
Abstract
Study Design
Systematic review and Meta-analysis.
Objectives
To quantify the association of preoperative depression on patient reported outcome measures (PROMS) after cervical spine surgery.
Methods
We systematically searched PubMed, Cochrane, Embase, Scopus, PsychInfo, Web of Science, and ClinicalTrials.gov until September 14, 2023. Studies including adults undergoing cervical spine surgery and comparing PROMs between depressed and non-depressed patients were included. The primary outcome was the postoperative change in disability, pain, and physical function. Secondary outcomes included absolute disease severity before and after surgery. We conducted random-effects meta-analysis.
Results
After screening 3813 articles, 20 studies were included, encompassing 3964 patients (mean age 57, 51% males) with median follow-up duration of 12 months. There was significant heterogeneity in estimates of the primary outcome (I 2 = 81%). While patients with depression had a greater magnitude of improvement compared with patients without depression, it was not statistically significant (SMD = 0.04, [95% CI: −0.07, 0.16], I 2 = 80%; P = 0.48). However, patients with depression exhibited worse absolute disease severity preoperatively (SMD = −0.31, [-0.44, −0.19], I 2 = 84%; P < 0.001) and postoperatively (SMD = −0.31, [−0.48, −0.15], I 2 = 89%; P < 0.002). Sensitivity analyses with meta-regression found that older age, sex (male-to-female ratio), percentage of comorbidities, study quality, follow-up duration, number of adjusted factors in the analysis, and surgical approach were significant sources of heterogeneity.
Conclusions
Patients with depression experienced similar improvements in disability, pain, and physical function after cervical surgery compared to patients without depression. However, patients with depression exhibited worse disease severity before and after surgery.
Introduction
Degenerative cervical spine disease is a major health problem, often presenting with symptoms such as pain, numbness, and weakness, which can severely impact quality of life.1-3 High-level evidence suggests that in selected individuals, cervical spine surgery leads to substantial improvements in pain and quality of life.4-6 Consequently, cervical fusion surgery is one of the most common surgeries performed in the United States, with 112,400 surgeries performed annually.7-9
While cervical spine surgery has demonstrated effectiveness in appropriate candidates, approximately 20%–30% of surgical patients continue to experience symptoms and long-term disability.10-12 The persistence of symptoms might be exacerbated by the presence of co-morbid mental health disease confounding evaluations, as depression has been previously reported as a significant risk factor for ongoing disability after cervical spine surgery. 13
Despite this proposed association, the influence of preoperative depression on cervical spine surgery outcomes remains undefined. To bridge this evidence gap, this study performed a systematic review and meta-analysis evaluating the impact of depression on outcomes of cervical spine surgery. Our secondary objective was to conduct meta-regression analyses to identify factors explaining the heterogeneity in the literature studying depression in cervical spine surgery.
Methods
Search Strategy and Selection Criteria
Our study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 14 and targeted the following PICO question: in patients undergoing cervical spine surgery, to what extent does preoperative depression affect patient-reported outcomes?
The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO: CRD42024607600). Eligible studies were prospective or retrospective cohort studies that had the following characteristics: included adult patients undergoing surgery for degenerative cervical spine disease, compared patient-reported outcome measures (PROMs) before and after surgery in patients with vs without depression (evaluated before surgery), had a minimum postoperative follow-up of 6 months, and used validated PROMs in cervical spine patients. These PROMs assess clinical domains relevant to cervical spine disease, primarily pain (eg, Visual Analog Scale for neck and arm pain), physical function (eg, PROMIS Physical Function), and disability (eg, Neck Disability Index), providing a structured assessment of disease severity and key patient outcomes. We excluded studies that did not measure depression preoperatively, as assessment after surgery could introduce recall bias. Other exclusion criteria were studies including surgeries for lumbar disease, tumor, trauma, and/or infection, studies using administrative datasets, case-reports, or literature reviews, and studies not published in English.
We searched PubMed, Cochrane, Embase, Scopus, PsychInfo, Web of Science, and ClinicalTrials.gov until September 14, 2023. The search strategies (eTable 1) were developed with a medical librarian (AH).
Selection of Studies and Data Extraction
Screening of titles and abstracts was done independently by two reviewers (SJ and JKZ). Disagreements were resolved by consensus or a third reviewer (JKG). Data extraction was done independently by two reviewers (BB and SY) using a customized data-extraction form gathering study and patient-level data. Subsequently, one reviewer (SJ) validated all the variables and calculated standardized mean differences (SMD) to assess the effect size of mean differences between patients with vs without depression. Discrepancies were resolved by consultation with the senior author (JKG). Agreement between the two reviewers was quantified using Cohen’s Kappa statistic. Information regarding the methods employed for depression classification and PROMs used for outcome assessment is available in eTables 2 and 3.
Outcome of Interest
Our primary outcome was the change in cervical spine related disability, pain, and physical function from baseline to postoperative follow-up. Our secondary outcome was the absolute disease severity reflected by PROMs measuring disability, pain, and physical function before and after surgery.
