
Abstract
Study Design
Systematic Review and Meta-Analysis.
Objectives
We analyzed patient-reported outcomes (PROs) focused on axial neck pain following cervical laminoplasty (CL) and foraminotomy (CF) for symptomatic cervical spondylosis to determine whether motion-preserving procedures targeting compressive radiculopathy/myelopathy also provide relief of axial neck pain and to investigate risk factors for persistent postoperative axial neck pain.
Methods
The PubMed and Cochrane Library databases were systematically searched for articles published from 2014 to 2023 describing pain-related outcomes following CL and CF. Data regarding PROs, reoperation rates, and risk factors for postoperative axial neck pain were also collected.
Results
Thirty studies met inclusion criteria for analysis. There were 2499 cases (2129 CL and 370 CF) with mean ages of 63.2 and 59.3 years for CL and CF, respectively. CL patients had improved mean postoperative visual analogue scale and neck disability index (NDI) scores compared to preoperative values, with mean differences of −1.97 (CI -2.52, −1.42; P < 0.0001) and −12.27 (CI −15.01, −9.54; P < 0.0001), respectively. CF patients had improved mean postoperative NDI scores compared to preoperative values, with mean difference of −15.15 (CI −23.79, −6.50; P = 0.0064). Presence of anterolisthesis, loss of cervical muscle volume, diabetes, age, and regional malalignment are independent predictors of postoperative axial neck pain.
Conclusions
Motion-sparing cervical decompressive surgery performed for compressive radiculopathy or myelopathy can also provide significant relief of axial neck pain, suggesting that preoperative axial neck pain is not an absolute contraindication to non-fusion decompressive surgery for degenerative cervical pathologies.
Keywords
Introduction
Cervical laminoplasty (CL) and cervical foraminotomy (CF) are common motion-preserving surgical approaches utilized for the treatment of degenerative cervical spondylotic myelopathy (CSM) and radiculopathy, respectively. CL was first described in the 1970s as an alternative to classic decompressive laminectomies, offering preservation of posterior muscular and ligamentous attachments in order to mitigate risks of post-laminectomy kyphotic deformity.1,2 CF is an alternative to anterior fusion-based procedures, such as anterior cervical decompression and fusion (ACDF), for foraminal decompression in cervical radiculopathy, and is being utilized in cervical radiculopathy foraminal disc herniation or stenosis, without fusion. 3
Since approximately 40-80% of patients with cervical myelopathy or radiculopathy endorse axial neck pain preoperatively 4 and axial neck pain is also frequently encountered following CL and CF,5,6 there is substantial controversy regarding whether preoperative axial neck pain constitutes a contraindication to motion-preserving procedures (CL and CF), and the degree to which neck pain may be alleviated or exacerbated by these approaches.7,8
The purpose of this systematic review and meta-analysis was to analyze patient-reported outcomes following cervical laminoplasty and cervical foraminotomy, in order to determine the impact of motion-preserving procedures on axial neck pain. We further investigated risk factors for the persistence of axial neck pain postoperatively following these procedures.
Methods
Inclusion Criteria and Search Strategy
We conducted a systematic search of the PubMed (NLM) and Cochrane Library (Wiley) databases in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines (Figure 1). The search focused on literature discussing axial neck pain following cervical laminoplasty and foraminotomy. The results were reviewed and independently evaluated by two reviewers. Inclusion criteria were (1) publication between January 1, 2014 and December 31, 2023, (2) English language publications, (3) inclusion of axial neck pain outcomes on at least one timepoint after cervical laminoplasty and/or foraminotomy procedures, and (4) a formal discussion or analysis of preoperative and postoperative patient-reported outcomes (PROs) related to axial neck pain secondary to these procedures. Exclusion criteria were review articles, editorials, basic science studies, and studies that failed to include preoperative PROs or mean PROs with standard deviations. PRISMA flow diagram and inclusion results.
An initial search of the PubMed and Cochrane Library databases was performed using the following search terms: “cervical foraminotomy,” “cervical laminoplasty,” “axial neck pain,” “((“Foraminotomy” [Mesh]) AND (“Neck Pain” [Mesh])),” “((“Laminoplasty” [Mesh]) AND (“Neck Pain” [Mesh])),” “(“Foraminotomy” AND “Neck Pain”),” and “(“Laminoplasty” AND “Neck Pain”).” An analysis of keywords contained in article titles, abstracts, and indexed terms was conducted to identify eligible studies. Additionally, the references of eligible studies were checked to identify additional sources beyond those that were found in our initial search. All screening was conducted independently by two reviewers (A.H.K. and J.P.A.), and differences were resolved by group discussion, with final adjudication by two additional authors (M.G. and S.H.L.).
Risk of Bias Assessment
Two independent reviewers critically assessed the risk of bias for each included study using the Cochrane Risk of Bias Tool for randomized controlled trials (Supplemental Table S1) and the Newcastle-Ottawa Scale for non-randomized, cohort studies (Supplemental Table S2). The domains appraised in randomized controlled trials include selection, performance, detection, attrition, reporting, and other sources of bias. For cohort studies, eight items categorized into three dimensions, including selection, comparability, and outcome were examined. Studies with total scores greater than 6 points were considered high quality and those with total scores less than 4 points were considered low quality. A third reviewer served as an arbitrator to resolve disagreements between the primary reviewers.
Data Extraction
When available, data regarding PROs including primary outcomes (Numerical Rating Scale (NRS) and Visual Analogue Scale (VAS)), and secondary outcomes (Nurick Scale, Japanese Orthopaedic Association (JOA) Scores, Neck Disability Index (NDI), EQ-5D, the 36-Item Short Form Health Survey (SF-36), and reoperation rates) were collected alongside identified risk factors for postoperative axial neck pain. Study characteristics, including journal, year of publication, sample size, mean age (years), and mean follow-up period (months) were also collected. When studies included multiple comparison groups, data was separated into their respective cohorts. Data regarding fusion-based procedures or cervical disc arthroplasty were excluded from our analysis.
Statistical Analysis
Assuming that primary and secondary outcomes were independent of each other across each procedure, we calculated the pooled mean effect size separately using random-effects models. We employed random-effects models due to the assumption of diverse effect sizes across studies, reflecting variations in study design and population characteristics. For all comparisons, we reported the mean difference and 95% confidence interval (CI). Studies were aggregated using inverse-variance weighting. The DerSimonian-Laird estimator was used to assess for between-study variance and the Jackson method was used to calculate confidence intervals of Τ2. Hartung-Knapp adjustment was applied to correct for overestimation. Heterogeneity between studies was estimated using the I2 test. An I2 value of <25% was categorized as low, 25-50% as moderate, and >50% as high heterogeneity. Significance was set at a P value <0.05. Funnel plots were used to assess for small study effects. 9 All statistical analyses were conducted independently by two authors (A.H.K. and C.H.P.). Statistical analyses were performed using R version 4.2.3, with the meta package utilized for the meta-analysis.
