
Abstract
Study design
Randomized controlled trial.
Objectives
In this study, we hypothesize administering fixed-dose intravenous steroid (Methylprednisolone) intraoperatively would reduce neuroinflammation and enhance functional and radiological outcomes in decompressive surgeries for DCM. Primary objectives were to assess effect of intraoperative MP on modified Japanese Orthopedic Association (mJOA) score, Nurick grade, and MRI signal changes.
Methods
This prospective triple-blinded randomized controlled trial included 65 patients allocated into MP (n = 33) and control (n = 32) groups. MP (dose-1g) was administered intraoperatively at the beginning of decompression. Clinical outcome measures included mJOA score, Nurick grading, mJOA recovery rate (mJOA RR), Nurick recovery rate (NRR), and complication rates in both groups at 1-, 3-and 24-month follow-up. Radiological outcome was assessed by analyzing regression of T2W and T1W SI changes on MRI scans as per Chen’s grading at 24-months follow-up.
Results
MP group exhibited greater improvement in mJOA scores at 24-months (mean improvement: +6.69 vs +6.42; difference: +0.27, 95% CI: −0.37 to +0.91) but was statistically insignificant (P = .107). Similarly, mJOA-RR showed a moderate effect size of 0.42 (95% CI: 0.04 to 0.80) and 0.37 (95% CI: −0.01 to 0.75) at 1-and 3-months follow-up respectively. NRR improvements were observed, with effect sizes of 0.40 (95% CI: 0.02 to 0.78) and 0.49 (95% CI: 0.11 to 0.87) at 1- and 3-months respectively, but not statistically significant (P = .28). At 24-months, MP group had significantly better MRI outcome (Chen grading: mean change +1.15 vs +0.83; effect size: −0.71, 95% CI: −1.09 to −0.33; P = .038).Complication rates were comparable between both groups, emphasizing safety of MP administration.
Conclusion
Although null hypothesis was not proven, intraoperative MP administration in DCM surgery demonstrated safety and suggested potential neuroprotective benefits to enhance clinical recovery and reduce spinal cord signal changes. However, further large-scale, multicentric studies are needed to validate these findings and optimize its dose.
Keywords
Introduction
Degenerative Cervical Myelopathy (DCM) is the leading cause of chronic spinal cord injury globally, which is a slowly progressing condition marked by degenerative or congenital changes in the cervical spine.1,2 This condition, more common with aging, results in chronic spinal cord compression due to increased immune cell recruitment and inflammatory cytokine production in the spinal cord.3,4
Despite intermittent symptom exacerbations, 5 myelopathic symptoms in DCM are largely irreversible, necessitating timely intervention. 6 Surgical decompression is the primary treatment,7-10 yet complications such as worsening myelopathy and delayed C5 palsy and a subset of non-responsive patients highlight the need for adjunctive approaches. Surgical procedures trigger a systemic proinflammatory response, 11 prompting our investigation into the potential benefits of methylprednisolone (MP) administration as an adjunct to cervical decompression and reducing surgical trauma.12,13
Glucocorticoids have been shown to reduce inflammation by inhibiting the expression of collagenase and proinflammatory cytokines.13,14 We proposed a hypothesis that MP administration during cervical decompression may reduce neuroinflammation and therefore serve to decrease postoperative neurological decline and promote better neural recovery. MP is a neuroprotective and anti-inflammatory medication that is frequently used in posttraumatic spinal cord injury (SCI).15,16 However, its utilization for SCI has been controversial due to mixed findings. 17 Furthermore, per-operative steroids can reduce pain and length of hospital stay in patients operated for cervical and lumbar radiculopathy due to degenerative etiopathogies.18,19 The study’s purpose is to explore the possibility of repurposing MP for neuroprotection in CSM in addition to surgical decompression.
This randomized control trial aims to investigate the effects of intra-operative administration of MP on DCM patients undergoing cervical decompression surgery, observe its side effects, and compare the long-term outcomes of patients receiving MP compared to a control group. Specifically, we hypothesize that intraoperative MP will lead to significant improvements in functional and MRI changes recovery as compared to control group. Secondary objectives include determining the correlation between mJOA score, Nurick grade, recovery rates, and MRI Chen grading before and after surgery. This study aims to contribute novel insights into the efficacy and safety of MP as an adjunctive neuroprotective treatment in CSM, potentially reshaping therapeutic approaches in this prevalent chronic spinal cord condition.
Materials and Methods
Study Design
