
Abstract
Study Design:
Retrospective review.
Objective:
The aim of our study was to quantify the frequency of complications associated with recombinant human bone morphogenetic protein 2 (rhBMP-2) use in anterior lumbar interbody fusion (ALIF).
Methods:
The orthopedic subset of the Medicare database (PearlDiver) was queried for this retrospective cohort study using International Statistical Classification of Diseases 9 (ICD-9) and Current Procedure Terminology (CPT) codes for ALIF procedures with and without rhBMP-2 between 2005 and 2010. Frequencies of complications and reoperations were then identified within 1 year from the index procedure. Complications included reoperations, pulmonary embolus, deep vein thrombosis, myocardial infarction, nerve-related complications, incision and drainage procedures, wound, sepsis, pneumonia, urinary tract infections, respiratory, heterotopic ossification, retrograde ejaculation, radiculopathy, and other medical complications. Odds ratios (ORs) and 95% confidence intervals (CIs) were used to assess the statistical significance.
Results:
We identified a total of 41 865 patients who had an ALIF procedure. A total of 14 384 patients received rhBMP-2 while 27 481 did not. Overall, 6016 (41.8%) complications within 1 year from surgery were noted within the group who received rhBMP-2 and 12 950 (47.1%) complications within 1 year from surgery were recorded in those who did not receive rhBMP-2 (OR = 0.81, CI = 0.77-0.84). Overall, exposure to rhBMP-2 was associated with significantly decreased odds of complications with exception to reoperation rates (0.9% rhBMP-2 vs 1.0% no rhBMP-2; OR = 0.88, CI = 0.71-1.09) and radiculopathy (4.4% rhBMP-2 vs 4.3% no rhBMP-2; OR = 1.02, CI = 0.93-1.13).
Conclusions:
The use of rhBMP-2 in patients undergoing ALIF procedure was associated with a significantly decreased rate of complications. Further studies are needed to elucidate a true incidence of complication.
Introduction
In recent years, recombinant human bone morphogenetic protein 2 (rhBMP-2) has come under scrutiny given the concerns for serious complications. rhBMP-2 was approved in 2002 by the Food and Drug Administration (FDA) for single-level anterior lumbar interbody fusions (ALIFs) within a lumbar tapered titanium cage as an iliac crest bone graft substitute. These first reports detailed excellent fusion rates and shorter hospital stays, 1,2 and as such, rhBMP-2 saw over 4-fold expansion between 2003 and 2007, with 85% of procedures using it in an off-label fashion. 3 Yet rhBMP-2 off-label use caused an increasing stream of reported complications in the cervical spine, and in 2008, the FDA issued a statement regarding the complications and use of rhBMP-2 in an off-label manner. In part, this matter added concern for the use of rhBMP-2 as a substitute for autogenous bone graft in its approved manner.
With regard to ALIFs, despite a 91% fusion rate at 6-year follow up, 4 rhBMP-2 use has been associated with osteolysis, graft subsidence, retrograde ejaculation, urological complications, and delayed infection. 5,6 Furthermore, 2 meta-analyses further challenged the benefits of rhBMP-2 and called attention to misrepresentation of previously published studies on positive outcomes of rhBMP-2. 7,8 More recent studies have refuted these associated complications, citing the underpowered nature of previous reports. 9 –13 Using a large insurance database, we sought to compare the complication rates in patients receiving rhBMP-2 for ALIF to those without rhBMP-2. We hypothesize that the complication rate will not be significantly different between the 2 groups.
Materials and Methods
The PearlDiver Patient Record Database (PearlDiver Technologies Inc, Warsaw, IN; www.pearldiverinc.com) is a national insurance database consisting of Medicare and multiple private insurance agencies. For the purpose of our study, the orthopedic subset of the Medicare database was queried using ICD-9 (International Statistical Classification of Diseases 9) and/or Current Procedural Terminology (CPT) codes between 2005 and 2010 to identify patients who underwent an ALIF procedure (Table 1). After identifying the correct fusion procedure, we identified those patients who had rhBMP-2 (ICD-9 84.52) utilized at the time of surgery, thus creating 2 groups for comparison. The specific complications were then identified within 1 year from surgery. Reoperations were defined as a repeat spinal fusion procedure within 1 year from index surgery. Due to the nature of this retrospective study, specific level of fusion could not be verified.
