
Abstract
Study Design
A retrospective database study of patients at an urban academic medical center undergoing an Anterior Cervical Discectomy and Fusion (ACDF) surgery between 2008 and 2019.
Objective
ACDF is one of the most common spinal procedures. Old age has been found to be a common risk factor for postoperative complications across a plethora of spine procedures. Little is known about how this risk changes among elderly cohorts such as the difference between elderly (60+) and octogenarian (80+) patients. This study seeks to analyze the disparate rates of complications following elective ACDF between patients aged 60-69 or 70-79 and 80+ at an urban academic medical center.
Methods
We identified patients who had undergone ACDF procedures using CPT codes 22,551, 22,552, and 22,554. Emergent procedures were excluded, and patients were subdivided on the basis of age. Then each cohort was propensity matched for univariate and univariate logistic regression analysis.
Results
The propensity matching resulted in 25 pairs in both the 70-79 and 80+ y.o. cohort comparison and 60-69 and 80+ y.o. cohort comparison. None of the cohorts differed significantly in demographic variables. Differences between elderly cohorts were less pronounced: the 80+ y.o. cohort experienced only significantly higher total direct cost (P = .03) compared to the 70-79 y.o. cohort and significantly longer operative time (P = .04) compared to the 60-69 y.o. cohort.
Conclusions
Octogenarian patients do not face much riskier outcomes following elective ACDF procedures than do younger elderly patients. Age alone should not be used to screen patients for ACDF.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is a surgical procedure used in the treatment of degenerative diseases of the cervical spine, enabling neural decompression, restoration of cervical lordosis, and improved spinal stability via solid osseous fusion. 1 ACDF was performed on average 1,37,000 times per year between 2006 and 2013, making it one of the most commonly performed spinal operations in the United States.2,3 Across that time period, the frequency of ACDF procedures increased from 1,20,617 in 2006 to 1,32,425 in 2013, an increase of 5.7%.2,3
A meta-analysis of ACDF complications found that while the mortality rate after ACDF is relatively low, the procedure was associated with a morbidity rate ranging from 13.2-19.3%.2,4-6 The complication rate of dysphagia specifically was found to be 1.7-67%.4,5,7,8 Additionally, Frempong-Boadu et al found dysphagia to be correlated with advanced age. 5 Similarly, Di Capua et al. found that patients over the age of 60 were twice as likely to experience a length of stay greater than 5 days, compared to their younger counterparts. 9 Additionally, they found that ACDF patients over 60 were more than 3 times as likely to experience pulmonary complications, significantly more likely to experience a venous thromboembolism, more than twice as likely to experience an UTI, more than 6 times as likely to experience cardiac complications, and more than 4 times as likely to develop sepsis. 9 These findings aligned with a similar study from Buerba et al finding increased complications in patients 65 and older, with patients over 75 significantly more likely to experience central nervous system complications and death. 10 Buerba et al did not find differences in complication rates between patients aged 18 to 39 and 40 to 64. 10 However, a separate study by Muzevic et al of 154 ACDF patients found no statistically significant difference in outcome by patient age using Odom’s criteria. 1
Much of the prior research on the age-dependent increase in risk associated with ACDF combines all “older” patients into a single group greater than the age of 60 or 65. There is a paucity of research looking more granularly at age-dependent risk between those who are in their 7th, 8th, and 9th decades of life. Many would agree that the average octogenarian has a different risk profile than someone who has recently retired at the relatively young age of 65. The aim of the present study is to analyze the disparate rates of complications following elective ACDF between patients aged 60-69 or 70-79 and 80+ at an urban academic medical center. The results should provide insight in identifying appropriate patient surgical selection and post-operative management.