Study Quality Assessment
The assessment of each study’s quality was performed using Newcastle-Ottawa Scale.15,16 Additionally, other study-level factors reflecting study quality were evaluated, including study design, journal impact factor, level of evidence, and rigor of analytical approach.
Data Analysis
Data necessary to calculate the standardized mean difference (SMD) included mean values, standard deviations (SD), and the patient count in each group. SMDs evaluated differences in outcomes between patients with and without depression. Because of substantial variability of methods defining depression and evaluating cervical disease severity across studies, a random-effects meta-analysis was used. Forest plots were used to display meta-analysis findings, and the extent of variability was quantified by I 2 statistics. Before inclusion in the meta-analysis, all PROMs were transformed to have the same direction (ie, increasing score reflecting worse disease severity). To prepare continuous data for synthesis, methods described in Cochrane Handbook were used to impute missing information (eg, estimating mean and SD from median and interquartile range or 95% confidence intervals). 16 Studies assessing the same PROMs were aggregated into groups and evaluated using sub-group meta-analyses.
Interpreting effect estimates of disease severity can be challenging when similar outcomes can be assessed using different scales (eg, numeric rating scale, visual analogue scale, etc.). To address this, we consolidated PROMs measuring the same aspect of disease into a standard metric as described previously 17 (rationale in eTable 4).
Sensitivity Analysis
To investigate potential sources of heterogeneity (I 2 ) in the relationship between depression and outcomes, sensitivity analyses were conducted via meta-regression. We extracted several variables that could potentially account for heterogeneity in outcomes across studies. These variables included patient-level, study-level, and intervention-level factors that may influence interpretation of the results. The association of each of these variables with our outcome was evaluated using univariable meta-regression. Any variable with R2 > 0 in univariable analysis was included in multivariable meta-regression analysis. To evaluate potential publication bias secondary to small study effects, funnel plots and the Egger test of asymmetry were used. All analyses were performed in R version 4.2.1 (R Project for Statistical Computing). Meta-analysis and meta-regression were performed using metafor package version 4.1.4. The threshold for significance was set at 2-tailed α < 0.05.
Results
Study Selection
A total of 3813 unique articles were screened and 207 underwent full-text review. Of those, 187 were excluded (reasons for exclusion in Figure 1) and 20 met eligibility criteria.18-37 There was substantial agreement between reviewers during full-text screening (0.8≤ κ ≤ 1). Prisma flow diagram of search results.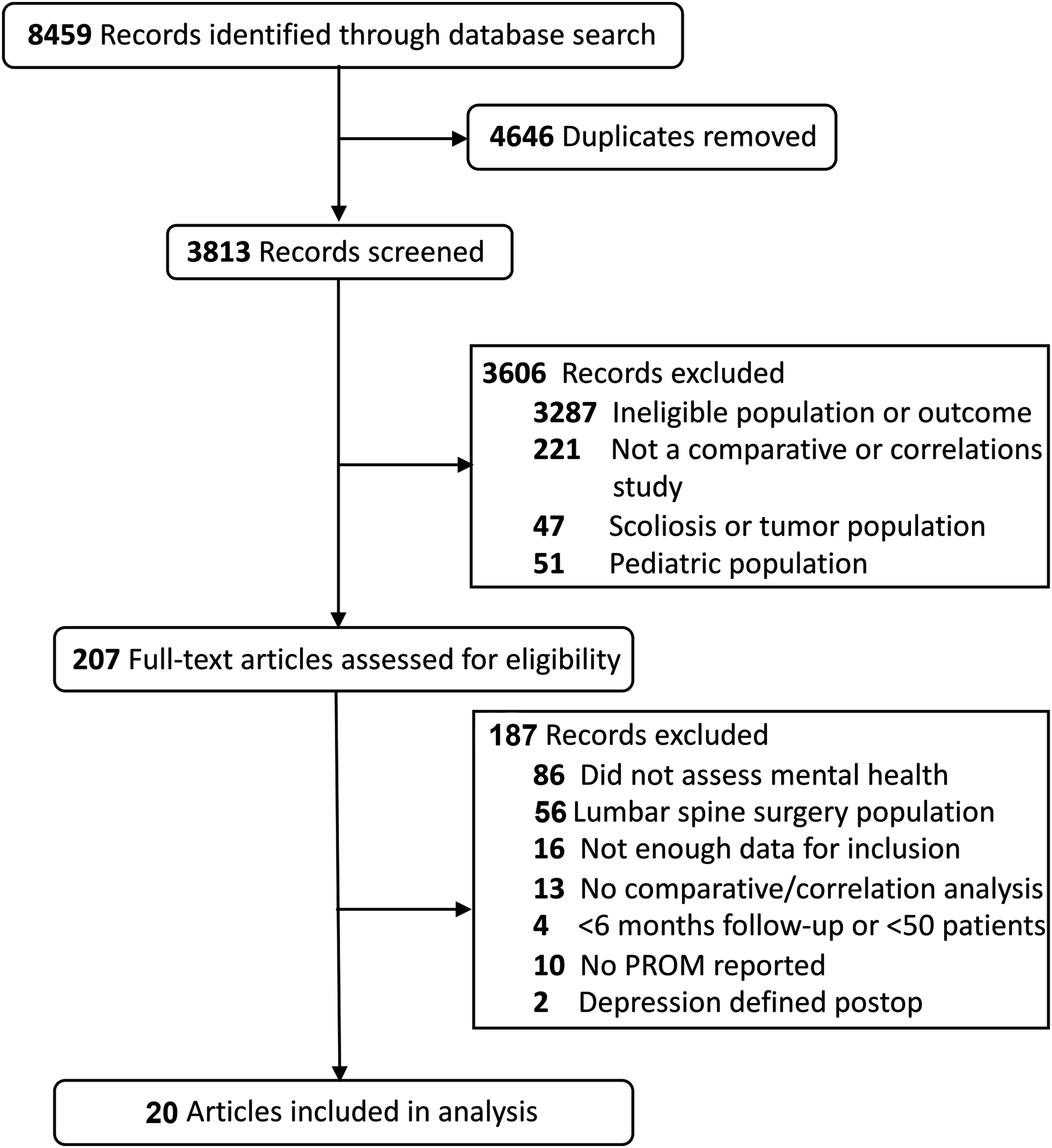
Study Characteristics
Study Characteristics.
