
Abstract
Study Design
Cohort study with consecutive cases.
Objectives
Dysphagia after anterior cervical spine surgery is a well-known complication. The aim of this study is to identify risk factors for dysphagia in patients with cervical myelopathy requiring surgery.
Methods
We conducted a prospective analysis of 92 consecutive patients with cervical spondylotic myelopathy (CSM) who underwent anterior cervical spine surgery. All patients underwent a pre- and postoperative swallowing evaluation using the Eating Assessment Tool (EAT-10) and the Hyodo–Komagane (H‒K) score, an endoscopic scoring method used by an examining otolaryngologist to assess dysphagia.
Results
None of the patients had dysphagia when assessed using EAT-10; however, 15.2% of patients had H‒K scores indicative of dysphagia. Preoperative latent dysphagia was highly correlated with postoperative dysphagia (r = 0.51, P < 0.0001). No significant difference was found for the presence of dysphagia due to a history of smoking, dialysis, diabetes, asthma, and restrictive and/or obstructive ventilation disorder. The 10-s grip and release test (P < 0.0001) and the upper extremity function (P = 0.004) and bladder function (P = 0.0008) items from the Japanese Orthopaedic Association scores significantly correlated with H‒K scores.
Conclusion
This study suggests that advanced age and severe preoperative upper limb and bladder dysfunction are risk factors for dysphagia in patients with cervical myelopathy requiring surgery.
Keywords
Introduction
Dysphagia, or swallowing dysfunction, commonly occurs in the elderly. Complications associated with dysphagia include aspiration, aspiration pneumonia, malnutrition, and increased risk of mortality. Due to dysphagia and its associated complications, the length of hospital stay for postoperative patients is often prolonged.1,2 Therefore, preoperative assessment of the likelihood of dysphagia is important. Specifically, postoperative dysphagia is an important consideration after anterior cervical spine surgery for cervical spondylotic myelopathy (CSM), with a reported frequency of 1%–79%.3-7 Surgery-related risk factors of postoperative dysphagia include prolonged operative time, surgical alignment changes, anterior plating, multilevel and upper level in anterior cervical surgery.7,8 However, postoperative dysphagia occurs in surgeries other than anterior cervical surgery, such as laminoplasty, and risk factors based on the patient’s clinical characteristics are also important.2,9
The Eating Assessment Tool-10 (EAT-10) is a recently established patient-reported assessment tool that can be used to easily evaluate dysphagia symptoms. 10 The Hyodo–Komagane (H‒K) scoring system is used during a flexible endoscopic evaluation of swallowing (FEES) using blue-dyed water and has been proven useful in otorhinolaryngology to evaluate dysphagia.11,12 We collaborated with otolaryngologists at our institution and investigated the mechanisms of postoperative dysphagia by performing two swallowing assessments before cervical spine surgery. Our past studies have elucidated that some patients have pre-existing dysphagia and are at risk for postoperative dysphagia and respiratory complications.13,14 This study aimed to determine the correlation between preoperative dysphagia and patient comorbidities and between preoperative dysphagia and background clinical characteristics.
Methods
Patient Groups and Surgical Techniques
We obtained informed, written consent from all eligible patients. The study was approved by the institutional review board of our institute (application No. 1182). In this study, all cases were diagnosed as cervical myelopathy caused by cervical degenerative diseases based on physical and imaging findings by spine surgery specialists. When necessary, neurologists were consulted preoperatively to rule out other neurological disorders. We conducted a prospective analysis of 94 consecutive patients with CSM who underwent anterior cervical spine surgery. Intraoperative esophageal injury occurred in one patient, and one patient required reoperation due to postoperative hematoma. Therefore, data from 92 cases, excluding these two patients, were analyzed. None of the cases included in this study had preoperative osteophytes measuring 3 mm or larger. Using the Smith–Robinson technique, two board-certified spinal surgeons performed the surgeries between 2015 and 2023. A left-sided approach was used at one institute. All eligible patients provided informed written consent. Each patient underwent spinal fusion using an anterior cervical titanium plate and fixation screws after decompression, including simple discectomy and/or corpectomy. All patients were treated using the MaxAn® anterior cervical plate system (Zimmer Biomet Spine, 2.5-mm-thick plate). We obtained patient comorbidities and background clinical characteristics from electronic medical records.
