
Abstract
Study Design
Retrospective Cohort Study.
Objective
The aim of this study was to evaluate the efficacy of our proposed surgical procedure named unilateral exposure channel-assisted (UCA) laminoplasty in treating degenerative cervical myelopathy (DCM), and the postoperative volume changes of cervical paraspinal muscles.
Methods
From January 2020 to January 2022, 104 patients with DCM underwent unilateral open-door laminoplasty, among which, 63 patients underwent UCA laminoplasty (UCA group) and 41 patients underwent traditional laminoplasty (LP group). The radiological and clinical parameters as well as postoperative complications were recorded and analyzed before operation and during the follow-up.
Results
The operation was completed successfully for all patients from both groups, who showed significant but comparable improvement in clinical outcome indicators including mJOA score, Neck pain VAS score, NDI score and radiological indicators including spinal canal diameter and area at the final follow-up compared to pre-operation. When conducting the intra-group comparison, less intraoperative time consumption and blood loss, less postoperative drainage and lower incidence of axial symptoms were observed in patients from UCA group than LP group. Furthermore, we found better preservation of C2-7 cobb angle, cervical curvature index (CCI) and cervical paraspinal muscle on the hinge side in patients underwent UCA laminoplasty than traditional laminoplasty.
Conclusion
The UCA laminoplasty showed similar efficacy on alleviating clinical symptoms, and priority on maintaining cervical sagittal balance, minimizing intraoperative invasion, speeding up postoperative rehabilitation, reducing paraspinal muscle atrophy and postoperative axial symptoms when compared with traditional unilateral open-door laminoplasty.
Keywords
Introduction
As the most common cause of spinal cord dysfunction in adults worldwide, degenerative cervical myelopathy (DCM) is characterized by acquired stenosis of the cervical spinal canal secondary to intervertebral disc degeneration or ligamentous aberration, which results in chronic spinal cord compression and disability. 1 According to existing clinical guidelines, mild DCM could be managed with conservative methods including cervical traction, pharmacotherapy, bedrest and avoidance of risky activities, surgical decompression may be inevitable for moderate and severe DCM. 2
The surgery procedures for cervical spine could be broadly divided into direct decompression anteriorly and indirect decompression posteriorly, our previous study had deeply compared the strengths and weaknesses of anterior cervical discectomy and fusion (ACDF), unilateral open-door laminoplasty (LP), or laminectomy with Fusion (LF) in treating DCM, the open-door laminoplasty was strongly recommend for multilevel DCM according to our data, 3 which was similar to the evidences reported in literature.
LP is widely performed in the management of DCM because of the straightforward approach, ease of multilevel application, and ability to obtain circumferential decompression.4-6 However, due to paraspinal muscle being dissected from the spinous process and lamina, almost all patients experience varying degrees of paraspinal atrophy postoperatively, this is strongly associated with worse clinical outcomes, as highlighted by concurrent axial symptoms (AS).7,8 Over the years, several studies used different modifications of LP procedures to prevent AS via reducing paraspinal muscle sarcopenia or atrophy, with no promising results reported. 9
In this study, we proposed a new surgical strategy termed unilateral exposure channel-assisted (UCA) laminoplasty, which could be an alternative strategy to solve the problem of AS through reducing muscle damage on the hinge side.
Material and Methods
Study Population
A total of 104 patients undergoing laminoplasty from January 2021 to January 2023 were included in this study, all patients signed informed consent. Ethical approval of this retrospective study was given by the Naval Medical University ethics committee review board (accession number: 2019SL019). The medical records, preoperative and postoperative radiographs, computed tomography (CT) and magnetic resonance imaging (MRI) of the cervical spine were reviewed on all patients.
Inclusion criteria: ① Patients underwent laminoplasty because of DCM; ② Patients treated with traditional open-door laminoplasty or unilateral exposure channel-assisted laminoplasty. The surgery involved no less than 4 laminas; ③ The patient is over 30 years old and under 70 years old. Exclusion criteria: ① Patients with incomplete imaging data or missing follow-up; ② Laminoplasty with the assistance of lateral mass screws; ③ Individuals with a history of cervical spine surgery; ④ Severe deformities, infections, tumors, etc. in the cervical spine; ⑤ Merge neurological related diseases such as syringomyelia and Parkinson’s disease.
Patient Demographics: Overall and by Treatment Group.
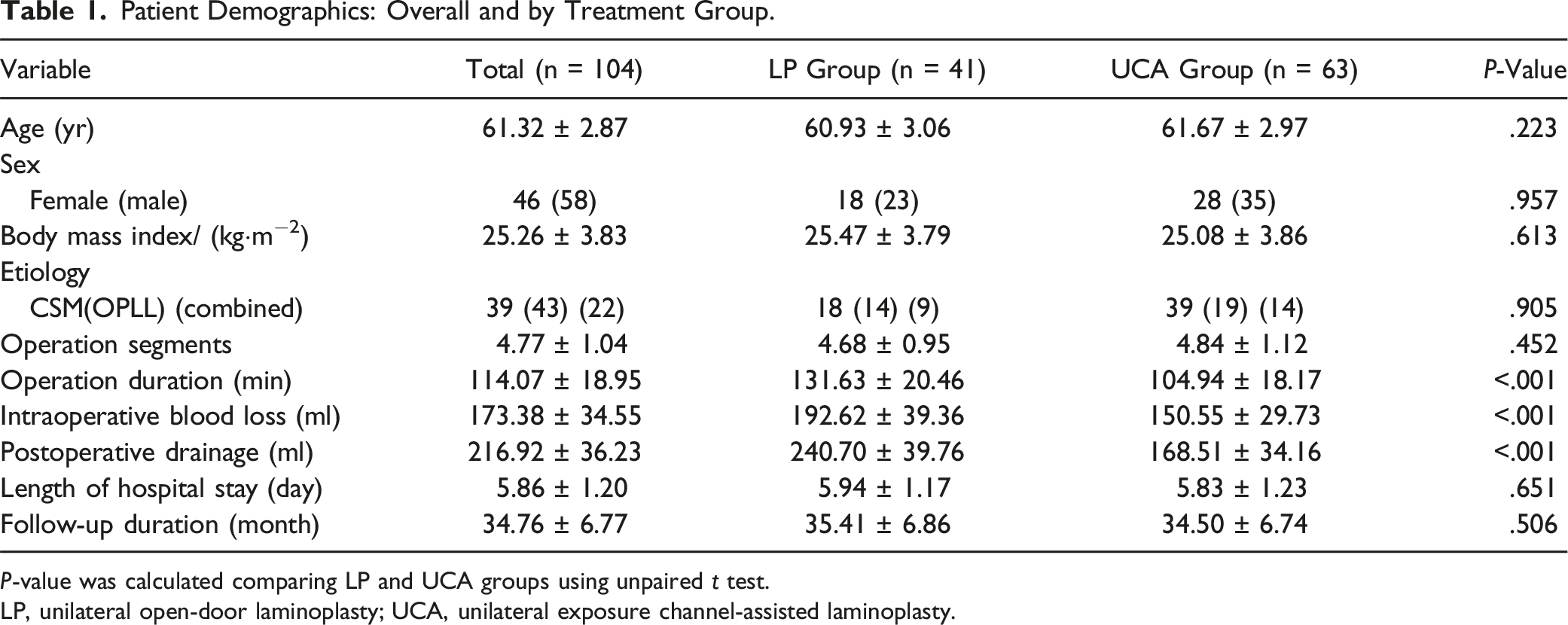
P-value was calculated comparing LP and UCA groups using unpaired t test.