Materials and Methods
Population
Patients from an urban academic medical center who underwent an ACDF surgery between 2008 and 2019 were included in the study, including patients with multilevel fusions, simultaneous foraminotomy, and myelopathy. These patients were identified through Current Procedural Terminology (CPT) codes 22,551, 22,552, and 22,554. The database was queried for these patients and those who had undergone cervical fusion with a posterior approach were excluded (CPT codes 22,600 and 22,614). Additionally, patients who were admitted due to emergent cases for infections, tumors, or fractures, identified through CPT codes 10,180, 22,325, 22,326, 22,327, 63,266, 63,267, 63,270, 63,275, and 63,276 were excluded from this study. CPT code definitions are specified in the supplement. 9 This was done to ensure all surgeries performed in this study were elective cases. 65 years of age was selected as a general cutoff for senior citizen status as delineated by Medicare guidelines. Patients who met both the inclusion and exclusion criteria were then also separated based on age into three cohorts: 60-69, 70-79, and 80+ years old. This study did not require IRB approval nor did it have an informed consent requirement.
Variables
Patient demographics such as age, sex, race, and body mass index (BMI) were collected as well as their American Society of Anesthesiologists (ASA) score. Patient comorbidities such as chronic pulmonary disease, complicated and uncomplicated diabetes, and liver disease were collected. Surgical outcomes such as 30- and 90-day readmissions, ICU stays, surgical times, length of stays, complication rates, and specific postoperative complications were collected and analyzed. Variables in this study labeled as “outlier” are defined as variables that were greater than the 75th percentile of the entire study population.
Propensity Score Matching
Analysis was performed comparing outcomes between patients in the 60 vs 80 year old cohort and the 70 vs 80 year old cohort. Before analysis, the patients within each cohort pair were matched based on their ASA status, gender, and race. A logistic regression model was used to generate matching scores and the patients were then subsequently matched through a nearest neighbors algorithm using a caliper of 0.01. The matching was completed by using the R MatchIt (v 4.0.0) package. 10
In the analyses, if the total number of patients in the paired cohort was not equal to the maximum number of patients of the smaller individual cohort, it was because the patients who were not included did not have an appropriately matched patient in the other cohort.
Statistical Analysis
The analysis of these variables were performed in Python 2.7.17, using the statsmodel API. 11 Chi-square testing was utilized for the analysis of categorical variables and student’s t-tests were used for the analysis of continuous variables. Univariate logistic regression was used to compare odds of outcomes between age groups. Outcomes were not included in regression if there were no positive instances in either group.
Results
Following the inclusion and exclusion criteria, 2262 patients were identified to have undergone ACDF surgery within the time period at this hospital. There were 25 patients in the 80+ cohort, 154 in the 70s cohort, and 409 in the 60s cohort.
60s vs 80s
Patients in their 60s were propensity matched and compared to patients in the 80s. After propensity matching, 50 patients were included (25 from each cohort) in this analysis. The two groups did not significantly differ in terms of gender (P = 1.00), ASA status (P = 1.00), race (P = 1.00), Elixhauser Comorbidity Index (P = .93), preoperative diagnosis (P = .06), or other comorbidities such as complicated or uncomplicated hypertension (P = 1.00, 1.00), complicated or uncomplicated diabetes (P = .35, .75), congestive heart failure (P = 1.00), or chronic pulmonary disease (P = .35).
Univariate Analysis of Patients in Their 60s vs 80s.
