
Abstract
Study Design
Retrospective cohort study.
Objective
To determine association between preoperative Patient-Reported Outcomes Measurement Information System Physical Function (PROMIS-PF) scores with postoperative pain, narcotics consumption, and patient-reported outcome measures (PROMs) following single-level lumbar microdiscectomy.
Methods
Consecutive patients who underwent single-level lumbar microdiscectomy were identified from May 2017–May 2020. Patients were grouped by their preoperative PROMIS-PF scores: mild disability (score≥40), moderate disability (score 30-39.9), and severe disability (score<30). Preoperative PROMIS-PF subgroups were tested for association with inpatient postoperative pain, total inpatient narcotics consumption, time to narcotic use cessation as well as improvements in postoperative PROMIS-PF, ODI, VAS-Leg Pain, VAS-Back Pain, SF-12 Physical Component Score (PCS), SF-12 Mental Component Score (MCS) at 2-, 6-, 12-weeks, 6-month, 1-year, 2-year follow-up.
Results
A total of 127 patients were included. Patients with greater disability reported higher inpatient maximum Visual Analog Scale (VAS) pain scores (P = .023) and total inpatient narcotics consumption (P = .008) but no difference in time to narcotic cessation after surgery (P = .373). However, patients with greater preoperative disability also demonstrated greater improvement from baseline in PROMIS-PF, ODI, SF-12 PCS, and SF-12 MCS at 2-week follow-up (P < .05). These higher improvements from baseline for patients with greater preoperative disability were sustained for PROMIS-PF, ODI, and VAS-Leg Pain at 2-year follow-up (P < .05)
Conclusions
Patients with greater preoperative disability, as measured by PROMIS-PF, had increased inpatient postoperative pain and narcotics consumption, but also higher improvement from baseline in long-term PROMs. This data can be utilized for patient counseling and setting expectations.
Keywords
Introduction
In the current healthcare environment of quality metrics and value-based care, patient reported outcome measures (PROMs) have become a valuable instrument to quantitatively measure clinical data before and after surgery.1,2 This is especially true in spine surgery where cost of care is high and the ability to define “effectiveness” of surgical intervention is therefore of vital importance. 3 The Patient Reported Outcomes Measurement Information System (PROMIS) has recently emerged as a valuable instrument in assessing patient health pre- and post-operatively. 4
The PROMIS instrument contains several domains including pain intensity, pain interference, physical function, fatigue, sleep disturbance, anxiety, depression, and social health. 5 In the spine literature, the PROMIS-Physical Function (PF) domain is especially applicable as it measures patients’ strength, mobility, and coordination.6-9 Compared to legacy outcome measures, the main advantage of PROMIS is that it allows for improved psychometric properties with reduced questionnaire burden for the patient. However, while various preoperative legacy outcome measures have been successfully correlated with surgical outcomes, the association between preoperative PROMIS-PF and outcomes after spine surgery is currently understudied in the literature.
Postsurgical outcome measures of major interest to spine surgeons and patients include postoperative pain and narcotics utilization.10-14 These variables are especially important to consider for ambulatory procedures, 15 such as lumbar microdiscectomy, since they may dictate case order, possible overnight admission, and outpatient opioid prescriptions. Currently, data on clinical utility of preoperative PROMIS-PF in predicting immediate postoperative pain, narcotics consumption, and other long-term PROMs after lumbar microdiscectomy is lacking.
Therefore, the main purpose of the current study was to determine any association between preoperative PROMIS-PF with immediate postoperative patient pain, narcotics consumption, and long-term PROMs after lumbar micro-disectomy.
Methods
Study Design and Population
A retrospective review of prospectively collected data from a single-surgeon surgical database May 2017–May 2020 was performed. The surgeon completed a residency in Orthopedic Surgery followed by a fellowship in spine surgery, and has been in practice at high-volume academic centers for 12 years, performing over 300 surgeries annually. The first assist was a spine fellow for over 85% of cases while in the remaining cases, it was an orthopaedic surgery resident.
Consecutive patients who underwent single-level lumbar discectomy for degenerative pathologies were selected. The procedures were performed using a tubular retractor system and an operating microscope. Details of the surgical techniques has been extensively described in previous publications.16,17 Patients who had multi-level procedures or prior surgery at that level were excluded. All patients underwent the same standard perioperative pain regimen through a standard postoperative spine pathway. The standard perioperative pain regimen included scheduled around-the-clock acetaminophen, an oxycodone or tramadol panel, and hydromorphone intravenous injection for breakthrough pain. A total of 127 patients were identified. Patients were grouped by their preoperative PROMIS-PF scores: mild disability (score≥40), moderate disability (score 30-39.9), and severe disability (score<30). These cutoffs were based on previous literature. 18 Institutional review board (IRB) approval was obtained for this study.
Data Collection
Data was collected and managed using REDCap (Research Electronic Data Capture)19,20 hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the following grant: CTSC GRANT UL1 TR002384. REDCap is a secure, HIPAA-compliant web-based software platform designed to support data capture for research studies. Patient demographics, comorbidities, operative factors, postoperative data, and PROMs were obtained from review of electronic medical records and REDCap.
Demographics and comorbidities data included age, gender, body mass index, insurance, smoking status, Charlson comorbidity index (without age), percentage back pain, percentage radiculopathy, preoperative depression, and preoperative anxiety.
Operative factors included operative level, operative time (minutes) and estimated blood loss (cc). Postoperative data included length of stay (in hours), average postoperative day (POD) 0 pain score (measured by Visual Analog Scale [VAS]), maximum POD 0 pain score (measured by VAS), total inpatient narcotics consumption (measured by Oral Morphine Equivalents [OME]), and time to narcotic discontinuation (measured in days). Average POD 0 pain score and maximum POD 0 pain score were stratified into >75th percentile versus ≤75th percentile.
Lastly, PROMs were recorded preoperatively and at 2-weeks, 6-weeks, 12-weeks, 6-months, 1-year, and 2-year follow up visits. Of note, not all patients had 2-year follow-up data as the study period concluded prior to follow-up completion. 37 patients had 2-year follow-up data for PROMs. Assessments included the PROMIS-PF, Oswestry Disability Index (ODI), Visual Analog Scale (VAS) - Back Pain, VAS - Leg Pain, Short Form 12 - Physical Component Score (SF12 - PCS), and SF12 - Mental Component Score (SF12 - MCS). These PROMs have all been validated for use in this patient population. 7
Statistical Analysis
Patient demographics, comorbidities, operative factors, postoperative data, radiographic parameters, and PROMs were summarized using descriptive statistics. Categorical variables were summarized as “number (percentage)” while continuous variables were summarized as “mean ± standard deviation”.