LP, unilateral open-door laminoplasty; UCA, unilateral exposure channel-assisted laminoplasty.
Surgical Management
The Traditional Unilateral Open-Door Laminoplasty With Bilateral Exposure (LP)
A posterior midline exposure was performed through skin and fascia down to spinous process, cervical lamina was exposed bilaterally to the junction of lamina and lateral mass. Both open side (the patient’s left side) and hinge side (the patient’s right side) gutter was made with a high-speed burr along an imaginary line separating laminar arches from the articular processes. The internal cortex of the lamina on the hinge side was preserved, which was completely resected on the open side. Then, the lamina was elevated from the open side, followed by arch plates fixation and mini screws insertion. 10
The Unilateral Exposure Channel-Assisted Laminoplasty (UCA)
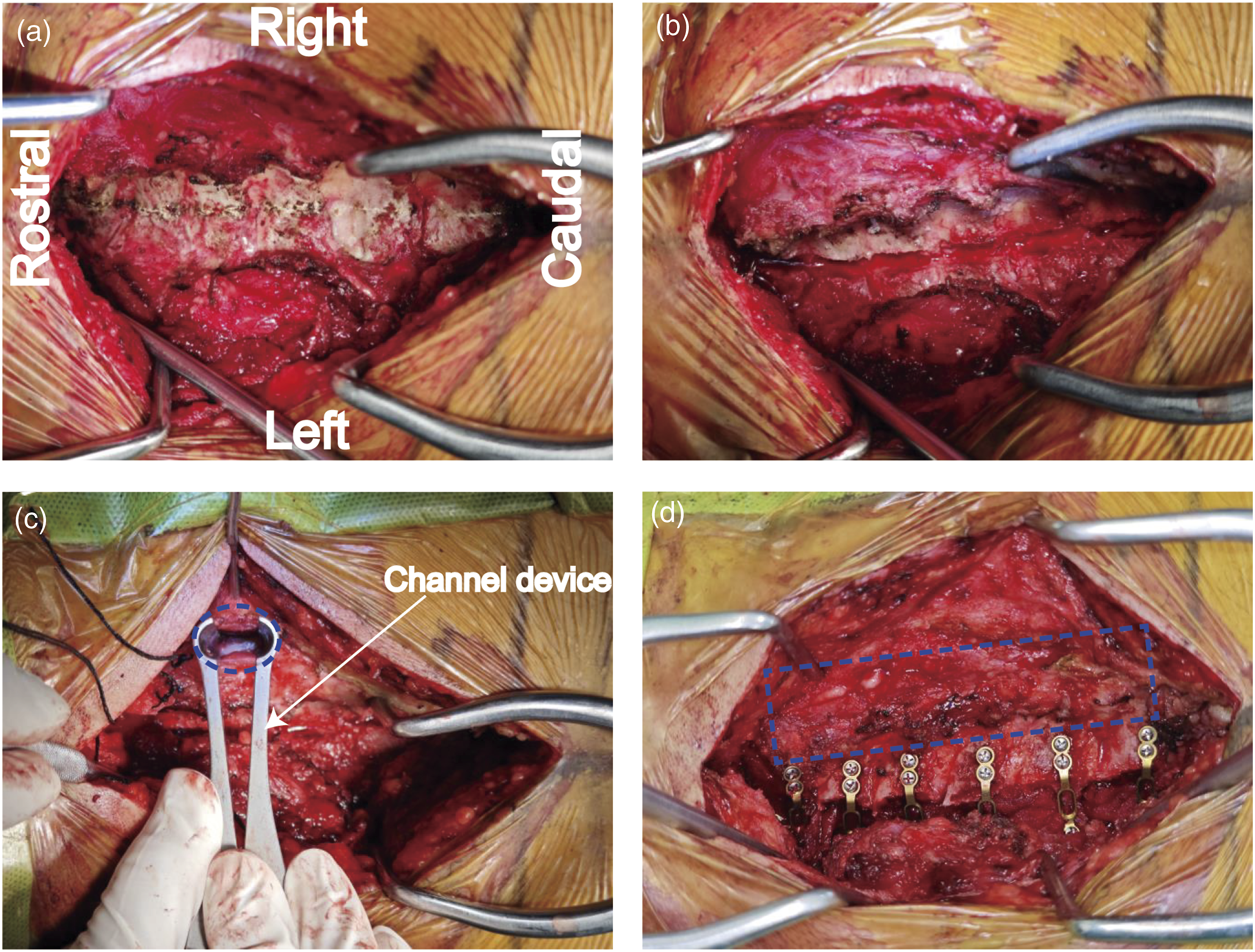
A posterior midline exposure was performed through skin and fascia down to spinous process, cervical laminas were unilaterally exposed at the patient’s left side (open side) (Figures 1 and 2). Then, a gutter of the open side was made with a high-speed burr, with internal cortex of the lamina resected completely. After blunt separation of paraspinal muscle at approximate 1.0 cm lateral to the spinous process, an expandable channel device was used to expose the lamina of the hinge side, it was critical for maintaining strict perpendicular alignment between the access channel trajectory and the laminar plane, the angulation and positioning of the channel were determined based on the fully exposed laminar inclination angle (abduction and cephalad tilt) on the open-door side. Later, the hinge gutter was made with a high-speed burr within this channel, with internal cortex of the lamina preserved, to prevent hinge lamina excessive thinning or fracture, it was recommended to elevate the laminar from the open-door side to feel the resistance with the access channel maintained in situ, which was convenient to add additional bone