In this prospective triple-blinded Randomised Controlled Trial (RCT), the patients, surgeons, and outcome assessor were all blinded to the intervention. The Institutional Ethics Committee gave its clearance (Reference number KMC/2020/002) and the study complied with ethical standards and the Declaration of Helsinki. All the study participants provided written informed consent.
Participants
The patients were recruited over 24 months, from February 2020 to January 2022. In this RCT, 65 patients receiving elective surgery for DCM were split into 2 groups at random: the Methylprednisolone (MP) group and the Control group (Figure 1). All patients diagnosed with DCM and older than 18 years of age were included in this study. Pregnancy, post-traumatic cervical myelopathy, prolonged preoperative steroid use, allergy to dexamethasone, MP, or related steroid drugs, uncontrolled diabetes mellitus, chronic kidney disease, intraoperative MP administered at the surgeon’s request, patients undergoing combined anterior-posterior surgery, any prior cervical spine surgery, neurological conditions such as Parkinson’s disease, poliomyelitis, cerebral palsy, multiple sclerosis, concurrent infection, and tandem stenosis were among the exclusion criteria. All patients were prospectively followed up for a minimum of 2-year duration. CONSORT (Consolidated Standards of Reporting Trials) diagram showing the flow of study participants through various stages of this RCT.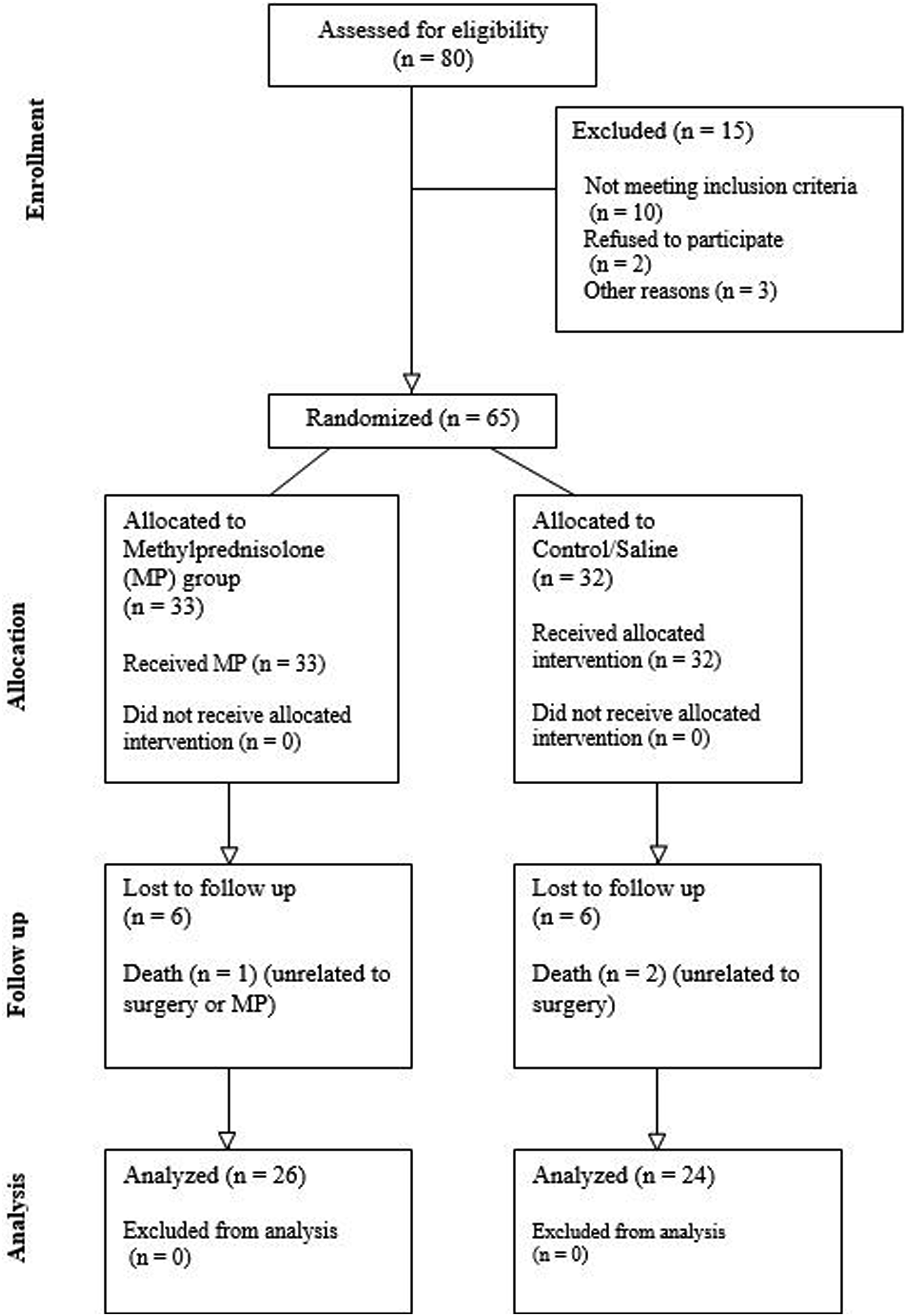
Randomization
An allocation ratio of 1:1 was used in a computer-generated randomized table. An anesthesiologist, not involved in sampling or collecting data, carried out the allotment of patients in the groups and intraoperative administration of MP or Normal saline. The drug administration remained hidden from the operating surgeon.
Intervention
The anesthesiologist gave the MP group 1g of methylprednisolone just before the commencement of spinal decompression, while the Control group received normal saline. MP was given right prior to the commencement of laminectomy in cervical laminectomy surgery, soon before commencing laminoplasty, and just before starting discectomy in anterior cervical decompression and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF).
Data Collection and Recording of Outcomes Measures
Patient demographics, presenting symptoms, radiological results, surgical details, and follow-up findings were all updated regularly in a prospective database. Clinical results were evaluated preoperatively and at 1, 3, 12, and 24 months after surgery using a modified Japanese Orthopaedic Association (mJOA) score and Nurick grading. Preoperative and 2-year follow-up MRI scans were included in the radiological evaluations.
Clinical and Functional Outcome Assessment
Clinical recovery was assessed by mJOA recovery rate (mJORR) and Nurick recovery rate (NRR) by using the following formula:


Radiological Evaluation
MRI was performed preoperatively and postoperatively at 2-year follow-up to diagnose pathological changes in T2WI and T1WI Sagittal and axial images (5 mm thickness slice). Intramedullary cord signal intensity (SI) changes were evaluated using Chen grading (Figure 2).
20
Chen et al
20
in 2001 proposed a qualitative classification of T2WI SI based on intensity and border pattern. Type 0 had no intramedullary signal changes on T2WI, Type 1 had a faint and fuzzy border of high SI, and Type 2 had an intense, sharp and well-defined border of high SI. The presence or absence of T1 hypointensity was also noted. Chen’s grading, which has a strong correlation with clinical recovery, has been widely validated in previous studies.20,38 Chen’s grading was performed by 3 independent consultants—an orthopedic spine surgeon, a neurosurgeon, and a neuroradiologist who were blinded to the patient groups. Intra-class correlation (ICC), which provided significant consistency in grading across all observers with an ICC score of 0.87, showed good agreement among the raters and evaluated the inter-rater reliability. MRI signal intensity changes: (A, B, C) Chen grading of T2WI signal changes; (D) Hypointensity on T1WI MRI.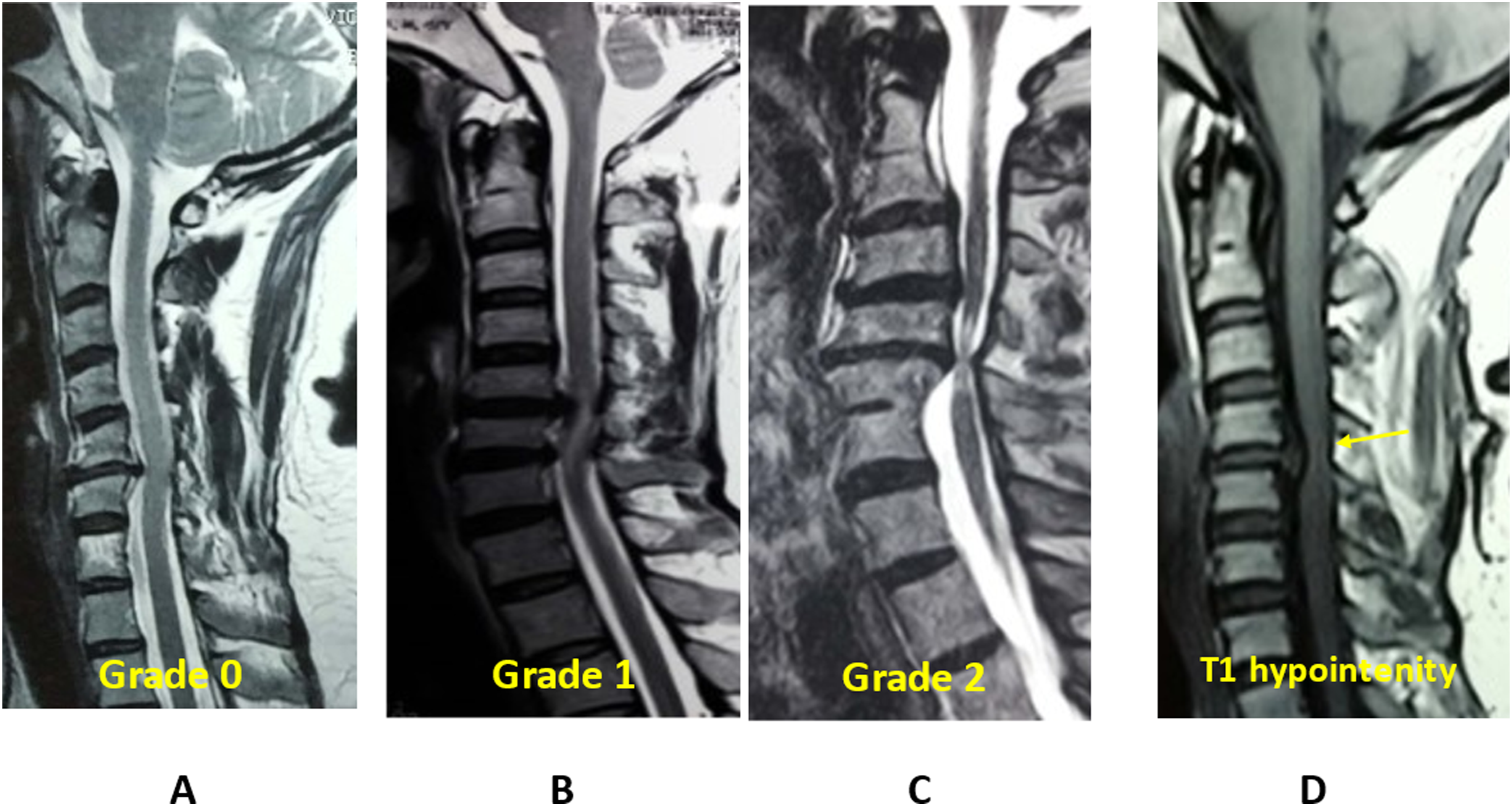
Statistical Analysis
IBM SPSS Statistics (Version 25.0) was used to evaluate the data. The mean and standard deviation values of quantitative data were presented. The normality of data was assessed by the Shapiro-Wilk test, and homogeneity of variances was evaluated by Levene’s test. For variable comparisons with normally distributed data, the independent 2-sample t-test was utilized, and correlation analyses were carried out using Spearman’s rank correlation coefficient, with a P-value of less than .05 designated as the statistical significance level. A non-parametric test (Mann-Whitney U test), was applied where normality assumption was violated and was used for comparing various domains of mJOA score amongst both groups.
