
Abstract
Study Design
Retrospective study
Objectives
The combination of oblique lateral interbody fusion (OLIF) with grade 2 posterior column osteotomy (PCO) is an effective treatment for adult spinal deformity. However, grade 2 PCO may lead to pseudoarthrosis because it involves complete removal of the bilateral posterior facet joints. The main study objective was to determine the achievement rate of anterior and posterolateral fusion resulting in circumferential fusion in patients who underwent combined OLIF and grade 2 PCO.
Methods
This retrospective study included consecutive patients who underwent OLIF and grade 2 PCO. The group comprised a long fusion group, with fusion from the thoracic level to the ilium, and a short fusion group, with fusion within the lumbar region. The OLIF with percutaneous pedicle screw insertion group was also used for reference. The Brantigan–Steffee–Fraser classification was used to assess interbody fusion and Lenke classification for assessment of posterolateral fusion.
Results
Sixty-six patients with 109 lumbar levels were included in the study. We observed 100% anterior fusion in all 3 groups. The fusion rate for posterolateral fusion between the OLIF-grade 2 PCO group was 97%, with very low (3%) non-circumferential fusion (pseudoarthrosis only at the osteotomy site). In most cases, solid posterolateral fusions (Lenke A) occurred within 24 months.
Conclusions
The combination of OLIF and grade 2 PCO resulted in circumferential fusion for most (97%) of the cases within 24 months. OLIF and grade 2 PCO are considered a good combination treatment to achieve sufficient lumbar lordosis and solid bone fusion.
Keywords
Introduction
Oblique lateral interbody fusion (OLIF) has been widely used in the surgical treatment of adult spinal deformity (ASD) and lumbar degenerative diseases in recent years. There are several advantages of using OLIF for the surgical treatment of these diseases. One of the advantages is relatively solid bone fusion, mostly due to the wider contact area of the OLIF cage with adjacent vertebral bodies, including the cortex area. 1 In the literature, the fusion rate of the anterior body with use of OLIF has been favorable, with reports of a fusion rate between 93% and 97.9%.1-3 Hynes et al. performed a retrospective analysis of 137 patients who underwent OLIF for degenerative lumbar diseases at 340 levels and noted a 97.9% fusion rate from CT findings. 2
Meanwhile, grade 2 posterior column osteotomy (PCO), as classified by Schwab et al., 4 is a very effective and widely used procedure to achieve lumbar lordosis for the surgical treatment of ASD. 4 In addition, obtaining appropriate lumbar lordosis for any type of lumbar degenerative disease is essential to achieve long-term results when we fuse any segment. This is partly due to the fact that patients lose the ability to compensate within the area of fusion after surgery.
However, one of the potential problems of grade 2 PCO is that the procedure potentially increases the risk of pseudoarthrosis as it removes the facet joint bilaterally. Historically, grade 2 PCO is often combined with posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF). PLIF/TLIF has been widely used for lumbar interbody fusion; however, these methods result in less contact area with adjacent vertebral bodies compared with OLIF.
If OLIF secures anterior bone fusion, we can achieve a relatively significant amount of lumbar lordosis by performing multilevel grade 2 PCO without potential risk of pseudoarthrosis for ASD. Taken together, we hypothesized that OLIF and grade 2 PCO are a good combination to achieve sufficient lumbar lordosis and solid bone fusion for ASD and other lumbar degenerative diseases.
We applied this combined OLIF-grade 2 PCO procedure for the treatment of these diseases. In this study, we retrospectively evaluated circumferential bone fusion at several time points after surgery. We also compared this combined procedure with the OLIF percutaneous pedicle screw (PPS) procedure for relative evaluation.
Materials and Methods
Patient Population
In this retrospective study, the inclusion criteria were as follows: (a) surgery (OLIF) performed after March 2014 at a single institution for ASD and lumbar degenerative diseases; (b) surgery performed by a single surgeon; (c) use of only autologous iliac crest bone graft (ICBG); (d) minimum follow-up of 2 years; and (e) CT of the lumbar spine scanned every 6 months for 2 years. These CT images were captured using very low-dose radiation. We did not perform CT for patients who had a relatively large risk of radiation and excluded these patients from the study. The authors collected consecutive patients who met the first 3 inclusion criteria, and 88 patients were identified. Among 88 patients, 66 patients met the last 2 criteria (Figure 1). Summary of patient grouping.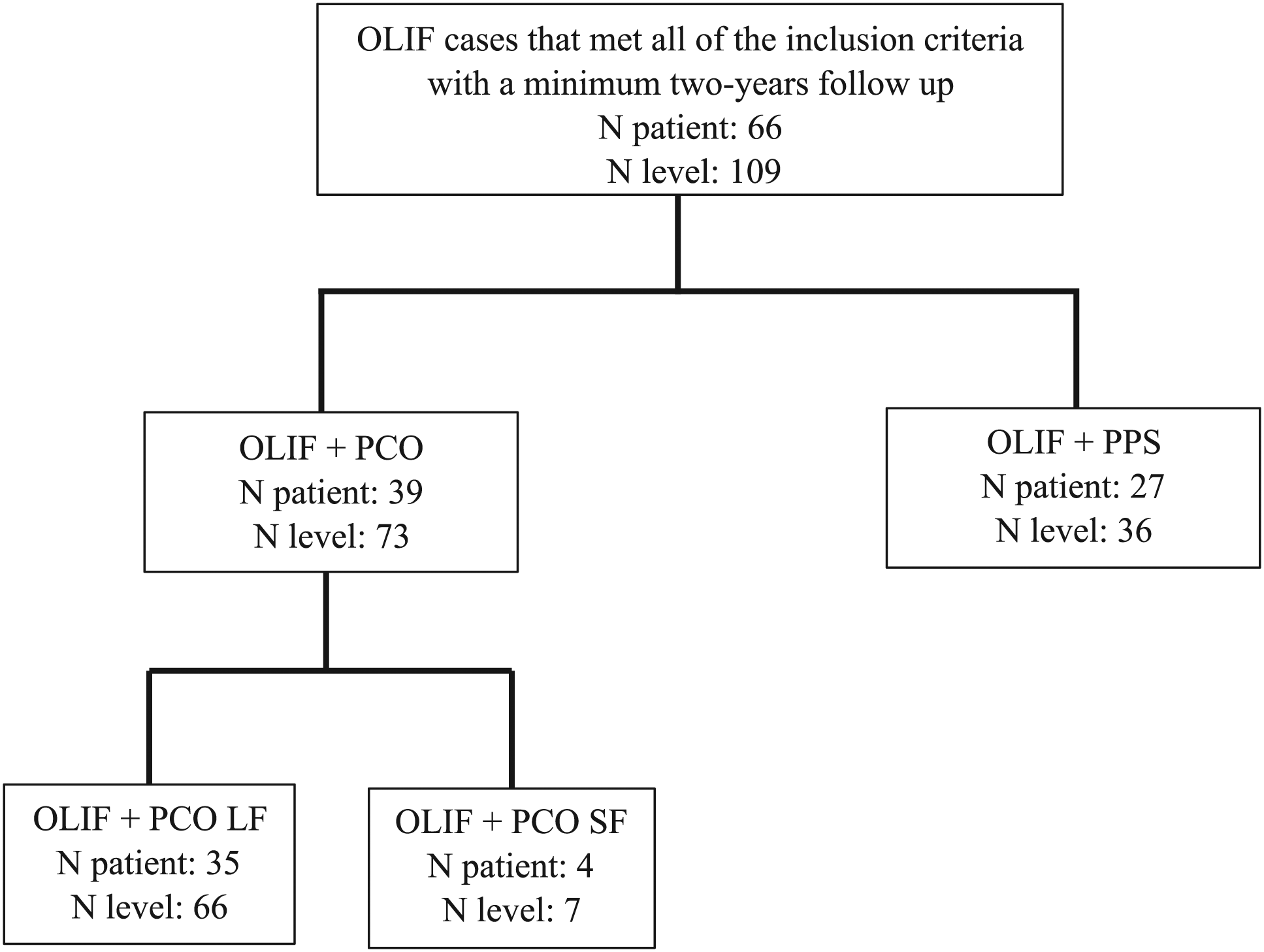
Cases in which we performed OLIF+grade 2 PCO with fusion from the thoracic level to the ilium were designated as the OLIF-long fusion (LF) group. Cases in which we performed OLIF+grade 2 PCO with fusion within the lumbar region were designated as the OLIF-short fusion (SF) group. Cases in which we performed OLIF combined with PPS procedure were designated as the OLIF-PPS group. Thirty-five patients belonged to the OLIF-LF group, 4 to the OLIF-SF group, and 27 to the OLIF-PPS group.
