
Abstract
Study Design
Retrospective cohort study.
Objective
To (1) determine whether preoperative neck pain improves after laminoplasty for cervical myelopathy and identify factors that could predict improvements in neck pain.
Methods
A total of 88 patients with preoperative neck pain visual analogue scale (VAS) of ≥4, who underwent laminoplasty for cervical myelopathy, and were followed-up for >2 years were retrospectively reviewed. Patients demonstrating ≥50% improvement in VAS scores for neck pain 2 years postoperatively compared toㅇ preoperative assessment were included in neck pain improved (NP-improved) group. The remaining patients were assigned to neck pain unimproved (NP-unimproved) group.
Results
Overall, 54 patients (61.4%) were included in NP-improved group and 34 patients (38.6%) were included in NP-unimproved group. NP-unimproved group more frequently underwent C3 laminectomy (P = 0.026) and had lesser degree of preoperative C2-C7 lordosis (P = 0.006) in the extension position compared to that in the NP-improved group. Furthermore, undergoing C3 laminectomy was associated with lower probability of achieving a ≥50% improvement in neck pain VAS scores (P = 0.018), while greater preoperative C2-C7 lordosis in the extension position was associated with a higher possibility of neck pain improvement (P = 0.048). A cut-off value of 20.5° for C2-C7 lordosis in the extension position predicted a ≥50% improvement in neck pain.
Conclusion
Preoperative neck pain should not be considered contraindication for laminoplasty as 61.4% of patients experienced ≥50% improvement in neck pain post-operatively. C3 laminectomy decreases the probability of neck pain improvement after laminoplasty, while greater C2-C7 lordosis in the extension position is associated with neck pain improvement.
Keywords
Introduction
Laminoplasty is widely performed for the treatment of cervical myelopathy caused by spondylosis and ossification of the posterior longitudinal ligament.1,2 Advantages of laminoplasty include a low complication rate, technical simplicity, and favorable neurological recovery. 3 For patients with preserved cervical lordosis and multi-level cord compressive lesions, laminoplasty may provide better outcomes compared to other approaches. 2 However, laminoplasty inevitably injures the posterior neck muscles and ligamentous complexes which may result in sagittal alignment aggravation and worsened neck pain.3-5 Therefore, a few authors have suggested that laminoplasty should not be performed in patients with moderate to severe preoperative neck pain.2,5
Nevertheless, not all patients suffer from aggravation of sagittal alignment or neck pain after laminoplasty, 6 with the postoperative course of sagittal alignment and neck pain widely varying among patients.5,7 Spinal cord or nerve root compression could be a source of neck pain and may limit neck extension. Therefore, relieving such compression may alleviate neck pain.8,9 Recent studies have reported that preoperative moderate to severe neck pain is not a contraindication to laminoplasty, and a significant improvement in neck pain could be expected after surgery for selected patients.8,10 However, some patients still experience significant neck pain after laminoplasty due to an iatrogenic neck muscle injury.11,12 Furthermore, injury of the muscle insertions of the C2 and C7 spinous processes could worsen outcomes since these are critical structures for paraspinal neck muscle function.13,14 Recent reports have highlighted the importance of assessing dynamic factors to predict postoperative axial symptoms after laminoplasty.7,15,16
It remains unclear how surgeons can distinguish between patients with neck pain likely to improve after laminoplasty and those with neck pain that is unlikely to improve or worsen. 8 Understanding the factors predicting neck pain improvement is crucial for determining whether laminoplasty is a suitable option for patients with significant preoperative neck pain. 17 Therefore, this study aimed to (1) determine whether preoperative neck pain could improve after laminoplasty for the treatment of cervical myelopathy and (2) identify factors that predict neck pain improvement.
Materials and Methods
Study Design and Population
This retrospective cohort study was approved by the relevant institutional review board. The requirement for informed consent was waived due to the retrospective nature of the study. Data from 176 patients who underwent cervical laminoplasty for cervical myelopathy between January 2015 and January 2020 and those who were followed-up for ≥24 months were retrospectively reviewed. To assess neck pain improvement after laminoplasty, patients with a preoperative neck pain visual analogue scale (VAS) score ≥4 were included in the study. Conversely, patients (1) with a history of previous cervical spine surgery; (2) preoperative neck pain VAS <4; (3) who underwent laminoplasty due to tumor, infection, or trauma; and (4) those who were followed-up for <24 months, were excluded (Figure 1). The decision to perform laminoplasty was based on cervical sagittal alignment, K-line state, and the number of levels warranting decompression.
