
Abstract
Study Design
Prospective cohort study.
Objectives
The purpose of this study was to prospectively evaluate the impact of a preoperative diagnosis of gastroesophageal reflux disease on the incidence and severity of postoperative dysphagia in a multicenter population.
Methods
After Institutional Review Board approval, written informed consent was obtained from all participating patients. Patients over 18 years of age who underwent an elective anterior cervical discectomy and fusion for a degenerative condition were prospectively enrolled at two academic centers from the years 2018 to 2020. Patients were separated into two groups: those with and without a preoperative diagnosis of GERD. Continuous variables were assessed using either an independent t-test or Mann Whitney U-test for parametric and non-parametric data. All categorical variables were compared using a chi-square test.
Results
A total of 116 patients met study criteria and were subsequently enrolled. Overall rates of postoperative dysphagia increased to 47.3% (n = 53) at 2-weeks but eventually decreased towards the preoperative prevalence of 25.0% at the 24-week mark. Patients with preoperative diagnosis of GERD had lower dysphagia severity scores on a continuous variable analysis in both the DSQ and EAT-10 surveys at 2-week follow-up in addition to the Bazaz survey at 24-week follow-up. Our follow up at 24-weeks was 85.7%.
Conclusions
Our study shows that having a preoperative diagnosis of GERD has no significant effect on the incidence of dysphagia following ACDF. Nevertheless, having a preoperative diagnosis of GERD does seem to provide some protective effect on the severity of dysphagia that this patient population develops at multiple intervals over a 24-week postoperative period.
Introduction
Dysphagia is one of the most common complaints following anterior cervical discectomy and fusion (ACDF). This complication, while commonly transient in nature, has been associated with increased postoperative morbidity including increased length of stay, higher rates of readmission, and functional disability.1,2 While the presence of numerous proposed etiologies of postoperative dysphagia emphasize its likely multifactorial nature, prolonged retraction, increased number of operative levels, longer operative time, and postoperative edema are commonly cited risk potential risk factors.3-6
While there is little doubt that the operative insult associated with anterior cervical spine surgery imposes a significant risk for postoperative dysphagia, numerous patient specific risk factors have yet to be fully explored. Recently, Okano et al found that preoperative smoking status and preoperative opioid use were independent predictors of dysphagia. 7 Similarly, Smith-Hammond et al found that increasing age places patients at risk for dysphagia following anterior cervical spine surgery. 8 While the impact of a preoperative diagnosis of gastroesophageal reflux (GERD) has yet to be evaluated as a potential risk factor for dysphagia, Rihn et al found that patients had an increased incidence and severity of postoperative GERD following ACDF relative to those patients undergoing lumbar spine surgery. 9 To our knowledge, no prior prospective study has reported on the incidence and severity of dysphagia following ACDF based on a patient’s preoperative diagnosis of GERD.
As such, the purpose of this study was to prospectively evaluate the impact of a preoperative diagnosis of GERD on the incidence and severity of postoperative dysphagia in a multicenter population.
Methods and Materials
Patient Selection and Data Collection
After Institutional Review Board (IRB) approval was obtained, all subjects provided informed written consent to participate in the study. Patients over 18 years of age who underwent an elective anterior discectomy and fusion (ACDF) for a degenerative condition were prospectively enrolled at two academic centers from the years 2018 to 2020. Patients were asked to complete a preoperative demographic survey in addition to dysphagia surveys (Bazaz, DSQ, EAT-10) both preoperatively and at 2, 6, 12, and 24 weeks postoperatively. Exclusion criteria included previous cervical fusion at the operative level or surgery for oncologic, infectious, or traumatic indications.
Statistical Analysis
Patients were separated into two groups: those with a preoperative diagnosis of GERD and those without. The diagnosis of GERD was made based on clinical presentation. All data were entered into and stored in a computerized database. Descriptive statistics were used to characterize patient demographics and outcome measures and are represented by mean ± standard deviation. Continuous variables were assessed using either an independent t-test or Mann Whitney U-test, for parametric and non-parametric data, respectively. All categorical variables were compared using a chi-square test. Statistical analyses were performed in R Studio software (R Foundation for Statistical Computing). A P-value of less than .05 was considered statistically significant.