ICD-9 and CPT Codes.
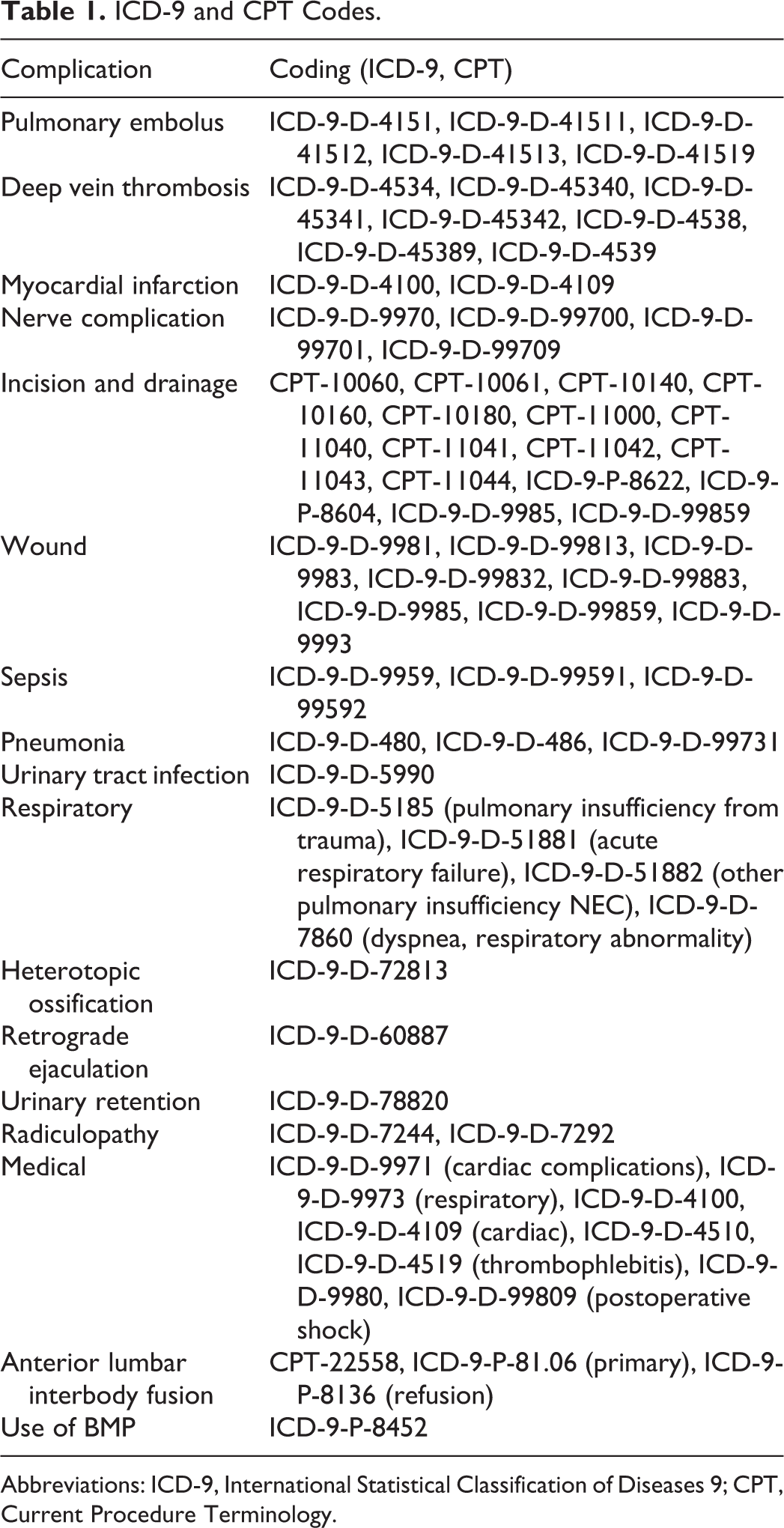
Abbreviations: ICD-9, International Statistical Classification of Diseases 9; CPT, Current Procedure Terminology.