2
Patients with preserved cervical lordosis, a K-line (+) state, and multilevel involvement (>3 levels) were referred for laminoplasty.2,18 Patient selection process VAS, visual analogue scale.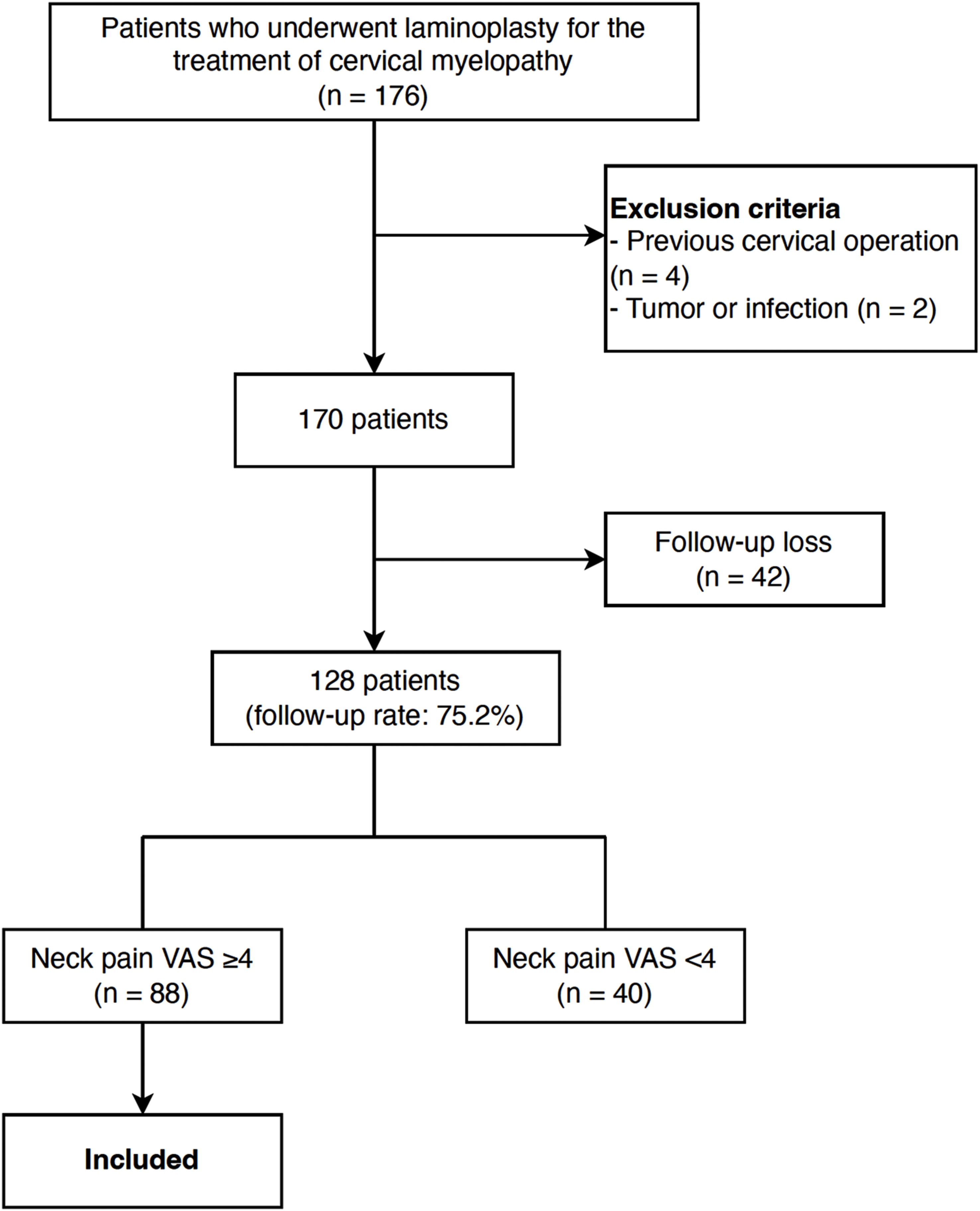
Patients with a ≥50% improvement in the neck pain VAS score 2 years postoperatively compared to the preoperative score were included in the neck pain improved (NP-improved) group, while those with an improvement <50% were included in the neck pain unimproved (NP-unimproved) group.
Surgical Techniques
All procedures were performed by a single surgeon. Patients were placed in the prone position with the neck flexed and head located on a Mayfield frame. Open door laminoplasty using mini-plate fixation was performed for all patients. The left side was chosen as the open side, and a trough was made on the right side in most cases. When C2 or C7 decompression was required, care was taken to avoid injuring the muscle attachments to the spinous processes during the exposure. Dome-shaped partial laminectomy was performed while sparing the spinous processes and muscles insertions. For C3 decompression, laminectomy was performed based on reports suggesting that C3 laminectomy better preserves range of motion (ROM) and avoids postoperative kyphosis compared to laminoplasty.
Variables
Patient-reported outcome measures, including the neck pain VAS score, neck disability index (NDI), and Japanese Orthopedic Association (JOA) score, were recorded preoperatively and at 2-year postoperatively. Patient-reported outcome-measure questionnaires were completed during outpatient clinic visits. Patients were asked to fill out the questionnaires based on their average pain and disability over the previous 2 weeks. The improvement rate in the VAS score and NDI were calculated as
The JOA recovery rate was calculated as
Radiographic assessments were performed preoperatively and 2 years postoperatively. Radiographic measurements were performed twice, by an independent spine fellowship trained surgeon with 5 years of experience. C2-C7 lordosis was measured using the Cobb angle between the lower endplates of C2 and C7 on cervical lateral radiographs taken in the neutral, flexion, and extension positions (Figure 2A). The cervical range of motion (ROM) was