Effect sizes (Cohen’s d) were calculated for each primary and secondary outcome to quantify the magnitude of differences between both groups. 95% confidence intervals (CI) were calculated for the precision and clinical relevance of these estimates. Emphasis was also placed on interpreting the effect sizes and their direction rather than solely relying on the P-value.
The sample size calculation was done to detect clinically meaningful differences in outcomes between both groups, assuming effect size of 0.35 with 80% power and a two-sided alpha of 0.05. The power analysis using an alpha = 0.05, a beta = 0.2, and a threshold clinically relevant difference of 35% in the primary outcome scores estimated that 24 patients were needed for each group.
Results
Demographics and Patient Characteristics
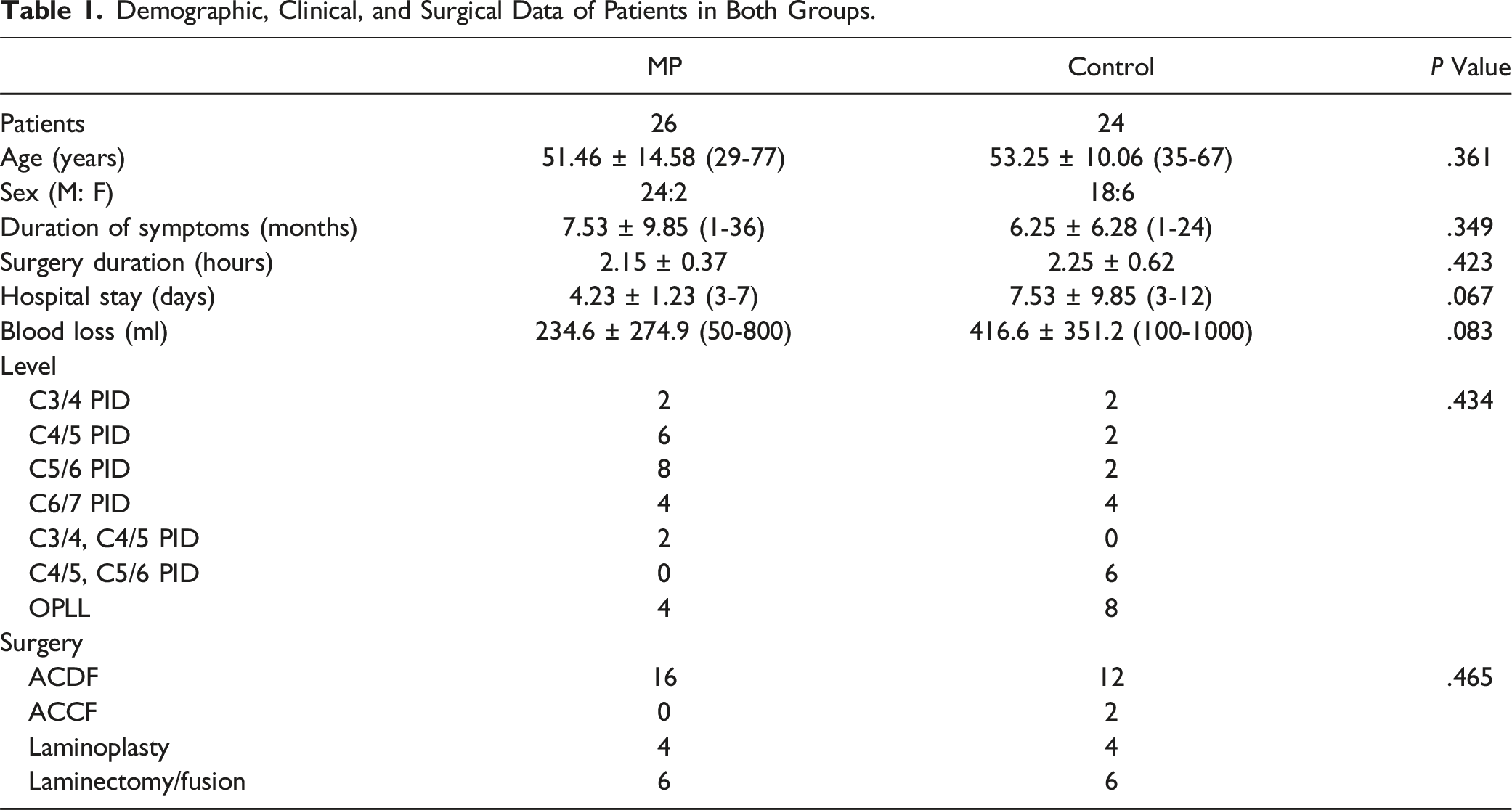
Demographic, Clinical, and Surgical Data of Patients in Both Groups.
Baseline Status
The study analyzed the preoperative functional status and radiological status of patients in both groups. Both groups had similar preoperative clinical and functional status, with no significant differences in mJOA score and Nurick grade (mJOA score MP vs Control, mean 9 ± 2 vs 8.166 ± 2.44, P = .181 and Nurick grade mean 3.46 ± 0.77 vs 3.66 ± 0.77, P = .258).
The study analyzed preoperative MRI results for Types 1 and 2 cord ISI in patients with a variety of conditions. In the MP group, Type 1 ISI was observed in 10/26 patients and Type 2 ISI in 16/26 patients, while in the control group, it was found in 4/24 and 20/24 patients, respectively. There was no significant difference in Chen grading on preoperative MRI (1.61 ± 0.50 vs 1.83 ± 0.38, P = .119), indicating comparable T2W signal intensity changes in both groups. T1 hypointensity was not observed in any of the groups.
