
Abstract
Study Design
Retrospective cohort study.
Objective
This study aimed to investigate the long-term outcomes of laminoplasty-alone (LP) and combined procedure (CP), consisting of laminoplasty and single-level anterior cervical discectomy and fusion, in comparable patients who had multilevel degenerative cervical myelopathy (MDCM) with concomitant anterior and posterior compression (CAPC).
Methods
Consecutive MDCM patients with CAPC underwent LP or CP between 2012 and 2015 from a same surgical group were enrolled and followed up for a minimum of 8 years. Preoperative demographic, radiological, and clinical variables were collected. Propensity score matching (PSM) analysis was performed to match patients with comparable conditions. The outcomes were evaluated by postoperative Japanese Orthopedic Association (JOA) score improvement, JOA recovery rate (JOARR) and complications.
Results
A total of 230 patients were included, of whom 146 underwent LP and 84 underwent CP. After PSM, 84 pairs of comparable patients were matched. The matched groups presented fair comparability in preoperative conditions. The CP group had significantly prolonged surgery time and greater blood loss. At the final follow-up, the postoperative JOA scores of LP and CP groups were 14.51 ± 1.79 and 15.47 ± 1.81 (P < 0.001) and the JOARR were 42.5% ± 53.3% and 68.5% ± 35.4%, respectively (P < 0.001). Three (3.6%) patients in the LP group underwent reoperations because of recurrent symptoms (P = 0.081).
Conclusion
Both LP and CP demonstrated considerable long-term neurological recovery in patients with CAPC. The CP showed a significantly higher JOA improvement and JOARR. The combined decompression might be a safe and effective alternative in treating MDCM with CAPC in experienced hands.
Keywords
Background
Degenerative cervical myelopathy (DCM) is a common disease characterized by progressive spinal cord deterioration, which can lead to severe neurological dysfunction in approximately 20% of older patients.1-4 Multilevel DCM (MDCM), involving three or more intervertebral segments, often presents with severe neurological deficits and concomitant anterior and posterior compression (CAPC).5-7 The ideal surgical decompression strategy for MDCM with CAPC remains controversial.
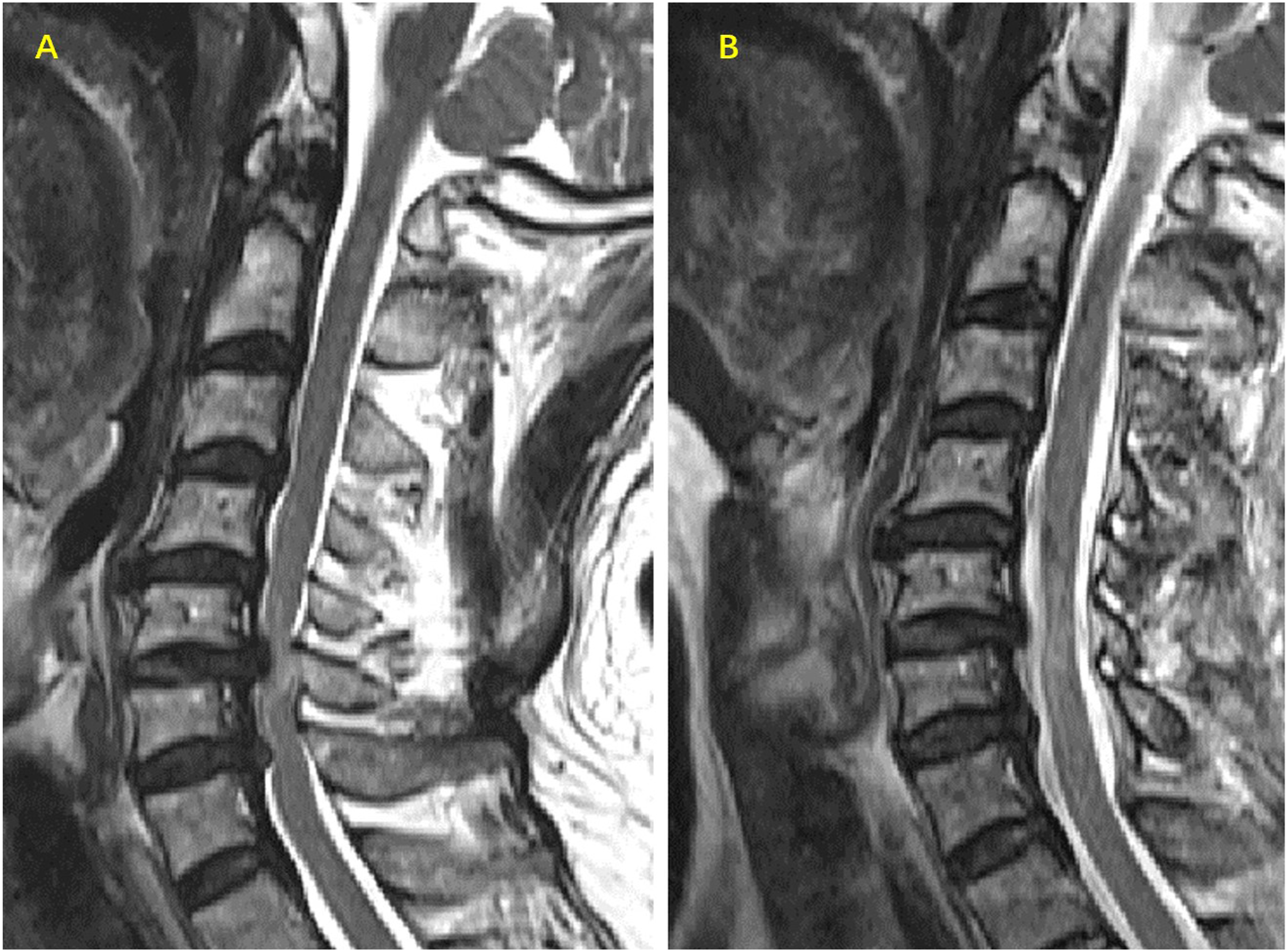
Different surgical approaches have been proposed for the treatment of MDCM, including posterior procedures such as laminoplasty or laminectomy with/without fusion, and anterior procedures such as anterior cervical discectomy and fusion (ACDF) or anterior cervical corpectomy and fusion (ACCF).8-10 The posterior laminoplasty (LP) allows for multilevel canal expansion and is generally preferred for treating MDCM patients with CAPC, especially in east Asia.11,12 However, in some MDCM patients with CAPC who presented with severe ventral compression, LP alone may not be sufficient to provide appropriate decompression (Figure 1). As the severe ventral compression (such as discs and/or osteophytes) might remain after posterior decompression, the ideal neurological recovery could not be achieved. Besides, the cervical disc degeneration may continue to progress, potentially leading to recurrent symptoms which requires reoperation soon. As a result, some surgeons have advocated for a combined procedure (CP) as an alternative for MDCM with CAPC.
