
Abstract
Study Design
Cross-Sectional Survey.
Objective
This study aimed to assess racial disparities in self-reported barriers to care, health literacy, and health status within a large cohort of cervical stenosis patients.
Methods
This cross-sectional study used ICD-9 and ICD-10 codes to identify cervical stenosis patients recorded in the NIH All of Us Research Program between 2017 and 2022. Demographic information and self-reported measures of health status, health literacy, and perceived barriers to care were compared among White, Black, and Hispanic patients using Chi square tests.
Results
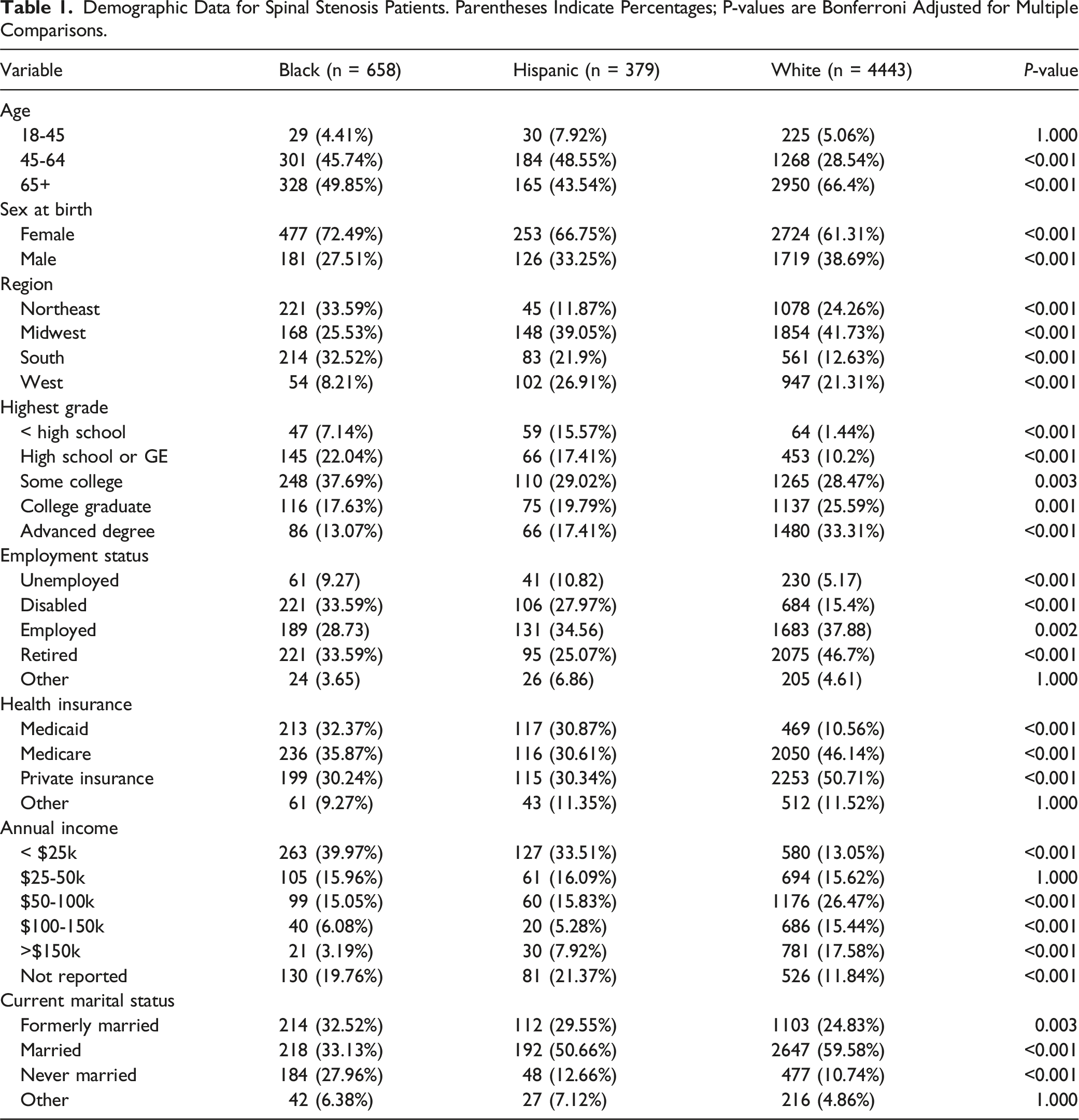
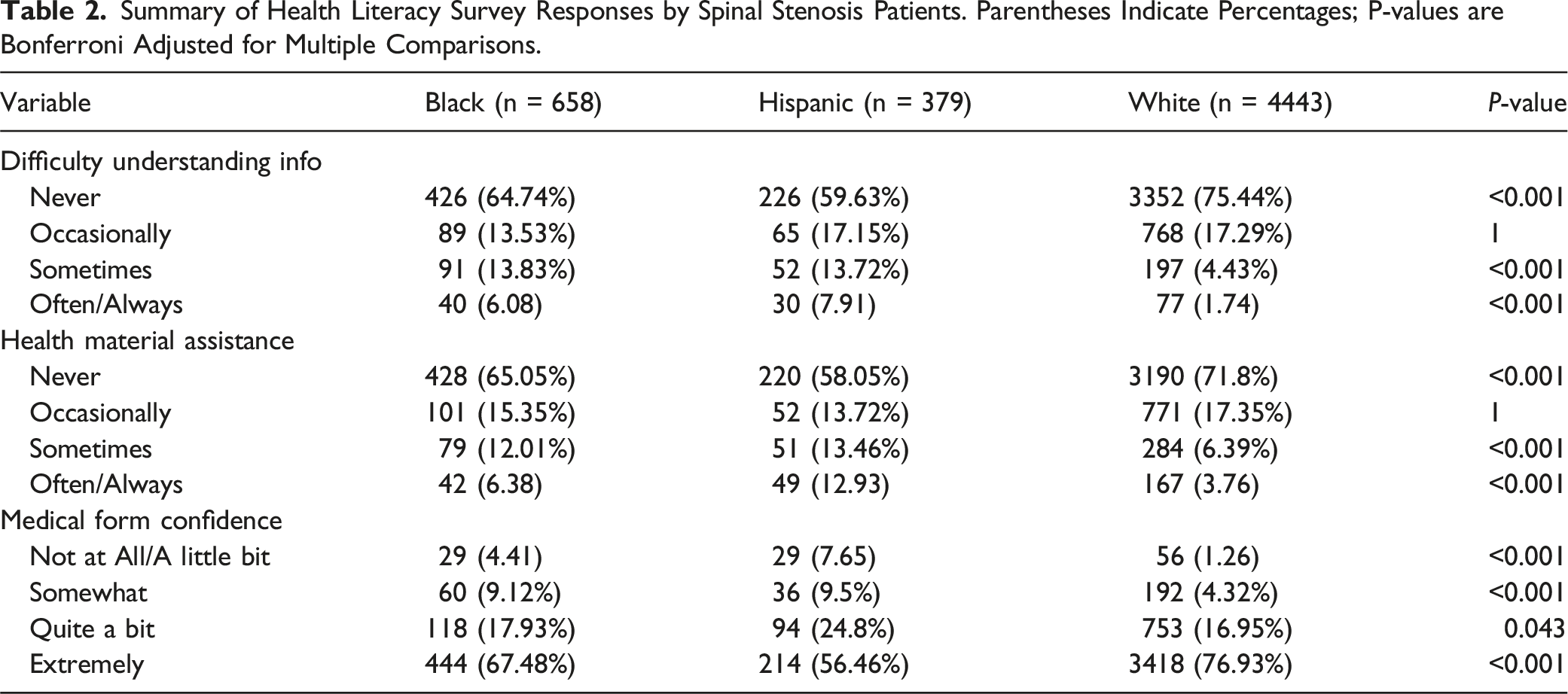
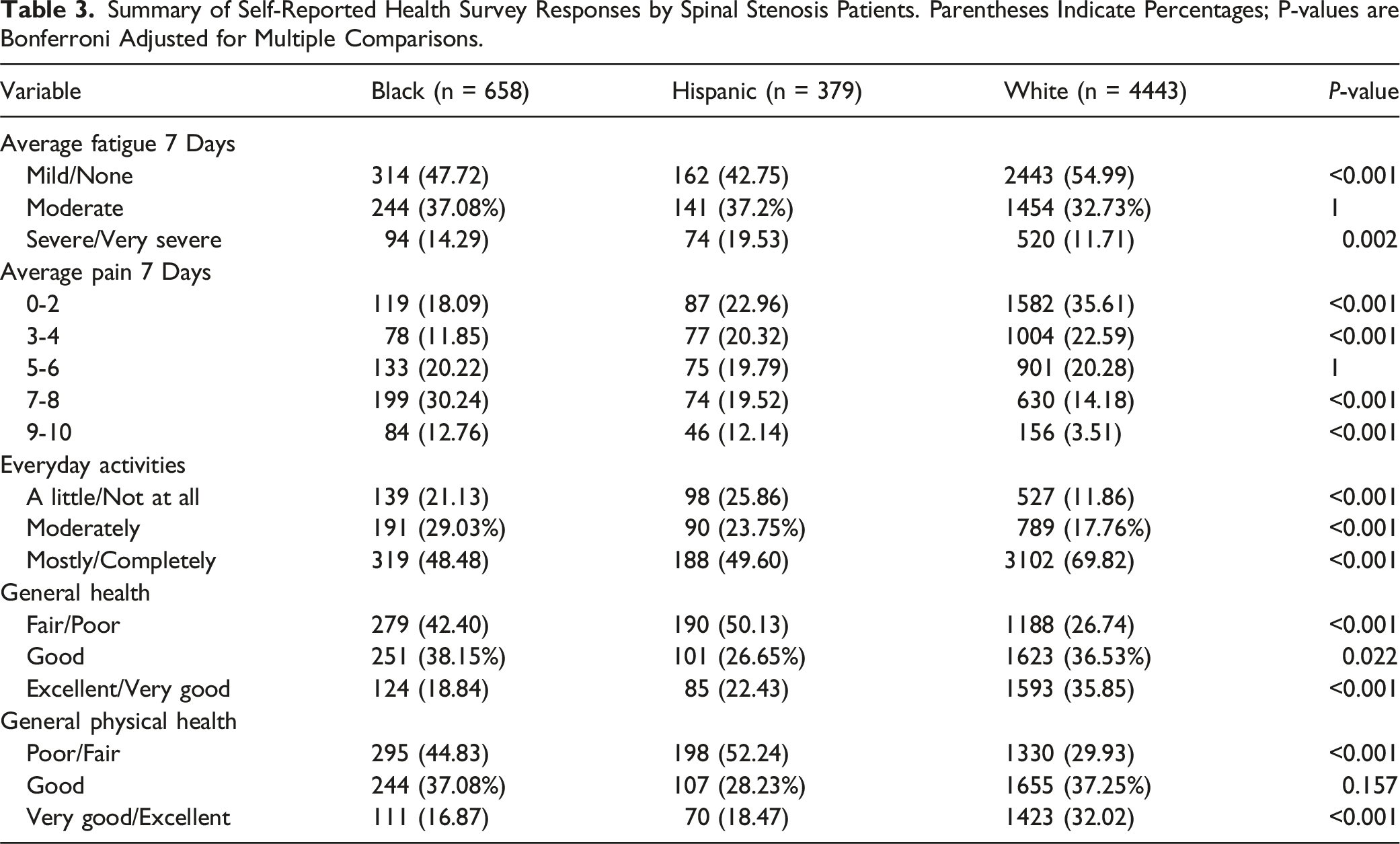
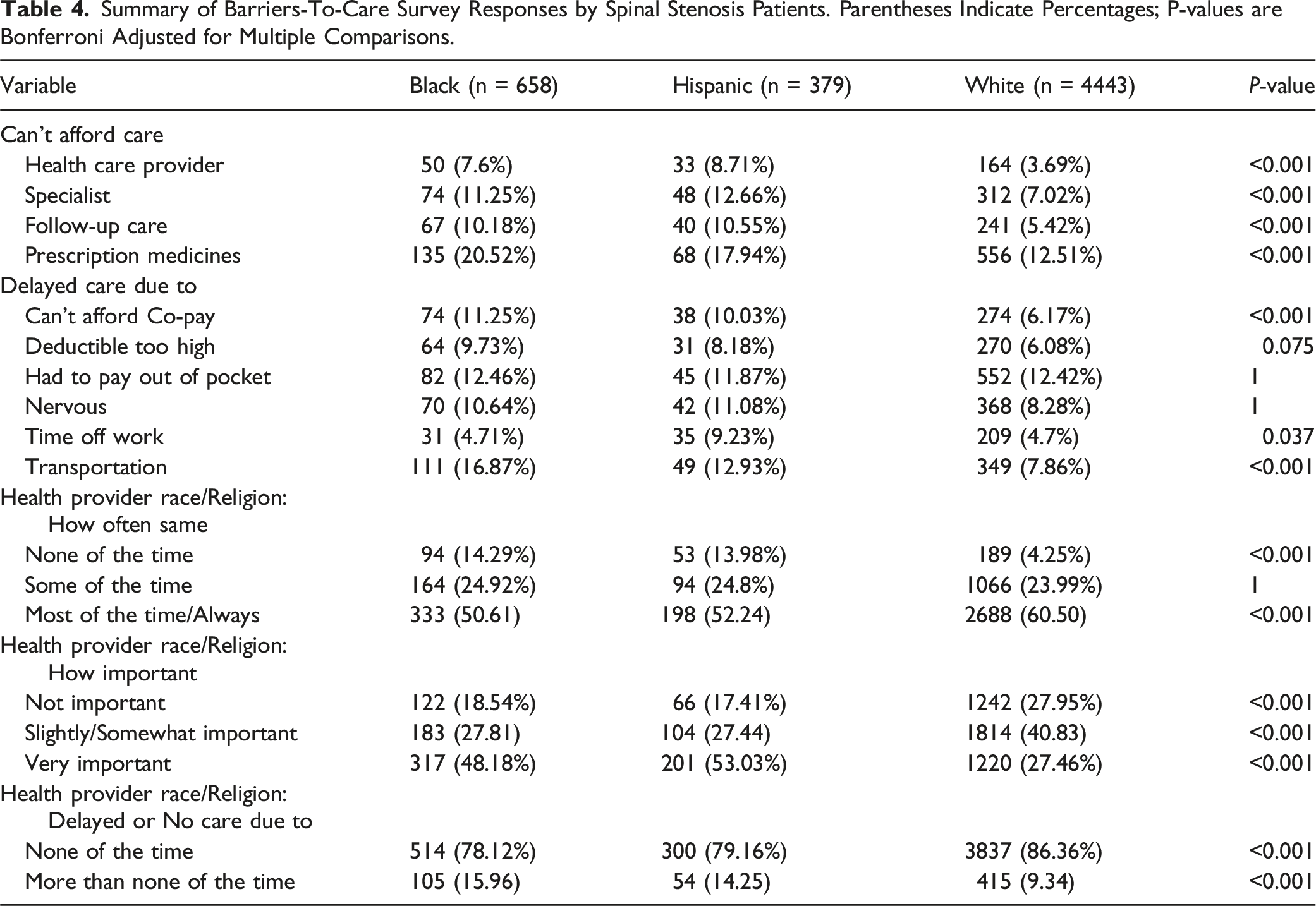
Of 5480 patients identified, 658 (12.0) were Black, 379 (6.9) Hispanic, and 4443 (81.1) White. White patients were more likely to possess college education (P < .001), income >$50k per year (P < .001), and non-disabled employment status (P < .001). Black and Hispanic patients reported higher levels of 7-10 pain (P < .001), “severe” 7-day fatigue (P < .001), and poor general health (P < .001). Black and Hispanic patients also reported greater difficulties understanding medical information (P < .001) and navigating medical forms alone (P < .001). Black and Hispanic patients were likelier to report delaying care due to unaffordable copays (P < .001), transportation difficulties (P < .001), or dissimilar provider background. Provider background was more likely to be described as “very important” by Black and Hispanic patients (P < .001).