Pulmonary Function Tests
All patients underwent a pulmonary function test (PFT) to measure lung capacity preoperatively. The tests were performed in a standing position. Spirometry was performed thrice, and the highest value was selected. PFT data were expressed as absolute (highest) values of forced expiratory volume in 1 s (FEV1, an assessment of lung capacity) and forced lung capacity (FVC), and percent predicted values were normalized by age, weight, and preoperative height or arm length. Obstructive and restrictive failures were defined as FEV1 <70% and FVC <80%, respectively.
Radiographic Evaluation
We obtained preoperative standard standing sagittal images, with the upper boundaries of the radiograph film positioned parallel to the hard palate. An experienced orthopedic surgeon measured the C2‒7 angle. A positive angle was defined as a lordotic curve.
Swallowing Function Assessment
An experienced otolaryngologist and a speech-language pathologist assessed dysphagia by using the EAT-10 and H‒K scores preoperatively and 1‒2 weeks postoperatively. The EAT-10 dysphasia screening tool consists of 10 items and rates the severity of dysphagia on a 5-point Likert scale. The EAT-10 has been proven reliable and valid. Based on previous reports, EAT-10 scores of ≥3 indicate dysphagia. 15 The H‒K score is simple and based on four parameters of clinically-based FEES scoring: (1) the degree of salivary retention in the epiglottis and pisiform sinus, (2) the glottal closure reflex elicited by endoscopic touch of the epiglottis or glottis, (3) the onset of the gag reflex assessed using the timing of “white out” initiation of the swallowing reflex, and (4) pharyngeal clearance after swallowing the blue-dyed water. Evaluations were classified as 0, 1, 2, and 3 for normal, and mild, moderate, and severe impairment, respectively. This system has been proven reliable and useful when assessing the severity and characteristics of dysphagia. Based on previous reports, dysphagia was defined as a total score >3.47.11,16
