
Abstract
Study Design
Systematic review.
Objective
While the occurrence of sexual dysfunction in patients sustaining traumatic cervical or thoracic injuries is well acknowledged, the evidence regarding its prevalence and outcome in individuals with degenerative cervical myelopathy (DCM) is still limited. The current systematic review was planned to comprehensively evaluate the existing literature regarding the prevalence, patterns, presentation, and outcome of sexual dysfunction in patients presenting with DCM.
Methods
A thorough search of the literature was performed on October 15, 2024, using 5 different databases (Google Scholar, Embase, PubMed, Web of Science and Cochrane Library). Studies on sexual dysfunction in DCM published until 2024 were scrutinized. Narrative or systematic reviews, opinions, letters to the editor, and manuscripts published in non-English languages were excluded.
Results
Overall, the literature search yielded a total of 384 articles of which 7 articles with 910 patients were included in the analysis. The overall prevalence of erectile dysfunction (ED) in CSM ranges between 3 and 6%. 82% of patients with preoperative ED had an abnormal psychogenic erection while the remaining had an abnormal reflexogenic erectile function. The erectile function was reported to improve substantially following decompressive surgery (68% recovery rate; P = 0.05). The presence of preoperative sexual dysfunction has been associated with poorer neurological outcomes (50% recovery rate; including poorer gait recovery). The data regarding ejaculatory disturbances and female sexual dysfunction in DCM patients are still limited.
Conclusion
ED occurs in 3 to 6% of patients with DCM, with a majority of patients suffering from ED from psychogenic origin. Surgical decompression can significantly improve the sexual recovery in these patients. Patients with ED have overall poorer neurological recovery.
Keywords
Introduction
Being a conduit extending between the brain and the rest of the body, a dysfunctional cervical spinal cord can effectuate diversified symptomatology and disability. 1 The term “degenerative cervical myelopathy” or DCM has been coined to describe all the pathologies of the cervical spinal cord that may develop consequent to the degenerative changes of adjoining spinal elements. 2 It is the most prevalent aetiology for spinal cord pathology, with a reported prevalence rate of approximately 2%. 3
Classically, multitudinous symptoms and presentation including neuropathic pain, gait imbalance, fine motor, coarse motor or sensory disturbances (including hyper-, para- or dysesthesias) of the hands, upper or lower extremities, coordination, as well as autonomic disturbances such as bladder or bowel incontinence (or dysfunction) have been reported in patients presenting with DCM. 4 These domains (in combination) have been incorporated into the traditional approaches employed in the evaluation of DCM, such as modified Japanese Orthopedic Association (mJOA) score, Nurick grade, neurosurgical cervical spine scale, gait analysis, grip dynamometer, GaitRite and GRASSP assessment tool.2,4-9
The presence of sexual dysfunction has been well-acknowledged to impact the biology, self-image, self-confidence, and overall mental or even physical well-being of an individual.10,11 While the published literature has already discussed the prevalence rate and outcome following sexual dysfunction in patients sustaining traumatic cervical or thoracic injuries; the evidence regarding the occurrence of sexual dysfunction in individuals with cervical spondylo-myelopathy (CSM) is still limited.12,13 The prevalence rate of sexual dysfunction in individuals with DCM is reported to be around 3%–6%. 4 However, it is well-recognized that there is a significant possibility of under-reporting in elderly patients, in whom the sexual problems may be attributed directly to their age or other associated comorbidities.14,15 As the adage popularized by Carl Segan goes, “an absence of evidence is not the evidence of absence”; the issue of sexual dysfunction in patients with DCM needs to be further explored in detail. 2 In this context, the current systematic review was planned to comprehensively evaluate the existing literature regarding the prevalence, patterns, presentation, and outcome of sexual dysfunction in patients presenting with DCM. No review articles have been published on this subject, hitherto.
Methods
The study was conducted adhering to the guidelines set forth for the conduction and reporting of systematic reviews as per Cochrane Collaboration 16 and Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) respectively. 17
Literature Search
A thorough search in the literature was performed on October 15, 2024, using 5 different databases (Google Scholar, Embase, PubMed, Web of Science and Cochrane Library). Studies on sexual dysfunction in DCM published until 2024 were scrutinized. The search was performed using the keywords in combination with the Boolean operators: (((sexual dysfunction) OR (sexual problems) OR (erectile dysfunction) OR (ED) OR (ejaculatory disturbances)) AND ((cervical myelopathy) OR (cervical spondylomyelopathy) OR (degenerative spondylomyelopathy) OR (myelopathy))).