Clinical and Functional Outcome
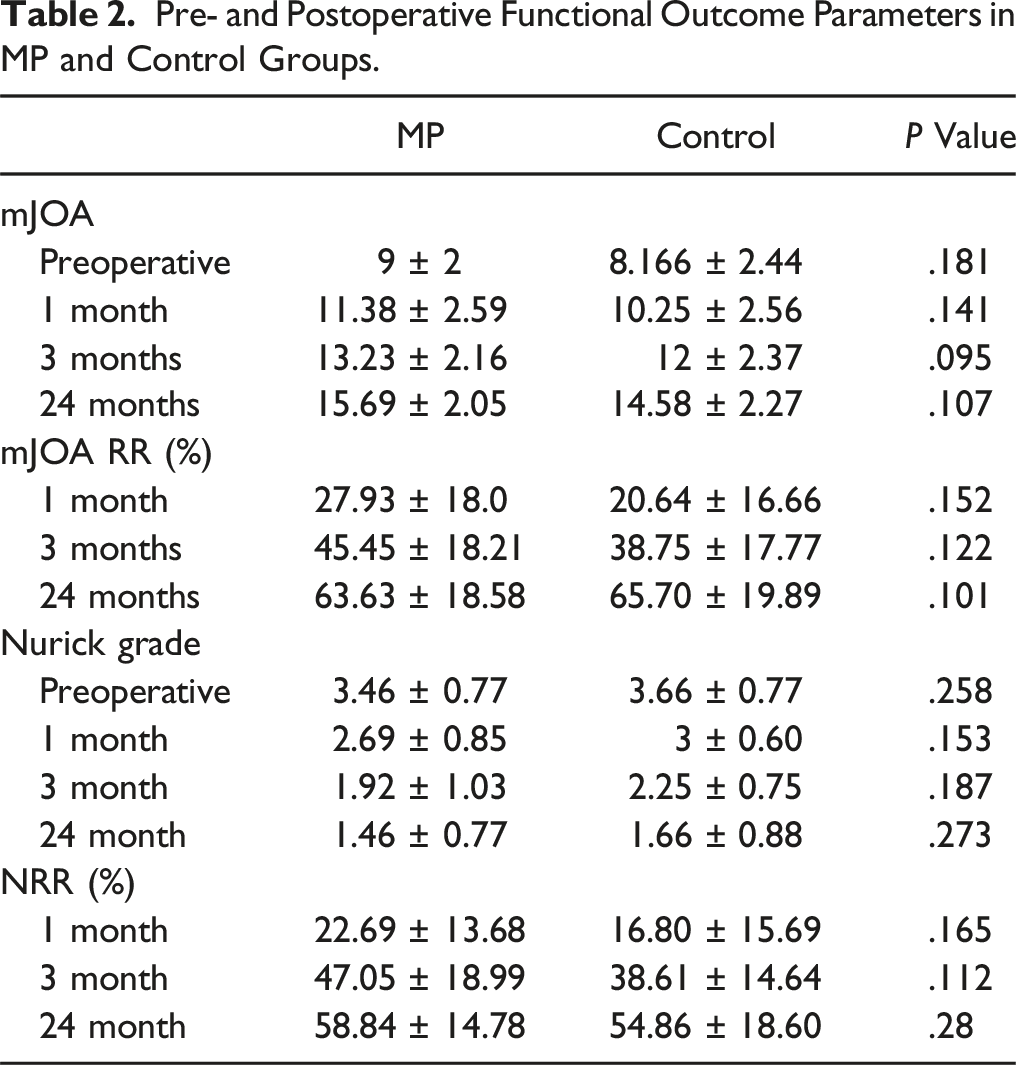
Pre- and Postoperative Functional Outcome Parameters in MP and Control Groups.
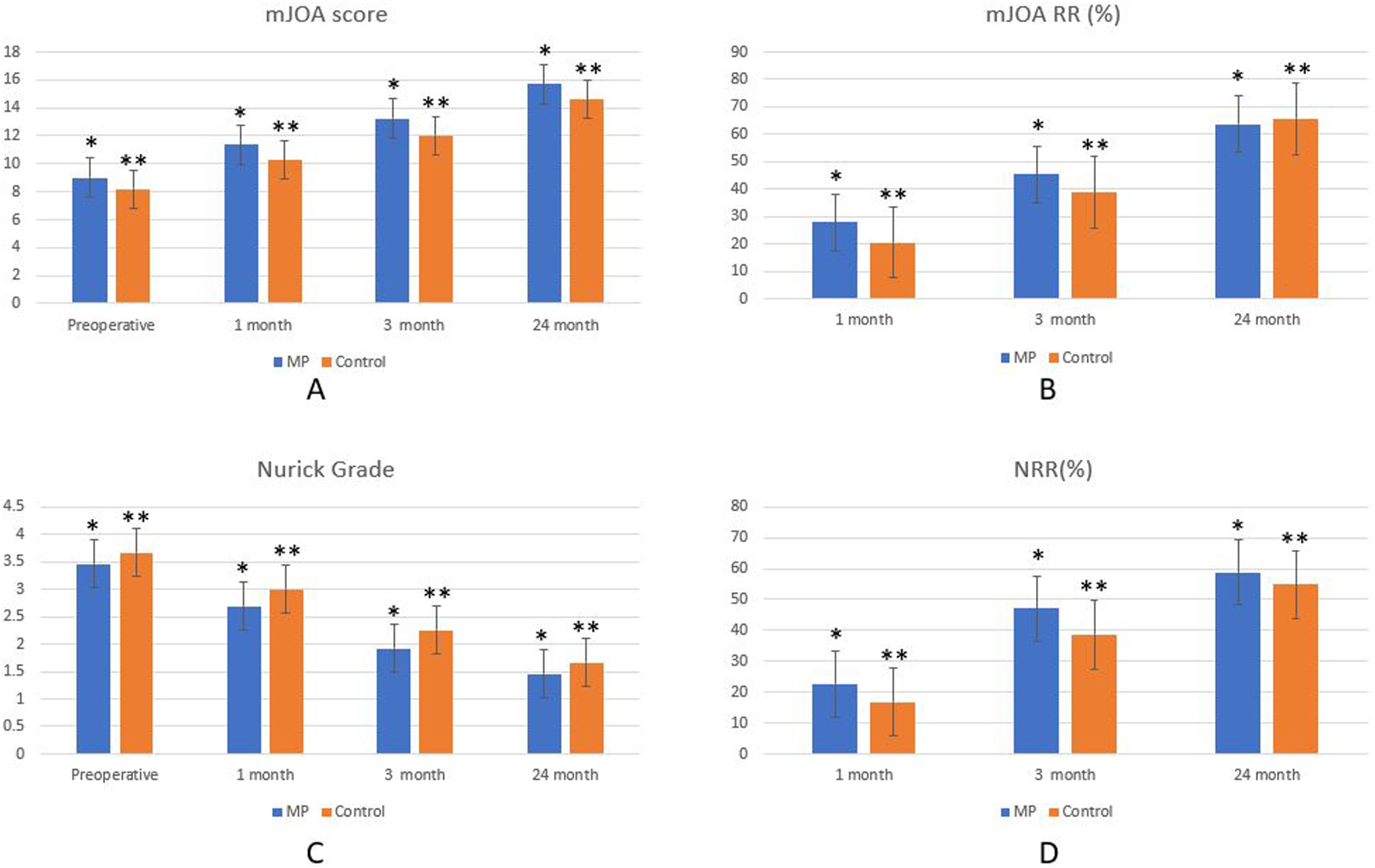
(A) mJOA score comparison between MP and control groups; (B) mJOA RR comparison between MP and control groups; (C) Nurick grade comparison between MP and control groups; (D) NRR comparison between MP and control groups.
Effect Sizes and 95% Confidence Intervals (CI) for Reported Outcomes at 1, 3 and 24 Months Follow up.
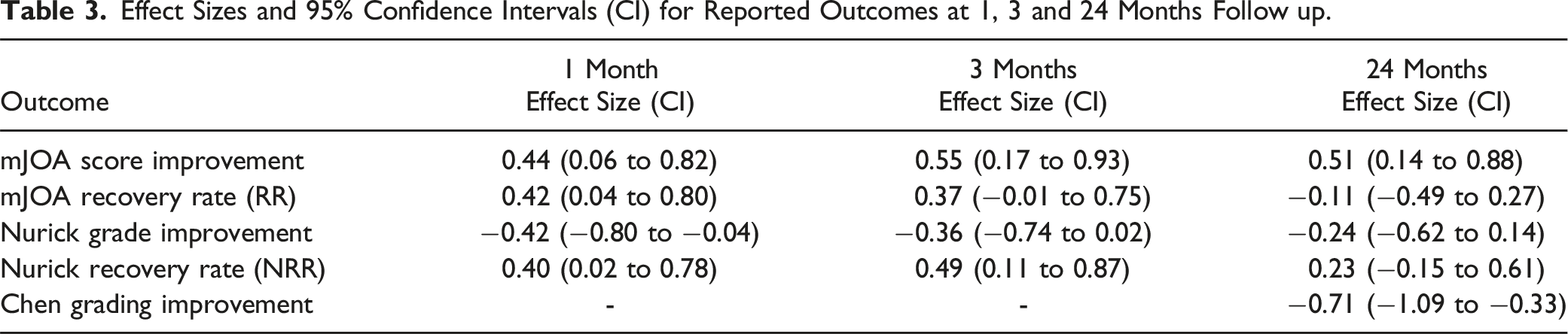
Similarly, mJOA-RR showed a moderate effect size of 0.42 and 0.37 at the 1—and 3-month follow-up, respectively. NRR improvements were observed, with effect sizes of 0.40 and 0.49 at the 1—and 3-month follow-up, respectively, but they were not statistically significant (P = .28) (Table 3).
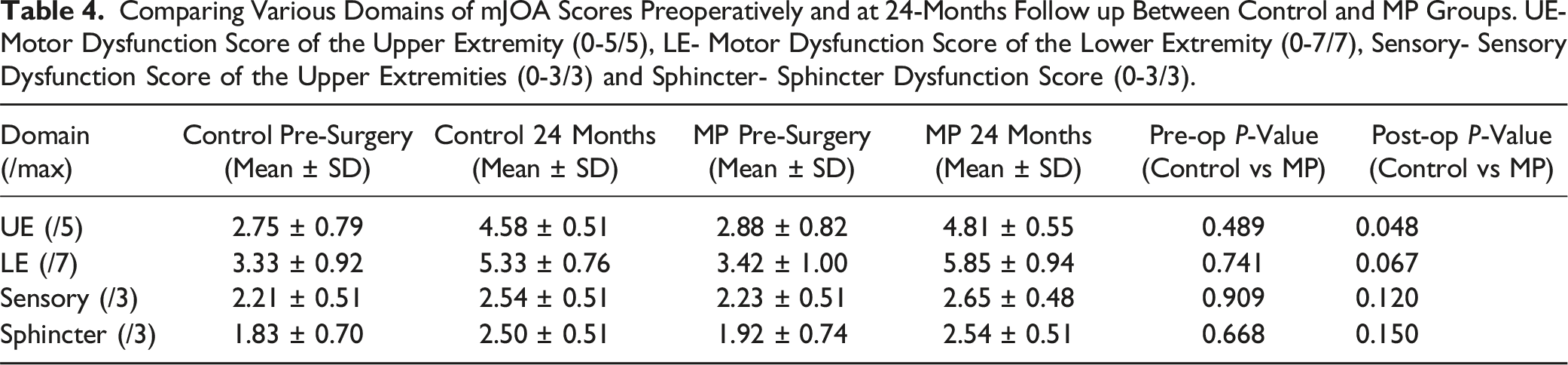
Comparing Various Domains of mJOA Scores Preoperatively and at 24-Months Follow up Between Control and MP Groups. UE- Motor Dysfunction Score of the Upper Extremity (0-5/5), LE- Motor Dysfunction Score of the Lower Extremity (0-7/7), Sensory- Sensory Dysfunction Score of the Upper Extremities (0-3/3) and Sphincter- Sphincter Dysfunction Score (0-3/3).
MRI Outcome
Both groups exhibited improved signal changes at 24 months follow-up on MRI. In the MP group, Type 0 ISI was observed in 14/26 patients, Type 1 ISI in 10/26, and Type 2 ISI in 2/26. Conversely, the control group showed Type 0 ISI in 2/24 patients, Type 1 ISI in 22/24, and no Type 2 ISI (Figure 4A). (A) Chen grade comparison between MP and control groups preoperatively and at 24 months follow up; (B) Comparison of Chen grading and mean change of Chen grading at 24 months (Δ Diff of grade) between MP and control groups.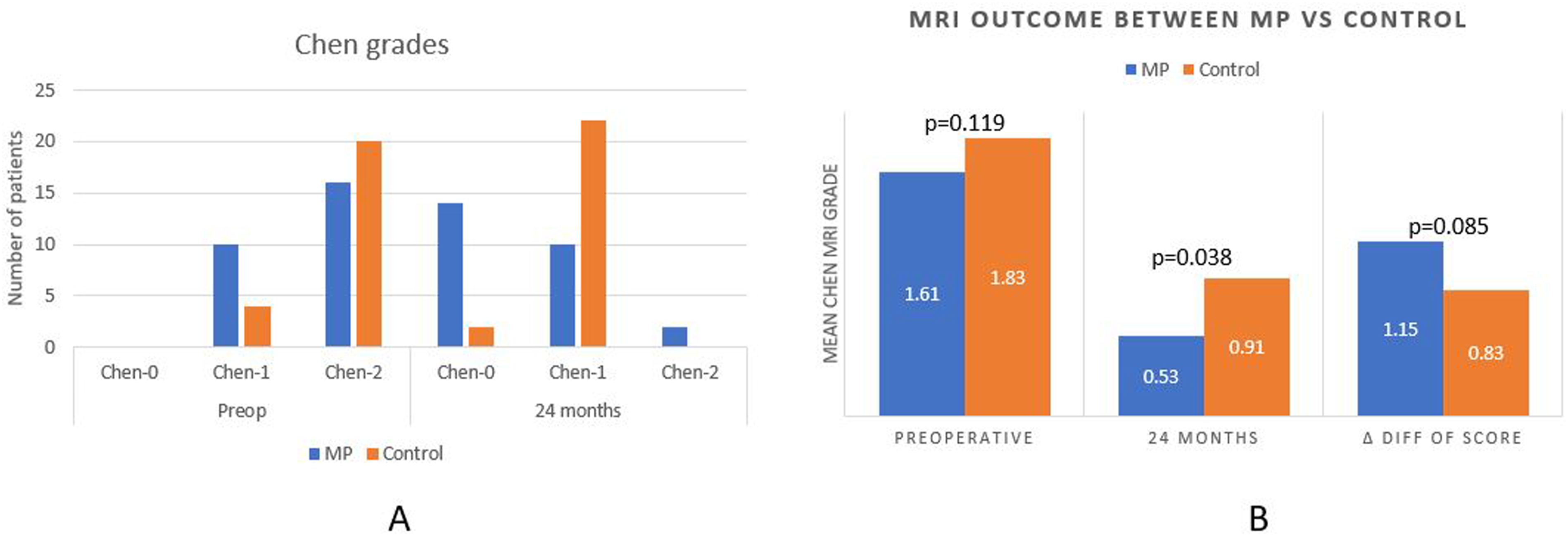
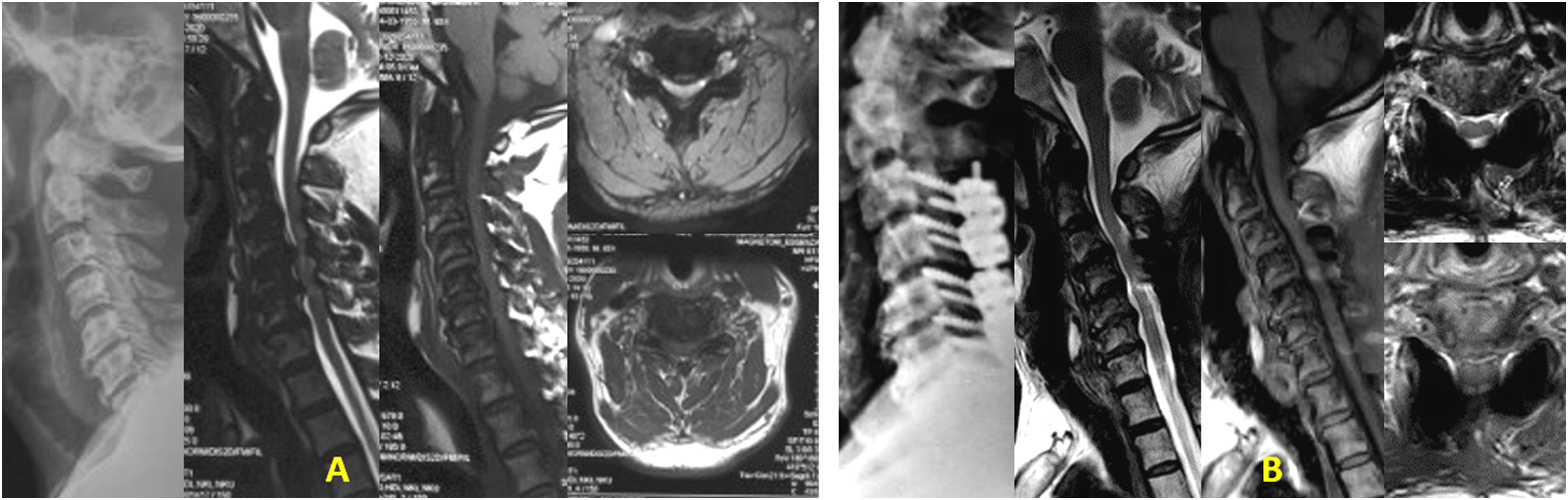
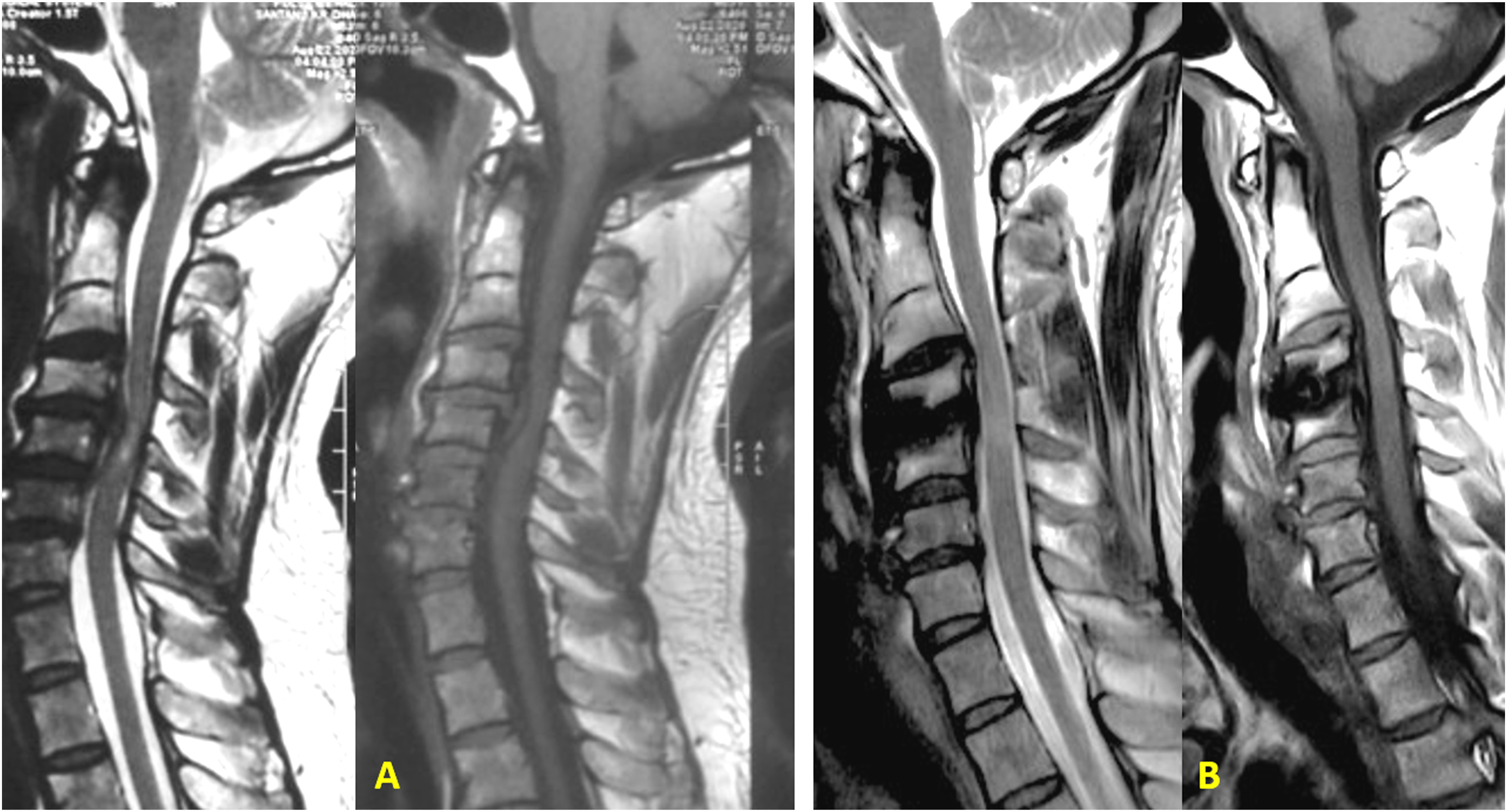
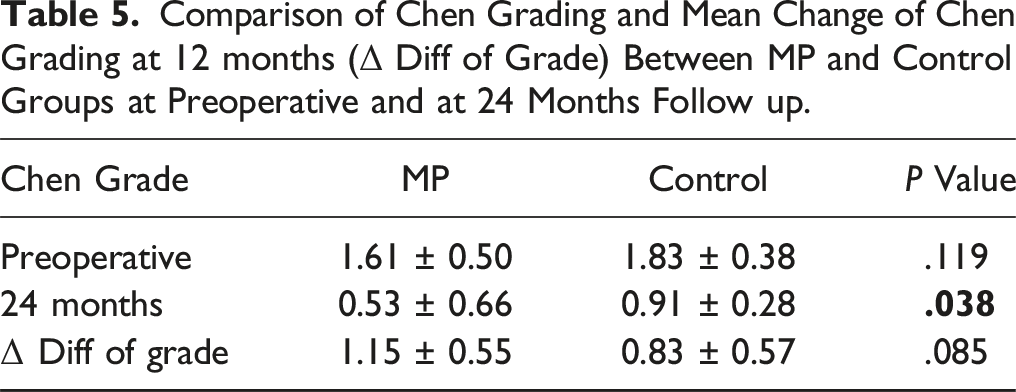
The improvement in signal changes within each cohort was statistically significant compared to preoperative grades (P < .0001). The MP group demonstrated a significantly better Chen grading at 24 months follow-up than the Control group (P = .038) with an effect size of −0.71 (95% CI: −1.09 to −0.33) (P = .038) (Table 3). Although the mean change of Chen grading at 24 months (Δ Diff of grade) was higher in the MP group (1.15 ± 0.55) than in the Control group (0.83 ± 0.57), the difference was not statistically significant (Table 5, Figure 4B). Figures 5-8 depict case examples of MP and Control groups with their radiological outcomes. Case1- 45-year-old male with C4/5 and C/6 PID with mJOA score 6, Nurick grade 4 with Chen grade 2 on MRI without any T1 hypointensity (Figure 5A). He underwent C4/5 and C5/6 ACDF. He belonged to the Control group. At 24 months follow up, mJOA score was 18 and Nurick grade 1 with MRI Chen grade 1 (Figure 5B). (A) Preoperative MRI T1 and T2 W images showing Chen grade 2 without any T1 hypointensity. (B) Postoperative MRI at 24 months follow up, showing reduction in signal intensity changes with Chen grade 1 with adequate decompression of the cord. Case 2- 64-year-old male with C6/7 PID with OPLL with mJOA score 9, Nurick grade 3 with Chen grade 2 on MRI without any T1 hypointensity (Figure 6A). He underwent C3-7 laminectomy and lateral mass screw fixation and fusion. He belonged to the Control group. At 24 months follow up, mJOA score was 16 and Nurick grade 1 with MRI Chen grade 1 (Figure 6B). (A) Preoperative MRI T2 and T1W images showing Chen grade 2 without any T1 hypointensity. (B) Postoperative MRI at 24 months follow up, showing reduction in signal intensity changes with Chen grade 1 with adequate decompression of the cord. Case 3- 66-year-old male with C5/6 PID with multilevel compression with mJOA score 7, Nurick grade 4 with Chen grade 2 on MRI without any T1 hypointensity (Figure 7A). He underwent C3-7 laminectomy and lateral mass screw fixation and fusion. He belonged to the MP group. At 25 months follow up, mJOA score was 14 and Nurick grade 1 with MRI Chen grade 1 (Figure 7B). (A) Preoperative MRI T2 and T1W images showing Chen grade 2 without any T1 hypointensity. (B) Postoperative MRI at 25 months follow up, showing reduction in signal intensity changes with Chen grade 1 with adequate decompression of the cord. Case 4- 66-year-old male with C4/5 PID with mJOA score 10, Nurick grade 3 with Chen grade 2 on MRI without any T1 hypointensity (Figure 8A). He underwent C4/5 ACDF. He belonged to the MP group. At 24 months follow up, mJOA score was 17 and Nurick grade 1 with MRI Chen grade 0 (Figure 8B). (A) Preoperative MRI T2 and T1W images showing Chen grade 2 without any T1 hypointensity. (B) Postoperative MRI at 24 months follow up, showing almost disappearance in signal intensity changes with Chen grade 0 with adequate decompression of the cord.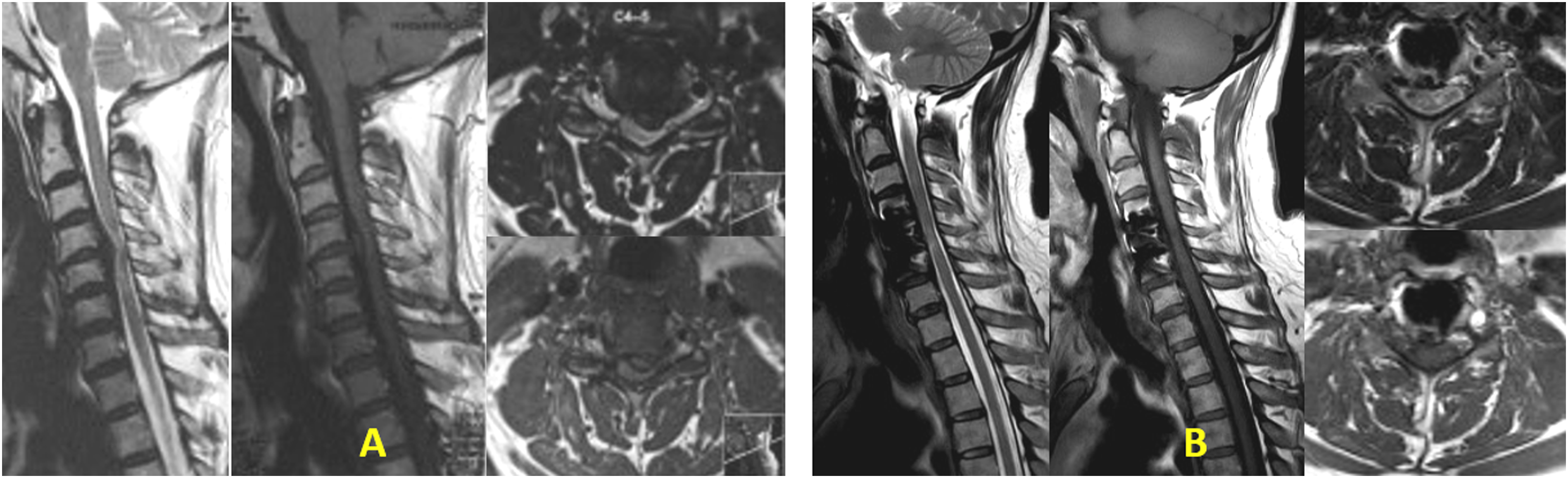

Correlation Analyses
The mJOA score and Nurick grade exhibited a robust negative correlation, with a stronger correlation observed preoperatively (Spearman’s ρ −0.8415) compared to 24 months postoperatively. The mJOA and Nurick grade recovery rates at 1-, 3-, and 24-month follow-ups demonstrated a positive correlation. Notably, the mJOARR showed a more robust correlation with NRR at 3 months (Spearman’s ρ 0.72287) than at 1 month (Spearman’s ρ 0.47093) and 24 months (Spearman’s ρ 0.64269).
In terms of functional measures (mJOA score, Nurick grade) and MRI outcome (Chen grade), preoperatively and at 24 months follow-up, the mJOA score exhibited a negative correlation with Chen grading, with comparable correlations (Spearman’s ρ Preoperative −0.4838, 24 months −0.4519). Similarly, Nurick and Chen grades demonstrated a positive correlation preoperatively and at 24 months follow-up, with comparable correlations (Spearman’s ρ Preoperative 0.4640, 24 months 0.4612).
Complications
Comparison of Chen Grading and Mean Change of Chen Grading at 12 months (Δ Diff of Grade) Between MP and Control Groups at Preoperative and at 24 Months Follow up.