13
An illustrated case with laminoplasty-alone who presented residual compression and further functional deterioration at 8-year follow-up. A 72-year old female patient presented with an 8-month history of numbness, weakness in left upper limbs, walking difficulty and unstable gait. The preoperative JOA score is 13/17. (A), (B): The preoperative sagittal and axial MRI showed multilevel stenosis with severe ventral compression at C3-4 (with arrow). (C): Preoperative sagittal CT. This patient underwent laminoplasty-alone. At 103 months after surgery, her postoperative JOA was 12. She had no improvement in neurological function and her numbness in left upper limbs worsened. But she still refused to accept secondary anterior decompression. (D), (E): The sagittal and axial MRI at the last follow-up revealed the residual ventral compression. F: The postoperative sagittal CT.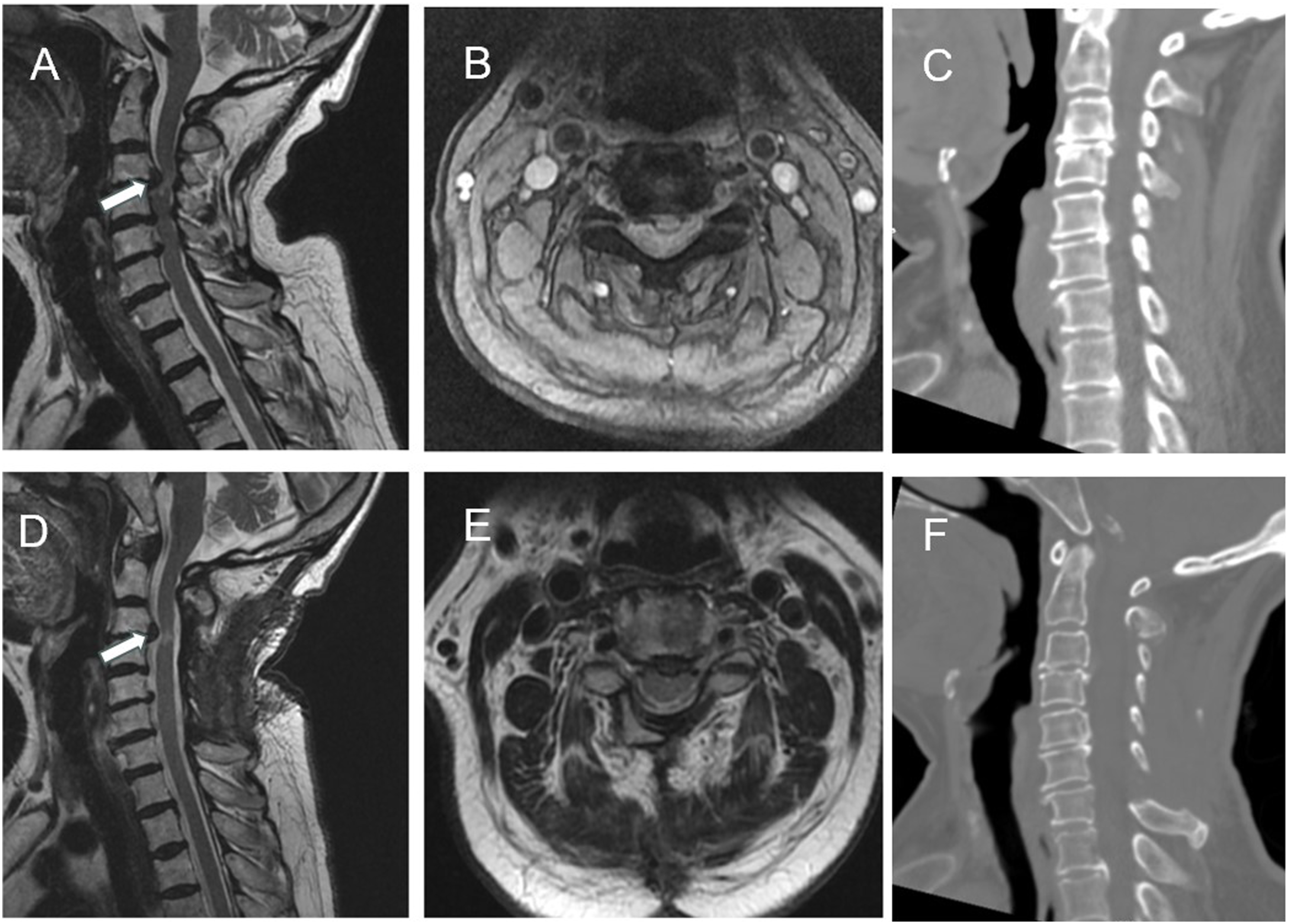
The CP involves performing a posterior decompression (typically laminoplasty) along with an additional anterior decompression (usually ACDF) at the level of the most severe compression, aiming to provide more appropriate decompression (Figure 2). An illustrated case with combined procedure consisting of a multilevel laminoplasty and single-level ACDF. A 48-year old male patient presented with a 24-month history of numbness, weakness, pain in upper limbs, and walking difficulty and unstable gait. The preoperative JOA score is 12/17. (A, B) The preoperative sagittal and axial MRI revealed multilevel stenosis and severe ventral compression at C5-6. (C) The preoperative sagittal CT. He had combined procedure with C3-7 laminoplasty and C5-6 ACDF. At 126 months after surgery, this patient had a normal neurological function and mild neck stiffness and has returned to routine life. The postoperative JOA was 17. (D, E) The sagittal and axial MRI at the last follow-up revealed there was no residual ventral compression. (F) The postoperative sagittal CT.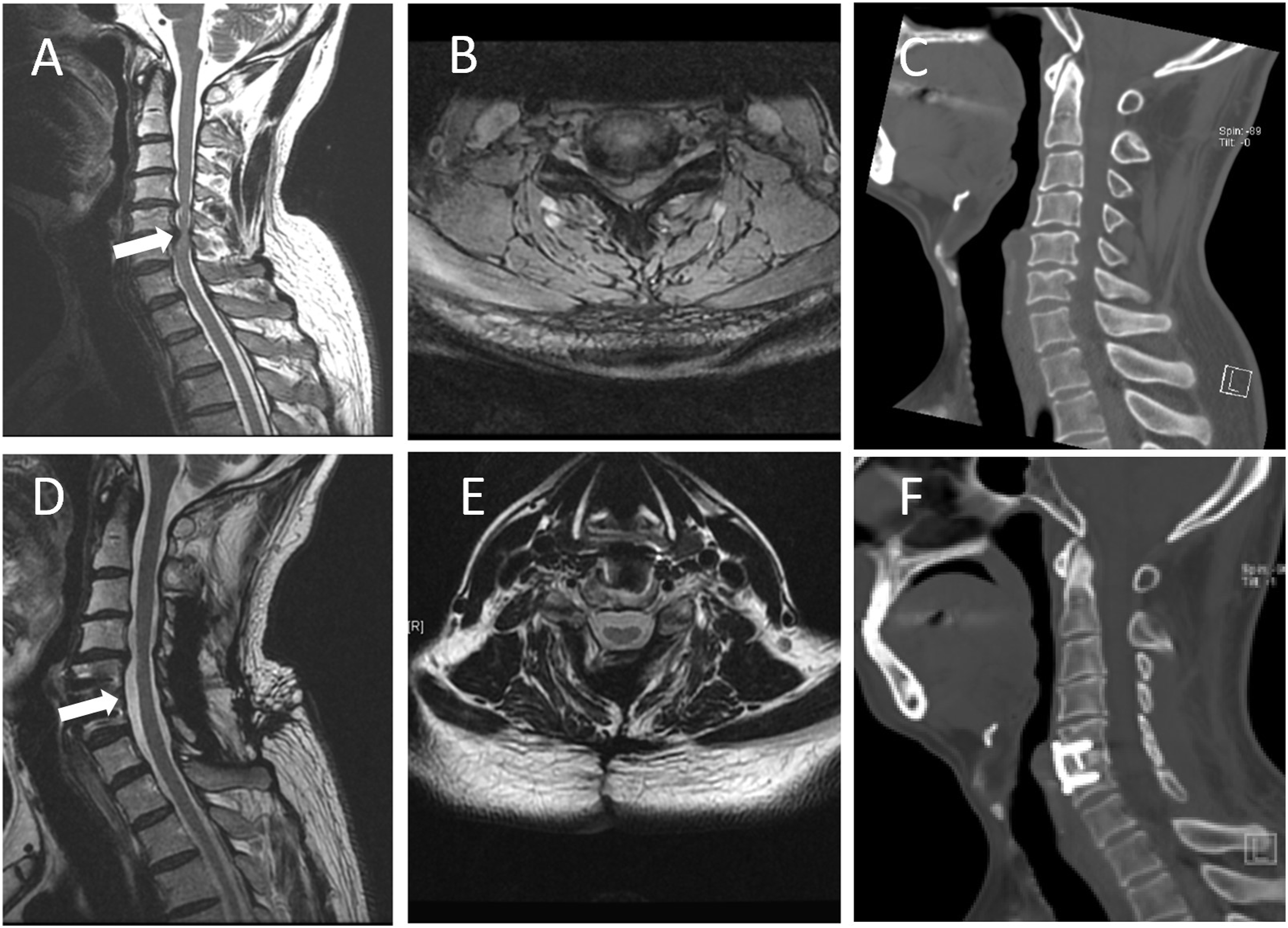