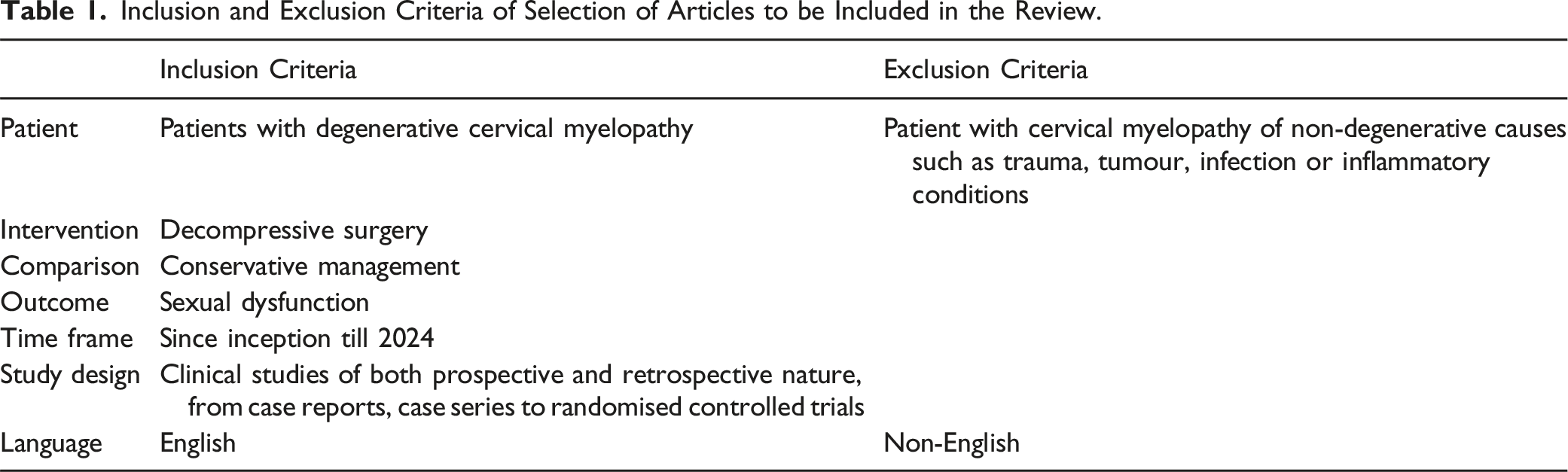
Criteria for Inclusion or Exclusion of Manuscripts
Inclusion and Exclusion Criteria of Selection of Articles to be Included in the Review.
Manuscript Selection and Data Extraction
The search outputs were downloaded from the specific databases. They were then extracted to End-Note, de-duplicated and then selected manually. The title screening was independently performed by 2 authors, following which the individual manuscripts were separately screened as described in the aforementioned criteria. Following this, the next round of screening was performed, wherein the complete manuscripts were extracted by the authors and analyzed in detail in duplicate. The final article selection was then completed. Any discrepancy among the authors was clarified based on mutual discussions with the senior author.
