
Abstract
Objective
To discuss how the sequence of spinal surgery and hip replacement is determined for patients with both degenerative scoliosis and hip disease.
Methods
Twenty-six patients treated for both degenerative scoliosis and hip disease from June 2012 to June 2015 were retrospectively studied. Eleven patients underwent hip replacement followed by lumbar surgery (Group A), and 15 patients underwent lumbar surgery followed by hip replacement (Group B). The average follow-up duration was 1.5 years. Related indicators were assessed preoperatively and postoperatively.
Results
The parameters showing significant differences between Groups A and B after surgery were acetabular anteversion, the Oswestry functional disability score, and the Harris hip score. Postoperatively, five patients in Group A had unequal shoulder heights and inclination of the trunk to one side. After lumbar surgery and before total hip arthroplasty in Group B, eight patients could not walk, and the limitation was more severe than that preoperatively.
Conclusion
Spinal surgery may be performed first to resolve lumbar nerve symptoms and restore sagittal balance of the spine; hip replacement may then be performed to simplify hip replacement difficulties and resolve the imbalance after spinal surgery. Severely limited range of motion exists after lumbar surgery and before total hip arthroplasty.
Keywords
Introduction
Degenerative scoliosis (DS) is characterized by asymmetrical intervertebral space collapse, rotatory subluxation of the vertebral body or side slippage caused by severe degeneration of the intervertebral disc, and scoliosis of the facet joints on the coronal plane (>10°) after skeletal maturation. However, DS does not include cases of organic spinal disease or an original medical history of scoliosis. On the sagittal plane, the main manifestations include the disappearance of lumbar lordosis (LL) and thoracolumbar segmental kyphosis. 1 In patients with spinal degeneration, hip joint degeneration is also present; this is called “hip–waist syndrome.”2–5 Relevant studies have shown that 18% of patients with both lumbar disease and hip joint disease require total hip arthroplasty (THA). 6 Moreover, hip joint factors can directly influence spinal sagittal balance and function. Surgical treatment and orthopedic strategies for patients with DS must take hip joint factors into account. In 2015, Phan et al. 7 proposed the concept of the spinal pelvic complex, which formally involves the entire spine and hip joint, and they systematically developed a classification system for the various types of this complex. However, no research has yet shown whether spinal surgery or THA should be carried out first in patients with DS. In this study, the surgical strategy for patients with concurrent DS and hip joint disease was evaluated.
Materials and methods
Ethical approval
This study was approved by the Institutional Ethics Committee of The General Hospital of Northern Theater Command. Written informed consent was obtained from all participants.
Patients
Patients with both DS and hip joint disease who were admitted to and treated at the PLA General Hospital and General Hospital of Shenyang Military from June 2012 to June 2015 were retrospectively studied. Group A comprised patients who underwent hip replacement first and then underwent lumbar surgery, and Group B comprised patients who underwent lumbar surgery first and then underwent hip replacement. All patients underwent unilateral hip replacement. All patients in both groups had nerve root compression symptoms, hip joint pain, and limited range of motion, and some patients also had severe lumbago and backache that affected their daily life and made walking difficult. The inclusion criteria were lumbar scoliosis with a Cobb’s angle of ≥10°; age of >50 years at the time of surgery; no history of spinal surgery; no history of scoliosis; diagnosis of unilateral hip joint disease, such as congenital acetabular maldevelopment, femoral head necrosis, or osteoarthritis (patients undergoing hip joint surgery were also included); four or more fixed segments; follow-up duration of ≥1 year; and complete imaging data.
Imaging parameters
Two chief physicians of the orthopedics department measured the imaging parameters using Surgimap version 2.2.9.7 (Nemaris, Inc., New York, NY, USA). 8 Anteroposterior images of each patient’s spine while standing were measured. Cobb’s angle, sagittal vertical axis, LL, thoracic kyphosis, pelvic tilt (PT), sacral slope, acetabular anteversion (AA), and hip joint flexion range of motion were measured preoperatively and at the final follow-up visit. Postoperative clinical function scores were also gathered, including the Oswestry functional disability score, 9 visual analog scale score for leg pain, and Harris hip score. All patients autonomously completed the functional ratings with the assistance of resident doctors at our hospital.
Surgical procedures
Patients in Group A underwent THA first and took rivaroxaban (0.5 pill/night) for 35 days postoperatively. The day after surgery, they could walk with two crutches. After 1.5 months, they could walk with a single crutch. After 2 months, they could walk autonomously. All 11 patients planned to undergo lumbar surgery 3 months after THA. Patients in Group B underwent lumbar surgery first and did not receive postoperative anticoagulation. The drainage tube could be removed within 1 week postoperatively, at which time the patients could walk with a walking aid. Three months later, they underwent THA with a posterolateral approach.
A systematic design was established before the surgery. In Group B, spinal surgery was conducted first. The theoretical PT (tPT) of each patient was calculated using the following formula: tPT = PI × 0.37 – 7, where PI is the pelvic incidence. The change in PT (△PT = PT – tPT) was used to calculate the degree of PT to be corrected. Next, according to the change in the value of AA 7 = △PT × 0.6°, the degree of AA was determined for THA. In Group A, THA was conducted first. The degree of AA was set to be approximately 20° according to the surgeon’s experience. Spinal surgery was then carried out according to the value determined from the following formula: tPT = PI × 0.37 − 7.