Neurological Assessment
The Japanese Orthopaedic Association (JOA) scoring system was used to assess preoperative neurological status. 17 The 10-s grip and release test (GR test) was used to quantitatively assess neurological performance. Each patient was asked to grip and release as quickly as possible with the fingers while keeping the forearm in a rotated position and the wrist in mild extension. The number of cycles of complete 10-s movements was counted separately for the left and right sides, and the mean value was calculated. 18
Statistical Analyses
To identify significant differences, data were analyzed using an unpaired t test, Mann–Whitney U test, and Fisher’s exact test. The correlation between pre- and postoperative H‒K scores, age, JOA scores, and GR test was determined using Pearson’s correlation coefficient. All statistical calculations were performed using Prism (version 9.0; Graph Pad Software, La Jolla, CA, USA). For all tests, P < 0.05 was considered statistically significant.
Results
Patient Background
Background Characteristics of Patients With Cervical Spondylotic Myelopathy who Underwent Preoperative Swallowing Evaluation.
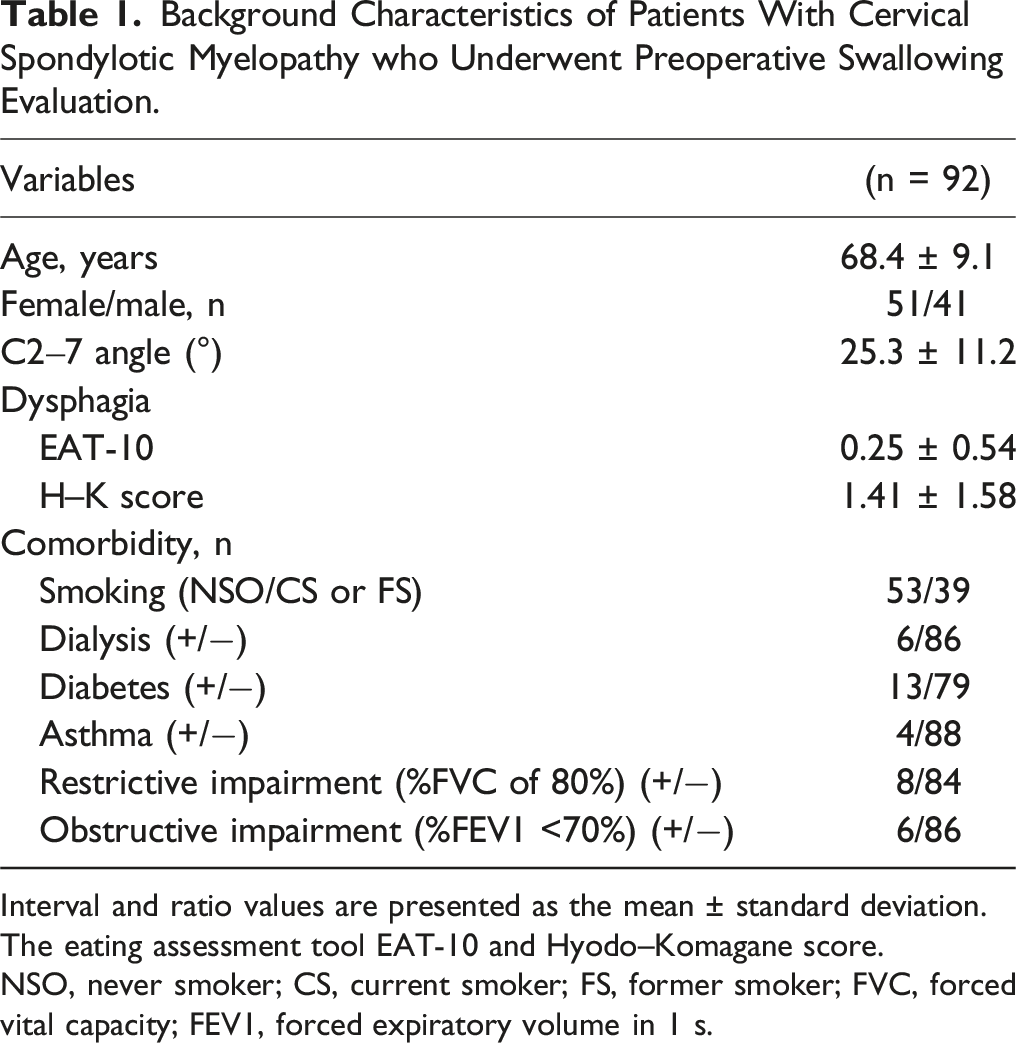
Interval and ratio values are presented as the mean ± standard deviation.
The eating assessment tool EAT-10 and Hyodo–Komagane score.
NSO, never smoker; CS, current smoker; FS, former smoker; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s.
Comparison of Patients with and without Dysphagia
Comparison of Patients With and Without Preoperative Dysphagia.
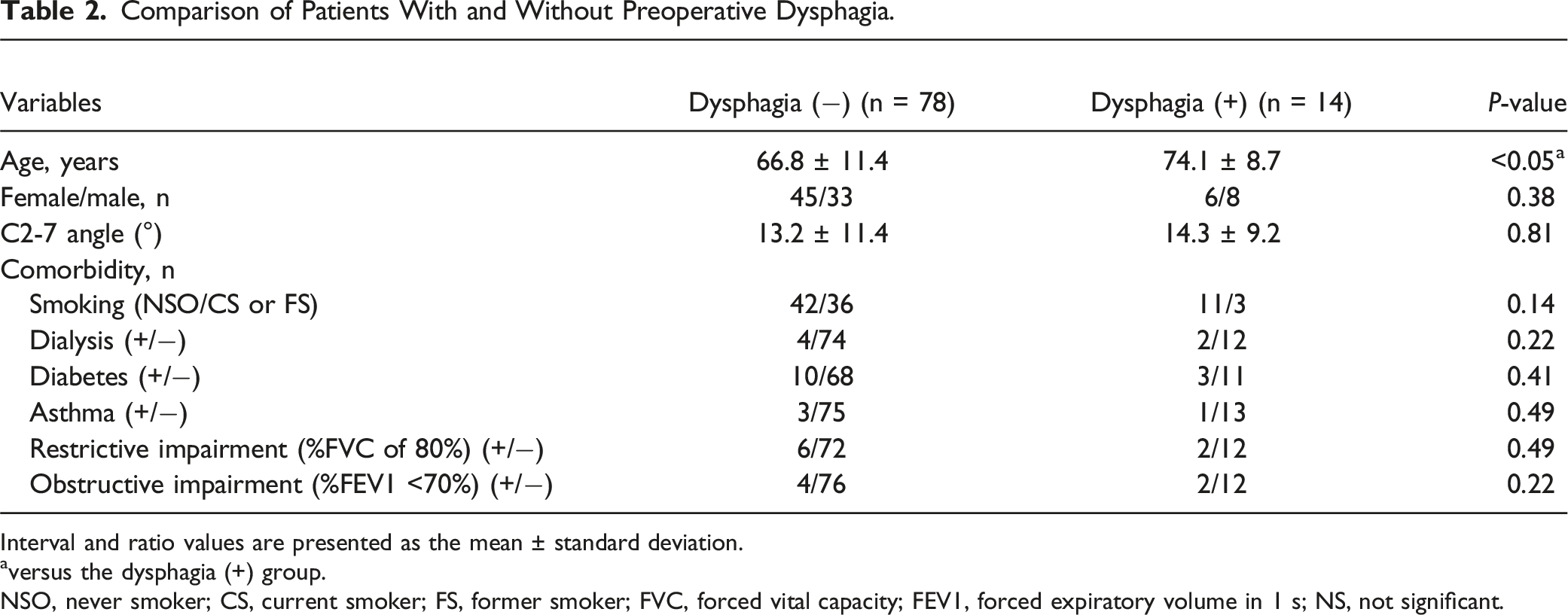
Interval and ratio values are presented as the mean ± standard deviation.