The age of the patients ranged from 43 to 84 years (mean 66.8), with 23 men and 43 women. The total spinal levels operated on were initially 112; however, ultimately, there were 109 spinal levels after 3 were excluded for anterior longitudinal ligament rupture when performing the posterior correction procedure. In all, 66 levels were analyzed in the OLIF-LF group, 7 levels in the OLIF-SF group, and 36 levels in the OLIF-PPS group (Figure 1). The data collected was from March 2014 to June 2019 only in cases with a minimum of 2 years of postoperative follow-up. Data beyond 2 years was not included in the study. Therefore, the follow-up period was 2 years for all cases.
All processes of the current study were reviewed and approved by the Institutional Review Board of the National Hospital Organization Murayama Medical Center (approval #12-10), and all patients provided written informed consent to participate in this study.
Surgical Indication
Surgical indications in the OLIF-grade 2 PCO group were based on the severity of spinal deformity and clinical symptoms. The LF subgroup consisted of spinal deformity with global malalignment; meanwhile, the SF subgroup consisted of spinal deformity without global malalignment. The relevant clinical symptoms were severe low back or back pain after a prolonged period in the standing position.
We regularly perform a preoperative casting test for patients with spinal deformity as a simulation tool by casting patients in the supine position. This confirms that there is an increased likelihood that the symptoms originating from spinal deformity would reduce by correction surgery. Patients who did not experience pain relief during the casting test were not considered candidates for this surgery.
Using radiological parameters, we regarded spinal deformity as “global malalignment” if the patient had at least 1 of the following conditions: pelvic incidence (PI)−lumbar lordosis (LL) ≥ 30°; pelvic tilt (PT) ≥ 30°; and coronal C7 plumbline offset ≥5 cm. Among the sagittal parameters, we mainly used PI-LL and PT in our practice, since PT is more reliable than the sagittal vertical axis (SVA) (SVA tends to be variable even in the same patient). Spinal deformity without global malalignment was considered for PI-LL of ≥20° (<30), PT of ≥25° (<30), and Cobb angle (scoliosis) (at the standing position) of ≥25°.
On the other hand, indication for surgery in the OLIF-PPS group was degenerative spine disease without spinal deformity. Radiologically, surgery was indicated when there was evidence of severe segmental instability with or without severe spinal canal stenosis at the lumbar level. Clinical symptoms in the OLIF-PPS group were severe lower limb symptoms (such as pain and numbness) or low back pain that had not been significantly reduced by non-surgical treatment, such as pharmacological treatment. For reference, we have included data regarding clinical symptoms of the patients in Table 5.
Surgical Procedure
A single surgeon at the same spine institution operated on all the patients. The spinal levels operated on for OLIF were L2/3, L3/4 and L4/5. For multilevel OLIF, only a single incision was made.
When performing OLIF, all patients were positioned in the right lateral decubitus position. The anatomical surface of the disc was obtained under fluoroscopic guidance in a true lateral view. Skin incisions were made parallel to the external oblique muscle fibers and centered at the targeted segment. The blunt muscle splitting technique was used to dissect the external oblique, internal oblique, and transverse abdominal muscles along the direction of the fibers until the retroperitoneal fat tissue was visualized. This fat was retracted anteriorly together with the retroperitoneal space, while the psoas muscle was retracted posteriorly. The disc space was exposed and the targeted level was confirmed with fluoroscopy. Tubular retractors were docked to the disc space, followed by discectomy and vertebral end plate preparation. An OLIF cage packed with pure autologous ICBG was inserted. The cages used were either polyetheretherketone (PEEK) or PEEK with titanium coating (PEEK-PTC) (Clydesdale Pure Titanium Coating) (Medtronic Sofamor Danek, Memphis, TN, USA) with lordosis of 6° or 12°.
Grade 2 PCO was performed via the posterior midline approach in the prone position. Total removal of bilateral facet joint, wide inferior and superior laminectomies, and resection of the ligamentum flavum were performed at the intersegmental level.