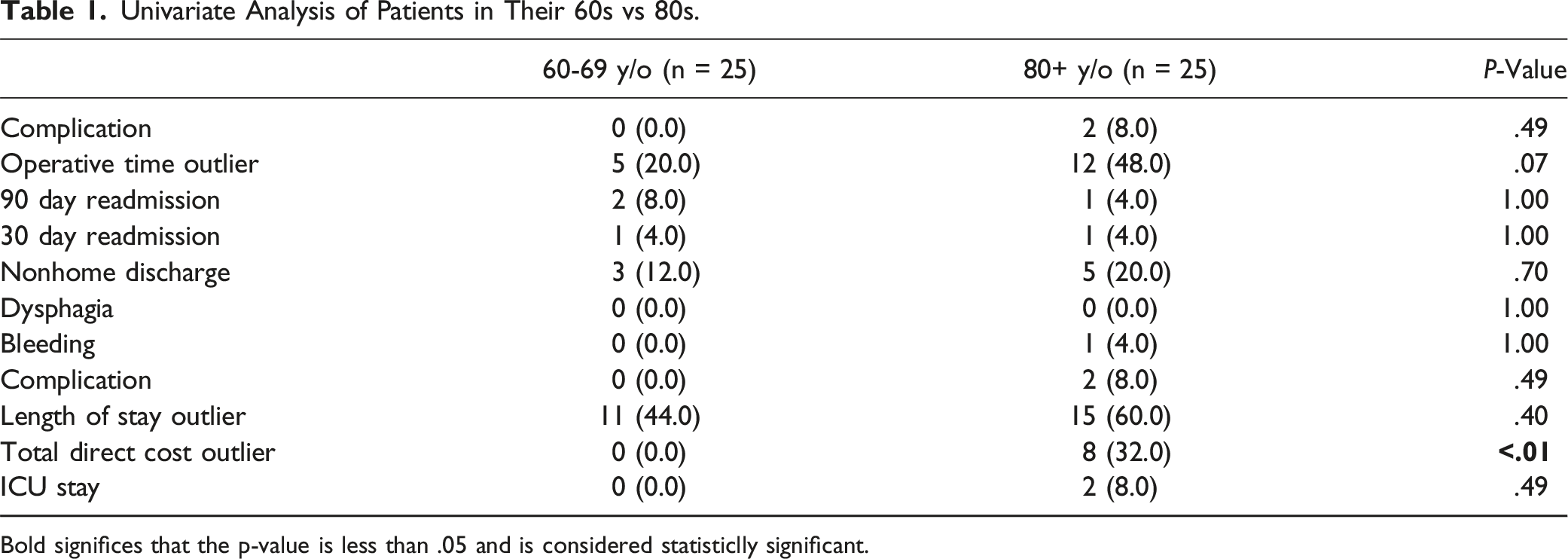
Bold significes that the p-value is less than .05 and is considered statisticlly significant.
Univariate Logistic Regression of Patients in Their 60s vs 80s.
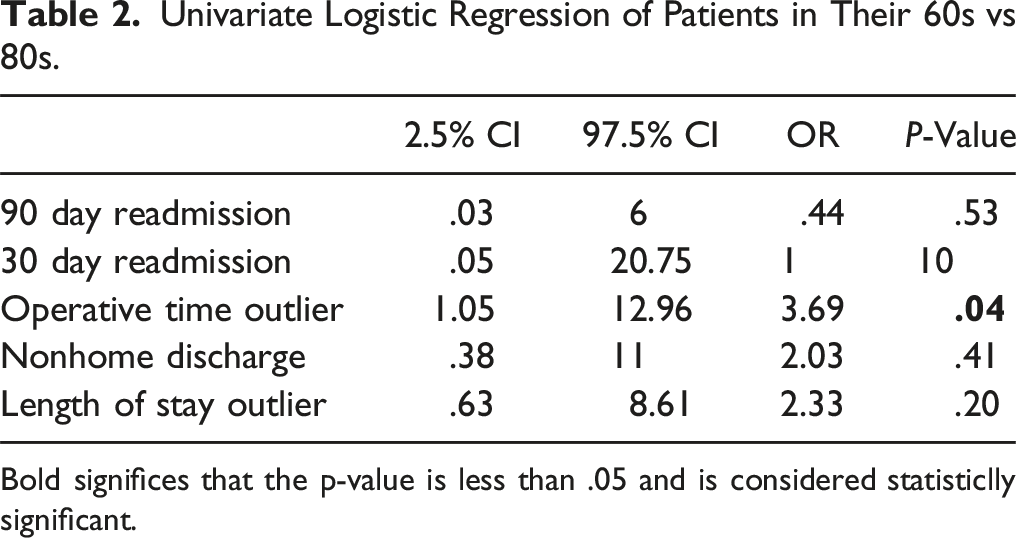
Bold significes that the p-value is less than .05 and is considered statisticlly significant.
