
Abstract
Study Design
Retrospective study.
Objectives
To analyze lamina hinge fusion failure after plate-only open-door laminoplasty.
Methods
Thirty-one patients who underwent plate-only open-door laminoplasty (110 levels) for cervical myelopathy and who had serial computed tomography (CT) scans at 6 and 12 months were analyzed. Risk factors for fusion failure at 12 months were analyzed, including age, sex, smoking, presence of diabetes mellitus and ossification of posterior longitudinal ligament, bone mineral density (T-score), preoperative cervical curvature, operated levels, presence of a ventral cortical bony continuity, and reflection angle of the lamina hinge. Clinical outcomes were assessed with neck pain score using visual analog scale, neck disability index, and Japanese Orthopedic Association score.
Results
Hinge fusion occurred in 84% (26/31) of patients at 12 months. A significant risk factor for fusion failure was the absence of a ventral cortical bony continuity at 6 months (p < 0.01; 100 versus 48%). No lamina with ventral cortical bony continuity at 6 months showed depression at 12 months, but two lamina without continuity showed depression of 2.5 and 2.1 mm, respectively, at 12 months. Clinical outcomes were not different between patients with and without hinge fusion.
Conclusion
Absence of a ventral cortical bony continuity at 6 months is a risk factor for fusion failure at 12 months. However, bicortically defective laminae usually heal with minimal displacement, although it may take longer than 12 months.
Introduction
Since Dr. Hirabayashi introduced open-door laminoplasty in 1977, 1 it has become a popular method for spinal cord decompression in patients with cervical spondylotic myelopathy or ossified posterior longitudinal ligament (OPLL). The procedure is associated with satisfactory clinical outcomes. 1 , 2 , 3 To maintain the widened spinal canal, opened and reflected laminae were originally anchored with stay sutures, and titanium plates and screws were recently introduced for open-door laminoplasty. 4 , 5 The plate-only open-door laminoplasty appears to be a simple alternative surgical method. 6 The risk of reclosure of the lamina after plate-only open-door laminoplasty was reported to be minimal, and the plate seemed adequately strong to keep the lamina open until bony fusion occurred at the lamina hinge, usually in 6 months. 5 , 6 , 7 , 8 However, the fusion rate was not 100%, and discontinuity of cortical bone at the lamina hinge was infrequently observed at 6 months. The fate and clinical significance of the unfused lamina at 6 months has not been addressed after plate-only open-door laminoplasty. The purposes of this study were to investigate hinge fusion rate and to determine risk factors for hinge fusion failure and its clinical significance.
Materials and Methods
Between September 2009 and September 2011, 42 consecutive patients who received plate-only open-door laminoplasty for cervical spondylotic myelopathy or OPLL at our institution were retrospectively reviewed after approval of Institutional Review Board. Of them, 31 (74%) patients (23 men, 8 women; mean age, 63.4 ± 9.6 years; range, 41 to 78) who underwent serial computed tomography (CT) scan at 6 and 12 months and were followed for at least 12 months were included in this study. Medical records and radiographic images were reviewed. The mean follow-up period was 17.2 ± 6.6 months (range, 12 to 28).
Surgical Procedure
The surgical procedure was performed as described elsewhere. 9 A midline incision was performed in the prone position. The spinous processes and laminae were exposed, and the joint capsules of the facets were preserved. Using a 3-mm high-speed cutting bur, bony gutters were made on the open side of the laminae. Then, the thin ventral cortex and ligamentum flavum were removed with a 1-mm Kerrison rongeur. Symmetric gutters were made on the contralateral laminae (hinge side) with a cutting bur while preserving the ventral bony cortex. The opening side was decided based on the laterality of the symptoms and the severity of spinal cord compression on radiographic images. After cutting the upper and lower supraspinous and interspinous ligaments at the corresponding levels, the laminae on the open side were gently elevated off the spinal cord. The elevated lamina was fixed with a titanium miniplate (double-bended 10- or 12-mm plate) and screws (6 or 8 mm in length; Arch Laminoplasty System, Synthes, West Chester, Pennsylvania, United States), thus bridging the elevated lamina and lateral mass on the open side. No bone graft was interposed in the laminar gap. Because the ventral lamina of the hinge side was not identifiable during the operation, we regarded the hinge as fractured if the lamina moved freely or if resistance of the hinge was different from the other laminae during the lamina reflecting procedure. With those criteria, there were no identifiable lamina hinge fractures in the 31 patients included in this study.