4
Closure of the gap was then performed using a compressive device applied on spinal titanium alloy rods until contact of the opposite lamina borders was achieved. Then, local bone grafts were placed in the posterior lateral lumbar spine. Then, fixation using instrumentation, such as pedicle screws, was performed for stabilization (Figure 2). Representative case. A 71-year-old female with degenerative lumbar kyphoscoliosis. Preoperative and postoperative standing whole spine Xp of P-A view (a,c) and lateral view (b,d). Multilevel oblique lateral interbody fusion (OLIF) (L2/3, L3/4, L4/5) combined with grade 2 posterior column osteotomy (PCO) was performed as corrective surgery in this case.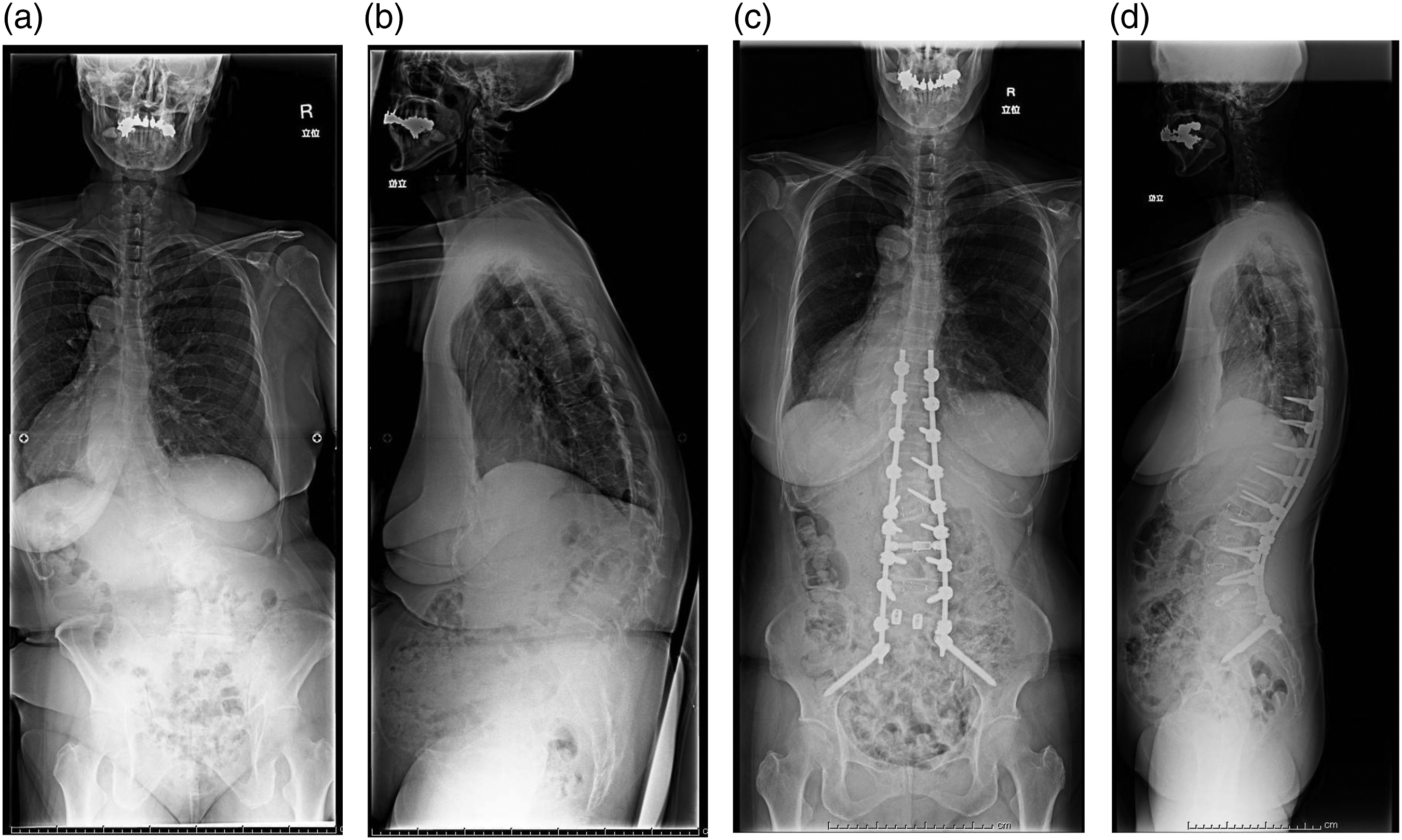
In the OLIF+PPS group, the OLIF cages were stabilized with PPS. The pedicles were identified using a radiographic imaging intensifier. A guide wire was inserted, followed by dilators, pedicle screws, and rods. Bone grafts were not inserted at the posterior site in the OLIF+PPS group.
Radiographic Assessment
The cage locations at the intervertebral space were divided into 3 areas: the anterior third, middle third, and posterior third.
Fusion was analyzed at 6 months, 12 months, 18 months, and 24 months postoperatively using CT imaging (Figure 3) by the examiner instead of the surgeon. Representative CT images of posterior facets at 1 week after surgery and 24 months after surgery. Coronal views of 3 different cases. Images at 24 months after surgery indicate posterolateral fusion of Lenke A for case 1, Lenke B for case 2, and Lenke C for case 3 (arrows).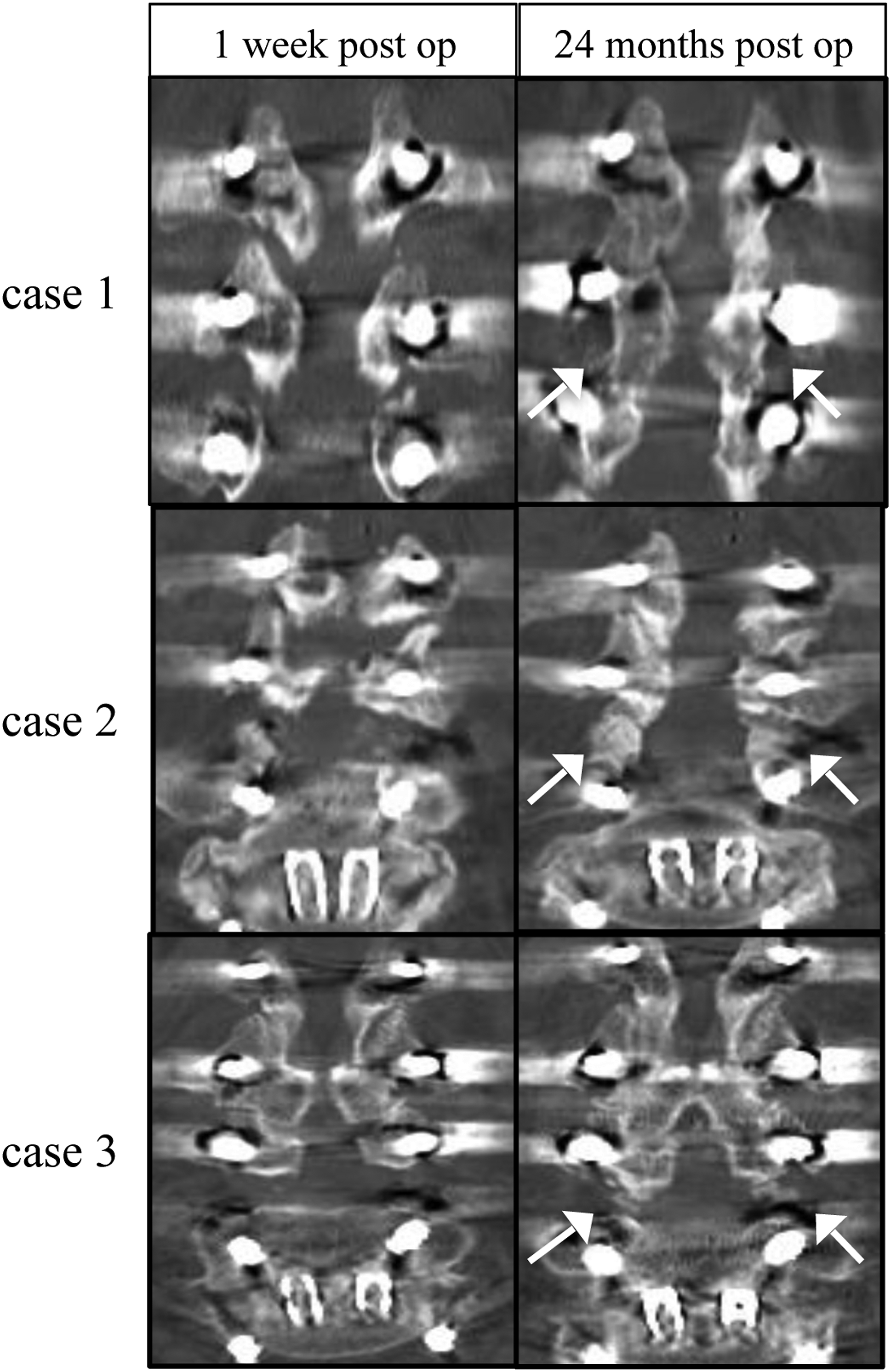
The Brantigan–Steffee–Fraser (BSF) classification was used for assessment of interbody fusion5,6 and Lenke classification for assessment of posterolateral fusion
7
(Figure 4). (A). Classification of interbody fusion performed by Brantigan, Steffee, and Fraser (BSF). (B). Lenke classification of posterolateral fusion.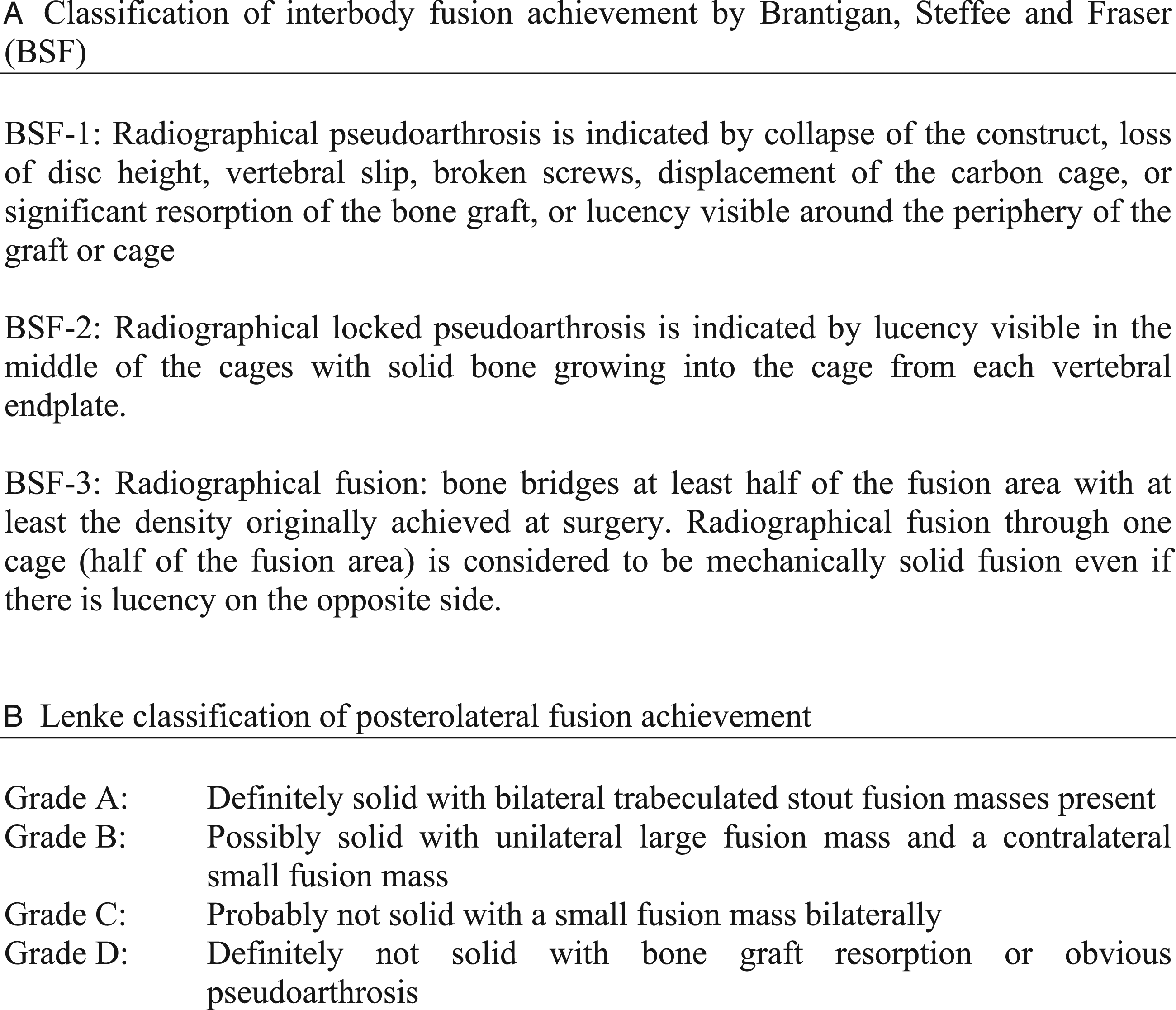