Patient demographics, comorbidities, operative factors, postoperative data, and PROMs (at pre-op, 2 weeks, 6 weeks, 12 weeks, 6 months, 1 year, and 2 year follow up) were compared between the preoperative PROMIS-PF sub-groups. For each of the six studied PROMs, the average change from baseline to each follow-up period was compared between the preoperative PROMIS-PF sub-groups. Categorical variables were compared using Pearson’s Chi Square tests or Fisher’s exact tests, as appropriate. Continuous variables were compared using Analysis of Variance or Kruskal–Wallis H test, as appropriate.
To further determine the clinical significance of changes as measured on these PROMs, the minimal clinically important difference (MCID) was determined for each instrument. The distribution-based method, as previously described in the literature,21,22 was used in this study. Briefly, the threshold for achieving the MCID for each instrument was determined by calculating the change in outcome equal to .5 standard deviation over a 1-year period. We considered any patient who met this threshold at 1-year follow-up to have reached the MCID. We had chosen 1-year follow-up in the MCID analysis as we had a higher number of patients with complete 1-year follow-up. In addition, recent studies have shown that PROMs at 1-year following lumbar spine surgery accurately predict those at 2-year follow-up.23,24
Multivariable Poisson regressions with robust error variance were used to determine the association between preoperative PROMIS-PF subgroups and achieving MCID in each PROM at 1-year follow-up while controlling for demographic differences (P < .50), which include gender, body mass index, and preoperative anxiety, identified on univariate analysis.
Statistical significance was set as P < .05. All statistical analyses were performed using STATA version 13 (StataCorp LP, College Station, TX).
Results
Patient Demographics and Comorbidities
Patient demographic and perioperative characteristics.
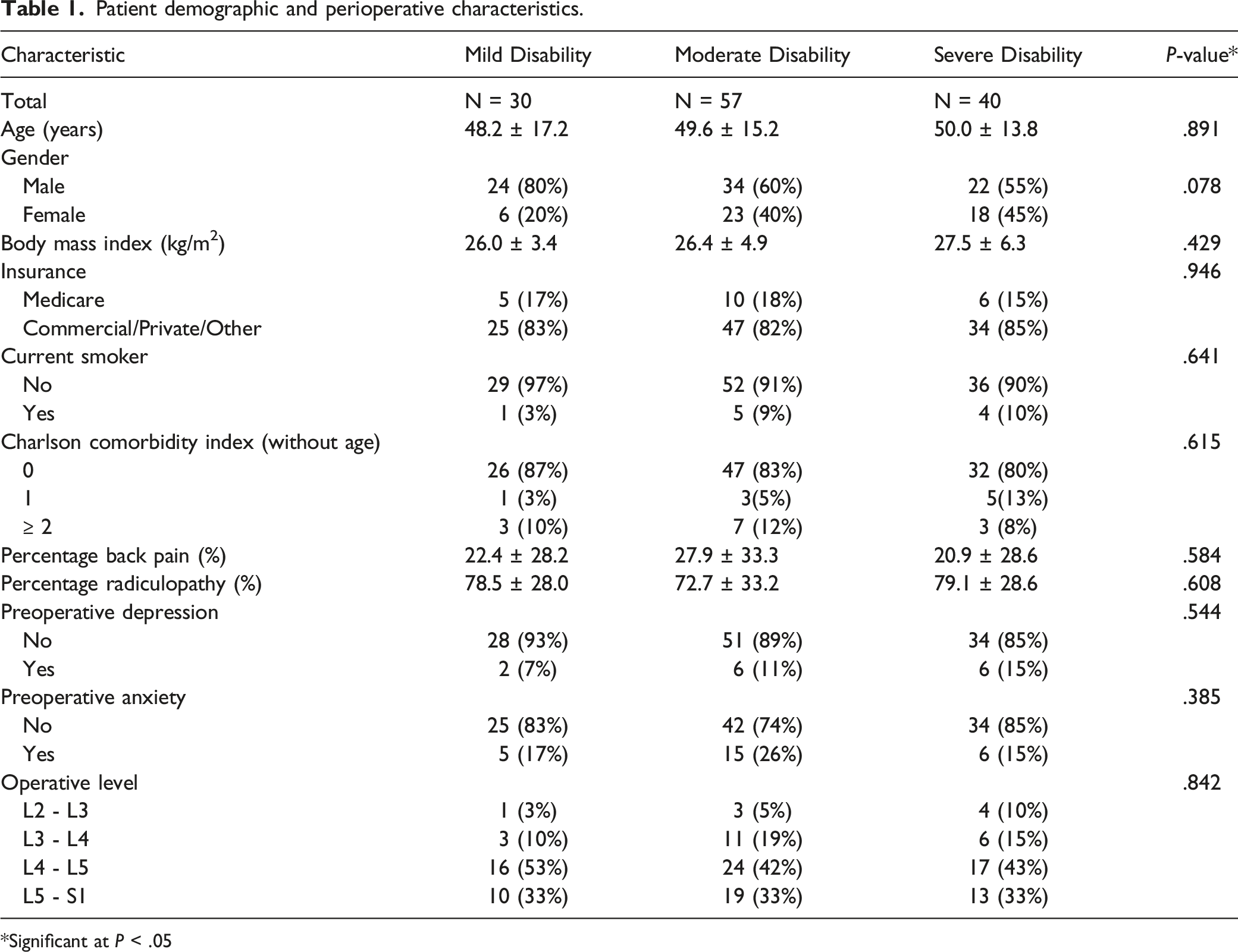
*Significant at P < .05
Operative Characteristics and Postoperative Outcomes
Perioperative outcomes.