aversus the dysphagia (+) group.
NSO, never smoker; CS, current smoker; FS, former smoker; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; NS, not significant.
Relationship Between Postoperative Dysphagia and Surgical Factors.

Relationship Between Postoperative dysphagia and Surgical Factors
According to the diagnosis using the HK score, 23 patients exhibited postoperative dysphagia. A comparative analysis between the dysphagia and non-dysphagia groups revealed no significant differences in operative time, blood loss, or the number of fused vertebrae.
Correlation Between Severity of Myelopathy, Age, and H‒K Score
Correlation Between Severity of Myelopathy, Age, and Preoperative H–K Score.
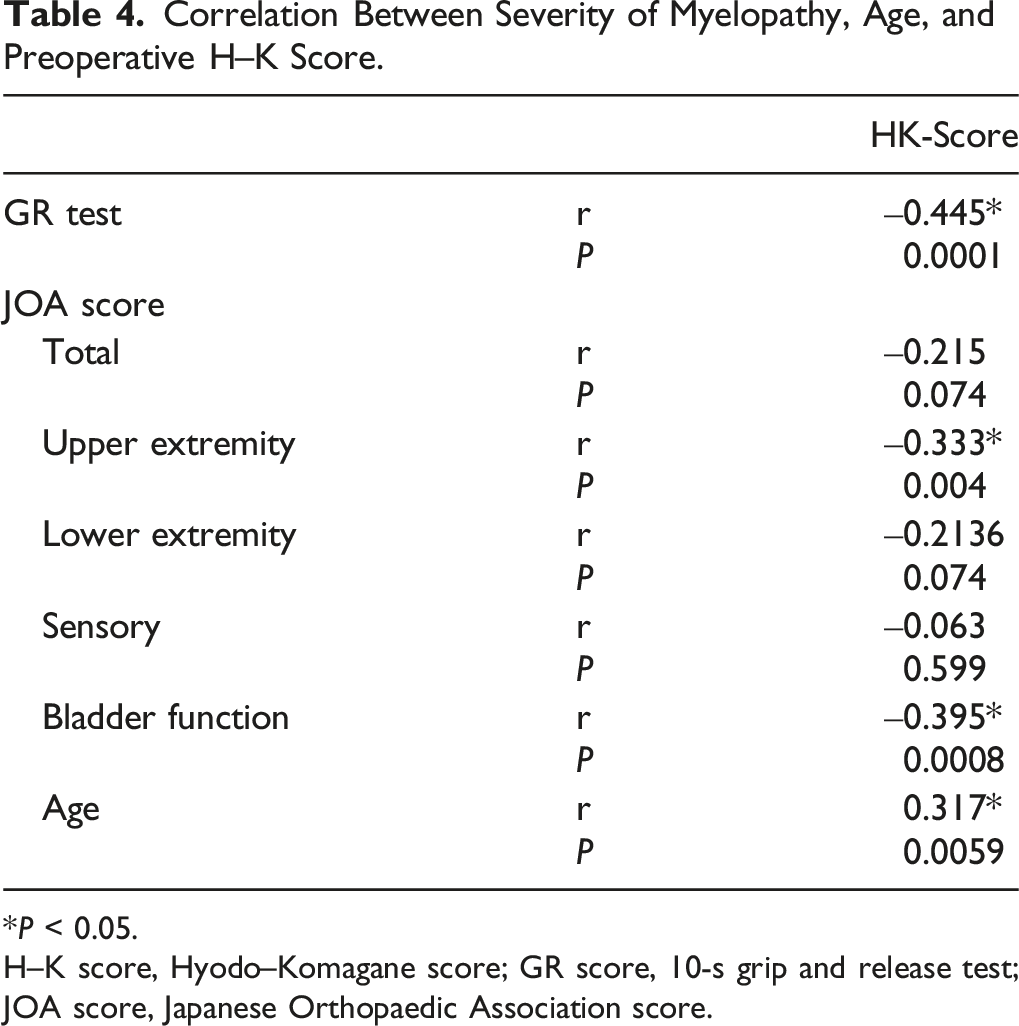
*P < 0.05.