Results
Study Characteristics
Characteristics of Included Studies.
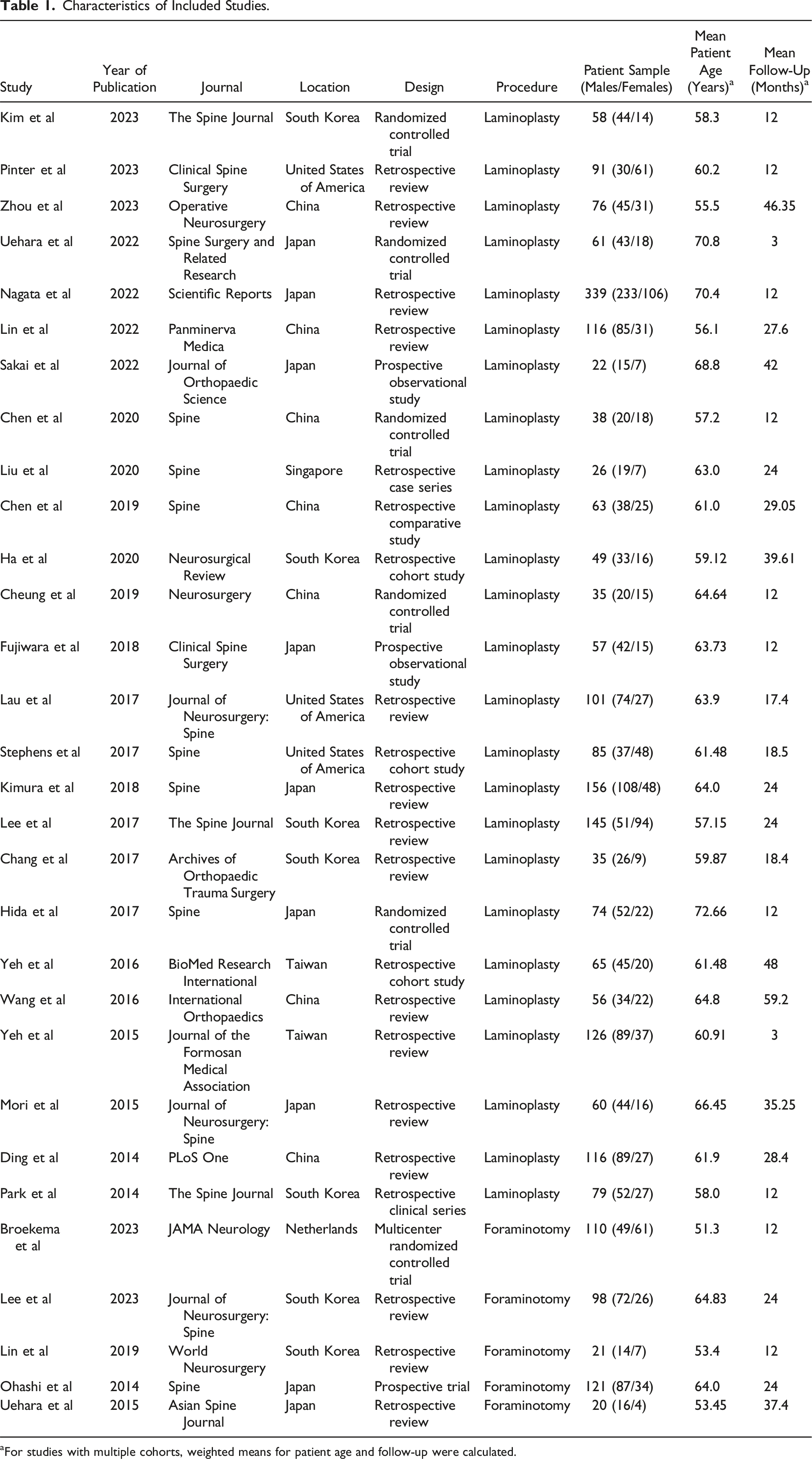
aFor studies with multiple cohorts, weighted means for patient age and follow-up were calculated.
Patient Demographics
A total of 2499 surgical procedures were performed, including 2129 CL and 370 CF (Table 1). Women comprised 35.74% (761/2129) of the laminoplasty cohort and 35.68% (132/370) of the foraminotomy cohort. Patients undergoing CL and CF had mean ages of 63.16 ± 5.13 and 59.27 ± 6.25 years, respectively. Average follow-up was 21.09 ± 13.01 months and 21.34 ± 9.54 months, respectively.