Clinical Assessment
All patients presented myelopathic symptoms signs, such as motor weakness, hand clumsiness, gait disturbance, and sensory abnormalities. Neck pain score using visual analog scale (VAS-neck, 10 points), neck disability index (NDI, 50 points), and Japanese Orthopedic Association (JOA, 17 points) scores were used for clinical assessment preoperatively, 6 and 12 months postoperatively, and yearly thereafter. The JOA score recovery rate, proposed by Hirabayashi et al, 2 was calculated as follows: recovery rate (%) = 100 × (postoperative JOA score – preoperative JOA score)/(17–preoperative JOA score).
Radiologic evaluation
The patients were scheduled for CT scan and plain radiographs at 6 and 12 months after the operation. If solid bony fusion was achieved in all laminae at 6 months, no further CT scan was taken. Axial CT scans at 6 and 12 months after surgery were independently reviewed for fusion, plate dislodgement, and lamina depression by one neurosurgeon. Fusion status was evaluated by the criteria proposed by Rhee et al in a previous study. 6 Fusion was defined as bony continuity at both ventral and dorsal lamina at the hinge side with either cortical bone or callus formation (Fig. 1). Fusion in all operated lamina was regarded as fusion for each patient. Lamina depression was defined as a lamina shift of more than 1 mm toward the spinal canal (Fig. 2). The cervical curvature was measured between C2 and C7 by a tangential method. 7 , 10 , 11
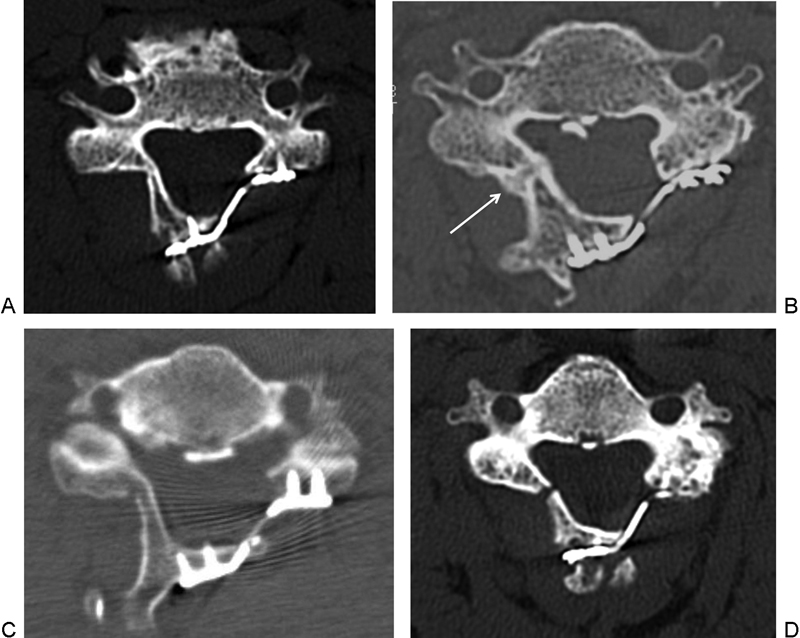
Computed tomography showing fusion and nonfusion of the hinge. Fusion was defined as (A) cortical bony continuity at both ventral and dorsal lamina or (B) callus formation and bony bridge (arrow) at both ventral and dorsal lamina. Only ventral cortical bony continuity (C) or no bony continuity (D) was defined as nonfusion.

Depression of the lamina. This lamina showed ventral cortical bony discontinuity at 6 months. It is fused at 12 months and is depressed 2.1 mm. Note that both dorsal and ventral cortical linings are disrupted (arrow).
Statistical Analysis
Risk factors for fusion failure at 12 months were analyzed, including age, sex, presence of diabetes mellitus, smoking history, presence of OPLL, bone mineral density (T-score), preoperative cervical curvature, number of laminoplasty level, and presence of a ventral cortical bony continuity at the hinge-side lamina by the 6-month CT scan. Factors affecting the cortical bony discontinuity at the 6-month CT scan were analyzed, and VAS-neck, NDI, and JOA recovery rates were compared between the patients on the basis of hinge fusion status at postoperative 6 and 12 months. SPSS statistical software package version 21.0 for Windows (IBM Corporation, New York, New York, United States) was used for statistical analysis. Student t test and chi-square test were used for continuous and binary values. For nonparametric tests, Mann-Whitney U test and Fischer exact test were used. Logistic regression analysis was used for multivariate analysis. A two-sided p value of <0.05 was considered significant.