sculpting as needed. After the hinge gutter was completed, brain cotton was packed into the access channel to establish graded compression hemostasis, then the channel device was extracted. Finally, the lamina was elevated from the open side, followed by arch plates fixation and mini screws insertion, muscles and ligaments on the hinge side were mostly intact after surgery. Schematic diagram of traditional laminoplasty and our UCA laminoplasty. (A) Before exposure. (B) During UCA laminoplasty, the lamina on the open side was exposed through the classical midline approach, where paraspinal muscles were subperiosteal dissected from the lamina; By contrast, the lamina on the hinge side was exposed through paraspinal approach, where paraspinal muscles were bluntly separated without dissection, and then an expandable channel device was inserted to create operating space for subsequent procedures. (C) Standard unilateral open-door procedure was performed using bilateral exposure of lamina through midline approach. The key steps of UCA laminoplasty (C2-7). (A) The cervical lamina of C2-C7 were exposed on the patient’s left side. (B) A full-thickness gutter was made on the open side with a high-speed burr. (C) Blunt separation of the paraspinal muscle and inserted the expandable channel at the hinge side of C4. A partial-thickness gutter with internal cortical bone preserved was made with a high-speed burr within this channel. The hinge of C2 and C3 were already completed. Blue dashed circle indicates the Channelview of lamina. (D) Muscles and ligaments on hinge side of C2-C7 were basically intact after surgery. Blue dashed rectangle indicates the intact muscle and ligament on the hinge side.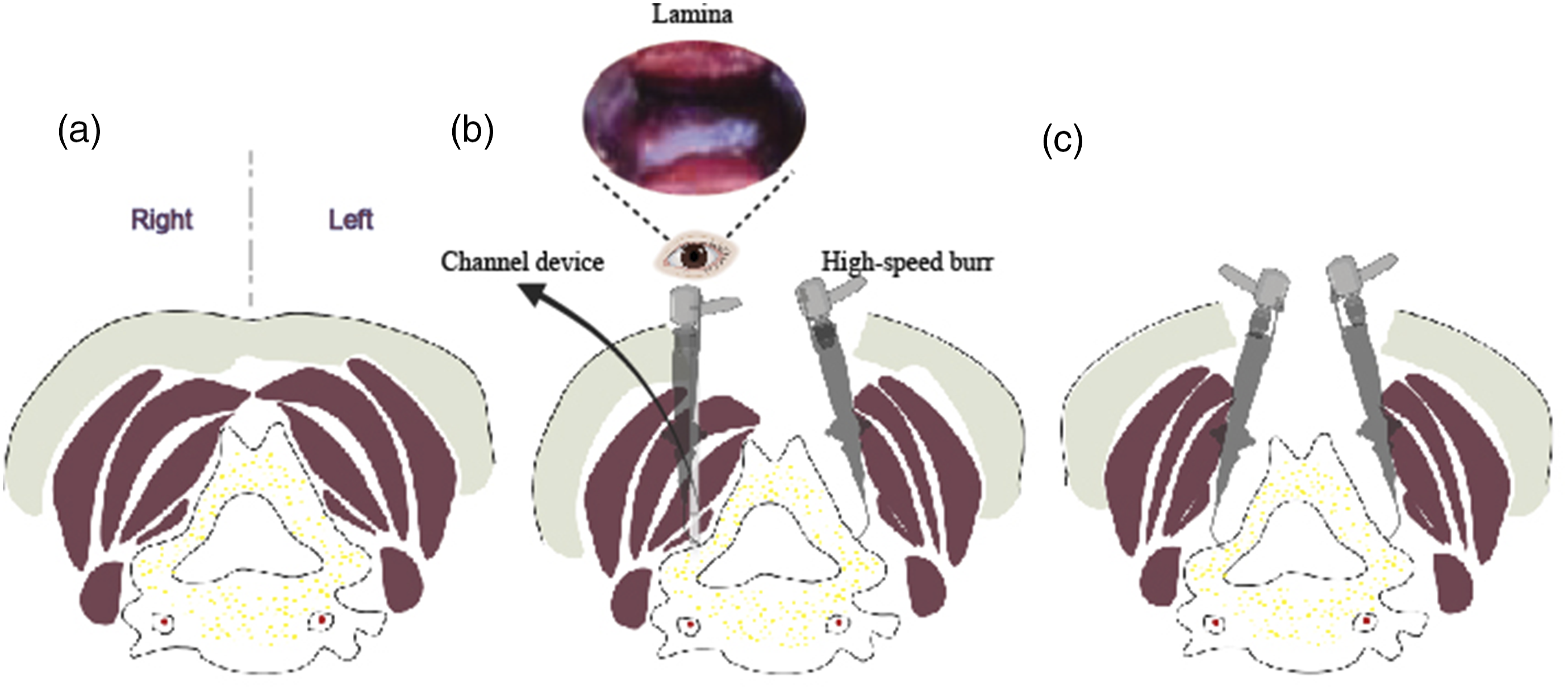
Radiographic Analysis
Preoperative and postoperative cervical alignment was measured by the C2-7 Cobb angle, which was measured between the lower endplates of C2 and C7. Cervical lordosis was measured on lateral radiographs using the cervical curvature index (CCI) as described by Ishihara.