Conclusion
This study identified significant disparities in health status, health literacy, and access to care among patients with cervical stenosis, highlighting diverse patient perspectives on barriers to care which may warrant further study.
Introduction
The narrowing of the spinal canal or foraminal spaces, also known as spinal stenosis, is a common imaging finding in the elderly. 1 Epidemiological data suggests that cervical spine stenosis has an incidence rate of 1 case per 100,000. 1 Narrowing of the spinal canal in cervical stenosis can lead to direct pressure on the spinal cord, causing cervical myelopathy. 2 Symptoms can manifest as neck pain, radiating arm pain, numbness or tingling in the arms and hands, upper extremity weakness and difficulty with balance and coordination. 3 Proper diagnosis of cervical stenosis requires imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI), and effective treatment of symptomatic cervical stenosis often involves surgical decompression procedures such as laminectomy, foraminotomy, discectomy, and corpectomy. While cervical stenosis itself is often asymptomatic, delays in diagnosis can lead to progression to potentially debilitating conditions such as radiculopathy or degenerative cervical myelopathy (DCM) wherein extended duration of symptoms have been repeatedly identified as predictors of worsened surgical outcomes.4-6 Moreover, even in non-surgically treated spinal stenosis patients, symptom duration of >12 months has been described as a predictor of reduced improvement in SF-36 Bodily Pain (BP), SF-36 Physical Function (PF), and Oswestry Disability Index (ODI). 7 Therefore, identifying and reducing barriers to care can provide increased access to these essential diagnostic and therapeutic services, improving the management and outcomes of patients with cervical stenosis.
Existing literature has thoroughly documented the persistent racial disparities which degenerative cervical spine disease patients face. Das et al 8 found that white patients were less likely to present with symptomatic manifestations of cervical stenosis such as myelopathy, plegia, and bowel-bladder dysfunction, in comparison to Black and Hispanic patients. Similarly, Schoenfeld et al 9 described higher baseline SF-36 BP, SF-36 PF, ODI, and Stenosis Bothersomeness Index in Black patients with spinal stenosis. One possible explanation for these differing presentations may lie in the reduced rate of surgical treatment for patients of minority races due to limitations accessing high-volume hospitals and outpatient surgical centers.8,10,11 Notably, a 2016 retrospective cohort study of 133 patients undergoing elective anterior cervical discectomy and fusion (ACDF) surgery found that black patients experienced disproportionate delay in the diagnosis and treatment of symptomatic cervical stenosis. 12 Moreover, such delays in treatment have been shown to persist even when adjusting for socioeconomic and community disadvantage. 13
Yet, there has been relatively limited investigation into the causes of racial disparities in time to treatment for patients with degenerative diseases of the cervical spine. Pope et al described in a cohort of 778 DCM patients that race alone predicted diagnostic delay while sex, age, county of residence, education status, and household income did not. 14 Similarly, Elsamidicy et al in a cohort of 133 cervical stenosis patients identified only race as a significant predictor for duration of symptoms prior to ACDF. 12 Employment status, marital status, age, anxiety, and baseline VAS neck pain all failed to meaningfully predict time to treatment in their cohort. Self-reported barriers to care remain understudied. One opportunity to identify the causes of existing disparities may lie in the All of Us Research Program, a database which collects a range of patient data including access to care surveys. 15 In this study, we used International Classification of Diseases (ICD) codes to query the All of Us database for patients diagnosed with cervical stenosis and investigated potential racial disparities in self-reported barriers to care.