Statistical analysis
Data are expressed as mean ± standard deviation, and data pairing and independent t tests were performed with IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA). A P value of <0.05 indicates a statistically significant difference.
Results
Twenty-six patients were included in this study. Group A comprised 11 patients (age range, 58–69 years; average age, 64.2 years), and Group B comprised 15 patients (age range, 60–68 years; average age, 64.3 years). The patients’ average age was not significantly different between the two groups. The baseline information of the patients in both groups is shown in Table 1. The bleeding volume and operative duration for THA were significantly higher in Group A than in Group B (P < 0.01 for both). The duration of hospitalization for lumbar surgery was significantly longer in Group B than in Group A (P < 0.01) (Table 1). None of the preoperative imaging parameters or functional scores were significantly different between the two groups (Table 2).
Comparison of patients’ baseline data between the two groups.
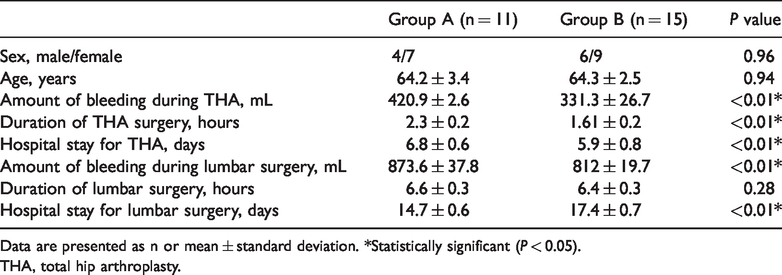
Data are presented as n or mean ± standard deviation. *Statistically significant (P < 0.05).
THA, total hip arthroplasty.
Comparison of preoperative imaging parameters and functional scores between the two groups.

Data are presented as mean ± standard deviation.
LL, lumbar lordosis; PT, pelvic tilt; SS, sacral slope; SVA, sagittal vertical axis; TK, thoracic kyphosis; AA, acetabular anteversion; VAS, visual analog scale.
After the surgery, there were no significant differences between the two groups in Cobb’s angle, LL, PT, sacral slope, sagittal vertical axis, thoracic kyphosis, or the visual analog scale score for leg pain (Table 3). However, significant differences were found between Groups A and B in the postoperative AA (26.8° ± 1.0° and 20.5° ± 1.5°, respectively), Oswestry functional disability score (25.8 ± 1.0 and 17.5 ± 2.0, respectively), and Harris hip score (81.34 ± 1.8 and 88.0 ± 1.2, respectively) (P < 0.01 for all). The AA value in Group A was different from the set value of 20°. After restoration of the sagittal imbalance of the spine, the anterior rotation of the pelvis increased the degree of AA, which increased the difficulty of achieving acetabular prosthesis anteversion. On postoperative follow-up, five patients in Group A had unequal shoulder heights and inclination of the trunk to one side (Figure 1). After lumbar surgery and before THA, eight patients in Group B could not walk because of limited hip joint range of motion, and the degree of limitation was more severe than that before lumbar surgery. This issue was related to the above-mentioned AA reduction. However, after the whole course of surgical treatment, Group B showed better outcomes and fewer complications than Group A. After spinal correction, the residual imbalance could still be remedied and corrected through THA, and performing spinal surgery first reduced the difficulty of performing THA (Figure 2).
Comparison of postoperative imaging parameters and functional scores between the two groups.

Data are presented as mean ± standard deviation. *Statistically significant (P < 0.05).
LL, lumbar lordosis; PT, pelvic tilt; SS, sacral slope; SVA, sagittal vertical axis; TK, thoracic kyphosis; AA, acetabular anteversion; VAS, visual analog scale.

Images of a 52-year-old woman with a 1-year history of lumbago accompanied by radiating pain in the left lower limb that had been exacerbated for 1 month. (a, b) Preoperative lumbar radiographs in the anteroposterior view, with Cobb’s angle of 26°. (c) Preoperative pelvic radiograph in the anteroposterior view. (d, e) Full-length spinal radiographs in the anteroposterior view after hip replacement, with the following parameters: Cobb’s angle, 33°; SVA, 61.42 mm; TK, 39°; TLK, 1°; LL, −55°; PI, 55°; PT, 11°; and SS, 44°. (f, g) Full-length spinal radiographs in the anteroposterior view after spinal surgery, with the following parameters: Cobb’s angle, 4°; SVA, 64.32 mm; TK, 29°; TLK, 4°; LL, −52°; PI, 55°; PT, 9°; and SS, 46°.