11
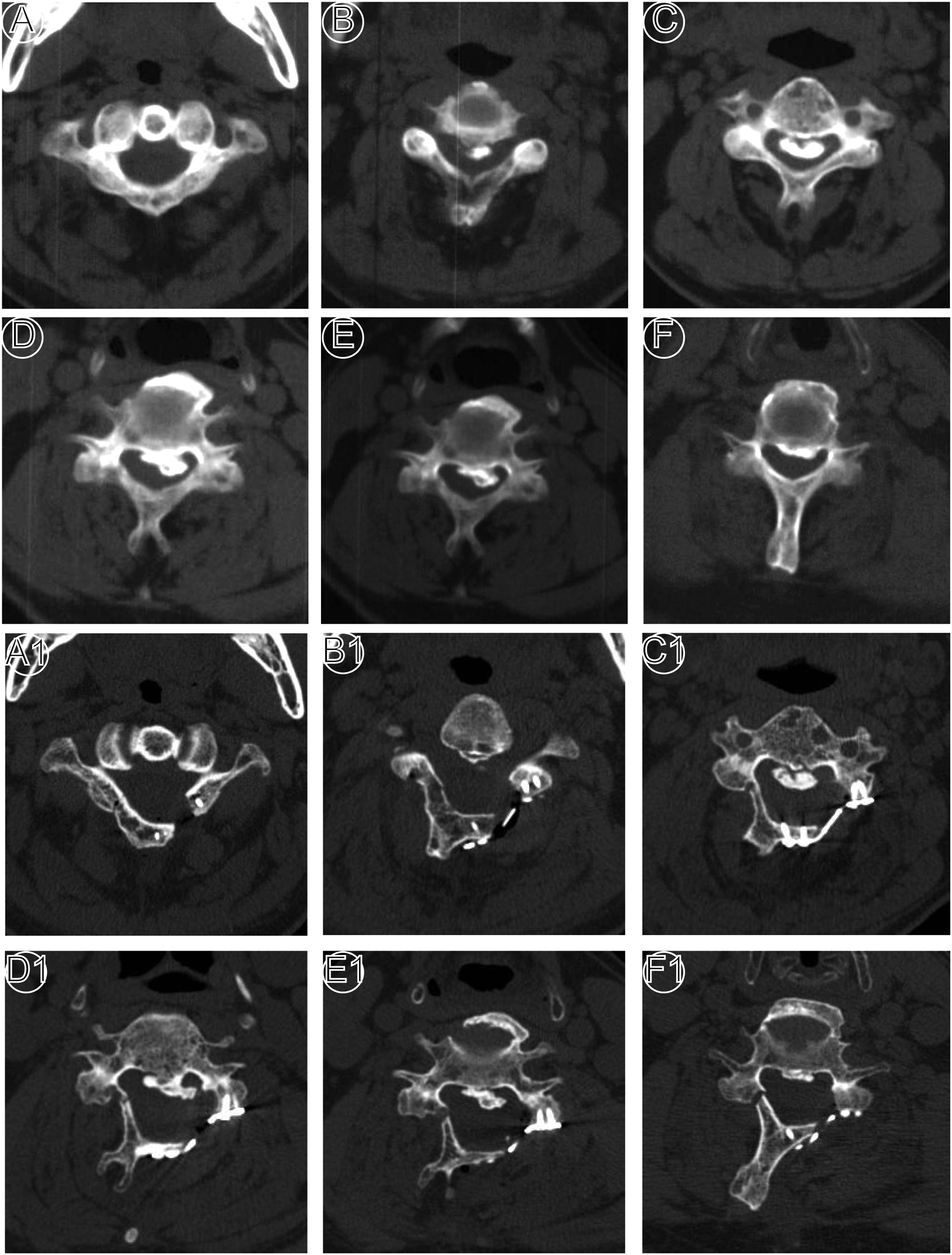
Spinal canal diameter and area of involved levels were measured in CT axial plane, and the mean values were used for analysis (Figures 3 and 4). Representative images of patient that underwent UCA laminoplasty. Preoperative and 3 days postoperative anteroposterior (A and E), lateral (B and F) X-ray radiographs, computed tomography sagittal plane images (C and G), T2-weight sagittal plane magnetic resonance images (D and H). Representative axial computed-tomography images of patient that underwent UCA laminoplasty. (A-F) Preoperative axial CT of C1∼C6; (G-L) 3 days postoperative axial CT of C1∼C6.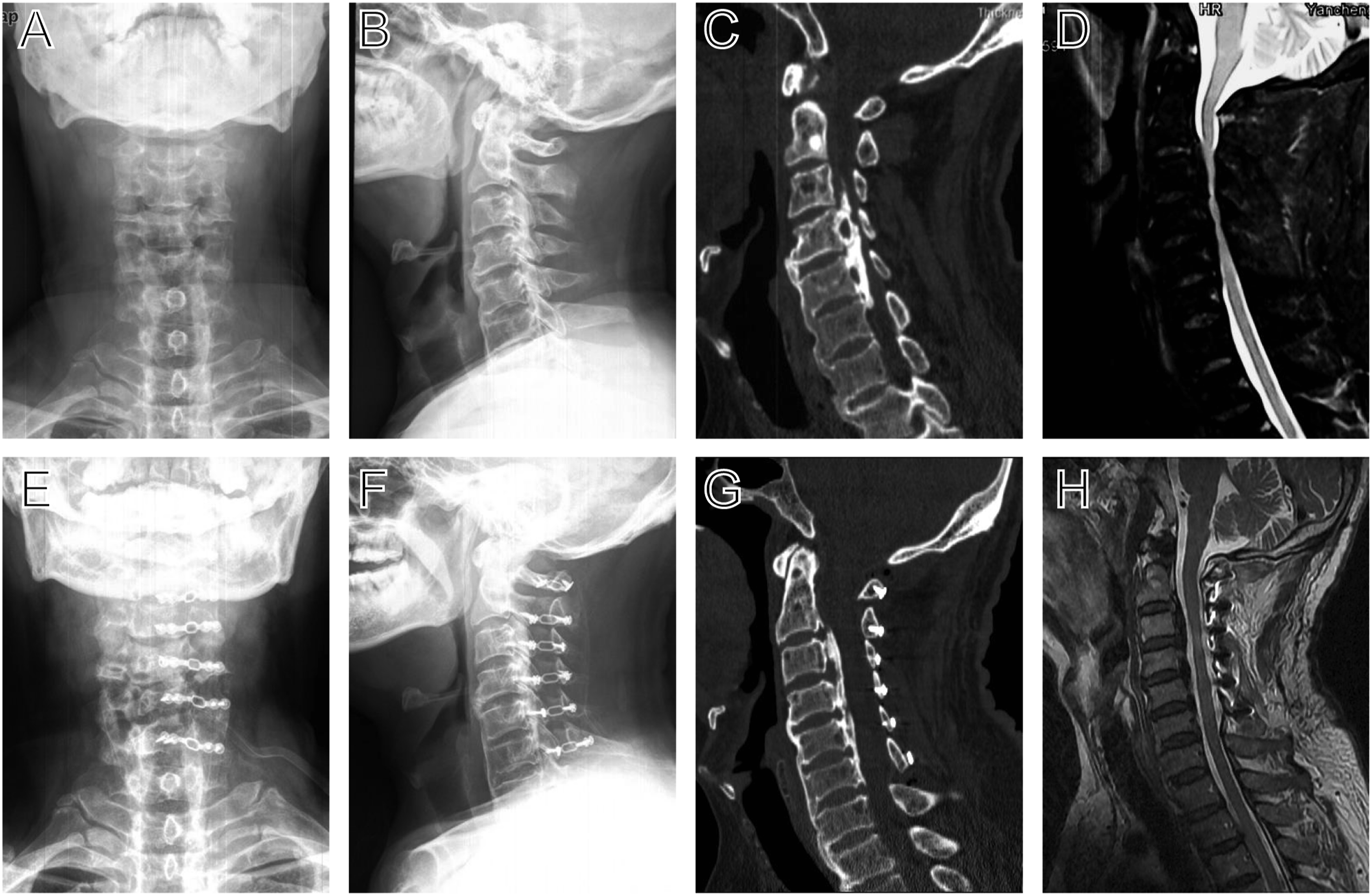
Paraspinal Muscle Volume Evaluation
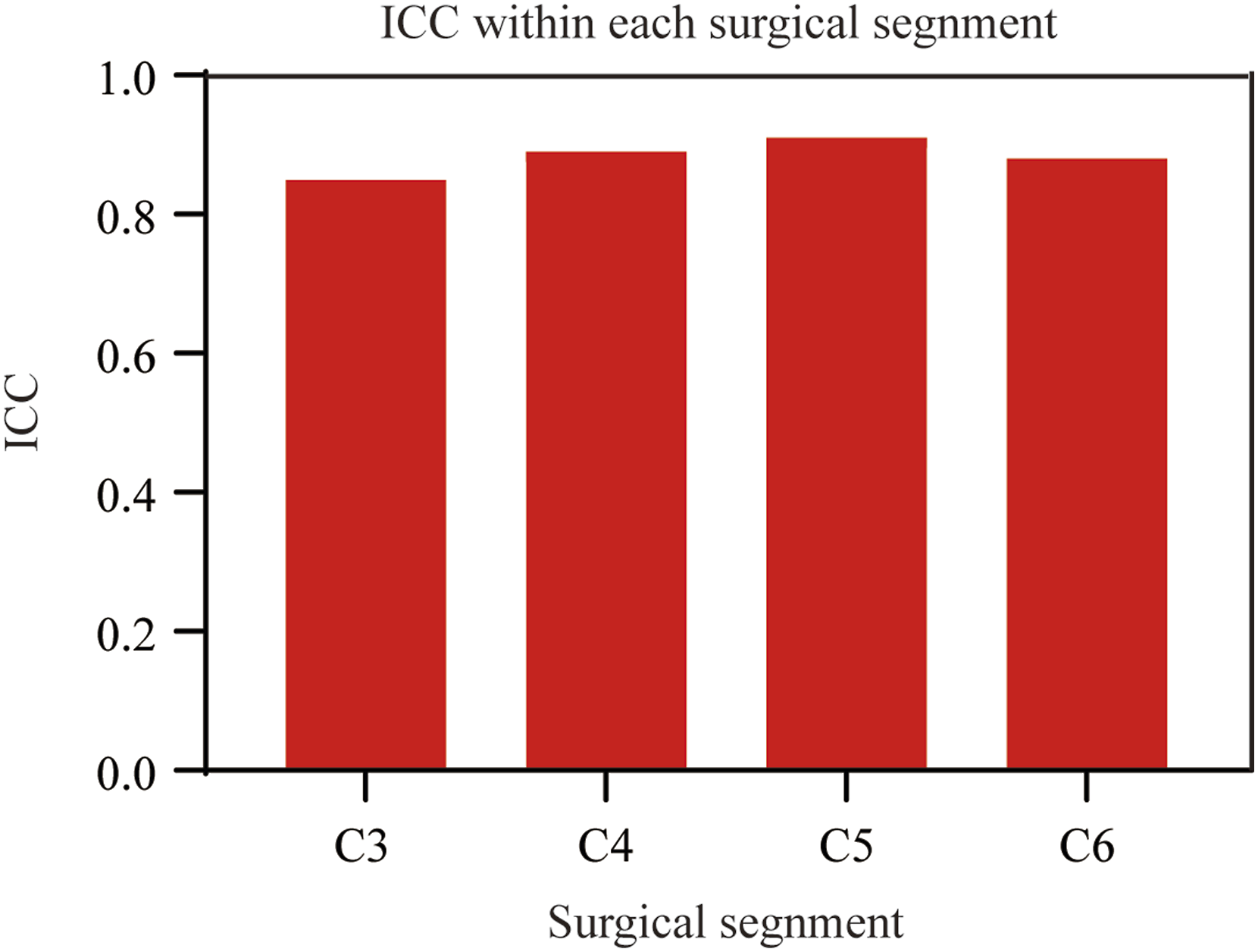
The volume of posterior paraspinal muscles was quantified using T2-weighted axial MRI. The muscle areas of the multifidus, semispinalis, and longissimus were measured as a group using Scion Image software (Figure 5). Since the surgical levels are generally C3-C7 or C2-C7, we routinely measure the paravertebral muscle volume at C3-C6 segments for statistical analysis. The representative area data of each level comes from the average of 3 consecutive image slices. Two independent clinical research assistants, who were blinded to all clinical information, performed radiological measurements, and the average values of both observers were