In clinical practice, the choice between CP and laminoplasty for MDCM patients with CAPC is often based on the location and extent of compressive pathology and the preferences of the surgeon. Some surgeons argue that the CP procedure may result in greater surgical trauma and multilevel LP is usually sufficient.11,12,14,15 Others recommended performing a posterior laminoplasty initially and waiting several weeks for neurological recovery outcomes before deciding whether to proceed with additional anterior decompression (two-stage combined posteroanterior decompression procedure),16,17 while there are also concerns that two separate admissions and operations might increase overall costs and delay neurological recovery, and one-stage combined procedure could achieve sufficient decompression in one surgery and have advantages in preserving sagittal stability and withstands further possible restenosis.18,19 Comparison of clinical outcomes of CP and LP-alone for MDCM patients with CAPC was needed to answer this debate.
However, as previous studies focused on short-term efficacy, the long-term outcomes of CP for MDCM patients with CAPC remain unknown.7,11-13,20,21 Furthermore, few studies have utilized appropriate statistical methods to control for confounding factors and ensure preoperative homogeneity, resulting in significant selection bias and limiting the reliability and applicability of their findings.
Therefore, controlling for preoperative differences is required to appropriately compare the long-term clinical outcomes of one-stage CP and LP procedures for MDCM patients with CAPC. This study employed propensity score matching (PSM) to achieve preoperative comparability and investigate the long-term surgical outcomes of one-stage CP and LP-alone procedures for MDCM patients with CAPC, with an 8-year follow-up. Our hypothesis is that the one-stage CP might have better efficacy in long-term neurological recovery.