Results
A total of 31 patients with 110 laminae were evaluated. Two patients had diabetes mellitus, 12 patients were smokers, and 18 patients were diagnosed with OPLL (Table 1). The mean preoperative cervical curvature was 9.9 ± 5.0 degrees and all patients had lordotic cervical curvatures. The mean number of laminoplasties for each patient was 3.6 ± 0.9 levels (range, 2 to 5).
Comparison of patient characteristics between hinge fusion group and nonfusion group at 12 months
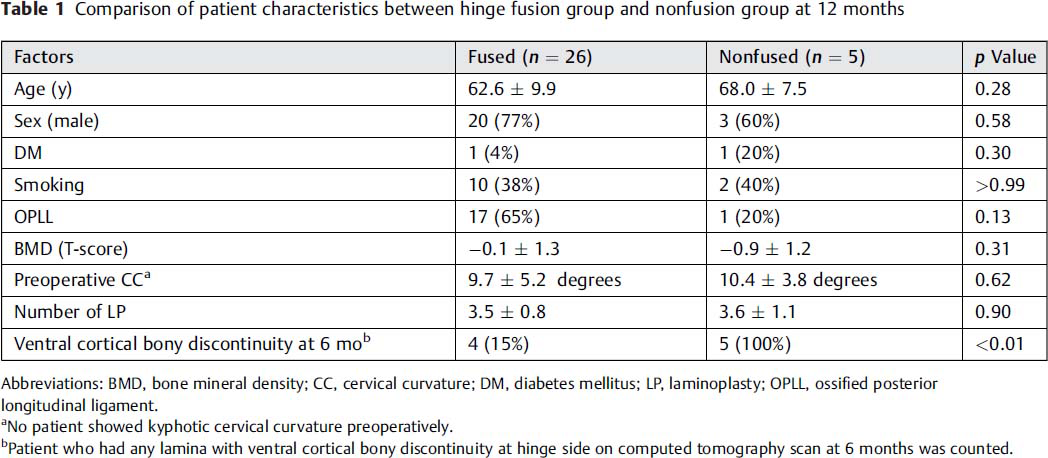
Abbreviations: BMD, bone mineral density; CC, cervical curvature; DM, diabetes mellitus; LP, laminoplasty; OPLL, ossified posterior longitudinal ligament.
No patient showed kyphotic cervical curvature preoperatively.
Patient who had any lamina with ventral cortical bony discontinuity at hinge side on computed tomography scan at 6 months was counted.
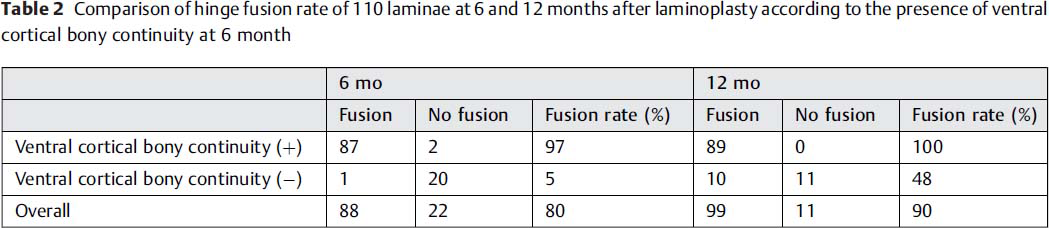
Fusion at the hinge-side lamina at 12 months was observed in 26/31 (84%) patients. The absence of ventral cortical bony continuity on the hinge-side lamina at 6 months was the only significant risk factor for fusion failure at 12 months (Table 1, p < 0.01). Among 110 laminae, 99 showed fusion (90%) at 12 months. Of those, 89 laminae had a ventral cortical bony continuity at 6 months, but 21 laminae did not. All laminae with a ventral cortical bony continuity at 6 months showed fusion at 12 months, and 10 of 21 laminae without ventral cortical bony continuity showed fusion at 12 months (48%; Table 2). Related factors affecting the ventral cortical bony continuity of the hinge at 6 months were age (p < 0.01), the presence of OPLL (p = 0.01), and the reflection angle of lamina (p = 0.04; Table 3).