used in the present study. The inter- and intra-observer reliability of our MRI measurements were assessed using intraclass correlation coefficient (ICC) (Figure 6). Representative axial magnetic resonance images of patient who underwent UCA laminoplasty. (A-D) Preoperative cross-sectional MRI showing the spinal cord under compression and normal paraspinal muscle. (E-H) 2 months postoperative cross-sectional MRI showing the spinal cord after decompression and muscle atrophy on the hinge side. Intraclass correlation coefficient (ICC) values of muscle volumn within each surgical segnment.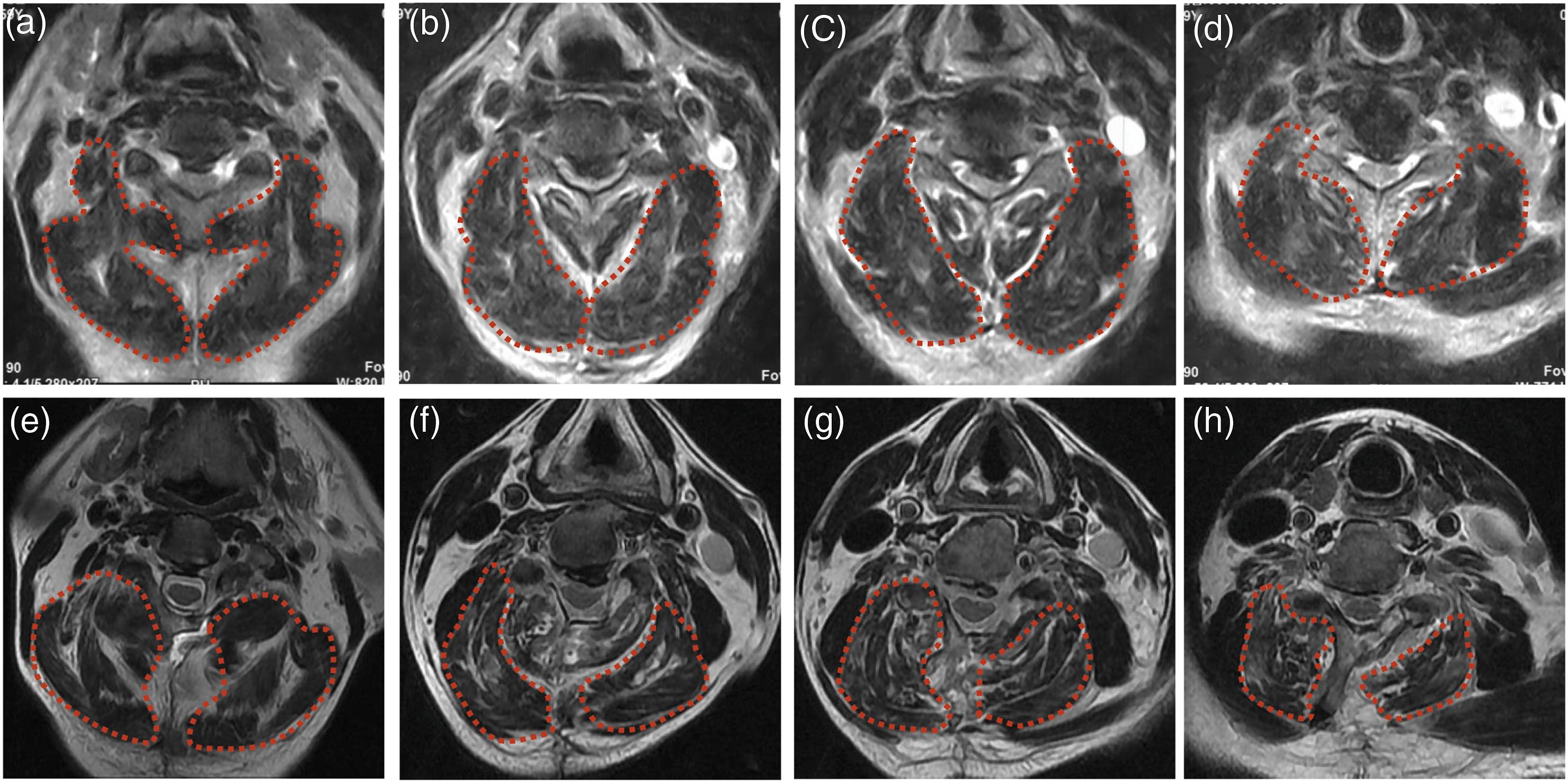
Clinical Evaluation
Cervical Dysfunction Index (NDI) and Japanese Orthopedic Society (JOA) scores were used to assess neurological function. Axial neck pain was evaluated by the Visual Analog Scale (VAS) score. Postoperative complications included C5 nerve root palsy, nerve root or cord injury, cerebrospinal fluid (CSF) leakage, and postoperative infection or implant displacement. Clinicians responsible for postoperative outcome assessments were blinded to treatment group allocation. Patient identifiers and group assignments were concealed through anonymized coding in the assessment database. All evaluations were performed by independent clinicians who had no involvement in the surgical procedures or perioperative care.
Blinding