calculated as the difference in C2-C7 lordosis measured on lateral flexion and extension images. The C2-C7 sagittal vertical axis (SVA) was defined as the distance from the posterosuperior corner of C7 and the vertical line from the center of the C2 body (Figure 2B). The T1 slope was measured as the angle between the horizontal line and upper endplate of T1 (Figure 2B). The K-line tilt was defined as the angle between the line connecting the midpoints of the spinal canal at C2 and C7 and the vertical line (Figure 2C).
19
Radiographic measurements (A) C2-C7 lordosis was measured using the Cobb angle between the lower endplates of C2 and C7 on a cervical lateral radiograph (B) The C2-C7 sagittal vertical axis (SVA) was defined as the distance from the posterosuperior corner of C7 and the vertical line from the center of the C2 body. The T1 slope was measured as the angle between the horizontal line and upper endplate of T1. (C) The K-line tilt was defined as the angle between the line connecting the midpoints of the spinal canal at C2 and C7 and the vertical line.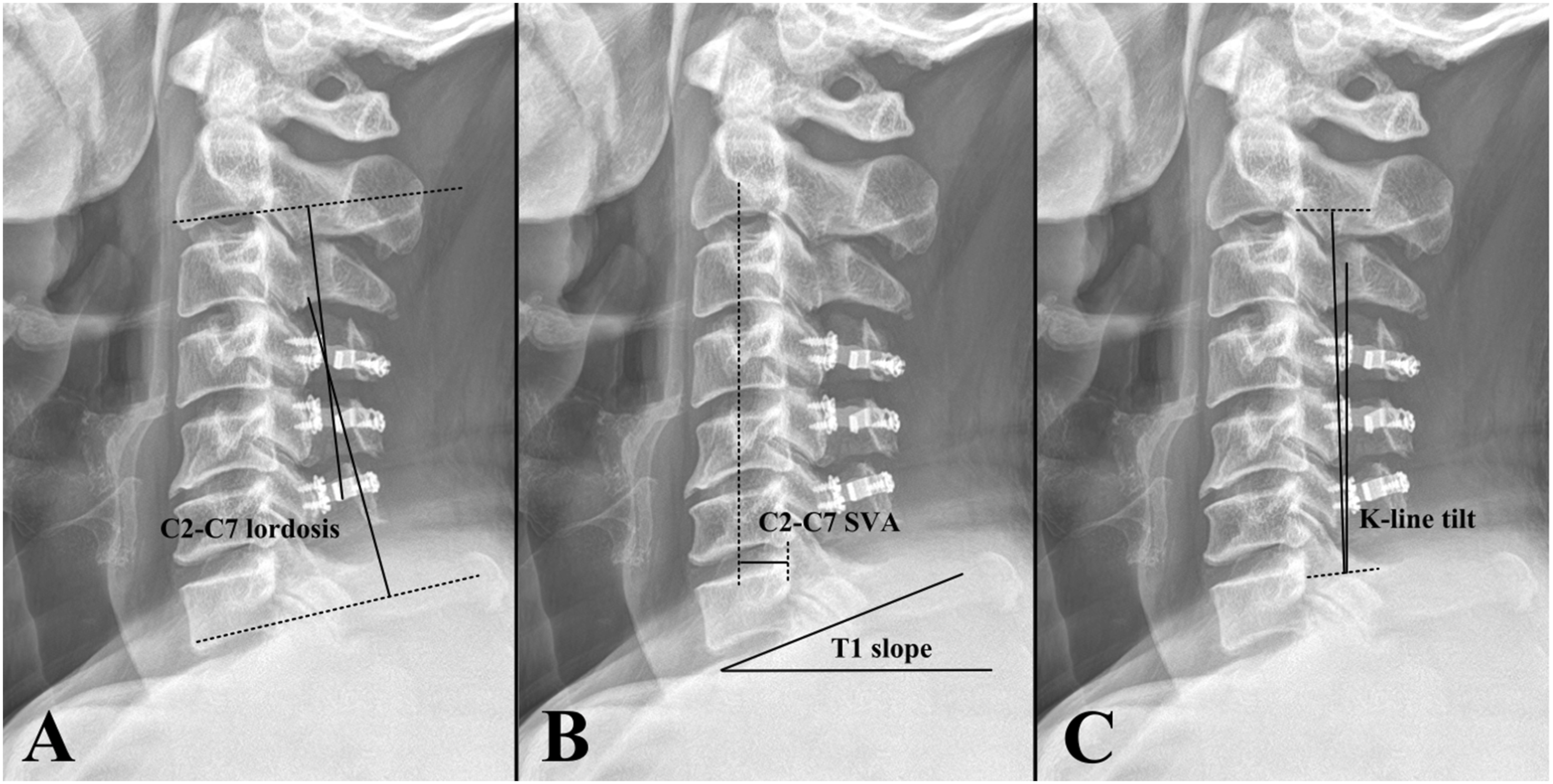
Statistical Analysis
All continuous variables were tested for normality using the Shapiro–Wilk text. Comparison between the NP-improved and NP-unimproved groups was performed using the Chi-squared test for categorical variables, and Student’st test for continuous variables. Logistic regression analysis was performed to identify factors associated with a ≥50% improvement in the neck pain VAS score. Receiver operating characteristic (ROC) curve analysis was performed to assess the capacity of risk factors to predict a VAS score improvement ≥50%. Interobserver reliability was assessed using intraclass correlation coefficients (ICC). The ICC for the measurement of radiographic parameters was 0.788. All analyses were performed using SPSS version 29.0 software (SPSS, Inc, Chicago, IL). A P value <0.05 was considered significant.
Results
Study Population and Operative Characteristics
Patient Characteristics.
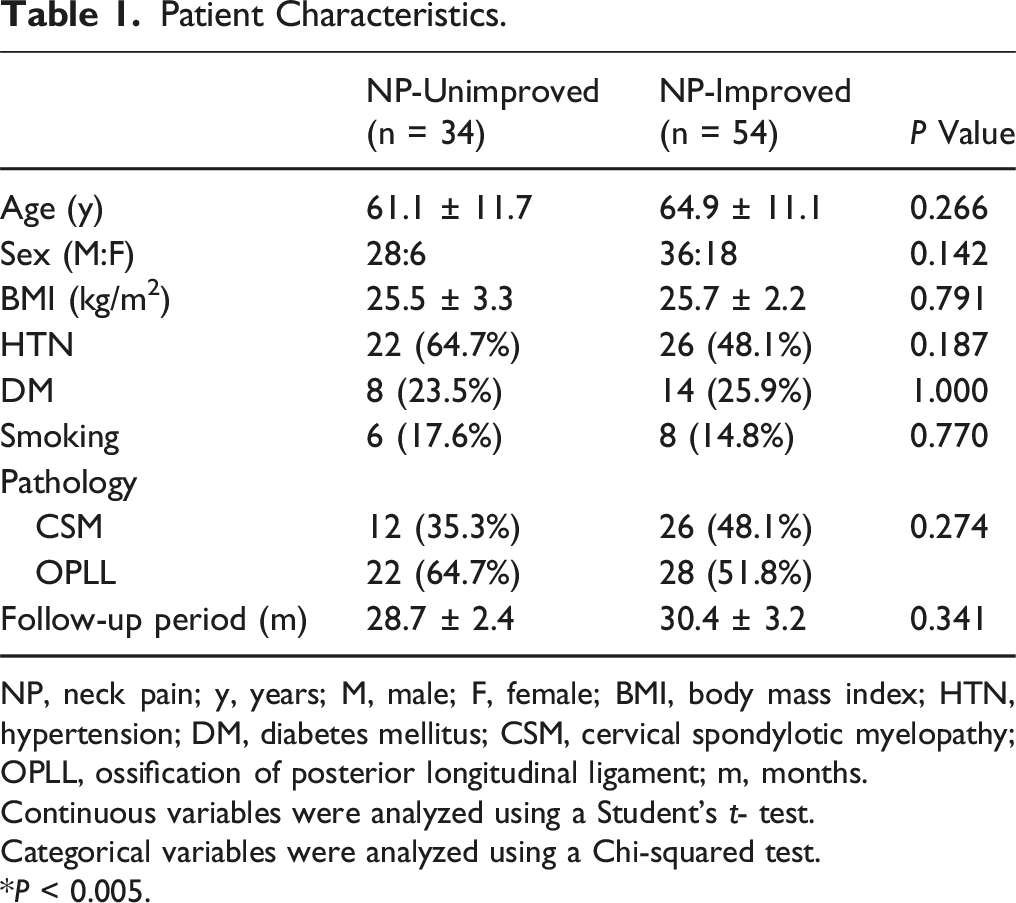
NP, neck pain; y, years; M, male; F, female; BMI, body mass index; HTN, hypertension; DM, diabetes mellitus; CSM, cervical spondylotic myelopathy; OPLL, ossification of posterior longitudinal ligament; m, months.