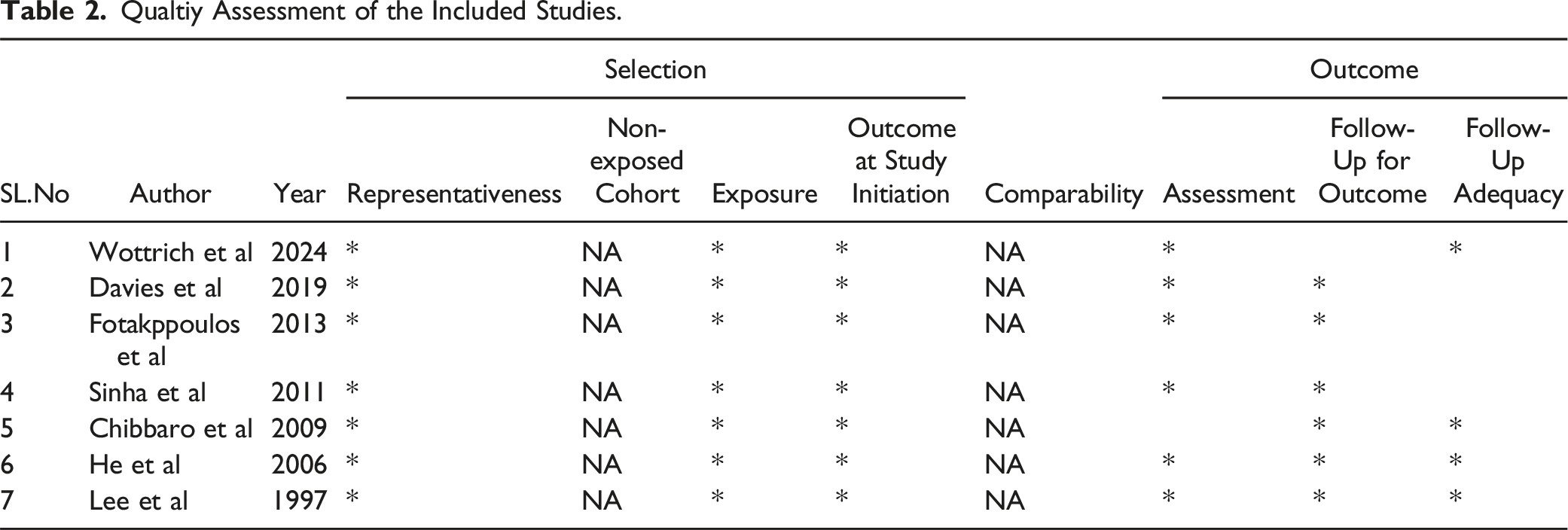
Quality Assessment
Qualtiy Assessment of the Included Studies.
Research Objective (RO)
The primary research objectives of the study included
RO1: Sexual dysfunction in DCM
RO2: Patterns of sexual dysfunction in patients with DCM
RO3: Prevalence of sexual dysfunction in patients with DCM
RO4: Effect of surgical decompression on sexual dysfunction in patients with DCM; RO5: Clinical outcome in patients with DCM-associated sexual dysfunction
RO6: Rehabilitative approach for sexual recovery in DCM patients
Results
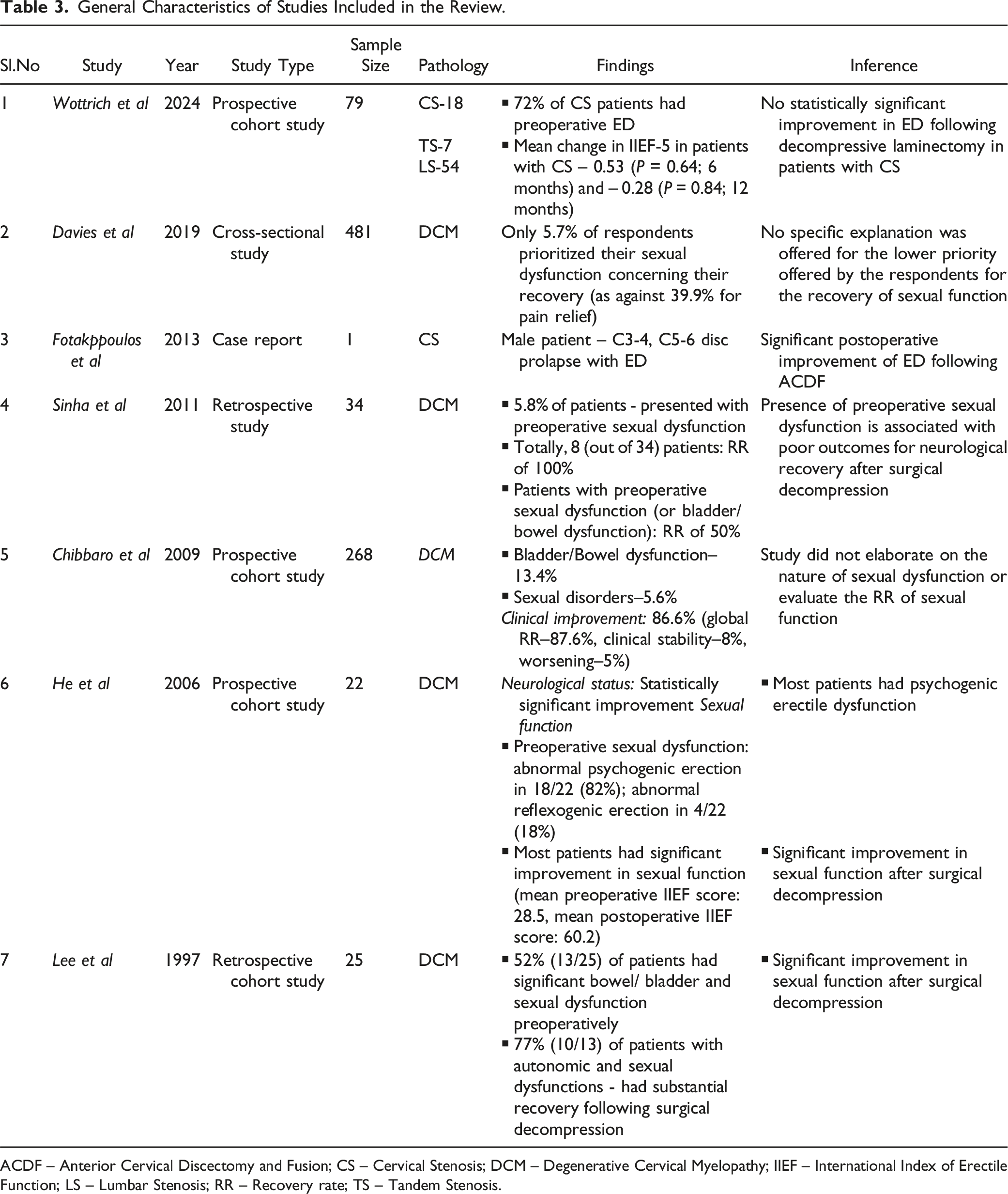
Overall, the literature search yielded a total of 384 articles. After de-duplication and compilation of the studies, 247 manuscripts were selected. After screening the titles of the selected articles, 33 manuscripts were qualified for the next level of screening. Finally, after the screening of abstracts and full manuscript texts, 7 articles were selected for the systematic review. The selection of studies included in this review is presented through the PRISMA flow diagram in Figure 1. The general characteristics and the outcomes from the individual studies included for analysis are presented in Table 3. Considering the paucity of literature on the topic, quantitative synthesis could not be performed and a qualitative summary of evidence is presented on the research objectives