To validate the method of fusion assessment, we performed intraobserver and interobserver reliability analyses of the method. 8 Intraobserver reliability was assessed by performing the fusion assessment once a day for 3 consecutive days, obtaining a total of 3 fusion assessments. For intraobserver reliability assessment, 15 different samples were used. Interobserver reliability was assessed by 6 spine surgeons. For the interobserver reliability assessment, 15 different samples were used for each assessor. Interobserver and intraobserver reliabilities were estimated by calculating intraclass correlation coefficients at 95% confidence intervals using IBM SPSS Statistics (version 27) (IBM, Armonk, NY, USA).
To assess the efficacy of grade 2 PCO in restoring adequate lordosis, we measured the lordotic angle of each level and compared it with that of the OLIF-PPS group. Reconstructed sagittal plane CT scans were used for accurate assessment of the lordotic angle at each level. We analyzed the levels for which an intervertebral cage with 12° lordosis was used. The levels at which end plate damage was observed were excluded. The actual postoperative lordotic angle at each level was divided by the lordotic angle of the intervertebral cage (12°), and the calculated value was regarded as the lordosis achievement rate.
All radiographic parameters were assessed by a digital viewer; Surgimap Spine (Nemaris, Inc., New York, NY, USA).
Statistical Analysis
Data was analyzed using IBM SPSS Statistics (version 27). Different parameters between the 2 groups were analyzed with a t-test for continuous variables and the chi-square test, or Fisher exact test, for categorical variables. Statistical significance was defined as a P value less than .05.
Results
Age, Sex, and Other Factors
Summary of each group’s demographics, cage types/placement.