70s vs 80s
Patients in their 70s were propensity matched and compared to patients in the 80s. After propensity matching, 50 patients were included (25 from each cohort) in this analysis. The two groups did not significantly differ in terms of gender (P = 1.00), ASA status (P = 1.00), race (P = 1.00), Elixhauser Comorbidity Index (P = .35), preoperative diagnosis (P = .56), or other comorbidities such as complicated or uncomplicated hypertension (P = .35, .78), complicated or uncomplicated diabetes (P = 1.00, .25), congestive heart failure (P = 1.00), or chronic pulmonary disease (P = .61).
Univariate Analysis of Patients in Their 70s vs. 80s.
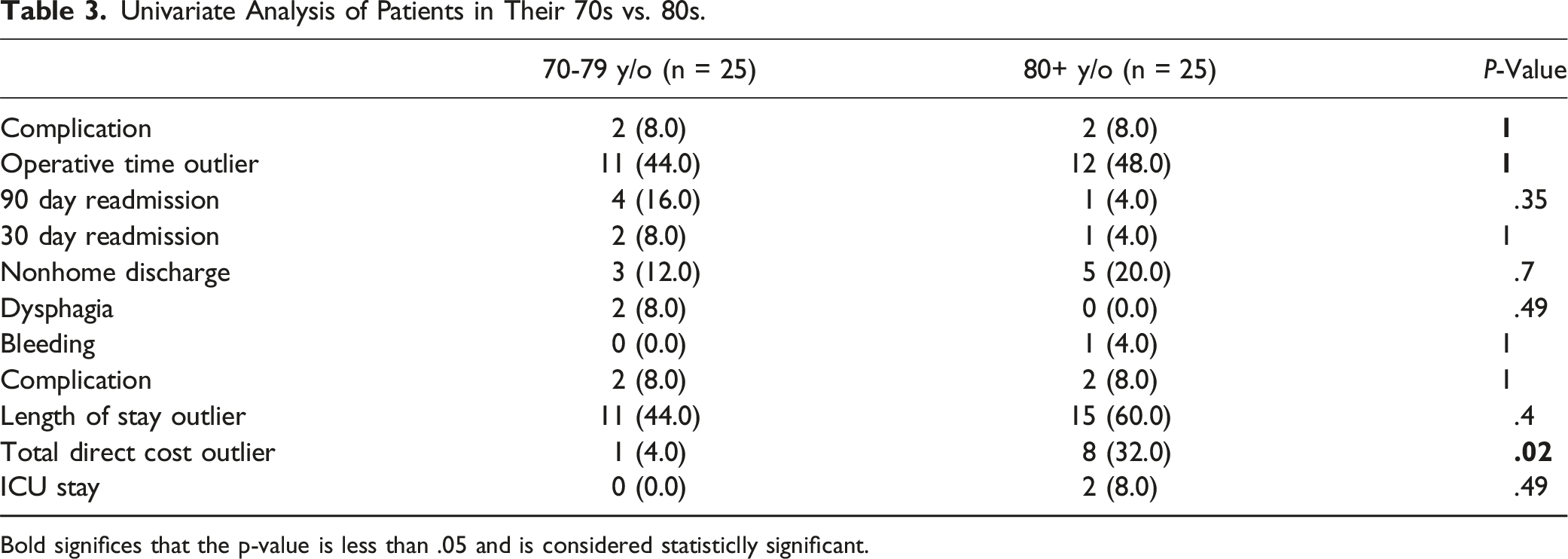
Bold significes that the p-value is less than .05 and is considered statisticlly significant.
Univariate Logistic Regression of Patients in Their 70s vs 80s.