Materials and Methods
Ethical Considerations
This study was exempt from institutional review board approval as data from the All of Us Research Program is de-identified. The requirement for informed consent did not apply due to the anonymized nature of the database. Approval for the original All of Us Research program was provided by the All of Us Institutional Review Board of the National Institutes of Health.
Study Design
The All of Us Research Program is a prospective cohort study funded by the National Institutes of Health (NIH) which collects data through self-reported surveys, Electronic Health Record, and biophysical sensors such as Fitbit. 16 The All of Us Research Program institutional review board approved all study procedures prior to database publication. This cross-sectional study was conducted on version 7 of the database using the All of Us Researcher Workbench and involved a cohort of cervical spinal stenosis patients. Patients were identified using ICD codes 723.0, 721.1, and 722.71 from ICD9 and M48.02, M47.12, and M50.0 from ICD 10. To ensure sufficient demographic sample sizes, only participants with racial identities of White, Black, and Hispanic or sex at birth categories of male and female were retrieved. Additionally, participants identifying as multiracial were excluded. These steps were taken to ensure compliance with the All of Us data reporting standards which prohibit reporting of data involving less than 20 participants. 16
Participants were subsequently stratified into Hispanic, Black race alone, and White race alone ethno-racial categories, using methods described in previous studies. 17 Self-perceived barriers to care were identified using survey questionnaires maintained by the All of Us Research Program. Utilized questionnaires included the physical health portion of the Patient-Reported Outcomes Measurement Information System (PROMIS-10) Global Health scale, the Brief Health Literacy Screen (BHLS), and All of Us internal questionnaires relating to self-perceived barriers to care.18-20 In addition, demographic information including sex, employment status, insurance status, marital status, and education level was retrieved. Participants were able to skip individual surveys and questions. Thus, to ensure complete cases, participants with missing surveys were excluded from analysis and answers of “Skip” and “I Don’t Know” were not reported in stratified survey counts. Exact questionnaire wording can be found within the All of Us data tools hub (https://www.researchallofus.org/data-tools/).
In order to assess objective health utilization across cohorts, rates of surgical intervention in the 2 years following diagnosis were retrieved using Current Procedural Terminology (CPT) codes described by Waddell et al. 21 The CPT codes used to assess surgical intervention included those for anterior cervical discectomy and fusion (ACDF) (22551, 22554, 63075, 22552, 22585), anterior corpectomy (63081, 63082), laminectomy (63001, 63015, 63045, 63048), posterior fusion (22600, 22614), posterior discectomy (63020, 63040, 63035, 63043), laminoplasty (63050, 63051), and cervical disk arthroplasty (22856, 22858). Potentially relevant prescribed medication classes was also retrieved using Anatomical Therapeutic Classification (ATC) codes for muscle relaxants (M03), opioids (N02 A), non-opioid analgesics (N02 B), corticosteroids (H02), and gabapentin (N03AX12). 22
Statistical Analysis
Survey data were compared between stratified cohorts using Chi-square tests when expected values were >5 and Fisher exact tests when expected values were below 5. Additional post hoc Chi-square pairwise tests comparing White patients to Black or Hispanic patients were conducted for groups with significant differences. Missing data were excluded from analysis. All P-values are shown adjusted following application of a Bonferroni correction to reduce risk of false discovery. P-values of P < .05 were considered significant. All data analysis was performed within the All of Us Researcher Workbench using R Studio version 4.2 and Python 3.
Results
Demographic Data for Spinal Stenosis Patients. Parentheses Indicate Percentages; P-values are Bonferroni Adjusted for Multiple Comparisons.
Summary of Health Literacy Survey Responses by Spinal Stenosis Patients. Parentheses Indicate Percentages; P-values are Bonferroni Adjusted for Multiple Comparisons.
Summary of Self-Reported Health Survey Responses by Spinal Stenosis Patients. Parentheses Indicate Percentages; P-values are Bonferroni Adjusted for Multiple Comparisons.
Summary of Barriers-To-Care Survey Responses by Spinal Stenosis Patients. Parentheses Indicate Percentages; P-values are Bonferroni Adjusted for Multiple Comparisons.