developed prior to the inception of the study. PRISMA flow diagram of inclusion of studies. General Characteristics of Studies Included in the Review. ACDF – Anterior Cervical Discectomy and Fusion; CS – Cervical Stenosis; DCM – Degenerative Cervical Myelopathy; IIEF – International Index of Erectile Function; LS – Lumbar Stenosis; RR – Recovery rate; TS – Tandem Stenosis.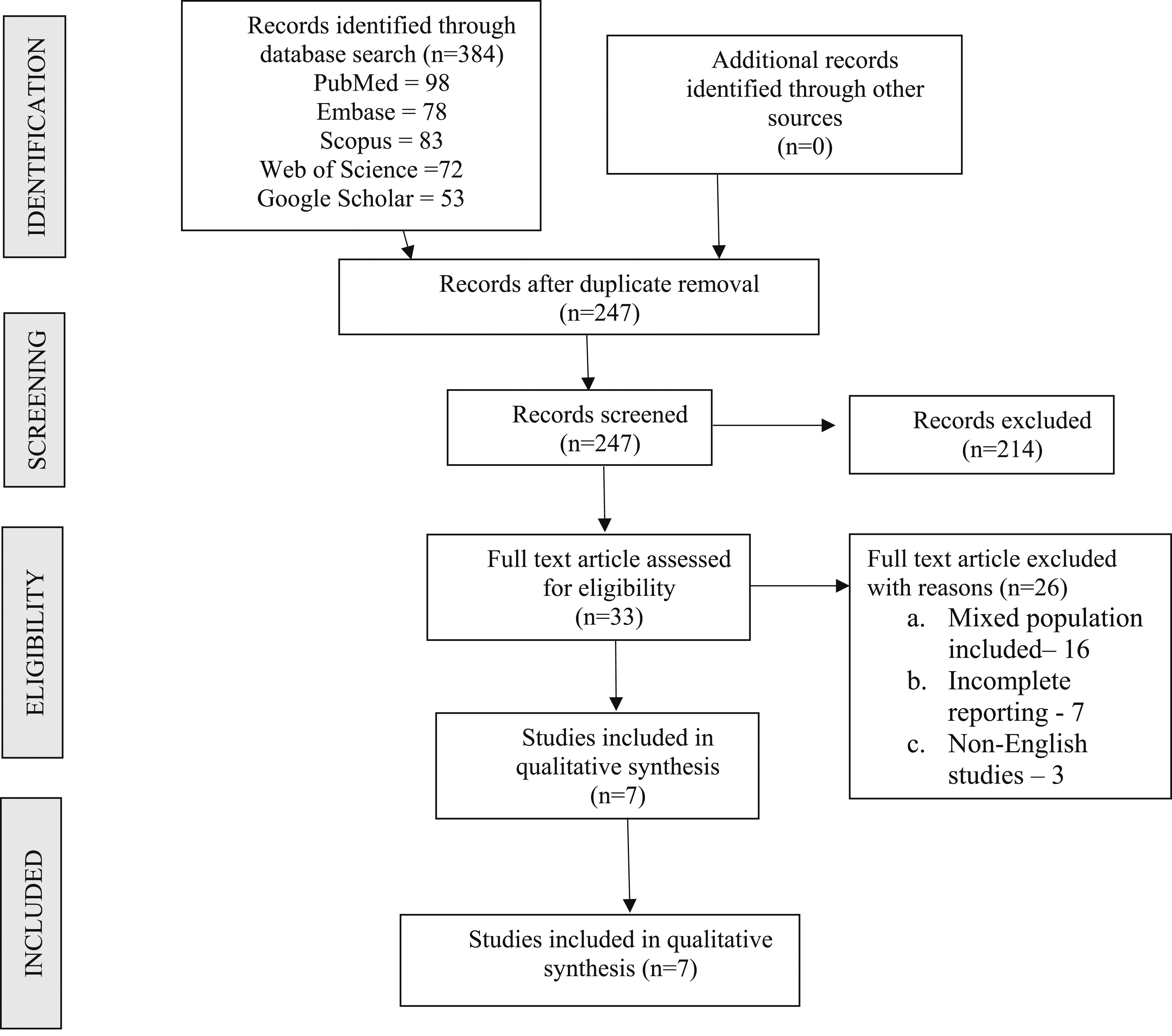
RO1: Sexual Dysfunction in DCM
CSM always effectuates partial or complete cervical spinal cord injury; and results in varying degrees of sensory, motor, and bladder/ bowel dysfunction. In a similar way, it may also cause sexual dysfunction. 4 In the study by Misawa et al, 18 it was observed that sexual dysfunction in patients with DCM is potentially underreported (especially considering the significantly low prevalence rates), owing to the embarrassment associated with the condition and the perception that sexual difficulties (such as ED or failure to achieve orgasm) can be consequences of natural ageing. All the studies hitherto published on sexual function in DCM patients have focused on male sexual health, and there is no evidence regarding its impact on female sexual activity.18,19 The male sexual pathologies broadly include disorders of erectile function and ejaculation.20,21 Erectile dysfunction (ED), in turn, is described to be reflexogenic or psychogenic in origin19.
Broadly, it has been reported that DCM is more likely to spare reflexogenic erectile function, for which the stimulation arises from the sacral segments of the spinal cord. 22 On the other hand, stimulation for psychogenic erection originates from the cerebral cortex and is transmitted across the thoracic/ lumbar segments; which makes it more vulnerable to be impaired in DCM.4,19,23 There is minimal information in the current literature regarding the occurrence of ejaculatory disturbance in CSM patients.
Pathophysiology of ED
ED has been associated with complications involving the vascular [endothelial production of nitric oxide (NO)] or neural pathways (with the final pathway constituted by sacral preganglionic parasympathetic fibres or nervi erigentes) or a combination of both.21,24-26 Diverse factors or comorbid conditions such as hyperlipidaemia, hypertension, diabetes mellitus (DM), obesity, alcohol abuse, neurodegenerative conditions (multiple sclerosis or Parkinson’s disease) and smoking have been associated with ED in adults. In addition, alterations in neuro-psychiatric and neuro-hormonal axes such as stress, hypogonadism and anxiety disorders have been implicated in the causation of ED.26-28 In the study by Wottrich et al, 26 the presence of ED was not independently associated with any of these major documented risk factors.