Methods and Materials
Subjects
Approved by the hospital ethics reviewing board, this study was conducted according to the principles of the Declaration of Helsinki (IRB00006761-2016001). Because of the retrospective nature of this study, the need for informed consent was waived. The data from consecutive patients who underwent surgery for DCM between January 2012 and December 2015 at our institute were retrospectively reviewed and the patients with confirmed MDCM and CAPC were collected and followed up. The inclusion criteria are as follows: 1. Radiographically confirmed MDCM with clinical symptoms and signs 22 ; 2. Confirmed with CAPC (concomitant ventral compression and multilevel stenosis, anterior compression caused by disc herniation with/without osteophyte, and posterior compression by ligamentum flavum infolding); 3. at least three surgical segments were operated with either the laminoplasty-alone (LP-alone) and one-stage combined procedure (CP). And 4. A minimum of 96 months of follow-up. The exclusion criteria were as follows: 1. Surgery involving a spinal tumor or trauma; 2. Cervical kyphosis >10° (C2-7 Cobb angle); 3. Accompanying cervical ossification of the posterior longitudinal ligament; and 4. History of previous cervical spine surgery.
The medical records, surgical characteristics, and imaging features were systematically investigated. Based on surgical approaches, patients were divided into LP and CP groups. The design of this study is shown in Figure 3. The flow chart of the study design, patient recruitment and follow-up. Abbreviation: LP: Laminoplasty, CP: combined procedure, JOA: Japanese orthopedics association score, JOARR: JOA recovery rate, MICD: minimally important clinical difference.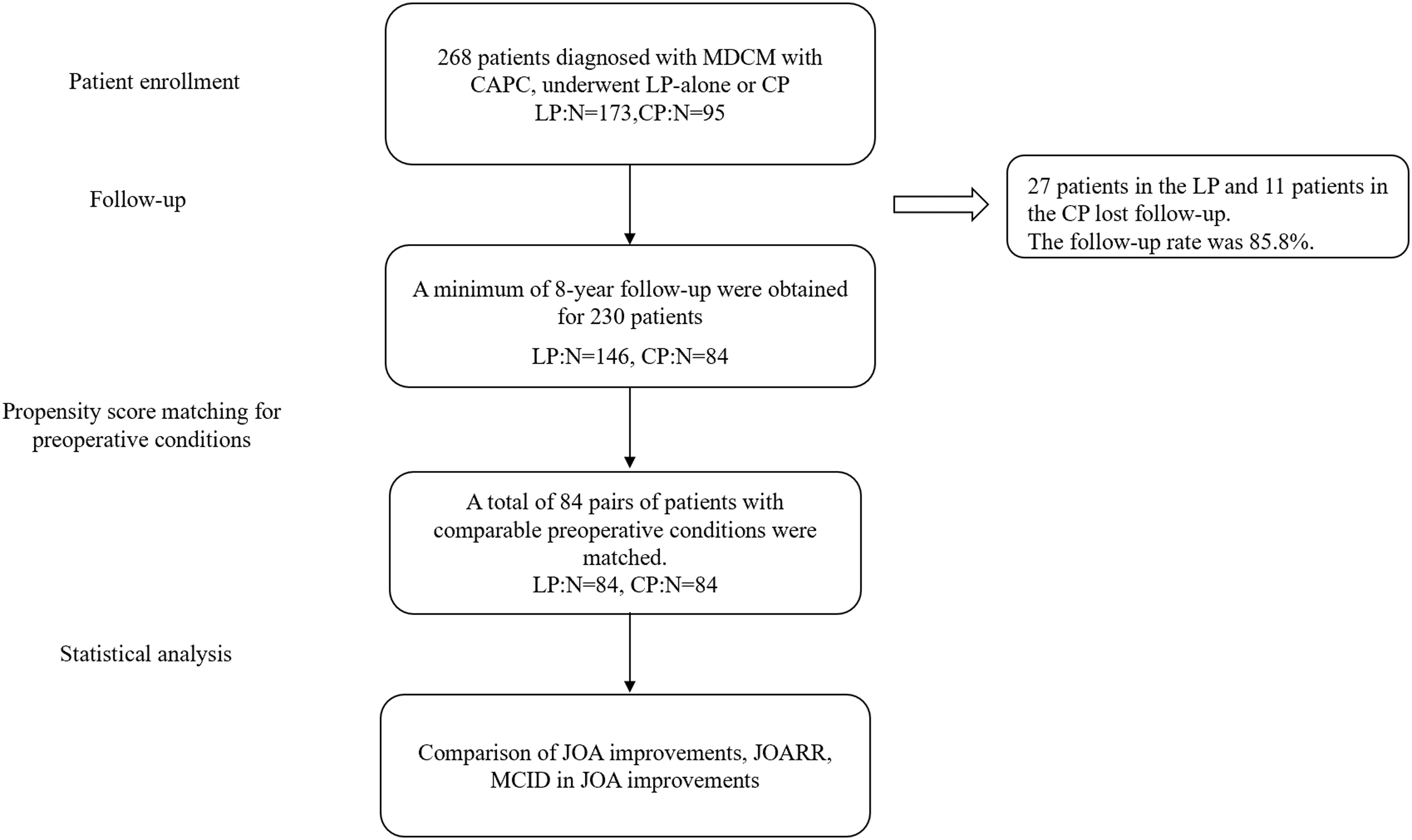
Surgical Management
All surgeries were performed by the three senior spine surgeons from same team. The posterior approach uses multilevel open-door laminoplasty; the one-stage combined approach consisted of an initial multilevel open-door laminoplasty in the prone position (posterior stage), and followed by a single-level ACDF at the level with most severe compression in the supine position (anterior stage).
22
The choice of surgical approach was determined based on the characteristics of spinal cord compression and was decided by our spine team discussion.