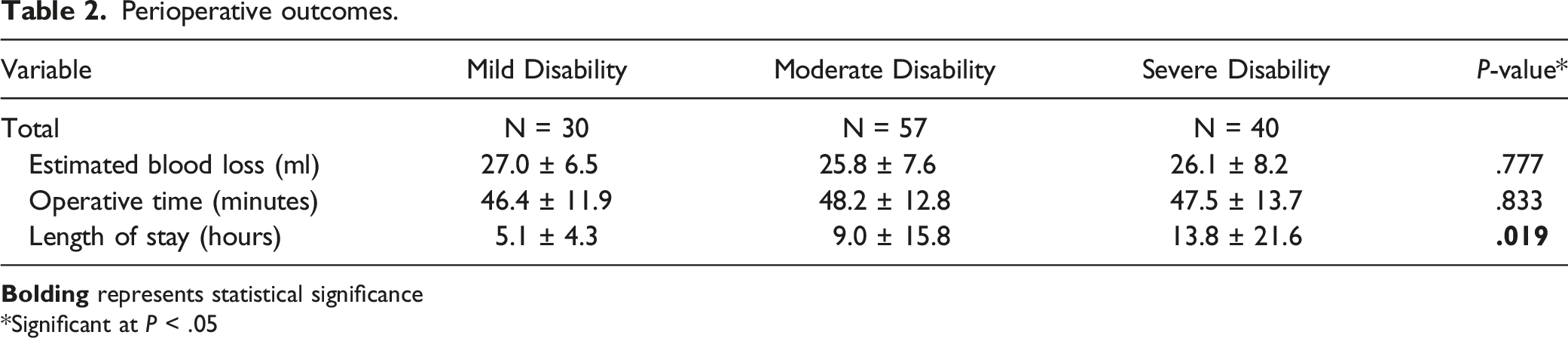
*Significant at P < .05
In terms of postoperative length of stay, there was a statistically significant association between preoperative disability, as measured by preoperative PROMIS-PF, and postoperative length of stay (hours). The average length of stay for preoperative severe disability patients is 13.8 hours, for moderate disability is 9.0 hours, and for mild disability is 5.1 hours, (P = .019) (Table 2). For patients with mild disability 2 patients (7%) stayed overnight, for patients with moderate disability 7 patients (12%) stayed overnight, and for patients with severe disability 12 (30%) stayed overnight, (P = .017)
Postoperative Pain and Narcotics Consumption
Postoperative VAS pain scores and narcotics use.
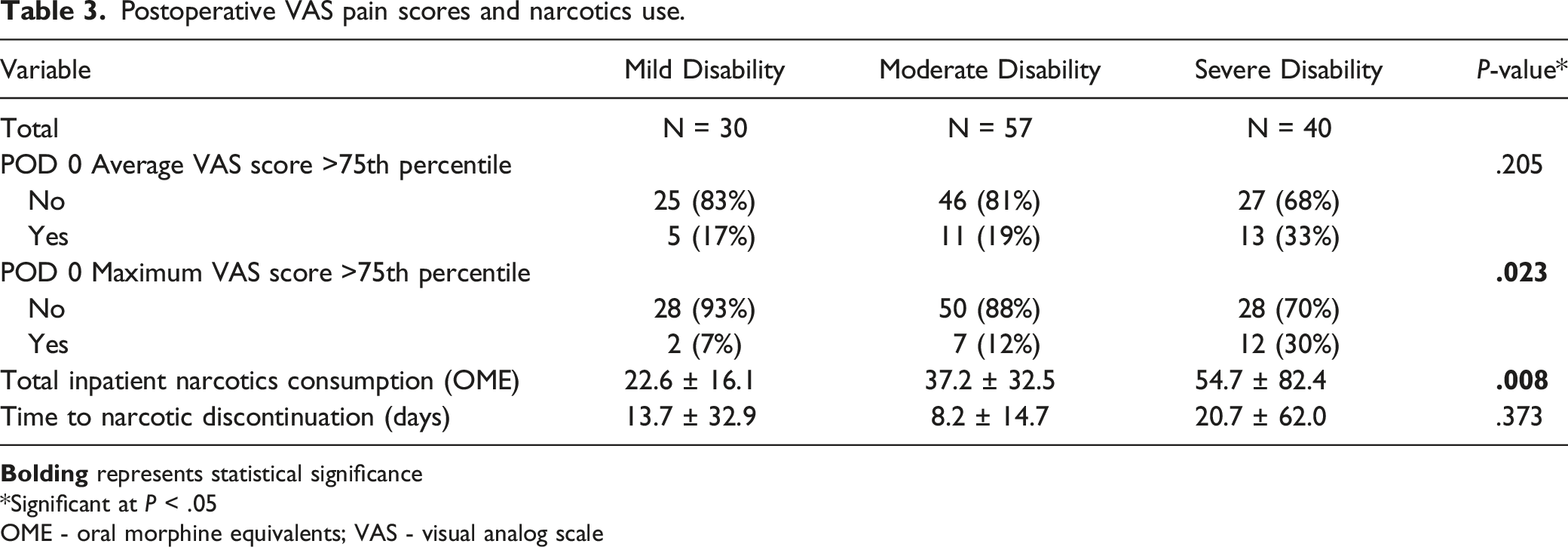
*Significant at P < .05
OME - oral morphine equivalents; VAS - visual analog scale
Further, patients with severe preoperative disability tended to consume higher amounts of total inpatient narcotics (54.7 OME) compared to those with moderate disability (37.2 OME) or mild disability (22.6 OME), (P = .008). However, there was no statistically significant difference in time to narcotic discontinuation after hospital discharge between the preoperative disability groups (P = .373) (Table 3).
Patient Reported Outcome Measures
Changes and improvement in PROMs.