Results
Patient Demographics and Surgical Characteristics
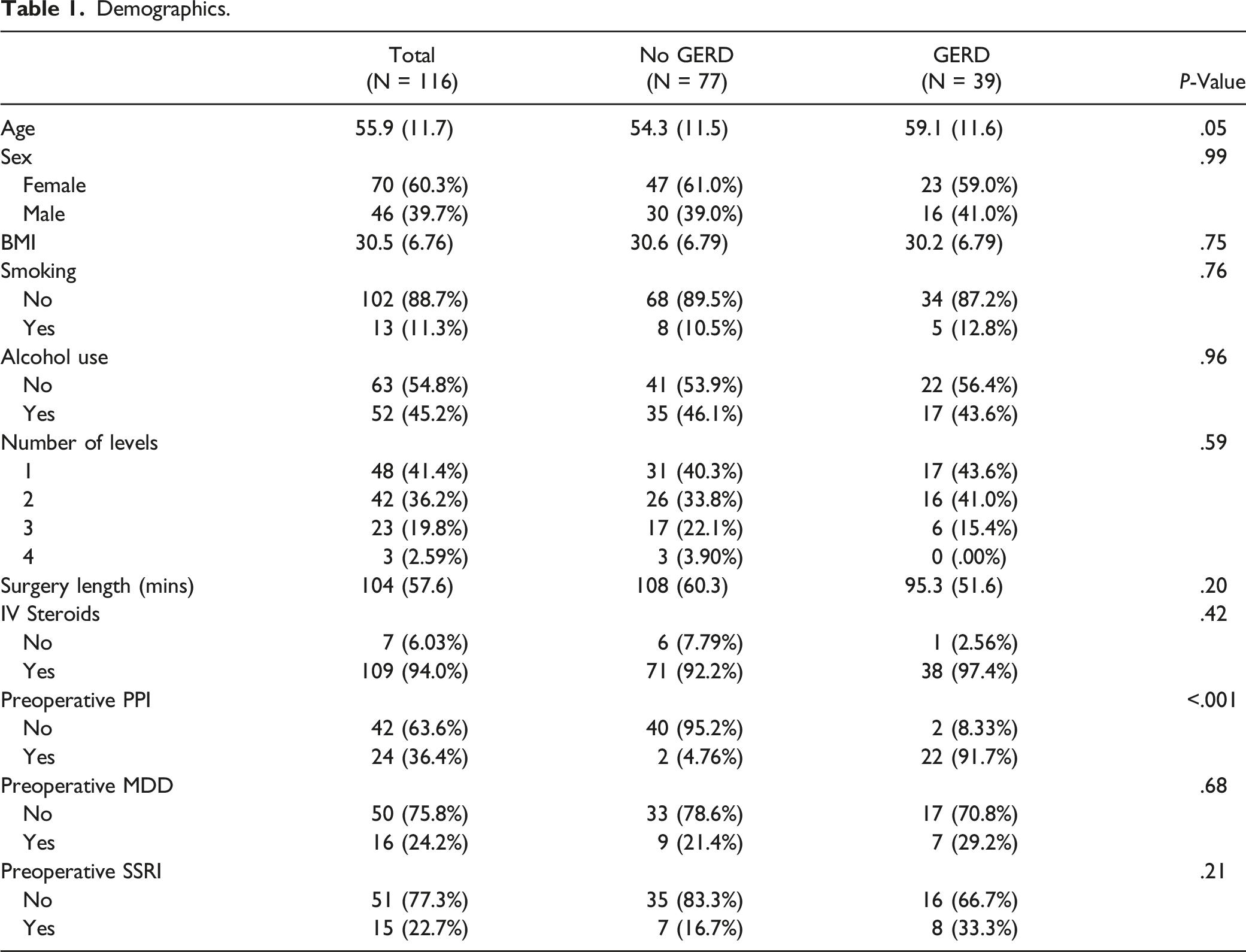
Demographics.