Continuous variables were analyzed using a Student’s t- test.
Categorical variables were analyzed using a Chi-squared test.
*P < 0.005.
Surgical Characteristics.
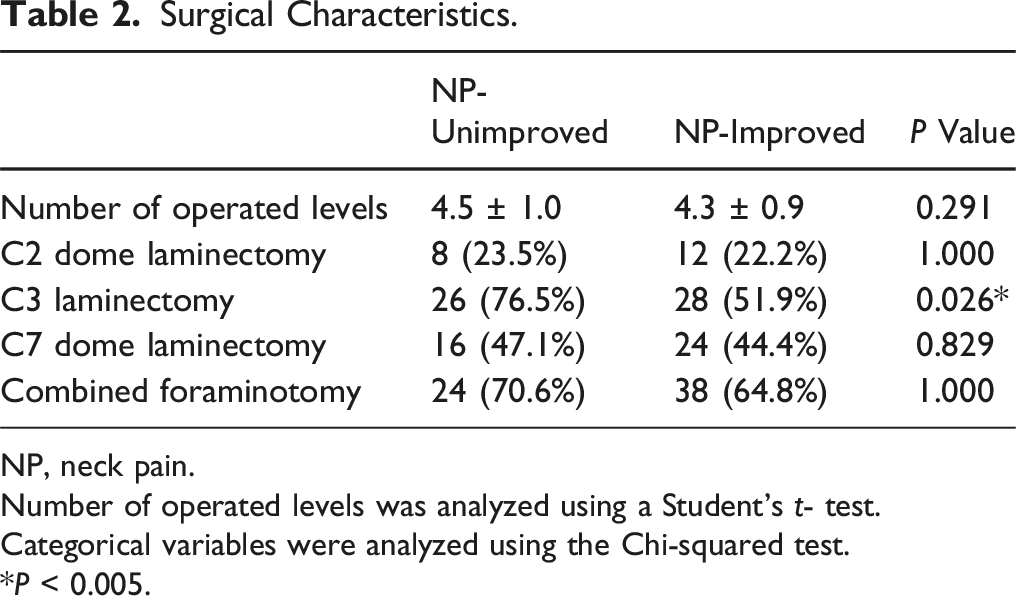
NP, neck pain.
Number of operated levels was analyzed using a Student’s t- test.
Categorical variables were analyzed using the Chi-squared test.
*P < 0.005.
Patient Reported Outcome Measures
Patient Reported Outcome Measures.
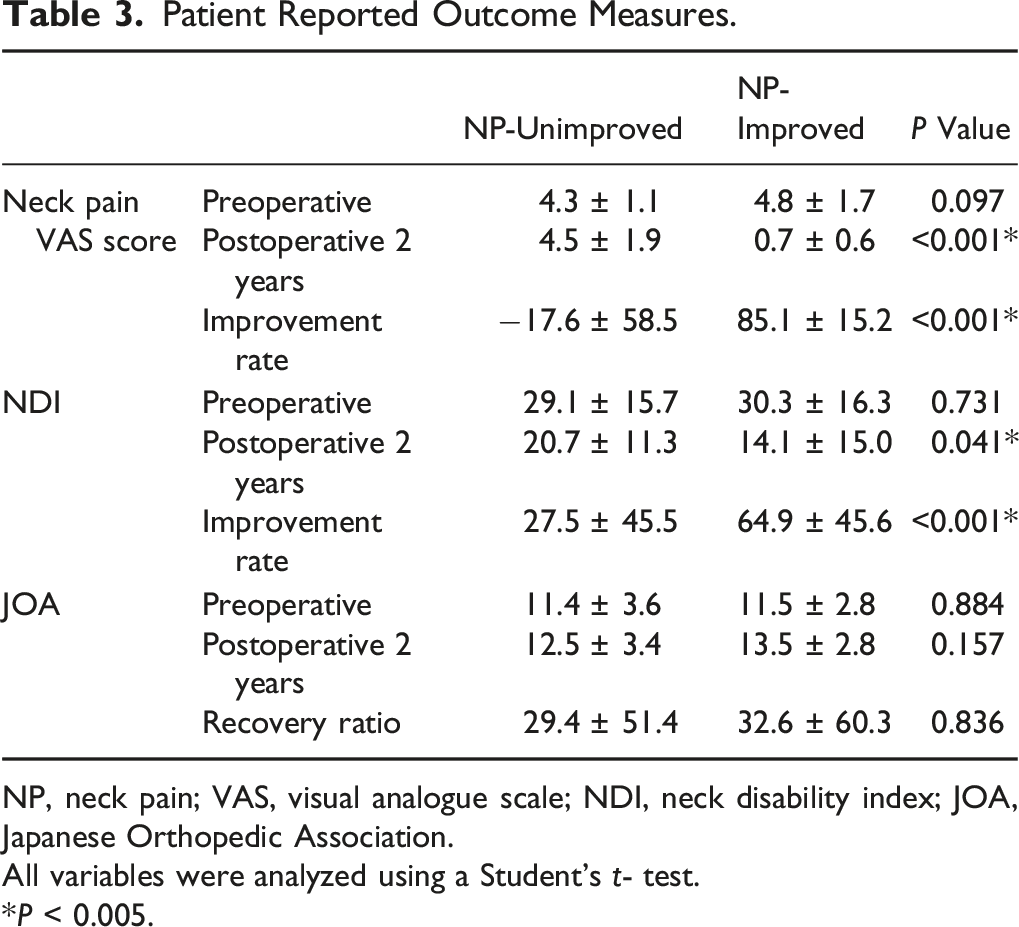
NP, neck pain; VAS, visual analogue scale; NDI, neck disability index; JOA, Japanese Orthopedic Association.
All variables were analyzed using a Student’s t- test.
*P < 0.005.
The preoperative NDI revealed no significant intergroup difference (P = 0.731). The NDI significantly improved after surgery in both groups (P < 0.001, <0.001, respectively). However, the NDI improvement rate was significantly higher in the NP-improved group (P < 0.001), and NDI at 2 years postoperatively was significantly lower in the NP-improved group compared to NP-unimproved group (P = 0.041) (Table 3).
The JOA score significantly improved after surgery both in the NP-unimproved (P = 0.007) and NP-improved (P < 0.001) group. There were no significant differences between the JOA score (P = 0.157) and JOA recovery rate (P = 0.836) of both groups 2 years postoperatively (Table 3).