Patient Reported Outcome Measures
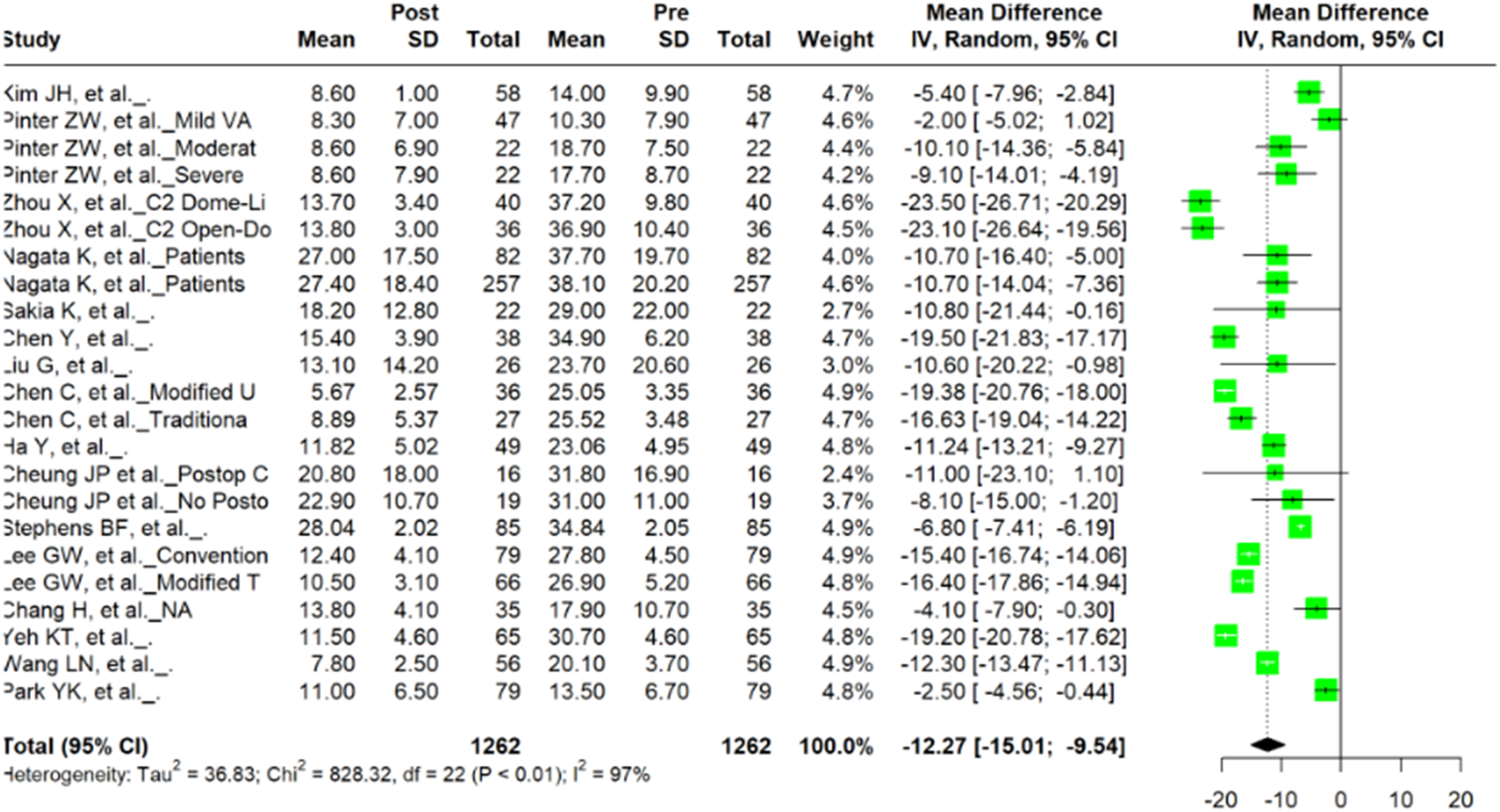
Among the 25 studies examining CL, preoperative and postoperative VAS and NDI were included in 17 and 16 studies, respectively. Meta-analysis of 27 unique cohorts within the 17 studies revealed a significant difference between preoperative and postoperative VAS scores (n = 2286; mean difference = −1.97; 95% CI = −2.52, −1.42; P < 0.0001) (Figure 2). A meta-analysis of 23 unique cohorts within 16 studies that included NDI scores revealed a significant difference between preoperative and postoperative values (n = 2524; mean difference = −12.27; 95% CI = −15.01, −9.54; P < 0.0001) (Figure 3). Forest plot of mean difference and 95% confidence interval for preoperative and postoperative VAS among patients undergoing cervical laminoplasty. Forest plot of mean difference and 95% confidence interval for preoperative and postoperative NDI among patients undergoing cervical laminoplasty.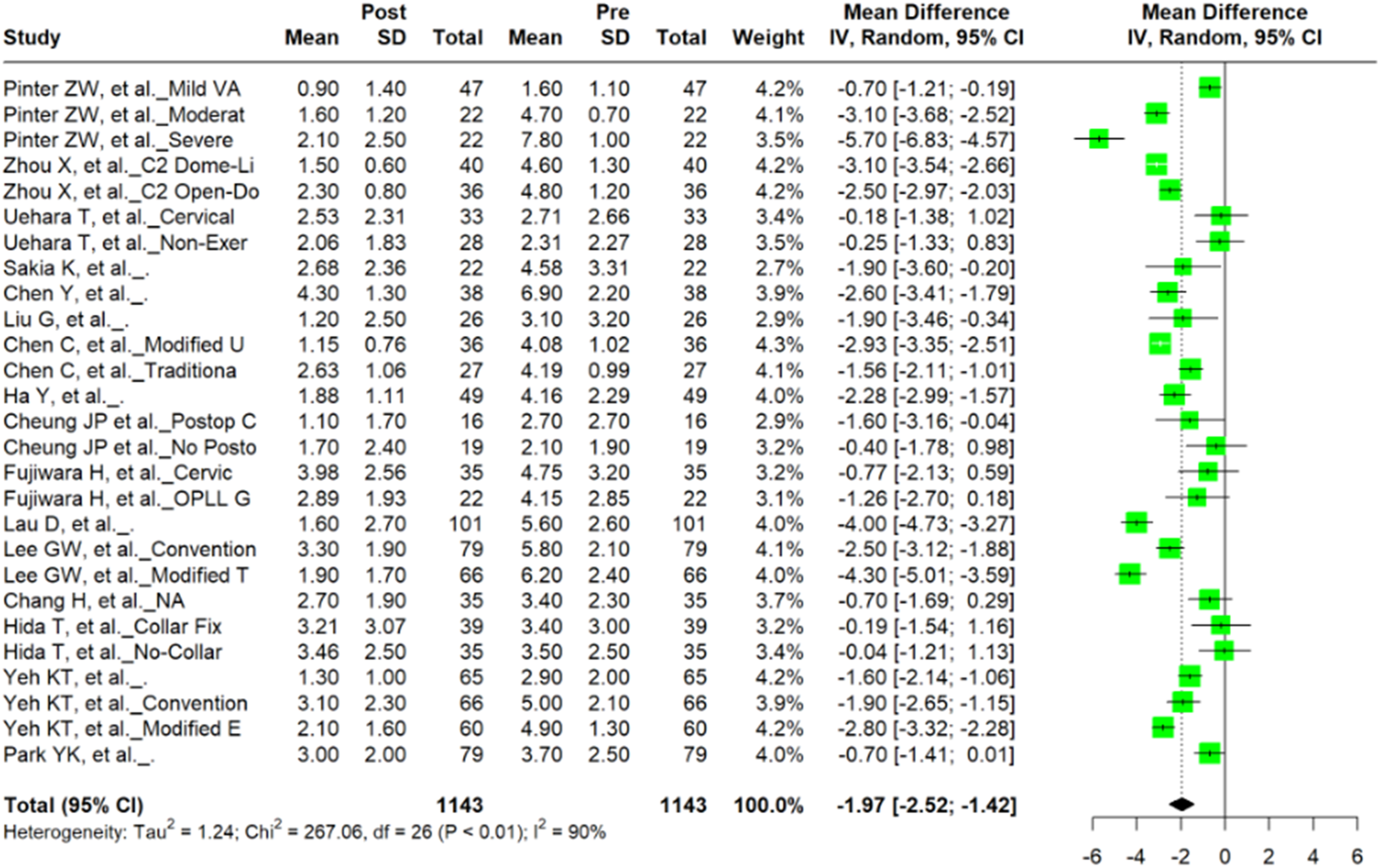
NRS was reported in four studies, Nurick Scale in four studies, JOA in fifteen studies, mJOA in two studies, EQ-5D in two studies, SF-36 MCS in six studies, and SF-36 PCS in seven studies. Meta-analysis of NRS scores revealed a significant difference in preoperative and postoperative values (n = 1290; mean difference = −0.67; 95% CI = −1.07, −0.27; P = 0.0094) with no evidence of heterogeneity (I2 = 5.4%; P = 0.38). Meta-analysis of Nurick Scale scores demonstrated a