Although well-acknowledged as a cause of significant disability and distress, the issue of sexual dysfunction after spinal pathologies has been often neglected across the existing literature.4,26 Even in the large-scale SPORT (Spine Patient Outcome Research Trial, 2010), which evaluated the improvement in health-related-quality-of-life (HRQOL) following decompressive laminectomy in lumbar canal stenosis (LCS), the impact of sexual dysfunction was not discussed. 26 In the AO Spine North American Perspective Multi-center Study (2013), it was demonstrated that surgical decompression was associated with statistically significant improvements in functional and quality-of-life-related parameters in patients with cervical spondylomyelopathy (CSM). 26 However, even this study did not analyse the effect of surgical decompression on ED or assess the role of surgery in cervical stenosis.
Similarly, the true impact of surgical decompression on the recovery of sexual function is also unclear. Previous large-scale, prospective studies by Hagg et al (2006) and Choy et al (1999) reported significant improvement in overall sexual function and satisfaction; as well as erectile function following surgical treatment or laser disc decompression of patients with chronic low back pain secondary to lumbar disc herniation.29,30 On the other hand, prospective studies by Siddiqui et al (2012 and 2013) showed that even though the mean visual analog scale (VAS – for back and leg), Oswestry Disability Index (ODI) and North American Spine Society (NASS) Score for neurogenic symptoms were significantly improved at 2 years; the mean International Index of Erectile Function (IIEF)-5 score did not significantly meliorate following surgical cervical decompression.31,32 Thus, the current review was planned to comprehensively discuss the association between sexual dysfunction and DCM, available treatment options and its outcome following surgical decompression.
RO2: Patterns of Sexual Dysfunction in Patients with DCM
Overall, 4 to 68% (with a weighted mean of 38%; 95% CI: 34%–43%) of patients with DCM have been reported to develop bladder-related symptoms. A majority of the studies in the existing literature did not differentiate between isolated bladder or bowel/ bladder disturbances. 19 Among the studies that discussed bowel dysfunction, the general frequency of difficulties with defecation (prevalence rate: 6%–33%) was generally lower than the bladder-related difficulties. 19 Overall, studies have discussed the frequency of sphincter disturbances and bowel/ bladder disorders in around 7 to 100% and 5 to 30% of patients with DCM, respectively.19,33-37 In the study by Misawa et al, 18 a significant proportion (5 to 68%) of patients developed a wide variety of subjective urinary symptoms (such as difficulty in voiding, sensation of incomplete voiding, and enhanced urgency or lack of desire to void). In this study, 2, 4, 1 and 4 patients had urinary retention, nocturia, oliguria and urge incontinence, respectively. A lesion involving the cervical spinal cord can sometimes manifest with a spastic bladder, which results from detrusor sphincter dyssnergia secondary to impaired feedback from the pontine micturition center. This typically presents with symptoms of urge incontinence and increased frequency of urination. 38 Unfortunately, despite similar pathophysiology, a majority of the aforementioned studies did not elaborate on the occurrence of sexual dysfunction in their cohort of patients with CSM.
Pathophysiology of ED in DCM
Penile erection is characterised by 2 different control mechanisms involving: a. Reflexogenic and b. Psychogenic stimuli organized through spinal and supraspinal reflexes.39,40 Reflexogenic erection is caused by direct tactile stimulation of the glans or shaft of the penis, and originates from sacral (S2-4) segments of the spinal cord and is transmitted via pudendal and pelvic nerves. 41 On the other hand, psychogenic erection originates after erotic stimuli or thoughts from the cerebrum, modulated by T11-L2 segments of the thoracolumbar spine; and is transmitted finally through hypogastric, pelvic and sympathetic nerves. 41
In a previous study involving patients with complete upper motor neuron (UMN) weakness; while 95% had intact reflexogenic erections, only 9% had intact psychogenic erectile function. 42 In contrast, in patients with incomplete UMN lesions, 48% could achieve psychogenic erection (while 93% had reflexogenic erection). In this study, in all patients where the lesion was caudal to the T12 spinal level, psychogenic erection could be maintained. In patients with lower motor neuron (LMN) weakness, only a small proportion of patients could achieve psychogenic (24%) and reflexogenic (12%) erections. Based on this understanding, CSM causes an injury at the cervical spinal cord level with maintained intactness of sacral (S2-4) and TL (T11-L2) segments.