Radiographic Results
Radiographic Results.
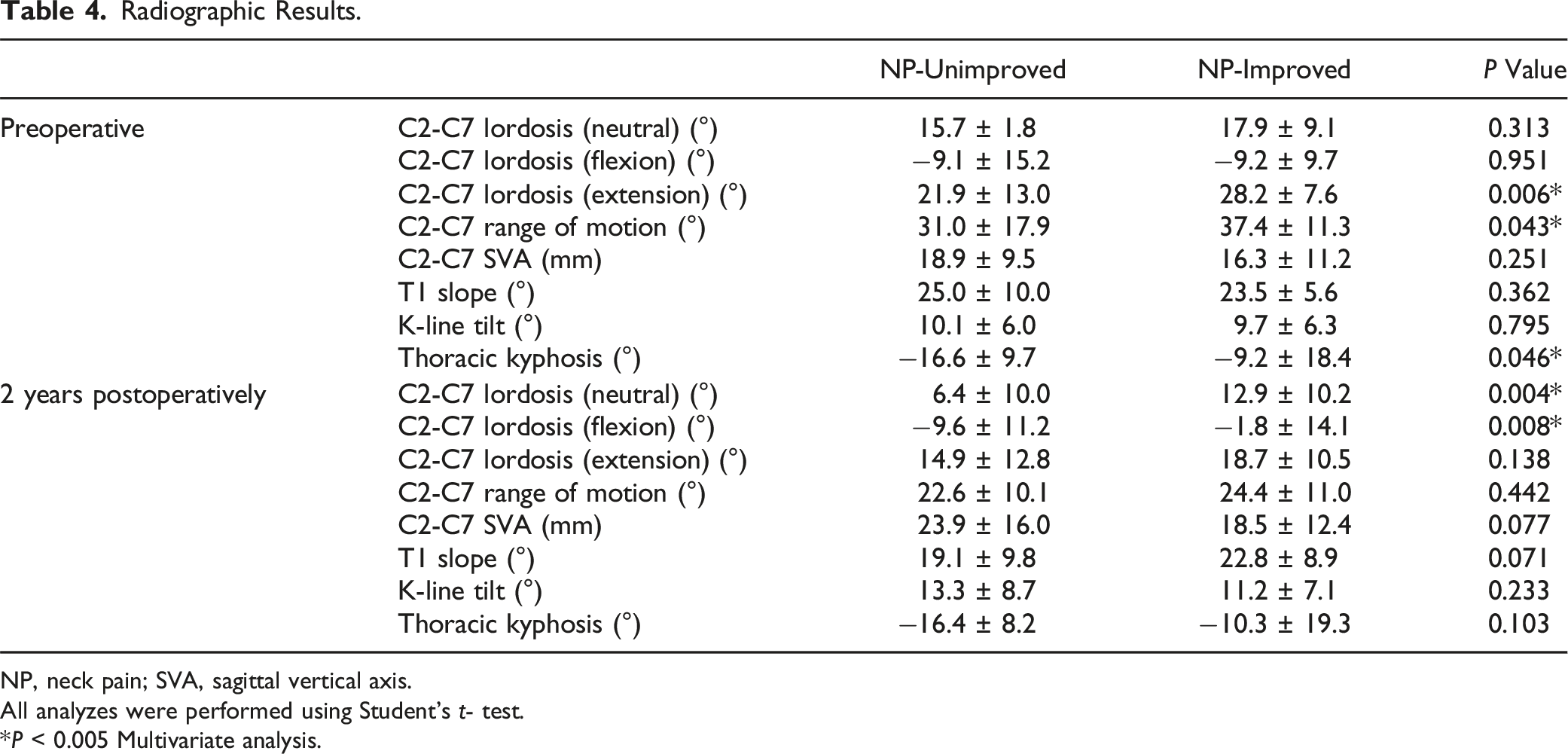
NP, neck pain; SVA, sagittal vertical axis.
All analyzes were performed using Student’s t- test.
*P < 0.005 Multivariate analysis.
C2-C7 lordosis in the neutral position (P = 0.006, and <0.001, respectively) and extension position (P < 0.001, and <0.001, respectively) significantly decreased after surgery in both the NP-unimproved group and the NP-improved group. C2-C7 lordosis in flexion position significantly decreased only in the NP-improved group (P < 0.001), remaining unchanged in the NP-unimproved group (P = 0.441).
At 2 years postoperatively, C2-C7 lordosis in the neutral position was significantly greater in the NP-improved group (P = 0.004), while C2-C7 lordosis in the flexion position was greater in the NP-unimproved group (P = 0.008). Lordosis in the extension position was not significantly different between the 2 groups (P = 0.138). Other radiographic parameters did not demonstrate significant intergroup differences 2 years postoperatively (Table 4).
Factors Associated with Neck Pain VAS Score Improvement of ≥50%
Logistic Regression Analysis Demonstrating Factors Associated With Neck Pain Improvement of ≥50%.