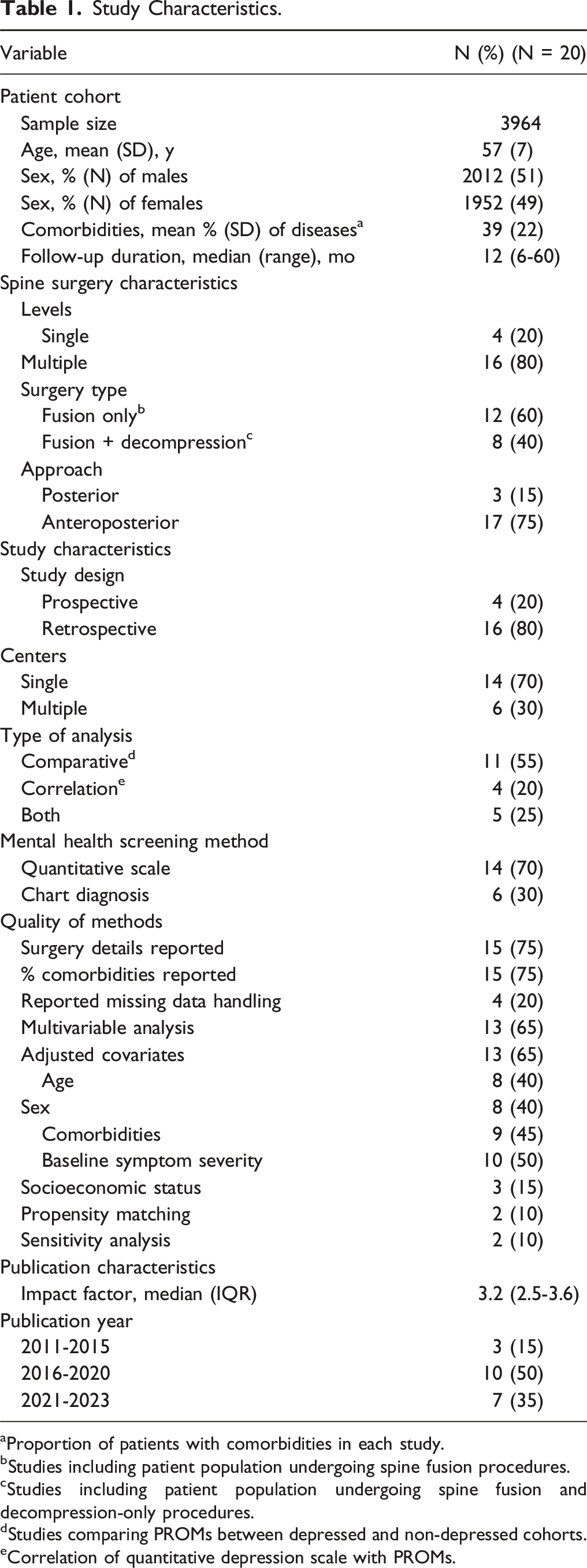
aProportion of patients with comorbidities in each study.
bStudies including patient population undergoing spine fusion procedures.
cStudies including patient population undergoing spine fusion and decompression-only procedures.
dStudies comparing PROMs between depressed and non-depressed cohorts.
eCorrelation of quantitative depression scale with PROMs.
Quality Assessment
Among included studies, 75% (15) reported information on surgical details (e.g., number of treated levels), 20% (4) reported approaches for handling missing data, and 65% (13) conducted multivariable analyses. However, more than half of the studies did not account for important confounders; for example, only 40% (8) of studies adjusted for age and sex, and 15% (3) adjusted for socioeconomic status (eg, insurance status) (Table 1).