RO3: Prevalence of Sexual Dysfunction in DCM
A recently published scoping review article by Jiang et al 19 comprehensively analysed the existing literature on DCM (published between 2005 and 2020); and discussed the distribution of clinical presentation and symptomatology in these patients. The clinical symptoms in these patients in terms of decreasing order of frequency included non-specific paresthesias (86%), hand numbness or paresthesia (79%–82%), gait disturbance (72%), neck or shoulder pain (51%), bladder impairment (38%), bowel disturbance (23%), low back pain (19%), and lower extremity pain (10%). Among the autonomic symptoms, while bladder dysfunction (38%) was most commonly reported; bowel-related symptoms and sexual disorders were observed in 23% and 4% of individuals, respectively.
In another study by He et al (2006), 4 the prevalence and presentation of sexual disorders in patients undergoing surgical decompression for CSM were comprehensively discussed. Overall, 3%–6% of these patients were reported to experience sexual dysfunction, which encompassed erectile and ejaculatory dysfunction. 5 In their study, 82% (18/22) of patients with preoperative sexual dysfunction had an abnormal psychogenic erection (erection secondary to extrinsic stimuli); while the remaining 18% (4/22) had an abnormal reflexive erection (elicited by direct stimulation of the penis).4,5,7
In a recent prospective, observational study, Wottrich et al 26 evaluated the prevalence of erectile dysfunction (ED) in patients with cervical and lumbar stenosis. Among the total of 79 patients, 18 and 7 patients had cervical spinal stenosis (CS) and tandem stenosis (combined cervical with lumbar stenosis), respectively. Based on the responses to the IIEF-5/ Sexual Health Inventory for Men (SHIM) questionnaire, 72% of patients with cervical stenosis had preoperative ED (total score ≤20). The mean preoperative IIEF-5 score in CS patients was 15.52. Therefore, the relative occurrence of ED in patients with CSM is largely varied, and large-scale studies are essential to determine their true prevalence rates. As already mentioned, data regarding ejaculatory disturbances and female sexual dysfunction in DCM patients are still sparse in the existing literature.
RO4: Impact of Surgical Decompression on ED in Patients with DCM
Three prospective studies namely He et al (2006), Zhu et al (2008) and Qian (2010) involving 22, 22 and 19 patients, respectively reported substantial improvement in ED following surgical decompression in patients with CSM.4,43,44 However, these studies also highlighted a relatively poorer neurological outcome and recovery in patients with significant autonomic or sexual dysfunction.
He et al, 4 in a prospective follow-up study, evaluated the recovery of sexual function in 22 patients with CSM and ED (reflexogenic and psychogenic – as evaluated by IIEF-5 score). There was a statistically significant improvement in the Japanese Orthopedic Association (JOA) score (around 3.6; P = 0.05). In this series, a majority of patients had abnormal psychogenic erection preoperatively (82% of psychogenic vs 18% of reflexogenic ED). The sexual function, as evaluated by the IIEF-5 score, substantially improved from 28.5 preoperatively to 60.2 at the final follow-up following surgery (12-25 months; 68% recovery rate (RR); P = 0.05). The improvements in sexual function during the interim periods were demonstrated by higher IIEF-5 scores of 55 (RR: 57%), 58.2 (RR: 64%), and 57 (RR: 63%) at 5-7 months, 11-13 months, 17-19 months’ postoperative time points, respectively. It was noted that postoperatively, 95% and 91% of patients had normal reflexogenic and psychogenic erectile function, respectively. Overall, the available evidence strongly favours the beneficial role of surgical decompression in the recovery of sexual function.
RO5: Clinical Outcome in Patients with DCM-Associated Sexual Dysfunction
In the study by Zhu et al 43 involving 22 patients with DCM, substantial improvement in sexual function was reported following surgical spinal decompression. In another article, Fotakopoulos et al 12 reported a single male patient presenting with C3-4, and C5-6 cervical disc herniation with ED (without myelopathy), who demonstrated significant postoperative improvement following anterior discectomy and fusion. In another study by Lee et al involving 25 consecutive CSM patients undergoing modified open-door expansive laminoplasty, it was shown that 52% (13/25) of patients had significant bowel/ bladder and sexual dysfunction preoperatively. Among this patient cohort with autonomic and sexual dysfunctions, 77% (10/13) of patients had substantial recovery following surgical decompression.