13
Generally, the CP procedure is recommended for MDCM patients with CAPC presenting with multilevel spinal canal stenosis and severe ventral compression, whereas the LP procedure is employed for MDCM patients with CAPC presenting with multilevel spinal canal stenosis with or without severe ventral compression. After surgery, patients were advised to wear a soft cervical collar for comfort during the following 4 weeks. Routine follow-up visits were scheduled at 3 months, 6 months, 1 year, 3 years, 5 years, and 8 years after surgery Figures 4 and 5. An illustrated case with concomitant anterior and posterior compression preoperatively who received laminoplasty-alone and presented slight residual compression and favorable functional recovery postoperatively. A 54-year old female patient presented with a 12-month history of numbness, weakness in upper limbs, weakness in lower limbs and walking difficulty and unstable gait. The preoperative JOA score is 12/17. (A, B) The preoperative sagittal and axial MRI revealed multilevel stenosis and severe ventral compression at C3-4. The patient had a C3-7 laminoplasty. At 96 months after surgery, this patient had a normal neurological function and has returned to routine life. The postoperative JOA was 17. (C, D) The postoperative sagittal and axial MRI revealed slight residual cord compression at C3-4. An illustrated case with concomitant anterior and posterior compression preoperatively who had laminoplasty-alone and presented slight residual compression and favorable functional recovery postoperatively. A 65-year old female patient presented with a 37-month history of numbness, weakness in upper limbs, walking difficulty and unstable gait. The preoperative JOA score is 12.5/17. (A) The preoperative sagittal MRI revealed multilevel stenosis and severe ventral compression at C5-6 and C6-7. The patient had a C3-7 laminoplasty. At 108 months after surgery, this patient had a normal neurological function with slight numbness in lower limbs and has returned to routine life. The postoperative JOA was 16.5/17. (B) The postoperative sagittal MRI revealed there was slight cord compression at C5-6 and C6-7.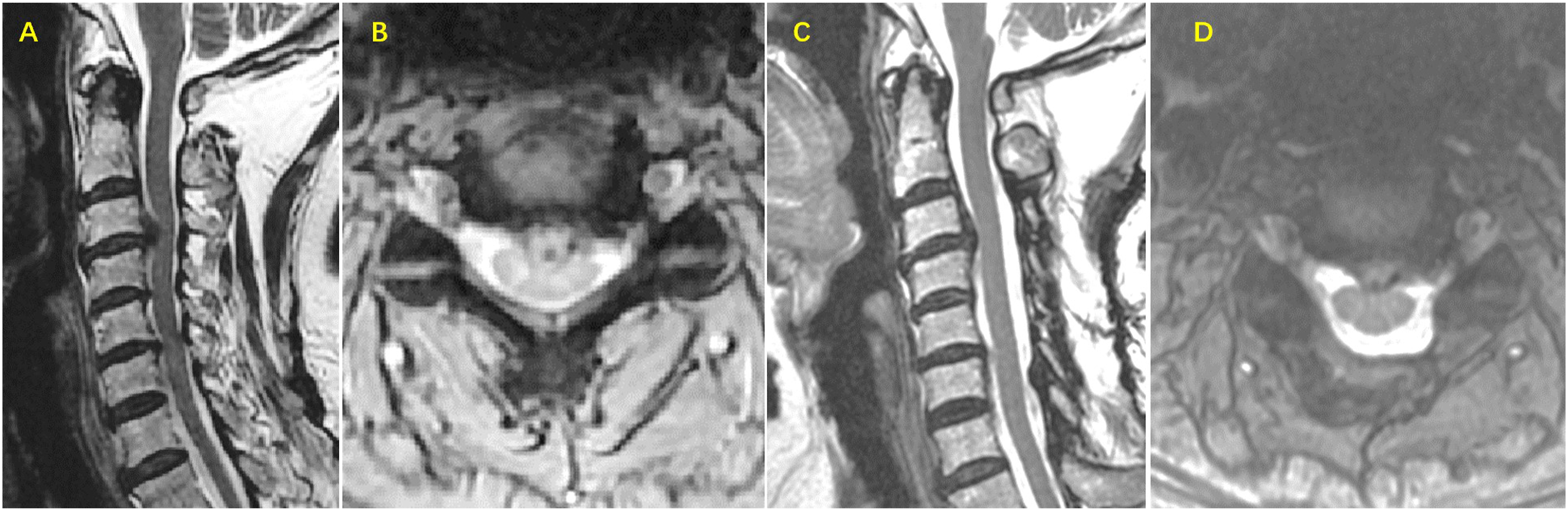
Radiological Measurements
The preoperative radiological examinations were systematically reviewed, including the radiography, computed tomography (CT), and magnetic resonance imaging (MRI). Cervical alignments (C2-7 Cobb angle) were measured using lateral radiographs at neutral position. 10 The sagittal occupancy ratio of the canal was measured at the maximal cord compression on the sagittal T2-weighted magnetic resonance images (T2WI) and is calculated by the diameter of anterior compression divided by the anteroposterior diameter of the canal. 23 All measurements were performed twice by trained orthopedic residents.
Outcome Assessments
Preoperative demographics, clinical variables, and surgical characteristics were collected from medical records. The surgical outcomes were evaluated using the Japanese Orthopaedic Association (JOA) score.24,25 and the JOA recovery rate (JOARR) a minimum follow-up period of 96 months after surgery. 26 The neck disability index (NDI) and visual analogue scale (VAS) were also documented. The JOARR was classified into four recovery grades based on Odom’s standard: <25% (poor), 25%–50% (fair), 50%–75% (good), and >75% (excellent). 27 The achievement of minimal clinically important difference (MCID) in JOA score improvement, defined as an improvement of more than 2.5, and the postoperative functional deterioration, defined as a decrease in postoperative JOA score, were documented. The patient-reported satisfactory rates of neurological recovery were also analyzed. These DCM patients were classified based on symptomatology. 28
Perioperative complications, including cerebrospinal fluid (CSF) leakage, wound complications, hematoma, esophageal fistula, C5 palsy, and iatrogenic neurological injury, were assessed using medical records. Other complications, such as dysphagia, dysphonia, C5 palsy, and axial symptoms (including postoperative discomfort in the neck, shoulder, or periscapular region, such as pain, fatigue, stiffness, and tightness), were evaluated at the final follow-up. 8
Statistical Analysis
The statistical analysis was performed using SAS version 9.2. Categorical and continuous variables were expressed as percentages and mean ± standard deviation, respectively. Chi-square (χ2) tests, analysis of variance, t-tests, or nonparametric analyses were used to assess differences between groups.12,24,27 PSM was employed to address confounding biases. The propensity score of the surgical procedure was calculated using age, gender, preoperative JOA score, preoperative C2-7 Cobb angle, and sagittal occupancy ratio in a logistic regression model. The C-statistic, indicating the model’s goodness-of-fit, was 0.63, indicating fair efficacy. Patients in the LP and CP groups were matched based on the calculated propensity scores using a caliper of <0.1. Statistical significance was defined as a two-tailed P-value less than 0.05.