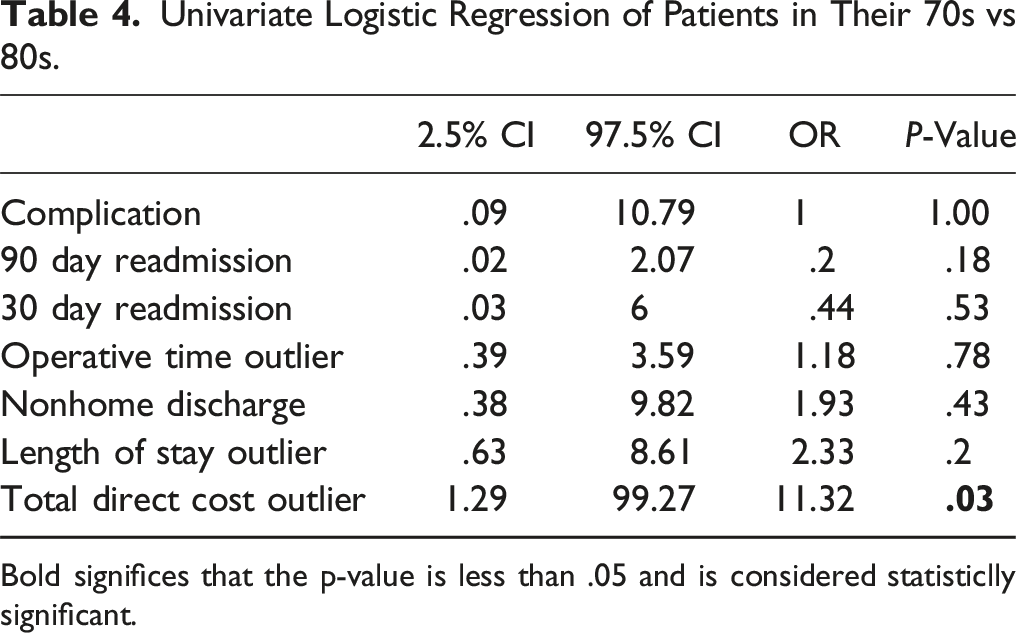
Bold significes that the p-value is less than .05 and is considered statisticlly significant.
Discussion
While ACDF is a well-tolerated procedure with rare complications, age has been shown to be a risk factor for complications and readmission following ACDF surgery.12-14 As the United States population continues to age, older patients are undergoing spine surgery at a higher rate than in past years. 15 Generally, “elderly age” has been defined as those older than 65, and studies have tended to broadly group these patients together. However, with improved medical advances, more patients now live far longer, such that 65 may be even considered “young-old. 16 ” Many patients in their 60s and early 70s still demonstrate high baseline functioning, whereas those in their 80s may see a marked increase in frailty. 16 Studies have sub-grouped elderly patients into young-old (∼65-74), middle-old (∼75-84), and oldest-old (∼85+).16,17 Thus, a more granular analysis is needed across the elderly age spectrum in ACDF. To our knowledge, this is the first study to perform a propensity score matched analysis of outcomes following ACDF across sub-groups of elderly patients.
60-69 vs 80+ and 70-79 vs 80+
Degenerative spinal pathology adheres to an age-dependent distribution.18-22 With medical and healthcare advances as well as the rise in life expectancy, the age of patients with cervical spondylotic myelopathy (CSM) will likely increase. 23 Naturally, it is not unlikely that the number of octogenarian and nonagenarian patients seeking ACDF will increase as well. Current literature focused on the octogenarian age group is limited. As the prevalence of octogenarians seeking spinal surgery increases, it is important to investigate preoperative risk counseling and postoperative considerations unique to the age group. In a retrospective cohort study studying elective ACDF octogenarian patients, Elsamadicy et al determined that the 80+ cohort experienced significantly longer hospital stays, complications, and non-routine discharge than 50-64 and 65-79 cohorts. 24 Similarly, in comparing fusion and/or decompression patients aged 20-79 with an octogenarian and nonagenarian cohort, Kumar et al reported a mean LOS difference of just over 1 day. 25 In contrast, Vonck et al found no significant difference in the odds of prolonged LOS, reoperation or readmission when comparing octogenarian CSM patients receiving posterior cervical fusion with patients aged 60-69 and 70-79. 23 However, octogenarians were more likely to experience non-home discharge. 23 In our propensity matched analysis, octogenarians fared similarly relative to the 60-69 and 70-79 cohorts in terms of complications and resource utilization. Relative to the 70-79 cohort, only cost was significantly higher among octogenarians, which one would expect to be positively correlated with LOS or dysphagia, the prevailing complication post-ACDF. Joseph et al reported patients who experienced post-ACDF dysphagia paid $21,245 compared to non-dysphagia patients who paid $13,099. 26 It is peculiar that we observe a cost disparity between the age 70-79 cohort and the octogenarian cohort without any observable difference in LOS or dysphagia, a common and costly complication seen in ACDF patients. It is well-observed in the current literature that patients older than 65 incur higher hospitalization costs due to complications and comorbidities.25,27 However, after matching by comorbidity burden, higher costs are still evident in the octogenarian cohort. Cost differences between octogenarians and septuagenarians may therefore be due to other factors not captured in this study, such as insurance reimbursement or social needs, highlighting this as an area of further