We differentiated incision and drainage (I&D) from reoperations, as we wanted to indirectly measure surgeries performed for a lack of fusion. The frequency of complications in ALIFs using rhBMP-2 was compared to that of ALIFs performed without rhBMP-2. Complications identified included pulmonary embolism, deep vein thrombosis, myocardial infarction, nerve-related, wound-related, pneumonia, sepsis, urinary tract infection, respiratory, heterotopic ossification, retrograde ejaculation, urinary retention, radiculopathy, and other medical complications (Table 1). Demographically, we were able to obtain age ranges and gender.
For statistical analysis, odds ratios (ORs) and 95% confidence intervals (CIs) were generated from these comparisons. Unadjusted ORs were calculated to compare the relative odds of the occurrence of complications given exposure to rhBMP-2. CIs (95%) were used to assess the precision of the OR, with statistical significance defined as an OR not overlapping the null value (eg, OR = 1). Stata statistical software (StataCorp LP College Station, TX) was used to perform analyses.
Results
Demographics
Our query of the Medicare database yielded 41 865 patients who underwent an ALIF procedure between 2005 and 2010. Of this subset of patients, 27 481 did not have rhBMP-2 utilized, while 14 384 received rhBMP-2. Demographically, both cohorts showed similar patient profiles in terms of age and gender (Tables 2 and 3). From patients who received rhBMP-2, 36.9% were males and 61.5% females. The absolute number per year in each category (gender and use of rhBMP-2) increased. Of those not receiving rhBMP-2, 38.3% were males and 60.5% were females (Table 2). With regard to age, 65.7% of patients who underwent ALIF with rhBMP-2 were 69 years of age and younger, as compared to 62.2% without rhBMP-2 in the same age group (Table 3).
Total and Yearly Gender Breakdown for ALIF Procedures With and Without rhBMP-2.
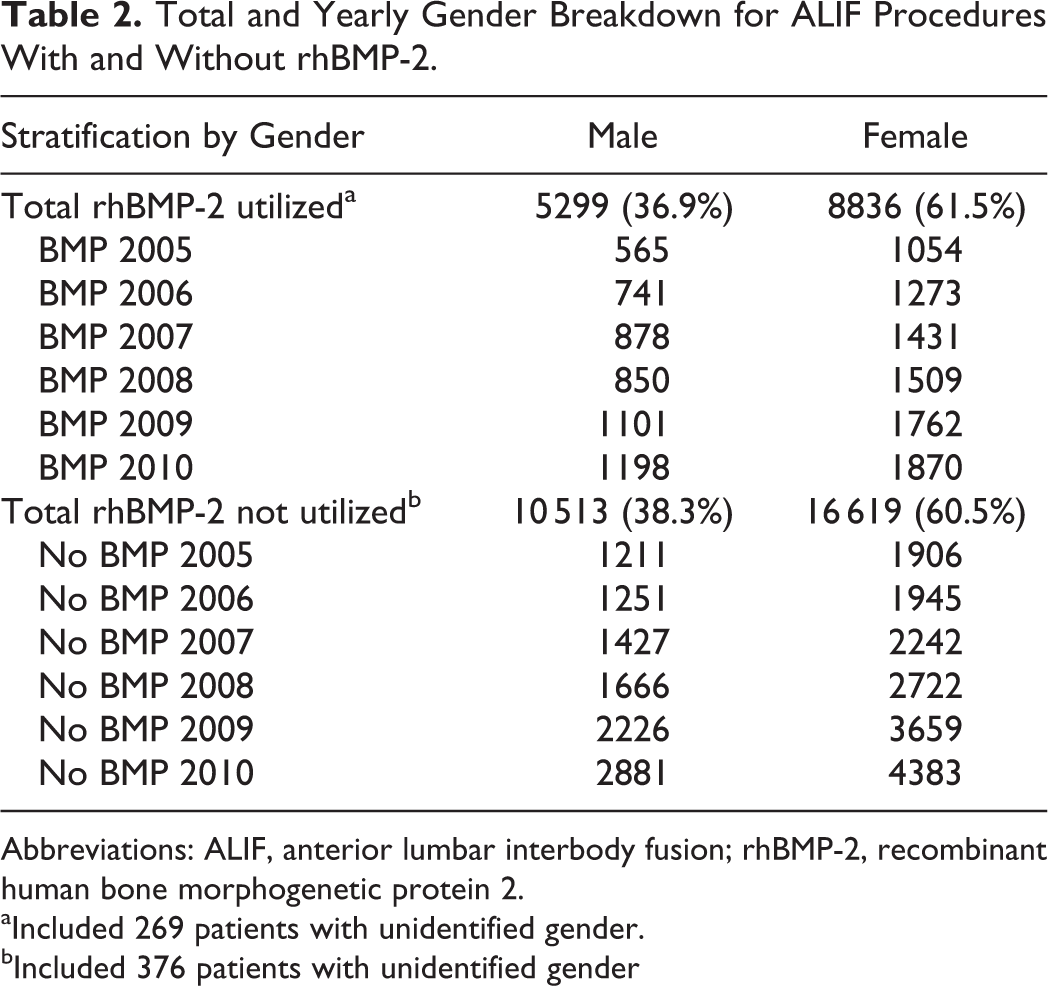
Abbreviations: ALIF, anterior lumbar interbody fusion; rhBMP-2, recombinant human bone morphogenetic protein 2.
aIncluded 269 patients with unidentified gender.
bIncluded 376 patients with unidentified gender
ALIF Procedures With and Without rhBMP2 Stratification by Age.
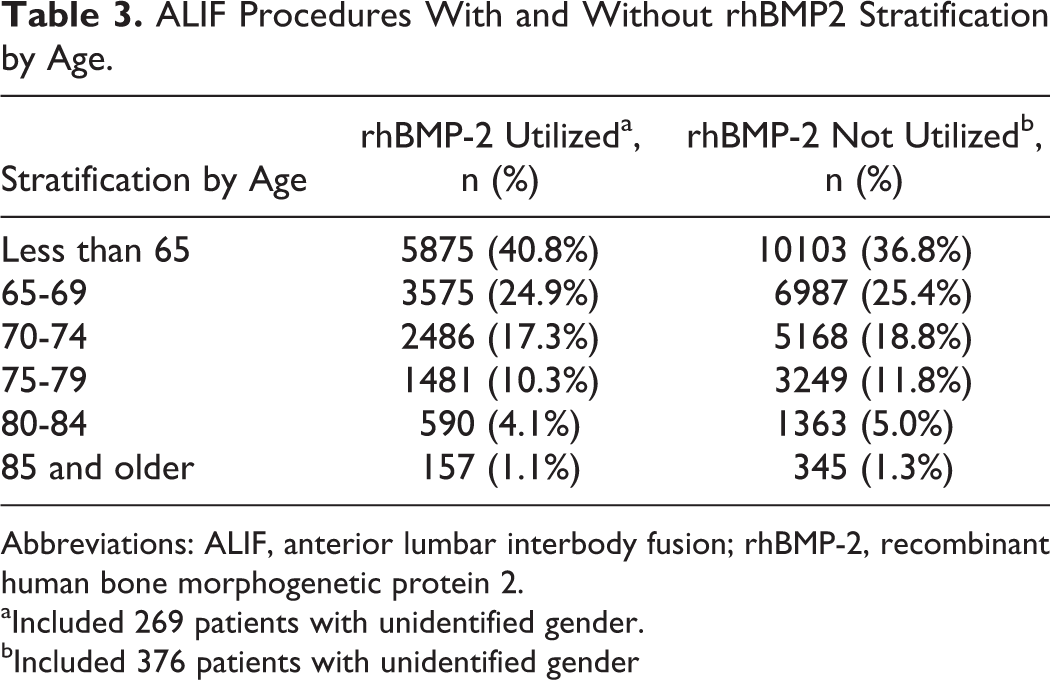
Abbreviations: ALIF, anterior lumbar interbody fusion; rhBMP-2, recombinant human bone morphogenetic protein 2.