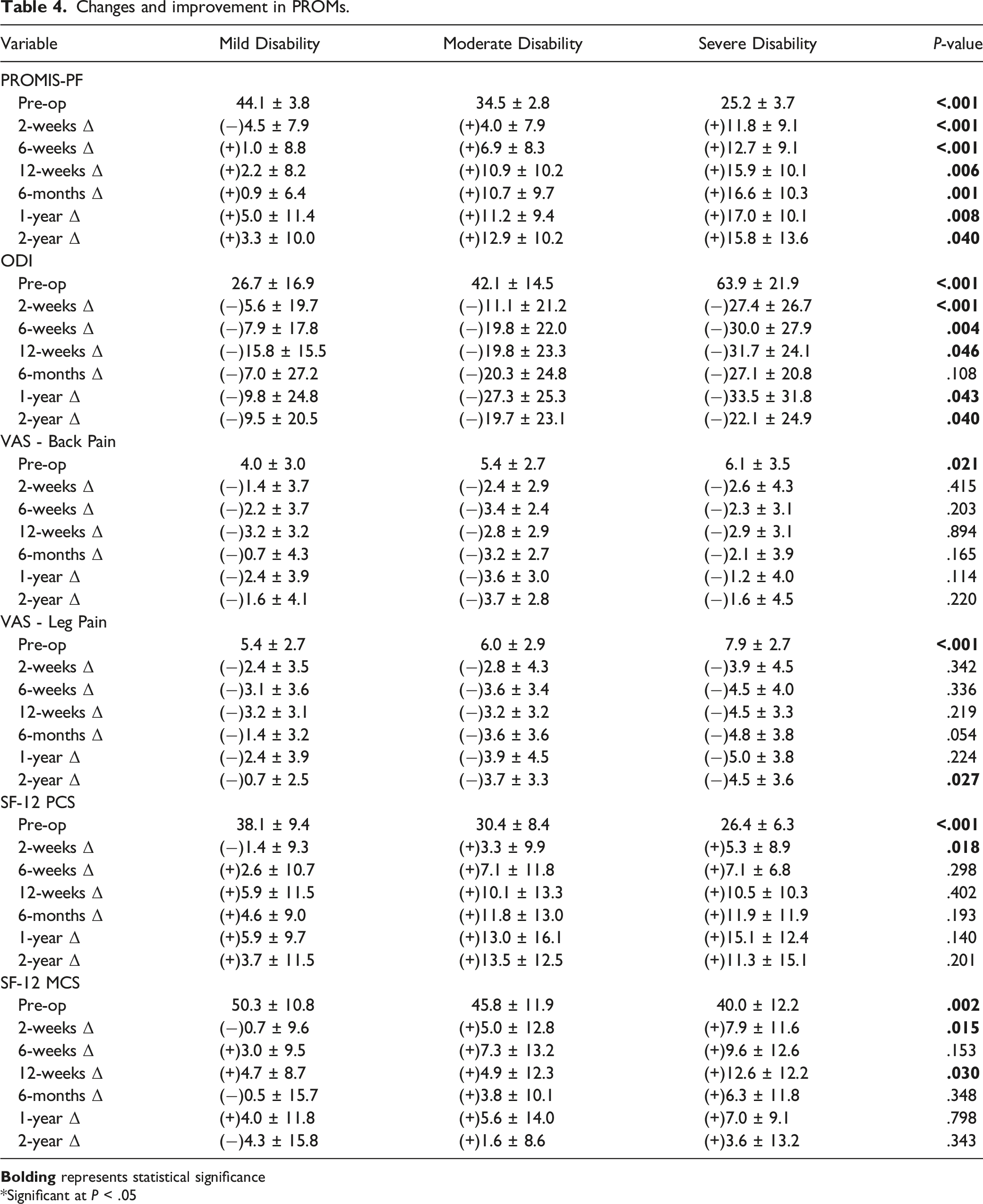
*Significant at P < .05
Association of preoperative PROMIS-PF and achieving minimal clinically important difference at 1 year follow-up.
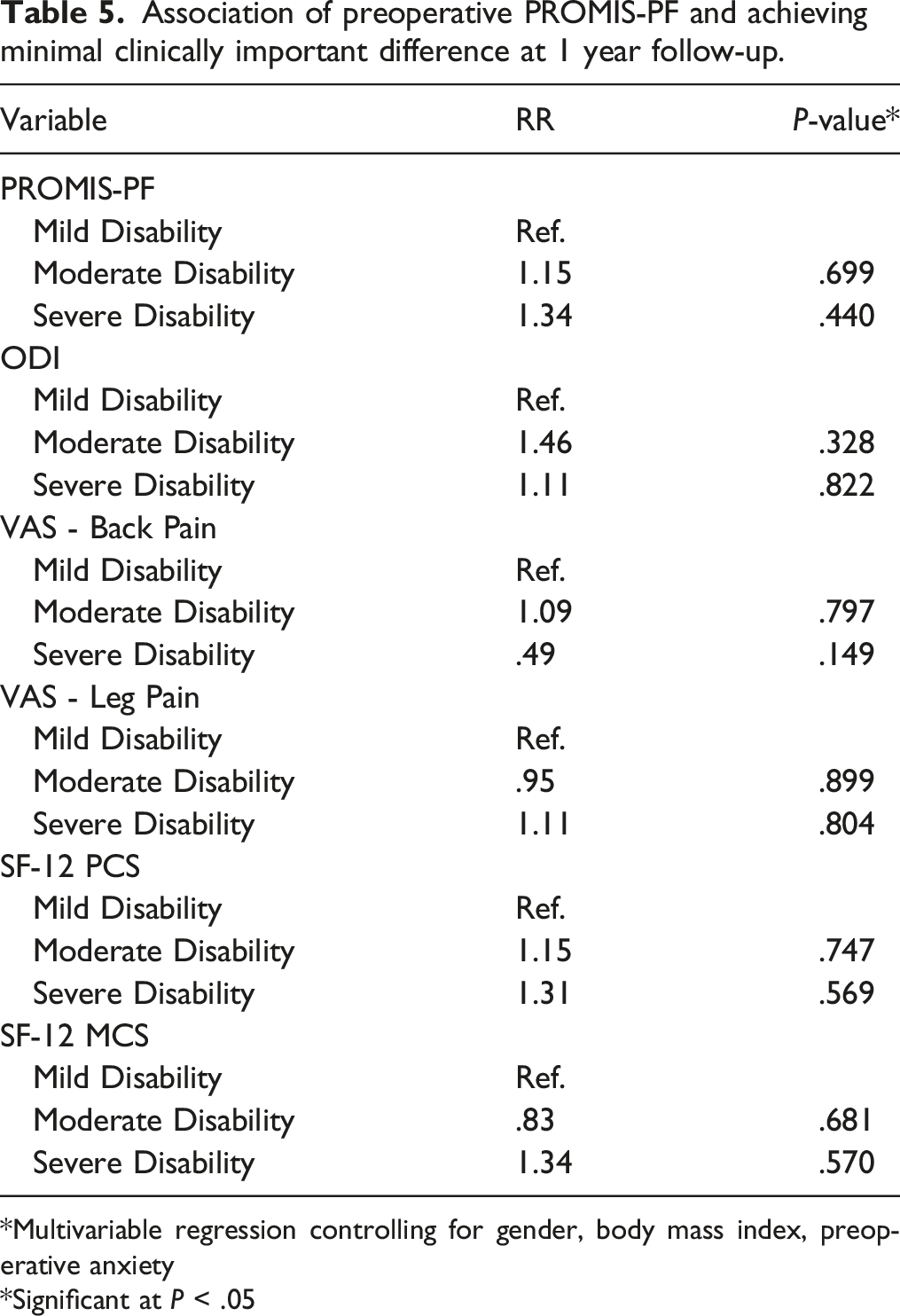
*Multivariable regression controlling for gender, body mass index, preoperative anxiety
*Significant at P < .05
Discussion
PROMIS-PF has been validated as an important tool for quantifying a patient’s physical function, including mobility, coordination, and strength.25-30 Its utility has been studied in a number of disease processes, including congestive heart failure, back pain, cancer, rheumatoid arthritis, and various orthopedic conditions.29-33 In spine surgery specifically, there has recently been a growing interest in the validity of PROMIS-PF and its ability to predict postoperative outcomes.34-41 However, there is a relative paucity of data on the relationship between PROMIS-PF and postoperative outcomes in patients undergoing lumbar microdiscectomy.