In this study, we have data independent managers and statisticians that are responsible for data collection and analysis, who were blinded about the surgical procedure, clinical staff were excluded from the data analysis and outcome assessment.
Statistical Analysis
Statistical analysis was performed using SPSS software version 20.0 (SPSS, Chicago, IL). Distributions of variables were presented as means ± standard deviation. We used t test and analysis of variance (ANOVA) for continuous variables and Chi-square tests for categorical variables. P < .05 was considered statistically significant.
Results
Patient Demographics
A total of 104 patients were included. Of these patients, 63 were in the UCA group and 41 in LP group. Age, Sex, Body mass index (BMI), underlying pathology, operation segments, length of hospital stay, and follow-up duration did not demonstrate any significant difference between 2 groups (P > .05, Table 1). The intraoperative time consumption, blood loss and the postoperative drainage in UCA group were significantly less than those in LP group (P < .05, Table 1), which suggests the superiority of UCA laminoplasty in reducing intraoperative invasion and speeding up postoperative rehabilitation.
Radiological Assessment
Comparison of Radiographic and Clinical Outcome Between LP and UCA Groups.
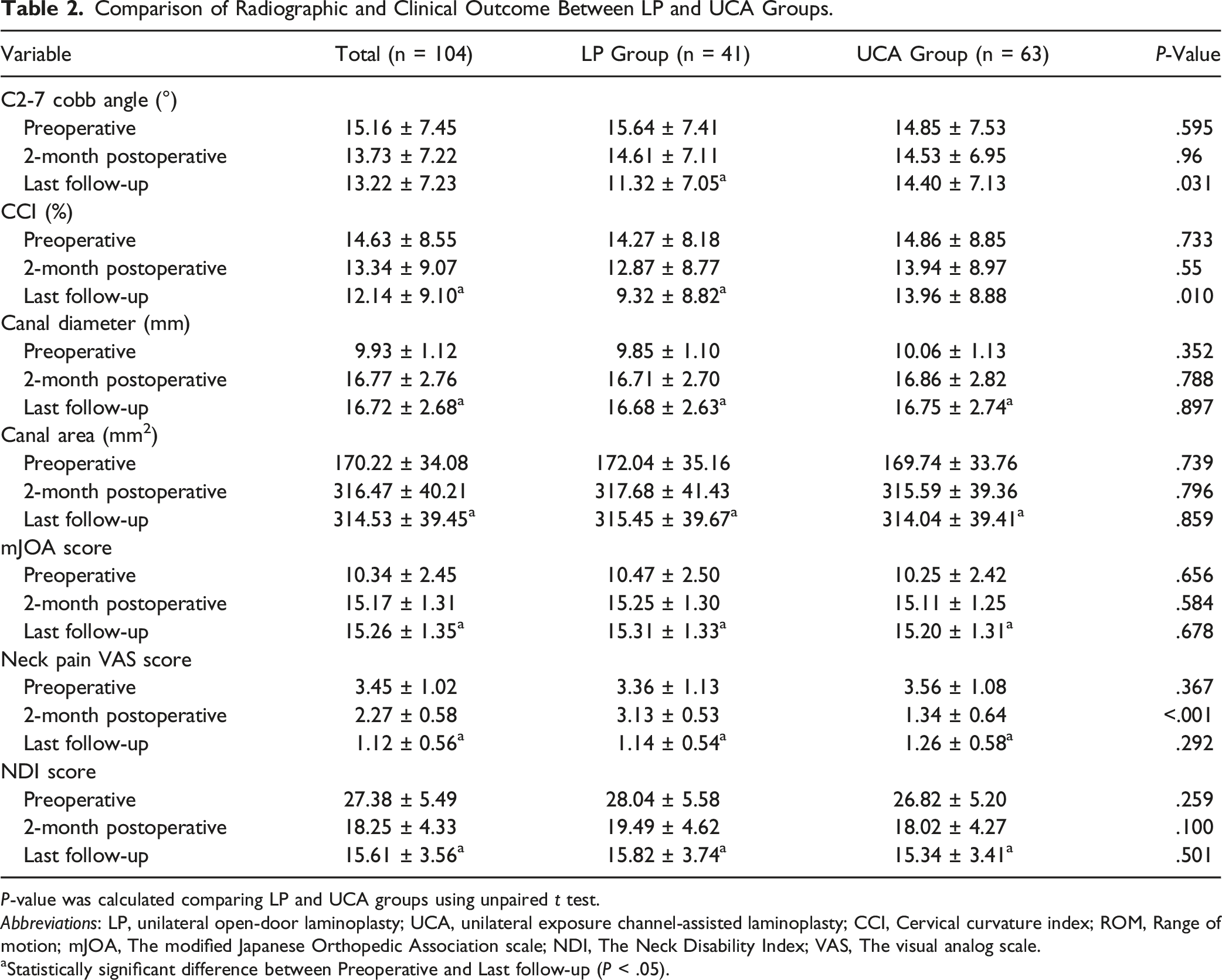
P-value was calculated comparing LP and UCA groups using unpaired t test.