aIncluded 269 patients with unidentified gender.
bIncluded 376 patients with unidentified gender
Complications
Overall, from the 41 865 ALIF procedures performed, there were 18 966 reported complications (Table 4). When comparing total complications between the groups at 1 year after surgery, exposure to rhBMP-2 exhibited a statistically significant lower complication rate of 41.8% versus 47.1% complication rate in the group with no rhBMP-2 (OR = 0.1, CI = 0.09-0.11). Prior studies have reported complication rates from roughly 20% to 40% in anterior fusion surgeries. The most common complications were urinary tract infections, wound-related issues, and respiratory complications. Overall, rhBMP-2 was associated with a significantly decreased rate of complications at 1 year after the index procedure (Table 4). The number of wound-related complications was significantly (OR = 0.83, CI = 0.79-0.88) lower in the rhBMP-2 group (1486, 10.3%) when compared to the no-rhBMP-2 group (3854, 14%). Urinary tract infections were also significantly lower (OR = 0.83, CI = 0.79-0.88), with a rate of 16.7% in rhBMP-2 patients and 19.4% in patients that did not receive rhBMP-2 (Table 4). Similarly, significant differences were observed for several other major complications such as deep vein thrombosis (3.9% rhBMP-2 vs 5.6% no-rhBMP-2), respiratory (9.0% rhBMP-2 vs 11.7% no-rhBMP-2), I&D (6.8% rhBMP-2 vs 9.7% no-rhBMP-2; Table 4).
List and Frequency of Complications.
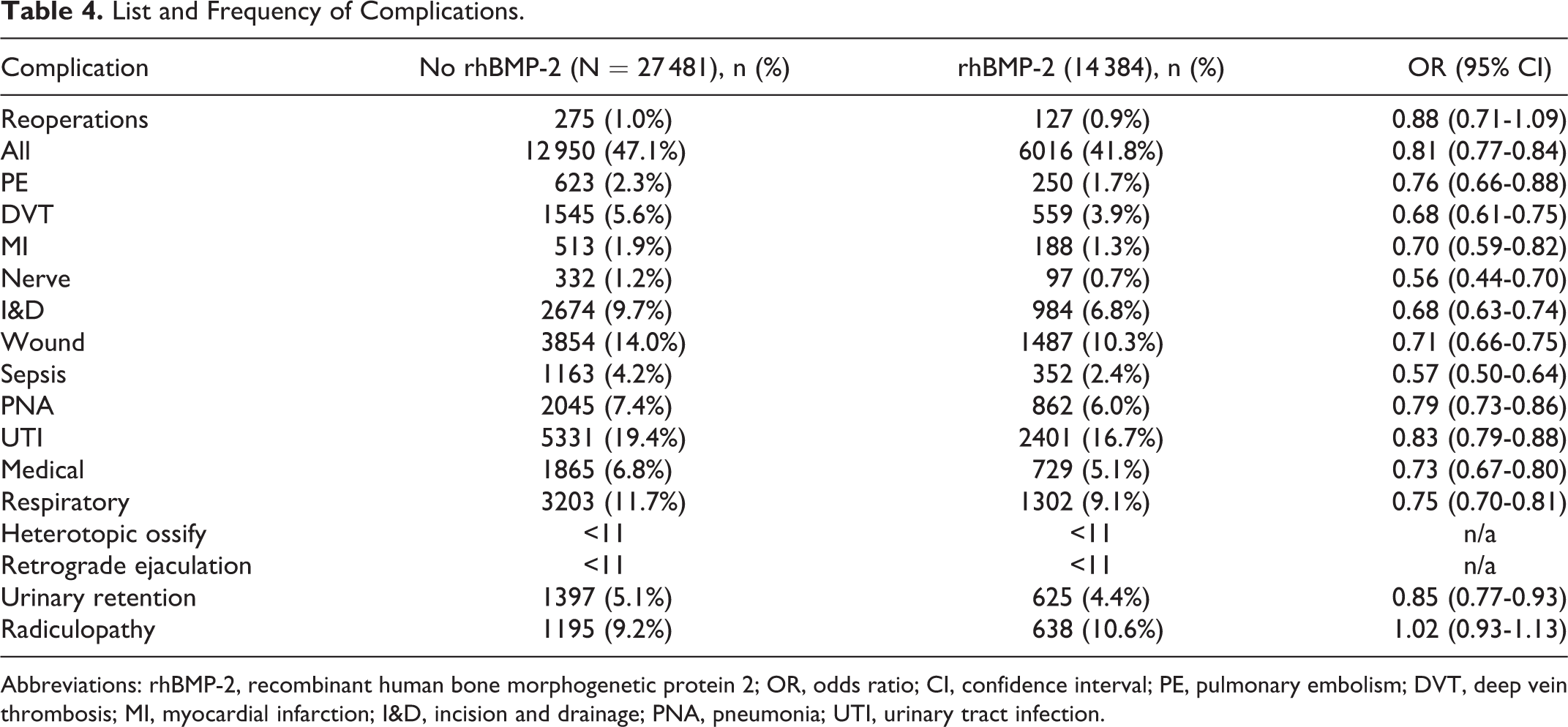
Abbreviations: rhBMP-2, recombinant human bone morphogenetic protein 2; OR, odds ratio; CI, confidence interval; PE, pulmonary embolism; DVT, deep vein thrombosis; MI, myocardial infarction; I&D, incision and drainage; PNA, pneumonia; UTI, urinary tract infection.