The current study found that patients with greater preoperative disability had increased inpatient postoperative pain and narcotics consumption. However, no significant differences were seen among the groups in the number of days to discontinue narcotics postoperatively. Furthermore, patients with greater disability demonstrated significantly greater improvement from baseline in PROMIS-PF, ODI, SF-12 PCS, and SF-12 MCS at 2-weeks following surgery. These higher improvements from baseline for patients with greater preoperative disability were sustained for PROMIS-PF, ODI, and VAS-Leg Pain at 2-year follow-up (P < .05) Finally, no significant associations were noted between preoperative PROMIS-PF scores and the ability to achieve MCID in any PROMs at 1-year postoperatively.
Some of the current study’s findings are in agreement with previous studies that analyzed different spine patient populations. Khor et al. developed a prediction model for postoperative pain and functional outcomes in patients undergoing elective lumbar spinal fusions. 42 In their model, preoperative ODI, which is a measure of functional disability due to back pain, was an important component of the prediction model for postoperative pain and disability following surgery. 42 Further, Patel et al. reported an association between worse preoperative PROMIS-PF scores and greater immediate postoperative pain and narcotics use in MIS-TLIF patients. 41 Similarly, Parrish et al. showed an association between greater preoperative disability and higher inpatient pain scores. 36 A particular strength of the current study was that we analyzed long-term use of postoperative narcotics by tracking the number of days that patients took to discontinue these medications, which has not been done in most previous studies.36,41 Interestingly, the current study revealed no significant difference in the number of days to discontinue narcotics postoperatively. Although it is clear from the data that patients with greater preoperative disability can expect to have higher immediate postoperative pain after lumbar microdiscectomy, they can be counseled