Overall, the studies were of moderate quality; the median Newcastle-Ottawa Scale was 7 (6-8) (eTable 6). There were heterogeneous methods used to assess preoperative depression, with 70% (14) of studies using quantitative scales and 30% (6) using depression diagnosis from medical history. The most common quantitative methods used were the Hospital Anxiety and Depression Scale scores in 20% (4) and Short Form Mental Component Summary used in 20% (4) of studies (eTable 2). Among common depression measures, 45% (9) of studies used differing cut-offs on the same scales to stratify depression diagnosis (eTable 2). In terms of outcomes, most studies reported primary outcomes related to cervical spine disability, pain, and physical function. The most common PROM was the Neck Disability Index (NDI), followed by the visual analogue scale (VAS) for neck and arm pain scores, and Short Form Physical Component Summary (SF-PCS). The full list of study outcomes measures with frequencies used is given in eTable 3. Overall, there was an excellent inter-rater reliability between the independent reviewers (eTable 7).
Disability, Pain, and Physical Function
Overall, there was significant heterogeneity [I
2
= 81%] in the estimates for the primary outcome of change in disability, pain, and physical function from preoperative baseline to postoperative follow-up. Postoperative change in all domains did not differ significantly between cohorts. However, the direction of change favored greater improvement in disease severity for patients with depression (SMD = 0.04, [95% CI: −0.07, 0.16], I
2
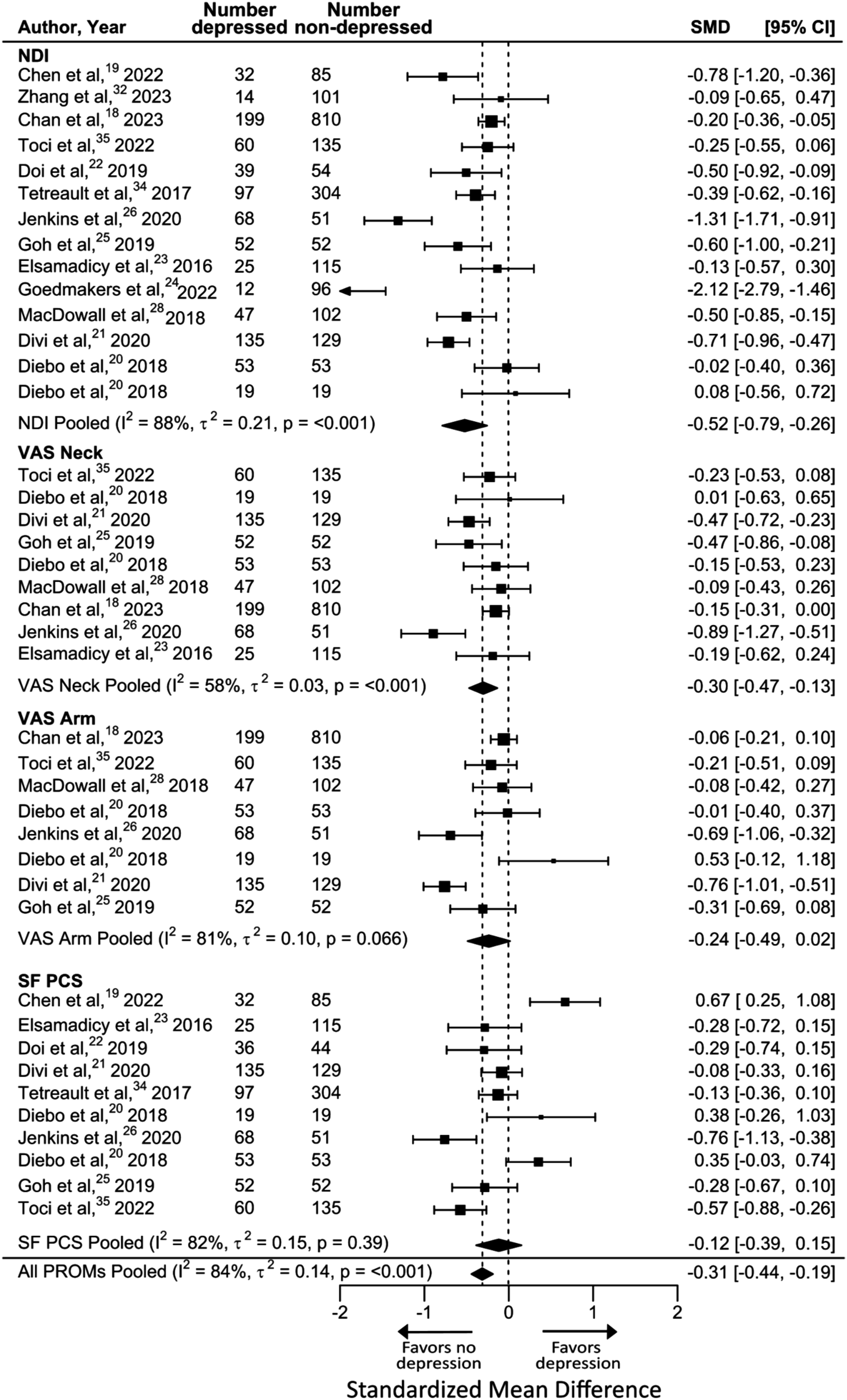
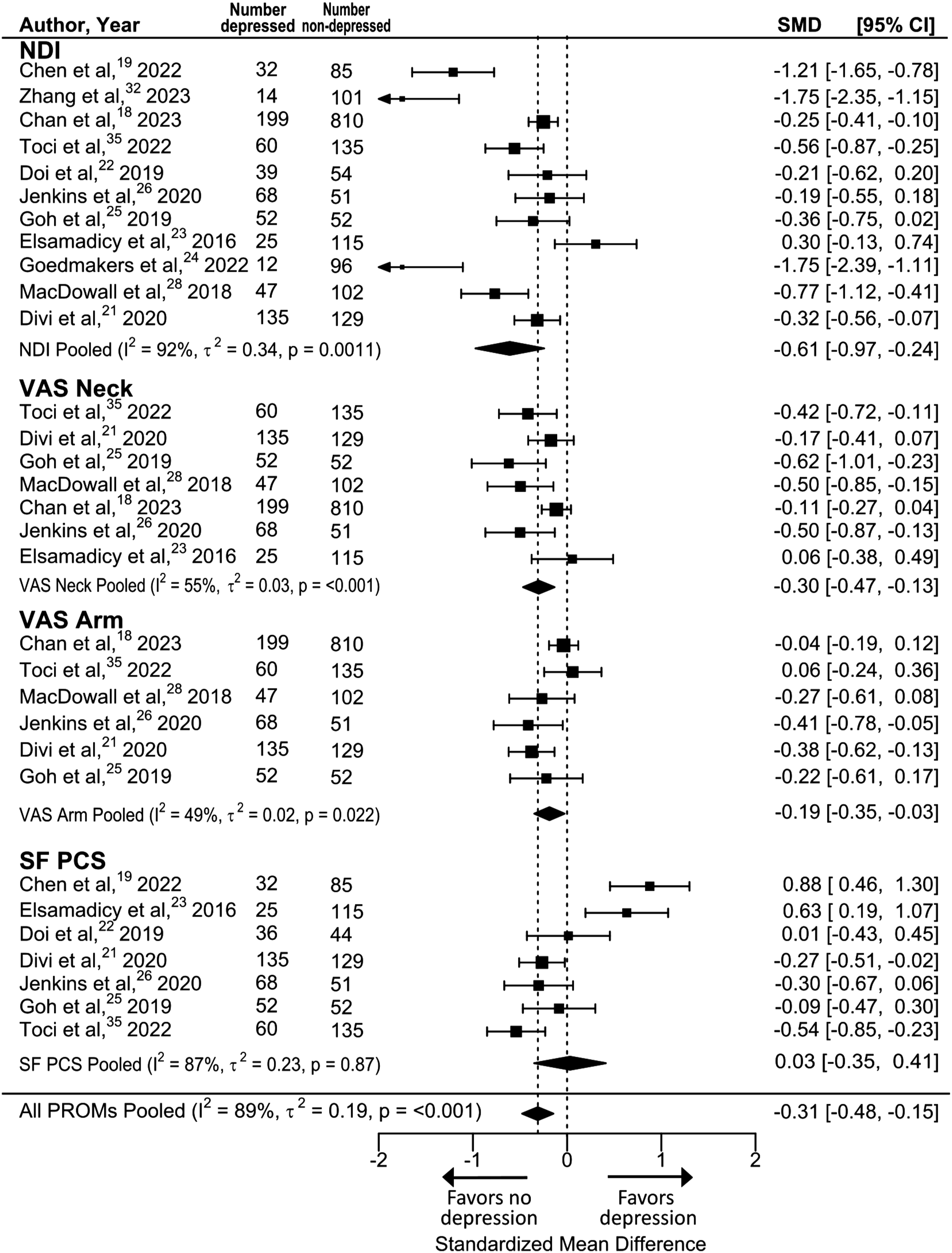
= 80%; P = 0.47) (Figure 2). Despite experiencing similar improvement after surgery, patients with depression had worse absolute disease severity in disability, pain, and physical function both before (SMD = −0.31, [−0.44, −0.19], I
2
= 84%; P < 0.001) (Figure 3) and after surgery (SMD = −0.31, [−0.48, −0.15], I
2
= 89%; P < 0.002) (Figure 4). Meta-analysis of primary outcomes, improvement in PROMs in patients with vs without depression preoperatively. Meta-analysis of secondary outcomes, pre-operative PROMs in patients with vs without depression preoperatively. Meta-analysis of secondary outcomes, post-operative PROMs in patients with vs without depression preoperatively.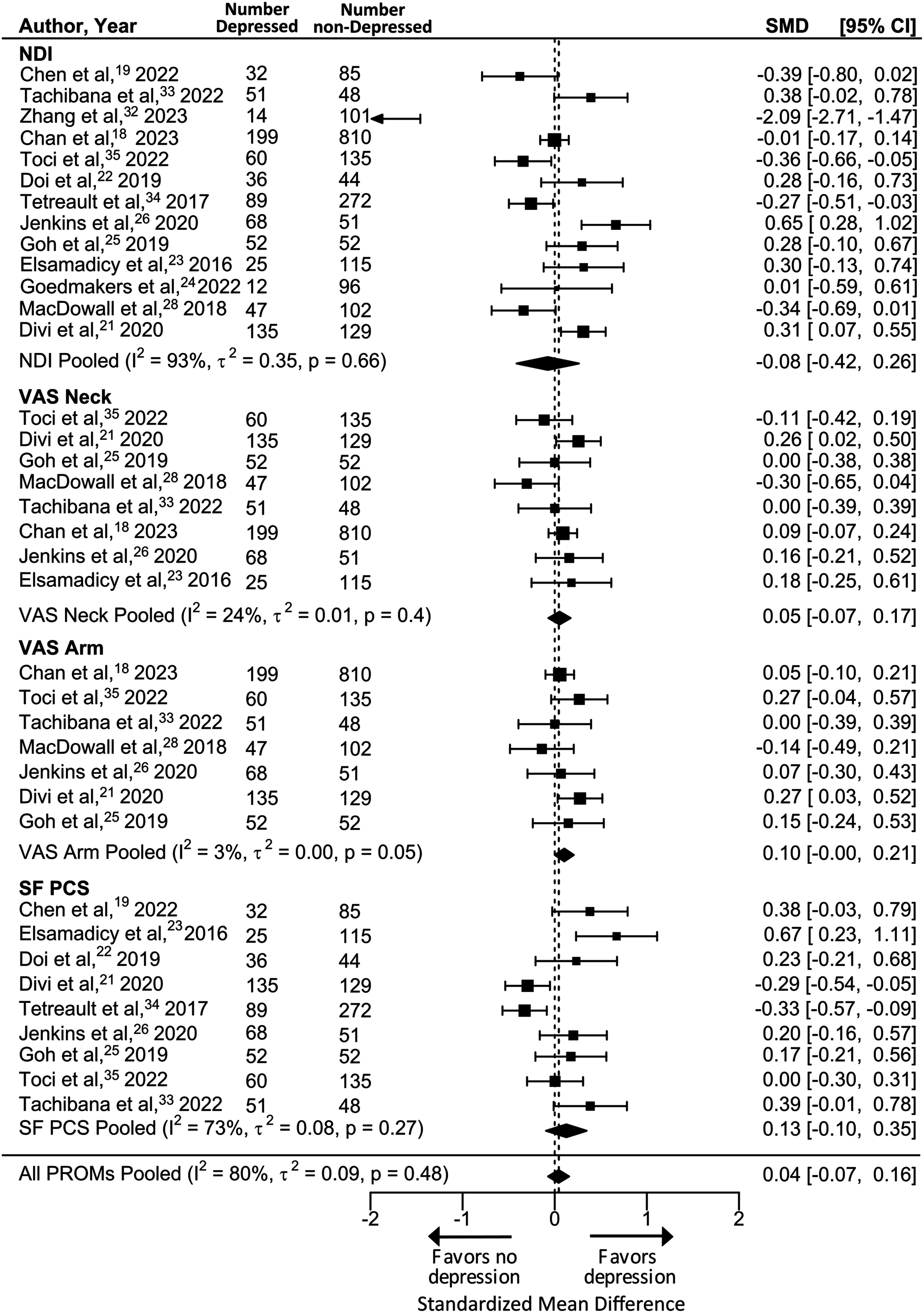
Quality of Life
Assessing the effect of depression on quality of life, seven studies reported the EQ-5D score. Significant heterogeneity (I2 = 62%) was found in the estimates for change in quality-of-life after surgery. Patients with depression experienced greater improvement in quality of life after surgery than patients without depression, but this difference was not statistically significant (SMD = 0.12, [95% CI: −0.14, 0.38]; P = 0.35). Regarding the absolute quality of life scores, patients with depression had significantly worse quality of life both preoperatively (SMD = −0.49, [-0.86, −0.13], I 2 = 75%; P < 0.008) and postoperatively (SMD = −0.31, [-0.56, −0.06], I 2 = 50.83%; P = 0.015).
Sensitivity Analyses
Meta-Regression Analysis
We next examined the heterogeneity of our results. The I 2 was 81%, which reflected high between-study variability for the primary outcomes. To determine if study-level, patient-level, or intervention-level factors explain this variance, we performed a meta-regression analysis.
Meta-Regressions to Identify the Variables Explaining I 2 in Improvement in PROMs in Patients With vs Without Depression.