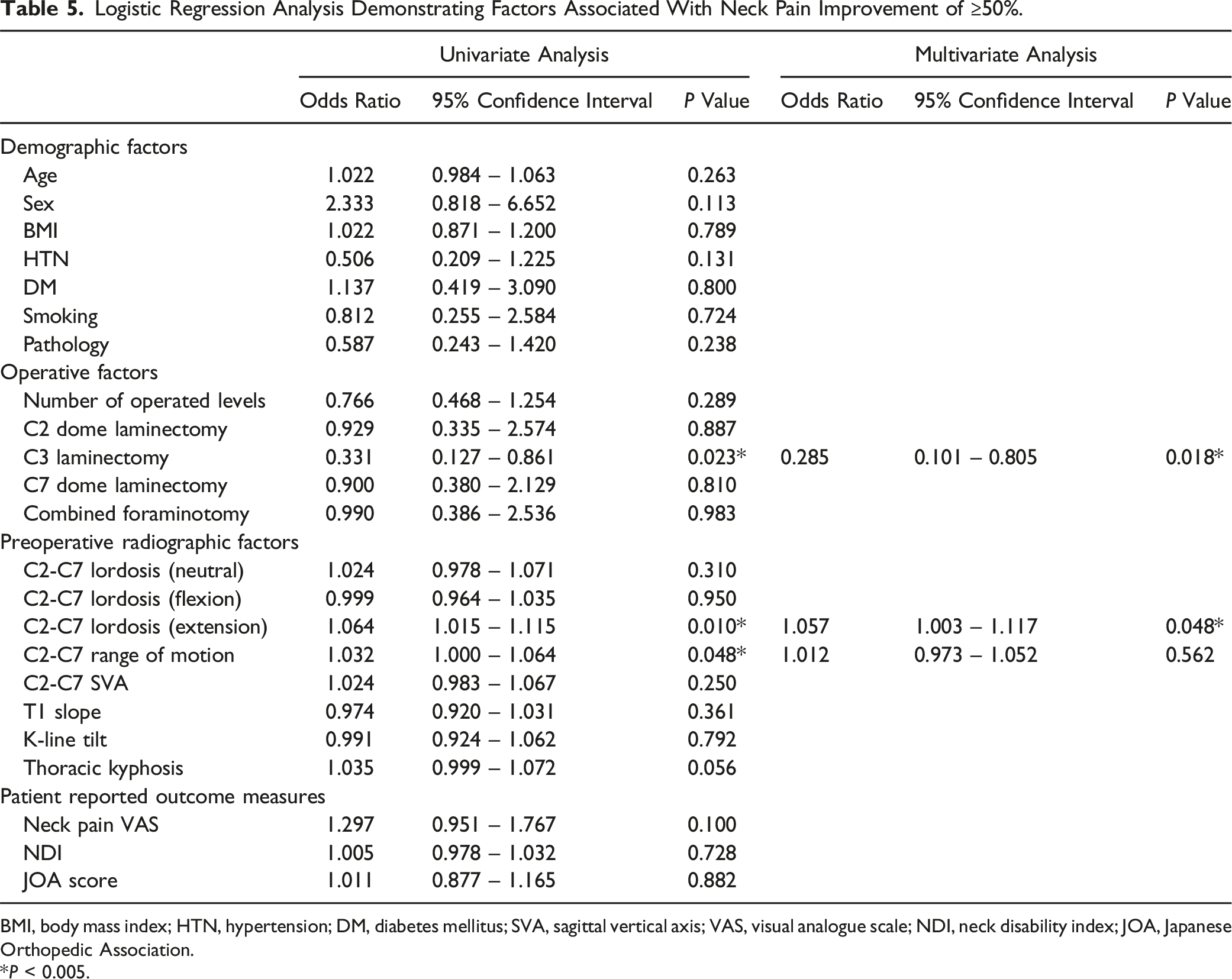
BMI, body mass index; HTN, hypertension; DM, diabetes mellitus; SVA, sagittal vertical axis; VAS, visual analogue scale; NDI, neck disability index; JOA, Japanese Orthopedic Association.
*P < 0.005.
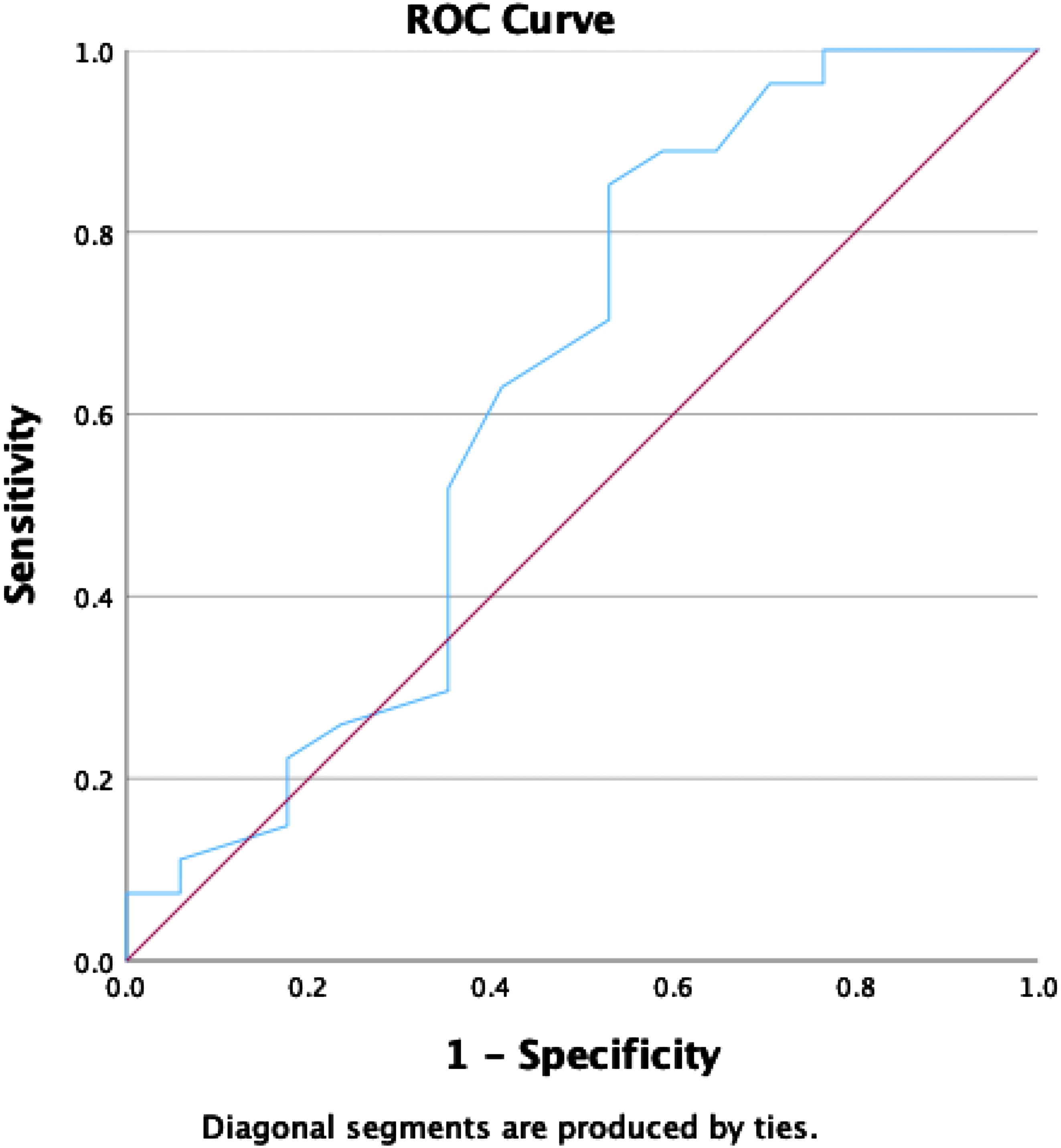
Receiver operating characteristics curve for preoperative C2-C7 lordosis in extension position.