Comparison of hinge fusion rate of 110 laminae at 6 and 12 months after laminoplasty according to the presence of ventral cortical bony continuity at 6 month
Risk factor analysis of the absence of ventral cortical bony continuity at 6 months in 110 operated laminae
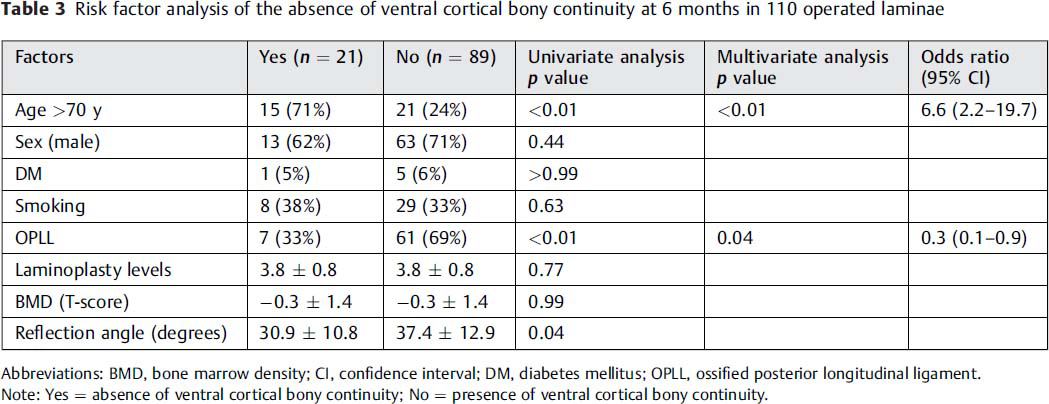
Abbreviations: BMD, bone marrow density; CI, confidence interval; DM, diabetes mellitus; OPLL, ossified posterior longitudinal ligament.
Note: Yes = absence of ventral cortical bony continuity; No = presence of ventral cortical bony continuity.
The hinge fusion status did not affect the clinical outcomes (Table 4). VAS-neck (2.4 ± 1.7 versus 3.3 ± 2.0, p = 0.29 at 6 months; 2.1 ± 2.0 versus 1.8 ± 2.1, p = 0.8 at 12 months) and NDI (13.1 ± 8.2 versus 15.3 ± 13.6, p = 0.61 at 6 months; 10.6 ± 7.1 versus 16.4 ± 15.9, p = 0.44 at 12 months) scores were not statistically different between the hinge fusion group and the fusion failure group. Median recovery rate of JOA at 12 months postoperatively was higher in the hinge fusion group (75 ± 38.9% versus 16.7 ± 33.2%, p = 0.10), but the difference was not statistically significant.
Clinical outcome comparison according to the hinge fusion status at postoperative 6 and 12 months
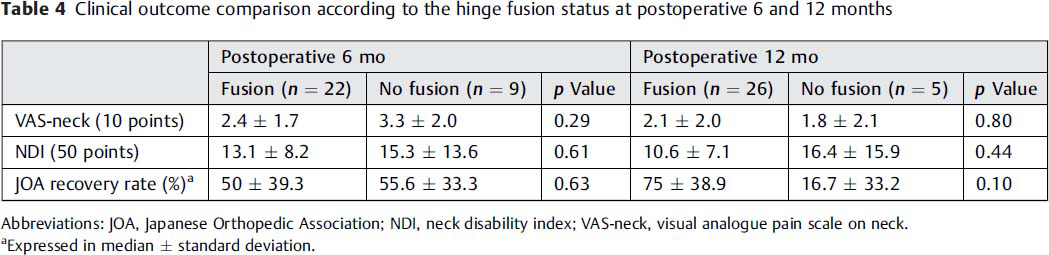
Abbreviations: JOA, Japanese Orthopedic Association; NDI, neck disability index; VAS-neck, visual analogue pain scale on neck.
Expressed in median ± standard deviation.
Consecutive hinge nonfusion was observed in 7/31 (22%) patients at 6 months and 4/31 (12%) patients at 12 months. There was no mechanical failure such as plate dislodgement, fracture, or pullout of screws during the follow-up period. No laminae with ventral cortical bony continuity at 6 months showed depression at 12 months, but 2 of 21 laminae without a ventral cortical bony continuity at 6 months showed depression of 2.5 and 2.1 mm, respectively, at 6 months with no progression at 12 months.