significant difference when comparing preoperative and postoperative values (n = 636; mean difference = −1.60; 95% CI = −2.44, −0.75; P = 0.0063), but with substantially higher heterogeneity (I2 = 90%; P < 0.01). Pooled data for JOA and mJOA had significant mean differences of 3.89 (n = 2046; 95% CI = 2.99, 4.80; P < 0.0001) and 3.22 (n = 240; 95% CI = 1.61, 4.82; P = 0.013), respectively. Studies including JOA displayed higher degrees of heterogeneity than those describing mJOA (I2 = 96%; P < 0.01 versus I2 = 35%; P = 0.21, respectively). Mean EQ-5D showed a statistically significant difference preoperatively vs postoperatively (n = 794; mean difference = 0.11; 95% CI = 0.043, 0.17; P = 0.019) without heterogeneity (I2 = 14%; P = 0.31). SF-36 MCS and SF-36 PCS also demonstrated significant mean differences of 5.58 (n = 1408; 95% CI = 1.05, 10.11; P = 0.021) and 8.87 (n = 1560; 95% CI = 4.17, 13.57; P = 0.0016) respectively.
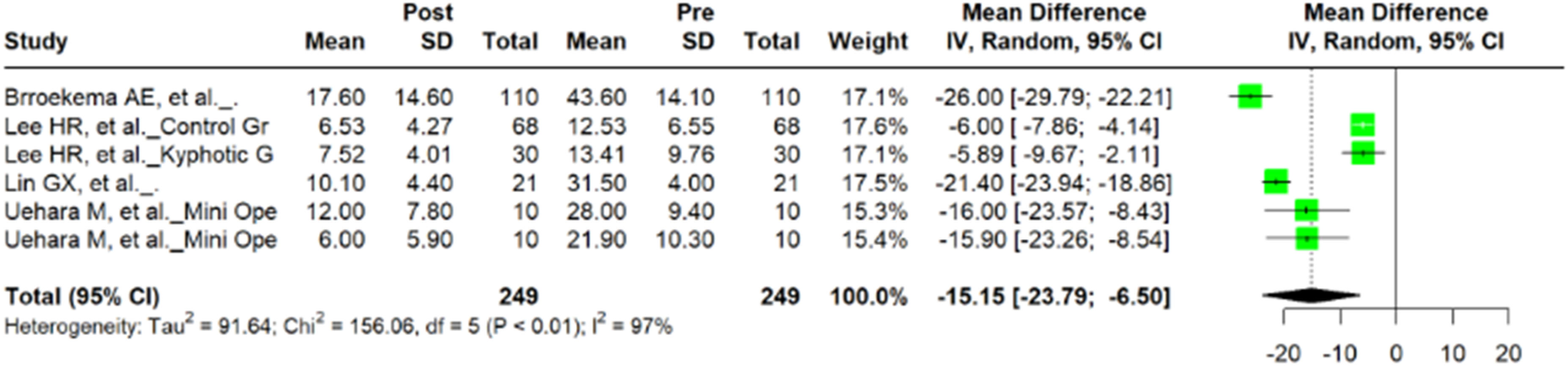
Among the five studies examining CF, five studies included preoperative and postoperative VAS values and four studies included NDI values. Meta-analysis of VAS revealed no significant difference in preoperative and postoperative VAS scores (n = 740; mean difference = −1.65; 95% CI = −3.64, 0.33; P = 0.088) with evidence of heterogeneity (I2 = 94%; P = < 0.01) (Figure 4). Pooled data for NDI demonstrated a significant mean difference in preoperative and postoperative values (n = 498; mean difference = −15.15; 95% CI = −23.79, −6.50; P = 0.0064) with significant heterogeneity (I2 = 97%; P = < 0.01) (Figure 5). Forest plot of mean difference and 95% confidence interval for preoperative and postoperative VAS among patients undergoing cervical foraminotomy. Forest plot of mean difference and 95% confidence interval for preoperative and postoperative NDI among patients undergoing cervical foraminotomy.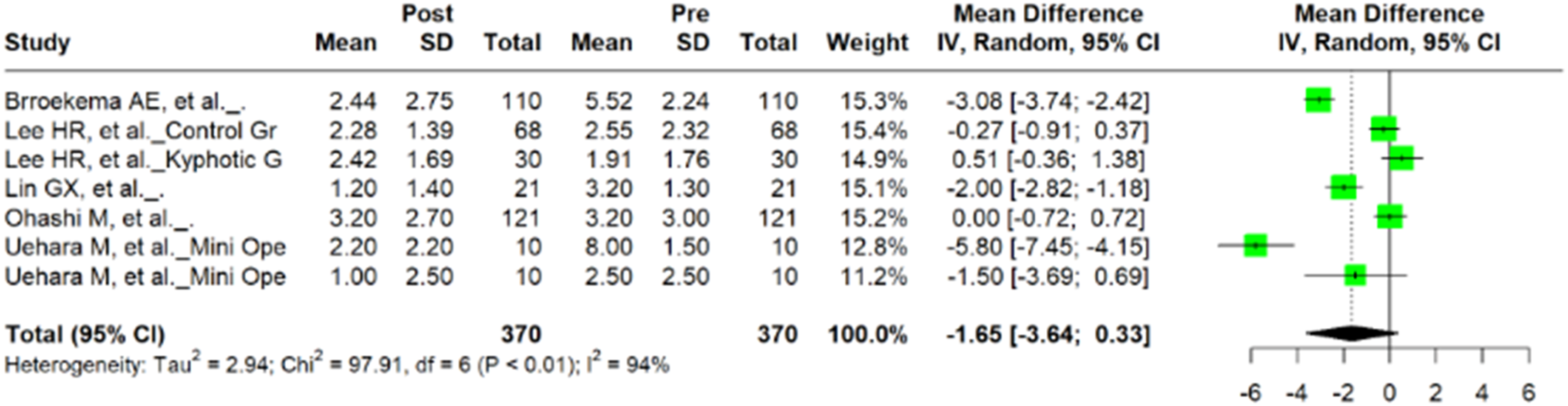
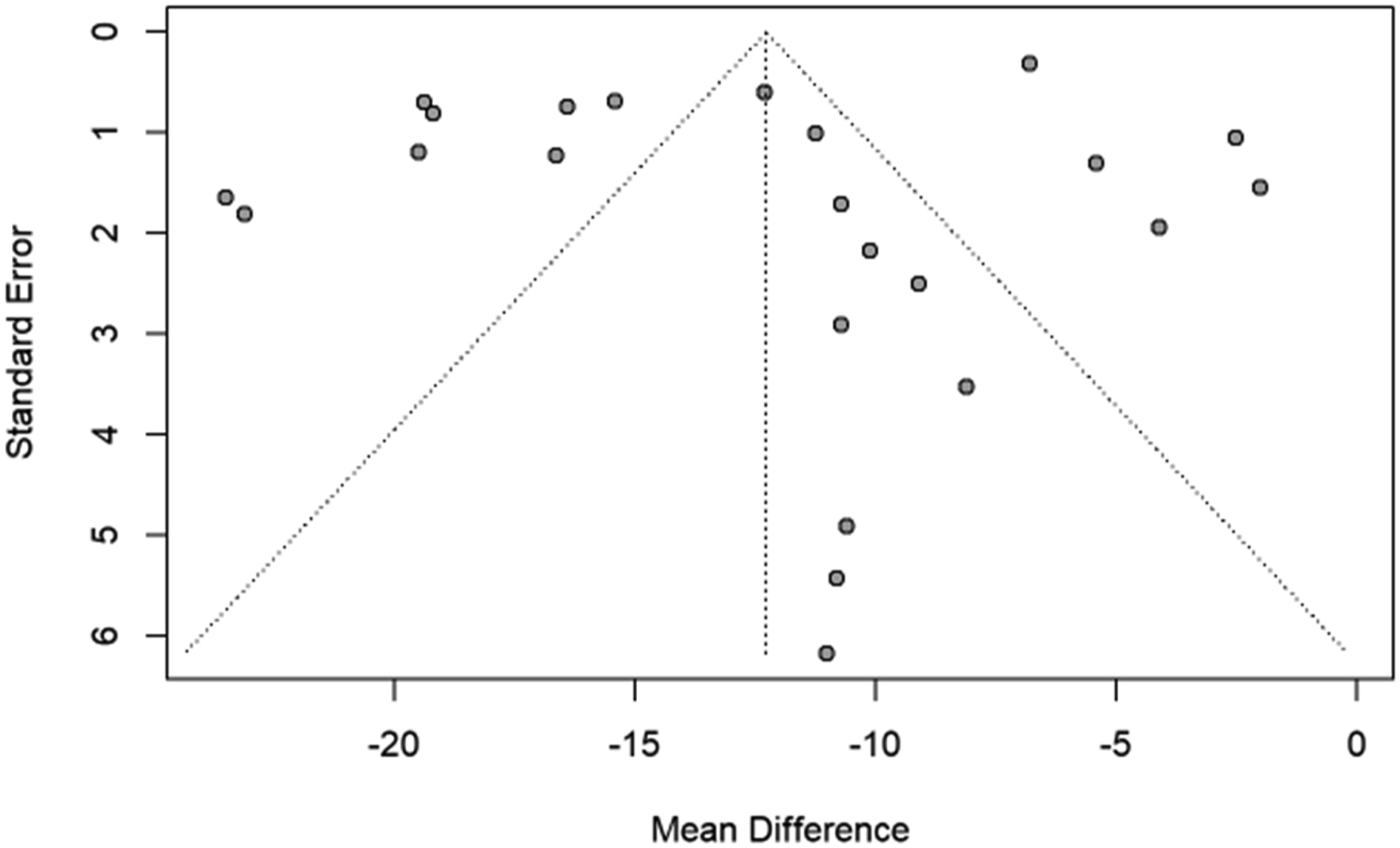
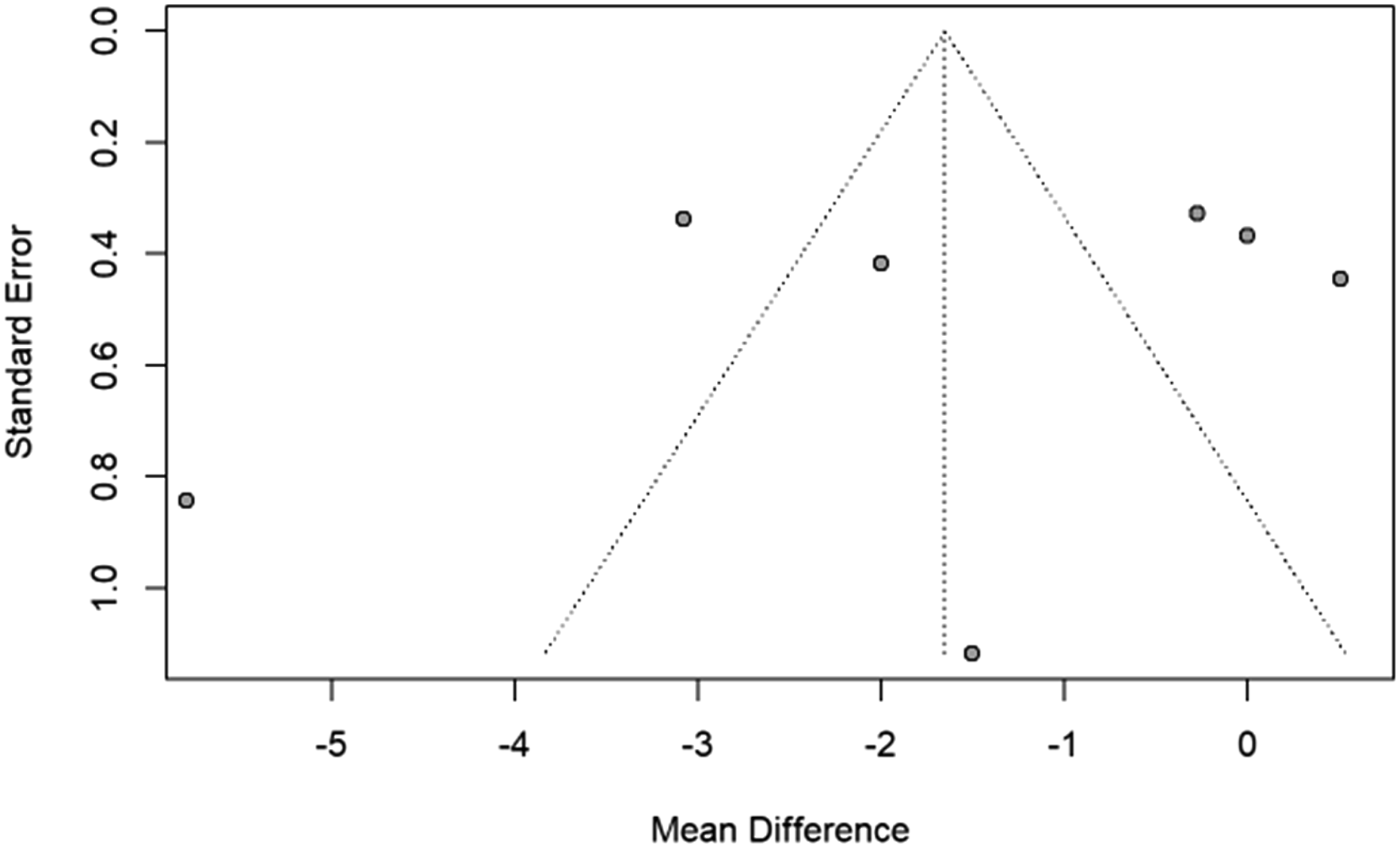
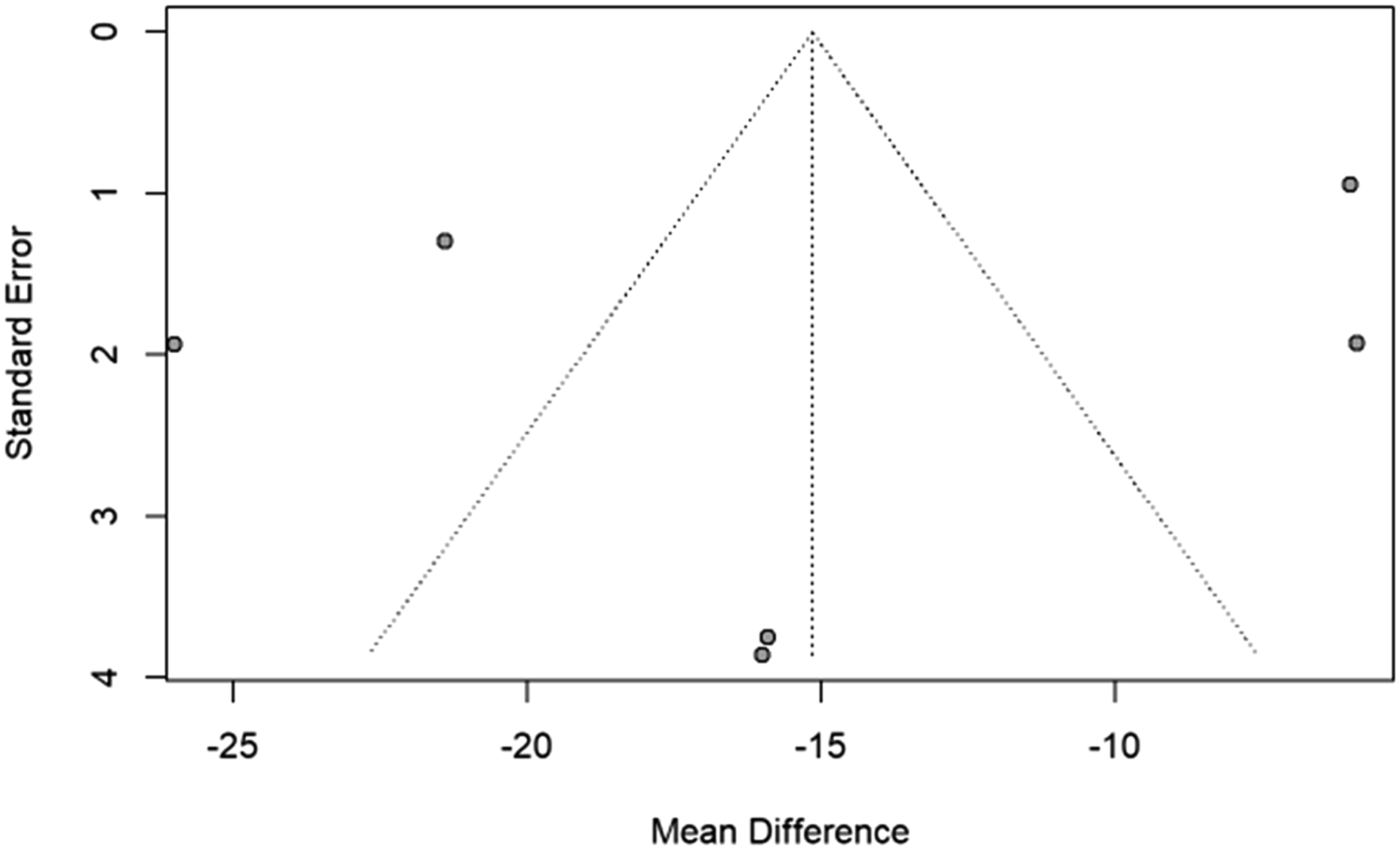
Meta-analysis of additional outcomes in studies examining CF was not performed as variable data was unavailable. Funnel plots are shown in Figures 6-9. Figures 6 and 7 demonstrate an absence of smaller studies with large effects, and Figures 8 and 9 are difficult to interpret due to the limited number of studies available for analysis. Funnel plot for assessment of reporting bias for VAS in laminoplasty studies. Funnel plot for assessment of reporting bias for NDI in laminoplasty studies. Funnel plot for assessment of reporting bias for VAS in foraminotomy studies. Funnel plot for assessment of reporting bias for NDI in foraminotomy studies.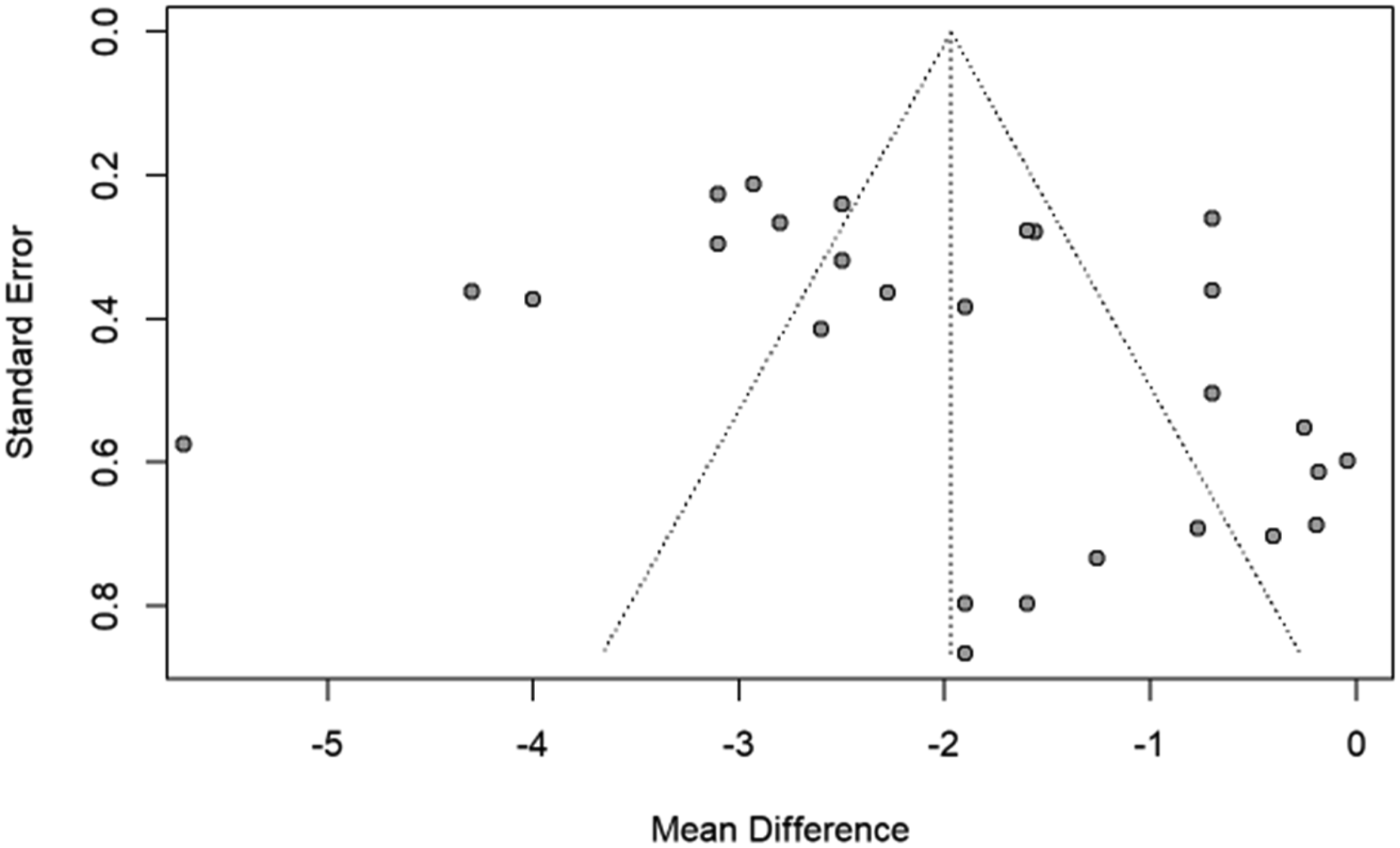
Reoperation Rates