Discussion
In this study, 61.4% of patients with moderate preoperative neck pain experienced ≥50% improvement after laminoplasty, suggesting the feasibility of the procedure for patients with neck pain. The NP-unimproved group more frequently underwent C3 laminectomy and had a lesser degree of C2-C7 lordosis in the extension position than the NP-improved group. Furthermore, logistic regression analysis revealed that C3 laminectomy was associated with a lower likelihood of neck pain improvement, whereas greater preoperative C2-C7 lordosis in the extension position was associated with a higher probability of achieving a ≥50% improvement in the neck pain VAS score. Finally, a cut-off value of 20.5° for C2-C7 lordosis in the extension position predicted of a ≥50% improvement in the neck pain VAS score.
Patients frequently face postoperative neck pain after laminoplasty whether it is transient or permanent.1,10 Laminoplasty inevitably damages the posterior ligament and extensor muscle attachments to the spinous processes and lamina which could be a cause of neck pain or sagittal alignment aggravation.5,20,21 While several muscle sparing approaches for laminoplasty have been proposed, conflicting results have been reported, and conventional laminoplasty remains the most popular technique. 10 Several clinical guidelines have suggested that laminoplasty should not be performed for patients with preoperative moderate neck pain. 2
However, 61.4% of patients in the current study experienced a neck pain VAS score improvement ≥50%. Recent studies have reported that a significant portion of patients with preoperative neck pain experience improvement after laminoplasty despite posterior neck muscle injury. 8 Pinter et al reported that patients with moderate or severe preoperative neck pain could achieve equivalent clinical improvement compared to patients with mild preoperative neck pain after laminoplasty. 8 Wang et al also suggested that with recent improvements in laminoplasty techniques sparing critical muscle attachments, postoperative neck pain is now a matter of less concern. 17 Finally, since neural compression affecting the C3 and C4 nerve roots may contribute to neck pain, relieving this compression through laminoplasty could alleviate neck pain. 9 Therefore, preoperative neck pain alone should not be considered a contraindication for laminoplasty. 8
C3 laminectomy was identified as a factor hindering neck pain improvement in this study. C3 laminectomy was originally recommended since it prevents interlaminar fusion and better preserves cervical ROM compared to C3 laminoplasty. Furthermore, it does not aggravate neck pain or kyphosis. 22 Based on these results, C3 laminectomy instead of laminoplasty was performed for all patients requiring C2-3 or C3-4 decompression.22,23 Therefore, the present study cannot compare the results of C3 laminectomy and laminoplasty in terms of postoperative neck pain since no patients underwent C3 laminoplasty.
The current study may suggest that complete exposure of C3 lamina and the resultant muscle insertion injury may contribute to the lack of improvement in neck pain after surgery. The insertion of the semispinalis cervicis to the C2 spinous process plays a critical role in cervical dynamic stability, with the detachment of these muscle attachments aggravating neck pain after laminoplasty.13,23 Several anatomical specifics make it challenging to preserve muscle insertions to the C2 spinous process during the exposure of the C2-3 interlaminar space, which is required for C3 laminectomy. Firstly, due to the large and caudally drifted shape of the C2 spinous process, interlaminar space between C2 and C3 is narrower compared to other levels. 24 Secondly, semispinalis cervicis muscles are attached at the caudal portion of the C2 spinous process. 25 Finally, approximately 50% of patients have a narrow-angled C2 spinous process, complicating exposure of the C2-3 interlaminar space and increasing the risk of injury to the semispinalis cervicis insertion on the C2 spinous process.6,13 Performing C3 laminectomy may have prevented neck pain improvement due to potential injury at the attachment sites of critical muscles to the C2 spinous process. Nevertheless, further investigation is required to verify whether the worsened neck pain with C3 laminectomy is caused by muscle detachment or performing laminectomy rather than laminoplasty. Kim et al reported that performing C3 laminoplasty may provide less postoperative neck pain compared to C3 laminectomy. 26 In this randomized controlled trial comparing patients who underwent C3 laminectomy vs laminoplasty, those who underwent C3 laminoplasty experienced significantly less neck pain at the final follow-up. 26 Muscle injury was associated with postoperative neck pain, however; using a muscle-sparing technique during C3 laminoplasty in their series could have reduced postoperative neck pain. 26
Preoperative C2-C7 lordosis in the extension position greater than 20.5° was a factor that increased the possibility of neck pain VAS score improvement. Recent studies highlighted that dynamic factors are important in predicting postoperative prognosis after laminoplasty and that a greater extension capacity is associated with favorable outcomes.3,15,16 Cheng et al reported that patients with extension capacites greater than 9.3° are more likely to experience an improvement of cervical lordosis after laminoplasty. 16 The authors suggested that greater extension capacity would indicate preoperative neck flexion caused by cord compression, although patients typically present with greater lordosis. 16 Further studies have also demonstrated that patients with greater extension experience reduced cervical lordosis loss after laminoplasty.3,7 Greater preoperative neck extension may represent the better functional reserve of paraspinal muscles, particularly the semispinalis cervicis which plays a critical role in neck extension. 3 Patients with well-preserved posterior neck muscles have a lower risk of sagittal alignment aggravation and worsening of neck pain after surgery. 3
Considering these results, surgeons should exercise more care when decompression of C3 level is warranted as C3 laminectomy and the resultant injury to the muscle attachments to the C2 spinous process might hinder neck pain improvement.
13
A modified surgical technique that decreases the amount of muscle detachment or partial laminectomy of C3 to preserve the C2-3 interlaminar space could be considered.5,10,13 Addtionally, Kato et al suggested that selective laminoplasty to preserve the paraspinal neck muscles decreases postoperative axial symptoms.
25
Further studies are required to clarify whether C3 laminoplasty rather than C3 laminectomy reduces neck pain.