investigation. Relative to the 60-69 cohort, only cost and operative times were higher among octogenarians. It is likely that higher costs are attributable to greater operative times in this specific subgroup comparison, although this was not evident when comparing octogenarians and septuagenarians. Operative times in the elderly population may be higher owing to greater degenerative disease or perhaps more careful measures taken during the procedure. Longer operative times have been associated with adverse outcomes following ACDF, though this was not borne out in our analysis. 28
It is interesting that octogenarians tended to have better outcomes than septuagenarians relative to the 60s cohort. The authors’ hypothesize that the octogenarian cohort may undergo greater preoperative optimization and selection in comparison to the septuagenarian cohort. This is evidenced by the fact that only 25 patients were at least 80 years old across the 25 years in this study (1.1% of study population). Surgeons may use less rigorous preoperative screening in younger populations. Thus, the octogenarians in this study may represent a highly selective group of healthy surgical candidates. At the institution in this study, patient selection does not follow specific criteria and rather relies on risk stratification based on input from primary care physicians, anesthesiology, and cardiology. Patients’ baseline functional status and ambulatory ability are also considered. Differences in preoperative diagnosis between sexagenarians and octogenarians trended towards significance (P = .06), supporting the theory that surgeons may be more selective in terms of both disease and patient characteristics for octogenarian surgical candidates. Regardless, our propensity matched comparison still ensures a degree of equivalency between groups. This suggests that in a select cohort of octogenarians ACDF is a safe procedure with comparable outcomes to the younger end of the elderly spectrum. Spine surgeons, therefore, should not exclusively screen out potential candidates for ACDF on the basis of age alone. However, the low sample size of our octogenarian cohort should also be considered and may limit detection of any significant differences.
Limitations
This study is not without limitations. Our dataset is derived from a single urban hospital system and may not generalize well to different demographic populations. Moreover, our dataset lacked a large sample size for patients who were 80 or older which may have confounded our results. The nature of performing a retrospective analysis introduces inherent biases with regard to the processes of patient data collection, selection bias, and outcome reporting.
Conclusion
This propensity score matched analysis compared outcomes following elective ACDF across sub-groups of elderly patients. Octogenarians fared similarly in comparison to younger age groups, likely reflective of higher preoperative selectivity. Age alone should not be used as an exclusive screening tool, as select patients at the older end of the elderly demographic may experience comparable outcomes to younger patients.
Supplemental Material
Supplemental Material - An 11-Year-Long Analysis of the Risks Associated with With Age in Patients Undergoing Anterior Cervical Discectomy and Fusion in a Large, Urban Academic Hospital
Supplemental Material for An 11-Year-Long Analysis of the Risks Associated with With Age in Patients Undergoing Anterior Cervical Discectomy and Fusion in a Large, Urban Academic Hospital by Justin Tang, Jonathan S. Gal, Eric Geng, Akiro Duey, Pierce Ferriter, Ryan Sicard, Bashar Zaidat, Steven Girdler, Hannah Rhee, Ivan Zapolsky, Paul Al-attar, Jonathan Markowitz, Jun Kim, and Samuel Cho in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.