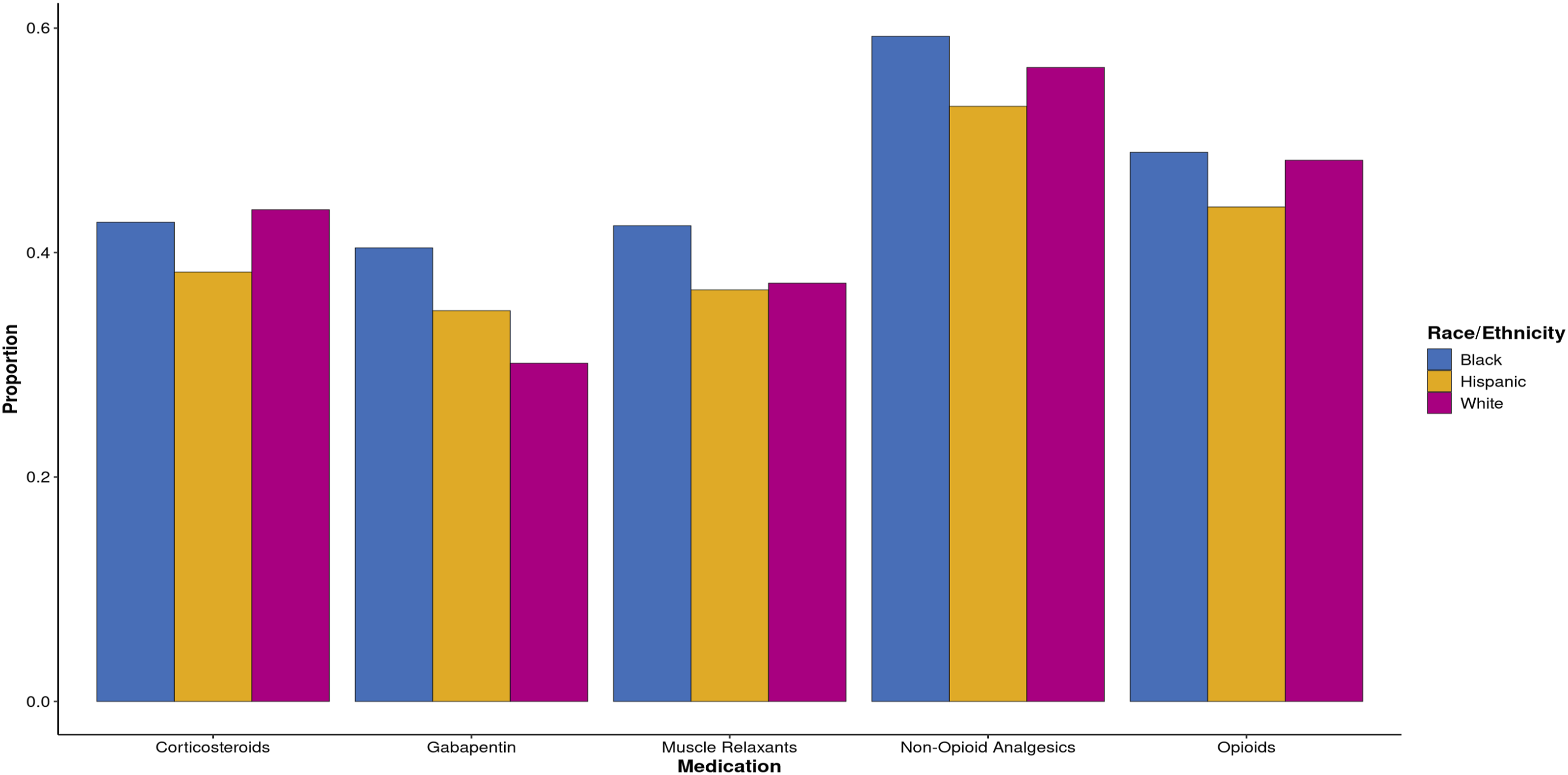
Objective utilization of medication and surgery in the 2 years following diagnosis were subsequently assessed using several CPT and ACT codes (Figures 1 and 2). The overall rate of surgical intervention was 5.6%, including 4.3% for Black patients, 5.0% for Hispanic patients, and 5.9% for white patients. Anterior approach was more common than posterior approach in all cohorts including Black (71.4%), Hispanic (63.2%), and White (64.1 %) patients. A predominance of multilevel interventions were observed in Black (57.1%), Hispanic (78.9%), and White patients (63.3%). The most common procedure was ACDF (53.2%), followed by posterior cervical fusion (20.5%), and laminectomy (16.2%). Several medications were relatively common, with 56.6% of patients receiving non-opioid analgesics, 48.0% of patients receiving an opioid, 43.3% of patients receiving a corticosteroid, 37.8% receiving a muscle relaxant, and 31.7% receiving gabapentin. Proportion of Patients Receiving Surgery by Race. Proportion of patients receiving surgery is shown, subdivided by approach, patient race, and single or multilevel operation. Proportion of Patients Receiving