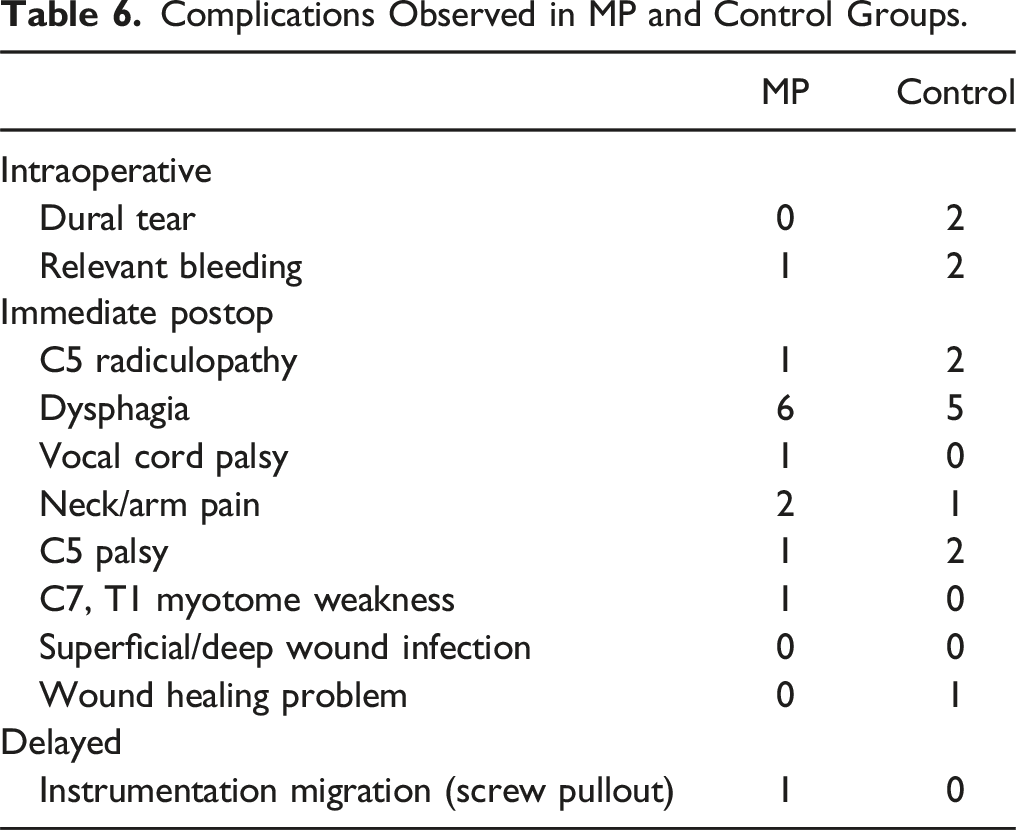
Complications Observed in MP and Control Groups.
Discussion
This study represents the pioneering exploration of Methylprednisolone (MP) as a neuroprotective and anti-inflammatory agent in DCM, coupled with its potential adjunctive role in surgical decompression. While MP has demonstrated positive effects in animal models of DCM, 21 its application in human DCM remains uncharted territory. Given the substantial inflammation caused by surgical decompression in DCM, this study is the first to investigate the use of the anti-inflammatory drug MP in mitigating this response and improving functional outcomes.
Drawing parallels with its role in posttraumatic spinal cord injury (SCI), some studies have shown the administration of MP within the first 8 hours has shown improved neurological results.22-28 However, its use in clinical practice remains debatable and not recommended by some studies due to conflicting findings and concerns about side effects. Although the context of acute SCI differs from DCM, the underlying mechanisms of inflammation and secondary injury remain similar, supporting the plausibility of MP’s beneficial effects in DCM surgery. Similarly, in experimental models of traumatic SCI and ischemic optic neuropathy, MP therapy has been demonstrated to prevent neurons from undergoing apoptosis and to decrease inflammation.29-31 It accelerates blood barrier recovery, reduces tissue damage, and attenuates macrophage recruitment into injured tissue.31,32 Moreover, MP may influence neurons and the networks that support them, perhaps reducing the loss of axonal excitability through 5-HT1A receptor, which is essential to the vertebrate locomotor network.33,34 Corticosteroids reduce surgical pain and hospital stays in patients with cervical radiculopathy or lumbar decompression.18,19 In our study, the MP group exhibited modest functional improvements compared to the Control group, particularly evident at the 1- and 3-month follow-ups. The short half-life of MP or the frequency of administration could account for this pattern, prompting the need for further investigations into the potential of repeated low-dose MP injections to induce long-term improvements.
This prospective study was carried out meticulously to obtain robust and unbiased results. Data bias was significantly reduced with the use of a triple-blinding in a Randomized Controlled Trial plus randomization using a computer-generated table and lastly independent observers to assess both MRI findings and Chen grade. Demographic data of patients, surgery parameters, and baseline status were comparable between the 2 groups and represented a pool of patients with different DCM pathologies (degenerative disc disease and OPLL).
The decompressive surgery for DCM showed statistically significant improvements in both groups throughout follow-ups, which aligns with promising results of surgery in the existing literature.35,36 Complications rates were similar in both groups; the temporary complications that were reported resolved within 1-3 months, providing evidence of the safety of MP use.
We used a multidimensional assessment of functional outcomes. Using both mJOA and Nurick scoring systems provides a more thorough evaluation of preoperative impairment and surgical outcomes. A strong association between mJOA scores and Nurick grade suggests that these 2 complement each other and are useful tools in DCM assessment. 37 Correlations (functional scores and Chen score) reflect the intricate relationships between the clinical, functional, and imaging markers, which offer valuable information on the overall effect of surgery and MP intervention on patients with DCM.
To provide a holistic view of effects of MP in DCM surgery, MRI signal changes were also assessed with clinical outcome. Corroborating with the existing literature, the T2-weighted MRI signal changes in our study correlated well with clinical scoring systems. 38 While our study did not have any patients with T1 hypointensity, the T2W signal changes were indicative of clinical outcomes. The low complication rates and the correlation between radiological and clinical parameters in our study further support the feasibility and safety of MP use in DCM.
Despite these insights, the study has limitations, including a small sample size, a monocentric study, and challenges in assessing MRI signal changes in the presence of metal implants and artifacts. This concern was addressed by assessing the MRI signal changes in both sagittal and axial cuts. Even though not every patient had an immediate postoperative MRI, full decompression was clinically determined by the combination of intraoperative findings and the improvement of symptoms postoperatively. Finally, the heterogeneity of this population (a variety of pathologies, and different surgical approaches used) strongly indicates future stratification of the results. Stratification in the data analysis can be achieved only with a much larger sample size. Future multicenter large sample-size study with longer follow-ups is required to take a more profound look at outcomes. Identifying and rectifying these shortcomings will also lead to an improved comprehension of the role of MP in DCM.
Conclusion
While the null hypothesis was not proven due to the limited nature of the study, the MP group demonstrated better functional and radiological outcomes than the Control group especially upper limb motor recovery and MRI signal changes. Although statistical significance was not reached for some outcomes, the effect sizes imply clinically meaningful benefits and merit further investigation. Importantly, intraoperative MP use proved to be safe, with no major complications observed. While recognizing the need for larger multicentric studies, we advocate the consideration of Methylprednisolone as a perioperative adjunct in DCM surgery to mitigate neurological complications and enhance outcomes. Future studies should focus on optimizing dosing and frequency of MP administration as well as developing a standardized protocol. The good correlation observed between mJOA score, Nurick grade, and MRI Chen grading emphasizes the robustness of our study in comprehensively assessing the MP’s impact in DCM surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.