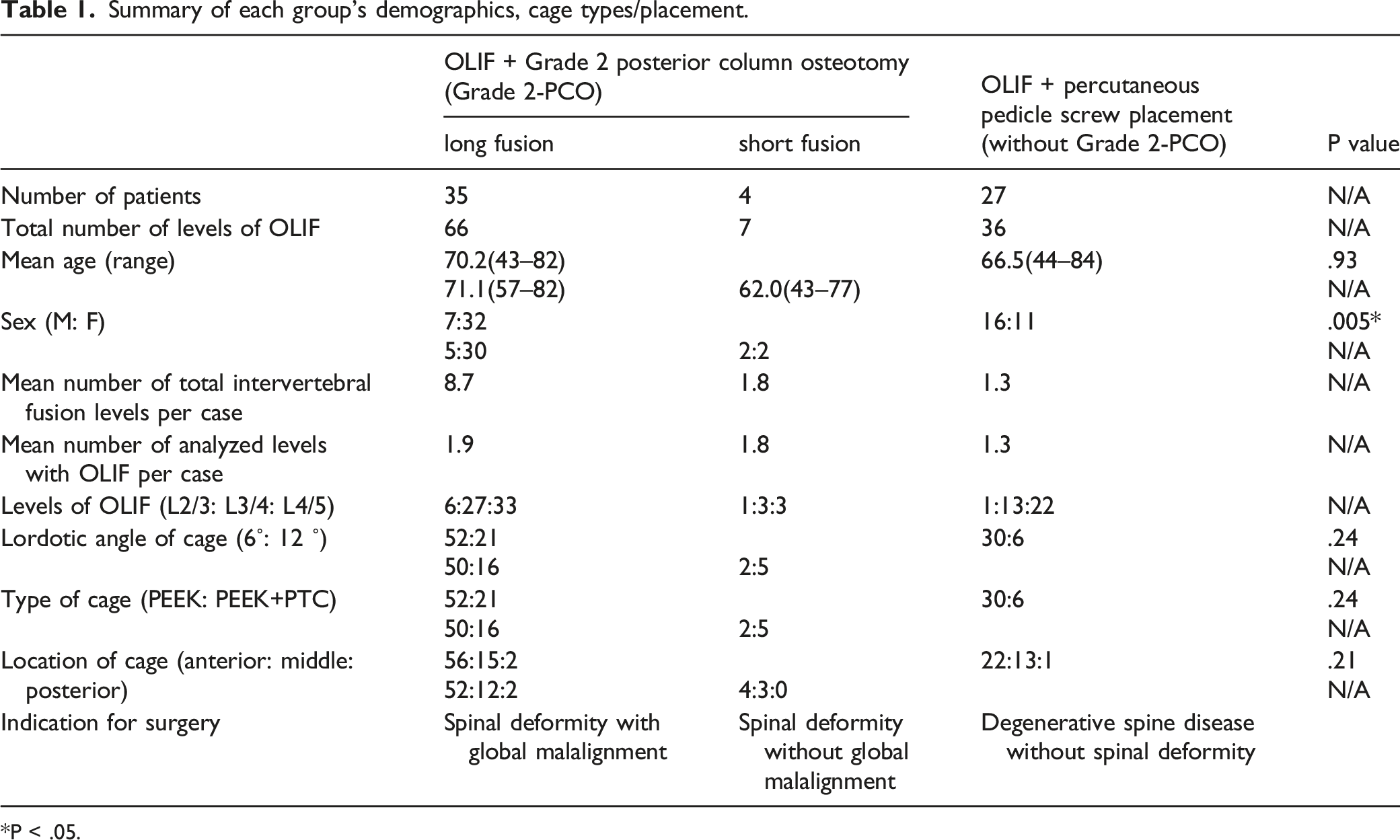
*P < .05.
Types and Location of the Cages
Two types of OLIF cages were used: 6° lordosis PEEK cage (6° PC) and 12° lordosis PEEK+PTC cage (12° PTCC). In the OLIF-grade 2 PCO group, 52 6° PC and 21 12° PTCC cages were used. In the OLIF-PPS group, 30 6° PC and 6 12° PTCCs were used.
Regarding the locations of the intervertebral cage, 56 cages were placed in the anterior third of the intervertebral space, 15 in the middle third, and 2 in the posterior third in the OLIF-grade 2 PCO group. Meanwhile, in the OLIF-PPS group, 22 were placed in the anterior third, 13 in the middle third, and 1 in the posterior third (Table 1).
Level of Surgery
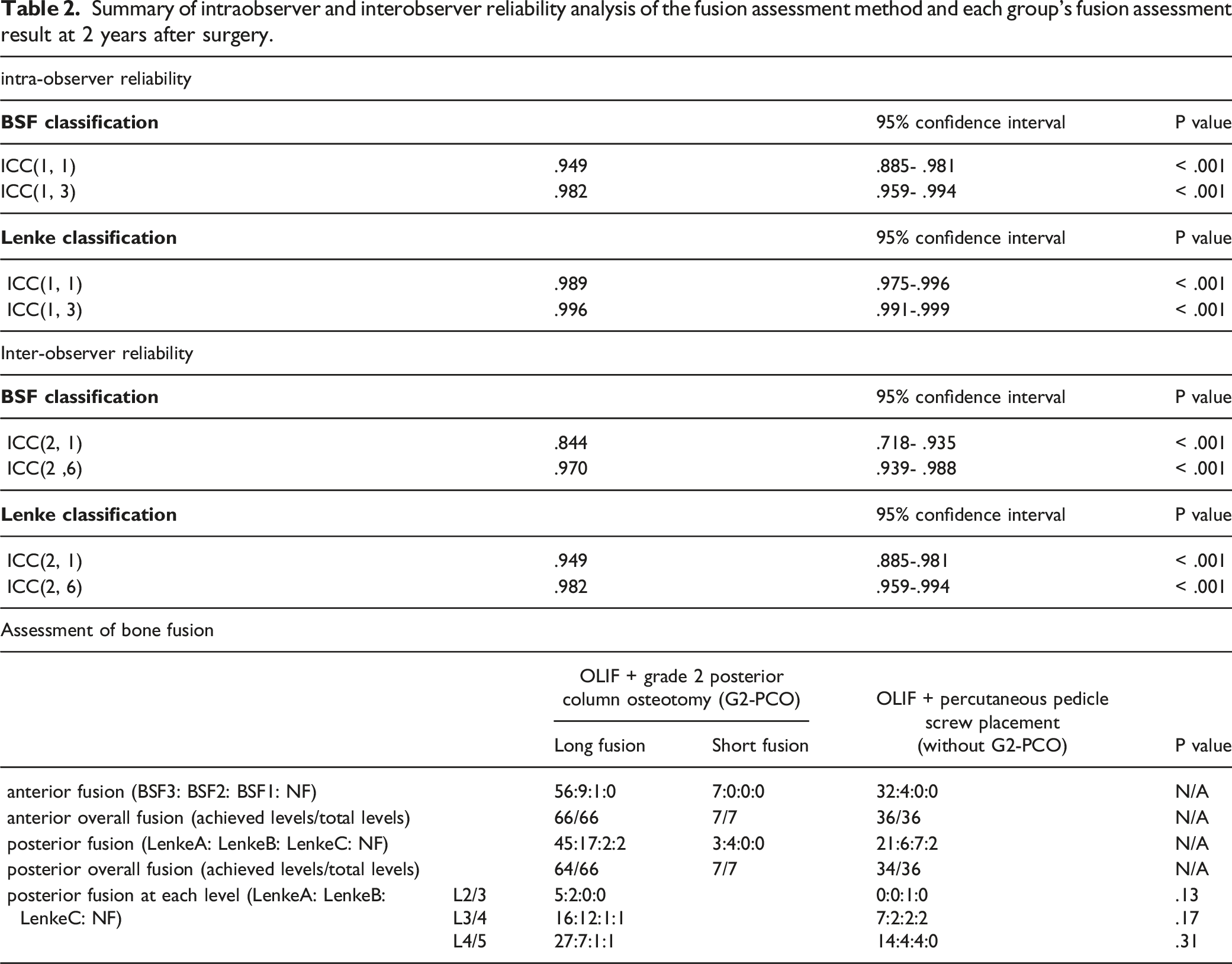
Summary of intraobserver and interobserver reliability analysis of the fusion assessment method and each group’s fusion assessment result at 2 years after surgery.