Results
Population Characteristics
A total of 268 MDCM patients with CAPC have underwent LP or CP during 2012 to 2015. A minimum of 8-year follow-up were obtained for 230 (85.6%) patients. The average follow-up duration was 106.3 ± 10.9 months. This preliminary cohort consists of 146 patients in LP group and 84 in CP group. Then, the patients in this cohort from the LP and CP groups were matched according to the calculated propensity scores. After PSM, 84 pairs of comparable patients from the LP and CP groups were matched.
The Baseline Demographic, Clinical and Radiological Characteristics of Laminoplasty-Alone and Combine Procedure Groups Before and After Propensity Score Matching.
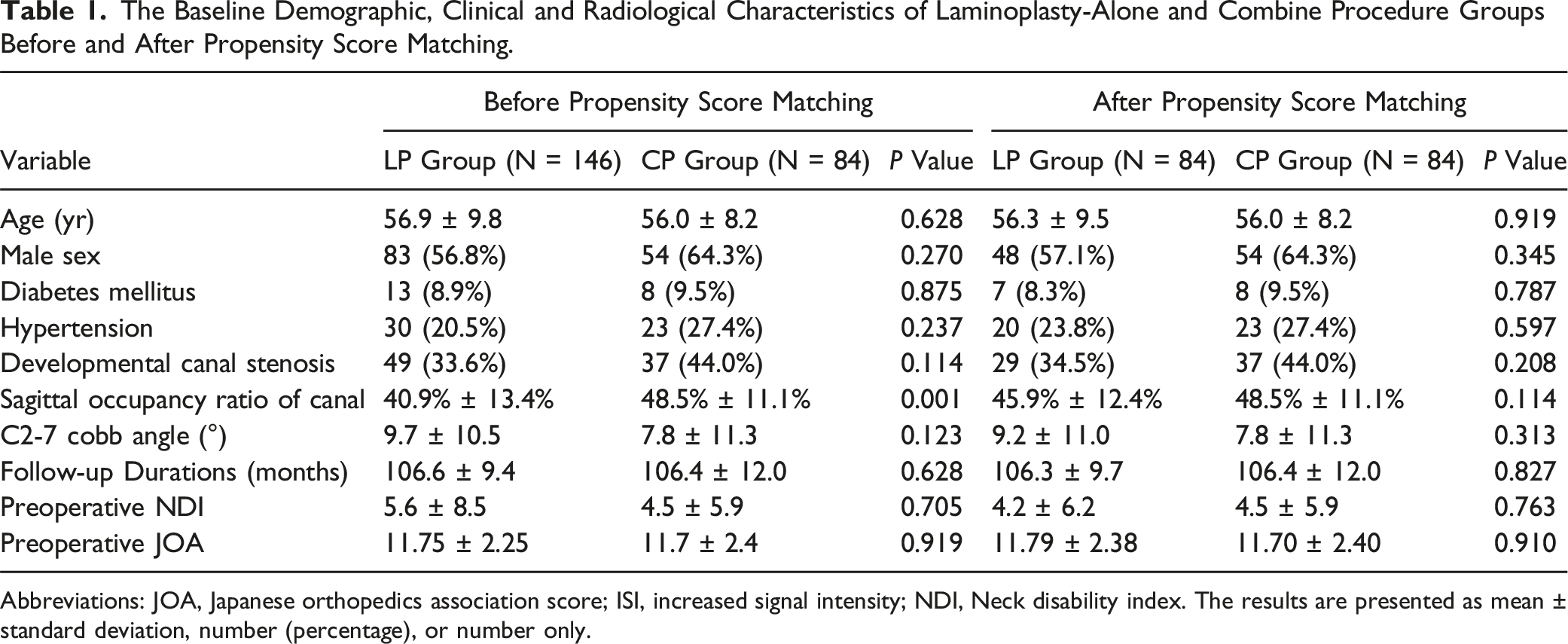
Abbreviations: JOA, Japanese orthopedics association score; ISI, increased signal intensity; NDI, Neck disability index. The results are presented as mean ± standard deviation, number (percentage), or number only.
The Symptomatology Classification of Patients in Laminoplasty-Alone and Combine Procedure Groups Before and After Propensity Score Matching.

Operation
The average number of segments operated on in the LP and CP groups was 4.9 ± 0.5 and 5.0 ± 0.3, respectively (P = 0.297). The CP group had a longer surgery duration (223.0 ± 53.7 min and 142.0 ± 43.5 min, respectively, P < 0.001) and greater blood loss compared to the LP group (340.1 ± 216.2 mL and 297.4 ± 233.5 mL, respectively, P = 0.007) (Table 2).
The overall complication rate did not differ significantly between the groups. No severe perioperative complications such as paralysis, esophageal fistula, iatrogenic neurological injury, or hematoma were observed in either group. In the CP group, two cases of CSF leakage, one case of C5 palsy, and one wound complication were reported. In the LP group, three cases of C5 palsy were reported. At the final follow-up, four patients (4.8%) in the CP group and one patient in the LP group reported dysphagia (P = 0.174). Additionally, 11 patients (13.1%) in the LP group and 10 patients (11.9%) in the CP group reported axial symptoms (P = 0.317). Three patients (3.6%) in the LP group underwent reoperation due to recurrent symptoms, while no reoperations were performed in the CP group (P = 0.081).
Surgical Outcome
The Surgery and Complication Characteristics in LP and CP Groups.