H–K score, Hyodo–Komagane score; GR score, 10-s grip and release test; JOA score, Japanese Orthopaedic Association score.
Correlation of Dysphagia Pre- and Postoperatively
In this analysis, with an increased number of cases compared with our previous report, a significant positive correlation was found between pre- and postoperative H‒K scores (r = 0.51, P < 0.0001; Figure 1). Significant positive correlation between pre- and postoperative H‒K scores. H‒K score, Hyodo–Komagane score.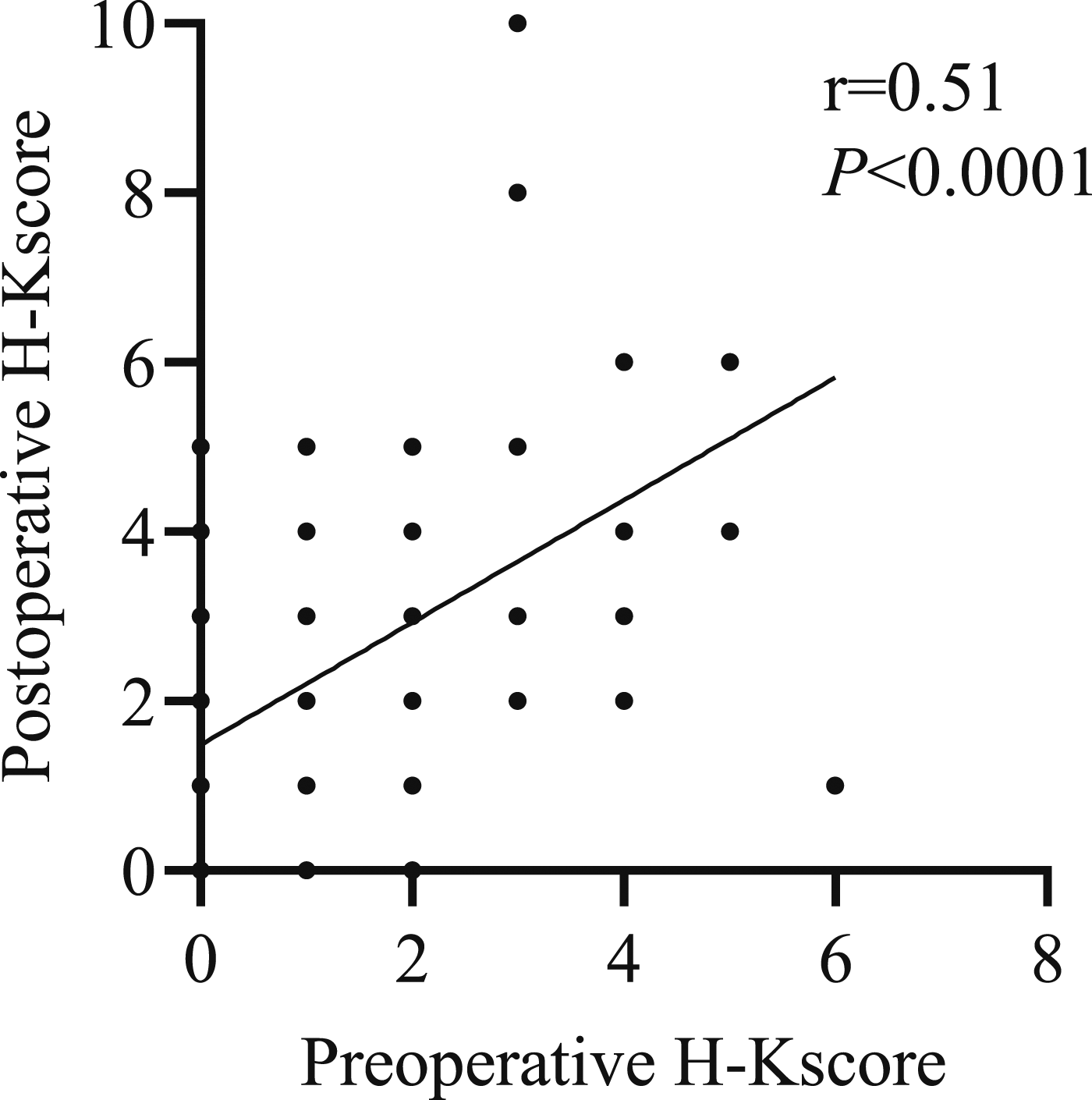
Figure 2 shows a typical case of postoperative dysphagia without abnormal findings on swallowing function tests preoperatively and H–K score, indicating subclinical dysphagia. Representative case of preoperative subclinical dysphagia and postoperative dysphagia (A) Swallowing function test was normal preoperatively, but abnormal postoperatively. (B) Pre- and postoperative videos of flexible endoscopic evaluation of swallowing and H–K score.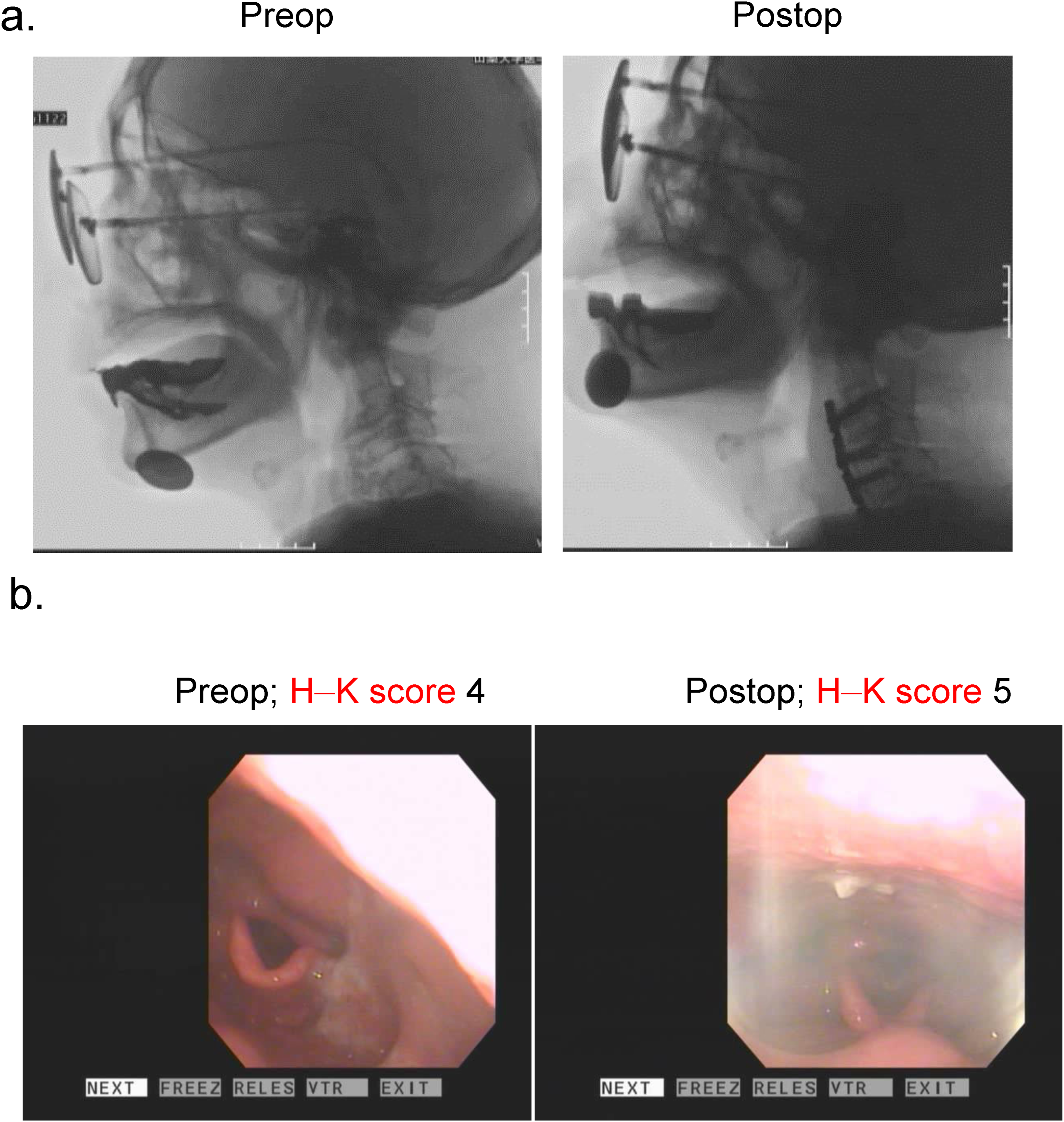
Discussion
Screening methods for dysphagia can be categorized into patient-reported questionnaires and objective assessments performed by clinicians, such as video fluoroscopic swallowing studies or FEES. Questionnaire-based evaluations are relatively simple and non-invasive, and there are reports suggesting their usefulness in screening for aspiration risk. However, as they rely solely on the patient’s subjective perception, there is a possibility of overlooking silent aspiration risks.15,19 The H-K score is a swallowing evaluation system established for its utility and reliability in the field of