Intraobserver and Interobserver Reliability Analysis of Fusion Assessment Methods
To validate the methods of fusion assessment (BSF classification and Lenke classification), we performed intraobserver and interobserver reliability analyses of the method. The interobserver and intraobserver reliability data are presented in Table 2. These values indicate that these assessment methods have excellent interobserver and intraobserver reliabilities. Taken together, we consider that these methods are sufficiently reliable to assess bone fusion in this study.
Assessment of Degree of Lordosis Achievement
To assess the efficacy of grade 2 PCO in restoring adequate lordosis, we measured the lordotic angle of each spinal level and compared it with that of the OLIF-PPS group. On average, the lordosis achievement rate (±S.E.M.) was 98.6% (±8.4%) in the OLIF-grade 2 PCO group and 65.3% (±4.5%) in the OLIF-PPS group, with a significantly higher lordosis achievement rate in the OLIF-grade 2 PCO group (P = .0059).
Assessment of Fusion and Health-Related Quality of Life Scores
Bone fusion was observed in the anterior interbody and posterolateral regions. Anterior interbody fusion was observed in all cases (100%) in the OLIF-grade 2 PCO and OLIF-PPS group within 2 years. Anterior fusion occurred as early as 6 months postoperatively. BSF type 3 was the most common form of anterior fusion (95%) 2 years after surgery (Table 2).
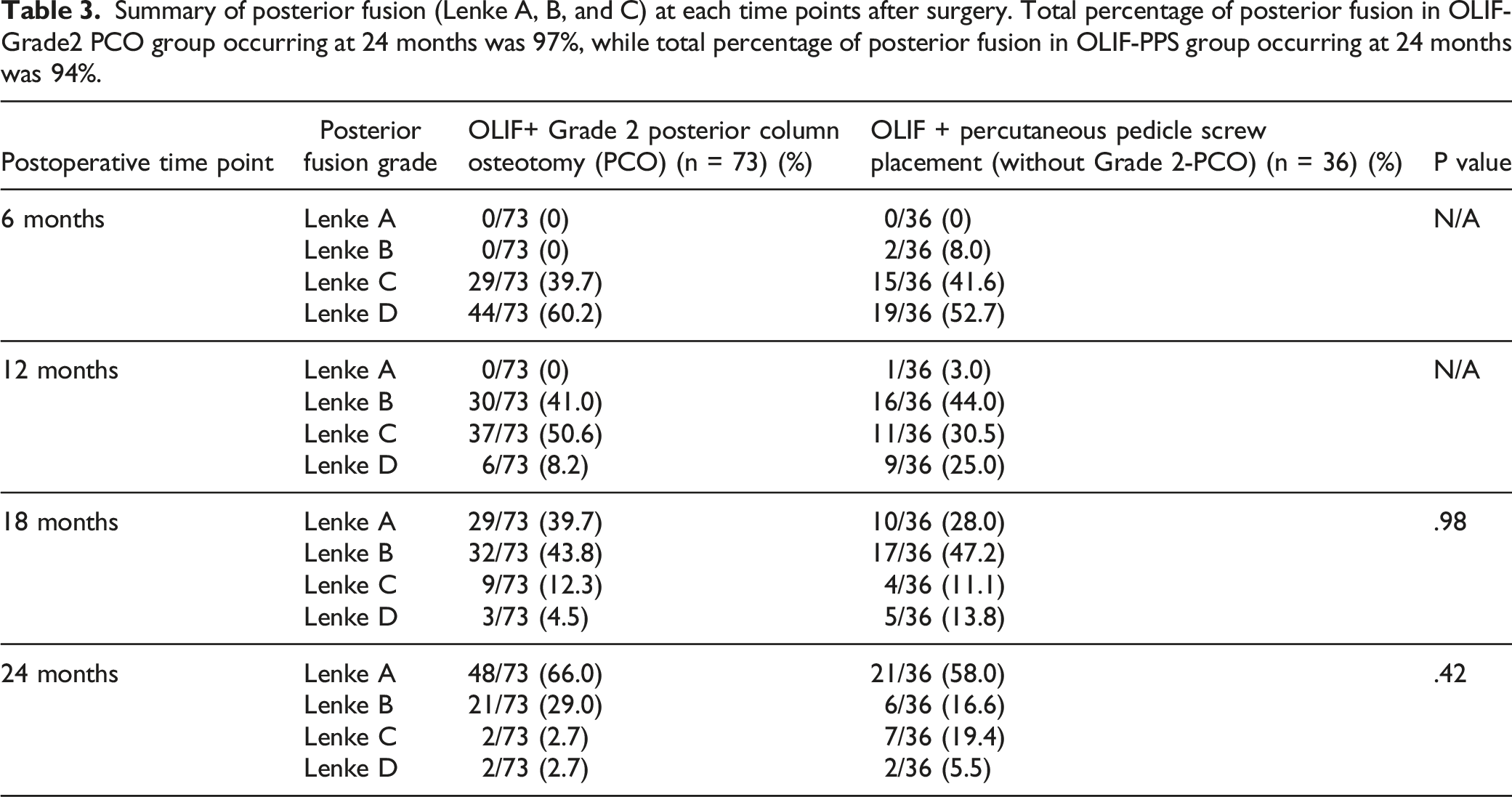
Summary of posterior fusion (Lenke A, B, and C) at each time points after surgery. Total percentage of posterior fusion in OLIF-Grade2 PCO group occurring at 24 months was 97%, while total percentage of posterior fusion in OLIF-PPS group occurring at 24 months was 94%.