Dysphagia Outcomes
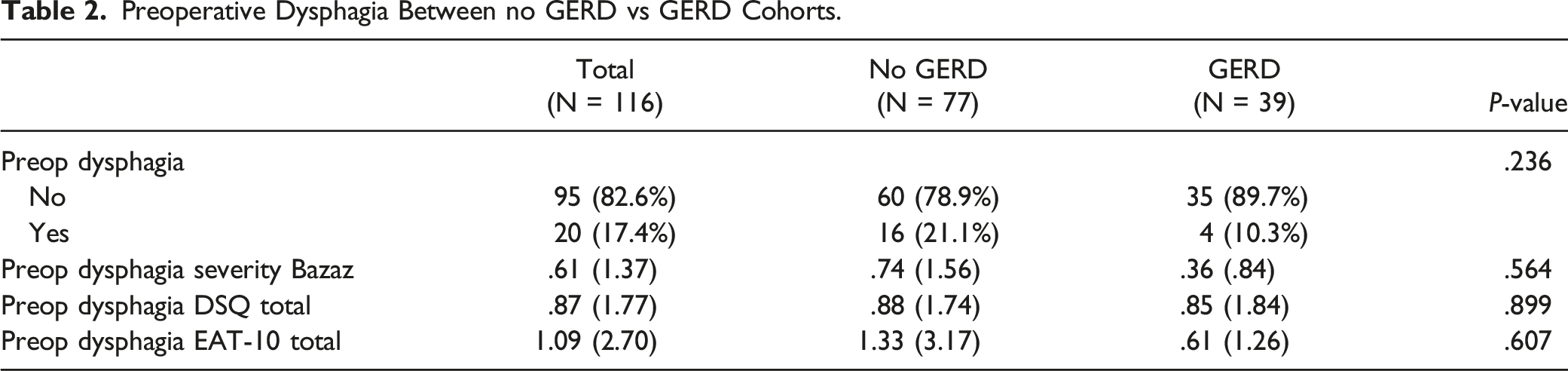
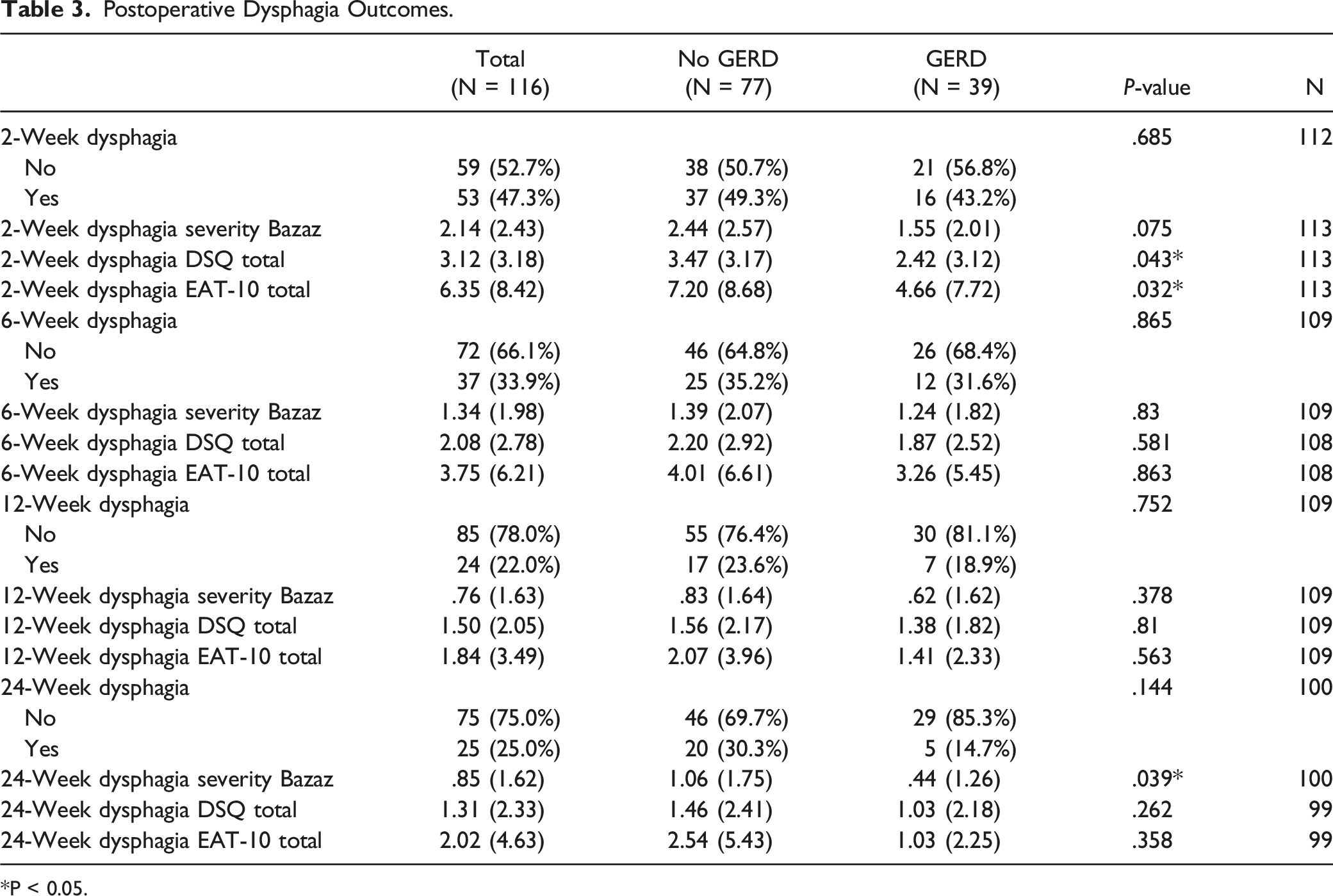
When evaluating for preoperative dysphagia, there were no significant differences in binary dysphagia status (10.3% vs 21.1%, P = .236) or continuous scores from the Bazaz (.36 ± .84 vs .74 ± 1.56, P = .564), DSQ (.85 ± 1.84 vs .88 ± 1.74, P = .899), and EAT-10 (.61 ± 1.26 vs 1.33 ± 3.17, P = .607) surveys (Table 2). Postoperatively, while there was no significant difference in the incidence of dysphagia on a binary analysis, patients with