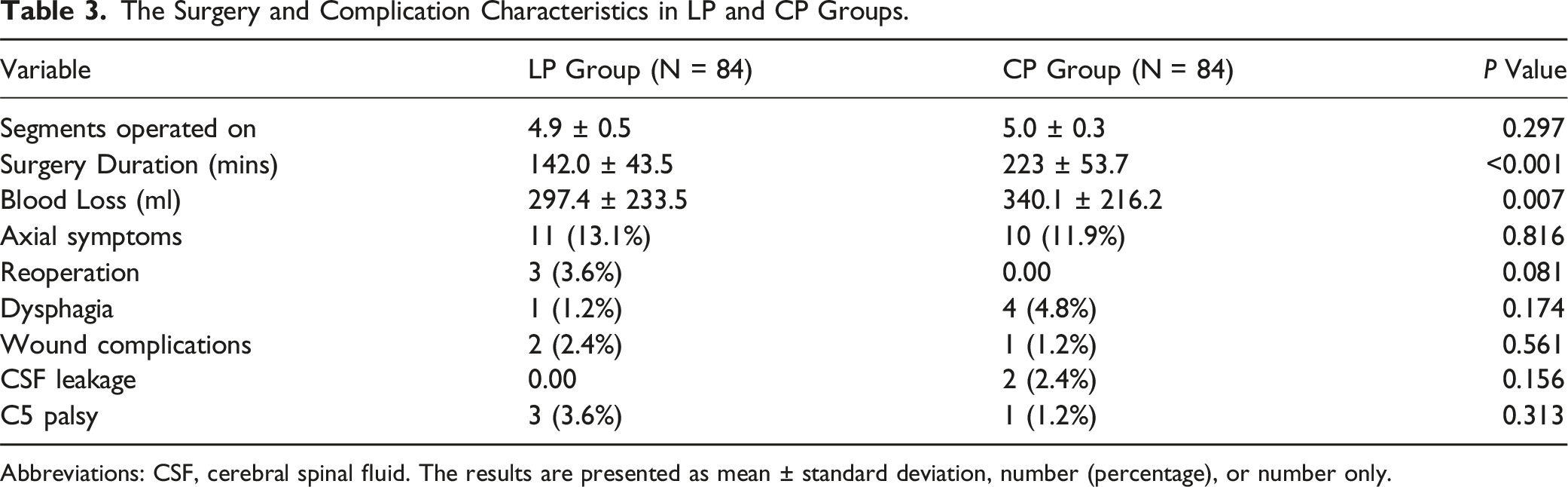
Abbreviations: CSF, cerebral spinal fluid. The results are presented as mean ± standard deviation, number (percentage), or number only.
In terms of JOARR grade, 18 patients (21.4%) in the LP group and 5 patients (6%) in the CP group reported poor recovery, 13 patients (15.5%) in both groups reported fair recovery, 32 patients (38.1%) in the LP group and 22 patients (26.2%) in the CP group reported good recovery, and 21 patients (25%) in the LP group and 44 patients (52.4%) in the CP group reported excellent recovery.
The Long-Term Surgical Outcomes in LP-Alone and CP Groups.
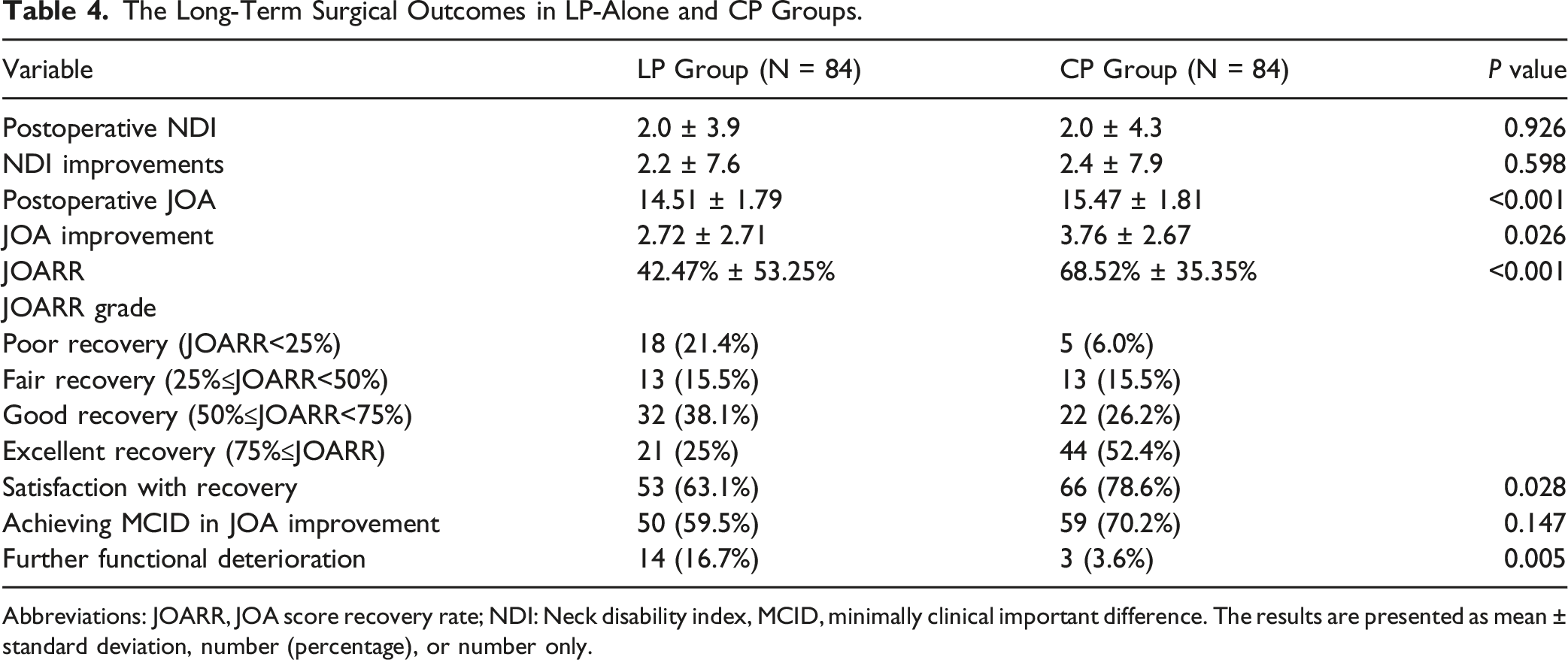
Abbreviations: JOARR, JOA score recovery rate; NDI: Neck disability index, MCID, minimally clinical important difference. The results are presented as mean ± standard deviation, number (percentage), or number only.