to expect similar time to opioid medication cessation after surgery. This lack of difference in time to cessation of opioid medications, despite a difference in initial postoperative opioid usage between the groups, may be, in part, due to patient heightened awareness of the consequences of long-term opioid use. 36 The opioid epidemic has increased patients’ eagerness to quickly stop postoperative use and has introduced new policies and law enforcement changes that highly regulate opioid prescriptions. 43
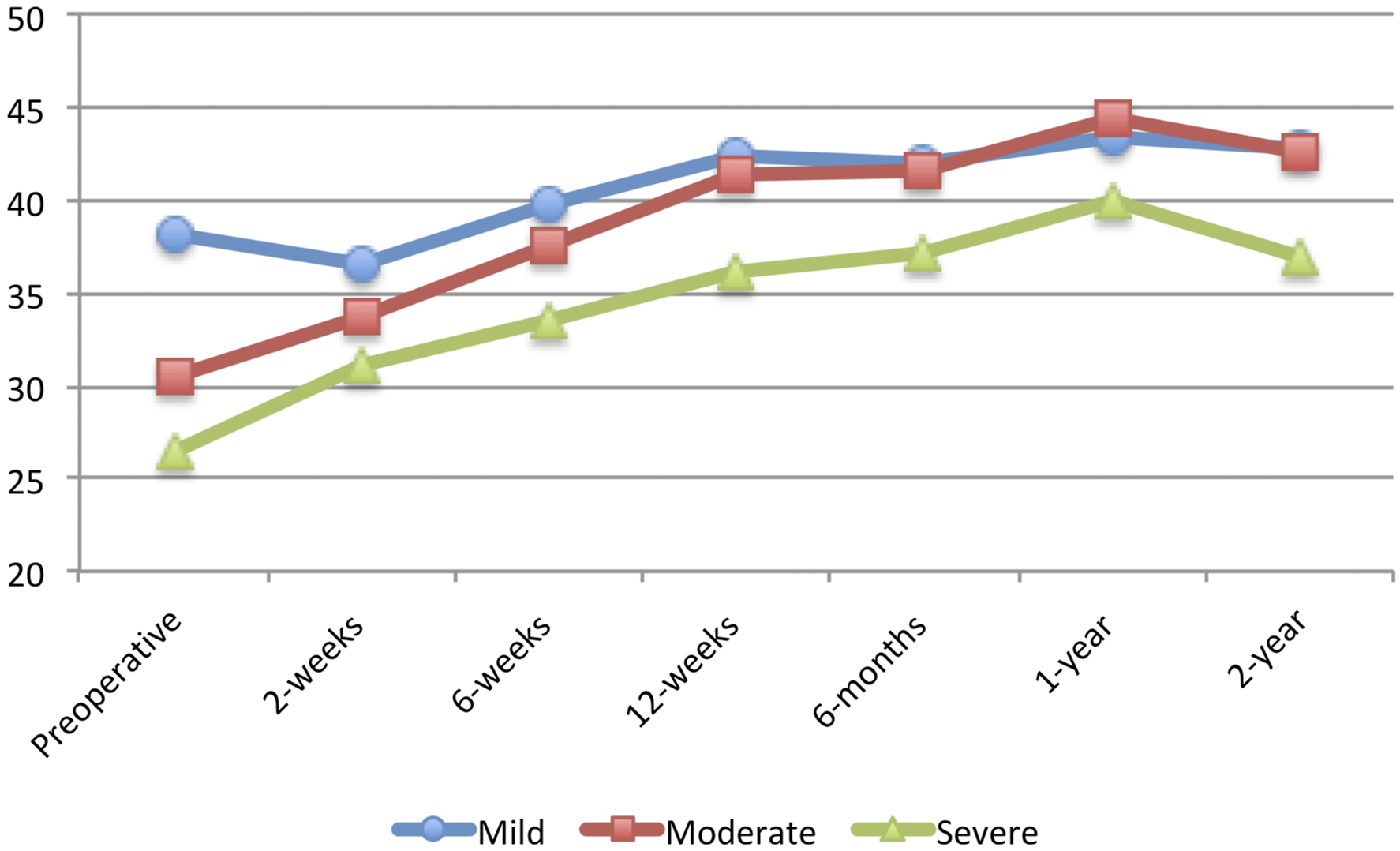
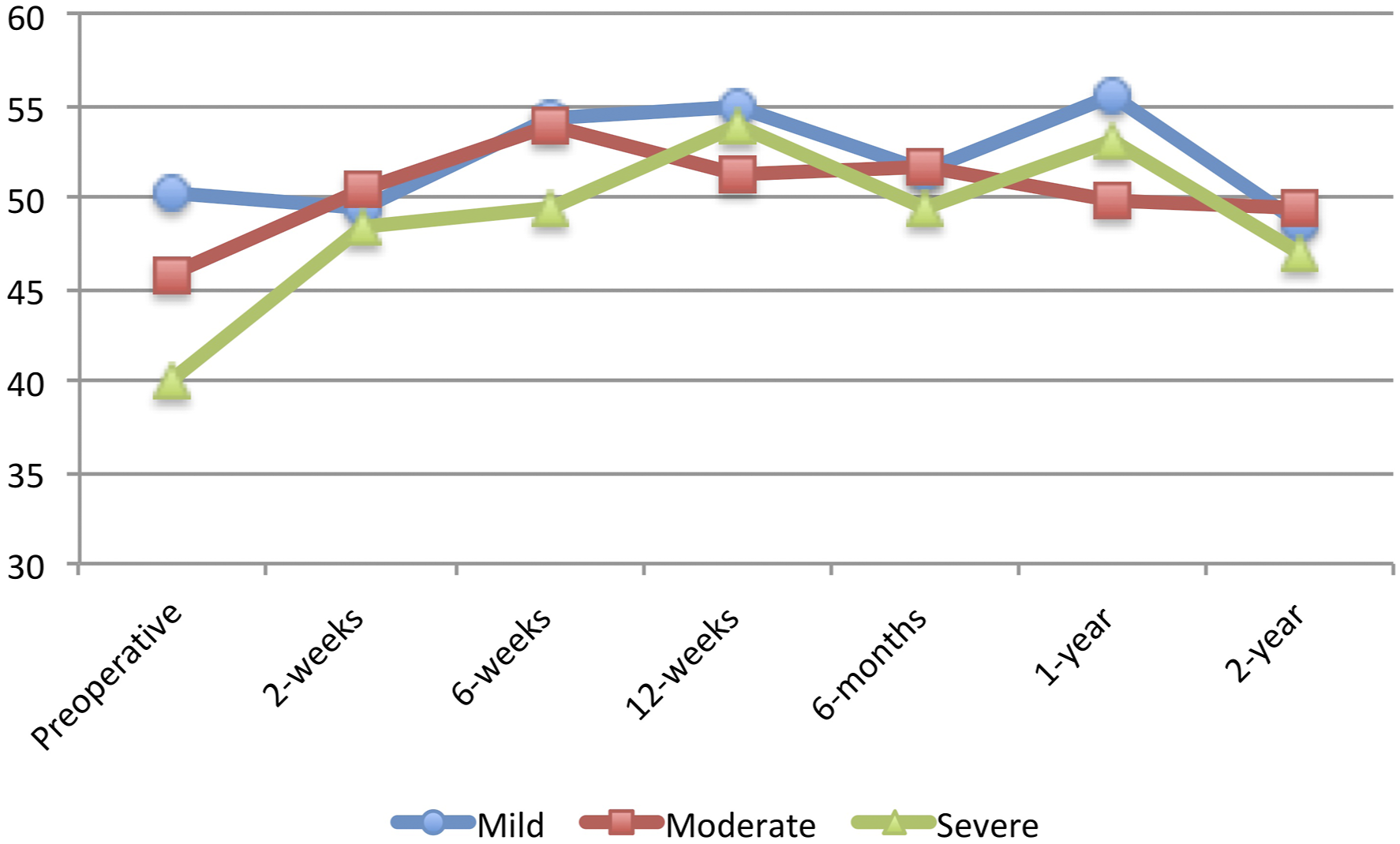
In terms of postoperative PROMS, the current study also demonstrated that patients with worse preoperative PROMIS-PF scores had greater improvements in PROMIS-PF, ODI, SF-12 PCS, and SF-12 MCS at 2-weeks postoperatively. These greater improvements were sustained for PROMIS-PF, ODI, and VAS-Leg Pain at 2-year following surgery. These findings differed from previous studies in different spine populations, which reported worse or similar improvements in PROMs for patients with worse preoperative PROMIS-PF scores.18,36-38 The reason for this difference in improvements is unclear; however, it may be due to the fact that outcomes after lumbar discectomy may be more intimately related to preoperative function. An older study by Saberi et al, demonstrated that a higher preoperative ODI resulted in better surgical outcomes (measured as postoperative ODI reduction) in patients who underwent lumbar discectomies. 44 It is worth noting that VAS-Back Pain and VAS-Leg Pain at 6-month, 1-year, and 2-year follow-up were not better than those at 3-month follow-up for certain sub-groups. For VAS-Back Pain, this may be due to the fact that improvements in back pain after lumbar discectomy procedures is less predictable. Indeed, previous studies have shown lumbar discectomy to be an effective and predictable treatment for radicular leg pain recalcitrant to nonoperative management, but not for isolated lumbar back pain.45,46 With regards to VAS-Leg Pain, this may be due to the fact that patients may achieve their minimal clinically important difference in VAS-Leg Pain at 3 months postoperatively. Another recent study has also shown that VAS-Leg Pain improvements after lumbar discectomy seem to plateau at 3 months following surgery. 39