otolaryngology. It involves otolaryngologists observing patients’ swallowing of colored water under fiberoptic endoscopic examination and scoring the results.1,11,12,16 In this study, we used both the patient-reported questionnaire EAT-10 and the H-K score, an objective assessment performed by otolaryngologists.We evaluated 14/92 (15.2%) patients as having dysphagia by using a preoperative endoscopic swallowing test. In contrast, we evaluated patients using EAT-10, which revealed the likelihood of symptomatic dysphagia, indicating a discrepancy between patients’ subjective and clinician’s objective assessments, implying the existence of asymptomatic dysphagia that patients were unaware of because of the nature of their disorder. Importantly, we have previously reported that preoperative asymptomatic dysphagia was highly correlated with postoperative respiratory complications. 14 Most previous studies of dysphagia in the spine have used a subjective patient assessment alone, which may have limited accuracy. Importantly, preoperative asymptomatic dysphagia was highly correlated with postoperative dysphagia. Previous reports have identified male sex, older age, smoking, chronic obstructive pulmonary disease, asthma, and diabetes as risk factors for patients with dysphagia and respiratory complications.20,21 We also examined respiratory function and found no association between the patient’s pre-existing medical conditions and dysphagia, except for older age. Finally, the GR test and upper extremity function and BBD items among the C-JOA were only significantly correlated with H‒K scores.