Illustrative Case
A 74-year-old man visited our clinic, complaining of weakness of both legs for 2 months. Neurologic examination revealed grade IV motor weakness in both extremities. His cervical magnetic resonance images showed spinal canal stenosis with cord signal change, and segmental type OPLL was observed at the C5 and C6 vertebral body levels by CT scan (Fig. 3A, B). Open-door laminoplasty from C4 to C6 was performed. Immediately after the operation, the spinal canal was widened (Fig. 3C, D), and gradually motor power of both lower extremities improved. On postoperative 6-month CT scan, the hinge of the C6 lamina was fused; two other laminae (C4, 5) were not fused and lacked a ventral cortical bony continuity (Fig. 3E–G). Postoperative 12-month CT scan revealed fusion of the C4 lamina hinge with callous bone formation, but the C5 lamina was still not fused without depression (Fig. 3H–J).
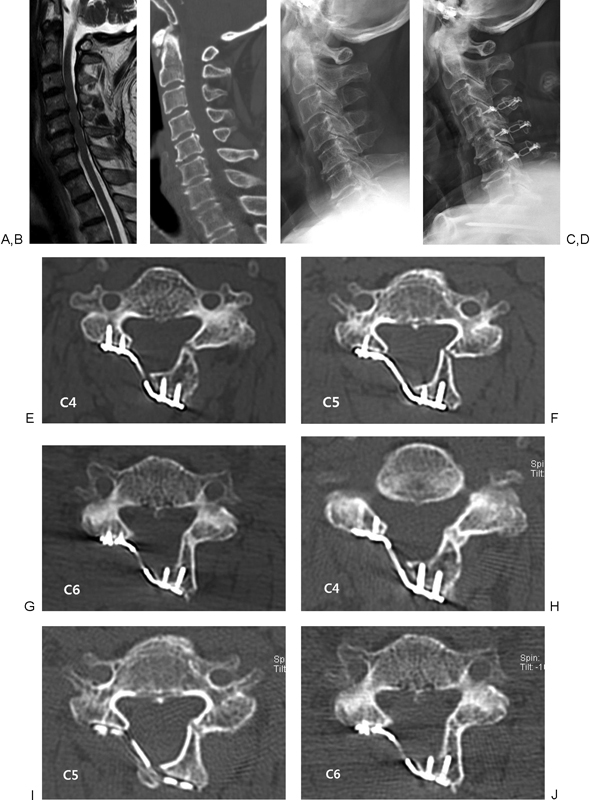
A 74-year old man complaining of weakness in both lower legs visited our clinic. (A) Cervical magnetic resonance imaging shows spinal canal stenosis with cord signal change at C4–6 level. (B) The segmental type of ossified posterior longitudinal ligament was observed at level C5–6 vertebral bodies. (C, D) Compared with preoperative simple lateral X-ray image, the anterior-posterior diameter of spinal canal was increased postoperatively. (E, F, G) At 6-month computed tomography (CT) scan, the C6 lamina was fused but the C4–5 laminae were not fused, without both dorsal and ventral cortical bony continuity at the hinges. (H, I, J) A 12-month CT scan showed fused C4 hinge-side lamina with definitely visible callous bone formation. The hinge of C5 lamina showed callous bone formation, but bony bridge was not clear and this lamina was regarded as nonfused. No interval change of the C6 lamina was observed.
Discussion
Overview
The main purpose of the present study was to present the fate and clinical significance of the potentially unstable unfused lamina at 6 months. In the present study, fusion at the lamina hinge was observed in 26/31 (84%) of patients at 12 months. For 110 laminae, the overall fusion rate was 80 and 90% at 6 and 12 months, respectively. This result is similar to previously reported fusion rates (77% at 6 months and 93% at 12 months). 6 We found that the hinge fusion rate at 12 months was significantly higher for patients with ventral cortical bony continuity at 6 months than in patients without it (100 versus 15%, Table 2). In addition, a low fusion rate of individual lamina was observed for laminae without ventral cortical bony continuity at 6 months (100 versus 48%). It appears that the absence of a ventral cortical bony continuity at 6 months is an independent risk factor for fusion failure at 12 months. The clinical parameters (JOA, NDI, and neck pain) were not associated with the fusion status.