26
Surgeons may perform laminoplasty in patients with moderate to severe neck pain and preoperative C2-C7 lordosis greater than 20.5° in the extension position as these patients are more likely to experience symptom improvement (Figure 4). Illustrative case A 52-year-old female presented with clumsiness of both hands, gait disturbance, and neck pain. The preoperative neck pain visual analogue scale score was 5. (A) On a preoperative sagittal MRI, cord compression by ossification of the posterior longitudinal ligament at the C3-5 levels is noted. (B) C2-C7 lordosis measured in the neutral position radiograph was 17°. (C) Preoperative C2-C7 lordosis in the extension position was 32°, which was a favorable prognostic factor indicating greater possibility of neck pain improvement after laminoplasty. (D) Laminectomy of C3, laminoplasty of C4 and C5, and dome shaped partial laminectomy of C6 were performed. (E) MRI at 2 years postoperatively demonstrates a well decompressed spinal canal. The patient’s Japanese Orthopedic Association score improved from 15 to 17. Furthermore, the neck pain visual analogue scale score improved to 1 at 2 years postoperatively.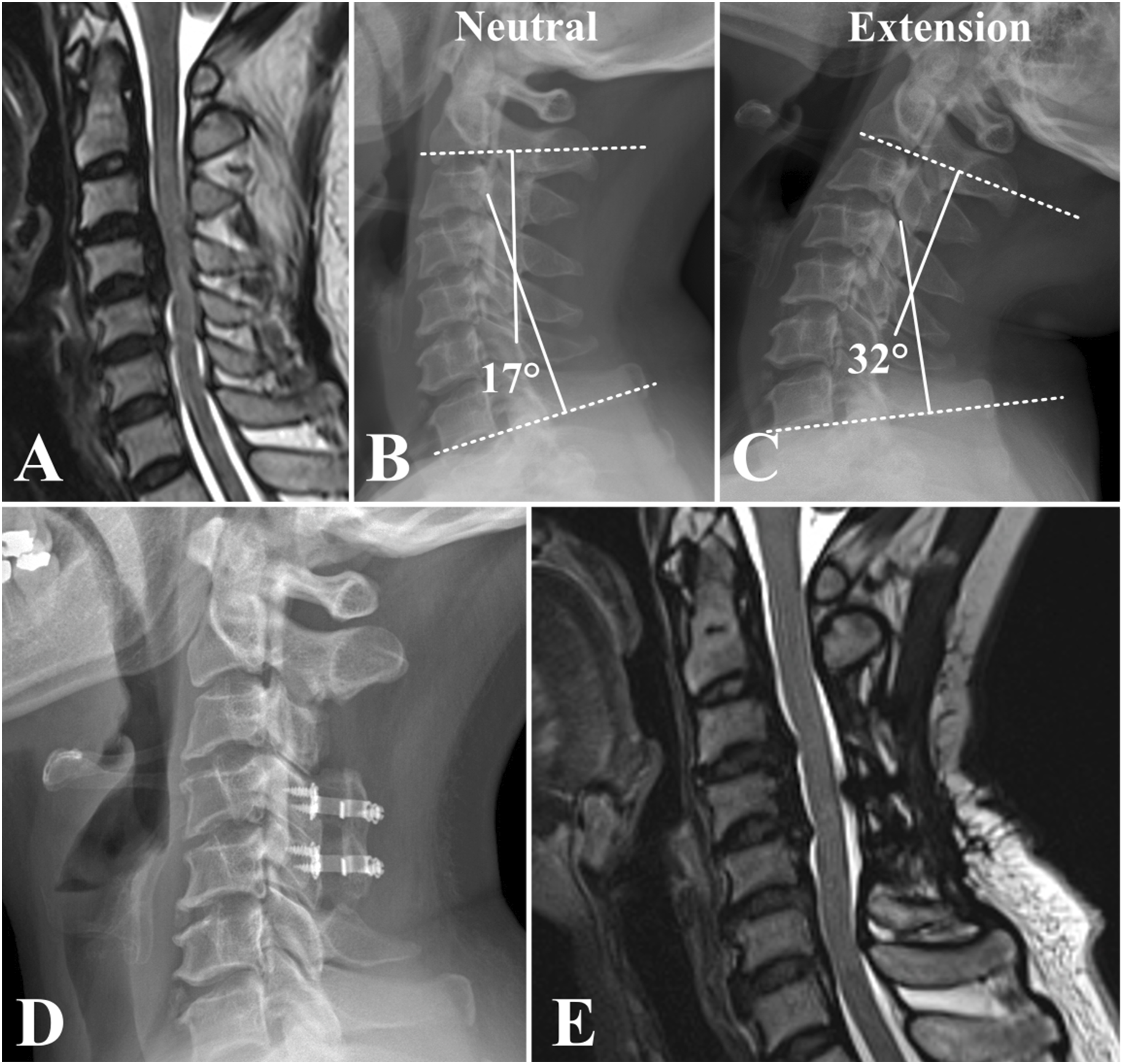
This study has few limitations. Firstly, the number of vertebral levels involved in the procedure varied among patients. However, number of levels involved was not associated with neck pain improvement in logistic regression analysis, and there were no significant intergroup differences in the levels involved between the 2 groups. Secondly, the current study did not compare outcomes between C3 laminectomy and C3 laminoplasty, as no patients underwent C3 laminoplasty. Therefore, further verification is required to clarify whether performing a C3 laminoplasty instead of a laminectomy is likely to result in greater improvement in neck pain. 26 Thirdly, the neck pain VAS score is a subjective outcome measure that may vary significantly depending on the timing of assessment. 27 NDI is another outcome measure of axial discomfort of the cervical spine, including both axial pain and function. However, it is not a tool for the assessment of axial symptoms alone. 28 Since neck pain was the outcome of interest in the present study, neck pain VAS score was used as the primary outcome measure. Furthermore, previous studies have demonstrated that the VAS score possesses good reliability. 29 Finally, the inherent biases of the retrospective design of this study cannot be excluded.
In conclusion, laminoplasty should not be considered a contraindication for patients with preoperative neck pain, since 61.4% of patients experienced a ≥50% improvement in neck pain. Additionally, undergoing C3 laminectomy decreased the possibility of neck pain improvement after laminoplasty, while greater C2-C7 lordosis in the extension position was a factor alleviating neck pain. Therefore, alternative surgical strategies or more meticulous soft tissue dissection are required for patients requiring C3 decompression. Furthermore, patients with a preoperative C2-C7 lordosis >20.5° are good candidates for cervical laminoplasty despite preoperative neck pain, since they are more likely to improve.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.