Abbreviations: LP, unilateral open-door laminoplasty; UCA, unilateral exposure channel-assisted laminoplasty; CCI, Cervical curvature index; ROM, Range of motion; mJOA, The modified Japanese Orthopedic Association scale; NDI, The Neck Disability Index; VAS, The visual analog scale.
aStatistically significant difference between Preoperative and Last follow-up (P < .05).
Clinical Assessment
All the clinical outcome indicators like mJOA score, Neck pain VAS score and NDI score showed significant improvement in both LP and UCA groups after surgery (P < .05, Table 2), while the mJOA score and NDI score did not demonstrate any significant difference between LP and UCA groups during the follow-up (P > .05, Table 2), only the neck pain VAS scores in the UCA group showed more reduction than LP group at 2 months postoperative (P < .05, Table 2), this kind of advantage was disappeared at the last follow-up.
Muscles Assessment
Comparison of the Volumes of the Posterior Cervical Paravertebral Muscles Between LP and UCA Groups.
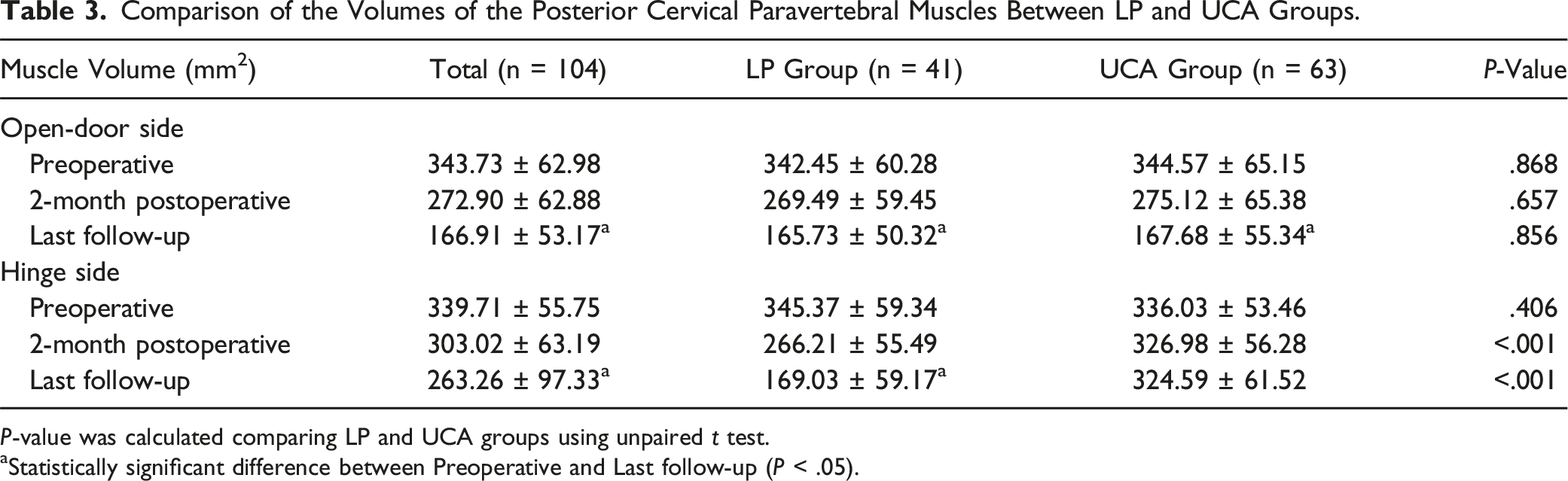
P-value was calculated comparing LP and UCA groups using unpaired t test.
aStatistically significant difference between Preoperative and Last follow-up (P < .05).
Complications
Post-operative Complications in Patients Underwent LP or UCA Surgery.
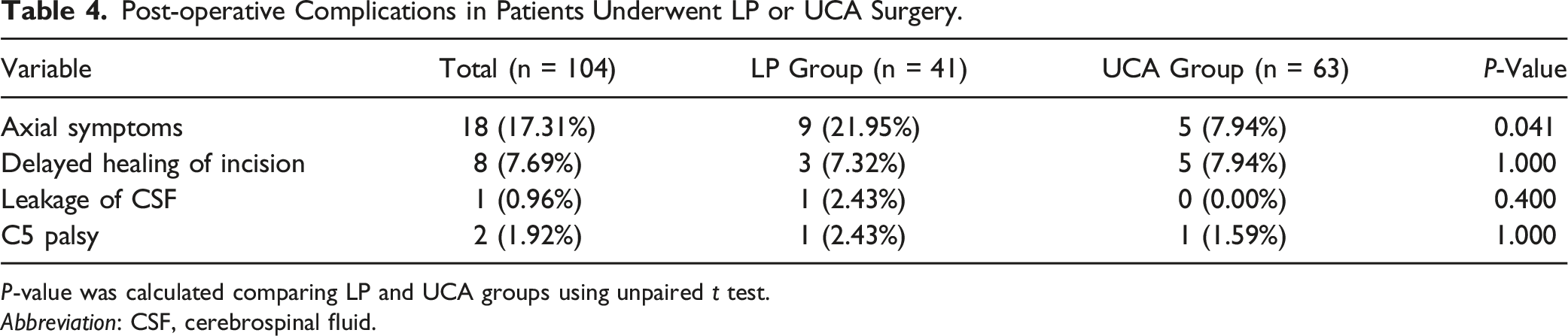
P-value was calculated comparing LP and UCA groups using unpaired t test.