preoperative diagnosis of GERD had lower dysphagia severity scores on a continuous variable analysis in both the DSQ (2.42 ± 3.12 vs 3.47 ± 3.17, P = .043) and EAT-10 (4.66 ± 7.72 vs 7.20 ± 8.68, P = .032) surveys at 2-week follow-up in addition to the Bazaz survey (.44 ± 1.26 vs 1.06 ± 1.75, P = .039) at 24-week follow-up (Figure 1 and Table 3). Postoperative dysphagia scores over a 24 week period between cohorts with and without preoperative GERD. Preoperative Dysphagia Between no GERD vs GERD Cohorts. Postoperative Dysphagia Outcomes. *P < 0.05.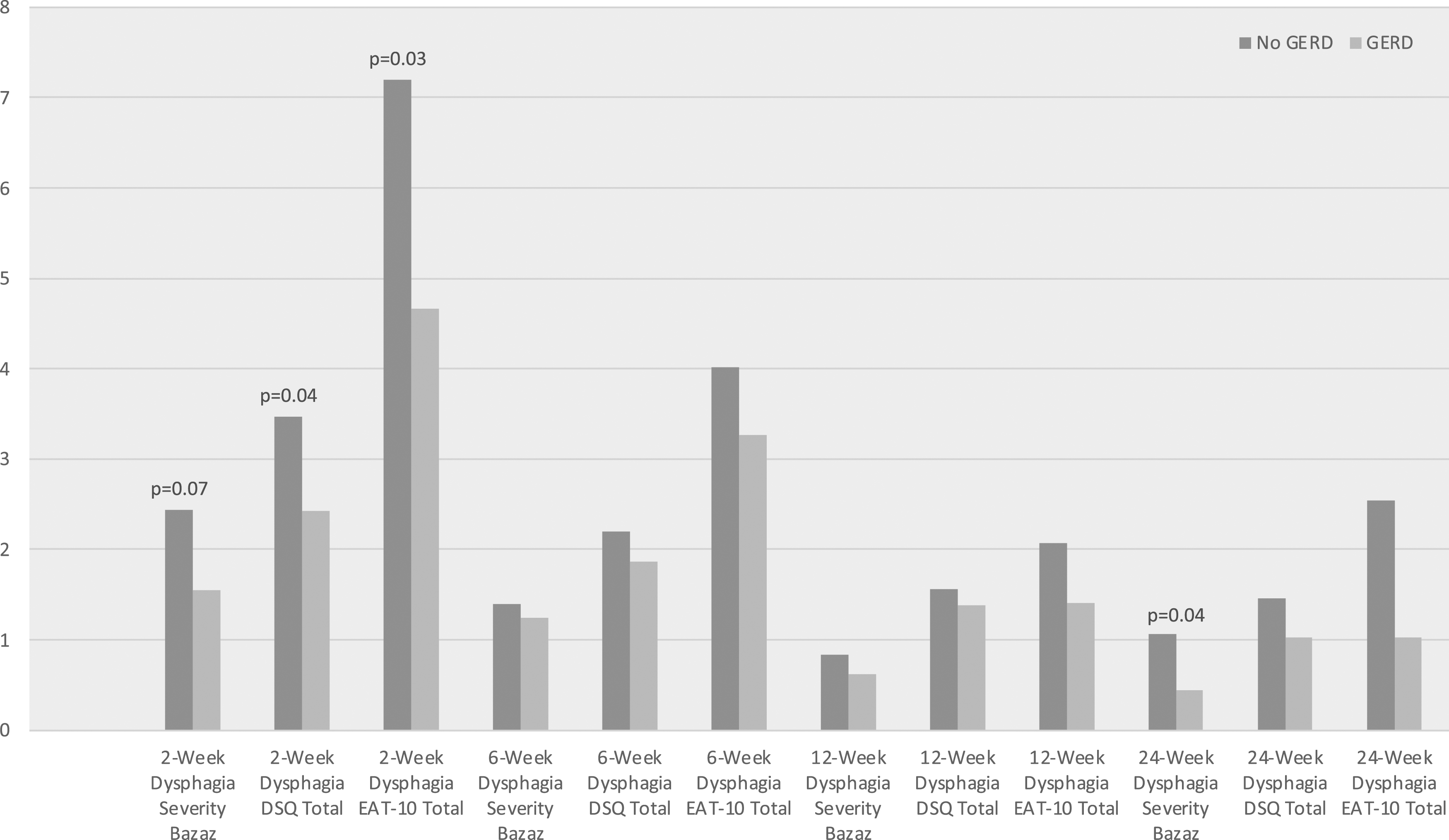
Discussion
Dysphagia is a common postoperative issue following anterior cervical spine surgery. 10 While it is difficult to assess due to a l ack of standardized and universally accepted tools for measuring this issue, current literature suggests that rates of dysphagia are as high as 71% in the early post-operative period.11,12 Despite this high rate, the risk factors for the development of dysphagia following ACDF are not well understood and remain an active area of investigation.