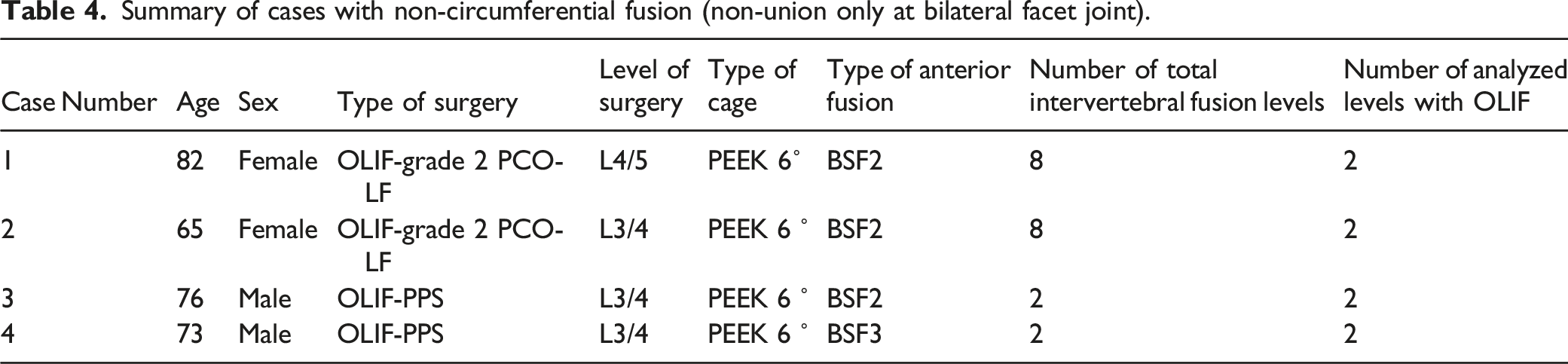
Summary of cases with non-circumferential fusion (non-union only at bilateral facet joint).
Summary of health-related quality of life scores etc.
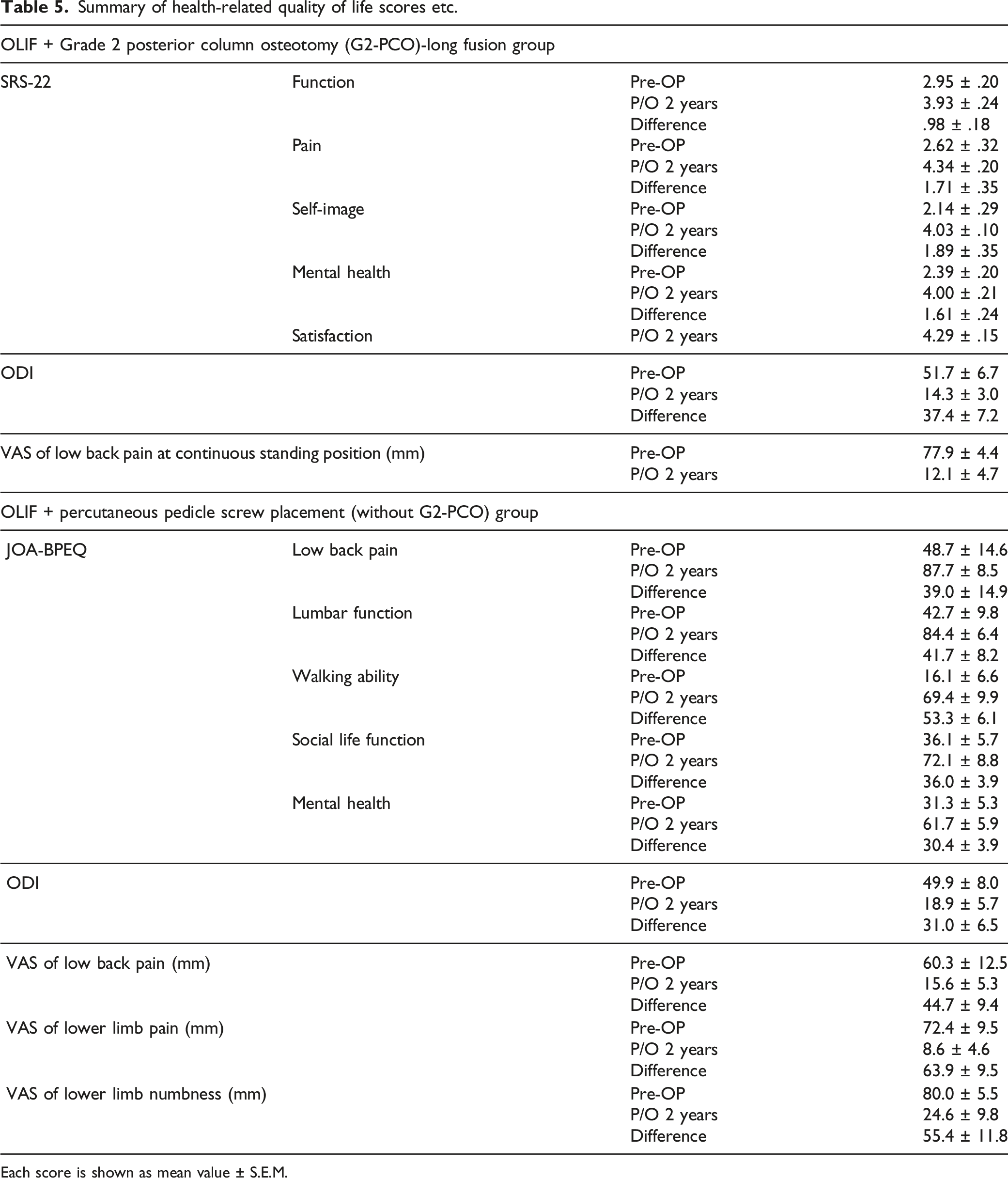
Each score is shown as mean value ± S.E.M.
Discussion
Many spine surgeons combine anterior and posterior lateral fusion to achieve circumferential fusion in treating spinal disorders. 13 Circumferential fusion is defined as fusion of the anterior body along with the posterolateral lumbar spine. Many authors have found satisfactory circumferential fusion rates of up to 96% with a combination of interbody cages, such as ALIF, PLIF or TLIF, and posterior rigid instrumentation. 13
Although fusion may be achieved by anterior interbody cages combined with posterior lumbar rigid instrumentation, 14 the situation differs in lumbar deformity cases that require osteotomy. The rate of pseudoarthrosis after three-column osteotomy, such as pedicle subtraction osteotomy (PSO), has been reported to be relatively high.15-27 Kim et al. reported a rate of 29% pseudoarthrosis in 35 patients. They reported that 5 cases developed pseudoarthrosis within 2 years and another 5 occurred between 2 and 4 years postoperatively. 20 Pseudoarthrosis may present as rod fracture, progression of deformity, or distal segment disc collapse. 18 Barton et al. 25 reported that the total incidence of rod fracture was 16.2% in PSO compared with 2.6% after SPO. 25
However, studies on the prevalence of fusion after grade 2 PCO are scarce. Therefore, we examined the incidence of circumferential fusion when grade 2 PCO was combined with OLIF (OLIF-grade 2 PCO) in the present study. We also examined the achievement rate of circumferential fusion of OLIF-PPS cases for reference. We hypothesized that the achievement rate of posterolateral fusion after grade 2 PCO is increased when combined with OLIF due to increased stability of anterior interbody fusion provided by the OLIF cages.