Of the 25 studies examining CL, eight provided reoperation data, with rates varied from 0% to 9.1%.12,18,20,26,30 Chen et al. reported a reoperation rate of 2.78% (1/36), with the one case of revision due to the development of postoperative spinal epidural hematoma. 16 Another study reported a 4.4% reoperation rate, with one patient suffering an adjacent level fracture following a postoperative mechanical fall, one patient experiencing adjacent-segment stenosis, and two patients due to wound infections. 28 Ding et al. observed a reoperation rate of 0.86% (1/116) as one of their patients experienced CSF leakage postoperatively. 27
Two studies provided reoperation rates following CF. Lin et al reported a reoperation rate of 14.3% (3/21), with recurrence of symptoms postoperatively the indication for revision in all three cases. 36 Broekema et al found a reoperation rate of 5.45% (6/110) within their cohort. 34
Risk Factors of Postoperative Axial Neck Pain
Several risk factors were identified as causes of postoperative axial neck pain following CL. Numerous studies have cited dissection of the muscle insertions on the C2 and C7 spinous processes13,14,19,26 and loss of cervical muscle volume10,15,16,29 as contributors for postoperative axial neck pain as muscle preservation maintains both tension and extensor function. Additional risk factors include local kyphosis, 23 duration of postoperative collar use,13,30 posterior bony impingement, 25 laminoplasty hinge fractures, 20 and severe damage to the paraspinal muscles or nuchal ligament.22,33 Studies regarding the association of postoperative axial neck pain and cervical sagittal malalignment are disparate.16,19,24 Kimura et al. reported that the presence of anterolisthesis, higher axial neck pain intensity, active smoking status, and lower SF-36 MCS scores are all independent predictors of axial neck pain at 2-year follow-up. 31
Following CF, deep extensor muscle denervation, facet injury, C2 or C7 muscle invasion, neural element compression, and prolonged postoperative cervical immobilization were identified as risk factors for postoperative axial neck pain. 37 Additionally, Lee et al. found that age and higher Pfirrmann grade were associated with axial neck pain. 35
Discussion
In this systematic review and meta-analysis, we found that patients undergoing cervical laminoplasty and cervical foraminotomy for compressive myelopathy and radiculopathy had significantly improved axial neck pain, mean postoperative VAS and NDI scores, and neurological outcomes when compared to their baseline preoperative values. We also found that the presence of anterolisthesis, loss of cervical muscle volume, regional malalignment, current smoking status, diabetes, age, and radiographic Pfirrmann grade were independent predictors of postoperative axial neck pain following these procedures.
Since CL and CF preserve degenerated discs and facet joint with segmental motion, it is a potential source of persistent axial neck pain after surgery. Concerns regarding persistent axial neck pain is controversial and may direct surgical strategy from CL to posterior instrumented fusion and from CF to ACDF.