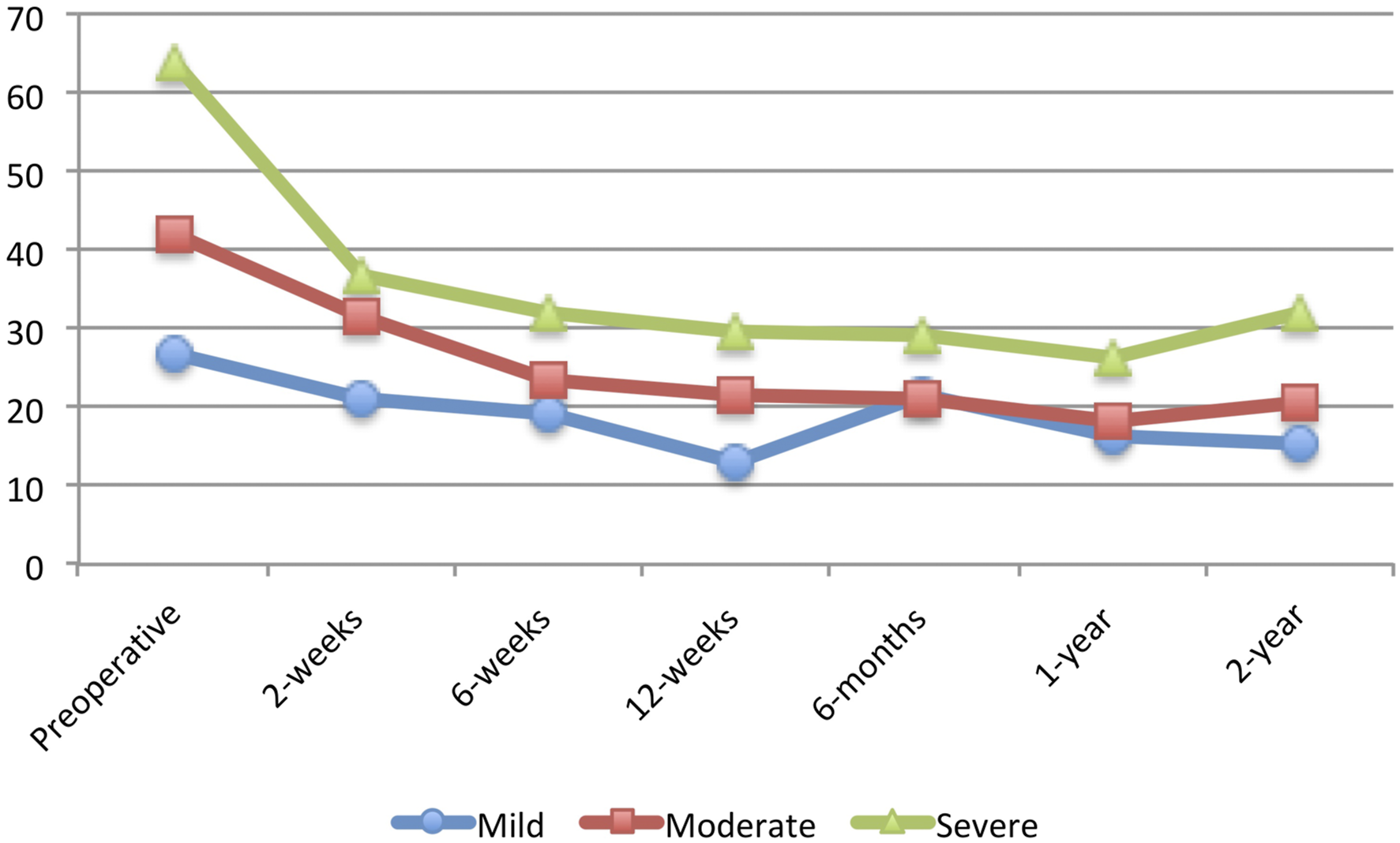
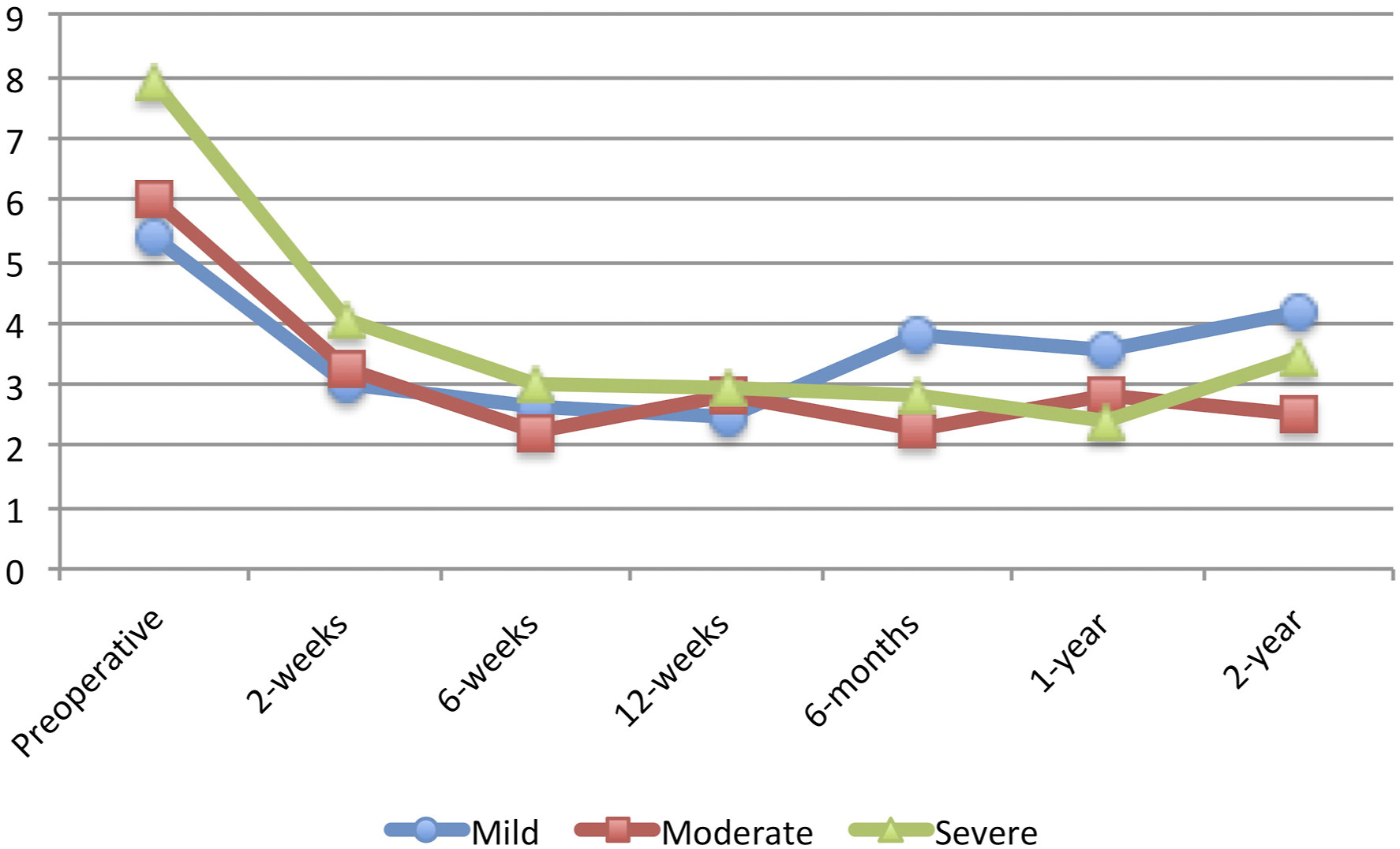
It is worth noting, however, that there was no association between preoperative disability and the ability to achieve MCID at 1-year for any PROMs following lumbar microdiscectomy. This finding demonstrates that regardless of preoperative disability, all patients are able to achieve MCID, although the absolute improvement may be greater for those with greater preoperative disability. Figures 1, 2, 3, 4, 5 and 6 Average Patient-Reported Outcomes Measurement Information System Physical Function for each study group for each follow-up time period. Average Oswestry Disability Index for each study group for each follow-up time period. Average Visual Analog Scale – Back Pain for each study group for each follow-up time period. Average Visual Analog Scale – Leg Pain for each study group for each follow-up time period. Average Short Form 12 – Physical Component Score for each study group for each follow-up time period. Average Short Form 12 – Mental Component Score for each study group for each follow-up time period.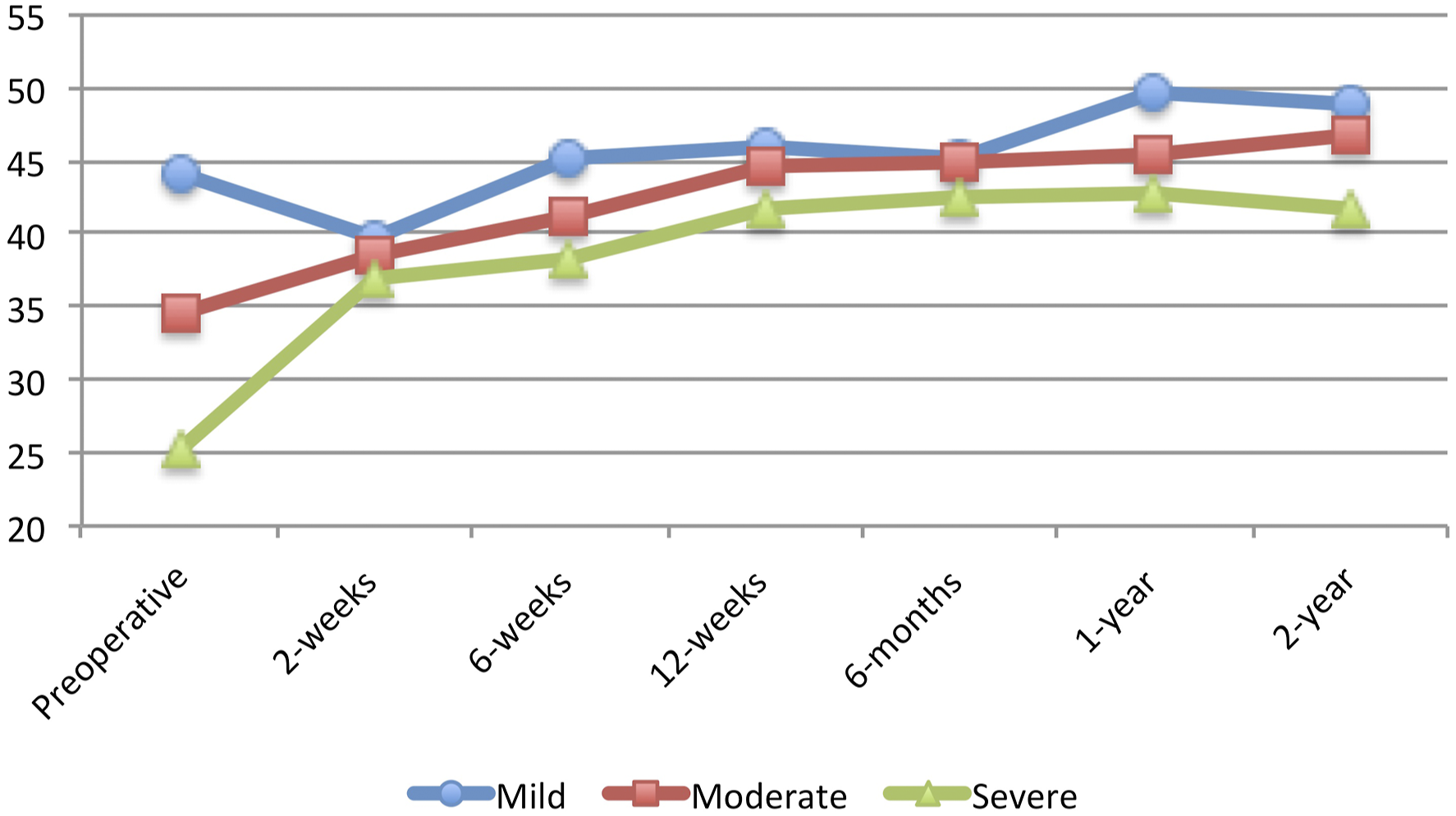

Of note, patients with worse preoperative physical functioning in the current study had a significantly longer length of hospitalization. In their study of MIS-TLIF patients, Jenkins et al. also reported an 8-hour difference in length of stay between patients with high and low preoperative PROMIS-PF scores. 38 This finding is important for surgical case order and logistics, as lumbar microdiscectomy is often performed as an ambulatory procedure. Patients with greater preoperative PROMIS-PF may need to be scheduled for surgery earlier in the day to facilitate same-day discharge.