As reported by many studies, the OLIF procedure results in a favorable rate of interbody fusion.1-3 In our series of patients, in addition to interbody fusion, we observed solid posterior lateral lumbar fusion even after posterior osteotomy at the bilateral facet joints. Within 6 months, all patients in the OLIF-grade 2 PCO group developed anterior interbody fusion predominantly of BSF type 2. Posterolateral fusion was observed within 12 months postoperatively, with Lenke grade B in most of the cases. These were later observed to progress to a more solid bone fusion, Lenke grade A, by 18 months.
When performing PSO, lordosis is achieved mainly at one vertebral level, resulting in different shape/alignment of lordosis (sharply bent shape) compared with physiological shape/alignment of lordosis, resulting in a concentration of mechanical stress at the level of PSO. This, in turn, can lead to a high percentage of pseudoarthrosis at the level of PSO. On the other hand, a multilevel grade 2 PCO combined with OLIF gives rise to a more physiological shape of lordosis by restoring sufficient degree of lordosis at each segmental level. This, in turn, may disperse mechanical stress, which may contribute to a lower percentage of pseudoarthrosis.
Interestingly, we observed up to 94% autofusion of the posterior facet joints in the OLIF-PPS group. Initially, posterolateral fusion was not expected in the OLIF-PPS group, as posterior bone grafts were not placed in this group. Autofusion is defined as evidence of fusion mass at a level not previously fused intentionally. 28 The exact pathophysiology of autofusion remains unclear; however, it is presumed to be similar to that of other osteogenic processes. Immobilization, inflammation, vascularization, and decortication are key factors in this process. 29 These factors have been demonstrated in spontaneous fusion in rabbits, where irritation to both vertebral endplates and intervening disc space was sufficient to induce auto fusion in 66.7% of animals. 29 This phenomenon suggests that stabilization of the anterior component by OLIF provides a good environment for posterior lateral fusion, even without posterior bone grafts.
The quality of the graft material is reported to be an important factor in creating circumferential fusion. We used an autologous ICBG for all patients in the present study. Previous studies have concluded that osteogenic and osteoconductive properties decrease with age, and that bone grafts from the anterior iliac crest should be avoided in the elderly. 30 However, this was not the case with our study, as the mean age of the OLIF-grade 2 PCO group was 70.2 years old, which can be regarded as a relatively elderly population, and 97% progressed to circumferential fusion within 2 years. This finding is contrary to the study by Kim et al. 31 that demonstrated that pseudoarthrosis can occur with increasing age, especially after 55 years of age. 31 Regarding bone mineral density, preoperative BMD was not statistically different between the OLIF-grade 2 PCO-LF group (.575 as average), OLIF-grade 2 PCO-SF group (.634 as average), and OLIF-PPS group (.640 as average). In addition, the value of bone mineral density was not statistically different between the non-circumferential fusion group (average .685) (posterior non-fusion) and circumferential fusion group (average .599). These results suggest that stabilization of the anterior component by OLIF provides an optimal environment for bone fusion, regardless of the bone mineral density.
Spinal fusion continues to improve secondary to advances in biologics, instrumentation and surgical techniques. 24 Titanium implants have been demonstrated to induce osteointegration in several clinical studies. This finding coupled with the graft material may enhance interbody fusion. However, in the present study, neither PEEK 6° nor PEEK-PTC 12° used in the OLIF-grade 2 PCO group demonstrated any statistically significant advantages. Similarly, placement of the cage at either the anterior, middle, posterior in the intervertebral space, or lumbar levels operated on at L2/3, L3/4, or L4/5 did not influence posterolateral fusion.
Overall, circumferential fusion was not statistically affected by any factors, such as age, sex, bone mineral density, cage material, and the site of the bone graft. We also observed a very high percentage of circumferential fusion, even in cases without posterior bone graft, in the OLIF-PPS group. As the percentage of achievement of circumferential fusion is already sufficiently high in our series, optimum stabilization of the anterior component by OLIF may provide an optimal environment for bone fusion and result in relatively good bone fusion, even with possible associated risk factors for non-union. As we have observed in the OLIF-grade 2 osteotomy group in this study, stabilization of the anterior component by OLIF ensures solid circumferential fusion regardless of the potential risk factors for non-union mentioned above and even after posterior osteotomy at the bilateral facet joints.
There are a few limitations to the current study. First, this was a retrospective study, and we did not have an ideal control group, such as the PLIF/TLIF-grade 2 PCO group. Future prospective studies may provide more evidence if the potential ethical issues related to the prospective study can be resolved. Another limitation is the limited number of samples in the OLIF-grade 2 PCO-SF group. In general, patients with ASD with severe deformity/global malalignment that require correction surgery are unsuitable for SF, which directly leads to a limited number of OLIF-grade 2 PCO-SF groups. Additionally, a limitation of the study is the disparity in the administration of teriparatide, which reportedly enhances bone fusion. 32 This bone-forming agent was administered to all patients with ASD in the OLIF-grade 2 PCO group compared to only some patients with low bone mineral density in the OLIF-PPS group. However, we employed the OLIF-PPS group for reference, but not for control groups, to assess the bone fusion of the OLIF-grade 2 PCO group in the current study. In other words, we did not perform a direct statistical comparison between the OLIF-grade 2 PCO group and the OLIF-PPS group regarding the bone fusion rate in this study. Furthermore, the OLIF-PPS group showed almost 100% bone fusion, regardless of teriparatide treatment. In the OLIF-PPS group, non-circumferential fusion (pseudoarthrosis only at the posterior osteotomy site) was observed in only 2 patients. Among the 2, 1 received teriparatide treatment and the other did not. Therefore, we consider that the use of teriparatide for all patients with ASD in the OLIF-grade 2 PCO group did not affect the main point of the study. Additionally, regarding smoking and its effect on fusion rate, the majority of the patients in our cohort were non-smokers, as we only performed surgery for non-smokers based on our department’s policy in principle. However, there was 1 smoker in the posterior non-circumferential fusion group (posterior non-fusion) and 3 smokers in the circumferential fusion group, which might have affected on the degree of bone fusion.
As previously described, if the OLIF procedure secures circumferential bone fusion, we can acquire a relatively large amount of lumbar lordosis by performing multilevel grade 2 PCO without potential risk of pseudoarthrosis. Based on the results of the present study, it is considered that OLIF and grade 2 PCO are a good combination treatment to restore adequate lumbar lordosis and solid bone fusion for ASD and other lumbar degenerative diseases.
Conclusion
Fusion of the lumbar spine requires favorable biological and mechanical environments. Although grade 2 PCO is a very effective and widely used procedure to restore lumbar lordosis for the surgical treatment of ASD, it may increase the risk of pseudoarthrosis because it removes the facet joint bilaterally. The result of fusion using the combined procedure of OLIF-grade 2 PCO resulted in 100% anterior fusion and 97% circumferential fusion, which can be regarded as a relatively good bone fusion rate compared with previous reports. Our study results reveal that the OLIF-grade 2 PCO combination is beneficial for achieving better correction and better fusion in ASD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.