Risk Factors of Ventral Cortical Bony Discontinuity
Older age and the absence of OPLL were shown to affect the occurrence of this bony discontinuity. As age advances, bone mass and its strength usually decline, 12 and the likelihood of fracture at the ventral cortex rises. A study reported increased bone mineral density in patients with OPLL compared with a normal control group, and presence of OPLL may protect ventral cortical bone discontinuity. 13 Another factor is the surgical technique especially during drilling and reflection of the lamina. In forming a gutter at the lamina hinge, drilling should not be too deep or shallow. The former would create a direct ventral bony defect, whereas the latter would result in a forcible fracture at the lamina hinge. Only the dorsal cortical and cancellous bone of the lamina is drilled, leaving the ventral cortical bone intact. Then, the lamina is gently lifted up to create a greenstick fracture at the hinge. After gentle elevation of the lamina, the lamina requires fixation with a plate of optimal length. A longer plate may lead to intolerable reflection at the lamina hinge. Therefore, great care should be taken during the surgical procedure in the formation of the lamina hinge gutter to avoid ventral cortical bone disruption, especially in older patients and those patients without OPLL. One contradictory finding in the present study was the higher lamina reflection angle in laminae with ventral cortical bony continuity. It is generally believed that greater lamina reflection would increase the bony fracture risk, but further study with a large number of patients is needed.
Clinical Significance
A low fusion rate of individual lamina was observed for laminae without ventral cortical bony continuity (fusion rate 97 versus 5% at 6 months, and 100 versus 48% at 12 months), but displacement occurred only in two laminae ∼2 mm during 12 months of follow-up. Because CT scan immediately after surgery was not available, ventral cortical bony discontinuity at 6 months may imply both fracture during operation and bone resorption during 6 months. Although fusion rate of bicortically defect lamina at 6 months was less than 50% at 12 months, it did not lead to poor outcome.
There might be several factors contributing to the stability of “potentially unstable lamina” even if it fails to fuse. First, the ligamentum flavum connecting the elevated lamina to the host and cranial/caudal lamina adds considerable strength for the resistance. Second, stickiness of the hinge might be formed by callus or soft tissue. Those supports may provide enough strength to keep the reflected hinge in place irrespective of fusion failure. In addition, it seemed that titanium plates may add stability. In this study, two or more consecutive laminae hinge failures were observed in seven and four patients at postoperative 6 and 12 months, respectively. But only two minimal displacements of hinges were identified. This was supported by the literature reporting a rare incidence of instrument failure or lamina reclosure in open-door laminoplasty using titanium plate. 6 , 14
Although the clinical significance of hinge fusion failure is unclear, some suggestions could be made. If the ventral hinge failure occurred during the postoperative 6-month period, it would likely be stable and would be expected to achieve fusion with callus formation. Because the incidence of hinge fracture during the surgery was not available with the present study, it would be misleading to state that the hinge failure during the surgery is not a problem at all. However, considering the fact that most spring-back lamina closures after open-door laminoplasty occurred within 6 months after the operation, 7 , 8 it seems that minimal fracture or bone resorption, causing ventral cortical bone discontinuity within 6 months, does not lead to poor clinical outcome. Further study is required to verify this matter.
Limitations
There are several limitations in this study. First, it is a retrospective study with a small number of patients, which may lead to statistical errors. There may be another risk factor for nonfusion in addition to a ventral cortical bony discontinuity. Second, we do not know exactly when the ventral cortical bony continuity was disrupted. The clinical outcome of lamina fracture versus bony resorption may be different, although imaging finding at 6 months may be similar. Immediately postoperative CT might be helpful to clarify the cause and clinical significance. However, considering radiation hazard, obtaining additional CT scans is unethical, and we need to find another way to differentiate them. Third, because only postoperative 12-month follow-up CT images are available in this study, we do not know the eventual fusion rate of unfused hinge at postoperative 12 months. This needs to be verified with a longer follow-up study.
Conclusion
The hinge fusion rate after plate-only open-door laminoplasty was 84% at 12 months. The absence of a ventral cortical bony continuity at the lamina hinge at 6 months was a strong risk factor for fusion failure at 12 months. However, bicortically defected laminae usually heal with minimal displacement, although it may take longer than 12 months.
Disclosures
Sungjoon Lee, none
Chun Kee Chung, none
Chi Heon Kim, none
Footnotes
Acknowledgments
This work was supported by Grant No. 03–2013–0330 from the Seoul National University Hospital Research Fund.
Notes
This study was approved by the Institutional Review Board of the Clinical Research Institute at Seoul National University Hospital (IRB No. H-1307-085-505).