There are several limitations to the current study. This was a retrospective review of prospectively collected data, which inherently introduces selection bias. Further, this was a single-surgeon and single-center study, which potentially limits the external validity of the study to more diverse populations. In addition, postoperative follow-up data were sufficient only up until the 2-year follow-up; thus, long-term associations beyond this time point could not be elucidated. However, recent studies have shown that PROMs at 1-year following lumbar spine surgery accurately predict those at 2-year follow-up.23,24 Further, though the current study was able to analyze the exact number of days to discontinue narcotics postoperatively, data on how long patients used narcotics preoperatively was not available. In addition, data on the amount of preoperative opioid usage for each patient was not recorded in the registry and therefore the effects of this variable on postoperative outcomes such as hospital length of stay, postoperative opioid use, patient-reported pain, and time to medication cessation cannot be analyzed.
In conclusion, the current study analyzed the association between preoperative PROMIS-PF with postoperative pain, narcotics use, and improvements in various PROMs following a single-level lumbar microdiscectomy. Patients with severe preoperative physical disabilities experienced greater pain and narcotics use in the immediate postoperative period but did not take a longer amount of time to discontinue narcotics. Patients with severe preoperative physical disabilities also saw greater improvements in various PROMs postoperatively up to 2-year following surgery. As preoperative PROMs are increasingly being studied and utilized to predict postoperative outcomes, physicians may use these findings to better counsel patients. Overall, this study adds to the growing body of literature demonstrating the usefulness and versatility of PROMIS-PF in predicting outcomes in spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No direct funding was received for this study. However, the study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health (NIH) under award number: UL1 TR002384.
IRB Statement
Our institutional review board approved the protocol of the current study.