Complications that were present at a similar rate in both groups were reoperation (0.9% rhBMP-2 vs 1.0% no rhBMP-2; OR = 0.88, CI = 0.71-1.09) and radiculopathy (4.4% rhBMP-2 vs 4.3% no rhBMP-2; OR = 1.02, CI = 0.93-1.13). In our study, the number of patients with heterotopic ossification or retrograde ejaculation was <11 in both groups. Due to the PearlDiver suppression policy, we were unable to calculate the incidences for those complications.
Discussion
Our study demonstrated that the use of rhBMP-2 in ALIF procedures was not associated with an increased frequency of complications when compared to ALIF procedures without rhBMP-2.
In 2002, rhBMP-2 was approved by the FDA as a substitute for autologous bone in anterior interbody spine fusion. The impetus of this limited approval was based in part on the study by Burkus et al, who showed similar outcomes at 2 years in the patients who received rhBMP-2 and a tapered titanium fusion cage versus those who received autogenous iliac crest bone graft. 1,2 With the morbidity of iliac crest bone graft ranging from 6% to 40%, 14 –17 rhBMP-2 was praised as a means to achieve solid fusion while avoiding harvesting complications. However, since 2002, several authors have reported complications with its use as well as concerns with regard to the cost and benefit in spine surgery. 4,18 –20 Controversy related to the “off-label” use of rhBMP-2 as well as apprehensions of underreporting caused several to question its necessity in ALIF. Carragee and coworkers reported several complications associated with the use of rhBMP-2 in ALIF. 5,6 However, in our retrospective study patients who received rhBMP-2 had a significantly lower incidence of complications compared to patients who underwent ALIF procedures without rhBMP-2.