In the study by Sinha et al, 7 the clinical presentation and final recovery were evaluated in 34 patients undergoing expansive cervical laminoplasty. Overall, 5.8% of patients in this cohort presented with sexual dysfunction. The overall recovery rate was assessed based upon the pre-and post-operative neurosurgical cervical spine score (which mainly evaluates the upper and lower extremity functional status, and pain/ sensory disturbances); with the RR% determined by the formula, [(postoperative score-preoperative score)/(14-preoperative score)]*100. Broadly, 8 patients had a RR of 100% in this series. The presence of preoperative sexual dysfunction (as well as bladder/ bowel dysfunction) was associated with poorer results (as low as 50% RR), in comparison with the cohort without any sexual abnormalities.
On the other hand, in another recent prospective, observational study by Wottrich et al, 26 there was no statistically significant improvement in the overall erectile function following cervical decompression surgery in patients who presented with ED preoperatively. The mean preoperative IIEF-5 score in CS patients was 15.52; while the mean change in IIEF-5 scores at the 6- and 12-month postoperative time points were 0.53 (P = 0.64) and −0.28 (P = 0.84), respectively. Based on reported evidence, the presence of autonomic abnormalities was associated with relatively poorer improvements following the surgical intervention.
RO6: Rehabilitative Approach for Sexual Recovery in DCM Patients
Boerger et al 8 reviewed the rehabilitative approaches in patients with sexual and other autonomic dysfunctions. Locomotor exercise and physical therapy play a significant role in meliorating the strength, stamina and mobility of patients with sexual dysfunction.45-47 In addition, pelvic floor exercises have also been reported to significantly improve the sexual function in DCM patients with ED, satisfaction-, orgasm- or arousal-related issues; and premature ejaculation.48,49 From the evidence available in patients with spinal injuries, body weight-supported treadmill exercises, assisted locomotor training, and pelvic floor muscle training are beneficial in improving bladder function and urinary incontinence.50,51
Prioritization of Sexual Function Recovery – Patients’ Perspectives
In a cross-sectional, observational study by Davies et al1,2,6 (involving data from an online survey conducted on 481 participants), the DCM patients were asked to organize and rank their recovery domains (such as arm and hand function, gait, trunk and upper body function, sexual function, sensory symptoms and autonomic symptoms) in the descending order of priority. Based on the responses of the patients, pain carried the highest priority for recovery among patients (39.9% of respondents); while the recovery of gait, sensory symptoms, and upper extremity functions were ranked by the respondents in the descending order of priority (constituting 20.2%, 11.9% and 11.5%, respectively). Based on the survey, the recovery of sexual, bladder/ bowel and trunk functions was prioritized by a substantially smaller proportion of DCM patients (with these functions chosen by only 5.7%, 3.7% and 3.5% of the respondents, respectively). There was no specific explanation for the lower priority given to the recovery of sexual function in this study; although relatively lower prevalence rate, older age category, higher degrees of disability associated with other symptoms, and greater hesitation among the patients to address these symptoms can be possible reasons underlying this observation.
Limitations
The current review has some limitations that need to be acknowledged. Considering the limited evidence on the topic we did not scrutinize the evidence based on their study design or quality. There was no study discussing the prevalence of ejaculatory dysfunction or female sexual disturbance. There are also concerns regarding the possible under-reporting of the symptoms and the need for enhanced awareness among patients and physicians. Although we found limited evidence on the topic, we tried to be comprehensive and elaborated on the all evidence obtained in the context of the prior research objectives developed. Again, quantitative evidence could not be synthesized owing to the variability in the assessment and paucity of the literature on the topic.
In order to overcome the underreporting of sexual dysfunction, future studies evaluating patients with DCM could include questions on their sexual function in their routine follow-up questionnaire during every follow-up to better estimate their incidence and prognosis following surgery.
Conclusions
ED occurs in 3 to 6% of patients with DCM, with a majority of patients suffering from ED from psychogenic origin. Surgical decompression can significantly improve the sexual recovery in these patients. Patients with ED have overall poorer neurological recovery. The need for large-scale, high-quality, prospective studies evaluating the exact prevalence, patterns of presentation, occurrence in female patients, prognostic indicators, rehabilitative approaches and outcome following surgical decompression cannot be understated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.