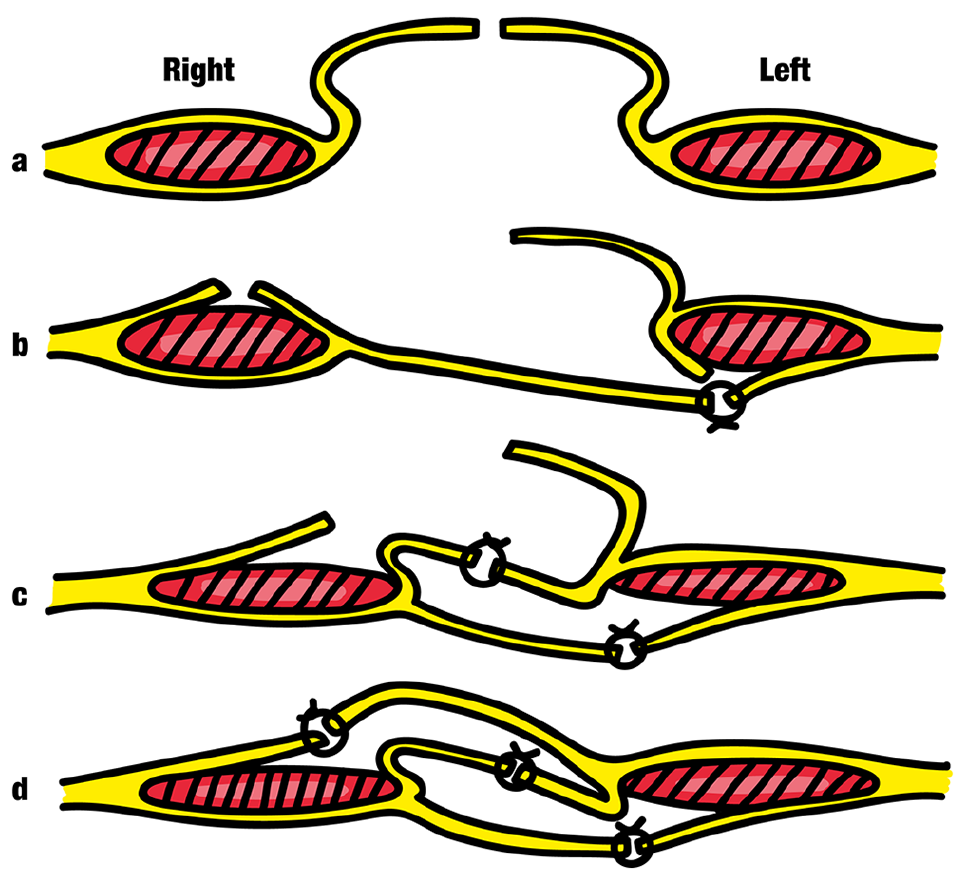
The Alcino-Lázaro technique.

Immediate post-op of the ventral hernia.

Late post-op of the ventral hernia.
One year after the surgery, the patient was contacted by telephone and responded to a quality of life questionnaire 9 which showed significant improvement and a better quality of life after the treatment. The patient reported that the elastic band was not necessary and that he was able to maintain physical activity.
Discussion
Incisional hernia represents the most common wound complication after abdominal surgery, with an incidence ranging from 10% to 20% and recurrence rates ranging from 20% to 46%. Careful evaluation of the patient is needed to observe any predisposing factors for hernia recurrence. This includes inadequate local fascial and muscular layers due to prior tissue loss; muscle denervation or vascular insufficiency due to prior irradiation or infection; wound infection; obesity; chronic pulmonary disease; malnutrition; sepsis; anemia; and corticosteroid therapy. 10
Furthermore, lack of long-term follow-up can lead to undetected recurrence of the incisional hernia. This is often common in public and teaching hospitals, as there is a high workload and a high turnover of surgeons and residents in these institutions. In these circumstances, the follow-up is performed by a team that did not perform the surgery and recurrence is not promptly detected. 7 Past studies have demonstrated a complication rate between 18% and 50%, while they observed a hernia recurrence of 11% after hernia repair with mesh. 11
Some studies reported that the use of mesh for hernia repair reduced recurrence rates up to 15%, 12 while a recent meta-analysis showed a significant reduction when compared with open surgery alone without mesh. 13 These papers, however, were performed with other surgical techniques, and the lack of studies with the treatment presented herein makes comparison difficult.
The “mesh use controversy” lies in the fact that it may lead to mesh-related complications, such as infections, seroma, fistulas and chronic pain. It is hypothesized that chronic pain is associated with suture-related nerve entrapment or suture-induced nerve irritation due to fixation of the mesh by sutures. 14
The procedure performed herein was developed by the Brazilian Professor Alcino Lázaro da Silva and it is known as the “Alcino-Lázaro technique” or “Alcino-Lázaro repair.” According to the literature, this technique possesses high success rates, despite not requiring the use of mesh. As such, it is cheap as it is reliable, since it can be performed without technological aid or expensive materials (mesh);15,16 thus, patients in low-income countries can greatly benefit from this procedure. This procedure is also highly effective in incisional hernias, especially in obese patients,15,16 which was one of the significant aspects of the case reported herein.
The Alcino-Lázaro technique uses rectus sheath flaps and the fibroperitoneal tissue of the hernial sac. Three overlapping layers are produced which approximate the medial edges of the rectus muscles to the midline and suture line tension is reduced by its distribution between the layers. 17
This procedure aims to close the defect by suturing reflected rectus sheath flaps, since it is speculated that this layer provides most of the strength of the anterior abdominal wall. It is reinforced by the inner and outer layers of fibroperitoneal tissue which share the tension across the wound. The rectus muscles are widened and their medial edges brought to the midline so that normal muscle activity would be expected to strengthen rather than disrupt the repair. 16
As previously stated, there is a lack in the literature regarding a greater number of patients treated with this procedure, although a study performed in 251 patients by Laizo et al. 18 observed a recurrence rate of 11% following inguinal hernia repair with this technique. In this article, the authors do not state whether the sample contained obese patients. Nielsen et al. 19 also reported a significantly low recurrence rate (2.8%) in 251 patients submitted to a peritoneal flap hernioplasty without mesh, a technique similar to the one presented herein.
The Alcino-Lázaro procedure is an easy technique with low recurrence and complications rates. It can be a strategy for incisional hernia repair. Alcino-Lázaro defended that “the fate of the hernia sac could not remain the operative room’s bucket: it is an autogenous and resistant tissue readily available, and the bigger it is, the better!.” 20
Conclusion
While incisional hernias possess a surgical challenge, the technique devised by Alcino-Lázaro seems to possess high success rates and does not require the use of mesh, which cheapens the surgery without losing the quality of the procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.