With respect to age and gender, our results are consistent with a previous database study. 18 Interestingly, at 1 year postoperatively, we showed with statistical significance that total complications in the group exposed to rhBMP-2 were less frequent than in the no-rhBMP-2 cohort. In contrast, Cahill et al 18 found a 6.97% overall complication rate when rhBMP-2 was used in lumbar fusion, and it was not significantly different from those who did not receive rhBMP-2. Additionally, in their extensive analysis, they showed that the complications were significantly more frequent with increase in age, Charlson comorbidity score, and nondegenerative and nonelective diagnosis and revision fusions. This is an important finding because it highlights the importance of choosing the right patient for the treatment. In addition, our data did not show an increased rate of retrograde ejaculation and urogenital complications in the rhBMP-2 group. On the other hand, Fu et al found that rhBMP-2 was associated with nonsignificantly increased risk of those complications with anterior lumbar interbody fusion. 7
While our results showed a decreased rate of complication with rhBMP-2, the frequency of our total complications was much higher than previously reported. 1,18,21 This is likely due to the following: (1) in an attempt to capture as many complications within 1 year, many of the complications identified by ICD-9 were likely not directly related to index surgery and (2) the fact that the authors in previous studies only included complications reported during the postoperative inpatient hospitalization, whereas we attempted to capture complications up to 1 year from the index procedure. Our total complication in both groups, rhBMP-2 and no-rhBMP-2, suggests the presence of other factors, such as overall medical health, are likely contributing to the inappropriately high amount of complications at 1 year.
The differences between the rhBMP-2 and no-rhBMP-2 groups in reoperation rate did trend toward decreased odds of reoperation in those exposed to rhBMP-2. As previously noted, we defined reoperation as a repeat lumbar fusion surgery within 1 year, thus not including incision and drainage/irrigation and debridement. However, we did look separately at I&Ds and wound-related complication and found that the cohort who received rhBMP-2 had decreased odds of such complications.
Based on the recent rhBMP-2 literature, other notable complications that we attempted to study were infection, wound complications, nerve-related complications, radiculopathy, retrograde ejaculation, heterotopic ossification, and generalized postoperative complications. Previous studies have reported wound and infection complications in lumbar fusion with rhBMP-2 to range between 2% and 17%. 18,22 –25 While our data did show a statistically significant lower frequency of those complications in the rhBMP-2 group, we found the rate of wound and infection complications to be 10.3%, which is within the reported rate seen in previous studies.
Postoperative radiculitis has also been reported in conjunction with rhBMP-2 use. Mindea et al evaluated the incidence of postoperative radiculitis after minimally invasive transforaminal lumbar interbody fusion and found that 11% of patients from the rhBMP-2 group developed symptoms of radiculitis on the fused side. 26 In our analysis, we did not find any difference in radiculopathy rates between the 2 groups. Separately, nerve-related complication rates were lower in patients exposed to rhBMP-2 (0.7% vs 1.2%, respectively). It is important to note that nerve-related complications have been previously reported in cases in which transforaminal lumbar interbody fusion or posterior lumbar interbody fusion were performed. 26 It is hypothesized that the physical proximity of rhBMP-2 to the neural structures and the potential to induce an inflammatory reaction or ectopic bone formation are the genesis of postoperative nerve-related complications, and thus, rhBMP-2 in ALIF is situated further away from the neural elements possibly explaining why the nerve-related complications are seen at a lesser frequency.
Retrograde ejaculation (RE) in association with rhBMP-2 has received particular attention in recent years. 27 In a retrospective analysis, the authors confirmed a higher rate of retrograde ejaculation associated with rhBMP-2. Our query did not yield enough incidences of RE in ALIF procedures to report per PearlDiver policy. This could very well be a failure of providers to report such incidence as RE may be a less concerning complication in the Medicare population. It is worth noting that previously reported RE complications related to ALIF procedures 28 –31 relied on questionnaire reporting of less or lack of ejaculate fluid. However, a recent study that used quantitative pre- and postoperative semen urine analysis found that the rates of RE were not significantly different between the rhBMP-2 and no-rhBMP-2 groups. 11
There were several limitations to our study. This was a retrospective study of a large database searched by ICD-9 and CPT codes and it is subject to failure in reporting specific complications. The use of the PearlDiver database does not allow for past medical history or clinical and radiographic outcomes to be reviewed. This limitation excluded the ability to perform multivariate analysis to account for any confounding variables between the groups, and as such, there was a high rate of complications noted. While lack of other medical history limits our ability to better discern such differences that may exist, the total complications after surgery seen in patients exposed to rhBMP-2 may be related to improved functional outcomes. Furthermore, we were unable to analyze other important factors such as rhBMP-2 dosing and very specific complications, such as subsidence, cage migration, and antibody formation. As an indirect way to measure this, we attempted to examine reoperation rates at 1 year. Additional limitations attributable to the use of a large database were that we did not have the ability to differentiate ALIFs from eXtreme Lateral Interbody Fusion (XLIFs)/Direct Lateral Interbody Fusion (DLIFs)/oblique lumbar interbody fusion (OLIFs) as they all have a common CPT code, and that there is the potential for input errors with regard to coding of procedures.