Medication by Race. The proportion of patients receiving several considered medications including gabapentin, corticosteroids, muscle relaxants, non-opioid analgesics, opioids is shown.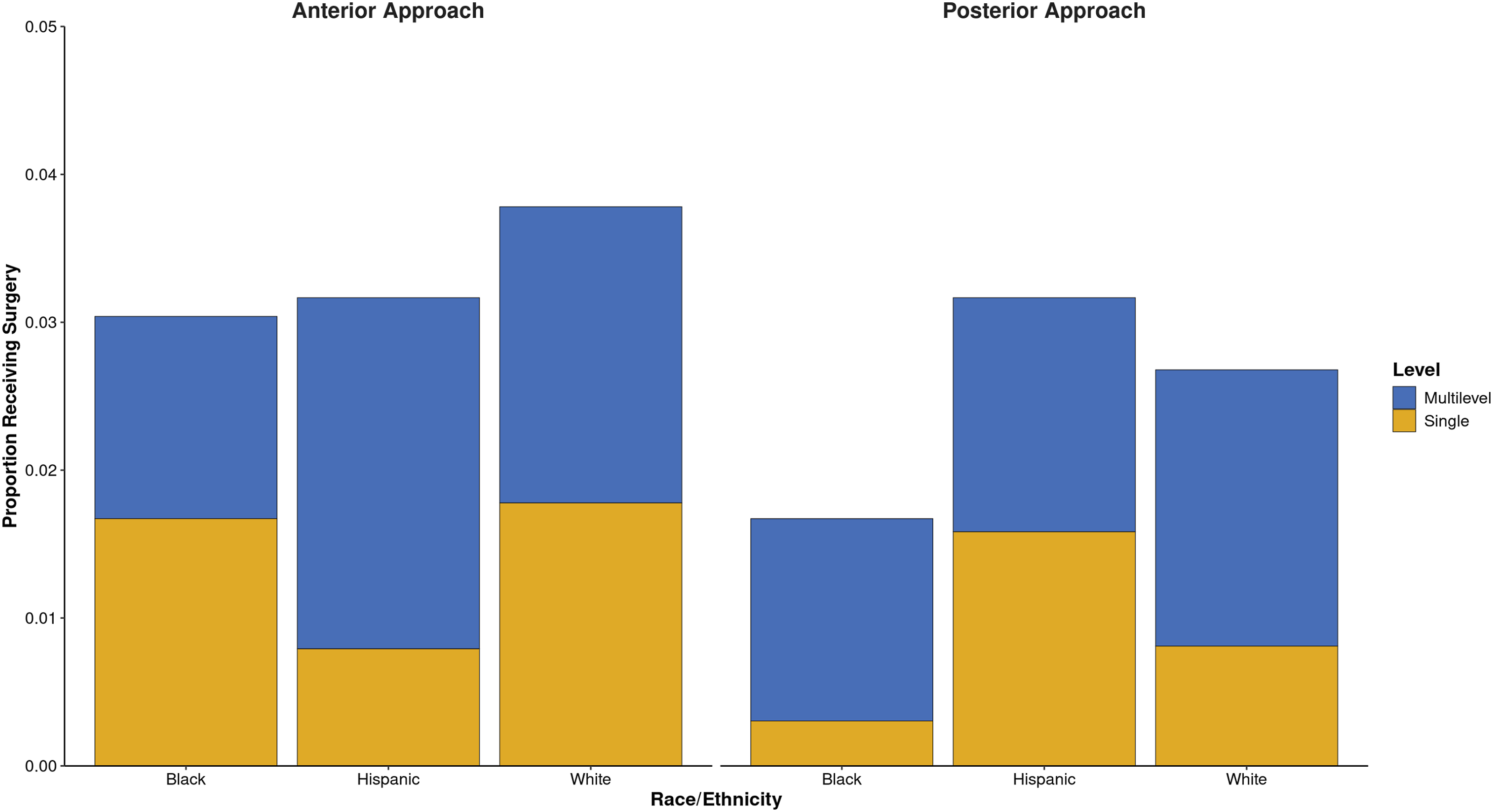
Discussion
Racial disparities in the quality of life (QOL) and post-operative outcomes of patients with degenerative spine disease continue to exist, despite extensive research and quality improvement efforts by surgeons in the past decade. 23 This cross-sectional study of cervical spinal stenosis patients identified racial disparities in the rates of several possible self-reported causes of delay in care. Among the many causes of delayed care highlighted by our study, the largest differences between racial groups were identified for non-concordant patient-provider backgrounds, transportation difficulties, and affordability of co-pays. In this study we identified large gaps in health literacy and perceived health status when comparing the investigated racial cohorts. Collectively, these insights provide a preliminary characterization of the diverse patient perspectives present within a large cohort of spinal pathology patients commonly referred for surgery.