Abbreviation: CSF, cerebrospinal fluid.
Discussion
Laminoplasty stands as a safe and effective surgical procedure for the treatment of DCM. It offers the advantage of spinal canal decompression without the need for fusion and is associated with fewer complications, such as postoperative kyphosis, anterior subluxation, and epidural scar formation, compared to laminectomy. 12 During traditional laminoplasty, bilateral paraspinal muscle detachment from the lamina and cutting-off the attached ligaments are often required, which result in posterior muscle-ligament complex (PMLC) impairment, leading to irreversible muscle atrophy and sagittal cervical spine imbalance. Consequently, axial symptom (AS), including neck pain and stiffness, can occur. 7 Hosono et al 13 reported that approximately 60% of patients experienced AS following laminoplasty. A comprehensive systematic review encompassing 26 studies and 1297 patients indicated that the incidence of AS varied between 5.2% and 61.5%. 14
The underlying mechanisms contributing to AS remain incompletely understood. Noteworthy, postoperative muscle atrophy has been demonstrated to be closely associated with worse clinical outcomes of laminoplasty. 8 Several modifications using less invasive and reconstructive techniques have been undertaken during posterior cervical surgery to reduce the damage of muscle-ligament complex. Yoshida et al 15 had performed expansive laminoplasty with reattachment of the spinous processes and extensor musculature in cases of cervical myelopathy, which called: laminoplasty with posterior muscle-ligament complex (PMLC) preservation. In this procedure, the posterior bony elements, such as the spinous processes, were not completely detached from the ligaments and musculature and were repositioned in the midline, to maintain normal cervical anatomic relationships. The follow-up evidence showed that Yoshida’s method is effective in reducing muscle atrophy and maintaining cervical lordosis, while failed to improving axial symptoms. 16 Shiraishi et al 17 proposed a new exposure technique focusing on the intermuscular plane between the right and left interspinalis muscles. Park et al and Feng Li et al18,19 performed a laminoplasty procedure using the inter-muscular plane between the semispinalis capitis and semispinalis cervicis to preserve the deep extensor muscles. The drawbacks of these intermuscular exposure technology were obvious: they are only suitable for short segment surgeries and time consuming.
Over the years, despite several studies used different modifications of LP procedures, these results are not effective as expected. 20 In order to reduce damage of the PMLC and reduce related complications. We proposed a new technique to perform cervical laminoplasty, which was termed unilateral exposure channel-assisted (UCA) laminoplasty. This technique was reported here to compare the effect of traditional laminoplasty and UCA laminoplasty on clinical efficacy, postoperative complication and paraspinal muscle atrophy. Our results showed evident paraspinal muscle atrophy on both open and hinge sides of traditional laminoplasty, which was not observed on the hinge sides of UCA laminoplasty. Consequently, we found more preservation of cervical sagittal balance and less axial symptom (AS) in patients from UCA group.
To preserve the integrity of the muscles and ligaments on the hinge side maximumly when performing UCA laminoplasty. There were some tips for our readers: First, the open side should be exposed using traditional methods. Second, a gutter was made with a 4 mm burr at each lamina. Third, an expandable channel was inserted through the paraspinal muscle at about 1.0 cm lateral to the spinous process. Then, a gutter was made with a 3 mm burr through this channel. Each lamina was treated by repeating this process. Finally, the lamina was elevated on the open side, plate and mini screws were inserted. This procedure showed several advantages: ① Preserved the integrity of the spinous process. ② No need to detach the muscles and ligaments of the hinge side. ③Reduced intraoperative bleeding and postoperative drainage. Noteworthy, our findings revealed a notable reduction in the incidence of AS and paraspinal muscle atrophy in the UCA group when compared with the traditional technology.
Our clinical observations identified delayed wound healing in 8 obese patients (BMI ≥30 kg/m2) exhibiting significant cervical subcutaneous adipose hypertrophy. Histopathological analysis indicated that the primary cause was electrocautery-induced thermal adipocyte necrosis, as evidenced by sterile chronic exudation (CRP 3.2 ± 1.1 mg/L, with negative cultures in 100% of cases). A conservative treatment regimen, consisting of twice-daily saline-moistened dressing changes and 830 nm infrared phototherapy (15 minutes per session, twice daily), resulted in complete epithelialization within 3 weeks postoperatively. To prevent this complication, we recommend strictly limiting the duration of electrocautery application within the subcutaneous adipose layer during surgery, as well as implementing a two-hour positional rotation regimen to reduce prolonged pressure on the wound interface post-surgery.
There are some limitations in our study. First, this was a retrospective study and the level of evidence was not high. Second, the number of patients was limited, and the follow-up period was not very long. Third, the participants were not fully blind due to the explicit nature of the intervention. Finally, single-center study may reduce the reliability of conclusion. Thus, multicentre randomised controlled trial with long-term follow-up and assessments such as return to work and daily activity levels (e.g., SF-36 or EQ-5D) is needed to further demonstrated the clinical significance of unilateral exposure channel-assisted laminoplasty.
Conclusions
Our unilateral exposure channel-assisted laminoplasty is effective for treating DCM with good recovery of neurological function. Furthermore, it shows the superiority in maintaining cervical sagittal alignment, minimizing intraoperative invasion, speeding up postoperative rehabilitation, reducing the occurrence of paravertebral muscle atrophy and the incidence of postoperative axial symptoms compared with traditional open-door laminoplasty.
Footnotes
Author Contributions
Conception and design: H.Z., H.C., W.Y, X.S. Acquisition of data: R.W., L.W., Analysis and interpretation of data: L.W., H.W. Drafting the article: X.S., H.Z. Critically revising the article: H.C., W.Y, X.S. Approved and reviewed the final version of manuscript: all authors. Statistical analysis: X.W., Y.L. Study supervision: H.C., W.Y., X.S.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by grants from National Natural Science Foundation of China (82072471), Shanghai Natural Science Foundation(23ZR1478000).