Despite these limitations, we believe that our study provides additional support to the notion that the rate of complications associated with rhBMP-2 use in ALIF is no different than ALIFs performed without rhBMP-2. Imperative in the future of biologics are further studies focusing on the mechanism of complications, optimal dosing, and long-term outcomes. The use of rhBMP-2 should be weighed thoughtfully and the surgeon should have a detailed discussion with patient with regard to the risks and benefits of its use.
Footnotes
Acknowledgments
AOSpine is a clinical division of the AO Foundation—an independent medically guided nonprofit organization. The AOSpine Knowledge Forums are pathology focused working groups acting on behalf of AOSpine in their domain of scientific expertise. Each forum consists of a steering committee of up to 10 international spine experts who meet on a regular basis to discuss research, assess the best evidence for current practices, and formulate clinical trials to advance spine care worldwide. Study support is provided directly through AOSpine’s Research Department.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Financial activities outside of this work: Kevork Hindoyan, Justin Tilan, Jong-Beom Park—nothing to disclose. Zorica Buser—Xenco Medical (consultancy), AO Spine (consultancy, past). Darrel S. Brodke—Consultant – Vallum, Royalties – America, DePuy Synthes, Medtronic, Fellowship Support – AOSpine (paid directly to institution). Hans-Joerg Meisel—Dr Meisel is consultant (money paid to institution) – Regenerate Life Sciences GmbH for Zyga, DiFusion (ongoing), Co.don (paid to Dr. Meisel past); royalties from: Medtronic, Fehling Aesculap (past); owns stocks (money paid to institution) – Regenerate Life Sciences GmbH in DiFusion. S. Tim Yoon—Dr Yoon owns stock in Phygen, Alphatec; Meditech, royalties Meditech Advisors, Stryker Spine (Paid directly to institution/employer), grant from AOSpine (Paid directly to institution/employer), research support from Biomet (Research support given to AREF), nonfinancial research support from Nuvasive and Medtronic. Jim A. Youssef—Royalties: NuVasive, Osprey Medical, Amedica, Integra; Stock Ownership: Benvenue Medical, Paradigm Spine, Promethean Surgical Devices, Spinal Ventures, VertiFlex, Spinicity, ISD, Providence Medical; Private Investments: Amedica, VertiFlex, Benvenue, NuVasive; Consulting: Integra, NuVasive, Amedica, HealthTrust; Board of Directors: Durango Orthopedic Associates (None); Research Support (Staff and/or Materials): Globus Medical (Paid directly to institution/employer), NuVasive (Paid directly to institution/employer), VertiFlex (Paid directly to institution/employer), Integra (Paid directly to institution/employer). Jeffrey C. Wang—Royalties: Aesculap, Biomet, Amedica, Seaspine , Synthes ; Stock Ownership: Fziomed; Private Investments: Promethean Spine, Paradigm spine, Benevenue, NexGen, Vertiflex, electrocore, surgitech, expanding orthopaedics, osprey, bone biologics, curative biosciences, pearldiver; Board of Directors: North American Spine Society (nonfinancial, reimbursement for travel for board meetings, courses, etc.), North American Spine Foundation (nonfinancial), Cervical Spine Research Society (nonfinancial, reimbursement for travel for board meetings), AO Spine/AO Foundation (honorariums for board position); Fellowship Support: AO Foundation (spine fellowship funding paid to institution).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by AOSpine and departmental funds.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.