Perceived health status and other patient-reported outcome measures have increasingly been considered as potential outcome measures in the treatment of spinal stenosis.24-27 Yet, despite the utility for predicting outcomes and patient satisfaction, PROMIS scores at intake have not been associated with the decision to pursue spinal surgery. 27 Elsamidicy et al previously identified in a cohort of 345 patients undergoing elective lumbar spine surgery significantly poorer baseline and post-operative ODI, visual analog scale for back pain, and visual analog scale for leg pain among black patients relative to white patients. 28 Our study replicated these findings, with Black and Hispanic patients in our cohort reporting substantially higher pain and impairment of everyday activities than White patients. Such disparities in patient reported pain and function underscore the importance of further study into the interaction of race with perioperative care planning and, naturally, the corresponding optimal management.29-31
Barriers to care may serve as an important mediator of the relationship between minority status and worsened outcomes. While few studies have investigated self-reported barriers among patients with degenerative disease of the cervical spine, Bove et al 32 previously identified transportation as the most frequently cited barrier to treatment in a cohort of fifty patients with lumbar spinal stenosis. While our study replicated this finding, it also identified out of pocket costs, dissimilar provider, and cost of prescription medications as widely cited barriers across racial and ethnic groups. The elevated prevalence of transportation barriers reported by patients of Black race present an interesting adjunct to prior studies showing Black race as a strong negative predictor of the geospatial distribution of cervical spine fusions. 13 This and other barriers to care identified by patients our study may help account for previously noted inequities, such as the higher rate at which minority patients undergo operation at low volume spine centers.10,33
Health literacy has previously been described as a predictor of health related QOL among spine patients at baseline.34,35 For operated cases as well, health literacy has been shown to predict post-operative PROMs such as pain and anxiety.35,36 Yet, the role of health literacy in delay of treatment for cervical stenosis and its resulting functional impairments has been relatively under-investigated. One recent retrospective cohort of 1141 cervical spondylotic myelopathy patients identified patients with low education levels as having an elevated risk of increased pre-operative symptom duration and intensity, higher post-operative neck disability index, and lower post-operative quality-adjusted life years. 37 Whatever the cause, when they do present for ACDF Black and Hispanic patients appear to demand more extensive resource utilization, greater length of stay, and higher likelihood of non-routine discharge. 38 Further investigation will be required to validate the relevance of between group differences in health literacy on cervical stenosis outcomes.
Importantly, despite the several self-reported barriers to care identified in our cohort, our study does not conclusively establish a relationship between subjective barriers, such as perceived discrimination, transportation difficulties, or financial challenges, and the objective utilization of health services. Observed rates of conservative and surgical interventions were broadly similar to those of previous studies such as the Davison et al. 22 ’s 2007-2017 cervical stenosis cohort, which identified NSAID utilization in 36.7% of patients, opioid use in 59.2%, muscle relaxant use in 38.2%, and surgical intervention in 7.4%. While Black and Hispanic patients showed lower absolute utilization of surgical procedures, they also showed higher utilization of some medication treatments such as gabapentin. Future studies which assess the association of self-reported barriers with utilization or health outcomes and control for confounding factors will be required to define any relationship between subjective barriers and objective health consumption.
Limitations
Several limitations must be noted for our study. First, inherent to any analysis of cross-sectional survey data is the possibility of recall bias or social desirability bias. Similarly, our use of ICD codes to identify spinal stenosis patients and CPT/ATC codes to measure health utilization could have introduced coding or reporting bias. Moreover, the retrospective nature of our study limits our ability to analyze confounding factors. We cannot follow up on incomplete data with regard to self-reported barriers to care. Lastly, only participants who completed at least one question from the surveys were considered for our analysis. Non-responders to individual surveys may have differed meaningfully from those who did complete all surveys, leading to a non-representative sampling of patients. Our inability to investigate Asian populations presents a key area of non-representativeness, particularly given suggestions that this population may be uniquely predisposed to DCM. 39 However, with only 90 individuals of Asian descent identified in our initial study cohort, All of Us data reporting guidelines prevented meaningful analysis of this population.
Despite these limitations, to our knowledge this is the largest cohort study to investigate self-reported barriers to care among cervical stenosis patients, providing valuable insights into the possible socioeconomic disparities present in this spinal pathology cohort.
Conclusion
In this study of cervical spinal stenosis patients, we found that Black and Hispanic participants were more likely to self-report delays in care due to a variety of causes, including cost of follow-up appointments, transportation challenges, and inability to access physicians of a similar background. Moreover, we identified disparities in self-perceived health literacy and overall health to the detriment of Black and Hispanic patients. The inequities observed in this study provide promising avenues for future research into previously described outcome gaps between cervical stenosis patients of different races.
Footnotes
Acknowledgments
We gratefully acknowledge All of Us participants for their contributions, without whom this research would not have been possible. We also thank the National Institutes of Health’s All of Us Research Program for making available the participant data examined in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.