Discussion
Our study demonstrated that both laminoplasty-alone and one-stage combined procedure could improve the neurological function of patients with MDCM over an 8-year follow-up period. In patients with comparable preoperative conditions, the CP presented better neurological function preservation than the LP. The combined procedure might be an effective alternative in treatment for MDCM patients with CAPC.
The ideal decompression choice for MDCM patients with CAPC remains challenging. Generally, the LP procedure is the most common choice for MDCM with CAPC, 7 especially in East Asia. The LP procedure allows for multilevel canal expansion through a single incision, facilitating posterior drifting of the spinal cord and providing adequate decompression and favorable neurological recovery in most cases. However, in patients with severe anterior compression or loss of cervical lordosis, laminoplasty-alone may not achieve sufficient decompression, leading to unsatisfactory neurological outcomes. 29 (Figure 1). Furthermore, some patients might experience postoperative function decline after further disc degeneration, which requires reoperation. 30 Faced with this difficulty, some surgeons proposed two-stage combined decompression as an alternative approach for these patients. However, there are limitations with implementing this procedure in clinical practice.16,17 The two separate admissions and operations increases overall costs, surgical trauma, risk and pain, and the patients’ compliance with the additional surgery is restricted by many real-world difficulties. The patients who require two-stage combined decompression could not always receive the necessary surgery, leading to poor neurological recovery and impacted quality of life.
Therefore, the one-staged CP was considered as a valuable alternative for selected patients with MDCM and CAPC in clinical practice, particularly those with severe ventral compression and a higher risk of inadequate decompression with laminoplasty-alone. Some studies have compared the short-term efficacy of CP and LP-alone, however, the results were not consistent and the long-term effectiveness of this procedure remains unclear.7,11-13,20,21 Furthermore, previous studies have not adequately controlled for the selection bias and baseline confounders when comparing different approaches. Therefore, using PSM analysis, this study aimed to match patients with preoperative homogeneity, there for reducing potential selection bias.
After PSM, both CP and LP groups presented similar preoperative clinical and radiological characteristics, including fair cervical lordosis and severe ventral compression. Furthermore, the patients showed similar distribution in symptomatology classification with high proportion of transverse symptoms. After an over 8-year follow-up, most patients in both groups maintained MCID in postoperative JOA improvement, with no significant difference between the groups. However, the CP group showed significantly greater improvements in JOA scores and higher JOARR, and presented significant advantages in preventing further functional deterioration and improving overall satisfactory rate. Possible explanations for this superiority might be that in the CP group, the direct thorough anterior decompression eliminate the risk of insufficient decompression and further degeneration of responsible disc. Additionally, the anterior fixation in CP helps to maintain cervical alignment and prevent further kyphosis, which can lead to neurological deterioration. Further investigations incorporating radiological characteristics at the final follow-up are needed to clarify these mechanisms.
Safety, technical complexity, and the extent of surgical trauma are significant factors that impact surgical planning. Obviously, the CP has greater technical complexity and surgical trauma compared to LP-alone, which may result in increased blood loss, prolonged surgical duration, and possibly a higher risk of complications. Fehlings et al. 31 reported that the CP had an increased incidence of complications, especially dysphagia. However, Li et al. 11 described the CP had a comparable perioperative and short-term complication rate as LP. In this study, the one-stage CP demonstrated a significant longer surgical duration and greater blood loss. However, there were no significant differences in the overall complication rate between the two groups. The CP presented a higher incidence of complications related to anterior fusion (such as dysphagia), but this difference was not statistically significant. Additionally, the reoperation rate was lower in the CP group compared to the LP group, and lower than the reported incidence of 2% to 3.2% for LP procedures in previous literature.32,33
In conclusion, the CP procedure might be an effective method for MDCM patients with CAPC, especially preserved for patients who faced higher risk of insufficient decompression and re-degeneration by LP alone, but only should be performed in experienced hands after cautious consideration of its technical complexity and invasiveness. On the one hand, the CP procedure presented kind of efficacy in preventing long-term further neurological functional deterioration and lead to higher satisfactory rate. On the other hand, the CP also carries considerations of being a more invasive procedure with greater surgical trauma, prolonged surgical duration and possible anterior fusion related complications. We advocate that surgeons carefully analyze the compression characteristics and potential risk of insufficient decompression and re-degeneration of each patient, and make individualized decompression strategy for MDCM patients with CAPC. Further investigation to identify the risk factors of insufficient decompression and postoperative further functional deterioration after LP would help to determine the precise indications of CP in MDCM patients.
Our study has certain limitations. Firstly, due to its retrospective nature, this study lacked randomization, which could introduce biases and limitations in acceptability of the results. Further multicenter prospective studies with large sample sizes and continuous follow-ups will enable further investigation of neurological recovery over time. Secondly, this study lacks the analysis of long-term radiological outcome of LP and CP. Further investigations involving postoperative radiographic characteristics and radiomics would help to clarify possible mechanisms the superiority of CP in clinical function. 34
Conclusion
Both the LP and CP groups demonstrated considerable long-term neurological recovery in MDCM patients with CAPC. In the patients with comparable preoperative conditions, the CP group showed a significantly higher JOA improvement and JOARR, but no significant difference was observed in the ratio of achieving MCID in JOA improvement. The combined decompression might be a safe and effective alternative for experienced hands in treatment for MDCM with CAPC, while also needs cautious considerations because of its invasiveness.
Footnotes
Acknowledgments
We thank Miss Qianqian Li for her help in data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the This study was supported by the Peking University Third Hospital Research Foundation (NO. BYSYZD2019005).
Ethical Statement
Data Availability Statement
Research data supporting this publication are available from the Peking University Third Hospital, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly.