
Abstract
Study Design
Retrospective study.
Objectives
To determine prevalence and clinical importance of patients who had postoperative CM after CMIS for ASD correction.
Methods
We reviewed patients who underwent CMIS technique. Inclusion criteria were patients who were diagnosed with ASD, which is defined as having at least one of the following: coronal Cobb angle >20, SVA >50 mm, PI-LL >10, PT >20. They underwent >4 spinal levels fusion with CMIS technique and had at least 1-year follow-up. Preoperative and 1-year postoperative radiographs and clinical outcome measures (VAS, ODI, and SRS-22 scores) were used to make the comparisons.
Results
120 patients were included. Radiographic outcomes, including CVA, coronal Cobb angle, LSF curve, SVA, LL, and PI-LL, and clinical outcomes, were significantly improved postoperatively in each of the 3 preoperative subgroups (Bao type A, B, and C). At 1-year post-operation, 10 patients (12.4 %) of type A turned out to be CM, 4 patients (21.1%) of type B, and 8 patients (40%) of type C remained CM. Comparing coronally aligned (CA) to coronally mal-aligned patients at 1-year follow-up in each coronal subtype revealed that clinical and radiographic outcomes were comparable.
Conclusions
CMIS technique significantly improves radiographic and clinical outcomes for ASD patients. Incidence rates of postoperative CM were similar to open surgery. Type C patients were at risk of postoperative CM than types A and B. However, most 1-year outcomes were not significantly different between postoperative CA and CM patients regardless of the preoperative coronal alignment characteristics except ODI scores in type A.
Keywords
Introduction
The goals of adult spinal deformity (ASD) correction surgery are to improve clinical outcomes, such as pain, daily function, and quality of life, and to restore optimal regional and global alignments.1,2 Recently, postoperative coronal malalignment (CM), which is a sequela after surgical correction for ASD, has gained attention. This complication can occur up to 40% after this complex surgery, including both the residual CM (under-correction of the preoperative CM), and newly (iatrogenic) postoperative CM.1,3,4 Ploumis et al. found that postoperative CM occurred in 20.4% of the ASD patients who underwent long posterior spinal fusion (PSF) and the incidence increased in the long-term follow-up. 5
Several authors reported unsatisfactory outcomes and increased complications in patients who had postoperative CM.4,6,7 Bao et al. classified the preoperative coronal alignment subtypes based on the coronal balance distance (CBD), defined as the horizontal distance between the central sacral vertebral line (CSVL) and the C7 plumb line (C7PL): (1) Type A: CBD <3 centimeters (cm); (2) type B: CBD >3 cm and shifted toward the concavity; and (3) type C: CBD >3 cm and shifted toward the convexity. The authors treated patients with degenerative scoliosis (DS) using posterior spinal osteotomies and reported that type C patients might have a greater risk of postoperative CM and worse clinical outcomes. Zhang et al. also found that type C may be a predictor for postoperative CM in patients with ASD who underwent long PSF and osteotomy. 3 In patients with severe preoperative global coronal malalignment, Buell et al. showed that those who had residual postoperative CM >3 cm were associated with worse results. 7
With the recent advancement in minimally invasive surgery (MIS), several MIS techniques were proposed and utilized in ASD correction surgery.9,10 Lateral lumbar interbody fusion (LLIF) is an alternative surgical technique used for treating patients with ASD.11,12 The minimally invasive nature of the LLIF procedure offers less soft tissue trauma, less bleeding, and shortened length of hospital stays compared to the open posterior approach.13-15 In addition, several studies demonstrated that LLIF could improve clinical outcomes and effectively restore the sagittal and coronal alignment in ASD patients.2,11,16 Anand et al incorporated the LLIF technique as a part of circumferential minimally invasive surgery (CMIS) of the spine and reported promising outcomes following ASD correction surgery even in severe deformity patients.10,12
However, data regarding the prevalence and clinical impact of postoperative CM following the CMIS technique for ASD surgery is underreported. Walker et al utilized CMIS for 42 degenerative scoliosis patients and reported promising results regarding clinical outcomes and coronal alignment correction. However, the authors found that type C patients were the most troublesome to treat coronally, and the type C patients, who had postoperative CM, had worse back pain scores at 1-year follow-up. 6 In this study, we aimed to determine the prevalence and clinical impact of postoperative CM following the CMIS technique for ASD surgery.
Materials and Methods
Subjects
The Institution Review Board of the Cedars-Sinai Medical Center approved this study (IRB No. 642/23) and the consent form was waived. We reviewed our prospectively collected data registry of 312 ASD patients who underwent the CMIS technique from January 2011 to September 2022 at a single institution. The inclusion criteria were the patients, over 18 years old, who was diagnosed with ASD, which is defined as having at least one of the following: coronal Cobb angle >20°, SVA >50 millimeters (mm), pelvic incidence/lumbar lordosis (PI/LL) mismatch >10°, pelvic tilt (PT) > 20°, In addition, the patients were being fused at least 4 spinal levels with CMIS technique and had at least 1-year of follow-up. The exclusion criteria were the patients who underwent posterior open spinal surgery or had evidence of spinal trauma, tumor, or infection. All surgeries were performed either in one-stage or two-stage by the senior author (NA). The details of surgical techniques were already described in previous studies.10,12 In short, the oblique lateral interbody fusion (OLIF) was performed at the appropriate spinal levels from L1/2 to L4/5 in the right lateral decubitus position with or without anterior lumbar interbody fusion (ALIF) at the L5/S1 level in the same patient’s position. The percutaneous pedicle screws fixation and additional spinal deformity correction by using rod contouring and translation without any posterior osteotomies were subsequently performed in the prone position either in the same setting together with the interbody fusion procedure or in the staged procedure.
All patients were classified into 3 subgroups according to the characteristics of preoperative CBD described by Bao et al
8
: (1) Type A: CBD <3 cm; (2) type B: CBD >3 cm and shifted toward the concavity of the main curve; and (3) type C: CBD >3 cm and shifted toward the convexity of the main curve. Type A was defined as preoperative coronally aligned (CA), and types B and C were defined as preoperative CM patients. Also, at 1 year post-operation, the patients in each subgroup were further categorized into 2 groups according to the postoperative coronal alignment status: (1) postoperative CA (CBD < 3 cm); and (2) postoperative CM (CBD > 3 cm) (Figure 1). Preoperative whole spine anteroposterior standing radiographs of each preoperative coronal alignment type and subsequent 1-year post-operation showing the postoperative CM after CMIS: (A) type A; (B) type B; and (C) type C. The white line designates the C7PL and the yellow line indicates the CSVL.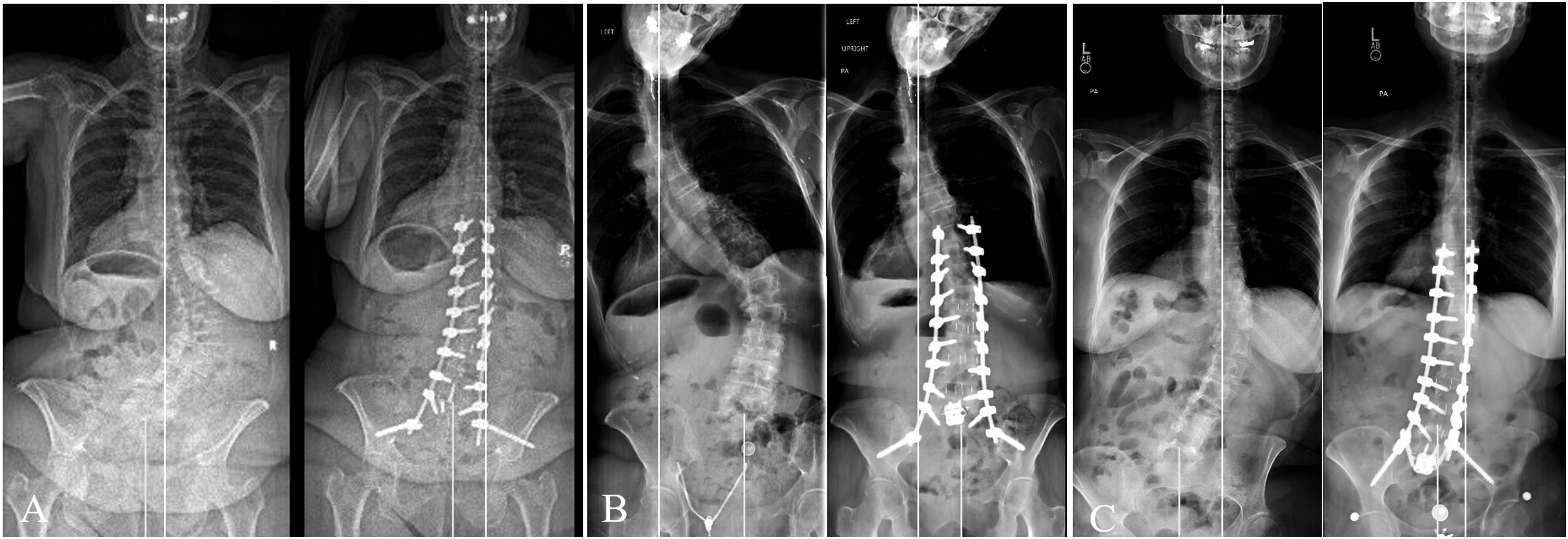
Outcomes Assessments
The demographic data, including age, sex, preoperative body mass index (BMI), and history of previous lumbar spinal surgery were collected. The pertinent operative variables, including total instrumented levels, location of the upper instrumented vertebra (UIV), location of the lower instrumented vertebra (LIV), number of spinal levels being fused, and length of stays (LOS), were also recorded.
The studied clinical parameters were preoperative and 1-year postoperative Visual Analog Scale (VAS), Oswestry Disability Index (ODI), and Scoliosis Research Society-22 (SRS-22) scores.
The standing full-length 36-inch anteroposterior (AP) and lateral radiographs were assessed in all patients preoperatively and at 1-year post-operation. The following radiographic parameters were measured: (1) CBD: the distance between the C7PL and the CSVL; (2) maximum Cobb angle: the preoperative maximum coronal angle of the following 3 curves: thoracolumbar, main thoracic, or proximal thoracic curve; (3) maximum Cobb angle correction: the value of the 1-year postoperative minus the preoperative maximum Cobb angle; (4) lumbosacral fractional (LSF) curve: the coronal angle between the superior endplate of the sacrum and the superior endplate of either L4 or L5 depending on alignment; (5) pelvic obliquity (PO): the angle subtended by the horizontal line and the line drawn across the most superior points of both iliac crests; (6) lumbar lordosis (LL); (7) thoracic kyphosis (TK); (8) pelvic incidence (PI); (9) PI/LL; 10) pelvic tilt (PT); 11) sacral slope (SS); and 12) sagittal vertical axis (SVA). All radiographic parameters were measured by two spine surgeons using Surgimap Spine software (version 2.4.1.3; Nemaris, Inc, Methuen, MA, USA).
Statistical Analysis
Continuous and categorical variables were analyzed by using t test and chi-squared analysis, respectively. Data analyses were conducted using STATA version 15 (StataCorp. 2017. Stata Statistical Software Release 15. StataCorp LLC, College Station, TX.). A P-value <0.5 was considered a statistically significant difference.
Results
Demographic and Operative Data.
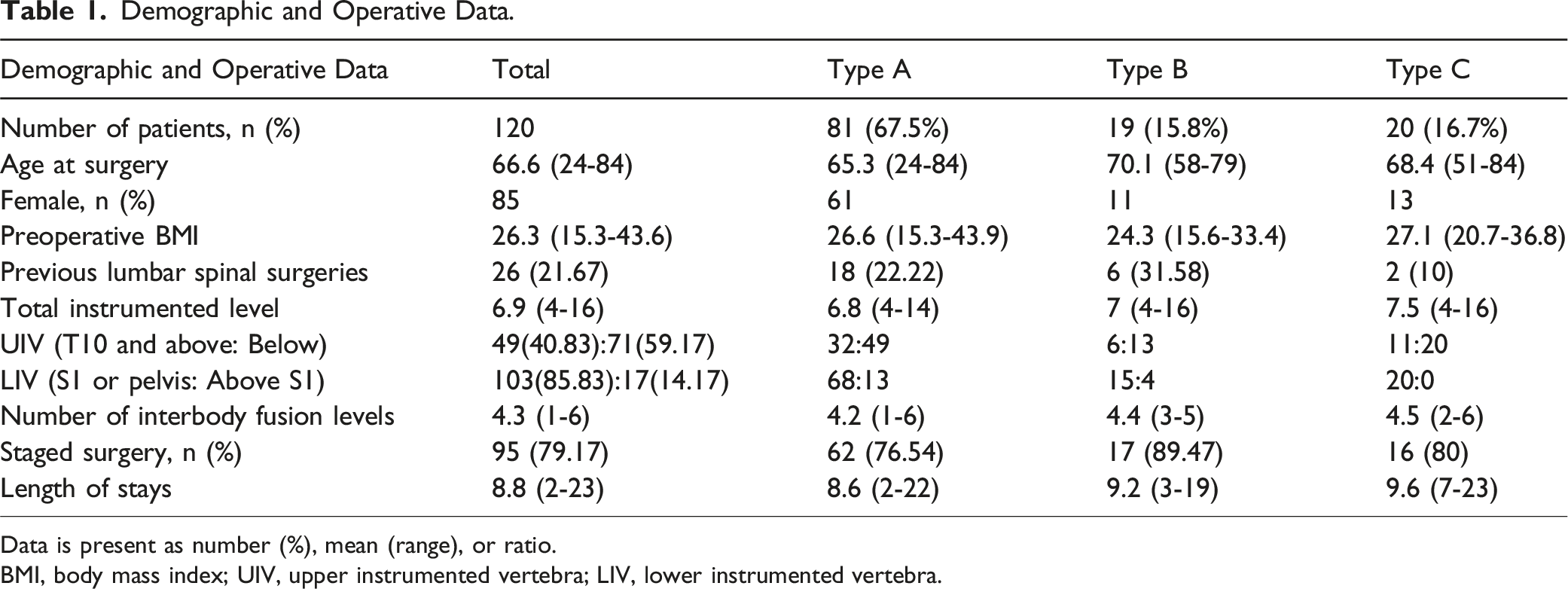
Data is present as number (%), mean (range), or ratio.
BMI, body mass index; UIV, upper instrumented vertebra; LIV, lower instrumented vertebra.
Preoperative and 1-Year Postoperative Clinical and Radiographic Outcomes of Each Coronal Alignment Subtype.
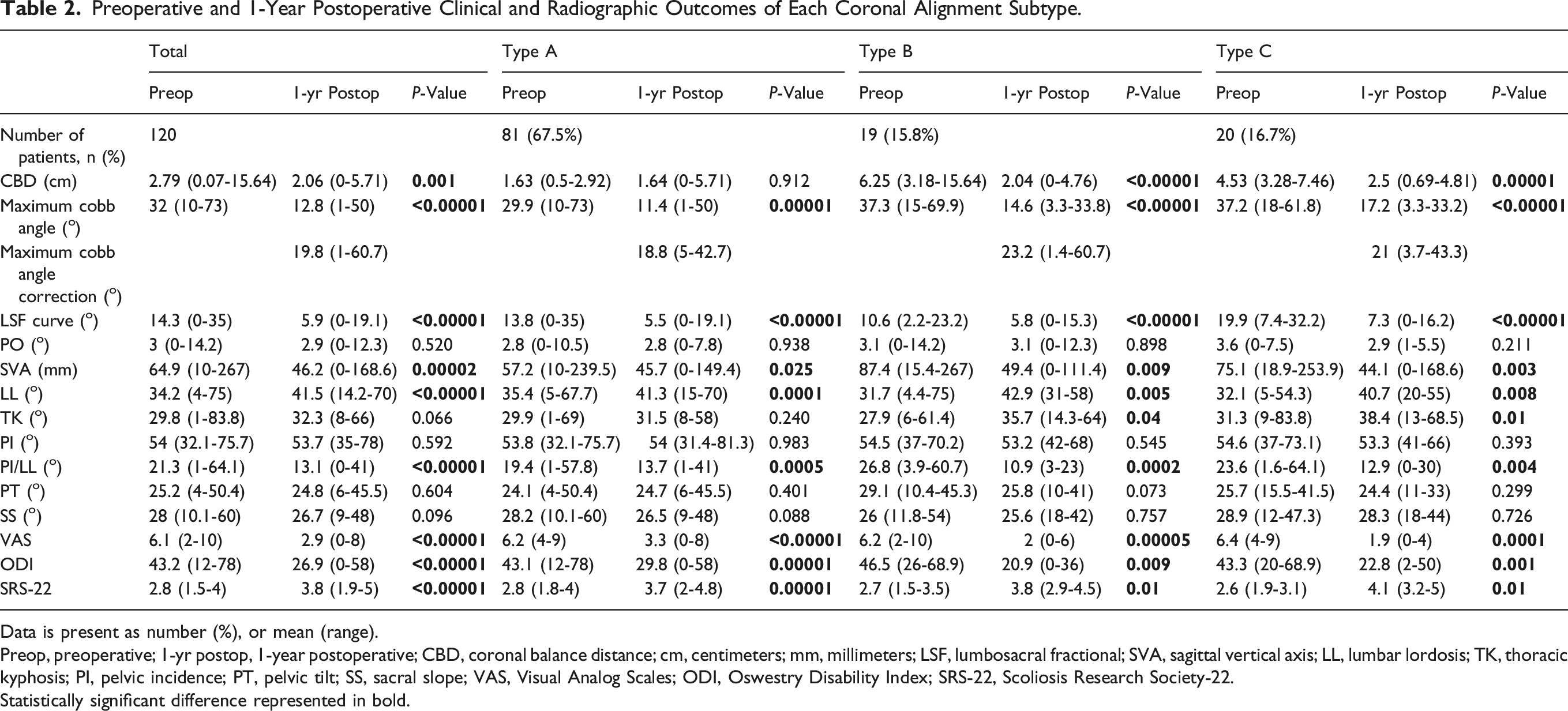
Data is present as number (%), or mean (range).
Preop, preoperative; 1-yr postop, 1-year postoperative; CBD, coronal balance distance; cm, centimeters; mm, millimeters; LSF, lumbosacral fractional; SVA, sagittal vertical axis; LL, lumbar lordosis; TK, thoracic kyphosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; VAS, Visual Analog Scales; ODI, Oswestry Disability Index; SRS-22, Scoliosis Research Society-22.
Statistically significant difference represented in bold.
The CBD was still maintained in type A patients and was significantly improved in type B and C patients from preoperative to 1-year postoperative period. The maximum Cobb angle was significantly improved in all subgroups with the maximum Cobb angle correction of 18.8 (5-42.7), 23.2 (1.4-60.7), and 21 (3.7-43.3) in types A, B, and C, respectively. The LSF curve was also significantly improved in all 3 subgroups. The PO was not significantly changed in all subgroups. The sagittal parameters, including SVA, LL, and PI/LL were significantly improved in all subgroups. The TK was significantly improved in type B and C patients, but still maintained in type A patients. The PI, PT, and SS were comparable between the preoperative and 1-year postoperative period in all subgroups.
1-Year Postoperative Clinical and Radiographic Outcomes of Patients in Each Coronal Alignment Subtype, Which was Sub-categorized Into the Postoperative CA and CM Subgroups.
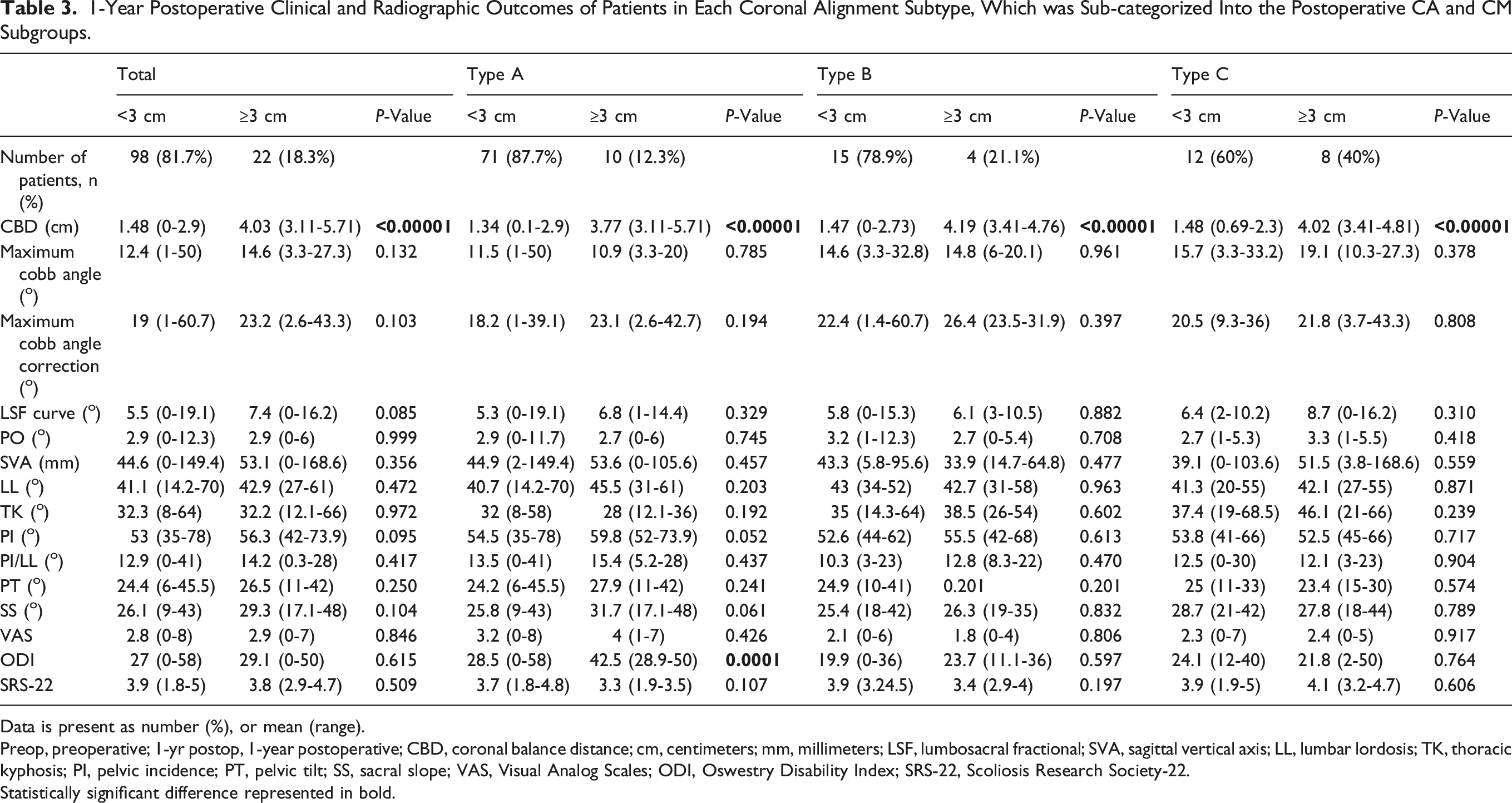
Data is present as number (%), or mean (range).
Preop, preoperative; 1-yr postop, 1-year postoperative; CBD, coronal balance distance; cm, centimeters; mm, millimeters; LSF, lumbosacral fractional; SVA, sagittal vertical axis; LL, lumbar lordosis; TK, thoracic kyphosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; VAS, Visual Analog Scales; ODI, Oswestry Disability Index; SRS-22, Scoliosis Research Society-22.
Statistically significant difference represented in bold.
Regarding type A patients, at 1-year post-operation, the VAS and SRS-22 scores were comparable between the postoperative CA and CM subgroups, but the ODI scores were significantly lower in the postoperative CA subgroup compared to the postoperative CM subgroup. All radiographic parameters were similar between the postoperative CA and CM subgroups.
For type B and C patients, at 1-year post-operation, all the PROs and radiographic parameters were comparable between postoperative CA and CM subgroups.
Discussion
The management of patients with ASD remains a challenging issue and postoperative CM is not an uncommon complication that occurs following ASD correction surgery. 1 This sequela can be found in up to 40% following open techniques and the incidence tends to increase over time.3,5,8,17,18 In addition, Walker et al. reported 14.3% incidence rates of postoperative CM following CMIS for ASD correction. 6 Our study found a total of 18.3% (22/120 patients) postoperative CM at 1 year after the CMIS technique which was in the range of previous studies.5,6,8,19 These findings implied that postoperative CM still occurred following CMIS with LLIF techniques for ASD surgery at similar rates to those patients who underwent open techniques.
Numerous predictors were reported to be associated with postoperative CM with preoperative type C being one of the strongest risk factors.1,3,8,19,20 We found similar results, in which postoperative CM occurred in type C (40%) more than in type B (21.1%), and type A (12.3%). Bao et al. defined type C as the preoperative trunk shifts toward the convexity of the coronal curve and reported that the C type was at risk of worsening the CM toward the convexity especially when surgeons focused on straightening the main coronal curve and paid less attention to correct the LSF curve. Obeid et al. also suggested that the deformity correction should be at the LSF curve for convex CM instead of focusing on correction at the apex of the main coronal curve like in concave CM. 21 Tanaka et al. found in their study that the LLIF was used more in the postoperative CM group than in those who had postoperative CA despite significant coronal correction gained by the LLIF. 17 The authors explained that the ALIF at L5/S1 was not used in their study so the L5 coronal tilt remained resulting in the coronal malalignment from an oblique foundation. This result emphasized the importance of correcting the fractional curve.
New onset or iatrogenic CM can also be found following ASD correction surgery in patients with preoperative coronally aligned, ranging from 9%–31% when using open techniques.3,5,8,19 Zuckerman et al. reported 9% of new-onset CM following ASD surgery in preoperative CA patients with an average number of instrumented levels of 13.5 and 71% of pelvic fixation. 4 The authors found that type A patients with coronal curve patterns similar to those of type C patients had a greater risk of postoperative iatrogenic CM. They also reported that patients with increased PO were at risk for new-onset CM. However, we found different results. In our study, the PO was not affected by CMIS in any of the groups and was not significantly different between postoperative CA and CM groups in any subgroups. Obeid et al. stated that the compensatory LSF curve is frequently stiff and more difficult to correct than the main curve, especially in severe lumbar scoliosis. This may result in an unbalanced correction of the two curves and lead to CM in type A patients. 21 They suggested that surgeons should avoid overcorrection of the main lumbar curve and aggressively correct the LSF curve to avoid new-onset CM in preoperative CA patients. Our study found the postoperative CM rates in range with previous studies which was 12.3% (10/81 patients) of preoperative CA patients had new onset CM with a mean total instrumented level of 6.8 and 83.9% of S1 or pelvic fixation in this subgroup. The potential causes of postoperative CM following CMIS surgery in type A patients of this study could be an unbalanced correction of the main curve and the LSF curve or an under-correction of a stiff fractional curve especially in the patients who had coronal curve characteristics like those of type C. Interestingly, Walker et al. also performed CMIS with LLIF in their study and found 0% of iatrogenic postoperative CM in type A patients with an average fused spinal segment of 4.4 levels, and 42.3% of the patients underwent ALIF at L5/S1 level. 6 However, they included only 26 type A patients in their study.