While the inherent nature of anterior cervical spine surgery, especially that done via the Smith Robinson approach, places anatomic structures including the esophagus and recurrent laryngeal nerve at risk for injury, it is unclear whether this iatrogenic stress is at fault for this common complication.13,14 In a 2010 systematic review regarding postoperative dysphagia following anterior cervical surgery, there was conflicting evidence on the degree to which number of operative levels in the cervical spine impacted the incidence of postoperative dysphagia. 15 Studies highlight number of operative levels as a risk factor for development of postoperative dysphagia possibly due to high esophageal retraction time and prolonged esophageal pressure.3,4,13,16 Due to these conflicting results on several iatrogenic risk factors, we wanted to further explore the possibility that preoperative non-iatrogenic pathology associated with the esophageal dysfunction may play a role in this postoperative complication.
Gastroesophageal reflux, like that of dysphagia, can be diagnosed and treated in multiple different manners.17-19 There are several risk factors for developing this pathology and again, like that of dysphagia, it is likely a multifactorial issue. 20 At the current time, there is no literature assessing the impact of this common preoperative pathology with that of dysphagia. Rihn et al looked at the impact of anterior cervical spine surgery on the development of postoperative GERD and determined that, relative to those patients undergoing lumbar spine surgery, patients undergoing ACDF developed GERD at a higher rate. 9 In our study, patients with and without a preoperative diagnosis of GERD had a similar postoperative incidence of dysphagia. With that being said, these two patient populations did not experience this postoperative issue to the same degree. In fact, having a preoperative diagnosis of GERD seemed to be protective, from a severity standpoint, for the development of dysphagia. Our study found that the severity of dysphagia in this population was significantly decreased at the 2-weeks, as defined by DSQ and EAT-10, and at 24-weeks postoperative period, as defined by the Bazaz survey relative to those patients without a preoperative diagnosis of GERD. While the etiology of this finding is not clear, it may simply be a relative finding – in that, patients who deal with dysphagia or reflux at baseline may quantify their degree of dysphagia to a lesser degree than that of other patients. Esophageal pain and discomfort are believed to be due to complex interaction of peripheral and spinal nerves. A phenomenon known as esophageal sensitization has been theorized as one of the contributing factors to disorders such as GERD, in which a hypersensitive esophagus has a lowered threshold for symptom perception due to noxious triggers such as reflux events.21,22 GERD and ACDF have different mechanisms of damage, or noxious triggers, to the esophagus. A patient with a preoperative diagnosis of GERD may have an esophagus with increased chemo- and mechano-receptor sensitivity to acid perfusion but decreased sensitivity to other events such as trauma due to ACDF. Thus, for patients with a preoperative diagnosis of GERD, their subjective scores for dysphagia on the postoperative surveys would be lower than those without a preoperative diagnosis of GERD.
Current literature suggests that older patients are more prone to development of dysphagia in general as well as postoperatively.23,24 However, we found that older patients who had preoperative diagnosis of GERD were not more likely to develop postoperative dysphagia, which further supports the conclusion that there is no significant effect between preoperative diagnosis of GERD and incidence of dysphagia after ACDF.
There are several limitations associated with this study design. One major limitation is the lack of objective measurement of GERD in the study patients. Objective measures, such as esophageal pH monitoring or manometry, would provide a more accurate assessment of both the incidence and severity of preoperative GERD and therefore its true impact on postoperative dysphagia. Additionally, while this was a prospective multicenter assessment, that relatively small patient population undoubtedly subjects our findings to a lack of generalizability. Lastly, inherent differences in the content of the three instruments used to determine dysphagia in the postoperative setting may also make the interpretation of our findings challenging. However, given the lack of a universally accepted and utilized tool for assessing this postoperative issue, we thought it prudent to employ the three most commonly tools.
Conclusion
Our study shows that having a preoperative diagnosis of GERD has no significant effect on the incidence of dysphagia following ACDF. Nevertheless, having a preoperative diagnosis of GERD does seem to provide some protective effect on the severity of dysphagia that this patient population develops at multiple intervals over a 24-week postoperative period.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
The authors and I have something to disclose.
IRB Statement
This study was approved by IRB approval number 18D.209.