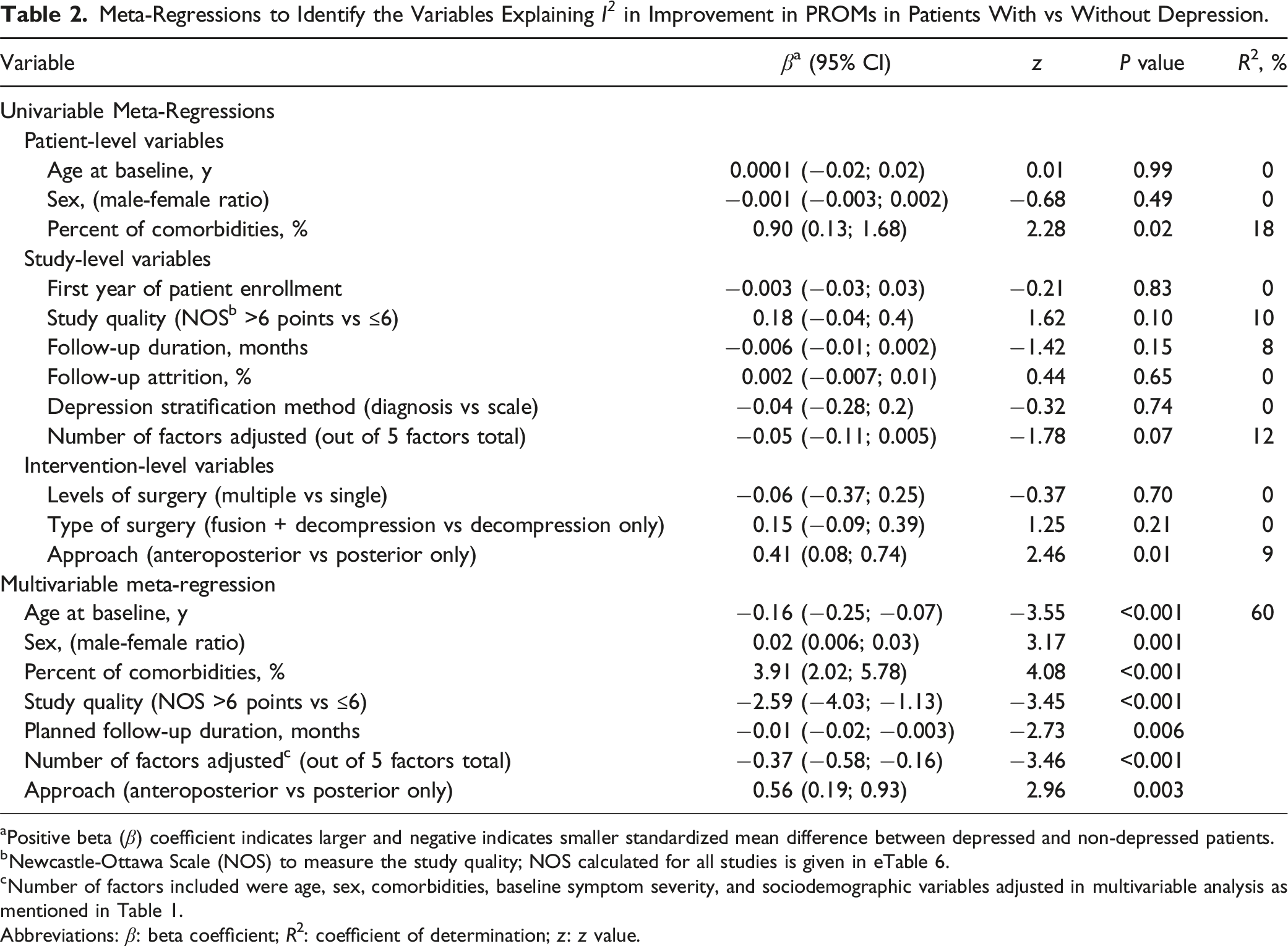
aPositive beta (β) coefficient indicates larger and negative indicates smaller standardized mean difference between depressed and non-depressed patients.
bNewcastle-Ottawa Scale (NOS) to measure the study quality; NOS calculated for all studies is given in eTable 6.
cNumber of factors included were age, sex, comorbidities, baseline symptom severity, and sociodemographic variables adjusted in multivariable analysis as mentioned in Table 1.
Abbreviations: β: beta coefficient; R2: coefficient of determination; z: z value.
Publication Bias
Visual inspection of the funnel plot for primary outcomes showed mild asymmetry (eFigure 1). 38 There was an evident outlier present (SMD ≤ −2) 34 ; removing this outlier slightly reduced asymmetry. According to the Egger test (z = 1.59, P = 0.11), no evidence of publication bias or small study effect was detected. In contrast, several studies clustered within the region of significance (ie, P < 0.05). This finding implies that the apparent asymmetry is likely attributable to factors such as varying study quality and/or differences in depression measures leading to heterogeneity in outcomes across studies. 39
Discussion
In our meta-analysis, we found that patients with preoperative depression had a similar magnitude of improvement in neck disability, pain, physical function, and quality of life after cervical spine surgery compared to patients without depression. Nevertheless, patients with depression had worse absolute disease severity at baseline and postoperative follow-up. These findings contribute important knowledge regarding the influence of preoperative depression in cervical spine disease and response to surgical intervention. This evidence may inform preoperative counseling and optimization for surgical intervention in patients with comorbid depression.
The association between psychological comorbidities such as depression and/or anxiety with worse postoperative pain outcomes has been well-studied in spine research.40-43 Degenerative cervical spine disease results in neck pain, radiculopathy, and myelopathy, significantly impacting function and quality of life.44-46 The incidence of psychiatric comorbidities is higher in patients with such symptoms, 47 particularly in patients with cervical myelopathy. 48 Though comorbid depression could attenuate treatment response and result in worse outcomes,49,50 the literature on this point remains inconclusive. This meta-analysis fills a crucial evidence gap regarding the relationship between depression and cervical spine surgical outcomes.
The results of this meta-analysis provide synthesized evidence that patients with comorbid depression undergoing cervical spine surgery have similar potential for improvement in disability as patients without depression. Our findings align with recent results in lumbar spine populations, 17 as well as studies evaluating depression in other musculoskeletal diseases where optimizing antidepressive therapy reduced pain severity and disability. 51 At the same time, patients with depression do present with more severe disease preoperatively, and on average, do not achieve the same level of function postoperatively as non-depressed patients.52-54 Therefore, while cervical spine surgery remains beneficial in patients with depression, further work is needed to evaluate the extent to which preoperative depression may be a modifiable risk factor that can be intervened upon to improve outcomes.
Interpretation of the meta-analysis results is complicated by heterogeneity in patient populations and study methods. Indeed, the studies included in this meta-analysis had significant heterogeneity (I2>80%) for the primary outcome, which might impact the interpretation of overall effect estimates. To assess sources of heterogeneity, we evaluated several study-level, patient-level, and intervention-level factors. Notably, a larger percentage of common comorbidities was associated with greater standardized mean difference in the primary outcome of PROM improvement. This suggests that, in studies with more comorbidities among patients, depressed patients tended to show greater improvement in disability than their non-depressed counterparts. This underscores the need to adjust for comorbidities that may be more common in depressed patients and could negatively impact outcomes. Additionally, our study showed that older age was associated with lower SMDs, suggesting that depression may have a more deleterious impact on surgical outcomes in older patients. This aligns with existing literature showing that depression in older adults may be associated with a greater impact on quality of life compared to depression in younger individuals.17,55 In addition, our meta-regression highlighted that substantial variance was associated with study design features; for instance, higher quality studies with higher Newcastle-Ottawa score and studies adjusting for more factors may have accounted for other variables confounding the impact of depression. These findings have important implications for future studies in spine surgery and related musculoskeletal literature regarding the impact of mental health comorbidities on surgical outcomes.
Although mental health comorbidities in general have become a growing focus in spine disease,56,57 depressive disorder is one of the most frequent psychiatric disease among patients with chronic musculoskeletal pain.58-60 Our finding that patients with depression may not achieve the same quality of life postoperatively as those without depression suggests that improved preoperative screening and perioperative depression treatment might lead to improved surgical outcomes. Incorporating mental health screening into routine preoperative assessments could allow clinicians to provide a more informed prognosis and refer patients for depression treatment. Screening and treating depression in cervical spine surgery appears to enhance postoperative perception of health status, 25 elevate patient satisfaction level, 61 and improve postoperative quality of life. 18 On the other hand, our findings showed that even with depression, patients have comparable potential improvement in all domains, suggesting that depression should not be considered a contraindication to cervical spine surgery. Finally, our investigation underscored a notable absence of standardization in preoperative instruments, emphasizing the need for uniform approaches to both instruments and cutoff selection for evaluating depression in spine surgery.
Limitations
Our study has strengths, including a thorough search strategy, robust evidence synthesis, and rigorous exploration of confounding factors. Nevertheless, it has limitations. First, substantial heterogeneity across studies may have impacted the meta-analysis conclusions. Likewise, heterogeneous depression screening methods and the lack of a clear definition for depression may have introduced additional variability into the analysis. Common data elements for depression evaluation should be a focus for future research. Second, patients were categorized into depression groups based on history and depression scales rather than a full psychological assessment. Third, this study was unable to further disentangle the role of other mental health comorbidities, such as anxiety. Finally, our study cannot establish a causal relationship between depression and spine-related disability, warranting future investigations.
Conclusions
Findings from this meta-analysis suggest that patients with depression have worse cervical disease severity before and after surgery. However, they had similar improvement in spine-related disability compared to patients without depression. Our findings support the role of appropriately indicated cervical spine surgery in patients with depression and emphasize the potential value of preoperative mental health treatments in improving surgical outcomes.
Supplemental Material
Supplemental Material - Influence of Preoperative Depression on Cervical Spine Surgery Outcomes: A Systematic Review and Meta-Analysis
Supplemental Material for Influence of Preoperative Depression on Cervical Spine Surgery Outcomes: A Systematic Review and Meta-Analysis by Saad Javeed, Salim Yakdan, Braeden Benedict, Samia Saleem, Muhammad Kaleem, Justin K. Zhang, Madelyn R. Frumkin, Angela Hardi, Brian Neuman, Michael P. Kelly, Burel R. Goodin, Thomas L. Rodebaugh, Wilson Z. Ray, Jacob K. Greenberg in Global Spine Journal .
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (1K23AR082986-01A1).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.