Unlike open surgery, which uses surgical strategies, such as posterior column osteotomies, 3-column osteotomies, and compression/distraction techniques for correcting spinal deformity, the CMIS technique usually utilizes the anterior or lateral interbody cages as the main tool for correcting the deformity instead of bony works at the posterior elements. 1 Several studies demonstrated that the LLIF technique was an effective procedure for correcting spinal deformity including sagittal and coronal malalignment.2,6,11 Walker et al. reported improved overall coronal alignment and curve magnitudes in degenerative scoliosis patients who underwent CMIS surgery. 6 Chou et al. found that the CMIS technique effectively corrected the fractional curve in the coronal plane similar to the traditional open surgery. 22 Anand et al. also showed that multi-level CMIS surgery significantly improved the coronal and sagittal alignment and functional outcomes even in severe ASD patients. 12 The LLIF provides the benefit of a large interbody spacer, which is powerful for disc height restoration and correction of segmental spinal deformity. In addition, the use of percutaneous screw extenders with large extender windows can enhance the abilities of rod manipulation and further correct the spinal deformity including the main curve and fractional curve during the posterior fixation step. 10
This study demonstrated that both the main curve and fractional curve were significantly corrected by using the CMIS technique in overall and each group of patients. However, the postoperative main curve and LSF curve were not significantly different between postoperative CA and CM groups regardless of the preoperative coronal alignment pattern. This result was in contrast with other studies that demonstrated the impact of coronal tilt on the coronal balance. Walker et al. reported a total of 11 type C patients and found that the patients who had persistent CM post-operation had higher postoperative L4 tilt angles than those who realigned. 6 Tanaka et al. showed that preoperative coronal balance and L5 coronal tilt angle were significantly correlated with postoperative CM. 17 Lewis et al. also found that both L4 and L5 coronal tilt angles were higher in the imbalanced than in the balanced group. 20
Regarding the clinical importance of postoperative CM, we found that all the 1-year postoperative PROs, including VAS, ODI, and SRS-22 scores, were comparable between the postoperative CA and CM patients in all subgroups except the ODI scores of type A patients, in which the CA group had significantly better scores than CM group. Previous studies reported mixed results regarding the clinical outcomes and complications in patients who had postoperative CM after ASD surgery. In addition, there was significant heterogeneity in the definition of CM and which PROs being used in the literature. Bao et al. used 3 cm as the cut-off for CM and found that the postoperative CM patients had lower VAS and SF-36 scores than those postoperative CA patients at 1-year post-operation. Walker et al. used the same definition of CM and showed worse VAS back pain scores in type C patients who had postoperative CM than those without CM at 1 year following the CMIS technique. 6 Acaroglu et al. demonstrated that the coronal malalignment negatively affected the SRS-22 scores in their multicenter study. 23 Contrasting to these results, Tanaka et al. defined the CBD of more than 20 mm as the imbalance and reported that postoperative CM had no significant correlation with the ODI and Roland-Morris Disability Questionnaire (RDQ) scores but it was correlated with the frequency of rod fracture at 2-year follow-up. 17 Zuckerman et al also found a significant association between postoperative CM and complications at a 2-year follow-up. However, it was not significantly associated with readmission, reoperation, and clinical outcomes, including ODI and SRS-22 scores. 19
This study has some limitations. First, this is a retrospective study and has only 1-year of follow-up. The CBD might change during the long-term follow-up. Second, we did not report the complications between the postoperative coronally balanced and imbalanced patients.
Conclusions
Our study suggests that CMIS with OLIF technique without the posterior osteotomies for ASD correction significantly improves radiographic and clinical outcomes. The postoperative CM occurs at similar rates to open surgery, and type C patients were at risk of postoperative CM than types A and B. However, most of the 1-year clinical and radiographic outcomes were not significantly different between the postoperative CA and CM patients regardless of the preoperative coronal alignment characteristics except that the postoperative CA patients had lower ODI scores than the postoperative CM patients in the type A subgroup.
Footnotes
Acknowledgments
Teerachat Tanasansomboon would like to express heartfelt gratitude to his wife, Thanachaporn Kittipibul for her devotion. We joyfully welcome our baby boy “Darwin” into this world.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.