Dysphagia is commonly caused by mechanical obstruction, but other important factors, such as anatomic, infectious, inflammatory, and neuromuscular diseases can all cause or contribute to dysphagia. Several studies have reported dysphagia in neuromuscular diseases such as Huntington’s disease, Parkinson’s disease (PD), amyotrophic lateral sclerosis (ALS), and spinal muscular atrophy (SMA). In a report investigating the mechanism of dysphagia in SMA, pharyngeal residuals were found in videofluoroscopic swallowing studies. Furthermore, abnormal echoes of the tongue were observed on muscle ultrasonography, and dysphagia was associated with mastication disorders. 22 A recent cohort study of patients with ALS reported that more than half had dysphagia 23 Additionally, dysphagia occurs at a high rate after cervical spine surgery in patients with comorbid PD. 24 These reports showed a close relationship between the mechanisms of dysphagia and neuromuscular disease. However, the impact of neuropathy caused by CSM on dysphagia has not been elucidated yet. To the best of our knowledge, this is the first study to report the relationship between the severity of myelopathy and pre- and postoperative dysphagia in patients with CSM. The present study suggests that postoperative dysphagia and respiratory complications require attention in patients with severe myelopathy who will undergo surgery.
Conclusion
This study suggests that advanced age and severe preoperative upper limb and bladder dysfunction are risk factors for dysphagia in patients with cervical myelopathy requiring surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.