Cervical Laminoplasty
The literature is disparate concerning laminoplasties and their relation to axial neck pain. Stephens et al demonstrated that in a select group of myelopathic patients with no significant preoperative axial pain and appropriate sagittal alignment, laminoplasty did not lead to worse axial neck pain, and was associated with significant improvements in other clinical outcomes. 8 Nurboja et al showed that laminoplasty was associated with greater levels of neck pain and worse quality of life when greater than 4 levels were decompressed when compared with laminectomies. 39 Conversely, Hosono et al compared laminoplasties to anterior cervical fusion, showing that patients undergoing laminoplasty had worse axial neck and shoulder pain. 7 The authors later indicated that lack of inclusion of C7 in laminoplasty could prevent postoperative axial pain, with deep extensor muscle detachment having no such effect. 40
Laminectomy with instrumented fusion is frequently utilized to address preoperative neck pain as well as segmental instability and deformity.41,42 Significant improvements of neck pain after laminectomy with fusion were observed in several studies.8,43-45 Two retrospective reviews reported a superiority of laminectomy with fusion to laminoplasty in reducing neck pain.8,44 One retrospective study found that patients who underwent laminectomy with fusion demonstrated a statistically significant reduction in VAS neck pain scores only at the 3-month postoperative mark compared to baseline. However, no statistically significant differences were observed at 12- and 24-month post-surgery, while laminoplasty showed significant reduction of VAS neck pain scores at 3, 12 and 24 month post-surgery. 45 In addition, one prospective, randomized trial established that VAS scores for neck, interscapular, and arm pain significantly improved only in patients treated with laminoplasty but not in patients treated with laminectomy followed by fusion. 46 Several systematic reviews have failed to find statistically significant differences between laminectomy with fusion and laminoplasty in alleviating neck pain.41,42,47,48
In the present study, we found patients undergoing CL had improved mean postoperative visual analogue scale and neck disability index (NDI) scores when compared to preoperative values, with mean differences of −1.97 (CI -2.52, −1.42; P < 0.0001) and −12.27 (CI -15.01, −9.54; P < 0.0001), respectively. This implies that preoperative axial neck pain following CL demonstrates improvement in both pain and neurological parameters, and that it is not a contraindication of CL.
Cervical Foraminotomy
Advantages of CF over ACDF include motion preservation, reduction in adjacent-segment reoperation rates, and expanding eligibility in patients who are poor candidates for fusion-based and/or anterior approach procedures. 3 In addition, recent advances in minimally invasive options using tubular retractor system or endoscopic access allow for less access-related morbidities, shorter hospital lengths of stay, and faster recovery. 49
Our analysis demonstrated that the literature reported PROs representing axial neck pain demonstrate no difference or significant improvement following CF. The reported significant risk factors related to postoperative axial neck pain are age and higher Pfirrmann grade. These results also imply that axial neck pain, combined with radiculopathy, would not be a contraindication of CF.
There are clinical limitations regarding the definition of axial neck pain in the literature, given the lack of an established definition and the wide clinical spectrum of neck pain. It is also unclear why central spinal canal decompression improves axial neck pain. Cervical radiculopathy from the C4 nerve root and periscapular pain from the lower cervical nerve root compression can be presented as ‘neck pain.’ However, it is evident that axial pain, as defined by VAS the neck or NDI, improve significantly among patients following CL or CF. The lack of consensus and wide spectrum of symptoms that encompasses ‘axial neck pain’ warrants future studies to further clarify and establish its definition.
This study is subject to the standard limitations of systematic reviews and meta-analyses of retrospective investigations. The patients included in these studies represent a heterogeneous cohort, with many factors that warrant further analysis in their relationship to surgical outcomes. Although Lee et al found age to be an independent predictor of axial neck pain, 35 our study had minimal variation in mean age. While several studies have demonstrated the impact of age on perioperative outcomes, the limited deviation in mean age observed in our study may highlight how even subtle differences in age can impact surgical outcomes and the resolution or persistence of axial neck pain,50-52 highlighting the need for additional studies to stratify these outcomes by age in subgroup analyses. Future research must also explore potential sources of heterogeneity through subgroup or sensitivity analyses, in order to better understand the underlying reasons for variability between study results. Additional sources of heterogeneity include variations in sample sizes as well as surgical indications, the use of analgesics, and operative approach selection; it is possible that many patients who experienced neck pain preoperatively were recommended for fusion procedures and were thus not included in these studies. Of note, we excluded studies with missing outcome values. Additionally, the location, character, duration and likely causes of neck pain are not specified in the majority of the studies, raising the possibility that different sources of neck pain may respond differently to posterior decompressive surgery. Variations in surgical technique must also be taken into account, particularly the role of preserving the C2 muscle attachments and C7 spinous process. 53 The greater number of studies analyzed from Asia may introduce regional discrepancy and affect the generalizability of our results. Although Asian spine surgeons more routinely perform less invasive and endoscopic approaches compared to their U.S. and European counterparts,54,55 our study primarily examined traditional laminoplasty and non-endoscopic laminoforaminotomy techniques, which are identical to the studies analyzed from the U.S. and Europe. Additionally, the greater number of Asian studies included for analysis may be attributed to the larger number of reports on motion-preserving decompression surgery from Asia, which has been found to have had the greatest increase over the past 5 decades. 56
Conclusions
This systematic review and meta-analysis found that posterior cervical laminoplasty and foraminotomy may provide significant relief of preoperative axial neck pain. These findings suggest that axial neck pain may not be an absolute contraindication to motion-sparing posterior surgical approaches for degenerative cervical radiculopathy or myelopathy in selected patients. Preoperative risk factors predisposing patients to unfavorable outcomes from axial neck pain following cervical laminoplasty or foraminotomy should be considered when determining optimal surgical strategy.
Supplemental Material
Supplemental Material - The Impact of Cervical Laminoplasty and Cervical Foraminotomy on Axial Neck Pain: A Systematic Review and Meta-Analysis
Supplemental Material for The Impact of Cervical Laminoplasty and Cervical Foraminotomy on Axial Neck Pain: A Systematic Review and Meta-Analysis by Andrew H. Kim, John P. Avendano, Marc Greenberg, Chathurangi H. Pathiravasan, Richard L. Skolasky, Mihir Gupta and Sang Hun Lee in Global Spine Journal.
Footnotes
Acknowledgments
This publication was made possible by the Johns Hopkins Institute for Clinical and Translational Research (ICTR) which is funded in part by Grant Number UL1TR003098 from the National Center for Advancing Translational Sciences (NCATS) a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Johns Hopkins ICTR, NCATS, or NIH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Institute for Clinical and Translational Research: UL1TR003098.
Disclosure
Andrew H. Kim, BS: None. John P. Avendano, BA: None. Marc Greenberg, MD: None. Chathurangi H. Pathiravasan: None. Richard L. Skolasky, ScD: None. Mihir Gupta, MD: None. Sang Hun Lee, MD, PhD: Consultant to Medtronic, Elliquence.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.