Images of a 56-year-old woman with a 6-year history of lumbago accompanied by a 3-year history of pain in the left lower limb that had been exacerbated for 1 year. (a, b) Preoperative full-length spinal radiographs in the anteroposterior and lateral views, with the following parameters: Cobb’s angle, 9°; SVA, 35.2 mm; TK, 30°; TLK, 41°; LL, −33°; PI, 47°; PT, 26°; and SS, 21°. (c) Preoperative pelvic radiograph in the anteroposterior view. (d, e) Full-length spinal radiographs in the anteroposterior view after lumbar surgery, with the following parameters: Cobb’s angle, 1°; SVA, 39.48 mm; TK, 36°; TLK, 25°; LL, −51°; PI, 47°; PT, 14°; and SS, 33°. (f, g) Full-length spinal radiographs in the anteroposterior view after hip replacement, with the following parameters: Cobb’s angle, 0°; SVA, 48.76 mm; TK, 25°; TLK, 21°; LL, −50°; PI, 47°; PT, 8°; and SS, 39°.
Discussion
The surgical treatment strategy for DS has been gradually recognized. Surgical treatment is no longer limited to management of lumbar spinal stenosis but now also includes coronal and sagittal imbalance correction. 10 Previous research has identified two key strategies to restore an individual’s overall sagittal balance: the spinal bony sagittal balance correction strategy11,12 and the intramuscular sagittal balance correction strategy.13–15 However, few reports have addressed the influence of joint factors on the efficacy of DS treatment. In addition, when hip joint disease also needs to be addressed, it is difficult to decide which procedure should be conducted first: joint replacement or spinal surgery. In this study, patients with both DS and hip joint disease were grouped according to the surgery sequence for comparison. The bleeding volume and operative duration for THA were significantly higher in Group A than in Group B. When performing THA first, after achieving hemostasis, we carefully selected the height of the osteotomy to achieve a good match; the average operative duration was thus extended to 1.61 hours. Patients who underwent THA first still showed a state of spinal imbalance and anterior rotation of the pelvis. In addition, the difficulty of evaluating the anteversion angle of the acetabular prosthesis, the operative duration, and the bleeding volume were greater in these patients. When THA was conducted first, the overall coronal and sagittal balance could not be fully evaluated. After spinal surgery, iatrogenic coronal imbalance may occur. The duration of hospitalization for lumbar surgery was significantly longer in Group B than in Group A. When spinal surgery was carried out first, sagittal imbalance could be corrected, the pelvis could be adjusted to a normal position, and the acetabular prosthesis could be easily placed. However, because some patients also had flexion contracture and their pelvis was anteverted to a state of hypokinesis, which led to a reduction in the degree of AA of the hip joint, the range of motion in anteflexion was altered. Thus, the postoperative hip joint motion was limited. Patients had difficulty walking and could not perform weight-bearing activities. Some patients needed to walk with crutches and had a longer hospital stay.
In this study, rigorous preoperative decision-making was performed to select the orthopedic strategy. For patients undergoing spinal surgery first, we must fully consider the sagittal balance of the spinal pelvic complex. In 2015, Phan et al. 7 proposed the concept of the spinal pelvic complex and developed the following classification system: type 1, spinal flexibility and sagittal balance; type 2, spinal stiffness and sagittal balance; type 3, spinal flexibility and sagittal imbalance; and type 4, spinal stiffness and sagittal imbalance. In this system, a balanced state is defined as PT of <25° and PI − LL of <10°, and an imbalanced state is defined as PT of >25° and PI − LL of >10°. This classification system is used to evaluate the influence of the spine on hip replacement and considers the differences between the standing and sitting positions. Moreover, we know that whenever PT changes by 1.0°, AA will positively change by 0.6°. Therefore, we calculated the degree to be corrected as △PT = PT − tPT and then determined the AA degree for THA according to the change in AA using the following formula: △PT × 0.6°. We found that because the pelvis of patients who underwent spinal surgery first was restored to a normal position, the preoperative AA value was close to 20°, which meets the standard for normal acetabular prosthesis placement and reduces the difficulty of performing THA. Moreover, during THA, we could adjust the residual coronal imbalance and unequal shoulder height that appeared after spinal surgery. In this way, the orthopedic effect could be improved. The treatment method in both groups had the same effect on lumbar scoliosis correction and sagittal orthopedics. Because root pain relief is related to intraoperative decompression, the pain score did not differ. Zheng et al. 16 also reported the adjustment effect of THA on spinal imbalance in the treatment of ankylosing spondylitis kyphosis with THA and hip joint fusion. If THA is implemented first, the AA angle will differ substantially from the normal value, increasing the surgical difficulty. In addition, if spinal surgery is performed after THA, the balance of the spinal pelvic complex will change, thus leading to a change in AA. Thus, the acetabular prosthesis placement angle will be poor, and anterior dislocation may easily occur.
If the hip joint pain is relieved in patients with poor health conditions who do not have a favorable economic situation or refuse to undergo hip replacement, how should their sagittal balance be corrected? At present, it seems that the LL correction rate should decrease with spinal surgery. Furthermore, a decrease in sacral slope and an increase in PT and AA (equivalent to a type 4 spinal joint complex) seem to compensate for a poor AA compensatory capacity and prevent anterior rotation of the acetabulum.
Limitations
The main limitations of this study are the small number of patients and the short follow-up time. More patients should be included in future research, and more complications should be observed.